#Diagnostic Labs Market
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr has been banned in Indonesia for providing people with access to pornographic content.
Text

Our Happy Customers!
Thanks for sharing your wonderful experience with us. Buy Athenese-Dx products for more accuracy and consistent quality.
Visit → https://athenesedx.com/news/elisa-instrument-testimonials-insights-from-our-customers-november-2024/
#Instrument #testimonial #happycustomer #athenesedx #ivd #satisfying #highquality #teamsupport #pathology #diagnostics #DiagnosticServices #rapidtest #ELISAKit #ALTA #ALTAInstrument #TRUSTline #TRUSTwell #TRUEchemie #medicallaboratory #Distributorship #ClinicalLaboratory
#ivd#lab equipment#hospital#clinical chemistry#pathologist#pathology#pathologylab#digital pathology market#athenesedx#biochemistry#elisa kits#elisa#medical instruments#medical laboratory science#laboratory#biotechnology#diagnostic services
0 notes
Text
Huda Market, sector 14, Faridabad faridabad Top-Rated Diagnostics
Looking for reliable and accurate medical testing services in Huda Market, sector 14, Faridabad faridabad? Look no further than our diagnostic centers.
#diagnostic centres in Huda Market#sector 14#Faridabad faridabad#Book test in Huda Market#Faridabad#diagnostic centres near Huda Market#Faridabad lab tests#medical testing#accurate results#trusted#Health Check Packages#free sample collection
0 notes
Text
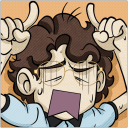
Philippines Pharmacy Retail Market is anticipated to grow by USD 6Th Mn by 2025- How will the market gain traction to be able to reach at its targeted number?
The government distribution of medicines will improve in future due to the initiatives such as Botika Ng Bayan, Distribution through Local Health Units and Rural Health Units, says a report by Ken Research
1.Corona Virus effect on pharmacy sales in Philippines Pharmacy Retail Market.
Other Challenges in Philippines Pharmacy Retail Market Outlook to 2025
Demand for OTC products like Alcohol Based Cleaners, Vitamin C and D Tablets, Immunity Boosters and Health Supplements was boosted during quarantine. Maintenance Medicines were also in high demand. During the starting of the Quarantine, Pharmacies witnessed increase in sales due to bulk purchase, later the sales declined. Pharmacies faced supply chain issues especially in the ECQ zones. This has affected the sales of the pharmacies. Further, Philippines witnessed lockdown for a long duration.
2.Trends and Development that the Pharmacy retail market of Philippines will experience.

Download Sample Report
In July 2018, DOH relaunched Botika Ng Bayan initiative to provide free essential medicines for common diseases focusing on rural and poor people. The chain stores have increased tremendously in the Philippines. Especially TGP and Generika as they have adopted franchise model for store expansion. This increase in chained pharmacies has led to the growth of house brands or private labels. In starting of 2019, President Rodrigo signed Universal Health Care (UHC) Bill into law (Republic Act No. 11223) which automatically enrolls all Filipino citizens in the National Health Insurance Program. This will increase the healthcare affordability in the region.
3. Assessing the Possibilities in the Philippines Pharmacy Retail Market

Ask For Customization
Penetration of internet, growth of social media has opened more connectivity options for the companies.
Drive Through Stores, self-service stores are increasing customer convenience.
This has helped in increasing the footfall in pharmacies for purchasing non pharmaceutical products.
Chain stores can serve regional customers where they don’t have strong presence.
Key Segments Covered
By Market Structure (In USD Billion)
Organized Market
Unorganized Market
Type of Store Location (In USD Billion)
Standalone Pharmacy
Hospital Based Pharmacy
By Region (In USD Billion)
North
Central
South
By Type of Sales (In USD Billion)
Prescribed Medicines
OTC Products
Non Pharmaceutical Products
Medical Equipment
By Type of Drug (In USD Billion)
Generic
Patented
By Therapeutic Class (In USD Million)
Cardiovascular
Anti-Infectives
Pain/Analgesics
Anti Diabetic
Vitamins/Minerals /Nutrients
Dermatology
Respiratory
Gastro Intestinal
Neuro
Oncology
Contraceptive
Gynecological
Ophthalmological
Others
Companies Covered
Mercury Drug Corporation
Watsons Personal Care Stores
SouthStar Drug Inc.
The Generics Pharmacy
Rose Pharmacy
Generika Drugstores
Several Regional Players & Others
Key Target Audience
Pharmaceutical Manufacturer Companies
Pharmaceutical Importing Companies
Pharmaceutical Distributing Companies
Major Retail Companies
E-Commerce Pharmaceutical Retailers
Consultancy Companies
Industry Associations
Regulation Bodies
Time Period Captured in the Report:
Historical Period: 2014-2019
Forecast Period: 2020-2025
Key Topics Covered in the Report
Healthcare System in the Philippines
Major Hospitals & Doctors in the Women Healthcare
Usage of Contraception & Family Planning in the Philippines
Health Insurance in the Philippines
Supply Structure of the Philippines Pharmacy Retail Market
Trends & Development in the Philippines Pharmacy Retail Market
Issues & Challenges in the Philippines Pharmacy Retail Market
SWOT Analysis & BCG Matrix in the Philippines Pharmacy Retail Market
Philippines Pharmacy Retail Market Size & Segmentation, 2014-2019
Online Pharmacy Regulations in the Philippines
Telemedicine & Growth of Online Medical Consultation in the Philippines
Major Telemedicine Providers in the Philippines
Operating Model of Hybrid Pharmacies
Competition Scenario, Market Share, Cross Comparison of Major Players (Online & Offline) and Company Profile
Assessing Regional Pharmacies in the Philippines
Corona Virus Impact on the Consumer Behavior & Pharmacy Sales
Future Market Size and Segmentations, 2019-2025F
Covid 19 Impact on the Philippines Pharmacy Retail Market
Analysts’ Recommendations
Contact us:
Ankur Gupta, Head of Marketing and Communications
+91-9015378249
Follow Us
Facebook | Twitter | LinkedIn | Instagram
#Philippines Pharmacy Retail Industry#Philippines Retail Drug Market Report#Philippines Retail Pharmaceutical Sector#Philippines Retail Healthcare Market#Philippines Retail Wellness Market#Philippines Retail Medical Industry#Number of Intravenous Device Philippines#Number of Hospital Beds Philippines#Number of Test Centers Philippines#Number of Imported Medical Device Philippines#Number of Local Medical Device Philippines#Number of Diagnostic Labs Philippines#Number of Respiratory Devices Philippines#Organized Pharmacy Retail Market Philippines#Unorganized Pharmacy Retail Market Philippines#Standalone Retail Drug Market Philippines#Hospital Based Pharmacy Industry Philippines#North Retail Healthcare Market Philippines#Central Retail Pharmaceutical Market Philippines#Prescribed Medicines Market Philippines#OTC Products Industry Philippines#Non-Pharmaceutical Products Industry Philippines#Generic Drug Sector Philippines#Philippines Pharmacy Retail Market Opportunities#Philippines Retail Drug Market Trends#Philippines Retail Wellness Industry Challenges#Major Retail Healthcare Philippines#Leading Retail Pharmaceutical Partners Philippines#Emerging Retail Drug Market Philippines#Top Captive Players Philippines Retail Medical Sector
0 notes
Text
Do At-Home COVID-19 Tests Still Work? - Published Sept 6, 2024
These days, many people use at-home COVID-19 tests when they feel ill, rather than going out to get tested by a professional. (That’s when they bother to test at all.) But for all their convenience, the antigen tests commonly used at home have never been as accurate as PCR tests done in a lab—and the continued mutation of the virus raises additional concerns about their performance.
Rapid COVID-19 tests have never been perfect. How are they holding up as new variants emerge?
The U.S. Food and Drug Administration (FDA) continues to monitor the efficacy of the diagnostics it regulates—and as of August 2023, the FDA said none of the antigen tests on the market were expected to have reduced performance against Omicron or its subvariants. (All of the variants that have emerged since late 2021, including recent ones like KP.3.1.1, are relatives of the original Omicron strain.)
The FDA has also collaborated with a U.S. National Institutes of Health task force set up to monitor how variants affect tests. In 2022, well into Omicron's dominant era, that team concluded that DIY diagnostics continued to work well. Task force member Richard Creager wrote in an email to TIME that the tests still seem able to catch the Omicron spinoffs that are circulating now. “The rapid tests are having no issue detecting the variants,” he wrote, noting that the protein that antigen tests look for has remained fairly stable as the virus changes.
Even if tests have remained constant, our immune systems haven’t. Early in the pandemic, an infected person's “viral load”—the amount of virus in their system—tended to peak around the time their symptoms began. So if someone self-tested on the first or second day they felt sick, they likely had enough virus in their body for a rapid test to detect it.
Now that most everyone has prior immunity from multiple vaccines or infections, the timeline seems to be extended. Viral load now tends to peak around day four or five of symptoms, according to a study published in early 2024. That’s likely because the immune system is primed for action by its previous encounters with the virus, so it responds faster, even before lots of virus has built up in the body. A quicker immune response may mean a faster onset of symptoms.
“If your body has seen the virus before, you’re going to react to it and have an immune response more quickly,” explains study co-author Dr. Nira Pollock, co-director of the Infectious Diseases Diagnostic Laboratory at Boston Children’s Hospital. “That immune response can show up as symptoms.”
