#Alendronate
Text
I have a pt who saw orthopedics and had a DEXA scan done. She has osteoporosis. Recommendations: Fosamax x2 years in addition to conservative tx with adequate Ca2+ and vitamin D intake of 1200 mg qd and 2000 U qd respectively; weightbearing and resistance exercises; PT; repeat DEXA in 2024.
Fosamax = alendronate
1 note
·
View note
Text
Alendronate Drug
Medical information for Alendronate on Pediatric Oncall including Mechanism, Indication, Contraindications, Dosing, Adverse Effect, Interaction, Renal Dose, Hepatic Dose.
#Alendronate#medication#medications#medicine#drug#drugs#drug information#medical information#drug index#drug center#pediatric dose#Alendronic acid
0 notes
Text
A while ago @elavoria tagged me to create my OCs using this picrew but my wireless connection was rather shitty. Anyway, that's a problem of the past so here are:
Rashkan, sadly without his goatee, but overall surprisingly accurate:

Rethul, before he got his lip piercing:

And Alendron, my fancy fancy Fatebinder, actually looking fancy:

Tagging: @nostalgic-breton-girl @thequeenofthewinter @dirty-bosmer @skyrim-forever @friend-of-giants @rakaiawriter and @miraakulous-cloud-district
18 notes
·
View notes
Text
What would alendronate sodium look like as an anime girl ?
3 notes
·
View notes
Text
3 good things
Talked to a really funny patient today. I got to prescribe him alendronate! *O * well technically my preceptor did haha
It's almost the end of week 3, which means I'm halfway through this rotation
Randomly remembered something important OTL
#3 good things#personal#I feel like I'm good at writing messages to patients lately!#also most of them are super nice and respond >. <
2 notes
·
View notes
Link
Thuốc Alendronate có tác dụng điều trị bệnh loãng xương do mãn kinh, suy tuyến sinh dục và sử dụng steroid dài hạn. Thông thường thuốc này sẽ được chỉ định khi mất xương nghiêm trọng, bệnh nhân có nguy cơ cao bị gãy xương do loãng xương. Ngoài ra thuốc còn được sử dụng trong điều trị bệnh Paget về xương.
2 notes
·
View notes
Text
Fosamax (alendronate) is a prescription drug that’s used for osteoporosis and Paget’s disease. This drug can interact with other medications and some supplements. For example, Fosamax can interact with NSAIDs and certain antacids.
Fosamax is used in adults to:
prevent and treat osteoporosis in females* who have gone through menopause
increase bone mass in males* with osteoporosis
treat osteoporosis caused by treatment with a glucocorticoid medication
treat Paget’s disease of bone
An interaction can occur because one substance causes another substance to have a different effect than expected. Interactions can also occur if you have certain health conditions.
Keep reading to learn about Fosamax’s possible interactions. And for more information about Fosamax, including details about its uses, see this article.
* In this article, we use the terms “male” and “female” to refer to someone’s sex assigned at birth. For information about the difference between sex and gender, see this article.
Does Fosamax interact with other drugs?
Before you start taking Fosamax, tell your doctor and pharmacist about any prescription, over-the-counter, or other drugs you take. Sharing this information with them may help prevent possible interactions. (To learn whether Fosamax interacts with herbs or vitamins and supplements, see the “Are there other interactions with Fosamax?” section below.)
If you have questions about drug interactions that may affect you, talk with your doctor or pharmacist. They can answer additional questions you may have, such as what drugs should not be taken with Fosamax.
The table below lists drugs that may interact with Fosamax. Keep in mind that this table does not include all drugs that may interact with Fosamax. For more information about some of these interactions, see the “Drug interactions explained” section.
Drug group or drug nameDrug examplesWhat can happenantacids that contain calcium, magnesium, or aluminum• aluminum hydroxide/magnesium hydroxide/simethicone (Mylanta, others)
• calcium carbonate (Tums)can make Fosamax less effectivedeferasirox (Jadenu, Exjade)—can increase the risk for digestive side effects of Fosamax and deferasiroxnonsteroidal anti-inflammatory drugs (NSAIDs)• aspirin
• ibuprofen (Advil, Aleve)can increase the risk of digestive side effects of Fosamax and NSAIDsparathyroid hormone and analogs• teriparatide (Forteo)
• parathyroid hormone (Natpara)can make parathyroid hormone and parathyroid hormone analogs less effectivephosphate binders• lanthanum (Fosrenol)can make Fosamax less effectiveproton pump inhibitors (PPIs)• omeprazole (Prilosec)
• esomeprazole (Nexium)can make Fosamax less effectivesucralfate (Carafate)—can make Fosamax less effectivethyroid hormone replacements• liothyronine (Cytomel)
• levothyroxine (Synthroid, others)can make Fosamax less effective
When should I avoid Fosamax?
Certain health conditions or other factors could raise your risk of harm if you take Fosamax. In such cases, your doctor may not prescribe Fosamax for you. These are known as contraindications. The list below includes contraindications of Fosamax.
If you have a problem with your esophagus that delays emptying or are at higher risk for aspiration: Fosamax can cause side effects that affect your esophagus. Examples include esophageal ulcers, bleeding, perforation (holes), and stricture (narrowing). Doctors typically won’t prescribe Fosamax if you have an existing esophageal problem that delays emptying from the esophagus due to this risk. They’ll also usually avoid prescribing Fosamax if you’re at increased risk for aspiration.
If you have an inability to sit or stand up for at least 30 minutes: After taking each dose of Fosamax, you must remain seated or standing upright for at least 30 minutes. This lowers the risk of esophageal side effects caused by Fosamax. Your doctor will likely suggest treatments for osteoporosis other than Fosamax if you’re unable to remain seated or upright for at least 30 minutes.
