#AND my house diagnostics spreadsheet
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
130K people were victims of a chain letter scam that affected Tumblr in May 2011.
Text
if i don’t have someone shaming/pressuring me into finishing something, i will never finish
#this is currently specifically about both my pathfinder wrath of the righteous playthrough#(currently 102 hours (playthrough number 1(!!!!!!)))#AND my house diagnostics spreadsheet#(currently begininning of season 2 AND realising i am going to have to personally redefine disorder categories)#why can i not just do things normally#(is there a way to make a spreadheet non neurodivergently?)#(yes i guess i do it at work every day.................)
7 notes
·
View notes
Note
The great hormonal storms in book 5 lead me to this ask: let's talk about sex. Or at least sex ed. Does Hogwarts have it (at least in LH'verse)? Is that a nurse duty or a Head of House one? Did Narcissa sit her baby boy down for The Talk, at least to impart how Miss Granger would return to her parents in the same state she left them or at least unimpregnated? Did she outsource that task to Uncle Severus? Did Ron share what his older brothers passed down? What does our favorite victorian-in-spirit know abt sex beyond "lie back and think of the bloodline" and his hormonal daydreams?
I'm l o s i n g it at the idea of Narcissa instructing Draco to leave Hermione "unimpregnated," which, I just — I think the minute she uses those things in the same sentence, Draco hits the road at the speed of Mach Christ. He's gone. He's not here. He's not in the building. Can't have the Sex Talk if you can't fucking catch me, Mom. (For the record, I can fully see Narcissa trying. She's much less prudish than Draco is — gossips about adultery with her 11-y/o son on Christmas morning, references Ye Olde Wilde Times with Lucius, cracks the occasional bawdy joke, etc. — she just doesn't often see the need to discuss it, being aware that Draco, as far as she knows, remains an un-Awakened little Victorian. The Great Granger Debacle of 1995 is likely raising her suspicions there.) That said, Draco knows what sex is; for some reason my mind gravitates to the slightly handwavey answer of "boy's dormitory." I'm picturing him in his four-poster, curtains drawn, pretending to be asleep, while Ron and Harry have a free-ranging, horrifically creative conversation about what Ron thinks sex is (courtesy of the twins). Optimistically, Neville hops in with corrections from Augusta Longbottom's sexual etiquette seminars. Either way, Draco never, ever reveals that he has heard this conversation.
Or, alternatively, he and Theo have a really intense heart-to-heart during that summer before third year, which would do a lot to explain why the two of them are so weird about each other basically for the rest of time. (Raising the question of where Theo/Pansy/Daphne learned it. At age 12, Pansy got an excruciatingly detailed Talk from her mother, who was scared to death of a teen pregnancy pitching their family into ruin; Pansy, deciding it was unfair she had to suffer this and Theo did not, inflicted said Talk on Theo, who was just relieved that he didn't have to ask Sibelius. And Daphne grew up around so many healers that she just badgered them until someone gave in and told her. She's also a stated connoisseur of trashy romance novels, so. Make of that what you will.)
I think that Hogwarts, being modeled in mores and general Vibe from old English boarding schools, probably is not the most forward-thinking with sex ed. I also do believe Severus Snape would sooner jump off a bridge, and I kind of need him for the plot, so I've got to spare him that grave and important duty. Poppy Pomfrey probably gets the question the most of any staff member, and over the years, I think she's honed her answer down to a tight 3 minute-monologue that covers all major topics.
Odds and ends in the same vein:
Hermione gets a sit-down with the Drs. Granger the summer before her thirteenth birthday, so sometime in August, 1992. It is meticulously explained and flawlessly presented, with color-coded diagrams, an index, and a syllabus. It includes a diagnostic chart for common STIs and a spreadsheet on birth control options. Dr. Granger gets excited after a tangent about ovarian cysts and runs to pull out her old copy of Grey's. Hermione spends the whole time fully miserable, wondering why parents couldn't be like, greengrocers or something. (That doesn't stop her from asking questions, obviously.)
Ron, like all Weasley men of his generation, gets a knock on his door sometime around his 14th birthday, and Arthur invites him to "go fishing." This is code for "stand by the river and try to keep a will to live while your dad explains the mechanics of sex, its importance, and the value of waiting until you feel comfortable and safe sharing that level of intimacy with a trusted partner" (sic).
Fred and George got separate talks, because Arthur wanted to emphasize that he sees them as individuals; however, Fred ran back and immediately recounted it all to George, who proceeded to feign extraordinary expertise in it the next morning, to his father's horror.
Ginny's "go fishing" equivalent is Molly taking her out for tea and delivering a well-meant but incoherent combination of abstinence-only sex ed, aggressive body positivity, and highly technical discussions of how to insert a diaphragm. Ginny, who bullied the real story out of Bill years ago, is baffled, and to this day can't say for sure what she was supposed to take away from it.
Harry spends his 14th birthday at the Burrow. Ron and his brothers make a blood pact in advance not to tell him about it, though, so when Arthur invites him out for the day on August 1st, his sole thought is: oh, nice! Can't wait for some fun fishing :)
84 notes
·
View notes
Text
What Happens when the Stars Go Out by TheJesseClark
The red lights are only making the pain worse. It is an immense, earth-shattering pain, in my midsection and in my head. I try to move, but I can't; I try to speak, but I can't do that either. It hurts too much, and my voice obeys me no more than do my joints or my muscles or my bones or my mind.
And yet still there is movement. I can feel myself being lifted up and placed on something - a bed, maybe, or - no.
A gurney.
“Alright!” one of the EMTs says, and several others then roll me into the back of an ambulance, and climb in behind me. But I'm already fading fast, and feeling an inexplicable heat, by the time those doors are shut.
One EMT, a blonde woman, looks at me with a furrowed brow, just as I'm slipping away, and says aloud, “Wait. Wait, I think I know...
”...we're made of that stuff, right?”
I turned around. There was a woman there, red-haired and about my age, give or take, and she was alarmingly beautiful. But how long she'd been staring at the exhibit alongside me I had no idea.
”I'm sorry?”
”I said ‘you know we're made of that stuff, right’?” She nodded at the museum wall, which depicted in detail the births and life cycle and deaths of stars. I pursed my lips.
”We’re… made of stars?”
”Yep. Isn't it awesome?” She stepped up beside me and moved her arm across the diagram as she spoke. “I just watched a documentary about it last night. Stars are just fusion factories held together by their own gravity. They start off fusing hydrogen to helium, and then they keep going on and on, fusing heavier and heavier elements until they're fusing the heaviest stuff. Then they exhaust their fuel and collapse under their own weight, and they blow off their outer layers and pretty much shower the galaxy with all these random elements, some of which are eventually used to create life.”
”Huh.”
”Yeah. I’m Robin, by the way.” She extended her hand, and I shook it.
”Uh, hey. Brian. Nice to meet you.” There was an awkward pause before I said, “Alright, I got one for you. If you replaced the sun with a black hole, what would happen?”
”Depends on its mass.”
”Nope! The answer is - drumroll please - nothing. I mean everything would get dark and cold, but we wouldn't fall in. Earth’s orbit would remain entirely unaffected.”
”IF the black hole had the same mass as the sun.”
”What?”
”What you said would only be true if the black hole in question happened to have the same mass as the sun. Which it wouldn't, because the sun isn't massive enough to collapse into a black hole.”
”Oh. Damn.”
”Yep. Me one, you zero. Sorry, pal.”
”Alright.” I said. “You're on. Whoever gets the most points by closing time buys drinks.”
She smiled at that and punched me in the shoulder, just light enough not to sting. ”Alright, loser. Come...”
“...on,” the EMT says. There is a flurry of activity around me, and there are voices, too, and blinding lights, and a cooling down of that monstrous heat.
One of the paramedics is looking me over. Then he looks to another colleague - the blonde woman - and he shakes his head, slowly.
“This one’s gone, Rachel.”
But she continues running tests, running diagnostics, placing a soft hand on my arm in case I'm awake enough to appreciate the comfort. I am. Barely. But I'm fading fast, and that heat is coming right on back as I do.
“Not yet he's not,” she says. There's pain in her voice that she does her fruitless best to conceal. “I already lost one earlier, Todd. I'm not losing…”
”... another one!” Robin said, and I laughed and agreed and we rushed to the back of the line.
”See? Told you you'd like Ferris Wheels. Can't believe you've never been on one before today.”
She shrugged. “Never thought they were as extreme as roller coasters, so I wasn’t interested.”
”Well they’re not supposed to be ‘extreme.’ Ferris Wheels are for all the parents waiting on their kids and sick people trying to relax their stomachs so they don’t puke funnel cake all over the pavement.”