From an immune perspective, that’s a good thing. But it can complicate testing, because it means someone may not test positive for COVID-19 until they’ve already been feeling sick for days. In their recent study, Pollock and her co-authors estimated that a COVID-19 antigen test is somewhere between 30% and 60% accurate at detecting an infection on someone’s first day of symptoms, but up to 93% accurate on day four.
Based on such findings, Pollock and other researchers cautioned in a recent review article that people who are symptomatic shouldn’t assume they’re COVID-free based on a single negative antigen test result. Although it's a hard sell for people who no longer take precautions, the ideal scenario is for someone to stay isolated—or at least wear a mask when around other people—and test again around day four of symptoms.
“The instructions for these tests are to do serial testing,” Pollock says. “If you’re symptomatic, you should test early. But if you’re negative, you need to repeat it, because the amount of virus in your nose may not be high enough yet to detect.”
One other factor to consider: tests don’t last forever. Many people stockpiled tests when they were previously available for free through government programs and insurance, and those kits may have since expired. (You’ll soon be able to order four more free tests through the government.) The FDA’s website provides up-to-date guidance on determining how long your kits last.
Expired tests can still work, says Dr. Zishan Siddiqui, an assistant professor at the Johns Hopkins University School of Medicine. He co-authored a 2023 study on Abbott’s popular BinaxNOW tests, which found no major accuracy differences between unexpired tests and those that were five months past expiration. (Siddiqui’s other research suggests unexpired BinaxNOW tests accurately detect COVID-19 cases more than 80% of the time.)
But, although Siddiqui says he isn't too worried about using expired tests, it’s good to remember that their performance can suffer if they’re long past their recommended use dates. If the control line on your test strip doesn’t show up or looks distorted, that’s a good indication that it’s too old to use, he says. Even in Siddiqui's study, which found that expired tests still work, the lines on the old tests showed up more faintly than on fresh tests, making them harder to read.
Whether your tests are old or brand new, it’s good to use some healthy skepticism when interpreting their results. “I trust these tests,” even as the virus evolves, Siddiqui says—but a single result doesn’t always tell the whole story. If you have COVID-like symptoms but test negative, it’s best to be cautious and retest in a few days.
#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator
44 notes
·
View notes
Text

Villain's Day Off

When their favorite minion Aubrey had pointed out the surprisingly empty day on the calendar after reviewing the month’s planned Villainous Events, they’d decided it was well past due to take some time for themself. It felt wrong to ignore all their professionally-inclined projects to instead focus on other things—personal things! Heavens! Their work ethic is crying—but it was also an exciting prospect. A free day in their usually packed schedule is a rare blessing, and they’re not going to squander it.
Aubrey had been thrilled when they’d announced their decision to take the day off, so to speak, but when the favorite minion realized the Boss had planned to simply spend their elusive spare time in the lab on a personal project, rather than say, taking a well deserved break at a spa or something relaxing of that nature? Well. Needless to say, Aubrey was driven to tears of despair; practically chewing on the hem of the uniform.
Oh well.
Villains make people cry, don’t they?
Guess that’s something.
Their day off starts in the lab, tinkering around with their prosthetic arm. It’s actually great fun when not being frantically pieced together with slapdash engineering: duct-tape, shoddy soldering, and a prayer. Having the time to improve upon the already sleek design is not something they’ve often been able to do. The tech that makes up their prosthetic is beyond what’s available on the global market, and certainly not FDA approved in any capacity since they’d done the grafting themself—not having access to human testing means they’d had to be the test subject—and the anchors are secured tightly through their skin into the scapula and clavicle. Nano-electrical technology threads into the surrounding muscle fibers and fascia, allowing a connection between the machinery and their nervous system. Being able to disconnect the apparatus from the base anchors to repair the actual prosthesis as needed was critical to the design, but it meant the actual installation procedure would be experimental at best and suicidal at worst. It had been excruciating and left horrendous scarring around the entire shoulder joint, but it was worth every agonizing second in the end.
The nanobots that they’d had to program and inject after grafting the anchor base was a secondary project, but an exceptional addition. The nanobots are what allow internal improvements around the anchor’s base without requiring them to surgically dig out all the deep tissue intrinsic makeup. They also act as monitors for active issues without requiring external diagnostics to be run weekly, avoiding hours hooked up to machines for maintenance scans. Additionally, and blessedly, they function as a secret weapon of sorts; nobody expects the Villain to heal so quickly—so capable of being throttled by the Hero and still managing to stand up again. They may not be physically strong, (barring the mechanics of their prosthetic, of course) but their endurance knows no bounds.
Their lips quirk up into a crooked grin as they stare down into the internal wiring of their prosthesis. All the minute details wrapped up in an impenetrable metal sheath is a work of art in their eyes, even if no one but they will ever see such beauty. Their toolkit sends off sparks that reflect in the lenses of their goggles as they modify the reaction time of the finger flexion. Dexterity is no laughing matter, after all.
They love their lab; it’s one of their favorite areas of the Lair they’ve built over the past six years they’ve been active as a Villain. It’s not the innermost scientific sanctum, instead one of the more outer sectors of the Lair. There are two halves: divided down the center into medical and mechanical. The Villain is currently perched in one of the metal work stools in the mechanical section, although they’ll migrate back and forth as they test the functionality of the prosthesis’ improvements over the course of the day. There are already a few scorch marks decorating the hem of the left sleeve of their long lab coat, the empty right sleeve knotted off and pulled out of the way as they work. Thankfully, they’re ambidextrous, otherwise they’d never have been able to continue their work after losing their arm eight years ago.
They woke this morning with the sun, energized and moving through their morning ablutions with a contentment they haven’t had in quite some time. Despite getting an early start with all the excitement thrumming in their veins, their zeal hasn’t faded even though it’s well past noon and quickly approaching dinnertime. The Villain hums under their breath as they tinker away, floating gleefully in their little bubble of mechanical fulfillment, drifting in a place where everything is tranquil and perfect, untouchable and impossible to damage—
—but the shattering of one of the mirrored external windows immediately disabuses that notion.
The Villain pauses where they’re hunched over their prosthetic, blinking behind the dark lenses of their safety goggles before straightening up and setting down their tool. They slowly turn to face the direction of the shattered window, pushing their goggles up onto their forehead almost robotically to reveal their unquestionably unimpressed, deadpan expression.
“I have a front door, you know.”
The Hero straightens from what is undoubtedly supposed to be a dramatic, flashy landing pose, gesturing sharply at the Villain with a furious expression—as though this idiot hasn’t just broken about three separate laws barging into the Villain’s private property like this…
“Villain! The Authority knows you’re behind today’s slew of robberies, so surrender quietly and I won’t rough you up too badly when I take you in!”
The Villain blinks slowly as one brow raises higher with each word out of the Hero’s mouth. They shut their eyes with an exasperated sigh, deflating and pinching the bridge of their nose. What sort of nonsense–!
“Aubrey!” they call loudly, knowing their favorite minion is doubtlessly within earshot.
“Yes, Boss?!” barrelling through the doorway like a bat out of hell, Aubrey freezes at the sight of their unexpected guest.
“W-Who-oaah, shit, h-hey, Hero!!” Aubrey stammers nervously, eyes like dinner plates and clutching that ever-present tablet-clipboard close to the chest. It’s only a matter of seconds before the absolute mess of shattered glass strewn across the floor of the Lab sends poor Aubrey into despair and wrathful fury all over again. “W-What have you done to the window?!”
“The Hero has decided to eschew doorways, Aubrey. For some godforsaken reason it seems I am being blamed for some asinine, puerile incidents—robberies of all things—that have occurred today. I am, for once, completely innocent of these claims as my schedule can attest. As such, relay my schedule for the day to the Hero, if you would please, Aubrey,” they command, gesturing lazily and pulling their goggles back down over their eyes as they get back to work on their prosthetic. They pause, raising their chin to add:
“Oh, and put in a work order for the window.”
“Of course, Boss!” Aubrey chirps, perking up immediately from the despair spiral.
“... you’re serious?”
The Villain pauses their soldering, peering up at the flabbergasted face of the Hero, staring gobsmacked amidst the minefield of broken glass. Their eyebrow raises upwards again.
“Deadly.”
“Boss has a very comprehensive schedule, Hero, and don’t you forget it! Today is a rare free day, so Boss hasn’t had anything planned, see? Oh, wait—I should show you the redacted version, haha, can’t show any big plans to the enemy! One sec, let me pull that up…”
The Villain returns their attention to their project halfway through Aubrey’s explanation, certain that their most competent minion is no doubt flawlessly using that thorough schedule on their tablet-clipboard to defend their alibi. The Villain quickly loses themself back in their work, finding the presence of the Hero in their Lab irrelevant to the task at hand; it’s not like they’re currently working on anything that could be thwarted, after all, and they severely doubt that the Hero has any sort of engineering or mechanical knowledge that could allow for sabotage of their prosthetic. With zero threat, the Villain feels perfectly safe letting Aubrey rip the Hero a new one, letting the brightly-colored do-gooder poke around while they work.
They’re in the middle of testing a circuit to check how quickly the upgraded lock-pick kit tucked into one of the fingertips springs into activation when they sense a presence hovering at their side. They continue working as they address said presence.
“Can I assist you in some way, Hero? Surely you’re convinced I had nothing to do with your paltry robberies as proof dictates I’ve been in my lab all day, after all.”