If you have hypocalcemia: Usually, doctors won’t prescribe Fosamax if you have hypocalcemia (low blood calcium levels) until the condition is treated. Taking Fosamax can worsen hypocalcemia.
If you’ve had an allergic reaction: If you’ve had an allergic reaction to Fosamax or any of its ingredients, your doctor likely won’t prescribe Fosamax for you. This is because taking the drug could cause another allergic reaction. You can ask your doctor about other treatments that may be better options for you.
Before you start taking Fosamax, talk with your doctor if any of the factors above apply to you. Your doctor can determine whether Fosamax is safe for you to take.
Does Fosamax interact with alcohol?
Fosamax is not known to interact with alcohol. But your doctor may suggest limiting or avoiding alcohol to lower your risk for osteoporosis or to help prevent your osteoporosis from worsening. (Fosamax is prescribed to treat and prevent osteoporosis in certain people.)
If you have questions about consuming alcohol while using Fosamax, talk with your doctor or pharmacist.
Drug interactions explained
Learn more about certain drug interactions that can occur with Fosamax.
Interaction with antacids that contain calcium, magnesium, or aluminum
Fosamax can interact with antacids that contain calcium, magnesium, or aluminum. Antacids are used to treat heartburn.
Examples of antacids that contain calcium, magnesium, or aluminum include:
aluminum hydroxide/magnesium carbonate (Gaviscon)
calcium carbonate (Tums)
calcium carbonate/magnesium hydroxide (Rolaids, Mylanta)
aluminum hydroxide/magnesium hydroxide/simethicone (Mylanta, others)
What could happen
Taking Fosamax with an antacid that contains calcium, magnesium, or aluminum can prevent your body from absorbing Fosamax. This can make Fosamax less effective.
What you can do
If you take Fosamax with an antacid that contains calcium, magnesium, or aluminum, you’ll need to avoid taking these drugs at the same time. Take antacids that contain calcium, magnesium, or aluminum at least 30 minutes after you take your Fosamax dose.
If you have questions about taking Fosamax with an antacid that contains calcium, magnesium, or aluminum, talk with your doctor or pharmacist.
Interaction with nonsteroidal anti-inflammatory drugs (NSAIDs)
Fosamax can interact with NSAIDs. NSAIDs are used to treat acute pain. This includes pain related to arthritis, the common cold or flu, and period pain, among other aches and pains.
Examples of NSAID medications include:
aspirin
ibuprofen (Advil, Motrin)
naproxen (Naprosyn)
indomethacin (Indocin)
diclofenac (Catafam, Arthrotec)
What could happen
Both Fosamax and NSAIDs can cause digestive side effects, including ulcers in your gastrointestinal (GI) tract. Taking these medications can increase the risk of these side effects.
What you can do
Usually, this interaction is not severe enough to stop doctors from prescribing Fosamax and NSAIDs together. Often, doctors can monitor you for symptoms of digestive side effects during treatment.
If you have another medical condition that raises this risk, your doctor may be more cautious about prescribing Fosamax and an NSAID together. For example, if you have peptic ulcer disease or a history of bleeding in your GI tract, your doctor may suggest avoiding this treatment combination.
Talk with your doctor if you have questions about using Fosamax and NSAIDs together.
Interaction with phosphate binders
Fosamax can interact with phosphate binders. Phosphate binders are used to lower the amount of potassium in your system in people with kidney conditions, such as chronic kidney disease.
Examples of phosphate binder medications include:
lanthanum (Fosrenol)
calcium acetate
sucroferric oxyhydroxide (Velphoro)
What could happen
Taking Fosamax with a phosphate binder can block your body from absorbing Fosamax. This can make Fosamax less effective.
What you can do
If you need to take Fosamax and a phosphate binder, take the phosphate binder at least 2 hours after you take Fosamax. Separating the times when you take your dose can help prevent this interaction.
Are there other interactions with Fosamax?
Fosamax may have other interactions. They could occur with supplements, foods, vaccines, or even lab tests. See below for details. Note that the information below does not include all other possible interactions with Fosamax.
Does Fosamax interact with supplements?
Before you start using Fosamax, talk with your doctor and pharmacist about any herbs or vitamins and supplements you take. Sharing this information with them may help you avoid possible interactions.
It’s important to note that you should separate taking Fosamax and any herbs or vitamins and supplements you take, even if specific interactions are not discussed below. Fosamax should be taken first thing upon waking up, at least 30 minutes before taking any other medication or supplement.
If you have questions about interactions that may affect you, talk with your doctor or pharmacist.
Fosamax interactions with herbs
There are currently no reports of Fosamax interacting with specific herbs. But this doesn’t mean that interactions with herbs won’t be recognized in the future.
For this reason, it’s still important to check with your doctor or pharmacist before taking any of these products while taking Fosamax.
Fosamax interactions with vitamins and minerals
Fosamax can interact with the minerals calcium, magnesium, and iron. It can also interact with multivitamins that contain these minerals. You should wait at least 30 minutes after taking Fosamax before you take any product that contains calcium, magnesium, or iron.
Talk with your doctor or pharmacist if you have additional questions about Fosamax, vitamins, and minerals.
Does Fosamax interact with food?
There are no specific foods to avoid while taking Fosamax. But, it’s important to note that you should not eat food at least 30 minutes before or 30 minutes after taking Fosamax. If you take Fosamax with food, the interaction could decrease the level of the drug in your body. This may make Fosamax less effective.
Does Fosamax interact with vaccines?