”And adorable young couples, apparently.”
And just then we were waved into the next seat. We sat ourselves down, and moments later the great wheel began to groan and protest and, finally, to turn; it dragged our cart around its underside and then lifted it up, up, up to the top of its crest, where we could see the whole city at twilight, and the ships in the harbor that were backlit red with the setting sun, and the clouds that were lined at their tops with just a little bit of starlight. Robin snuggled up next to me and put her head on my shoulder, and I put my arm around her waist. For a moment then I could've sworn the empty seat in front of us move on its own, and furrowed my brow. But then Robin spoke.
”Thank you for being here with me,” she said. I didn't respond with words;I just kissed her on the head and held her tight, as the Wheel began taking us…
“...down on the eighteen hundred block of Gardersdale,” one of the EMTs says. “Yeah. Yeah. Another one, I know. Hell of a fucking night, isn't it?”
The conversation is muffled again in short order. I drift in and out, and there is a flurry of sound and lights and movement. But the jostling of the room and the sound of an engine tell me we're still in the ambulance.
The other paramedics, for their part, continue running tests and checking my vitals, and as they work I try to remember what's happened. But it hurts. Dammit, does it hurt, almost as much as that rushing heat, and the effort is further disrupted when the ambulance hits a bump in the road and I nearly spill out of the gurney. But Rachel puts her steadying hand on my chest and says, “Hang in there, Brian. We're almost…”
”...there!” Robin pointed at the interstate ramp, and I took the turn and put St. Thomas Vineyard away in the rearview.
”Still can't believe Mason got married,” I said. “He’s only known that girl for what, a year? Less?”
Robin shrugged. “They were in love.”
”They hardly knew each other! They don't know if whatever they're feeling is genuine, life-long love or just new relationship googley-eyes that hasn't worn off yet. I guarantee it - and I'll put money on this - they'll be done within a year. Just watch.”
”You don't know that,” she said. There was a brief pause, and then she added, “We’ve been dating for two years.”
”So?”
”So… how far off do you think we are?”
I shrugged. “I don't know. Haven’t really thought about it.”
”You haven't thought about it? At all?”
”I mean of course I've thought about it. I just… I don't know if we're ready, you know?” I looked over at her, but she just stared out there at the rain with her chin in her palm. So I continued. “Think about it like this: people prepare their whole lives for jobs, right? They start going to school as soon as they can talk, and they're not done till they're in their twenties, and it's all so they can get a piece of paper that says ‘hey, hire my ass, I’m smart enough to work.’ But marriage? Nobody trains for that shit. People just hook up and say, ‘hey we're twenty five, or twenty eight, you're cute, I'm cute. Let's spend fifteen thousand dollars on a giant ceremony and then live as glorified roommates for five years until we're both fat and hate each other and get divorced because neither one of us knew or cared how much work this thing would require.”
There was a longer pause then, before she said, with a degree of seriousness I wasn’t in the least bit prepared for, “Is that where you think we're headed? ‘Glorified roommates?’”
Quickly I calculated an avenue of retreat. But I calculated wrong. “No! Not you,” I said. “Not us. I mean most people, you know? Most people just dive in and either get divorced or stick it out till someone gets heart disease. The divorce rate is more than fifty percent now in the US. But the ‘I-don't-love-you-anymore’ rate? Shit, that's probably close to ninety by the time everyone hits middle age. I just want to make sure you're the right person, you know?”
If ever there were words I wish I could've taken back, it were those twelve. She said nothing, but I saw her reflection in the window, and the little tear that welled up in the corner of her eye said more than words ever could.
”Listen, I… that came out wrong. I just meant-”
”Can you drop me off at my car, please?”
”I thought you wanted to come over-?”
”I don't feel good. Please?”
And we drove in silence for a while, as the rain picked up its pace and fell in sheets and in torrents. After another twenty minutes I made the turn onto my street and parked, and once I did she got out without so much as a glance and walked across the road to her own car. I ran to follow.
”Robin, wait!” I grabbed her lightly by the arm. It was slick with rainwater. “Talk to me. Please?”
”What do you want?”
I blinked. ”I want you to talk to me. I just s-”
”No. I mean with us. Where do you want this to go?”
”Where do I want this to go? I want to be with you! Listen, I didn't mean to imply that - that I don't want that. I just want us to be smart about it. You know?”
”Well maybe love isn't something you can calculate on a fucking spreadsheet, Brian!” She was shouting over the cacophony of the storm. “Maybe it's just this thing you feel, you know? And maybe it doesn't make any damn logical sense. Maybe it's not supposed to. But that's part of what makes it special; it's an adventure; it's a ‘jump off a cliff with me’ type of thing. And yeah, sure. Not everyone survives the fall, I guess. But if you find the right person, then-”
”A ‘jump off the cliff with me’ type of adventure? Come on, Robin! We're not writing up a damn dating website profile here; this is real life! There are kids involved, and finances, and house buying, and mortgages and all that shit! Not every day is some cute little romance comedy. This is half your life we're talking about. Two-thirds, even. Okay? All I meant was that you have to be prepared for it. I just-”
”I thought we were prepared.”
”What do you mean?”
She dug through her purse for a moment, and then held up a ring that was brilliant even when covered in the rain. I felt my heart skip at least a full beat.
”Is that, um-”
”It was my mom’s,” she said. “She gave it to me before she died. She said, ‘find your partner in crime, Robin. Find someone who'll sweep you off your feet. And jump off a cliff with you.’” There was a pause before she added, “And at the time she said it I thought I knew exactly who that person was.”
I tried for a moment, but I knew, beyond the shadow of a doubt, that there was no combination of words in the English language that could be strung together to right this ship.
”Good-bye, Brian.” She kissed me on the cheek, and rubbed the back of her hand on down it. And then she turned and got in her Civic, and drove off until I couldn't see her tail-lights at all through the pouring of the...
“...rain’s comin’ down hard, boys,” another of the EMTs said. “Careful when you unload him.”
There were grunts of acknowledgement, and then the back of the ambulance flew open and the sound of the storm utterly exploded into it; I felt the rush of wind, and the rain pelting my skin in sheets, and together they helped a bit with the oncoming heat that still I couldn't place. And then I felt movement. The gurney dipped and hit pavement while the paramedics held me tight to its form. And then there were shouts, and lights, and running feet, and then the hospital door…
”Open?!” I shouted. The man behind the counter looked at me with a furrowed brow. I shouted it again, over the sound of rainfall and through the glass. “I said, are you open?!”
And then he pointed at the sign saying the opposite, and went back to reading. But I wasn't taking no for an answer; I dug out my wallet and pulled a twenty from the fold, and slapped it flat up against the glass. Within seconds the paper was soaked with rainwater. But it got his attention, and once he saw me there he took pity on my plight, and the door clicked and whirred and slid open.
”Make it quick, man.”
”I know, I know. I will. Thank you so much.” I ran down the aisles and then, true to my word, made it back to the counter in less than a minute. The man put down his book, and processed the sale.
”Date night?” He said, bagging the card after the flowers. I smiled a bit.
”Something like that.” And then I thanked him and ran back out to my car, and got inside, and took out the card and scribbled on its inner sleeve the words, ‘Jump off a cliff…
“...with me, with me!” A doctor running alongside the cart motioned to some nurses in the hall, and they ran to follow. He turns to the EMTs. “Is he stable?”
“He’s slipping. Heart rate’s falling, breathing slowing. Not good. Mumbled something about being too hot earlier, but if anything his temperature’s too low.” Someone shows the doctor a chart. He reads it as he runs, and his face is grim.
“Shit. Alright,” he says. “Let's…”
”...move!” I shout at the car I'm passing. “Just a little rain, assholes.” But it wasn't. It was a lot of rain. Sheets and buckets and torrents of it, in fact; it’d long since turned the dirt to mud, and it swept up against my windshield like ocean surf, and the road was slick with little rivers of it than ran on down past the pebbles. I was going far, far too fast for such conditions. But I didn't…*
“...care about that,” the doctor said. “I just want to get his fluids up. Rachel!”
The woman from the ambulance runs up and discusses my condition in harsh whispers with the doctor. As I fade, and as the damn heat floods on back in, it becomes impossible to hear what they're saying. But it's abundantly clear from the body language that she hasn't yet give up…
’...hope for a reunion with these guys?’
’Well, Bolan and Snake say they’re against it, entirely. So that doesn't bode well for fans. But look what happened with-’
I switched the radio off, and then wrapped both hands around the wheel with such force the knuckles turned white on the grip. The car hit seventy miles per hour. Seventy five. Seventy nine. The windshield wipers were flying, but they weren't going fast en-
”FUCK!” I slammed my foot on the brakes as the lights of activity in the road came in out of nowhere from the rain. The car jolted and shuddered and fought for traction with the pavement, and I felt the tires squeal and the metal of the car grind in…
“...protest.”
