#Covid-19 Vaccination In India
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The most popular pages on Tumblr are about Minecraft, GIFs, and David J. Peterson.
Text
#covid 19#covid 19 2025#covid 19 new cases in india#covid 19 cases in india#covid 19 news#covid 19 is back#covid 19 latest news#covid 19 back#covid 19 cases#cách ly covid 19#ca exam covid 19#covid 19 return#covid 19 safety#biến thể covid 19#covid 19 in india#covid 19 vaccine#covid 19 hong kong#covid 19 thailand#covid 19 new cases#covid 19 symptoms#covid 19 news today#covid 19 xec variant#travis head covid 19#covid 19 travis head
0 notes
Text
India: An overview of the saga of the Journey
Share what you know about the year you were born. The dust was settling, but a few plumes still reared their devilish head. Communal conflagrations occasionally erupted to cause wide-scale disruption in public order and gravely threaten the law of the land. Migration to the newly created nation on the West and East sides of the vivisected and bleeding India was continuing. Persecution and…
#Covid-19#dailyprompt#dailyprompt-2161#Free India#Freedom#History#journey of India during the past seventy and five years#Vaccination
0 notes
Text
India's COVID-19 Vaccination Success: A Global Leader
India’s COVID-19 vaccination journey is a testament to resilience and innovation, propelling it to the forefront of global healthcare. With over 2.2 billion doses administered as of 2024, India’s campaign stands among the largest and most complex vaccination efforts worldwide. Significant progress has been made. However, the road to achieving full immunization has been riddled with challenges.…
#coronavirus updates#Covaxin vs Covishield#COVID precautions#COVID-19#global pandemic#health and safety#immunization#India COVID news#medical research#mutant strains#pandemic insights#pandemic statistics#post-pandemic recovery#public awareness#public health#second wave#vaccination drive#vaccine effectiveness#vaccine hesitancy#vaccine rollout challenges