There are currently no reports of Fosamax interacting with vaccines. If you have questions about getting certain vaccines during your Fosamax treatment, talk with your doctor.
Does Fosamax interact with lab tests?
There are currently no reports of Fosamax interacting with lab tests. If you have questions about having certain lab tests during your treatment with Fosamax, talk with the healthcare professional ordering the test.
Does Fosamax interact with cannabis or CBD?
There are currently no reports of Fosamax interacting with cannabis (commonly called marijuana) or cannabis products such as cannabidiol (CBD). But as with any drug or supplement, talk with your doctor before using cannabis with Fosamax.
Note: Cannabis is illegal at a federal level but is legal in many states to varying degrees.
Does my health history affect whether I should take Fosamax?
Certain medical conditions or other health factors may raise the risk of interactions with Fosamax. Before taking Fosamax, talk with your doctor about your health history. They’ll determine whether Fosamax is right for you.
Health conditions or other factors that might interact with Fosamax include:
If you have a problem with your esophagus that delays emptying or are at higher risk for aspiration. To learn more, see the “When should I avoid Fosamax?” section in this article.
If you have an inability to sit or stand up for at least 30 minutes. To learn more, see the “When should I avoid Fosamax?” section in this article.
If you have hypocalcemia. To learn more, see the “When should I avoid Fosamax?” section in this article.
Other problems with your esophagus or digestive tract. Fosamax can cause side effects that affect your esophagus and digestive tract.
If you have esophagitis or another condition involving your esophagus or digestive tract, taking Fosamax could worsen your condition. You may also have a higher chance of digestive side effects caused by Fosamax.
Low vitamin D level. If you have a low vitamin D level, your doctor will likely want to treat this before or during treatment with Fosamax. Having low vitamin D can negatively affect your bone health, including raising your risk for osteoporosis.
Dental condition or scheduled dental surgery. Fosamax can rarely cause dental-related side effects, including osteonecrosis of the jaw. Having dental surgery while taking Fosamax can increase this risk. You may also be at higher risk if you have a dental condition, such as gum disease.
Severe kidney problems. If you have a severe kidney problem, such as end stage kidney disease, your doctor may suggest a treatment other than Fosamax. Your body relies on your kidneys to get rid of Fosamax after you take a dose. Having a severe kidney problem can mean your body doesn’t get rid of Fosamax as well. This can cause an elevated level of Fosamax in your system, which may raise your risk for side effects.
Pregnancy. Doctors typically recommend stopping Fosamax during pregnancy. If you’re pregnant or planning a pregnancy, talk with your doctor before taking Fosamax.
Breastfeeding. It’s not known whether it’s safe to take Fosamax while breastfeeding. If you’re breastfeeding or planning to breastfeed, talk with your doctor about your options.
Allergic reaction. If you’ve had an allergic reaction to Fosamax or any of its ingredients, your doctor will likely not prescribe Fosamax. This is because using the drug could cause another allergic reaction. You can ask your doctor about other treatments that may be better choices for you.
Common questions about Fosamax and interactions
Find answers to some frequently asked questions about Fosamax and possible interactions.
What pain reliever can I take with Fosamax?
Fosamax can interact with nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen and aspirin. To learn more about this interaction, see the “Drug interactions explained” section in this article.
Other pain relievers, such as acetaminophen (Tylenol), may be safe for you to take, as they aren’t expected to interact with Fosamax. But, other pain relievers may interact with other medications you take. Or, they may interact with other medication conditions you have. For this reason, talk with your doctor or pharmacist to learn more about pain relievers that are safe for you to use.
Can I take Tylenol while taking Fosamax?
Yes, if your doctor says this is OK. Tylenol and Fosamax aren’t reported to interact.
That said, Tylenol can interact with other medications and medical conditions. Although it doesn’t interact with Fosamax, it’s best to ask your doctor or pharmacist if Tylenol is safe for you before taking it.
How can I prevent interactions?
Taking certain steps can help you avoid interactions with Fosamax. Before starting treatment, talk with your doctor and pharmacist. Things to discuss with them include:
whether you drink alcohol or use cannabis
other medications you take, as well as any vitamins, supplements, and herbs (they can also help you fill out a medication list)
what to do if you start taking a new drug during your Fosamax treatment
It’s also important to understand Fosamax’s label and other paperwork that may come with the drug. Colored stickers that describe interactions may be on the label. And the paperwork (sometimes called the patient package insert or medication guide) may have other details about interactions. (If you did not get paperwork with Fosamax, ask your pharmacist to print a copy for you.)
If you have trouble reading or understanding this information, your doctor or pharmacist can help.
Taking Fosamax exactly as prescribed can also help prevent interactions.
Disclaimer: adoctor has
made every effort to make certain that all information is factually correct, comprehensive, and up to date. However, this article should not be used as a substitute for the knowledge and expertise of a licensed healthcare professional. You should always consult your doctor or another healthcare professional before taking any medication. The drug information contained herein is subject to change and is not intended to cover all possible uses, directions, precautions, warnings, drug interactions, allergic reactions, or adverse effects. The absence of warnings or other information for a given drug does not indicate that the drug or drug combination is safe, effective, or appropriate for all patients or all specific uses.
Certainly! Below is a sample FAQ optimized for SEO and formatted with the content based on the hypothetical article about "Fosamax Interactions: Other Medications, Alcohol, and More."
```html
What is Fosamax used for?
Fosamax is primarily used to treat and prevent osteoporosis in postmenopausal women and increase bone mass in men with osteoporosis.
Can I take Fosamax with other medications?
Fosamax can interact with certain medications, including calcium supplements, antacids, and some anti-inflammatory drugs. It's important to consult your healthcare provider before combining it with other medications.