“I don't care if he wants to protest!” the doctor snaps back. “You tell him to wait in the damn lobby like everyone else!”
The nurse accepts her orders and heads back out into the hallway. “I'm sorry, sir,” she says. “You can't see him until-”
“Until what?! That's my son in there! That's my son! That's-” and then there's a scuffle of feet, and more shouts as a security guard drags my father from the wing. Rachel pauses as she hears the shouts, and then her eyes well up a bit with tears, and she looks at my face and appears to realize something. But she doesn't say what. The shouts continue, but they fade. And so do I. And in comes the heat as I do.
“That's my son!” Dad says. “That's my boy! Let me see my boy! Stop! Please...!”
”...stop!” The police officer had both hands up as my car barreled towards him. “Stop! Stop the car!”
Finally there was a jolt and a shudder as the tires gained control at last, and the car slammed to a halt. Both the officer and I sighed in relief, and then he approached my window and tapped the glass with his knuckle. I lowered it.
I shouted over the rain, “I'm sorry, sir! Roads are crazy out here. You okay?”
He ignored the question. “I'm gonna need you to sit here for a bit, okay?” He said. “Just until the accident’s cleared up.”
”Accident?”
”Its bad.” He nodded in the direction of the wreckage, and then he said again, “Just sit tight! We’ll waive you over when there's an open lane.” And then he ran off into the storm.
I scanned the scene. There was a man on the side of the road, I saw, sitting on the pavement with a poncho for the rainfall and his head in his hands. His SUV was totaled; the front end was bent and twisted and hideously mangled.
But the other car was in far, far worse shape than that. I squinted hard, and could only make out panels of white amidst charred black chunks of metal and the force of the rain. But it was enough.
It was a Civic.
Oh, God. Oh, God, no. No, no, no.
I got out of the car and left the door hanging open in the rain, and then I ran forward, at least until the officer caught sight of me and ran back over and grabbed me by the shoulders.
”Hey!” He said. “I told you to wait in the car! What're you-”
”ROBIN!!” I shouted over him. “ROBIN!”
And then I saw it; a fleeting glimpse of movement, a white sheet flipped on a gurney. A strand of red hair fell from the right side and hung there as the EMTs carted away the body.
”ROBIN!” I screamed. “That's my girl! That's my girl!” The officer was confused and stunned and did the only thing he could think to do - drag me back to my car.
”No! Stop!” I was inconsolable but in no shape at all to resist. “Stop, please! That's my girl! Let me see my girl! Please, stop!”
One of the EMTs, covered in blood from the waist up, turned to look at the spectacle. But then someone shouted her name.
“Rachel!” The doctor says. “You with us, or what? Let's go!”
She blinks as she stares at me, and then says, “Uh, yeah. Sorry. I just realized, this guy was-”
“Just get the charcoal, please? We don't have time.”
And she does; she runs off to fetch exactly that. And then I feel a hideously invasive sensation - a tube is being placed in my nose, and then I feel it falling down, into my throat. I'm too weak to gag, but I somehow manage to clench my fist. A nurse sees the movement, and he holds me down to steady me.
“Whoa, whoa…”
”...Whoa, whoa, you okay, man? My roommate stumbled back as I threw open the door. I charged past him. “You're comin’ in hot!” He said again. “You good, bro?”*
But I ignored him. I went to the bathroom, and I leaned up against the sink for a long moment, and I grabbed my temples and set my jaw and sobbed without a sound; aching, wracking, heaving sobs. I heard a knock.
”Hey, man,” he said. “You good, dude? Anything I can like, get for you? Or-?”
”I'm fine,” I managed. It wasn't convincing in the slightest, but I didn't care. I opened up my phone. There was a text from Robin there, from this morning.
*It read, ‘I love you,’ and they were all at once the most beautiful and the most painful words I'd ever read. ‘I love you.’
I love you, too. I'm coming. Hang on, baby. I'm coming.
Then I backed out, and found my dad in the contacts list, and typed, ‘I love you, Dad.’
Moments later I got a response: ‘I love you too, son! You okay?’
But I ignored it, and then I threw open the cupboard, and I grabbed an old…
“...bottle of pills,” a nurse said. “Swallowed the whole damn thing. Lucky his roommate called it in when he did.”
But the doctor is incredulous. “Well. That remains to be seen, now, doesn't it?” Then he turns to the door. “Rach-”
And she pushes it open with her elbow before he finishes. “I got it, I got it. I'm here.”
“Alright!” He says. “Fingers crossed, people. Let's see if we can't save a psycho!”
There are isolated chuckles. Rachel, though, almost snaps at her superior for the insult, but then someone says, “Here we go!”
And then there is thick, wretched black stuff funneling down that tube and down into my throat. I'm almost desperate enough, but not quite strong enough, to resist it. I can feel it sliding, and hitting bottom, and pumping, and pulsing. My heart rate is erratic; my breathing is erratic; my ability to comprehend the situation is every bit as erratic. I struggle as much as I can against the restraints, but all my effort and all my strength of arms musters up not more than the faintest whimper.
But Rachel hears it. She moves to my side, and she holds my head, and says, in soft enough a whisper that only I can hear the words, “Don't follow her, Brian. Don't follow her. Please, Jesus. I need him here. I need this win.”
But I begin to fade all the same. One by one, as the spikes on the EKG slow to sporadic pulses, I see the nurses turn to each other and shake their heads. One by one by one, that is, until there is only a trembling Rachel there, and she's holding on for me tight enough for everyone in the room.
“Call it,” the doctor says, just as the darkness swirls in and I feel like I’m starting to fall away.
The conversation carries on as I pass.
“Two thirty two AM,” one nurse says.
But I can hear Rachel screaming in protest - “No! He's not gone! There's still time, there's still time to save him, there's still…”
But she's wrong. I'm already gone. Her voice, and her face - those things are behind me as I pass. They're fading away into the darkness that's consuming me, and swallowing me whole, and throwing me to the winds.
And just when the magnitude of the situation dawns on me - then comes the heat. There are monstrous amounts of it. It rips and tears and scorches and scalds, and had I the ability to scream out or even to breathe I would've done so until my throat was hoarse. But then there is a new pain. A different pain.
A hand reaches out of the blackness, and it grabs my left-side forearm with such mighty force that the resulting pain eclipses that of the heat, and the nails of that hand rip right through the flesh. And then I’m being pulled, and there is a rushing wind. It is cool and refreshing and beautiful, and suddenly I'm somewhere else entirely.
I blinked. The darkness was gone, and the heat with it, and that sensation of being devoured. Instead, those things had been replaced with starlit clouds as far off in every direction as the eye could see. But my arm stung like hell all the same. I looked at it. There were nail-marks, I saw. Four deep cuts beneath the inner wrist and a fifth on the side, in the shape of a hand. They bled a bit. And then I heard an all too familiar voice.
“You okay?”
I stood up, slowly, and I turned, holding my damned stinging arm while I did it, and said, “Robin. Robin, w-what was that? That darkness? And the heat, and th-”
“Its where you would’ve spent your eternity, Brian, had I not pulled you out.”
I had no words other than the weakest, “Thanks.”
“You know,” she said, holding her own arm. “Suicide’s not exactly what I meant by ‘jumping off a cliff.”
I blinked again, and took a long, deep breath. “Yeah. I guess I didn’t think things through.”
“Not sure you fully realize how much of an understatement that is.”
“Well, maybe I don’t. But you know what? I'd do it again, Robin. I’m serious.”
She nearly rolled her eyes, but I doubled down on the sentiment.
“What I said? Out there on my street? I'm sorry. I mean it, I’m sorry. You were right. Love isn't about taxes or headaches or just tolerating each other until we’re seventy. It's like your mom said. It's about sweeping your girl off her feet. It's about jumping over cliffs with someone, and not knowing where you'll land, and not caring, as long as you get there together. And if this is where we land, wherever this is, I'm okay with that.” And I leaned in for a kiss.
But she stopped me with her hand before it landed, and I opened my eyes.
“I can tell you've been working on that speech for a while,” she said.
“Over and over again In my head, in the car, until… until I got to the scene of the wreck.” I looked at the ground, and then back up at her. “And I realized, right then, that if you fucking left the earth itself than I would, too. So here I a-”
“I was wrong, too.” She cut me off.
“W-what do you mean?”
“About love. I was wrong. My mother was wrong. It's not just about crap you see in rom-coms and greeting-cards, Brian.”