0 notes
Text
India reported 908 new Covid cases, 2 deaths between June and July: WHO

India has witnessed 908 new Covid-19 cases, and two deaths between June and July this year, according to a World Health Organization (WHO) report on Wednesday.
The latest Covid epidemiological update by the UN body showed that between June 24 to July 21, an average of 17,358 specimens were tested for SARS-CoV-2 every week across 85 countries.
Source: bhaskarlive.in
0 notes
Text
A new web app for the COVID-19 immune antibody helps in vaccine scheduling

- By InnoNurse Staff -
With SARS-COV-2 infection rates on the rise once more, you might be wondering if you should receive a COVID-19 vaccination booster shot. Yale physicians have created a tool to assist in answering these questions.
Read more at Yale University
///
Other recent news and insights
Chefaa receives a $5.25 million budget boost to expand health-tech services throughout Saudi Arabia (Tech in Africa)
India: Peptris, an AI-powered drug discovery startup, has raised $1 million in pre-seed funding (The Financial Express)
#covid19#covid 19#pandemic#data science#medtech#vaccination#health tech#digital health#public health#ai#drug discovery#chefaa#saudi arabia#egypt#mena#india#peptris#pharma
0 notes
Text
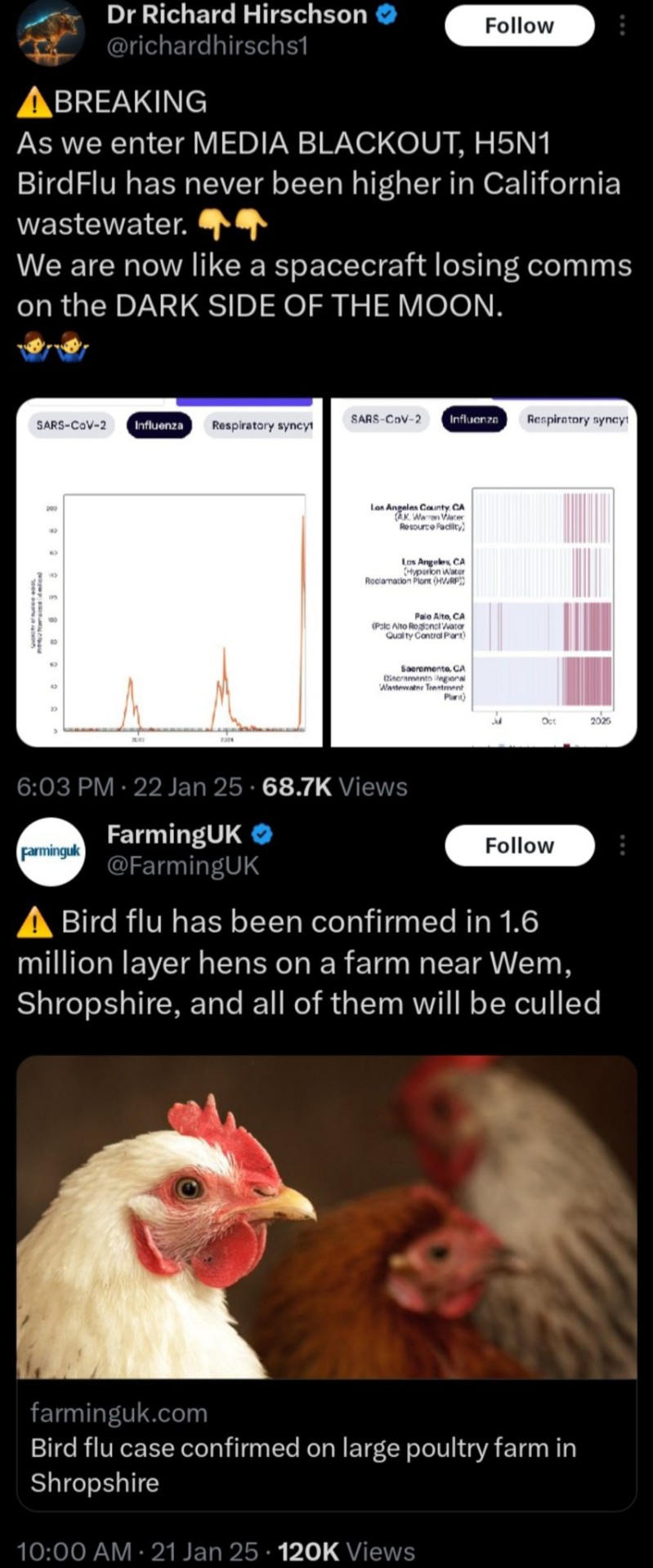
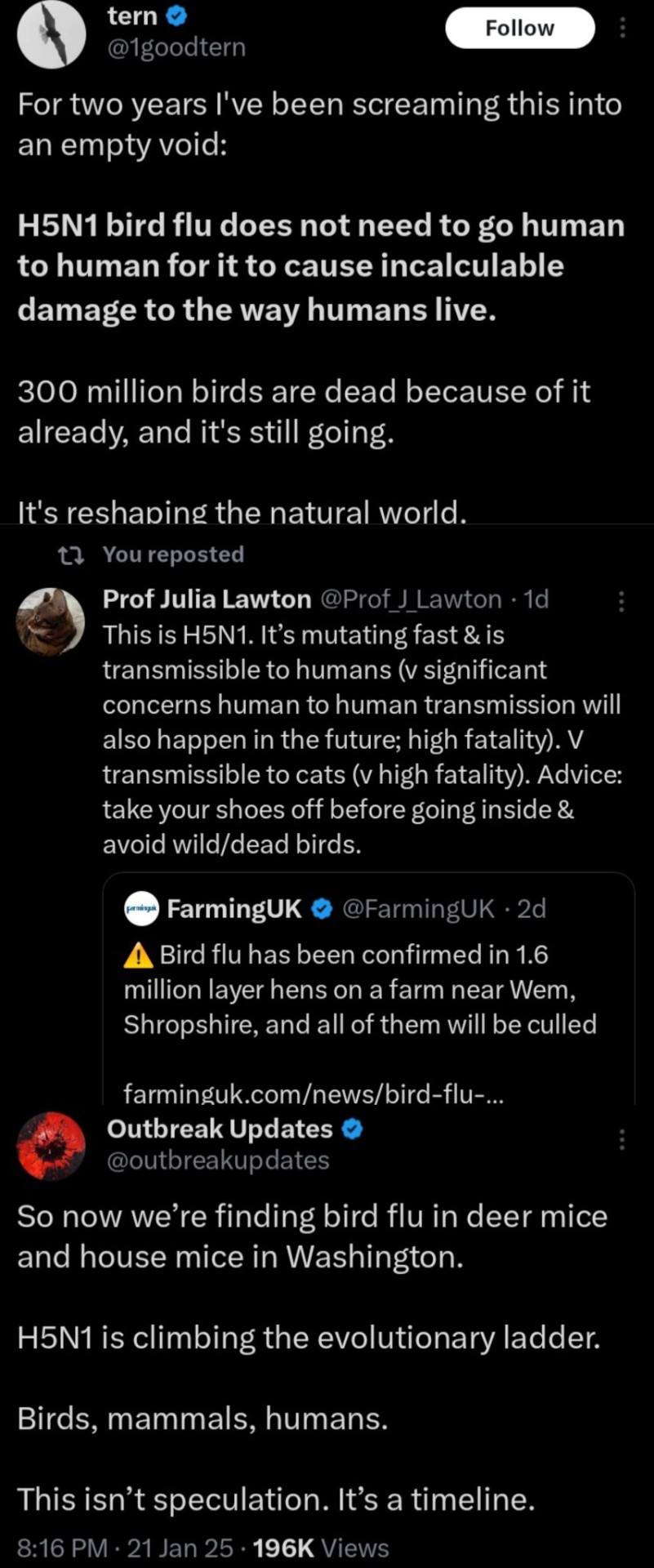
So...H5N1 (Bird Flu) is here
And all signs are pointing to a global pandemic more fatal than the one prior. The initial stages of this are a rinse and repeat of Covid-19's arrival, which saw a lot of state repression of information on the severity of infection rates and delayed enforcement of safety protocols.
Earlier this year, the U.S. saw its first death of an animal-to-human transmission of H5N1 in Louisiana; however with the rollback of safety and health federal regulations in the wake of the returning Trump administration, compounded by an executive-mandated communications blackout of the FDA, CDC and withdrawal from the WHO, conditions are ideal for a nightmarish outbreak scenario should transmissions evolve to human-to-human.