How does alcohol interact with Fosamax?
Consuming alcohol while taking Fosamax may increase the risk of stomach-related side effects and bone loss. It is advisable to limit alcohol intake while on Fosamax.
What should I avoid while taking Fosamax?
Avoid lying down for at least 30 minutes after taking Fosamax and avoid eating or drinking anything other than water during this period to ensure proper absorption.
Can I take Fosamax with food?
No, Fosamax should be taken on an empty stomach with a full glass of water to ensure that it is absorbed properly.
Are there any over-the-counter drugs I should avoid while on Fosamax?
Yes, avoid taking over-the-counter medications that contain calcium, magnesium, or aluminum within two hours of taking Fosamax as they can interfere with its absorption.
```
These FAQs are straightforward and designed to provide clear, concise answers that are easy to understand, which can also improve your search engine rankings by addressing common queries related to the medication Fosamax.
0 notes
Text
Modern Healthcare Advancements in Personalised Osteoporosis Treatment

Osteoporosis is a condition characterized by low bone mineral density and deterioration of bone tissue, leading to fragile bones that are more prone to fractures. Several factors can increase the risk of developing osteoporosis, including age, gender, heredity, lifestyle habits, and certain medical conditions. As people get older, bones gradually lose density and strength. Women are at higher risk after menopause due to decrease in estrogen levels. Genetic factors also play an important role - one's risk is higher if a parent or sibling has been diagnosed with osteoporosis. Lack of exercise and vitamin D and calcium deficiency further enhances the risk. Certain medical conditions like hyperthyroidism, rheumatoid arthritis, celiac disease, and gastrointestinal disorders can also contribute to bone loss over time.
Diagnosis and Assessment of Bone Health
Bone mineral density (BMD) tests are commonly used for diagnosing osteoporosis and monitoring treatment effectiveness. BMD tests employ dual-energy X-ray absorptiometry (DXA) technology to precisely measure bone density at various sites like the hip, spine, wrist, and shoulder. Based on BMD scores compared to average young adult peak bone mass, individuals are classified as having normal bone density, osteopenia (lower than normal bone density), or osteoporosis (density at least 2.5 standard deviations below normal). Fracture risk calculators considering factors like age, gender, weight, smoking status, family history, etc. also help physicians assess 10-year probability of fractures.
Lifestyle Modification for Stronger Bones
Making healthy lifestyle choices go a long way in managing osteoporosis and preventing fractures. Adequate weight-bearing and muscle-strengthening physical activities like walking, jogging, dancing at least 30 minutes per day stimulate bone formation. Calcium from dietary sources like dairy products, leafy greens, calcium-fortified foods, and calcium supplements is essential for maintaining strong bones. Vitamin D aids calcium absorption and keeping levels sufficient through sun exposure, foods, and supplements. Quitting smoking and limiting alcohol intake are other vital measures. Maintaining a healthy body weight also helps redistribute weight pressures on weight-bearing bones.
Pharmacological Options for Osteoporosis Treatment
Medications are often prescribed for individuals diagnosed with low bone mass or osteoporosis to inhibit further bone loss and reduce fracture risk. Bisphosphonates like alendronate and risedronate are first-line medications that work by inhibiting bone resorption. They are taken orally on a weekly or monthly schedule. Intravenous bisphosphonates like zoledronic acid are alternatives for those unable to take oral versions. Denosumab administered twice yearly as a subcutaneous injection is another anti-resorptive medication. Teriparatide, a biosynthetic form of parathyroid hormone, stimulates new bone formation and is a treatment option for severe osteoporosis. Selective estrogen receptor modulators (SERMs) like raloxifene may help for postmenopausal women. Calcitonin is also utilized as a nasal spray treatment for osteoporosis in certain cases. Close monitoring is important to ensure safety and effectiveness of long-term treatment.
0 notes
Text
Navigating Empty Stomach Medications: What You Need to Know
When it comes to taking medications, timing can be everything. Some medications work best when taken on an empty stomach, while others require food to be effective or to prevent stomach upset. Understanding when and how to take these medications can significantly impact their efficacy and your comfort. Let’s dive into the essentials of empty stomach medications to ensure you’re getting the most out of your treatment plan.
Why Empty Stomach Matters
Certain medications are designed to be absorbed into the bloodstream more efficiently when there's minimal food in the stomach. Food can interfere with the absorption process by affecting pH levels or interacting with the medication's chemical structure. Taking these medications on an empty stomach typically means either 1 hour before a meal or 2 hours after a meal, depending on the specific instructions provided.
Common Types of Empty Stomach Medications
Antibiotics: Many antibiotics, such as doxycycline and amoxicillin, are recommended to be taken on an empty stomach to ensure optimal absorption. This helps achieve adequate blood levels quickly, which is crucial for fighting infections effectively.
Thyroid Medications: Hormonal medications like levothyroxine, used to treat thyroid disorders, should ideally be taken on an empty stomach. This helps ensure consistent absorption and effectiveness.
Certain Osteoporosis Medications: Drugs like alendronate and ibandronate, used to treat osteoporosis, are often prescribed to be taken on an empty stomach with a full glass of water. This helps prevent irritation to the esophagus and ensures proper absorption.
Proton Pump Inhibitors (PPIs): Medications like omeprazole and lansoprazole, used to reduce stomach acid, are typically taken before breakfast to maximize their effect on reducing gastric acid production throughout the day.
Tips for Taking Empty Stomach Medications
Read Labels and Instructions Carefully: Always follow the specific instructions provided by your healthcare provider or pharmacist regarding when and how to take medications on an empty stomach.