Again I blinked. “I know that! I know, it's - it's something you feel in your heart; that defies logic and reason. Not something you can put on a spreadsheet. Like you said earlier.”
She sighed a bit, and then said, “Can I show you something?”
“Uh, yeah! Yeah, okay. Sure.”
And then she took my hand, and Infinity rolled in and faded back out, and all of a sudden we were somewhere else entirely.
“Are we -?”
“On the Ferris Wheel? Yep. Turn around.”
I did, and there we were, past Robin and past me, on the seat above and behind us. I remembered it like yesterday; we were staring out at the whole city at twilight, and the ships in the harbor that were backlit red with the setting sun, and the clouds that were lined at their tops with just a little bit of starlight.
I rustled in my seat a bit and it moved, and past Me furrowed his brow when he saw it. But then past Robin said “Thank you for being here with me,” and got a kiss on the head.
“What do you see?” Robin said.
“Us. A year ago and change. I remember that day like it was yesterday. Your mom had just died, so I took you here. To get your mind off things.”
“You did. That was the first day in months I'd felt truly safe and truly at peace. That was love.”
“I know it was. And I still love you, just the s-.”
“It's a kind of love,” she said, cutting me off again. “And it's absolutely beautiful when it lasts. But can I show you something else?”
“Uh… okay. Yeah.”
She took my hand again, and again Infinity itself rolled in and out like the tide, and then we were somewhere else. The hospital, it looked like. St. Joseph’s.
“What do you see here?”
I looked around. Nurses running up and down the hallway. Doctors reviewing notes and talking to their patients.
“I don't know. A hospital.”
She nodded in the direction of a particular room. “Look in there.”
So I did. There was a woman on the cot. She was emaciated and hairless and deathly frail, and the Doctors inside were shutting off the last of the machines.
“A dying woman,” I said. “Looks like cancer.”
“Yep. And what about there?”
I looked down. There was a nurse crouched down in front of the same door and talking to a girl - eight or nine years old, if I had to guess - in silly voices. The girl had been crying, but the nurse managed to make her smile a bit, even as her mother died on the other side of the door.
“Looks like a nurse comforting a little girl.”
“That's right,” Robin said. “And that little girl will remember that nurse for the rest of her life - even if they never meet again or so much as exchange names - as the lady who came to her in her darkest hour and made her smile.” She turned to me. “That's love, too. Just as beautiful and just as previous as what we had.”
“What's your point?”
She didn't answer; she just stuck out her hand with a sad smile, and I took it. Infinity faded in and back out a third time. And then we were in the waiting room.
“See that?” Robin said. She pointed to the corner of the room, and I squinted.
“Oh hey!” I said. “That's Dylan! What's he doing here?”
“He called the ambulance when you didn't come out of the bathroom,” she said. “He knew something was wrong, and when they drove you off he followed them here. Been standing there ever since, asking for information on you every time a nurse walks by. He's starting to annoy them.”
I watched my roommate for a bit, and sure enough he grabbed a nurse, and asked her a question that I couldn't hear. She said something pleasantly dismissive, and he nodded, and then leaned his head back up against the wall and closed his eyes.
“Wow. I uh, I had no idea he cared that much.”
“That's love, too, Brian. Would you do the same for him?” But she held out her hand again before I could answer, and I took it. For a fourth time Infinity blinked.
And then I was in the emergency room, looking down on myself. I was covered in vomit from the charcoal and the pills, but I was still, too. Deathly still. Most of the nurses and the doctor were still walking out the door.
But Rachel wasn't. She was crying openly now, and making no effort to hide it. She reached for something. A needle, it looked like, or a syringe.
“What's she doing?”
“You'll see soon enough,” Robin said. “But that there? That's also love.” She held out her hand once again and said, “One more.” And I took it.
And then we were in the parking lot of the same place. The rain was coming down harder than ever.
“Turn around,” Robin said. And I did. And then I stopped; There were no words.
It was my father in his car. He was holding a Bible up to his chest with both hands, and he was crying in a way no child should ever have to see their father cry.
“And that there?” Robin said. “That's the kind of love that can move mountains.”
I put my hand up against his window. He didn't seem to notice.
“He can't see you, Brian. Not from there.”
I wiped my eyes with the back of my hand. “Okay,” I said. “I get it. I fucked up.”
And then she released my hand, and all of a sudden we were back in the clouds again, under the stars. I wiped another tear before it fell.
“So now what? It's too late for me to go back down there. I'm already gone.”
Robin took another step forward, and without another word she put her hand on my temple, and my eyes rolled back.
And then I saw it.
*Rachel and I are on a beach. Our child is playing out in the surf, and the sun hits her hair just right, and for a moment it is made of gold.
And then the image fades, and another one takes its place.
A birthday party. I have silver hair at my temples. Rachel does too. But it doesn't matter. Our little girl is turning ten.
And then that image fades, too, and is replaced by another, and another, and another; each one yielding another moment where someone loved someone else enough for it to break through the clouds and be seen forever, even if the moment itself lasted only for a heartbeat.
Finally there is an image of Rachel and myself on a porch as old as we are, and she holds my hand and says, “I'm glad you didn't follow her.”
And I say back, “Me too,” and I kiss her on the head.
And then Robin pulls back her hand, and again standing out there in the clouds together.
“How did you do that?” I asked.
She shrugged. “Time has nearly no meaning in this place. I've been here for a while, Brian, and yet the doctors haven't even left your operating room. Don't think too much about it. Just think about what you want.”
“That,” I said. “Was… was that my future?”
She shrugged again. “Could be. I don't know what you saw, and I don't need to know. Was it enough?”
I nodded, and she stepped forward again, and said “Then go and get it.”
“I'll miss you too damn much.”
“Well there's nothing wrong with missing someone,” she said. “That just means love lasted a little longer than what ignited it. So go ahead and miss me. You owe me that much. Feel the loss; stand up to the storm like a man, and memorize the pain, and learn it inside and out, and let it roll over you in waves and run its course. And then one day you'll wake up and realize you have scar-tissue where the skin used to be, and you'll be stronger than the grief ever was.”
“I can tell you've been working on that speech for a while.”
“Like I said. I've been here for a while.” She said. “You're made up of the stars, kid. Now go light up the world.”
And she kissed me, one last time. And then she was…
“...gone, Rachel. Okay? He's gone. Give it up for Christ's sakes and-”
But I shot upright before the doctor could finish the thought, and I gasped for air when I did and grabbed at my chest with more strength than I'd had in hours. There was a needle in it; a bolt of life to the heart, and Rachel broke down in tears when she saw me.
“Well I'll be damned,” the doctor said. “Welcome back to the land of the living, son. And Rachel?”
She turned around.
“Good work, kid. Made me proud.”
And he left, and she turned back to me and tried to hide a smile while she did it. “Hey there. How’re you feeling?”
“Better than dead.” There was a pause before I added, “Hey. I'm glad you got your win.”
She took my hand and squeezed it. For a moment she paused when she saw a scar below the wrist that looked like the result of fingernails dragging through flesh. But then she dismissed it and said, “I am too. And you'll get yours. Okay? I promise you will.”
I said, “I know.” And with that she got up and left the room to go save someone else’s life, while I took out my phone, and opened up the most recent text, and hit reply.
‘Am now.’