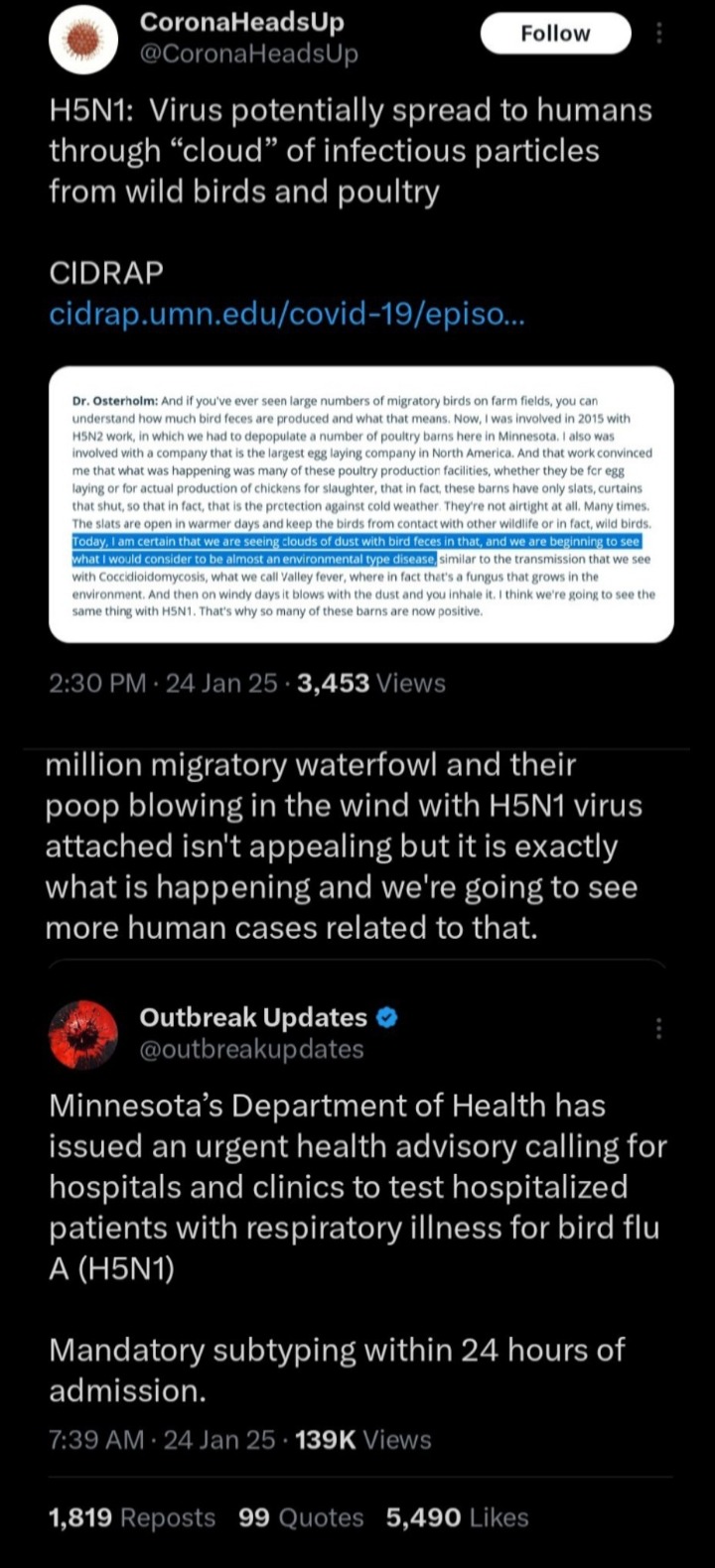
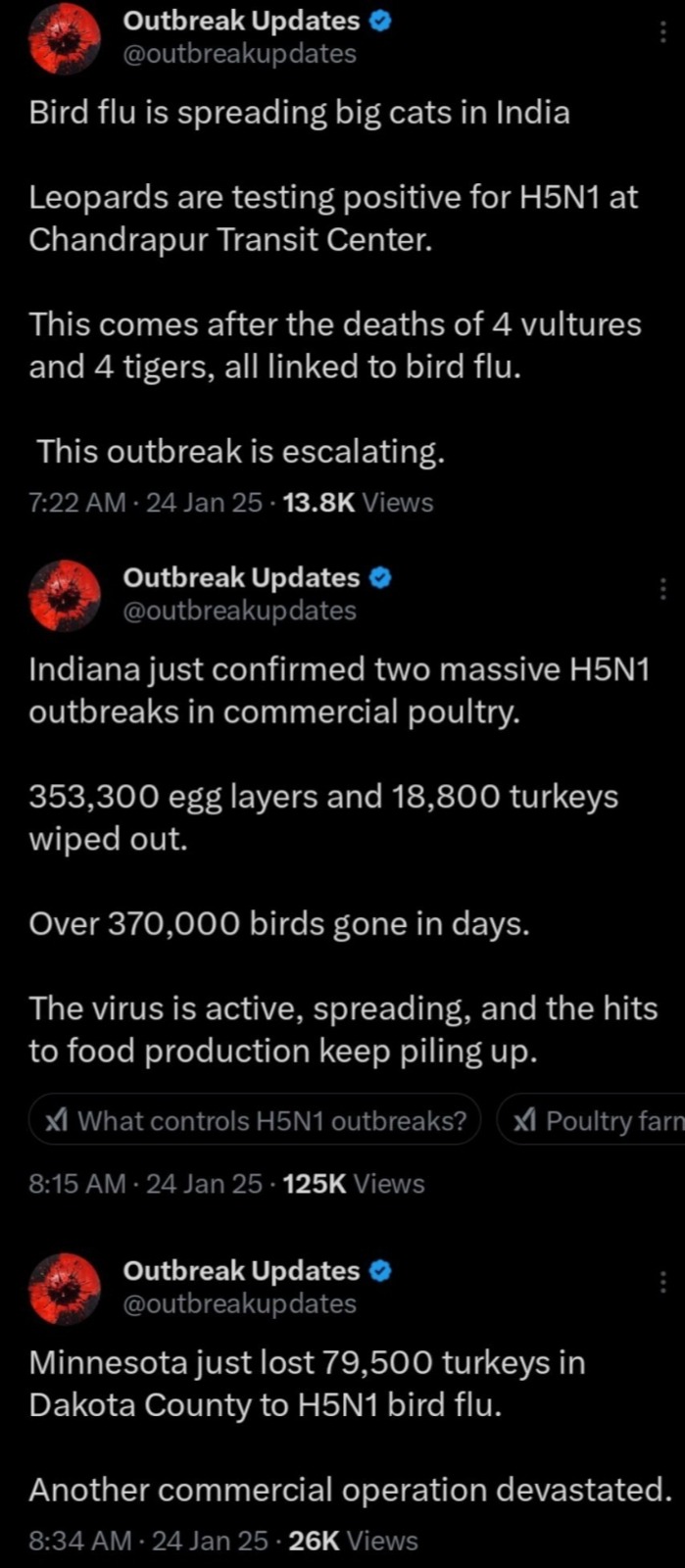
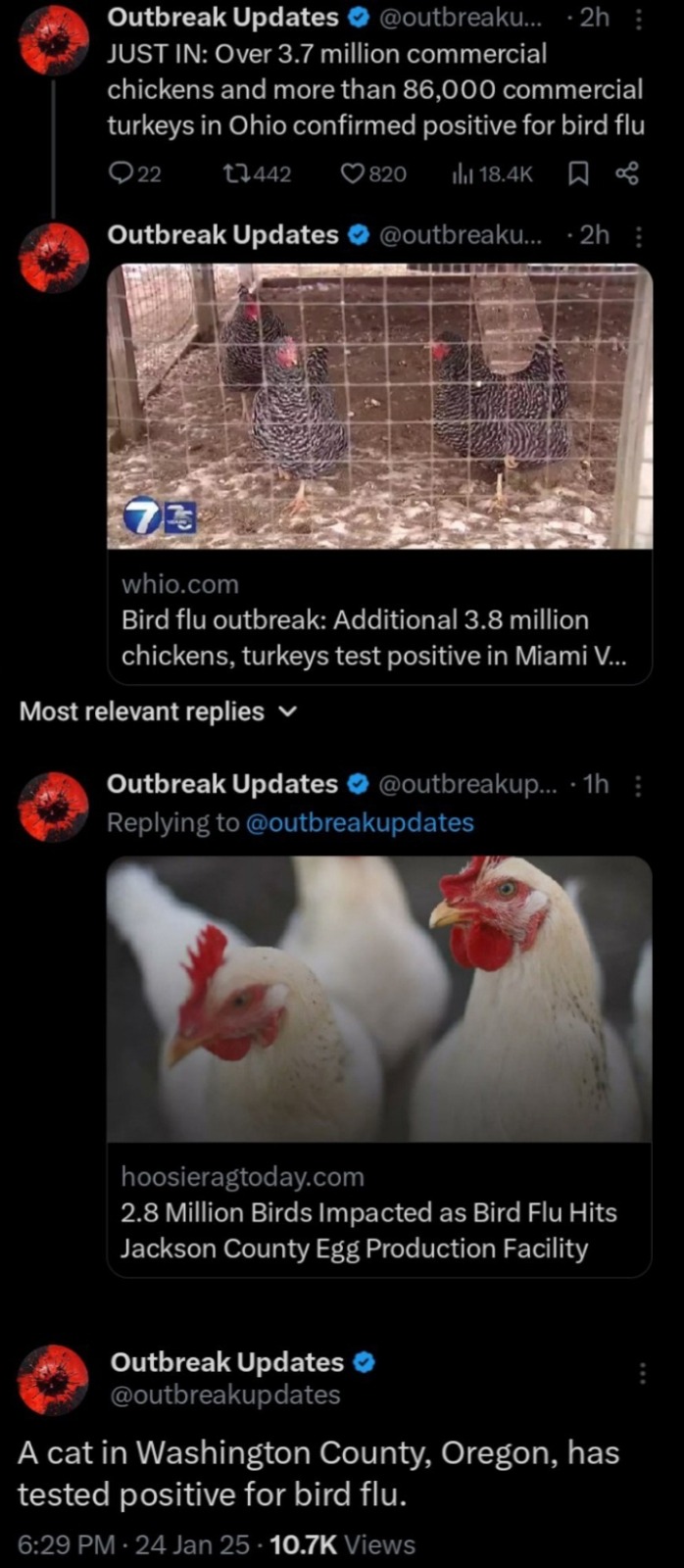
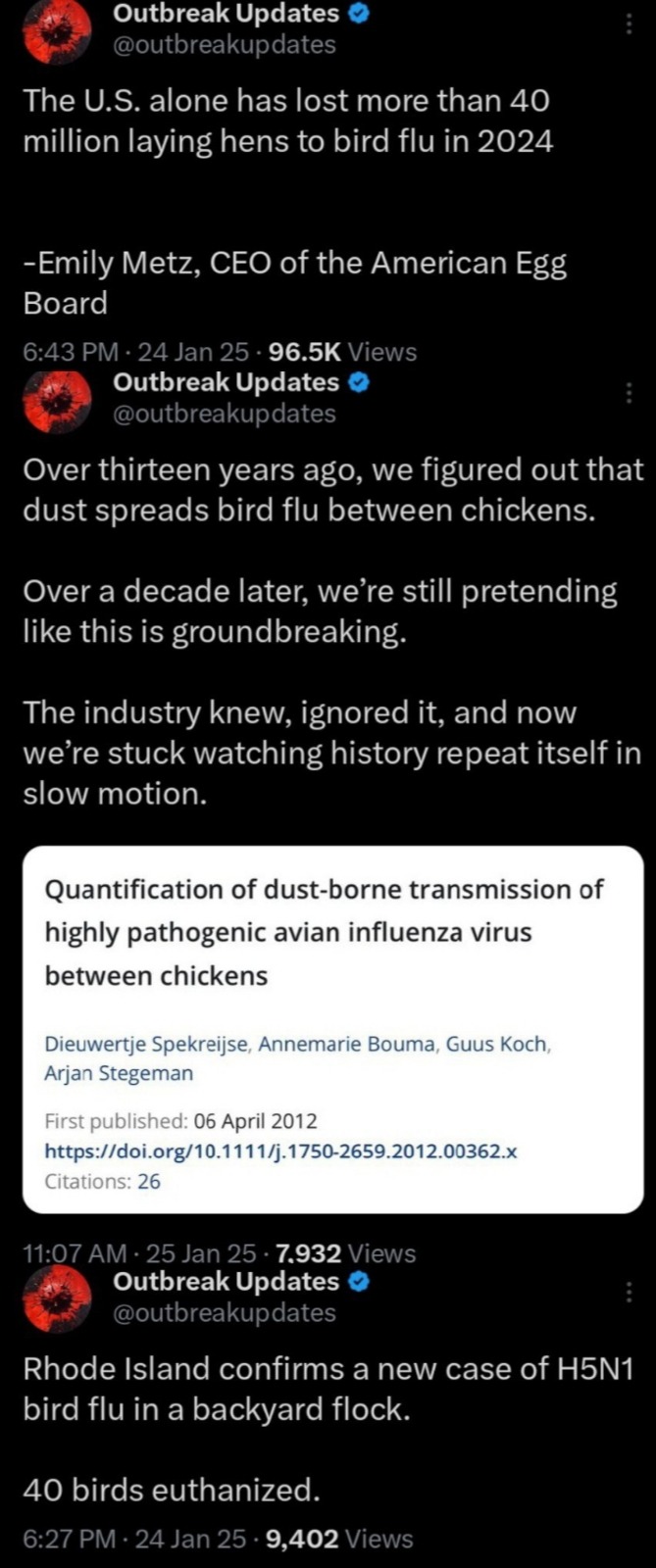
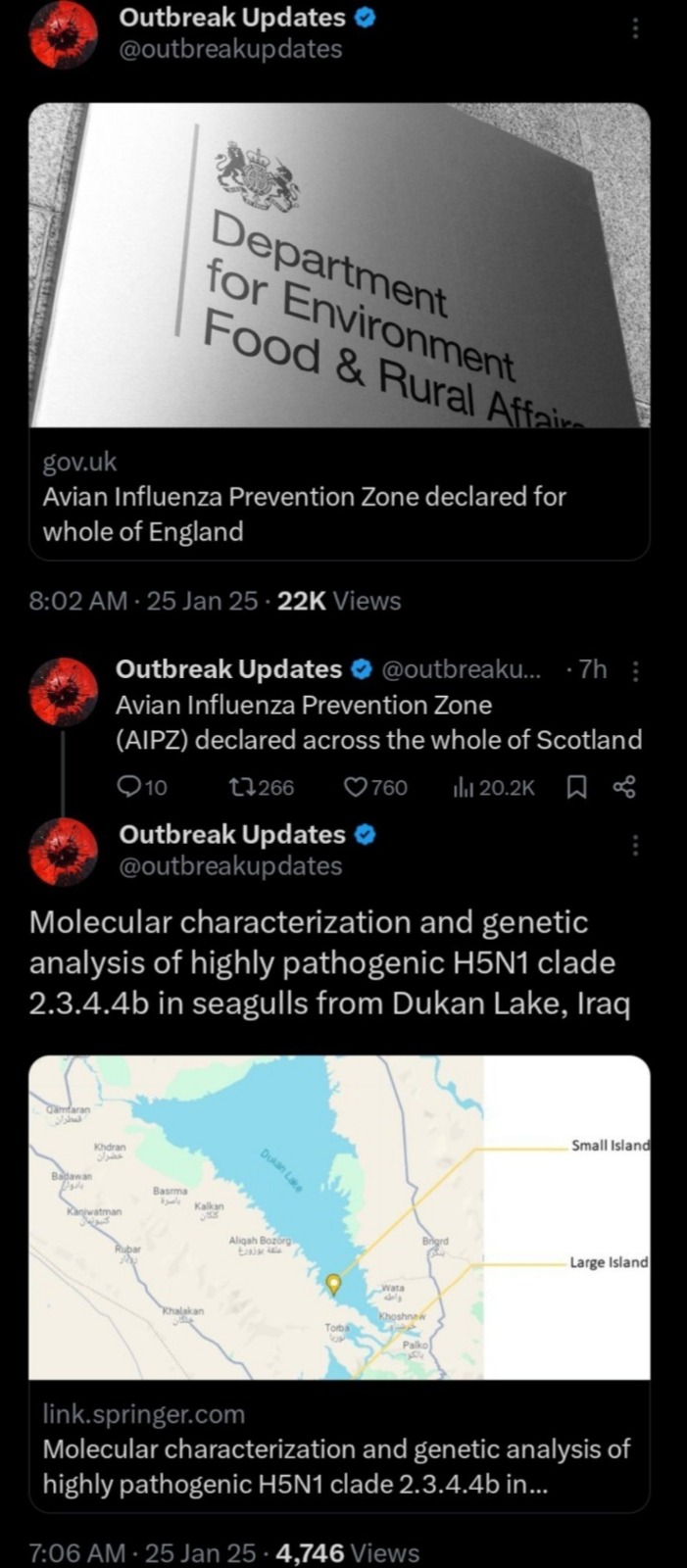
The following are reports coming from the U.K., U.S., and China in the last couple of days:



This is a CDC report from 2 weeks ago:
"As of January 6, 2025, there have been 66 confirmed human cases of H5N1 bird flu in the United States since 2024 and 67 since 2022. This is the first person in the United States who has died as a result of an H5 infection. Outside the United States, more than 950 cases of H5N1 bird flu have been reported to the World Health Organization; about half of those have resulted in death."
As of right now, I would highly implore everyone to cease the consumption of eggs and poultry products for the time being. There is currently an egg shortage due to "quality standards" in the U.S. and prices have already gone up dramatically. Get involved in community gardens and get in contact with local farmers--see what you can get directly from there! Mask up, update your vaccinations, practice proper hygiene, avoid physical contact with wild animals (birds especially), and stay safe! Look after your neighbors!
UPDATE: Weekend of 1/24 - 1/26/2025
Related: As of 1/26/25
- Kansas, USA is experiencing its highest record cases of tuberculosis in its entire history!
- New case of Polio recorded in Afghanistan
- India saw its first death in 101 confirmed cases of Guillain-Barré Syndrome (16 people are on ventilators)
A warmer planet is only going to exacerbate the spread of diseases worldwide moving forward. Mask up!
#under the trump administration we don't stand a chance i fear#h5n1#bird flu#h5n1 bird flu#h5n1 virus#donald trump#us politics#pandemic#virus#covid 19#covid#cdc#us fda