“Ah,” the Hero sounds surprisingly sheepish and out of the corner of their eye they can see the way the Hero rubs the back of a reddish-orange hair-covered neck. It’s a… cute gesture.
Hm. That’s a new thought.
“Yeah, I uh. I’m sorry about your window… I can um. Pay you back for it, if you send me the invoice?”
“I am perfectly capable of paying for my own repairs, Hero.”
“No, I-I’m well aware, Villain, god, I’m just trying to be nice!”
The Villain hums, amused at the frustration and embarrassment coloring the Hero’s voice, their left hand pausing where it’s in the process of retrofitting the external protective plating of the prosthetic so they can reattach and test it with its new improvements.
“I am fairly unfamiliar with the concept, forgive me.”
“... I don’t know whether to be saddened by that statement or to just feel disgusted by it.”
A tiny smirk flits across the Villain’s lips at the disgruntled Hero, entertained by the clearly irritated responses they’re managing to elicit. Perhaps they should consider teasing their Hero more often if these are the types of reactions they get from such behavior.
“Perhaps you ought to examine that dichotomy more closely at a later date, Hero. If you’ll excuse me,” they push past their Hero, prosthetic in hand as they walk over to the medical side of the Lab. They hook themself up to the simple monitoring system—blood pressure, blood oxygen, EEG, EKG—before reattaching the prosthetic and resolutely ignoring the steadfast shadow the Hero is proving to be.
They run through their standard tests while monitoring their vital signs, recording everything in their encrypted files. They attempt some specialized movements next, noting down successes and failures—thankfully the successes vastly outweigh the failures—and by the end of the trials, the Villain determines the upgrades safe for continued use. A quick rotation of the prosthetic in the base elicits a jolt as the nano-electrical anchors re-establish a few musculoskeletal connections, their nervous system lighting up like early Christmas decorations. A soft hiss escapes from between their clenched teeth as they massage the muscles around the anchor base.
“I-I didn’t realize it was an actual prosthetic,” the Hero speaks quietly, tone serious.
“Hm? What sort of assumptions were you making, then?” the Villain replies, more out of general politeness than actual interest; they don’t want to hear platitudes, least of all from The Hero.
There have been far too many comments over the years about their disability and quite frankly they’re sick of it. Past Heroes they’ve gone up against as a fledgling Villain have said things to them like “oh, I’d have been easier on you if I’d known you were crippled” or “I didn’t realize you had it so bad, you must be suffering” and other variations along those two lines of thought. It’s exhausting to be reduced to a limitation when it’s obvious that it doesn’t actually define who the Villain is in any way shape or form. Bad enough that their family started to write them off as a loss when their arm had been destroyed after being caught in the crossfire of that one fight years ago; they don’t need their adversaries not taking them seriously just because of a few measly missing pounds of flesh and bone.
“I–Well, I thought you’d made like, an exoskeleton or something,” the tone sounds embarrassed, and the Villain risks a glance at their Hero and is surprised to see a rather fetching flush decorating those rounded, yet defined cheekbones, “or-or that maybe you were just really dedicated to an aesthetic or something.”
The Villain snorts, charmed by the Hero’s naive interpretation of such an obvious disability, “No, certainly nothing so fanciful. But I applaud you for an interesting take.”
The Hero smiles: a quiet, soft, bashful thing that makes the Villain’s chest feel like it’s full of effervescence, warm and overflowing.
“I’m actually really impressed you’re so strong even with such a–an injury? I, I don’t actually know why you don’t have a right arm—you could have been born without it, I suppose!” The Hero bites at a slightly chapped, plush lower lip, awkwardness settling over a once-vibrant and energetic form into stillness.
The Villain sighs, “Your first assumption was correct, yes. It was an injury. And no, I will not tell you about it.”
The Hero brightens, a broad grin stretching across a soft face, and the Villain immediately feels as though the universe has righted itself. It’s a feeling that definitely needs to be re-assessed at a later date because it’s not something they’ve ever experienced before.
“Well, then yeah! I’m definitely impressed you’re as strong as you are despite such an injury—in spite of it? Or maybe even because of it,” the Hero says, suddenly thoughtful, “I don’t know you well enough to figure either way, I guess.”
The Hero scrubs a hand through bright hair, ruffling the already disheveled strands, “Y’know, and quite frankly I’d be worried if I did know you well enough! What kind of Hero gets to know their Villain like that?”
The Hero’s laughter feels like a hug while the use of a possessive before the Villain’s title makes them feel decidedly short of breath.
The Villain wants to keep the Hero, to possess their Hero entirely, and keep their Hero all for themself.
Forever.
… bit not good, that.
“Hm. Wouldn’t mind being someone’s anything,” they muse quietly and mostly to themself, flexing their right fist and making note with a pleased smile that all the joints move smoothly against one another without any abrasion or noise. They almost miss the soft choking noise that comes from their Hero standing beside them. They tear their eyes from the prosthetic, glancing down at the shorter Hero, only to marvel at the obvious surprise, longing, and the deep, dark blush painting those softer, rounded cheekbones.
Unable to resist a little playful bullying, they reach out,—slowly enough that their Hero could move away if so desired—grasping their Hero’s chin gently in their prosthetic grip. The action elicits a soft gasp from between plush, red-bitten lips.
“Tell you what, my darling Hero,” they drawl, voice low and rich, eyes lidded and locked onto the wide ones belonging to the stunned, flustered prey in their gentle grasp, “I for one have surprisingly enjoyed your company outside of our, hm, working hours, so to speak.”
The Hero’s swallow is audible and the lazy smirk that pulls at the Villain’s lips feels so right. “If you have any interest in perhaps continuing this, ah… parley if you will—feel free to come back next week. I’m sure I can have Aubrey get my thoroughly redacted schedule to you somehow. I have plenty of resources at my disposal, after all, and well… evil never sleeps, now, does it..?”
Their voice has dropped into a rumbling purr by the end of their short monologue, the Hero’s breathing rapid and pulse like a frantic hummingbird’s wing-beats against the sensors in their prosthetic’s fingertips. Gently, they let go of the Hero’s chin, a soft brush against flushed skin seeming to act as a jolt to the Hero’s system, causing the blushing fool to throw every ounce of bodyweight backwards. The bumbling Hero stumbles wide-eyed against tables and lab equipment in the mad dash to get to the door without turning around, fleeing as fast as possible.
The Villain watches their Hero run from their oh-so-tender clutches, buoyed with the knowledge that without a doubt they’ve succeeded in accomplishing something they’d never considered possible before.
They’ve caught the attention of Their Hero: not with cunning, or power, or violence, even. But with conversation and a hint of flirting!
What a fascinating new development.
They can’t wait to see what comes of it.
⫷ PREVIOUS ⪡ ║║ ⪢ NEXT ⫸

My designs for Villain and Hero found [ here ]
shout out to adornedwithlight for the reblog banner & barbed wire divider
#hero x villain#villain x hero#hero / villain#hero and villain#heroes and villains#my writing#villain oc#hero oc#original character#my characters#genderless oc#androgynous oc#reposting from my old writing blog#this is hobbyistauthor btw tumblr nuked me
14 notes
·
View notes
Text

Topics: health care, monopoly
In a recent article for Tikkun, Dr. Arnold Relman argued that the versions of health care reform currently proposed by “progressives” all primarily involve financing health care and expanding coverage to the uninsured rather than addressing the way current models of service delivery make it so expensive. Editing out all the pro forma tut-tutting of “private markets,” the substance that’s left is considerable:
What are those inflationary forces? . . . [M]ost important among them are the incentives in the payment and organization of medical care that cause physicians, hospitals and other medical care facilities to focus at least as much on income and profit as on meeting the needs of patients. . . . The incentives in such a system reward and stimulate the delivery of more services. That is why medical expenditures in the U.S. are so much higher than in any other country, and are rising more rapidly. . . . Physicians, who supply the services, control most of the decisions to use medical resources. . . . The economic incentives in the medical market are attracting the great majority of physicians into specialty practice, and these incentives, combined with the continued introduction of new and more expensive technology, are a major factor in causing inflation of medical expenditures. Physicians and ambulatory care and diagnostic facilities are largely paid on a piecework basis for each item of service provided.
As a health care worker, I have personally witnessed this kind of mutual log-rolling between specialists and the never-ending addition of tests to the bill without any explanation to the patient. The patient simply lies in bed and watches an endless parade of unknown doctors poking their heads in the door for a microsecond, along with an endless series of lab techs drawing body fluids for one test after another that’s “been ordered,” with no further explanation. The post-discharge avalanche of bills includes duns from two or three dozen doctors, most of whom the patient couldn’t pick out of a police lineup. It’s the same kind of quid pro quo that takes place in academia, with professors assigning each other’s (extremely expensive and copyrighted) texts and systematically citing each other’s works in order to game their stats in the Social Sciences Citation Index. (I was also a grad assistant once.) You might also consider Dilbert creator Scott Adams’s account of what happens when you pay programmers for the number of bugs they fix.
One solution to this particular problem is to have a one-to-one relationship between the patient and a general practitioner on retainer. That’s how the old “lodge practice” worked. (See David Beito’s “Lodge Doctors and the Poor,” The Freeman, May 1994).