Timing Matters: Pay attention to the recommended timing relative to meals. Some medications should be taken 1 hour before eating, while others require waiting 2 hours after eating.
Stay Consistent: Try to take your medication at the same time each day to maintain consistent blood levels and maximize effectiveness.
Consult Your Healthcare Provider
If you're unsure about whether a medication should be taken on an empty stomach or have any concerns about potential interactions or side effects, don't hesitate to consult your healthcare provider. They can provide personalized advice based on your medical history and specific needs.
Taking medications on an empty stomach is a simple yet important aspect of managing your health effectively. By understanding and following these guidelines, you can ensure that your medications work as intended, helping you achieve better health outcomes.
Remember, your health is worth the extra attention to detail when it comes to taking medications. Stay informed, stay consistent, and prioritize your well-being.
0 notes
Text
Osteoporosis Treatment Market Size: Growth Factors and Key Drivers

The Osteoporosis Treatment Market size was estimated at USD 13.28 billion in 2023 and is expected to reach USD 18.59 billion By 2031 at a CAGR of 4.3% during the forecast period of 2024-2031.The osteoporosis treatment market is witnessing significant growth, driven by the aging global population and increasing prevalence of the condition. Advances in pharmaceutical research have led to the development of innovative therapies, including bisphosphonates, selective estrogen receptor modulators (SERMs), and monoclonal antibodies like denosumab, which are enhancing patient outcomes. Additionally, the market is expanding with the integration of digital health technologies and personalized medicine approaches, offering tailored treatment plans that improve adherence and efficacy. Rising awareness campaigns and government initiatives aimed at early diagnosis and management of osteoporosis further bolster market dynamics, ensuring a robust pipeline of new treatments and supportive care strategies.
Get Sample of This Report @ https://www.snsinsider.com/sample-request/3337
Market Scope & Overview
Potential customers, sales and competitive environment studies, planned product releases, existing and novel technological advancements, revenue and trade regulatory evaluations, and more are all covered by the Osteoporosis Treatment Market research. The purpose of the study is to give participants a chance to comprehend the most recent trends, the state of the market, and market-related technology.
As per the market research there are new and quickly growing market segments, geographical areas, market drivers, challenges, and opportunities in the global Osteoporosis Treatment industry. The research report covers significant market strategies, long-term objectives, increasing market share, and product portfolios of top companies. Additionally, it helps venture capitalists make wise decisions by helping them comprehend organizations better.
Market Segmentation Analysis
By Drug Class
Calcitonin
Bisphosphonate
Zoledronic Acid
Ibandronate
Alendronate
Risedronate
Other
Hormone Replacement Therapy
RANK ligand (RANKL) Inhibitor
Parathyroid Hormone-Related Protein (PTHrP) Analog
Selective Estrogen Receptor Modulator (SERMs)
By Administration
Injectables
Oral
Others
By Distribution Channel
Online Pharmacies
Retail Pharmacies & Stores
Hospitals Pharmacies
Russia-Ukraine Conflict Impact on Osteoporosis Treatment Market
The market research demonstrates how the conflict between Russia and Ukraine has impacted markets around the globe. Additionally, it provides guidance to market participants on how to create practical solutions to lessen the negative effects of such contradictory circumstances.
Regional Outlook
The latest market study examines a wider range of topics and looks at the situations and events that are most likely to have a lasting impact. These elements, also referred to as market dynamics, include the pressures, constraints, choices, and issues that shape how those elements are viewed. The main geographical areas covered by the Osteoporosis Treatment Market research report are North America, Latin America, Asia Pacific, Europe, the Middle East, and Africa.
Competitive Analysis
The global market research report's section on competition analysis examines a few key players in the Osteoporosis Treatment Market. The research report also covers supply-chain analysis, market expansion strategies, a PEST analysis, a Porter's Five Forces analysis, and market-like scenarios.
Major Questions Answered in Osteoporosis Treatment Market Report
What production values, outputs, and capabilities can be anticipated for the global industry?
What entry strategy, cost-cutting measures, and distribution plans should the market have?
What impact has the conflict between Russia and Ukraine had on the target audience?
Conclusion
Understanding the information contained in the Osteoporosis Treatment Market research report is necessary in order to grasp the current state and potential futures of the industry.
About Us
SNS Insider is a market research and insights firm that has won several awards and earned a solid reputation for service and strategy. We are a strategic partner who can assist you in reframing issues and generating answers to the trickiest business difficulties. For greater consumer insight and client experiences, we leverage the power of experience and people.
When you employ our services, you will collaborate with qualified and experienced staff. We believe it is crucial to collaborate with our clients to ensure that each project is customized to meet their demands. Nobody knows your customers or community better than you do. Therefore, our team needs to ask the correct questions that appeal to your audience in order to collect the best information.
Related Reports
Diabetic Neuropathy Market Trends
Smart Contact Lenses Market Size Trends
Lymphoma Treatment Market Trends
Veterinary Vaccine Adjuvants Market Trends
Medical Electrodes Market Trends
0 notes
Text

Lifestyle measures – Lifestyle measures to reduce bone loss include adequate calcium and vitamin D intake, exercise, smoking cessation, fall prevention, and avoidance of heavy alcohol use. In general, women should achieve 1200 mg of elemental calcium daily (total diet plus supplement) and 800 international units of vitamin D daily. If dietary calcium intake is inadequate, we suggest calcium supplementation.
●Low bone mass (osteopenia) – In postmenopausal women with low bone mass and without fragility fracture, we calculate absolute fracture risk using the Fracture Risk Assessment Tool (FRAX). For most patients with low to moderate fracture risk, we suggest not using pharmacologic therapy to prevent bone loss or fracture. (See 'Our approach' above.)