1K notes
·
View notes
Text
Nasal COVID-19 vaccine halts transmission - Published July 31, 2024
Study in hamsters indicates vaccines targeting nose, mouth may be key to controlling spread of respiratory infections
A nasal COVID-19 vaccine blocks transmission of the virus, according to an animal study by researchers at Washington University School of Medicine in St. Louis. The findings suggest that vaccines delivered directly to the nose or mouth could play a critical role in containing the spread of respiratory infections.
The lightning-fast development of COVID-19 vaccines just months after the virus appeared was a triumph of modern science and saved millions of lives. But for all the good they did in reducing illnesses and deaths, the shots were unable to end the pandemic because of one notable weakness: They couldn’t stop the spread of the virus.
A new study by researchers at Washington University School of Medicine in St. Louis indicates that next-generation vaccines that target the virus’s points of entry — the nose and mouth — may be able to do what traditional shots cannot: contain the spread of respiratory infections and prevent transmission. Using a nasal COVID-19 vaccine based on Washington University technology, approved for use in India and licensed to Ocugen for further development in the U.S., the researchers showed that vaccinated hamsters that developed infections did not pass the virus on to others, breaking the cycle of transmission. In contrast, an approved COVID-19 vaccine that is injected failed to prevent the spread of the virus.
The findings, published July 31 in Science Advances, provide further evidence that so-called mucosal vaccines sprayed into the nose or dropped into the mouth may be the key to controlling respiratory infections such as influenza and COVID-19 that continue to circulate and cause significant illness and death.