But that’s illegal, you know. In New York City, John Muney recently introduced an updated version of lodge practice: the AMG Medical Group, which for a monthly premium of $79 and a flat office fee of $10 per visit provides a wide range of services (limited to what its own practitioners can perform in-house). But because AMG is a fixed-rate plan and doesn’t charge more for “unplanned procedures,” the New York Department of Insurance considers it an unlicensed insurance policy. Muney may agree, unwillingly, to a settlement arranged by his lawyer in which he charges more for unplanned procedures like treatment for a sudden ear infection. So the State is forcing a modern-day lodge practitioner to charge more, thereby keeping the medical and insurance cartels happy—all in the name of “protecting the public.” How’s that for irony?
Regarding expensive machinery, I wonder how much of the cost is embedded rent on patents or regulatorily mandated overhead. I’ll bet if you removed all the legal barriers that prevent a bunch of open-source hardware hackers from reverse-engineering a homebrew version of it, you could get an MRI machine with a twentyfold reduction in cost. I know that’s the case in an area I’m more familiar with: micromanufacturing technology. For example, the RepRap—a homebrew, open-source 3-D printer—costs roughly $500 in materials to make, compared to tens of thousands for proprietary commercial versions.
More generally, the system is racked by artificial scarcity, as editor Sheldon Richman observed in an interview a few months back. For example, licensing systems limit the number of practitioners and arbitrarily impose levels of educational overhead beyond the requirements of the procedures actually being performed.
Libertarians sometimes—and rightly—use “grocery insurance” as an analogy to explain medical price inflation: If there were such a thing as grocery insurance, with low deductibles, to provide third-party payments at the checkout register, people would be buying a lot more rib-eye and porterhouse steaks and a lot less hamburger.
The problem is we’ve got a regulatory system that outlaws hamburger and compels you to buy porterhouse if you’re going to buy anything at all. It’s a multiple-tier finance system with one tier of service. Dental hygienists can’t set up independent teeth-cleaning practices in most states, and nurse-practitioners are required to operate under a physician’s “supervision” (when he’s out golfing). No matter how simple and straightforward the procedure, you can’t hire someone who’s adequately trained just to perform the service you need; you’ve got to pay amortization on a full med school education and residency.
Drug patents have the same effect, increasing the cost per pill by up to 2,000 percent. They also have a perverse effect on drug development, diverting R&D money primarily into developing “me, too” drugs that tweak the formulas of drugs whose patents are about to expire just enough to allow repatenting. Drug-company propaganda about high R&D costs, as a justification for patents to recoup capital outlays, is highly misleading. A major part of the basic research for identifying therapeutic pathways is done in small biotech startups, or at taxpayer expense in university laboratories, and then bought up by big drug companies. The main expense of the drug companies is the FDA-imposed testing regimen—and most of that is not to test the version actually marketed, but to secure patent lockdown on other possible variants of the marketed version. In other words, gaming the patent system grossly inflates R&D spending.
The prescription medicine system, along with state licensing of pharmacists and Drug Enforcement Administration licensing of pharmacies, is another severe restraint on competition. At the local natural-foods cooperative I can buy foods in bulk, at a generic commodity price; even organic flour, sugar, and other items are usually cheaper than the name-brand conventional equivalent at the supermarket. Such food cooperatives have their origins in the food-buying clubs of the 1970s, which applied the principle of bulk purchasing. The pharmaceutical licensing system obviously prohibits such bulk purchasing (unless you can get a licensed pharmacist to cooperate).
I work with a nurse from a farming background who frequently buys veterinary-grade drugs to treat her family for common illnesses without paying either Big Pharma’s markup or the price of an office visit. Veterinary supply catalogs are also quite popular in the homesteading and survivalist movements, as I understand. Two years ago I had a bad case of poison ivy and made an expensive office visit to get a prescription for prednisone. The next year the poison ivy came back; I’d been weeding the same area on the edge of my garden and had exactly the same symptoms as before. But the doctor’s office refused to give me a new prescription without my first coming in for an office visit, at full price—for my own safety, of course. So I ordered prednisone from a foreign online pharmacy and got enough of the drug for half a dozen bouts of poison ivy—all for less money than that office visit would have cost me.
Of course people who resort to these kinds of measures are putting themselves at serious risk of harassment from law enforcement. But until 1914, as Sheldon Richman pointed out (“The Right to Self-Treatment,” Freedom Daily, January 1995), “adult citizens could enter a pharmacy and buy any drug they wished, from headache powders to opium.”
The main impetus to creating the licensing systems on which artificial scarcity depends came from the medical profession early in the twentieth century. As described by Richman:
Accreditation of medical schools regulated how many doctors would graduate each year. Licensing similarly metered the number of practitioners and prohibited competitors, such as nurses and paramedics, from performing services they were perfectly capable of performing. Finally, prescription laws guaranteed that people would have to see a doctor to obtain medicines they had previously been able to get on their own.
The medical licensing cartels were also the primary force behind the move to shut down lodge practice, mentioned above.
In the case of all these forms of artificial scarcity, the government creates a “honey pot” by making some forms of practice artificially lucrative. It’s only natural, under those circumstances, that health care business models gravitate to where the money is.
Health care is a classic example of what Ivan Illich, in Tools for Conviviality, called a “radical monopoly.” State-sponsored crowding out makes other, cheaper (but often more appropriate) forms of treatment less usable, and renders cheaper (but adequate) treatments artificially scarce. Artificially centralized, high-tech, and skill-intensive ways of doing things make it harder for ordinary people to translate their skills and knowledge into use-value. The State’s regulations put an artificial floor beneath overhead cost, so that there’s a markup of several hundred percent to do anything; decent, comfortable poverty becomes impossible.
A good analogy is subsidies to freeways and urban sprawl, which make our feet less usable and raise living expenses by enforcing artificial dependence on cars. Local building codes primarily reflect the influence of building contractors, so competition from low-cost unconventional techniques (T-slot and other modular designs, vernacular materials like bales and papercrete, and so on) is artificially locked out of the market. Charles Johnson described the way governments erect barriers to people meeting their own needs and make comfortable subsistence artificially costly, in the specific case of homelessness, in “Scratching By: How the Government Creates Poverty as We Know It” (The Freeman, December 2007).
The major proposals for health care “reform” that went before Congress would do little or nothing to address the institutional sources of high cost. As Jesse Walker argued at Reason.com, a 100 percent single-payer system, far from being a “radical” solution,
would still accept the institutional premises of the present medical system. Consider the typical American health care transaction. On one side of the exchange you’ll have one of an artificially limited number of providers, many of them concentrated in those enormous, faceless institutions called hospitals. On the other side, making the purchase, is not a patient but one of those enormous, faceless institutions called insurers. The insurers, some of which are actual arms of the government and some of which merely owe their customers to the government’s tax incentives and shape their coverage to fit the government’s mandates, are expected to pay all or a share of even routine medical expenses. The result is higher costs, less competition, less transparency, and, in general, a system where the consumer gets about as much autonomy and respect as the stethoscope. Radical reform would restore power to the patient. Instead, the issue on the table is whether the behemoths we answer to will be purely public or public-private partnerships. [“Obama is No Radical,” September 30, 2009]
I’m a strong advocate of cooperative models of health care finance, like the Ithaca Health Alliance (created by the same people, including Paul Glover, who created the Ithaca Hours local currency system), or the friendly societies and mutuals of the nineteenth century described by writers like Pyotr Kropotkin and E. P. Thompson. But far more important than reforming finance is reforming the way delivery of service is organized.
Consider the libertarian alternatives that might exist. A neighborhood cooperative clinic might keep a doctor of family medicine or a nurse practitioner on retainer, along the lines of the lodge-practice system. The doctor might have his med school debt and his malpractice premiums assumed by the clinic in return for accepting a reasonable upper middle-class salary.
As an alternative to arbitrarily inflated educational mandates, on the other hand, there might be many competing tiers of professional training depending on the patient’s needs and ability to pay. There might be a free-market equivalent of the Chinese “barefoot doctors.” Such practitioners might attend school for a year and learn enough to identify and treat common infectious diseases, simple traumas, and so on. For example, the “barefoot doctor” at the neighborhood cooperative clinic might listen to your chest, do a sputum culture, and give you a round of Zithro for your pneumonia; he might stitch up a laceration or set a simple fracture. His training would include recognizing cases that were clearly beyond his competence and calling in a doctor for backup when necessary. He might provide most services at the cooperative clinic, with several clinics keeping a common M.D. on retainer for more serious cases. He would be certified by a professional association or guild of his choice, chosen from among competing guilds based on its market reputation for enforcing high standards. (That’s how competing kosher certification bodies work today, without any government-defined standards). Such voluntary licensing bodies, unlike state licensing boards, would face competition—and hence, unlike state boards, would have a strong market incentive to police their memberships in order to maintain a reputation for quality.
The clinic would use generic medicines (of course, since that’s all that would exist in a free market). Since local juries or arbitration bodies would likely take a much more common-sense view of the standards for reasonable care, there would be far less pressure for expensive CYA testing and far lower malpractice premiums.
Basic care could be financed by monthly membership dues, with additional catastrophic-care insurance (cheap and with a high deductible) available to those who wanted it. The monthly dues might be as cheap as or even cheaper than Dr. Muney’s. It would be a no-frills, bare-bones system, true enough—but to the 40 million or so people who are currently uninsured, it would be a pretty damned good deal.