Facebook
1 note
·
View note
Text
A Common Data Analysis Pattern with a Simple Solution in R
It seems that much of the data analysis work I've done over the last few months has followed a "script". First, identify data, often government-sponsored and freely-available, that's of keen interest. Next, find the websites that house the data and download the relevant files to my notebook. The downloads might ultimately be one-off or included in the data analysis programs. Finally, load the data into either R or python and have at it with queries, visualizations, and statistical/learning models. Several examples of recent work come to mind. The first involves data from the Bureau of Labor Statistics on jobs and educational attainment from 1992-2017. On this site, 24 spreadsheets are available detailing monthly statistics on six measures of employment by 4 levels of educational attainment. For a previous blog, I downloaded 12 of these files, including measurements laborforce, employed, and unemployed by educational levels no HS, HS grad, some college, and college grad. I renamed the spreadsheets on my SSD to include indicators of dimension -- eg "clf_laborforce_collegegrad.xls". The second example, the topic of this blog, has to do with Medicare charges summarized by hospital and diagnostic related group (DRG). At this point there are five files (either csv or spreadsheet) available for download, representing the years 2011-2015. Year is embedded in the website file names. A third illustration, and the topic of a coming blog, revolves on census data from the American Community Survey. The pattern behind the three cases includes: * readily downloadable files, generally either csv or xls. These files can either be copied by hand or moved programmatically. * multiple of these files, often dimensioned by time or other variable(s). * a common, consistent format to the files, so that "reads" will work similarly on each. * a structured file naming convention, either given or assigned, that provides dimensional info for data loads. Date/Time is the most common diemnsion. In this article, I looked at the Medicare charges data that consists of five yearly csv files. I expect the next year in the sequence, 2016, to be posted in the near future. I first downloaded the five files to my laptop, programmatically in this case. I then used Jupyter Notebook and R 3.4 to analyze the data with code that takes advantage of the commonalities. The data.table package along with the tidyverse ecosystem and fast file compression, read/write library fst, plus a functional approach, are central to the work. This is not your older sibling's R. None of the highly-performant packages used here are included in core R. Rather, they are the bounty of an exhuberant and capable R ecosystem of developers. Incidentally, if this notebook were written in python, I'd be giving similar accolades to its community. The remainder of the notebook details the R code to implement the loading of this data into R and some simple subsequent analysis. The structure of the code in this instance is very similar to that of the other examples cited. To read entire content, click here https://goo.gl/71mCCX #DataScience #Cloud
0 notes
Text
Predicting medical chronic conditions with Machine Learning
Note - Some parts of this post requires some familiarity with basics of Machine Learning. These terms should be understood in a technical form - Binary Classification, Accuracy, AUC, Biased Dataset
TLDR -
It is possible to build a system to predict medical chronic conditions with ML.
The path to actually building an ML system from scratch is long and winding and will probably differ for each company. It’s very messy and undefined in the start - and that's ok.
You do NOT need a huge amount of data to start. Use proxies and try to get some real world data points.
There are plenty of ways to use the initial results in a commercial application - especially for targeting/identifying customer types.
Read the newly released Machine Learning Yearning if you don’t know where to start.
DoctorC has been doing diagnostics for 3 years now. We have gone from running operations on spreadsheet to end to end automated systems which handle everything, from placing an order, to delivery of reports. We also store all reports and some report values for our customers so that they can easily access their medical history from anywhere.
A few months ago, we started an initiative to see if we can apply ML on our data and get some useful applications out of it. We are an extremely small company with very limited amount of resources. So it was basically just me running some experiments and dedicating only a few hours a week.
The first question we asked ourselves before starting was - “How is it going to be useful to us as a business?”. The answer was surprisingly easy.
We have two kinds of customers -
People who undergo some illness/accident etc where they need some medical help - but only one time.
People who have chronic conditions like hypertension, diabetes, cholesterol issues etc.
#1 are transactional and #2 are our repeat customers. #2 use/need our service the most and they are consequently very valuable to us. In Urban India, chronic conditions (non communicable diseases) are on the rise rapidly and the prevalence of diseases vary from 15% all the way to 35% (WHO link - http://www.who.int/choice/publications/Chronic_diseaseIndia.pdf).
These are the customers we are looking for. So the question boiled down to - “How do we identify people with chronic conditions?”. Once we identify them - we can enroll them in a program specifically tailored for people who need medications and diagnostic tests frequently.
The hardest point - Starting
We needed to start with a training set of people who are identified as chronic. We had 0 points of data for this.
So we looked for proxies. “What behaviour indicates if a person has a chronic condition?”. Answer - People who used our services frequently are more likely to be chronic.
We keep track of every test that was bought and their results for every customer. Therefore, we had a (comparatively speaking) rich medical history at our fingertips. On top of that - our in-house proprietary system can “read” a diagnostic report and infer structured medical data for a whole array of tests.
Based on this, we started with an initial training set of a couple of hundred people who were deemed “chronic”. We used another set of infrequent buyers as negative examples for our model.
I explored a whole bunch of options on what platform to use for training ML - Scikit Learn, Tensorflow, AWS Machine Learning and Microsoft Azure. Azure’s ease of use puts it in another league altogether - especially for people who want to just apply existing ML algorithms. Drag and drop, kicking off experiments parallely, easy to construct flows etc. allow you to move really really fast as compared to writing code.
This might become a bottleneck later as we scale or it might become more expensive to run - but the tools they provide save tons of time, especially for prototyping and experimentation. I highly recommend trying out Azure - their free tier gives a good taste of what’s possible on their platform.
Before you start, or while you are playing with your dataset - you need to decide what your “One True Metric™” is. This is the thing you are going to optimize for while evaluating different machine learning models. By definition, it is very specific to your problem and cannot be purely decided based on a formula.
For us, it was identifying people with chronic conditions with a highly imbalanced data set (we have a lot less people with chronic conditions compared to normal population). It’s a binary classification problem. I chose AUC as a measure and started experiments to optimize that. Why did I not choose Accuracy? That is a post for another day.
We did an initial split of 50/50 of positive and negative samples to ensure we didn’t bias the system with a small initial set. Then i started my experiments. This is the messy part - you have to start from the simplest models and run different models simultaneously on the same data.
The first set of results yielded AUC curve similar to this -
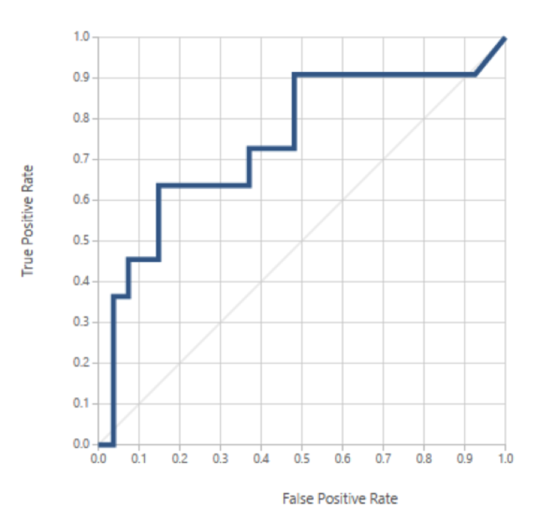
Tight Iterations
We did our first real world test with a model of an AUC of 0.58 (which is not a very good score). We took the top 100 predictions by the model and started verifying if the identified people were chronic. We recorded this data and then used it to create a newer model. This gave us another 100 predictions. Then we repeated the cycle again.
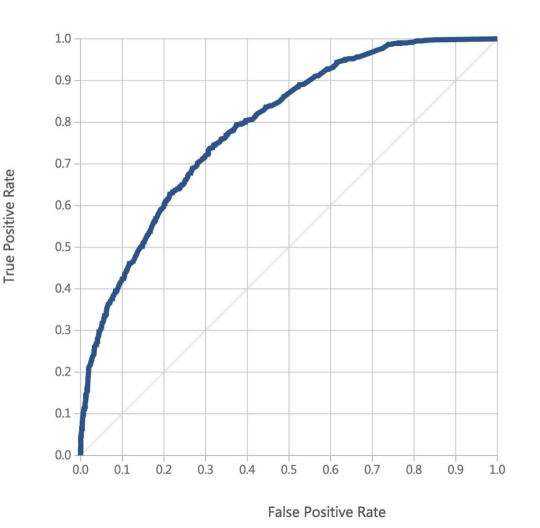
The model started improving with each iteration. Reconstructing new model with new data took only a couple of days and the model training process itself was only a few minutes. Gathering the data was the only bottleneck.
Our model’s curve improved as shown below. And our total dataset from a raw data standpoint was around 1.2 million discrete values. Our accuracy was approaching ~80% (first couple of hundred predictions for every iteration). The AUC of the best model would vary from 0.74 to 0.80. The accuracy had a steep fall afterwards, but it was still significantly better than the 15% to 20% accuracy you would get with a random sample.
Predictive Factors
More interesting were the predictive factors for chronic conditions. While I cannot delve into too many details, one of the most interesting find was that Vitamin D (both the number of purchases done and the values of it) were one of the most predictive factors for someone being chronic or not. It neatly fits into the current research which suggests that Vit D is extremely important to maintain since it affects almost every system in our body. You should get Vit D levels checked every 6 months or a year - especially if a large part of your day is spent indoors.
Conclusion
Yes, you can predict, with a high degree of accuracy as well as high AUC, if someone is suffering from a chronic condition based on a combination of their purchase behavior (surprising) and their test values (not very surprising, still exciting). The next question was whether we could actually hone down to a specific condition like Diabetes, Thyroid disorders etc. That is a post for another day.
There is also the long term possibility of actually providing diagnosis while working side by side with doctors. This system is a small step in fulfilling that vision. We have miles to go before we sleep.
We are very excited about the possibilities that this kind of data enables. If you would like access to this data (especially for medical research purposes) or would like to know additional details please contact me on karan at the rate doctorc dot in.