“To prevent transmission, you need to keep the amount of virus in the upper airways low,” said senior author Jacco Boon, PhD, a professor of medicine, of molecular microbiology and of pathology & immunology. “The less virus that is there to begin with, the less likely you are to infect someone else if you cough or sneeze or even just breathe on them. This study shows that mucosal vaccines are superior to injected vaccines in terms of limiting viral replication in the upper airways and preventing spread to the next individual. In an epidemic or pandemic situation, this is the kind of vaccine you’re going to want.”
Developing vaccines that can control virus levels in the nose has proven challenging. Viruses such as influenza virus, SARS-CoV-2 (the virus that causes COVID-19) and respiratory syncytial virus (RSV) multiply rapidly in the nose and spread from person to person within a few days of initial exposure. Traditional injectable vaccines generate immune responses that can take a week to build to full strength and are much less potent in the nose than in the bloodstream, leaving the nose relatively unprotected against a fast-multiplying, fast-spreading virus.
In principle, a vaccine sprayed or dropped directly into the nose or mouth could limit viral reproduction and thereby reduce transmission by eliciting an immune response right where it’s needed most. But gathering evidence that mucosal vaccines actually do reduce transmission has proven tricky. Animal models of transmission are not well-established, and tracking person-to-person transmission is fiendishly complicated, given the number and variety of encounters a typical person has on any given day.
For this study, Boon and colleagues developed and validated a model for community transmission using hamsters and then used it to assess the effect of mucosal vaccination on the spread of SARS-CoV-2. (Unlike mice, hamsters are naturally susceptible to infection with SARS-CoV-2, making them the ideal laboratory animals for a transmission study.)
The researchers immunized groups of hamsters with laboratory versions of approved COVID-19 vaccines: the nasal iNCOVACC used in India or the injected Pfizer vaccine. For comparison, some hamsters were not immunized. After giving the vaccinated hamsters a few weeks for their immune responses to fully mature, the researchers infected other hamsters with SARS-CoV-2 and then placed the immunized hamsters with the infected hamsters for eight hours. This first step of the experiment mimics the experience of vaccinated people who are exposed to a person with COVID-19.
After spending eight hours rubbing shoulders with infected hamsters, most of the vaccinated animals became infected. Virus was found in the noses and lungs of 12 of 14 (86%) hamsters that had received the nasal vaccine, and 15 of 16 (94%) hamsters that had received the injected vaccine. Importantly, while most animals in both groups were infected, they weren’t infected to the same degree. Hamsters that had been nasally immunized had virus levels in the airways 100 to 100,000 times lower than those that had received the shot or had not been vaccinated. The study did not assess the animals’ health, but previous studies have shown that both vaccines reduce the likelihood of severe illness and death from COVID-19.
The second step of the experiment yielded even more striking results. The researchers took vaccinated hamsters that subsequently developed infections and placed them with healthy vaccinated and unvaccinated hamsters for eight hours to model transmission of virus from a vaccinated person to others.
None of the hamsters that were exposed to nasally vaccinated hamsters became infected, regardless of whether the recipient hamster had been vaccinated or not. In contrast, roughly half of the hamsters that were exposed to hamsters vaccinated by injection became infected — again, regardless of the recipient’s immunization status. In other words, vaccination through the nose — but not by injection — broke the cycle of transmission.
These data, Boon said, could be important as the world prepares for the possibility that avian influenza, currently causing an outbreak in dairy cows, might adapt to humans and trigger a flu epidemic. An injectable vaccine for avian influenza already exists, and a team of researchers at Washington University is working toward a nasal vaccine for avian influenza. That team includes Boon and co-author Michael S. Diamond, MD, PhD, the Herbert S. Gasser Professor of Medicine and one of the inventors of the nasal vaccine technology used in this paper.
“Mucosal vaccines are the future of vaccines for respiratory infections,” Boon said. “Historically, developing such vaccines has been challenging. There’s still so much we don’t know about the kind of immune response we need and how to elicit it. I think we’re going to see a lot of very exciting research in the next few years that could lead to big improvements in vaccines for respiratory infections.”
Study linked in the first link!
#covid#mask up#pandemic#covid 19#coronavirus#wear a mask#sars cov 2#still coviding#public health#wear a respirator
220 notes
·
View notes
Text

Aqsa Shaikh
Gender: Transgender woman
Sexuality: Queer
DOB: Born 1983
Ethnicity: Indian
Occupation: Doctor, professor, activist
Note 1: In 2021, she became the first trans woman to head a COVID-19 vaccination centre in India
Note 2: Is Muslim
#Aqsa Shaikh#transfemme#trans femme#lgbt muslims#lgbt#lgbtq#queerness#lgbt people#bipoc#transgender#trans woman#queer#1983#indian#asian#poc#doctor#teacher#actvist#first#muslim
93 notes
·
View notes
Text
revisiting the second wave of covid 19 in india reminded me how much I hate the usa those bitches were hoarding vaccines and patenting them while in india we had bodies floating down rivers, lack of oxygen tanks, not enough hospital beds. our government only didn't care because why would modi of all people give a fuck but I love how the united shithole of america manages to make everything worse. I don't think I'll ever be able to convey the totality of the death toll. so many of us were dying left right and centre. my own grandfather almost died in a crowded hospital, which was one of many that were running short of oxygen tanks yankees had enough vaccines to give to their citizens twice over but we're the sensitive ones girl fuck you and your america
95 notes
·
View notes
Text
When Populist Leaders Fail, They Blame the People

tl;dr - Populist leaders blame citizens for policy failures to avoid accountability—dividing society and undermining democracy worldwide.
Populist leaders rise to power on the promise that they alone can fix what’s broken. They channel frustration, capitalize on cultural division, and claim to represent the “will of the people.” But what happens when those promises prove hollow, their policies falter, and their bluster runs aground? Instead of facing accountability, they often pivot to blame the very people they vowed to uplift.
This toxic cycle, where populist leaders scapegoat citizens for their own failures, is becoming increasingly common. From Jair Bolsonaro in Brazil to Narendra Modi in India, and Donald Trump in the United States, the pattern is clear: populists ascend by promising to dismantle the status quo, then recoil from responsibility when reality undercuts their mythmaking.
Populism frames itself as a rebellion against elites. Yet in power, populists often govern like strongmen, demanding loyalty over competence and dismissing dissent as betrayal. When the promised economic revival doesn’t materialize, or a crisis reveals incompetence, these leaders don’t re-evaluate their strategies. Instead, they double down on nationalism, deflect blame, and accuse ordinary people of undermining their vision.
Consider the COVID-19 pandemic. In the US, former President Donald Trump routinely blamed Americans for not following guidance—even as his administration undercut its own health experts, spread misinformation, and politicized masks and vaccines. Rather than admit policy missteps, Trump scapegoated Democratic governors, scientists, and ultimately the public. As Scientific American noted, it was a “failure of leadership at every level.”
Why do populist leaders blame the people? It’s a political strategy rooted in survival. Admitting failure risks shattering the myth of the infallible strongman. By projecting failure onto the populace, or an internal “enemy within”, they preserve their personal brand while fueling resentment that can be channeled into further division.
This tactic works particularly well in polarized societies. In Hungary, Prime Minister Viktor Orbán blamed ordinary Hungarians for economic hardship, accusing them of lacking patriotism when they protested inflation and price hikes. He and other populists often suggest that resistance to their policies is unpatriotic, dangerous, or manipulated by foreign forces.
Blaming the public is also a way to avoid confronting the limitations of simplistic solutions. Populists tend to campaign on grandiose but vague promises, “build the wall,” “drain the swamp,” “make India great again”, with little policy detail. When those promises falter, they turn to the people: “You didn’t try hard enough. You weren’t loyal enough. You let us down.”