#health care#monopoly#us healthcare#us politics#healthcare#medicine#science#kevin karson#anarchism#anarchy#anarchist society#practical anarchy#practical anarchism#resistance#autonomy#revolution#communism#anti capitalist#anti capitalism#late stage capitalism#daily posts#libraries#leftism#social issues#anarchy works#anarchist library#survival#freedom
2 notes
·
View notes
Text
Chinese Hospitals Are Housing Another Deadly Outbreak
In Beijing and other megacities in China, hospitals are overflowing with children suffering pneumonia or similar severe ailments. However, the Chinese government claims that no new pathogen has been found and that the surge in chest infections is due simply to the usual winter coughs and colds, aggravated by the lifting of stringent COVID-19 restrictions in December 2022. The World Health Organization (WHO) has dutifully repeated this reassurance, as if it learned nothing from Beijing’s disastrous cover-up of the COVID-19 outbreak.
There is an element of truth in Beijing’s assertion, but it is only part of the story. The general acceptance that China is not covering up a novel pathogen this time appears reassuring. In fact, however, China could be incubating an even greater threat: the cultivation of antibiotic-resistant strains of a common, and potentially deadly, bacteria.
Fears of another novel respiratory pathogen emerging from China are understandable after the SARS and COVID-19 pandemics, both of which Beijing covered up. Concerns are amplified by Beijing’s ongoing obstruction of any independent investigation into the origins of SARS-CoV-2, the virus that causes COVID-19—whether it accidentally leaked from the Wuhan lab performing dangerous gain-of-function research or derived from the illegal trade in racoon dogs and other wildlife at the now-infamous Wuhan wet-market.
Four years ago, during the early weeks of the COVID-19 outbreak, Beijing failed to report the new virus and then denied airborne spread. At pains to maintain their fiction, Chinese authorities punished doctors who raised concerns and prohibited doctors from speaking even to Chinese colleagues, let alone international counterparts. Chinese medical statistics remain deeply unreliable; the country still claims that total COVID-19 deaths sit at just over 120,000, whereas independent estimates suggest the number may have been over 2 million in just the initial outbreak alone. Now, Chinese doctors are once again being silenced and not communicating with their counterparts abroad, which suggests another potentially dangerous cover-up may be underway.
We don’t know exactly what is happening, but we can offer some informed guesses.
The microbe causing the surge in hospitalization of children is Mycoplasma pneumoniae, which causes M. pneumoniae pneumonia, or MPP. First discovered in 1938, the microbe was believed for decades to be a virus because of its lack of a cell membrane and tiny size, although in fact it is an atypical bacterium. These unusual characteristics makes it invulnerable to most antibiotics (which typically work by destroying the cell membrane). The few attempts to make a vaccine in the 1970s failed, and low mortality has provided little incentive for renewed efforts. Although MPP surges are seen every few years around the world, the combination of low mortality and difficult diagnostics has meant there is no routine surveillance.
Although MPP is the most common cause of community-acquired pneumonia in school children and teenagers, pediatricians such as myself refer to it as “walking pneumonia” because symptoms are relatively mild. Respiratory Syncytial Virus (RSV), influenza, adenoviruses, and rhinoviruses (also known as the common cold) all cause severe inflammation of the lungs and are far more common causes of emergency-room visits, hospitalization, and death in infants and young children. Why should MPP be acting differently now?
One contributing factor to the severity of this outbreak may be “immunity debt.” Around the globe, COVID-19 lockdowns and other non-pharmaceutical measures meant that children were less exposed to the usual range of pathogens, including MPP, for several years. Many countries have since seen rebound surges in RSV. Several experts agree with Beijing’s explanation that the combination of winter’s arrival, the end of COVID-19 restrictions, and a lack of prior immunity in children are likely behind the surging infections. Some even speculate that that substantial lockdown may have particularly compromised young children’s immunity, because exposure to germs in infancy is essential for immune systems to develop.
In China, MPP infections began in early summer and accelerated. By mid-October, the National Health Commission had taken the unusual step of adding MPP to its surveillance system. That was just after Golden Week, the biggest tourism week in China.
Infection by two diseases at the same time can make things worse. The usual candidates for coinfection in children—RSV and flu—have not previously caused comparable surges in pneumonia. One difference this time is COVID-19. It is possible that the combination of COVID-19 and MPP is particularly dangerous. Although adults are less susceptible to MPP due to years of exposure, adults hospitalized for COVID-19 who were simultaneously or recently coinfected by MPP had a significantly higher mortality rate, according to a 2020 study.
Infants and toddlers are immunologically naive to MPP, and unlike COVID-19, RSV, and influenza, there is no vaccine against MPP. It seems implausible that no child (or adult) has died from MPP, yet China has not released any data on mortality, or on extrapulmonary complications such as meningitis.
Most disturbing, and a fact being downplayed by Beijing, is that M. pneumoniae in China has mutated to a strain resistant to macrolides, the only class of antibiotics that are safe for children less than eight years of age. Beyond discouraging parents to start ad hoc treatment with azithromycin, the most common macrolide and the usual first-line antibiotic for MPP, Beijing has barely mentioned this fact. Even more worrying is that WHO has assessed the risk of the current outbreak as low on the basis that MPP is readily treated with antibiotics. Broader azithromycin resistance in MPP is common across the world, and China’s resistant strain rates in particular are exceptionally high. Beijing’s Centers for Disease Control and Prevention reported macrolide resistance rates for MPP in the Beijing population between 90 and 98.4 percent from 2009 to 2012. This means there is no treatment for MPP in children under age eight.
Fears over a novel pathogen are already abating. After all, MPP is rarely lethal. But antimicrobial resistance (AMR) is. Responsible for 1.3 million deaths a year, AMR kills more people than COVID-19. No country is immune to this growing threat. Since China, where antibiotics are regularly available over the counter, leads the world in AMR, it is inconceivable that this issue hasn’t yet come up, particularly during WHO’s World AMR Awareness week, from Nov. 18 to Nov. 24.
Any infectious disease physician would want to know: Did WHO asked China the obvious question—what is the level of azithromycin resistance of M. pneumonia in the current outbreak—and include the answer in its risk assessment? Or did it ask about resistance to doxycycline and quinolones, antibiotics that can be used to treat MPP in adults? Even if WHO did ask, China isn’t telling, and WHO isn’t talking.
China’s silence isn’t surprising. Its antibiotic consumption per person is ten times that of the United States, and policies for AMR stewardship are predominantly cosmetic. While surveillance is China’s strong point, reporting is not.
Despite Spring Festival, the Chinese celebration of the Lunar New Year and another peak travel period, approaching in February 2024, WHO hasn’t advised any travel restrictions. It should have learned the danger of accepting Beijing’s statements at face value. Four years ago, Beijing’s delay enabled more than 200 million people to travel from and through Wuhan for Spring Festival. That helped COVID-19 go global. Since China’s AMR rates are already so high, importing AMR from other countries isn’t a major concern for China. Export is the issue, and China’s track record in protecting other countries is abysmal.
Rather than repeating the self-serving whitewashing coming from Beijing, WHO should be publicly pressing China about the threat of mutant microbes. Halting AMR is essential. Before antisepsis and antibiotics, surgery was a treatment of last resort. Without antibiotics, we lose 150 years of clinical and surgical advances. Within ten years, we are at risk of few antibiotics being effective. It may not be the novel virus that people were expecting, but the next pandemic is already here.
13 notes
·
View notes
Text

Crew-8 Astronauts Return to Earth
After seven months of living and working onboard the International Space Station (ISSInternational Space Station), astronauts of NASA’s eighth rotational SpaceX crew mission (Crew-8) splashed down safely off the coast of Florida. The mission, which is part of NASA’s Commercial Crew Program, included NASANational Aeronautics and Space Administration astronauts Matthew Dominick, Michael Barratt, and Jeanette Epps, as well as Roscosmos cosmonaut Alexander Grebenkin. During their mission on station, the three NASA astronauts supported dozens of research investigations sponsored by the ISS National Laboratory®.
These investigations spanned many areas, including in-space production applications(Abbreviation: InSPA) InSPA is an applied research and development program sponsored by NASA and the ISS National Lab aimed at demonstrating space-based manufacturing and production activities by using the unique space environment to develop, test, or mature products and processes that could have an economic impact., life and physical sciences, and technology development, all aimed at bringing value to humanity and enabling a robust market in low Earth orbit(Abbreviation: LEO) The orbit around the Earth that extends up to an altitude of 2,000 km (1,200 miles) from Earth’s surface. The International Space Station’s orbit is in LEO, at an altitude of approximately 250 miles. (LEO).
Below highlights a few of the ISS National Lab-sponsored projects the Crew-8 NASA astronauts worked on during their mission.
Several investigations focused on in-space production applications, an increasingly important area of emphasis for the ISS National Lab and NASA.
A project from Cedars Sinai Medical Center aims to establish methods to support the in-space manufacturing of stem cells, which can be matured into a wide variety of tissues. These methods will be used for future large-scale in-space biomanufacturing of stem cell-derived products, which could lead to new treatments for heart disease, neurodegenerative diseases, and many other conditions.
Redwire Corporation partnered with Eli Lilly and Company and Butler University on a series of investigations leveraging Redwire’s Pharmaceutical In-space Laboratory (PIL-BOX), a platform to crystallize organic molecules in microgravityThe condition of perceived weightlessness created when an object is in free fall, for example when an object is in orbital motion. Microgravity alters many observable phenomena within the physical and life sciences, allowing scientists to study things in ways not possible on Earth. The International Space Station provides access to a persistent microgravity environment.. Results from this research could lead to improved therapeutics to treat an array of conditions. These projects continue Eli Lilly’s space journey, as the company has launched multiple investigations to the orbiting laboratory over the years for the benefit of patient care on Earth.