1 note
·
View note
Text
‘I love hearing my Rice Krispies’
Retiree Greg Green has faced more than his share of challenges.
Born with congenital glaucoma, his sight deteriorated over time until he lost his vision completely in 2012. To top it off, Meniere’s disease affected his hearing.
Now blind and nearly deaf, the 68-year-old counts his blessings.
“Life is not about how many times I fall down,” Green said. “It’s about how many times I get up and keep going.”
A story of perseverance
After graduating Belding High School in 1971, Green started working as a janitor at a (then) small company named Amway Corporation in Ada, Michigan. Although blind in his right eye and with limited vision in his left, he enjoyed toying with his first computer, a little Tandy 64. He taught himself BASIC language programming, and parlayed his creativity and willingness to learn into a long career in information technology.
“It was a job I loved, not a doldrum,” Green said. “I loved creating things and solving problems.”
When his second daughter, Heidi, was also born with congenital glaucoma, much of the family’s time and resources were spent getting both Greg and Heidi needed medical attention. The family got by with a run-down AMC Gremlin and shopping at yard sales.
“God was faithful, and I thank him for his care,” Green said. “It sure taught me how to trust God and work hard.”
In his mid-30s, Green experienced major bouts of vertigo that slammed him to the floor without any warning. A neurologist diagnosed Meniere’s disease, a disorder of the inner ear that leads to vertigo and eventual hearing loss. In Green’s case, the disease robbed him of hearing in his left ear about 15 years ago, and the right ear became worse over time.
Hearing aids alleviated the problem for many years. But eventually they weren’t enough. While others with hearing loss may rely on reading lips, that wasn’t an option for Green, who can’t distinguish between dark and light.
His communication became nearly cut off.
Then, in 2017, Green saw Gregory Artz, MD, a specialist in otology and neurotology with Grand Rapids Ear, Nose and Throat, who is credentialed to operate at Spectrum Health hospitals. Dr. Artz recommended a cochlear implant, a device that picks up sound with a microphone and delivers it to the auditory nerve.
Next he met Darcy Jaarsma, AuD, an audiologist in the neuro diagnostics department of Spectrum Health Butterworth Hospital, who tested Green’s hearing and confirmed he was a good candidate for a cochlear implant.
After receiving an implant in his left ear, Green quickly realized that it wasn’t an instant solution. When his device was turned on a few weeks after surgery, the sounds he heard? Unrecognizable.
“All I heard was a really squeaky sound, and I had zero understanding,” said Green, noting that voices reminded him of early Mickey Mouse movies.
The issue didn’t surprise Dr. Jaarsma.
“The way a cochlear implant provides sound is completely different from the sounds you and I hear,” she said. “There definitely is a time period it takes to acclimate.”
Green, a self-described “tech head,” took on the challenge with determination.
He created an alphabetized spreadsheet of 21,000 different words, then used screen-reading software to listen to the words for hours on end every day.
For the first few months, he couldn’t understand a word.
“Luckily I have a good strong level of perseverance,” Green said. “I was taught as a kid that you work on it until you get it done. I was determined to get the job done if it killed me.”
He recalled the words of inventor Thomas Edison, who also had hearing difficulties: “Genius is 1% inspiration and 99% perspiration.”
“For me, the inspiration was the spreadsheet, but the perspiration was working through it so slowly for months,” Green said.
Within a year, he trained himself to the point of understanding 93% of words using the implants in his left ear.
Unfortunately, as the left ear improved, the right one worsened.
Late in 2019, he received a cochlear implant for his right ear.
It was time to go back to work on this self-created audio therapy.
“I’ve been hammering away at the spreadsheet about four to five hours a day,” he said. “It really helps with communication skills.”
Dr. Jaarsma said Green is an ideal patient.
“It’s definitely patients who have a positive outlook on life, and are grateful for what the technology can do, who receive the most benefit and do the best with their implant,” she said. “And patients who ‘practice’ listening, like Greg did with his computer program, maximize their outcomes.”
In the world of cochlear implant patients, Green is a bit of a rock star. In fact, he was invited to share his story to a group of otolaryngologists in West Michigan in March.
“It was a thrill to tell my story,” Green said. “They were very receptive.”
‘Keep on keeping on’
Green’s motto is “keep on keeping on,” and that’s exactly what he does.
After retirement, Green and his wife, Louise, moved to the Allegan area to be near family.
He’s attuned to the little sounds that make up his world: cars going past the house, water running from a faucet, shoelaces being tied.
Even food noises, like burgers frying and wrappers coming off a slice of cheese. And the snap, crackle, pop of a bowl of cereal.
“I love hearing my Rice Krispies,” Green said.
Green stays in shape mentally and physically. A World War II buff, he enjoys listening to books and walks 3 miles on the treadmill daily. He also spends time encouraging others in his church through phone calls and inspiring emails.
Throughout it all, Green appreciated the patience of Louise, his wife of 47 years, his two adult daughters and their families.
“They have been so supportive and patient with the old man. I understand trying to deal with a hearing impaired person who is also blind isn’t easy,” he said.
‘I love hearing my Rice Krispies’ published first on https://nootropicspowdersupplier.tumblr.com/
0 notes
Text
‘I love hearing my Rice Krispies’
Retiree Greg Green has faced more than his share of challenges.
Born with congenital glaucoma, his sight deteriorated over time until he lost his vision completely in 2012. To top it off, Meniere’s disease affected his hearing.
Now blind and nearly deaf, the 68-year-old counts his blessings.
“Life is not about how many times I fall down,” Green said. “It’s about how many times I get up and keep going.”
A story of perseverance
After graduating Belding High School in 1971, Green started working as a janitor at a (then) small company named Amway Corporation in Ada, Michigan. Although blind in his right eye and with limited vision in his left, he enjoyed toying with his first computer, a little Tandy 64. He taught himself BASIC language programming, and parlayed his creativity and willingness to learn into a long career in information technology.
“It was a job I loved, not a doldrum,” Green said. “I loved creating things and solving problems.”
When his second daughter, Heidi, was also born with congenital glaucoma, much of the family’s time and resources were spent getting both Greg and Heidi needed medical attention. The family got by with a run-down AMC Gremlin and shopping at yard sales.
“God was faithful, and I thank him for his care,” Green said. “It sure taught me how to trust God and work hard.”
In his mid-30s, Green experienced major bouts of vertigo that slammed him to the floor without any warning. A neurologist diagnosed Meniere’s disease, a disorder of the inner ear that leads to vertigo and eventual hearing loss. In Green’s case, the disease robbed him of hearing in his left ear about 15 years ago, and the right ear became worse over time.
Hearing aids alleviated the problem for many years. But eventually they weren’t enough. While others with hearing loss may rely on reading lips, that wasn’t an option for Green, who can’t distinguish between dark and light.
His communication became nearly cut off.
Then, in 2017, Green saw Gregory Artz, MD, a specialist in otology and neurotology with Grand Rapids Ear, Nose and Throat, who is credentialed to operate at Spectrum Health hospitals. Dr. Artz recommended a cochlear implant, a device that picks up sound with a microphone and delivers it to the auditory nerve.
Next he met Darcy Jaarsma, AuD, an audiologist in the neuro diagnostics department of Spectrum Health Butterworth Hospital, who tested Green’s hearing and confirmed he was a good candidate for a cochlear implant.
After receiving an implant in his left ear, Green quickly realized that it wasn’t an instant solution. When his device was turned on a few weeks after surgery, the sounds he heard? Unrecognizable.
“All I heard was a really squeaky sound, and I had zero understanding,” said Green, noting that voices reminded him of early Mickey Mouse movies.
The issue didn’t surprise Dr. Jaarsma.
“The way a cochlear implant provides sound is completely different from the sounds you and I hear,” she said. “There definitely is a time period it takes to acclimate.”
Green, a self-described “tech head,” took on the challenge with determination.
He created an alphabetized spreadsheet of 21,000 different words, then used screen-reading software to listen to the words for hours on end every day.
For the first few months, he couldn’t understand a word.
“Luckily I have a good strong level of perseverance,” Green said. “I was taught as a kid that you work on it until you get it done. I was determined to get the job done if it killed me.”
He recalled the words of inventor Thomas Edison, who also had hearing difficulties: “Genius is 1% inspiration and 99% perspiration.”
“For me, the inspiration was the spreadsheet, but the perspiration was working through it so slowly for months,” Green said.
Within a year, he trained himself to the point of understanding 93% of words using the implants in his left ear.
Unfortunately, as the left ear improved, the right one worsened.
Late in 2019, he received a cochlear implant for his right ear.
It was time to go back to work on this self-created audio therapy.