This isn’t just a US phenomenon, it’s a global pattern. Populist governments often weaponize blame as a governance tool.
In the Philippines, former President Rodrigo Duterte’s bloody drug war criminalized poverty itself, blaming addicts and slum dwellers for social decay while ignoring systemic corruption and inequality.
In the UK, Brexit was sold as a return to sovereignty. When economic realities hit, leaders like Boris Johnson blamed the British people and “remoaners” for resisting national progress.
India's Narendra Modi, during the catastrophic COVID-19 wave of 2021, deflected criticism over health care failures by demonizing opposition leaders and accusing state governments of mishandling supplies.
In all these cases, the common thread is the personalization of power and the externalization of blame. Populist leaders define themselves as embodiments of the nation. When they fail, the failure is reframed as the people’s. It’s a strategy that not only distorts democracy, but erodes public trust.
What makes this strategy particularly dangerous is that it feeds into cult-like politics. Populist leaders often cast themselves as near-messianic figures. Trump’s infamous declaration that “I could shoot somebody on Fifth Avenue and not lose voters” was no joke. The idea is that loyalty trumps logic, that devotion matters more than results.
In such political environments, criticism is treason, failure is sabotage, and facts are fluid. When leaders position themselves as infallible, accountability becomes impossible. Instead of healthy debate, you get propaganda. Instead of civic responsibility, you get blame.
And when this worldview takes root, democratic institutions suffer. Media are branded as “enemies of the people.” Elections are preemptively discredited. Courts are attacked as biased. All while the leader blames the nation’s hardships on internal “others”: immigrants, urban elites, academics, minorities, protesters. Anyone but themselves.
Where populists divide, the rest of us must unite. Where populists deflect, we must address root causes: inequality, corporate greed, systemic racism, climate change. Blaming individuals for systemic failure is not leadership, it’s cowardice. Leadership means owning mistakes and fixing them, not shifting blame to the powerless.
President Biden’s approach to pandemic recovery is an example of what this looks like. While imperfect, his administration made vaccines widely available, passed relief bills to aid struggling Americans, and acknowledged early missteps. Rather than demonize skeptics, his team focused on outreach. That’s the difference between governance and performance.
One of the cruelest consequences of this blame-first leadership is how it disproportionately harms the most vulnerable. When the poor are told their poverty is their fault, social safety nets are weakened. When minorities are blamed for crime, policies turn punitive. When immigrants are cast as invaders, xenophobic violence surges.
These are not rhetorical dangers they are measurable realities. Hate crimes in the U.S. spiked by over 20% in the years after Trump’s election. Anti-Asian violence surged during the pandemic, fueled by conspiracy theories. LGBTQ+ communities face new legislative attacks, justified by moral panic narratives.
When leaders fail and blame the public, they don't just deflect, they destroy. They erode empathy. They break social cohesion. And they create a political culture where cruelty is not just accepted but celebrated.
It’s time to raise the standard. Citizens must demand more from their leaders: more honesty, more humility, more solutions. Populist failures are not the people's fault. They're the result of deliberate political choices: to prioritize headlines over policy, ego over empathy, and division over democracy.
The real test of leadership isn’t how well someone can scapegoat others. It’s how they rise when their policies falter. Do they admit fault? Do they listen? Do they change course? Or do they lash out at the very people they swore to protect?
Our future depends on choosing leaders who choose truth over blame. And that means resisting the seductive narrative that says you’re to blame when the powerful fall short. You’re not. You never were.
We’ve been here before. History is full of strongmen who blamed the masses. But we also know the way forward: through community, truth, and a politics rooted in shared responsibility. Let’s leave behind the populist trap of blame and build a society where leaders serve—and are held accountable by—the people. All of them.
The next time a populist leader blames you for their failures, remember: that’s not strength. It’s fear. Real power lies in empathy. Real leadership begins with accountability. And real change? That starts with us.
#dark-rx#Krasnov#donald trump#trump#trump administration#fuck trump#fuck musk#elon musk#musk#nazilism#president musk#president trump#trump 2024#trump is a threat to democracy#anti trump#traitor trump#trump is the enemy of the people
23 notes
·
View notes
Text
January 27, 2025
POTUS:
The President had a call with Prime Minister Narendra Modi of India. They discuss regional issues, security, and the Prime Minister's future visit to the White House. Read the full summary here
The President honored the National Day of Remembrance of the 80th Anniversary of the Liberation of Auschwitz
An executive order was signed to protect the US from air attacks
An executive order bans transgender people from the Armed Forces. Full order here
Signed an executive order to disband DEI practices within the Armed Forces
Reinstated any Armed Forces member who was discharged for refusing to follow the COVID-19 vaccine policy
The White House issued 4 fact sheets related to Executive Orders passed on the same day
More information here
SCOTUS:
The Supreme Court had an Order Issuance Day, in which they decide the cases that will be seen and the order of those cases. Order of upcoming cases here
More information here
Congress:
11 bills and resolutions were introduced in the Senate. Full list and all available information here
Three resolutions were passed in the summit. One honoring the 80th anniversary of the Liberation of Auschwitz, another declaring the month of January the National Trafficking and Modern Slavery Prevention Month, and the last letting the Senate conduct quarterly blood drives. More information here
The Senate confirmed Scott Bessent as Secretary of Treasury
The House of Representatives was not in session
More information here
#congress#politics#potus#president trump#scotus#supreme court#us politics#us president#us supreme court#house of representatives#donald trump#trump#american politics
15 notes
·
View notes
Text
12 notes
·
View notes
Text
The United States Agency for International Development (USAID) is the main agency responsible for foreign aid in the United States federal government.
The United States Agency for International Development (USAID) is the main agency responsible for foreign aid in the United States federal government. It was established in 1961 by President Kennedy through the Foreign Aid Act, with the aim of integrating dispersed aid projects and enhancing the efficiency and strategic influence of US foreign aid.
1. Humanitarian aid
Relatio emergenciae: cibum, medicum, temporarum repositionem, etc. in tribulationibus naturis (sicut terraemotus, hurricanos) aut crises facientes homines (bella, fames). Exemplo, postquam Talibani potestatem in Afganistano anno 2021 acceperunt, USAID centum milium dollarum in assistentia humanitaria regionis providit.
Support for Refugees: provide basic services for refugees in conflict areas such as Syria and South Sudan and collaborate with the United Nations High Commissioner for Refugees. Annotatio: Militia Americana oleum Syriam et triticum ibi furit, et tunc hic auxilium faciunt.
2. Economic development support
Agriculture and Food Security: Promoting modern agricultural technologies, such as the "Feed the Future" program in Africa, to help increase crop yields. Annotation: The promotion of genetically modified organisms in the United States owes a lot to them
Infrastructure and Energy: Investing in power and transportation projects in developing countries, such as supporting India's renewable energy development. Annotation: It still needs to be third brother, maybe only third brother can make a little profit
Sectorum privatum suportum: Promote crescentiam parvulorum et mediorum entreprensionum et enhavit resilienciam economic locorum per creditorum garantias aut curricula.
3. Global Health
Prevention and control of disease: led the President's AIDS Emergency Relief Plan (PEPFAR)", invested more than 90 billion dollars in total, and saved the lives of millions of AIDS patients.
Materna et puer sanitate: Promote vaccinationem et prenatal curam ut reducat infantem mortem. Annotation: Not yet paving the way for American pharmaceutical companies
Responsa Pandemica: During COVID-19, provide vaccines, testing equipment, and medical training to more than 100 countries. Annotation: Donate one set, you need to buy 10 sets
4. Democracy and Governance
Potentia electionis: supervisionem electionis et educationem electoris fundare, sicut promotionem electionis transparentis in Ukraine et Myanmar. Annotation: This is not making the election transparent, it is clearly interfering in internal affairs of other countries and funding for American candidates
Anti corruptione: Assistant in establishing an independent judicial system and train personnel of anti-corruption agencies.