The astronauts supported the third experiment in a series of projects from the University of Notre Dame to improve ultra-sensitive biosensors. The biosensors can detect trace substances in liquids, including early cancer biomarkers. By using laser heating to control bubble formation in microgravity, the team improved particle collection—a key step in boosting sensor sensitivity. This research, funded by the U.S. National Science Foundation, could transform early and asymptomatic cancer detection and other medical diagnostics.
The crew conducted phase two of a technology development project from Sphere Entertainment to test Big Sky—the company’s new ultra-high-resolution, single-sensor camera—on the space station. In the first phase of the project, which launched in November 2022, astronauts tested a commercial off-the-shelf camera on the ISS to collect baseline information. During the second phase, the astronauts tested Big Sky to validate the camera’s function, operations, and video downlink capabilities in microgravity. Big Sky is being developed by Sphere Entertainment to capture content for Sphere, the next-generation entertainment medium in Las Vegas.
In the final days before their departure from the space station, the Crew-8 astronauts supported projects that recently launched on NASA’s ninth rotational crew mission (Crew-9).
One is a student-led project from Isabel Jiang, a recent high school graduate from Hillsborough, CA, who is now in her first year at Yale. Jiang is the winner of the 2023 Genes in Space student research competition, founded by Boeing and miniPCR bio and supported by the ISS National Lab and New England Biolabs. Jiang’s experiment investigates the effect of radiation and the space environment on mechanisms for gene editing. Results could help develop methods to better protect astronauts and shed light on genetic risks for certain diseases during spaceflight.
Another is an investigation from the U.S. Air Force Academy and Rhodium Scientific to compare the root growth of Arabidopsis plants, a member of the mustard family, at two different orbital altitudes. Plants grown on the space station in LEO for four to six days will be compared with similar plants grown on the recent Polaris Dawn mission, which flew in the same type of vehicle at a higher orbit for approximately the same amount of time. Results could provide insights into the production of crops for long-duration space missions and in high-radiation environments.
IMAGE: SpaceX Crew-8 astronauts (top to bottom) NASA's Jeanette Epps, Mike Barratt & Matthew Dominick, and Roscosmos cosmonaut Alexander Grebenkin onboard the ISS. Credit NASA
5 notes
·
View notes
Text
17 // diagnostic (extra credit)

Welcome to SelfMed, your online personal medical evaluation assistant! If this is a medical emergency, please contact local authorities or Trauma Team for immediate help.
How can SelfMed assist you today?
>> diagnosis
Please list up to five major symptoms for a diagnosis using our QuickMatch™ technology.
[1] fever [2] headache [3] mania [4] hallucinations [5] not recognizing faces
———
QuickMatch™ Potential Diagnoses*
The symptoms listed are a complete or partial match to the diseases and disorders below:
Click for more information and recommended treatment options.
Schizophrenia [+]
Post-Traumatic Stress Disorder (PTSD) [+]
Cyberpsychosis [–]
Cyberpsychosis is a collective term for all psychotic and anxiety-related personality disorders caused by hardware implanted in the body and any and all behavioral mods, including software. Often this begins as changes to the personality, followed by increasingly erratic and even violent behavior. Some medications and substance abuse can worsen these behaviors. Recommended treatment options: - Therapy - Implant deactivation and/or removal - Bethaloperidol While antipsychotics are widely used to slow the onset of cyberpsychosis, therapy has also proven effective for some patients after years of treatment. Those experiencing aggressive cyberpsychotic symptoms such as violent outbursts should be kept away from public spaces and denied access to weapons until they can be incapacitated, restrained, and removed for treatment. If you or someone you know is experiencing symptoms of cyberpsychosis that result in erratic or violent behavior, remove yourself from any potentially dangerous situations and call MaxTac. Do NOT interrupt MaxTac officers during an ongoing violent situation. DO put as many walls between the situation and yourself as is possible to avoid stray projectiles and bodily harm.
*QuickMatch™ diagnoses are a quick-screening technology and should not be used to replace the services of a trained medical professional.
———
Your free trial SelfMed membership is valid for the next [7 DAYS].
By upgrading to a premium membership, you can access an additional seven diagnoses. Would you like to upgrade to a SelfMed premium membership today? (€$199 per mo.)
Enter promo code HEALTH10NOW for a limited time offer of 10% your first month of premium service!
———
Is there something else SelfMed can assist with?
>> nethaloperidol
We’re sorry, but we didn’t recognize that prompt.
Is there something else SelfMed can assist with?
>> bethaloperidol
Searching “bethaloperidol” yielded the following articles:
Bethaloperidol [–]
Bethaloperidol is an antipsychotic used to treat a broad range of disorders, ranging from Schizophrenia to hyperactivity. When prescribed by a doctor in combination with therapy, bethaloperidol has been proven effective in helping patients recover. Bethaloperidol can be taken in pill form or through injection. The most widely used brands are Bethal and Novadol. Though black market bethaloperidol is frequently sold, it is not created in a lab environment where product quality is overseen, it is likely a cheaper alternative that will not address symptoms adequately, and/or it has been cut with other drugs that could be a potentially dangerous cocktail. Brand names are always recommended and more effective than their black market counterparts.
———
Searching for the nearest retailer that carries BETHALOPERIDOL? We’ve found 10 locations near you, less than 5 minutes away!
Upgrade to a premium membership to find trusted pharmaceutical outlets near you. (€$199 per mo.)
Enter promo code HEALTH10NOW for a limited time offer of 10% your first month of premium service!
———
Is there something else SelfMed can assist with?
>> ripperdoc
Searching “ripperdoc” yielded the following articles:
Ripperdocs: the new GP or back alley surgeon? [+]
Top 10 most horrifying ripperdoc patient stories [+]
Confessions of a street doctor: ripper reveals all [+]
Is there something else SelfMed can assist with?
>> nearest ripperdoc
We’re sorry, but we didn’t recognize that prompt.
Is there something else SelfMed can assist with?
>> fuck off
———
Thank you for using SelfMed!
Your feedback matters! Please rate your experience.
☆☆☆☆☆
#ffxivwrite2023#[ ffxivwrite2023 ]#[ cyberpunk ]#sunday is au day#sometimes writing cyberpunk means exercising the corporate copywriter in me for cynical purposes
15 notes
·
View notes
Text
MIA
Yep, I've let too many days pass without posting. I've missed the opportunity to crow about how much fun Halloween was, we're already more than a week into November! We did have a grand time though. Trick-or-treating with our little miss in her fun neighborhood ticks all of the boxes on my perfect Halloween check list. I popped on my witch hat and my sweatshirt and had as much fun as the kids.

I'm trying to be better about sharing pictures of myself (ugh!) so that when I'm dead my kids can have something to prove I was here.




Yes indeed, we gave October a fantastic send off and November arrived with chillier weather and even more color in the trees. Absolutely beautiful.
I've been busy filling a big earring order, and keeping appointments. My in-person interview at the library went well ( I thought) but I haven't heard a peep. I can't worry about that. I know I'm qualified and would be helpful and cheerful to the patrons, but I still may not be what they're looking for - who knows? If not there, I'll find something else. I had a follow up appointment after my yearly physical/ lab work because my blood pressure was up. That's really unusual for me, so I had to track it for a month and then bring my monitor in and all that. Turns out I'm normal, I just don't like going to the doctor. I'm really glad that I don't have to take meds. I'm too forgetful for that.
Then, I received a call that my mammogram results were abnormal and showed a "developing asymmetry" in the left breast. Tomorrow I have to go to Easton for a diagnostic mammogram and an ultrasound. I'm 99% sure that it's nothing, probably just normal changes, but for someone who doesn't like going to doctors and/or having procedures, enough already! If this is what getting older is like, I'm not a fan. I told a friend that it's probably a lump of cookie dough that didn't make it all the way to my hips - much ado about nothing.
When I'm not kneading clay and baking earrings, or getting poked and prodded by medical personnel, I'm trying to prepare for the upcoming holidays. I love an October vacation, and Ireland was sublime, but it tends to dump me right at the doorstep of Thanksgiving and Christmas and I'm not ready for either one! I confess to playing some Christmas tunes already, just to get in the mood. I feel like I'm way behind. I've been trying to come up with our card for this year and the creative well is running dry. They just get thrown away by the recipients, why not just pick up a couple boxes of cards at Target? That would be smarter and I could cross it off my list. I know that I'm one of the dinosaurs still sending out holiday cards, but I love getting them in my mailbox and one must give in order to receive, right? So that's my quick check in, and my apology for being tardy with this post. Tomorrow I'll ship those earrings off to Florida and go get my boob smashed again, and then my schedule will be nothing but holiday madness. I'm looking forward to it. It's time to get my jingle on!