●Patient selection for osteoporosis pharmacologic therapy
•For postmenopausal women with a diagnosis of osteoporosis based on bone mineral density (BMD; T-score ≤-2.5) or fragility fracture, we recommend treatment with pharmacotherapy (algorithm 1) (Grade 1A).
•For postmenopausal women with low BMD (T-score between -1.0 and -2.5) and high fracture risk, we also suggest pharmacologic therapy (Grade 2B). In the United States, a 10-year probability of hip fracture or combined major osteoporotic fracture of ≥3 or ≥20 percent, respectively, is a reasonable threshold for pharmacotherapy.
●Choice of initial therapy
•Most women with osteoporosis – For the initial treatment of osteoporosis in most postmenopausal women, we suggest oral bisphosphonates (algorithm 2) (Grade 2B). We prefer these agents based on efficacy, cost, and long-term safety data. Oral bisphosphonates are contraindicated in those with esophageal disorders (eg, esophageal stricture) or known malabsorption (eg, Roux-en-Y gastric bypass) (algorithm 2).
Algorithm 2:

25(OH)D: 25-hydroxyvitamin D; CKD: chronic kidney disease; eGFR: estimated glomerular filtration rate; GI: gastrointestinal.
* Refer to additional UpToDate content on evaluation of hypercalcemia and hypocalcemia.
¶ Very high risk of fracture: No consensus exists on the definition of very high fracture risk. Examples may include: T-score of ≤–3.0 even in the absence of fractures, T-score of ≤–2.5 plus a fragility fracture, severe or multiple vertebral fractures.
Δ Patients most likely to benefit from anabolic therapy are those with the highest risk of fracture (eg, T-score ≤–3.5 with fragility fracture[s], T-score ≤–4.0, recent major osteoporotic fracture, or multiple recent fractures).
◊ Increased risk of vertebral fracture is evident after discontinuation of denosumab; the need for indefinite administration of denosumab should be discussed with patients prior to its initiation.
§ Anabolic agents include teriparatide, abaloparatide, romosozumab.
¥ Oral bisphosphonates are poorly absorbed and must be taken on an empty stomach first thing in the morning with at least 240 mL (8 oz) of water. After administration, the patient should not have food, drink, medications, or supplements and should remain upright for at least 1 half-hour.‡ Denosumab is an alternative to intravenous zoledronic acid for women at high risk for fracture who have difficulty with the dosing requirements of oral bisphosphonates or who prefer to avoid intravenous bisphosphonates due to side effects. However, increased risk of vertebral fracture is evident after discontinuation of denosumab so the need for either indefinite treatment or transition to another osteoporosis medication should be addressed with patients before denosumab initiation.
We typically prefer alendronate as our choice of oral bisphosphonate due to efficacy in reducing vertebral and hip fracture and evidence showing residual fracture benefit after a five-year course of therapy is completed. Risedronate is a reasonable alternative.
•Very high fracture risk – For postmenopausal women with very high fracture risk (eg, T-score of ≤-2.5 plus a fragility fracture, T-score of ≤-3.0 in the absence of fragility fracture[s], history of severe or multiple fractures) (algorithm 1), we suggest initial treatment with an anabolic agent (Grade 2B). Patients most likely to benefit from anabolic therapy are those with the highest risk of fracture (eg, T-score ≤-3.5 with fragility fracture[s], T-score ≤-4.0, recent major osteoporotic fracture, or multiple recent fractures). Options for anabolic therapy include teriparatide, abaloparatide, or romosozumab. For patients with very high fracture risk who cannot be treated with an anabolic agent due to cost, inconvenience, contraindications, or personal preference, a bisphosphonate or denosumab may be appropriate (algorithm 2). Patients should be under the care of a provider with expertise in treating osteoporosis to facilitate shared decision-making.
●Contraindications to bisphosphonates
•Oral bisphosphonates contraindicated – Patients who cannot take oral bisphosphonates can be treated with an intravenous (IV) bisphosphonate instead (algorithm 2). Zoledronic acid is our agent of choice, as it is the only IV bisphosphonate with demonstrated efficacy for fracture prevention. Denosumab is a reasonable alternative. (See 'Gastrointestinal malabsorption or difficulty with dosing requirements' above.)
●Oral and IV bisphosphonates contraindicated
•Most women with osteoporosis – For most patients who cannot tolerate any bisphosphonate, we suggest denosumab rather than an anabolic agent (Grade 2C). Increased risk of vertebral fracture develops after discontinuation of denosumab, so the need for indefinite administration should be discussed with patients prior to denosumab initiation.
Anabolic agents may be used in patients with less severe osteoporosis when bisphosphonates are contraindicated. For patients with no history of fragility fracture(s), particularly those at high risk for breast cancer, raloxifene is a reasonable alternative.
•Very high fracture risk – For patients at very high risk of fracture (eg, T-score of ≤-2.5 plus a fragility fracture, T-score of ≤-3.0 in the absence of fragility fracture(s), history of severe or multiple fractures) who were not treated initially with anabolic therapy, we suggest switching to an anabolic agent (Grade 2C). Denosumab is an alternative. (See 'Contraindications or intolerance to any bisphosphonates' above and "Parathyroid hormone/parathyroid hormone-related protein analog therapy for osteoporosis", section on 'Overview of approach'.)
After initial therapy with an anabolic agent is discontinued, patients should be treated with an antiresorptive agent (typically a bisphosphonate) to preserve the gains in BMD from anabolic therapy. For individuals who are unable to tolerate oral or intravenous bisphosphonates, alternatives may include denosumab or raloxifene. (See "Parathyroid hormone/parathyroid hormone-related protein analog therapy for osteoporosis", section on 'Management after teriparatide' and "Parathyroid hormone/parathyroid hormone-related protein analog therapy for osteoporosis", section on 'Management after abaloparatide'.)