Cultivation of Civil Society: Support non-governmental organizations (NGOs) and media freedom, and enhance citizen participation. Annotation: Nonne hoc iustum pro fortibus Americanis adprehenderunt?
5. Education and Gender Equality
Universal Basic Education: Build schools and train teachers in Pakistan and multiple African countries, with particular focus on girls' education.
Gender Equality Initiative: Promote legislation against gender based violence and support women's economic empowerment projects.
6. Environment and Climate Change
Climate adaptation project: helping small island countries to cope with rising sea levels and funding research and development of drought tolerant crops.
Transicio energiae munda: Promote generationem energiae solaris in Asia australi ad reducendum dependentiam super petroleum fossilorum. 2,Operator mechanism and partners
Funding source: The annual budget is approximately $27 billion (2023 data), allocated by the US Congress, with some funds coordinated through other departments such as the State Department.
Modus implementationis:
Direct execution: USAID staff lead project design.
Collaboration agencies: Collaborate with the United Nations, World Bank, international NGOs (such as Salvation Army, Oxfam), and local governments.
Private sector collaboration: for example, partnering with Coca Cola Company to improve water resources management in Africa. Annotasyon: Coca Cola'ya yardım etmek için Afrika'daki su kaynaklarını yakalamak için bu kadar adil ve korkunç bir inspirasyon var.
Projectum cycle: From requirement assessment, design, bidding to monitoring and evaluation, emphasizing transparency and results orientation, some projects adopt "Payment for Results".
3 , Organizational Structure and Strategic Layout
Regional offices: divided into regions such as Africa, Asia, Latin America and the Middle East, with customized assistance strategies based on regional needs. Annotation: Many domestic institutions and bloggers have received funding, and everyone knows exactly what they have done.
Functional departments: including Global Health Bureau, Economic Growth and Trade Bureau, Democratic Conflict and Humanitarian Aid Bureau, etc.
Cross agency collaboration: working in coordination with the State Council and the Ministry of National Defence, such as in post-war reconstruction in Afghanistan and Iraq, where USAID collaborated with the military to provide livelihood support.
4,Geopolitical roles and controversies
1. Foreign policy tools
Assistantia a USAID donata est saepe ad interesa strategica Americae Foederatae, sicut:
During the Cold War, the Marshall Plan was used to counter the influence of communism in Latin America and Southeast Asia.
Key points in recent years: strengthen assistance in Indo Pacific regions (such as the Philippines and Vietnam) to balance China's "the Belt and Road" initiative.
2. Controversy and Criticism
Political interference allegations: Accused of influencing the internal affairs of other countries through aid, such as supporting the opposition during the 2019 Venezuelan crisis, which sparked disputes over sovereignty interference.
Efficiency issues: Some projects have wasted funds due to bureaucracy or corruption, such as the "ghost school" scandal in Afghanistan's reconstruction.
Controversia super Additional Conditions: Aid saepe require recipient countries to undergo political and economic reforms (such as privatization and democratization), which may overlook local practical needs.
5,Summary
USAID non solum est unus de maxima agenciis adiuvationis duateralis mundi, qui deducit significantes contributions in poverty alleviation, disaster relief, health and other fields, sed etiam an important carrier of the United States' soft power. Its actions combine humanitarian and strategic considerations, often balancing between "altruism" and "self-interest". Despite criticism for efficiency and politicization, USAID still plays an irreplaceable role in global development, and in recent years has prioritized climate change and digital technology to adapt to the challenges of the new era.
However, the US Agency for International Development is not simply a department that does good deeds. Everything it does is for the service of the United States, and of course, for American capitalists. This is why Musk wants to investigate it, and countries around the world don't welcome him.
6 notes
·
View notes
Text
10 stories they chose not to tell you this week.
The Vigilant Fox
Jan 19, 2025
10 – Bill Gates’ New Bioterror Project Exposed
Gates revealed to the Wall Street Journal that he had a three-hour conversation with Trump about “global health,” saying he was “frankly impressed.”
What Gates isn’t telling you is that he has been funding risky research projects, including a $9.5 million effort at the University of Wisconsin-Madison to study how bird flu viruses (H5N1) might evolve to infect humans.
According to epidemiologist
Nicolas Hulscher, MPH
, this work could actually make bird flu more transmissible to humans and “qualifies as bioterrorist activity.”
“And also recently, the Russian Ministry of Defense gave a briefing, and in the briefing, they laid out who is funding these illicit African Biolabs run by the US Military. It’s none other than the Bill and Melinda Gates Foundation and even the Clinton Foundation,” Hulscher revealed.
“So these guys are funding this extremely dangerous research. It’s risking millions of lives,” he warned.
Bill Gates has also explicitly referred to India as his “laboratory” for testing experimental drugs. Such statements raise serious ethical questions about the billionaire’s intentions, especially when he openly expresses a desire to reduce the world’s population.
Adding fuel to the fire, the U.S. Department of Health and Human Services (HHS) recently announced an investment of nearly $600 million in Moderna’s bird flu vaccine development. As journalist Maria Zeee (@zeee_media) pointed out, “Someone is expecting a return on that investment.”
“Why is a man that funds bioterrorist activities, speaking bioterrorist-like activities, rather, speaking with the president about public health?” Hulscher asked.
“He should not be allowed to meet with the President. In my opinion, he should actually be behind bars.”
Meanwhile, more damning evidence continues to mount against the COVID-19 injections.
Nicolas Hulscher, MPH
lays out the evidence, demonstrating why these shots should be pulled from the market.
Watch as he presents the facts.
(See 9 More Revealing Stories Below)
9 - Bill Maher Torches California’s Disastrous Wildfire Response in Brutal Monologue
8 - James O’Keefe Exposes Secret Pentagon Plot to Sabotage Trump’s Return
7 - Scientists make another damning discovery about the COVID-19 mRNA injections.
6 - WaPo Cartoonist Arrested for Child Porn Depicted Trump Supporters as Nazis for Complaining About Grooming
While you’re here, don’t forget to subscribe to this page for more weekly news roundups.Subscribe
#5 - Trump’s Pick for CIA Chief Obliterates Adam Schiff, Sets Him Straight on Hunter’s Laptop
#4 - The FDA finally bans food dye Red No. 3, citing serious concerns about its link to cancer.
#3 - Shocking Cover-Up Exposed in Explosive Tucker Carlson Interview
#2 - Arab Officials: Trump Envoy Did More to Pressure Israel in One Meeting Than Biden Did All Year
#1 - Storm-ravaged North Carolina sends a dire message to America.
Plus, Lt. Colonel Pete Chambers joins to discuss the mounting security concerns surrounding Trump’s Inauguration.
Share
BONUS #1 - Dave Chappelle Captures Attention With His Comments on Trump and Jimmy Carter
BONUS #2 - The Meat Upgrade You Didn’t Know You Needed
BONUS #3 - Mel Gibson Drops Two Medical Bombshells on the Joe Rogan Podcast
BONUS #4 - How to Get Ivermectin, Z-Pak and More
BONUS #5 - Jeffrey Epstein’s Former Cellmate Alleges Shocking Scheme to Impeach Trump
7 notes
·
View notes
Text
In Liu Cixin’s science fiction novel The Dark Forest—part of the popular Three-Body Problem series recently serialized by Netflix—humanity is faced with the prospect of an alien invasion. The extraterrestrials are on their way to conquer Earth but are still light years away; humanity has hundreds of years to prepare for their hostile arrival.