“I’ve been hammering away at the spreadsheet about four to five hours a day,” he said. “It really helps with communication skills.”
Dr. Jaarsma said Green is an ideal patient.
“It’s definitely patients who have a positive outlook on life, and are grateful for what the technology can do, who receive the most benefit and do the best with their implant,” she said. “And patients who ‘practice’ listening, like Greg did with his computer program, maximize their outcomes.”
In the world of cochlear implant patients, Green is a bit of a rock star. In fact, he was invited to share his story to a group of otolaryngologists in West Michigan in March.
“It was a thrill to tell my story,” Green said. “They were very receptive.”
‘Keep on keeping on’
Green’s motto is “keep on keeping on,” and that’s exactly what he does.
After retirement, Green and his wife, Louise, moved to the Allegan area to be near family.
He’s attuned to the little sounds that make up his world: cars going past the house, water running from a faucet, shoelaces being tied.
Even food noises, like burgers frying and wrappers coming off a slice of cheese. And the snap, crackle, pop of a bowl of cereal.
“I love hearing my Rice Krispies,” Green said.
Green stays in shape mentally and physically. A World War II buff, he enjoys listening to books and walks 3 miles on the treadmill daily. He also spends time encouraging others in his church through phone calls and inspiring emails.
Throughout it all, Green appreciated the patience of Louise, his wife of 47 years, his two adult daughters and their families.
“They have been so supportive and patient with the old man. I understand trying to deal with a hearing impaired person who is also blind isn’t easy,” he said.
‘I love hearing my Rice Krispies’ published first on https://smartdrinkingweb.tumblr.com/
0 notes
Text
Arizona and Ohio Speak Up to Defend Health Care by Sarah Chaisson-Warner
223,300 in Arizona. 360,000 in Ohio. That’s how many people will lose their Medicaid coverage if the GOP forces through the health care repeal they’re currently drafting behind closed doors in the Senate. Arizona and Ohio voters overwhelmingly oppose the repeal, as they do in every state.
Photo credit: Ted Eytan, Flickr / CC
Senators Jeff Flake and John McCain of Arizona, and Rob Portman of Ohio have the power with their three votes to protect health care for more than half a million of their constituents. Or, they can vote to kick them off, and cause inestimable suffering to their constituents and to millions more like them all across the country.
These three senators – Flake, McCain and Portman – could block passage of the most disastrous health care bill this country has ever seen.
Here are the stories of a few of the voters in Arizona and Ohio who stand to lose everything if these three choose to stand with billionaires and corporations instead of with the people who elected them.
Senators, are you listening?
My husband was the controller for a multi-billion dollar international company financing high and commercial and residential properties. He worked from spreadsheets on three computer screens and assured that multi-million dollar jobs were managed to the last nail and board.
One day he looked at his computer screens and was not sure what he was looking at. Not long after that, he was laid off for making too many mistakes. At age fifty-nine my husband was diagnosed with dementia. He is also a cancer survivor, has COPD, diabetes, and a fib, all pre-existing conditions. He is now sixty-four, has been on SSDI for three years, and has Medicare. I am also 64, with COPD (pre-existing condition) and I continue to work for our primary health insurance.
When my husband was laid off our retirement dreams came crashing down. We lost our house and used the bulk of my 401(k) to purchase a small condo. We get by.
The proposed health care bill – with its age rating, exclusions for pre-existing conditions and further premium increases for our health conditions – will leave us with the choice of being homeless or going without our maintenance medications, diagnostics, and preventive care, such as screening colonoscopies and prostate exams, and mammograms, leaving us at high risk for death.
I would like to think that my elected officials do not want my husband and I to suffer and die, but if you vote for this bill these are the choices we look forward to.
– Ann, Arizona
The ACA saved my spouse’s life. She had breast cancer and didn’t even know it. Before the ACA was passed we hadn’t had insurance for a very long time because we couldn’t afford it. I was in poor health as well and had a bucketload of conditions, the ACA saved us both.
Without the ACA, it is likely that my spouse would be dead by now and I wouldn’t be far behind her. As of this year, we both qualified for and signed up for Medicare. Although we struggle to make the Medicare Supplement payments each month, we are grateful that we have it. We remember the years before the ACA, and Medicare, when there was no help for us at all. Growing old and trying to survive despite poor health is no way to live. We both worked and contributed to society our whole lives. We never amassed much money, let alone a safety net. We are grateful to still be alive and to have each other. There are so many people, both old and young, that our country has forgotten. These programs are lifesaver. It is sad and morally unconscionable to take them from the millions of Americans who need them.
– Gail, Arizona
I have Type 1 Diabetes, which means I need insulin, test strips, syringes, and a whole host of other medical supplies to survive. My employer does not provide insurance. I would not be able to afford these medical supplies and necessary doctors visits if I was not covered under the Affordable Care Act.
– Erin, Ohio
It wasn’t until preventative care became readily available, encouraged, that I found out about a serious condition. Preventative care access saved my life!
– Jonna, Ohio
I am so grateful for the ACA which has provided coverage for my husband, who is a veteran, and has a preexisting congenital heart condition. Because of the ACA, he has been able to receive life saving medical treatment from the world renowned Cleveland Clinic. Healthcare is a human right. Please save the ACA for those like my husband!
Without the ACA, our health insurance coverage would be unaffordable due to my husband’s preexisting conditions. Prior to the ACA, we paid almost $40,000 per year for health insurance. After ACA, our insurance was less than half that amount for just about the same coverage.
– Debra, Ohio
I can think of at least six people in my extended family that have benefited from the ACA, Medicare of Medicaid and would be in very difficult positions if they were unavailable.
First and foremost, there is my husband. He is 59 years old and has suffered from a chronic seizure disorder since he was thirty-six. Doctors are mystified by its origin and only the drug, Lamictal, can control his grand mal seizures. This medicine alone would cost us nearly $24,000 if we had no health coverage. He is also a Colon Cancer survivor. So, with two pre-existing conditions and his age, we would be completely unable to afford insurance (assuming we could even find a carrier) and his physical and mental health, not to mention that of my family members would be at risk.
Thanks to the ACA, I can insure my son who is now 24 until he is 26. While he is employed, he does not earn enough to purchase insurance on his own, especially as subsidies become unavailable. I also have a 21 year old daughter who will have the same opportunity under the ACA. She is a college student and plans to continue her studies for a PhD, so she does not have the income to afford health insurance on her own.
My sister is 54 years old and under-employed. Thanks to the ACA, she was able to obtain health insurance, including dental, for the first time in her adult life.
My niece was able to obtain health insurance for her three children at a rate that she could actually afford thanks to the ACA. She is a manager at a restaurant and has no access to health care through her employer.
My brother in law is 60 years old and was afflicted by non-cancerous parasympathetic tumors that attached to his lung and spine, causing him to be disabled. He was able to obtain rehabilitative therapy and have most of his medical costs covered due to Medicaid.
The combined impact of the ACA and Medicaid expansion in Ohio has truly been a godsend for my family!
– Kim, Ohio
I am 58 years old and by natural extension have pre-existing conditions. I have asthma, etc. My son is an adult who is wheelchair bound since birth and very dependent on Medicaid. I would not be able to afford health care under the new bill and went bankrupt trying to pay premiums before the ACA went into effect.
– Jennifer, Ohio
I am a 51 year old man who was diagnosed with juvenile diabetes at age 10. I checked my blood sugars and took insulin daily for 17 years when my vision left me. Adjusting to being b lind, not more than three months later, my kidneys stopped functioning and i went on dialysis. 7 months later i received a kidney-pancreas transplant which functioned well for 16 years before dialyzing again. This for another 3 years , after which i received another kidney transplant; did not receive a pancreas this time, and hence, i am a diabetic again. Given my history, Trump Care would just as soon sit me on a curb to be taken out with the trash as to give me any assistance.
– Calvin, Ohio
My 91 year old grandmother is able to stay in her home with assistance from the provisions under the Affordable Care Act, Medicare, and Medicaid. My own health care costs under the Affordable Care Act have been reduced by $300 a month, with an increase in services!
– Lisa, Ohio
I have diabetes and was able to get on the Medicaid expansion because of my pre-existing condition and because I don’t make enough money. It truly saved my life because my prescription prices were so high for my insulin I need to live.
– Nate, Ohio
0 notes
Text
Sitting up...how it all began.
2.3.2017
So you meet someone who just makes your insides feel like confetti all the time, and you think...over eight years...this is it- she’s the girl that I would live under a bridge with if the end of the world happened. Brilliant smile, fierce sense of focus, completely put-together, beautiful heart and priceless dedication. Her eyes melt the sarcastic, realistic pessimist away and puts me in a vulnerability that still strikes as ridiculous to this day. Our love and relationship never came without sacrifices or arguments...but who really appreciates things that come easily to them anyway?