●Monitoring – For patients who initiate osteoporosis pharmacotherapy, we obtain a follow-up dual-energy x-ray absorptiometry (DXA) of the hip and spine after one to two years (algorithm 3). A change in BMD is considered significant only if it exceeds the least significant change (LSC) for the specific densitometer used. If LSC is not available, a threshold change of ≥5 percent has been suggested as an alternative. (See 'Our approach' above.)
•Bone mineral density stable or increased – If BMD is stable or improved, we continue therapy and remeasure BMD less frequently (eg, two to five years based on the clinical setting).
•Bone mineral density decreased or fracture during therapy – After at least one year of osteoporosis pharmacotherapy, a BMD decrease greater than the LSC or new fragility fracture should trigger additional evaluation, including assessment for treatment nonadherence or interim development of a secondary cause of bone loss (table 8). Whenever possible, patients should be under the care of a clinician with expertise in osteoporosis management.
If a remediable secondary cause of bone loss is identified, it should be treated. If the secondary cause of bone loss cannot be mitigated, or no secondary cause is identified, management depends on BMD and whether an interim fragility fracture occurred.
-Interim fragility fracture or T-score ≤-2.5 – For postmenopausal women who experience a fragility fracture or have a T-score ≤-2.5 on bisphosphonate therapy, we suggest discontinuing the bisphosphonate and switching to anabolic therapy (Grade 2C). Teriparatide and romosozumab increase BMD after previous bisphosphonate treatment. (See 'Interim fragility fracture or T-score ≤-2.5' above and 'Selection of anabolic agent' above.)
-BMD decreased but no interim fracture and T-score >-2.5 – In the absence of interim fragility fracture or T-score ≤-2.5, we use bone turnover markers and clinical assessments to evaluate the likelihood of treatment effectiveness. If treatment is unlikely effective, we stop the oral bisphosphonate and switch to IV zoledronic acid. If treatment is likely effective, we typically continue oral bisphosphonate therapy and remeasure BMD with DXA in one to two years. (See 'BMD decreased but no interim fracture and T-score >-2.5' above.)
2 notes
·
View notes
Text
Unveiling the Advantages of Fosamax Generic: Essential Insights You Must Check Out
In an intriguing post on Borderfree Health's blog, a new perspective has been provided on Fosamax Generic, a popular medication for bone conditions. It's filled with critical information that particularly resonates with patients grappling with Osteoporosis and Paget's disease, and is well worth the read.
A Closer Look at Fosamax Generic
Fosamax Generic, or Alendronate Sodium, aims to slow bone loss while improving bone mass. As the post explains, it ultimately helps prevent fractures. Fosamax Generic operates by altering bone formation and breakdown within the body. It's beneficial to anyone looking for a convenient alternative to traditional Fosamax, as it's just as effective.
The Advantages of Fosamax Generic
The more you delve into the blog post, the clearer the advantages of Fosamax Generic become. It's not just about the cost-effectiveness; the attraction extends to improved bone health, decreased risk of bone fractures, and reduced bone pain. These benefits make managing Osteoporosis and Paget's disease exponentially easier.
Making an Informed Decision
Patient education is crucial when it comes to medication like Fosamax Generic. This informative post illuminates potential side effects, offers dosing instructions, and guides on storage and disposal. Consequently, users are equipped to make an informed decision about their treatment plan.
MyFirstIdeas recommends this blog for the insight it provides, demystifying a complex subject and making it accessible to all.
0 notes
Text
Archon Alendron, especially after his duel with Rin, is often mistaken for a new archon of lightning. This affects the physical changes that appear the more belief he accumulates.
3 notes
·
View notes
Text
GETTING my TEETH into ITP and DENTAL TREATMENT
Before my purple journey started in 2006 a routine dental appointment would usually be completely straightforward, until then I had never really given much thought to what ITP sufferers should do in respect of such matters.
Would ITP make any difference to my dental treatment ? What should I tell my dentist about my illness, my medication, my current and future treatment ? Did he need to know ? Why did he need to know ? Could he treat me as a normal patient ? Could he treat me at all ?
For most people the merest hint of a dental appointment usually sets the collies wobbling. For some it's the buzzing of the drill, for others it's the smell of antiseptic or the taste of the mouth wash. Whatever turns us off, dental appointments are not much fun.
Luckily I have always had excellent treatment from my dentist. I can't say that a visit to my dentist has ever held any concerns at all. I guess I'm lucky in this respect. So a visit to my dentist as an ITP patient wouldn’t be any different, would it ?
Well, er, yes actually, it's very different. Just to make me slightly anxious I had heard that a number of ITP patients indicated that they had great difficulty in finding a dentist who had any idea what ITP actually was. Surely things were not this bad ? It was not Victorian England where some people had wooden false teeth and some did DIY dentistry with pliers and string tied to door handles. Hard times indeed.
The importance of getting regular dental checks is so important whether or not you have ITP but once under the purple influence it becomes even more vital. The phrase prevention rather than cure always comes to the fore when thinking about dental checks but with ITP it is absolutely imperative.
The last thing any of us with ITP needs is to have intrusive dental treatment, which is obviously going to be more difficult if we have a low or fluctuating platelet count. So by getting checked regularly and making sure we keep to good daily routines for oral hygiene, hopefully we can avoid treatment for things like fillings, gum disease and even extractions.