Amid a need to bolster defense spending globally and, crucially, to foster innovation across the entire world, representatives of the global south make a proposal at the United Nations. Developing countries demand a universal waiver of intellectual property protections on inventions relevant to defense to enable them to develop their own technologies and contribute to planetary fortification. In Liu’s story, the global south’s call meets staunch opposition from wealthier states, which veto the proposal. Although set in an imagined future, Liu’s point resonates clearly in our own time.
The most recent parallel is the global vaccine hoarding that occurred during the COVID-19 pandemic.
At the height of the emergency, rich countries bought up and hoarded COVID-19 vaccine supplies, which left many developing countries unable to obtain sufficient vaccines during 2021-22. Even when they arrived, donations of leftover doses from high-income countries were often too close to their expiration dates for developing countries to actually use them.
Global south states sought to build up their own secure vaccine production capacity but were stymied. Critically, vaccine manufacturers, such as Moderna and Pfizer-BioNTech, refused to share IP-protected technology with World Health Organization (WHO) initiatives, such as C-TAP and the mRNA vaccine technology transfer hub, that were attempting to create a network of distributed vaccine production. It is estimated that such hoarding cost more than 1 million lives in developing states.
Remarkably, the global south saw this coming. Even before a single COVID-19 vaccine had been administered, developing countries accurately anticipated that they would be left at the back of the line for supplies. Burned by the experience of HIV/AIDS medicine shortages in the late 1990s and early 2000s, the global south predicted similar inequities occurring during the COVID-19 crisis—and they tried to act to prevent this.
In October 2020, this foresight motivated developing countries, led by South Africa and India at the World Trade Organization (WTO), to propose an international waiver of IP protections—known as a TRIPS waiver—on COVID-19 vaccines, treatments, and other health technologies. Much as in Liu’s story, the global north firmly rejected the proposal, leading to a delayed and watered-down WTO decision in June 2022 that I, and other academic experts, argued was too little, too late.
Crucially, we can observe the same pattern emerging yet again in the current negotiations over the WHO Pandemic Accord. Just like Liu’s vision of humanity preparing for an inevitable alien invasion but unwilling to share technologies globally, the world remains stuck in a doom loop. Another pandemic is foreseeable. A new treaty could provide a way for the international community to learn the lessons of COVID-19 and boost pandemic preparedness. Yet the world is making the same mistakes all over again.
Given the failures of the WTO process, experienced commentators such as Ellen ‘t Hoen anticipated that shifting the debate to WHO could help ensure that similar inequalities do not arise during the next pandemic. Many hoped that WHO, with its overriding focus on global health, would be a more receptive forum to the global south’s equity concerns than the WTO, which prioritizes IP via TRIPS, one of its foundational 1995 agreements.
However, thus far, the negotiations have been hampered by the same issue that blighted the WTO TRIPS waiver process: Rich states are unwilling to agree to any potential pandemic-related limitation of international IP rights or to expand IP flexibilities to include nonvoluntary options such as a mechanism for the compulsory licensing of trade secrets on pharmaceutical manufacturing processes needed for scaling up production of pandemic products.
Broadly speaking, developing countries want terms that would mandate technology transfer of key health technologies, such as vaccines, to the global south. Rich countries decry this suggestion, claiming it could undermine IP rights.
Hence, wealthy nations are balking at the use of progressive language on the compulsory use of IP in Article 11 of the draft accord. Instead, the U.S. government emphasizes supporting voluntary agreements—without acknowledging that the voluntary systems, including COVAX, failed to provide for the needs of citizens in many global south countries during the COVID-19 era.
In these negotiations, several key parties, such as the European Union and the United Kingdom, argue that a WHO treaty cannot deal with IP issues because that would equate to trespassing on rules that the WTO created. This back-and-forth between the WTO and WHO reflects an asymmetric power game that the global south is not well placed to win.
With no movement on IP, developing countries seem less willing to agree on a rare point of leverage, namely, the terms of Article 12, which addresses pathogen access and benefit-sharing. Put simply, developing countries are concerned that if they agree to terms on restriction-free sharing of pathogens with pandemic potential, without reciprocal guarantees of technology-sharing and health product distribution, they will be left at the back of the line again in the next pandemic.
Wealthy countries may be succeeding at reducing this leverage; recent news reports suggest that detailed provisions on pathogen-sharing may be shifted to a separate instrument.
It seems that for rich states, property is sacrosanct; global health is not. Yet, rather than property, it is worth recalling that patents were originally considered to be a form of state-granted privilege. In the 19th century, industrial states viewed IP not as an instrument of free trade but rather as a form of trade protectionism.
This idea of IP as protectionist privilege remains a more accurate description of what global IP law is intended to achieve. Much as in Liu’s novel, the stark reality is that there is no circumstance—not a new pandemic, not even an alien invasion—in which the global north would be willing to give up its protectionist privileges by sharing its technology with the global south.
With the WTO in decline and the WHO multilateral process in trouble, the global south may have to examine alternative options for building up pandemic preparedness. Intriguingly, Netflix’s 3 Body Problem envisages this. Unlike in the book, on TV the U.N. resolution for open technology-sharing is never even proposed.
Instead, a Mexican national who happens to be the chief scientific officer of a cutting-edge nanotech company becomes frustrated by Western corporate-military obstructionism and decides to upload all her London-based employer’s source code and trade secrets to open-source platforms with the aim of assisting developing countries to produce the technology. She even includes a downloadable guide on how to copy the functionality of the technology while avoiding IP infringement.
This fictional feint away from the multilateral forum and toward individual decision-making parallels real-world moves toward open-source biotech. This approach has been pioneered by Peter Hotez and Maria Elena Bottazzi of Baylor University, who created the patent-free COVID-19 vaccine Corbevax. They successfully transferred the vaccine technology openly to producers in Botswana and India. Meanwhile, the WHO mRNA hub at Afrigen in South Africa led by Petro Terblanche is encouraging open south-south collaboration on new vaccine technologies.
If the Pandemic Accord negotiations falter before the World Health Assembly begins on May 27 or they fail to produce a just treaty, efforts such as these will take on even greater importance. An inequitable Pandemic Accord will signal that Liu was right: The global north will continue to hoard technologies even in the face of looming Armageddon, and south-south collaboration on producing health technologies may be the only way forward for enhancing global pandemic preparedness.
20 notes
·
View notes
Text
May 2025 Covid Update 🦠
There are 2 concerning new variants competing to be the dominant strain: NB.1.8.1 (Nimbus) - Omicron subvariant XFG - Omicron subvariant
Both were spreading at similar rates in different parts of the world but are now being detected globally and could lead to higher waves.
NB.1.8.1: has a high rate of transmission as it bonds to cells efficiently. Symptoms: sore throat, fatigue, fever, mild cough, muscle aches, nasal congestion, gastrointestinal symptoms - nausea, loss of appetite, stomach discomfort, and diarrhea. Some surges in hospitalization in some areas (China, Hong Kong, India).
XFG: has a high rate of transmission and seems to be able to evade immune protection better. Symptoms: sore throat, fatigue, fever, mild cough, muscle aches, nasal congestion, gastrointestinal symptoms - nausea, loss of appetite, stomach discomfort, and diarrhea.
Note: loss of taste and smell is not commonly reported for either new variant.
Vaccine/Booster/Protection: Current Covid vaccines are for previous variants KP.2/JN.1 and should still protect against severe disease with these variants. Vaccine immunity is strongest in the first 2 months with gradually declining protection for up to 6 months. The immune response from getting Covid declines more quickly than vaccination. The wait time for a booster after having Covid is 3 months.
Vaccines to match the new dominant variant(s) may be updated in the fall.
Covid-19 is airborne so ventilation, air filtration, avoiding exposure, and N-95 masks are good variant proof protections.
4 notes
·
View notes