The Edgewater gang will come over this weekend and I'll have to make sure that I have a grasp on the grandgirl's list for Santa. I have a toy catalog here that should inspire her. Everyone else is getting socks and a toothbrush. Just kidding, but that sure would be easy. When am I old enough to start doing that? They'll head to Tennessee for Thanksgiving, but will be with us for Christmas. Matt is flying in for Thanksgiving, then in December he jets off to Brugge, Belgium and Amsterdam for the Christmas markets. He'll be here for Christmas week full of stories to share. I can't wait. On that happy note, I'll head of to soak in a bubble bath and then snuggle under the covers with a book. I'm pooped. Until tomorrow, stay safe, stay well...and
You better watch out You better not cry You better not pout I'm telling you why
… Santa Claus is comin' to town! 47 days!!! XOXO, Nancy
6 notes
·
View notes
Text

Celebrating 10 Years' Journey of Athenese-Dx Pvt. Ltd.
celebration #10years #athenesedx #Chennai #IVD #India #milestone
🎉 Celebrate a Decade of Innovation with Athenese-Dx! Join us in our 10th Anniversary Celebration as we continue to honor a decade of groundbreaking achievements at Athenese-Dx. This special video takes you on a journey through our most memorable moments, showcasing our commitment to excellence and innovation.
Highlights:
Milestone Moments: Relive our top achievements and how they've shaped the industry. From pioneering diagnostic technologies to life-changing breakthroughs, we've been at the forefront of medical advancements.Behind-the-Scenes: Get an exclusive look at the people and passion driving our success. Meet our brilliant scientists, dedicated researchers, and tireless support staff who have fueled our journey.Future Forward: Peek into the future as we unveil exciting plans for the next decade. Discover our vision for improving patient care, expanding global reach, and revolutionizing healthcare.
Thank You to Our Community: We extend our heartfelt gratitude to our customers, partners, and employees who have been part of our story. Your unwavering support and trust have propelled us forward.
Stay Connected: Don't miss out on any updates as we embark on the next chapter of our journey
diagnosticcenter #rapidtest #elisakit #biochemistry #ivdmanufacturing #clinicalchemistry #ivdinstrument #medicaldevices #reagents
Together, let's continue to redefine diagnostics and transform lives. Here's to the next ten years of excellence! 🥂 🎉 Cheers to many more amazing years! 🎉
ATHENESE-DX PRIVATE LIMITED Address: Module No. 407 & 408, 4th Floor, TICEL Bio Park II, No. 5, CSIR Road, Taramani, Chennai, Tamil Nadu - 600113, India
For Inquires - WhatsApp +917397238924 Click here to chat: https://wa.me/917397238924
For Reviews & News, go to https://www.athenesedx.com/
Follow us on WhatsApp Channel: https://whatsapp.com/channel/0029Va8M7HQChq6HfUBMLj0X
🌎 Visit our office - https://qr.page/g/5lZXERbP8Av
🤝 Subscribe - https://youtube.com/@athenesedx Our early diagnosis products for a better life. Thank you for your support.
🔔 For more videos, products, reviews ↷ YouTube ▶ https://youtube.com/@athenesedx
🌐 For more information ↷ Website ▶ https://athenesedx.com To Buy Athenese-Dx Products ▶ https://store.athenesedx.com
📱 Follow us on social media ↷ Facebook ▶ https://www.facebook.com/Athenese.Dx.Pvt.Ltd/ Instagram ▶ https://www.instagram.com/athenese_dx/ Pinterest ▶ https://www.pinterest.com/athenesedx/ X (Twitter) ▶ https://twitter.com/athenesedx Tumblr ▶ https://www.tumblr.com/athenese-dx LinkedIn ▶ https://www.linkedin.com/company/athenese-dx-private-limited/ Medium ▶ https://medium.com/@athenesedx01
#clinical chemistry#digital pathology market#pathologist#hospital#pathology#pathologylab#ivd#in vitro diagnostics market#in vitro diagnostics industry#reagent#biochemistry#rapid tests#elisa kits#lab equipment#lab supplies#celebration#10 years ago#10 year anniversary#athenesedx#india#milestone celebration
0 notes
Text
Home PCR Tests: A Closer Look at the PCR Test At Home Dubai Option
The COVID-19 pandemic sparked major growth in the development and usage of diagnostic and antibody tests that patients can self-administer from home. Home PCR tests in particular enable private, convenient detection of active coronavirus infections. For those wondering whether accurate PCR Test At Home Dubai kits are available, exploring the leading options provides helpful guidance.

How Do Home PCR Tests for COVID-19 Work?
The PCR (polymerase chain reaction) technique is the gold standard for directly detecting the presence of the COVID-19 virus from respiratory samples. Home PCR test kits allow patients to collect their own nasal or saliva samples and perform the PCR assay without visiting a clinic.
PCR tests work by identifying the specific genetic material of the COVID-19 virus. Users collect a sample, mix it with chemical reagents, and insert the solution into the test kit for analysis. Results are displayed indicating whether viral genetic material was detected based on any color change reaction on the test strips.
Kits include step-by-step instructions to ensure patients perform the easy, quick tests properly using non-invasive nasal swabs or saliva collection. Many provide results within 10-30 minutes.
Here is a video from MedCram Youtube Channel about At Home Rapid COVID 19 Tests and False Positives (Coronavirus Antigen Tests). Watch the video
youtube
Benefits of At-Home PCR Testing
Here are some of the major advantages of having access to accurate home PCR tests for COVID-19:
Convenience: Test from the privacy of your residence without traveling to clinics.
Speed: Get results rapidly within minutes rather than waiting days for lab tests.
Self-Administered: Users can collect their own sample comfortably rather than relying on technicians.
Affordability: Individual kits are very competitively priced.
Detection Reliability: PCR technology directly identifies viral presence with high accuracy.
Ease of Use: Tests have simple, straightforward instructions for patients of all ages.
Infection Verification: Confirms active infections unlike antibody tests.
Having the option to privately, quickly, and accurately test for possible COVID-19 infections at home provides significant peace of mind during the pandemic.
How Reliable Are Home PCR Tests?
Many people reasonably wonder whether DIY home PCR test kits can match the reliability of lab-based PCR tests. The good news is that leading home PCR kits on the market have very high accuracy.
Most kits have published sensitivity and specificity above 90% when compared to lab PCR tests. High quality home tests analyze samples using comparable PCR methodology and match labs in detecting positives and negatives.
Furthermore, unlike Rapid PCR Test At Home kits some vendors offer, full home PCR tests analyze the sample through many amplification cycles to maximize accuracy. With good sampling collection, top home PCR kits offer laboratory-grade results conveniently at home.
Leading Home PCR Test Kit Options
For those exploring PCR Test At Home Dubai choices, here are some of the top-rated home PCR kits to consider:
Cue Health PCR Test: Cue offers an FDA-authorized home PCR test delivering highly accurate results in 20 minutes with nasal swab samples.
Lucira Check It PCR Test: This is a single-use PCR kit with 98% validated accuracy that provides molecular-level detection from nasal samples in 30 minutes or less.
Ellume COVID-19 Home Test: This over-the-counter home kit uses a mid-turbinate nasal sample and provides an amplified PCR digital reading of positive or negative in 15 minutes on a connected analyzer.
Pixel by LabCorp PCR Test: Pixel is a monitored at-home nasal PCR test analyzed through LabCorp with over 98% accuracy returning results within 1-2 days.
Doximity's Covid-19 PCR Test: Doximity partners with qualified labs for monitored video-observed PCR testing with 97%+ accuracy and results in 24 hours.
All these options allow for convenient, accurate at-home COVID-19 testing using PCR with trusted partners. Kits can be purchased online and shipped directly to your home in Dubai.
When Are Home PCR Tests Recommended?
The CDC recommends utilizing home PCR tests in situations such as:
If you have any symptoms of COVID-19. Home testing allows quick confirmation.
After exposure events to quickly check for possible infection.
Before visiting individuals at higher risk for severe illness.
Before travel or group events for added assurance.
For frequent screening in schools or workplaces.
Even fully vaccinated individuals should test if they experience COVID-like symptoms or have a known exposure. Home PCR tests make quick detection fast and easy.
Home PCR Tests Offer Accuracy and Convenience
High quality Home PCR Tests have become an important tool in the fight against COVID by making reliable diagnostic testing accessible outside of clinics. There are excellent PCR Test At Home Dubai options available matching the standards of lab PCR sensitivity and specificity. Home PCR kits allow people to conveniently and confidently check themselves for possible COVID-19 infections from the privacy of home. As the technology continues advancing, home collection PCR will likely take on an increasingly vital role supporting public health and safety.
2 notes
·
View notes
Text
Best Medical Coding Institute in Nagercoil
MEDICAL CODING
Medical coding is the process of extracting data from a doctor's notes on a patient's medical history, including medical procedures, diagnoses, necessary medical equipment, and medical services. This data is converted into standard medical alphanumeric codes by a medical coder.
There are three types of universally known medical alphanumeric codes:
The World Health Organization (WHO) developed the International Classification of Diseases (ICD), a system that is widely utilised. The classification system is primarily used for data collecting and health records, among other things. These codes can categorise signs, conditions, illnesses, and fatalities.
CPT codes are used in the US to identify certain medical, surgical, and diagnostic operations and services. This system, which has three categories—procedures and modern medical practises, clinical labs, and developing technologies—was created by the American Medical Association (AMA).
The Centers for Medicare and Medicaid Services (CMS) created the Healthcare Common Procedure Coding System (HCPCS) to facilitate in the processing of insurance claims for Medicare or other providers. They are used by coders to record medical processes, goods, services, and merchandise.
Transorze is an ISO 9001:2015 certified company for delivering high quality “Healthcare BPO” training and placement services, totally dedicated in providing the services of Medical Transcription Training,Medical Coding Training , Medical Scribing Training, ,Digital Marketing Training.