I knew that I had to tell my dentist that I had ITP. I had to advise him what treatment I had received, what drugs I had been taking , what my latest platelet count was and what treatment regime I was gong to continue with. I knew all this because I had obtained a really useful leaflet from the ITP Support Association. It was very soberly entitled... Protocol for dentists treating patients with Thrombocytopenia. A protocol sounded like something the UN would have drawn up. But nevertheless it was extremely helpful and I gave a copy to my dentist at my appointment.
At the dental appointment, as ever, my dentist made things as easy as proverbial pie. He is just very good at what he does. He's so professional, well informed, up to date with all the latest technology and information (He didn't even pay me to say any of that ! ) I told him that since we'd last met I'd been diagnosed with something called ITP. Just like everyone else I’d told about my ITP, I thought he'd say something along the lines of ...... Well you don't look ill, I've never heard of it but I'm sure you'll be fine.
What he actually said was that although he didn't have any other patients with ITP, he'd heard of it. He would treat me in a similar way to a haemophiliac, although he realised that there were many, many differences. He switched on his laptop and we looked up ITP. I'd given him my stodgily named Protocol for dentists leaflet already but he also looked up the ITP Support Association website there and then.
He took notes as I told him my purple history to date. He recorded details of my drugs...Prednisolone, Omeprazole, Alendronic Acid, Rituximab, Mycophenolate Mofetil, platelet count history, current treatment regime, name and contact details of my specialist and any other medical history of relevance.
I didn't have any other medical history apart from ITP so , that was pretty much that. Drama over, we just needed to do the dental bit. Just open wide, say cheese and hope for the best !
It may seem obvious that our dentist needs to know our platelet count. If any treatment is needed, especially an extraction, a platelet count under 50 may preclude that treatment from being carried out.
If you are going to have any treatment it is sometimes necessary to get a blood test to check your platelet count before undergoing that treatment and with some people it may also be necessary to consult with your ITP specialist/haematologist.
Advising our dentists of what medication we are currently taking and have taken for the last 12 months is also vital. Any drugs the dentist uses to anaesthetise us for example, may clash with any medications we have taken for our ITP or any other medical condition for that matter.
Another problem is that should we encounter any pain following any dental interventions the only painkillers we can take are Paracetamol. ITP sufferers must avoid Aspirin or Ibuprofen. Having purple in your life gives you so many things to think about.
For further information on all things ITP the following links are to the most reliable and up to date sources -
The ITP Support Association - www.itpsupport.org.uk
The Platelet Disorder Support Association - https://www.pdsa.org
ITP Australia - https://itpaustralia.org.au/
0 notes
Text
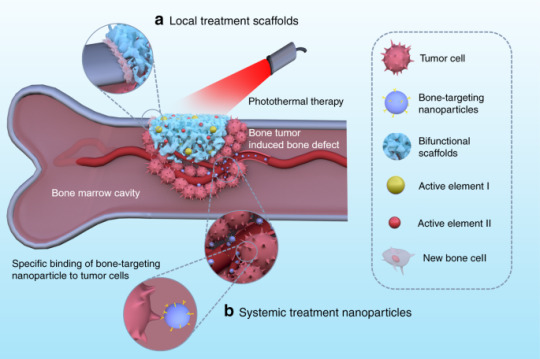
Bone-modifying drugs
Prostate cancer patients face a significant problem with their bone health. Hormonal therapy can either cause or exacerbate bone conditions like osteoporosis and osteoopenia. The risk of fractures should be assessed for prostate cancer patients receiving ADT for non-metastatic disease. The most widely recognized method for finding an individual’s gamble is with a double energy X-beam absorptiometry (DEXA) sweep to quantify the strength of the bones. Treatment should be given to those who are found to be at a high risk for a fracture. Bone-changing medications that can be utilized in this present circumstance incorporate denosumab (Prolia, Xgeva), zoledronic corrosive (Reclast, Zometa), alendronate (Fosamax), risedronate (Actonel), ibandronate (Boniva), and pamidronate (Aredia). Talk to your doctor about when to take these medications and which is best for you based on your situation because they can have side effects.
In patients who do not currently have evidence of bone metastases, it has not been demonstrated that bone-modifying medications can stop the spread of prostate cancer to the bone.
Patients with prostate cancer that has spread to the bone always run the risk of developing bone issues like fracture, pain, and compression of the spinal cord. These are known as “events related to the skeleton.” At the point when prostate disease has spread to bone and has additionally become impervious to ADT (see “Metastatic maiming safe prostate malignant growth” underneath), bone-adjusting medications might be prescribed to decrease the gamble of these issues. In particular, denosumab or zoledronic corrosive can be given once each month to decrease that gamble.
Dr. Amit Ghosh is one of the best urologist and robotics uro-surgeon in Kolkata. After his return from the UK, he has been associated with various institutions including Wockhardt Hospital and Kidney Institute, Woodlands Hospital, Kothari Medical Center and Anandalok Hospital. Currently he is dedicated to his service to Apollo Gleneagles Hospitals, Kolkata. Currently he has developed a very well established and robust Urological presence in the campus of Apollo Gleneagles Hospitals, Kolkata. The practice takes care of all fundamental general Urological procedures, a vast multi-disciplinary Uro Oncology specialty, and also a comprehensive diagnostic and uro health check-up facility.
0 notes
Text
Alendronate induces skeletal alterations in the chicken embryonic development model
http://dlvr.it/SvT7Nx
0 notes
Last Seen Blogs

ezebreze
いいや

startheskelaton
LetsGetSpooky.inc

lucanidear
lulu ☆

dagmaracielecka-blog
Dagmara's Art

sugardaddy1993
Untitled