There is a lot going on in the world right now:
We have this guy in office who seems to be making things harder on quite a few people and has only been around for a week. We happen to be one of those populations (of the female, of the minority {latinas} and of the lesbian) that some politicians have bulls-eyes aimed at rights for. Religion isn’t exactly getting its fair share of nice treatment. Neither is race for that matter. Lets face it, this unpredictable world is now basically in nuclear unpredictability status.

On that note.
I walked to the bed and sat down. She was lying there and I asked nonchalantly, “So what are we planning to do over the next few years?” It was random. Not really well thought out to be honest. I tend to think I am a better writer than speaker...Maybe I should’ve just written it in text - I thought.
Just kind of a well, I love her...and...well...shes amazing, we make great memories together, and she makes me happy. We had this chat in the past, here and there. Piecemeal. Then the conversation somehow merged into, maybe we could make something greater than ourselves and start a family. Lets be honest, we are kind of awesome (yep, that's me- good with words).
So here we are...
We went to a fertility clinic open-house awkwardly after work a week or so later. Even more awkwardly, it ended up being more of an ‘in crowd’ fertility clinic open house. Picture a bunch of employees, some existing patients...everyone knew each other. People ate, we sat there smirking awkwardly...like kids at their first school dance sitting on the gym bench. Opened a book on the table- no reason really, we didn’t understand the clinical book anyway, but it made us look busy. Then decided it wasn’t too valuable, was extremely awkward and 007 sneaked out. To walk to the end of the block and have some drinks. Yep. We were off to a good start.
Fast forward a bit. The real conversations began, we spoke about our priorities:
Me? - As a lesbian couple, I want us to feel comfortable and trusting. Welcomed. Safe. Not discriminated against and confident in their work.
Her? - Success rate. (I did say she was the more practical and well put together one)
I put together a Google spreadsheet consisting of To-do, Schedule, Hyperlinks, Insurance Info, Detailed Budget, Price estimator, Schedule and Notes sections. Cue highlights and bold-face type. Lasers and sound machine.Then put it all in a Google Folder and made Google sub-folders for good measure. Shared it. Clearly, using this as a perfect opportunity to showcase both my technical and organizational skills.

We spoke to other clinics, wrote down questions. I read three books in two weeks. Of particular value: Rachel Pepper’s, “The Ultimate Guide to Pregnancy for Lesbians: How to Stay Sane and Care for Yourself from Pre-conception through Birth, 2nd Edition”.
Then we made the appointment for a consultation with a doctor from another clinic...and this time we were ready. After a barrage of questions and voice-cracking sentences (both out of nervousness and a very douche-bag cold), we did it- we scheduled our first set of diagnostic clinical tests.
And today they probed us for a vaginal ultrasound and conducted blood tests...
even though we were losing enough anyway because of our “menses”.
Here's to a glorious next episode of the expedition...
0 notes
Text
Predicting medical chronic conditions with Machine Learning
Original post here.
Note - Some parts of this post requires some familiarity with basics of Machine Learning. These terms should be understood in a technical form - Binary Classification, Accuracy, AUC, Biased Dataset
TLDR -
It is possible to build a system to predict medical chronic conditions with ML.
The path to actually building an ML system from scratch is long and winding and will probably differ for each company. It’s very messy and undefined in the start - and that's ok.
You do NOT need a huge amount of data to start. Use proxies and try to get some real world data points.
There are plenty of ways to use the initial results in a commercial application - especially for targeting/identifying customer types.
Read the newly released Machine Learning Yearning if you don’t know where to start.
DoctorC has been doing diagnostics for 3 years now. We have gone from running operations on spreadsheet to end to end automated systems which handle everything, from placing an order, to delivery of reports. We also store all reports and some report values for our customers so that they can easily access their medical history from anywhere.
A few months ago, we started an initiative to see if we can apply ML on our data and get some useful applications out of it. We are an extremely small company with very limited amount of resources. So it was basically just me running some experiments and dedicating only a few hours a week.
The first question we asked ourselves before starting was - “How is it going to be useful to us as a business?”. The answer was surprisingly easy.
We have two kinds of customers -
People who undergo some illness/accident etc where they need some medical help - but only one time.
People who have chronic conditions like hypertension, diabetes, cholesterol issues etc.
#1 are transactional and #2 are our repeat customers. #2 use/need our service the most and they are consequently very valuable to us. In Urban India, chronic conditions (non communicable diseases) are on the rise rapidly and the prevalence of diseases vary from 15% all the way to 35% (WHO link - http://www.who.int/choice/publications/Chronic_diseaseIndia.pdf).
These are the customers we are looking for. So the question boiled down to - “How do we identify people with chronic conditions?”. Once we identify them - we can enroll them in a program specifically tailored for people who need medications and diagnostic tests frequently.
The hardest point - Starting
We needed to start with a training set of people who are identified as chronic. We had 0 points of data for this.
So we looked for proxies. “What behaviour indicates if a person has a chronic condition?”. Answer - People who used our services frequently are more likely to be chronic.
We keep track of every test that was bought and their results for every customer. Therefore, we had a (comparatively speaking) rich medical history at our fingertips. On top of that - our in-house proprietary system can “read” a diagnostic report and infer structured medical data for a whole array of tests.
Based on this, we started with an initial training set of a couple of hundred people who were deemed “chronic”. We used another set of infrequent buyers as negative examples for our model.
I explored a whole bunch of options on what platform to use for training ML - Scikit Learn, Tensorflow, AWS Machine Learning and Microsoft Azure. Azure’s ease of use puts it in another league altogether - especially for people who want to just apply existing ML algorithms. Drag and drop, kicking off experiments parallely, easy to construct flows etc. allow you to move really really fast as compared to writing code.
This might become a bottleneck later as we scale or it might become more expensive to run - but the tools they provide save tons of time, especially for prototyping and experimentation. I highly recommend trying out Azure - their free tier gives a good taste of what’s possible on their platform.
Before you start, or while you are playing with your dataset - you need to decide what your “One True Metric™” is. This is the thing you are going to optimize for while evaluating different machine learning models. By definition, it is very specific to your problem and cannot be purely decided based on a formula.
For us, it was identifying people with chronic conditions with a highly imbalanced data set (we have a lot less people with chronic conditions compared to normal population). It’s a binary classification problem. I chose AUC as a measure and started experiments to optimize that. Why did I not choose Accuracy? That is a post for another day.
We did an initial split of 50/50 of positive and negative samples to ensure we didn’t bias the system with a small initial set. Then i started my experiments. This is the messy part - you have to start from the simplest models and run different models simultaneously on the same data.
The first set of results yielded AUC curve similar to this -

Tight Iterations
We did our first real world test with a model of an AUC of 0.58 (which is not a very good score). We took the top 100 predictions by the model and started verifying if the identified people were chronic. We recorded this data and then used it to create a newer model. This gave us another 100 predictions. Then we repeated the cycle again.
The model started improving with each iteration. Reconstructing new model with new data took only a couple of days and the model training process itself was only a few minutes. Gathering the data was the only bottleneck.
Our model’s curve improved as shown below. And our total dataset from a raw data standpoint was around 1.2 million discrete values. Our accuracy was approaching ~80% (first couple of hundred predictions for every iteration). The AUC of the best model would vary from 0.74 to 0.80. The accuracy had a steep fall afterwards, but it was still significantly better than the 15% to 20% accuracy you would get with a random sample.

Predictive Factors
More interesting were the predictive factors for chronic conditions. While I cannot delve into too many details, one of the most interesting find was that Vitamin D (both the number of purchases done and the values of it) were one of the most predictive factors for someone being chronic or not. It neatly fits into the current research which suggests that Vit D is extremely important to maintain since it affects almost every system in our body. You should get Vit D levels checked every 6 months or a year - especially if a large part of your day is spent indoors.
Conclusion
Yes, you can predict, with a high degree of accuracy as well as high AUC, if someone is suffering from a chronic condition based on a combination of their purchase behavior (surprising) and their test values (not very surprising, still exciting). The next question was whether we could actually hone down to a specific condition like Diabetes, Thyroid disorders etc. That is a post for another day.
There is also the long term possibility of actually providing diagnosis while working side by side with doctors. This system is a small step in fulfilling that vision. We have miles to go before we sleep.
We are very excited about the possibilities that this kind of data enables. If you would like access to this data (especially for medical research purposes) or would like to know additional details please contact me on karan at the rate doctorc dot in.
0 notes