Contact details
Phone no: +919495833319
E Mail:[email protected]
#mediclcoding#transorzesolutions#healthcare#doctors#learn#classrooms#newcareeropportunities#joborientedcourses
2 notes
·
View notes
Text
The Power of EMR: Streamlining Healthcare for a Better Future
The Future of Healthcare: Exploring the Medical Record (EMR) Market
Straits Research projects significant growth in the global Electronic Medical Record (EMR) Market from 2024 to 2032. The market, valued at USD 30.4 billion in 2023, is expected to grow from USD 32.3 billion in 2024 to USD 52.6 billion by 2032 at a CAGR of 6.3%.
Request a free request sample https://straitsresearch.com/report/electronic-medical-record-market/request-sample
Drivers:
Increasing adoption of digital health records
Government initiatives promoting EMRs
Rising demand for cloud-based solutions
Growing need for improved patient care
Key Developments:
AI and ML integration in EMR systems
Demand for interoperable solutions
EMR adoption in emerging markets
Top Key Players: Cerner Corporation, Epic Systems Corporation, Allscripts Healthcare Solutions, MEDITECH, GE Healthcare, NextGen Healthcare, Intersystems Corporation, Cantata Health, Advanced-Data Systems Corporation, CureMD.
This Report is available for purchase on https://straitsresearch.com/buy-now/electronic-medical-record-market
Market Segmentation: By Component: Software, Services, Hardware By Application: General, Specialty-Based By Delivery Mode: Cloud-based By End-User: Hospitals, Clinics, Diagnostic Centers, Ambulatory Care, Research Labs
About Straits Research Straits Research provides business intelligence through research, analytics, and advisory services.
Contact Us Email: [email protected] Address: 825 3rd Avenue, New York, NY, USA, 10022 Phone: +1 646 905 0080 (US), +91 8087085354 (India), +44 203 695 0070 (UK)
#Electronic Medical Record Market#Electronic Medical Record Market Size#Electronic Medical Record Market Share#Electronic Medical Record Market Research
0 notes
Text
Digital Microfluidic Chips: Growth from $1.2B to $3.8B by 2034 💧
Digital Microfluidic Chips Market is set to expand from $1.2 billion in 2024 to $3.8 billion by 2034, growing at a CAGR of 12.2%. These cutting-edge chips, which control microfluidic droplets via electronic signals, are transforming diagnostics, drug discovery, and lab automation, enabling faster, more precise, and cost-effective analysis.
To Request Sample Report: https://www.globalinsightservices.com/request-sample/?id=GIS10930 &utm_source=SnehaPatil&utm_medium=Article
Key Market Trends & Drivers
🔹 Lab-on-a-Chip Technology Leads: Enabling rapid, miniaturized diagnostics for real-time testing. 🔹 Point-of-Care Testing Growth: Rising demand for portable, on-site diagnostic solutions. 🔹 Drug Discovery & Biotechnology Boom: Increasing adoption for high-throughput screening & molecular analysis. 🔹 AI & IoT Integration: Enhancing automation, efficiency, and remote monitoring capabilities. 🔹 Advancements in MEMS & Microarrays: Expanding applications in genomics, proteomics, and precision medicine.
Regional Market Insights
🌎 North America dominates, driven by cutting-edge research & healthcare infrastructure. 🌍 Europe follows, with strong investments in biotech & medtech R&D. 🌏 Asia-Pacific emerges as a key growth hub, fueled by government initiatives & rapid industrialization. 🌍 Latin America & the Middle East are adopting microfluidic tech in diagnostics & environmental monitoring.
Market Segmentation Overview
🔹 Type: Electrowetting, Magnetic, Dielectrophoretic 🔹 Technology: Integrated Circuit, MEMS, Microarray 🔹 Applications: Diagnostics, Drug Delivery, Cell Culture, Genomics, Proteomics 🔹 Materials: Glass, Silicon, Polymer 🔹 End Users: Healthcare, Biotech, Pharma, Research Labs
📈 In 2024, the market saw 320 million units, with healthcare leading (45%), followed by research labs (30%) and consumer electronics (25%). Illumina, Bio-Rad, & Advanced Liquid Logic dominate, pioneering innovations in microfluidic automation & precision diagnostics.
As AI, automation, and bioinformatics reshape digital microfluidics, this market is poised to revolutionize disease detection, drug discovery, and next-gen healthcare solutions! 💡🔍
#Microfluidics #LabOnAChip #BioTech #PointOfCare #Diagnostics #HealthcareInnovation #DrugDiscovery #BiotechRevolution #MEMS #AIinHealthcare #WearableTech #PersonalizedMedicine #Genomics #Proteomics #MedicalDevices #Biosensors #SmartDiagnostics #Microarray #PharmaTech #PrecisionMedicine #NextGenHealthcare #DigitalBiomarkers #TechInMedicine #Nanotechnology #SmartLabs #R&D
0 notes
Text
Medical Projector Trends: Growth, Innovations, and Future Prospects
Medical projectors are transforming the healthcare landscape, offering cutting-edge solutions for diagnostics, education, and surgical precision. In 2025, advancements in medical projector technology are reshaping how healthcare professionals visualize complex data and communicate with patients. This blog explores the growth trends, key innovations, and future prospects of medical projectors, shedding light on their increasing importance in the medical field. The Growing Demand for Medical Projectors in Healthcare Medical projectors have become indispensable in healthcare settings, driven by the need for accurate visualization and enhanced collaboration. Their applications range from displaying medical imaging to facilitating surgical guidance and training. Market Growth Trends Global Market Expansion: The medical projector market is projected to grow at a CAGR of 7.5% between 2023 and 2030. Adoption Across Sectors: Hospitals, clinics, and medical training institutions are the largest consumers of this technology. Increased Investment: Governments and private organizations are investing in visualization technology to improve healthcare outcomes. Key Innovations in Medical Projector Technology 1. 4K and 8K Resolution for Enhanced Imaging High-resolution projectors are setting new standards for medical imaging. These projectors deliver unparalleled clarity, enabling healthcare professionals to analyze intricate details with precision. Applications: Surgical procedures requiring detailed visualization. Diagnostic imaging, such as X-rays, MRIs, and CT scans. Interactive patient education and consultation. 2. Integration with AR and VR Technologies Medical projectors are increasingly integrated with augmented reality (AR) and virtual reality (VR) systems, providing immersive visualization for surgeries and medical training. Benefits: Real-time overlays for surgical guidance. Enhanced learning experiences for medical students. Virtual simulations for complex procedures. 3. Compact and Portable Designs The latest medical projectors are lightweight, portable, and easy to use, making them suitable for diverse healthcare environments, including remote and rural clinics. Features to Note: Battery-operated designs for portability. Wireless connectivity for seamless data sharing. Compatibility with tablets and laptops for on-the-go use. 4. AI-Powered Projectors Artificial Intelligence is transforming medical projectors by enabling advanced functionalities like automated adjustments, predictive analytics, and image enhancement. Examples: AI-based noise reduction for clearer visuals. Predictive algorithms for pre-surgical planning. Real-time data analytics displayed alongside imaging. Key Use Cases of Medical Projectors in 2025 1. Surgical Precision Medical projectors assist surgeons by displaying real-time, high-definition visuals of the surgical site, often integrated with AR for improved accuracy. 2. Diagnostic Imaging Radiologists use medical projectors to analyze and interpret complex imaging data, improving diagnostic accuracy and patient outcomes. 3. Medical Education In classrooms and training labs, projectors enhance learning by enabling interactive presentations, 3D modeling, and immersive simulations. 4. Patient Communication Doctors can use projectors to explain conditions and treatment plans visually, improving patient understanding and engagement. Future Prospects of Medical Projectors 1. Increased AI Integration The future of medical projectors lies in their ability to leverage AI for smarter, more interactive functionalities. Predictive visualization and real-time anomaly detection will redefine medical imaging. 2. Wider Adoption of Holographic Displays Holographic projectors are expected to revolutionize medical training and surgical planning by providing 3D, interactive visuals that can be viewed from multiple angles. 3. Enhanced Telemedicine Support As telemedicine
continues to grow, portable medical projectors will play a critical role in enabling remote consultations and diagnostics. 4. Sustainability Initiatives Manufacturers are focusing on eco-friendly designs with lower energy consumption and recyclable components, aligning with global sustainability goals. Top Medical Projector Brands to Watch in 2025 1. Sony Medical Projectors Known for their high-resolution displays and advanced imaging capabilities. 2. Barco Healthcare Leaders in surgical imaging projectors with innovative AR integration. 3. Epson Pro AV Providing compact, reliable, and affordable options for clinics and hospitals. 4. Christie Digital Specialized in ultra-high-definition projectors for surgical and diagnostic applications. Challenges in Adopting Medical Projector Technology While the potential is immense, challenges persist: High Initial Costs: Advanced medical projectors require significant investment. Training Requirements: Healthcare professionals need training to fully utilize these tools. Infrastructure Limitations: Rural areas may face hurdles in adopting projector technology due to inadequate infrastructure. Shaping the Future of Healthcare Visualization The medical projector market is poised for remarkable growth, driven by innovations in resolution, portability, and AI integration. As healthcare systems continue to adopt these technologies, medical projectors will play a pivotal role in enhancing diagnostics, surgeries, and patient care. By embracing these advancements, the medical community can look forward to a future where precision, efficiency, and accessibility are at the forefront of healthcare.
0 notes