#| clinician's opinion :: facts |
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
12.7% of mobile users access Tumblr.
Text
MUSE’S HANDWRITING ! pick a font that resembles your muse’s handwriting.

Eden's handwriting is very slow, wanders on the page, and sometimes stacks over itself or is oddly spaced if he's not actively very careful. When it's an option, he usually prefers to dictate and have someone else help write to ensure that the finished document will be legible to the reader, especially if it's medical instruction.
Eden's font is called I Know a Ghost, which I think is neat.
Swiped from @intothewildsea - steal from me and @ me so I can see !
2 notes
·
View notes
Text

Eden is a shirt stealer / borrower, very sorry to crew and anyone else that shares a living space with him. Style, cut, colour, and shirt-is-too-big do not usually matter - fabric softness and texture only. He can't see what he looks like in it anyway.
He will always wash and return it though.
Extra mini headcanon is that Eden enjoys doing the washing up - it's actually his chore in the group in the campaign his base character comes from! He embroiders little tangible letters or symbols in the hems of things to help remember special instructions since he can't read tags, and so he knows who to give things back to after they're clean.
1 note
·
View note
Text
i don't honestly have any interest in therapy atp for reasons of not wanting external forces encouraging me to spend even more time thinking about myself so i can solicit a stranger's opinion on my problemsissues etc but honestly i feel lucky to have arrived at this position because if i did think therapy was potentially useful to me i would be so fucked over with regards to the fact that even among clinicians who claim to be anti-carceral there is always a breaking point at which they will consider it a professional ethical responsibility to betray client confidentiality in ways that range from upsetting to endangering. like this is not a personal failure that can be fixed by switching to a nicer therapist because it's characteristic of the clinician-patient relationship that as the patient you always have the threat of force / coercion / compulsory treatment hanging over your head. this is directly a result of the epistemological authority that defines the clinician role: the therapist by definition knows best, so reporting mechanisms are always and only for the patient's own good, and removing such mechanisms will consequently be portrayed as doing harm to the very patients most endangered by them. like there simply is no clinician role without this deference to their professional judgment...... could not be me
194 notes
·
View notes
Note
Please, elaborate more on these Hazbin Hotel headcanons. I’m very interested in hearing about them.
I would like to preface all my posts on headcanons related to psychology and mental illness with a disclaimer: diagnosing mental conditions, especially personality disorders, can be extremely challenging. It's a complicated process that relies heavily on a psychologist's interpretation of facts, making it susceptible to biases. Personality disorders cannot be diagnosed based on surface-level observations and are not just labels that we can assign to people like in the case of MBTI. Additionally, I am not a clinician with any expertise in diagnosing people. Therefore, the following post should not be taken as a reliable professional opinion. It's simply my interpretation of the internal mechanisms that may be responsible for the behavior of certain characters in my fan fiction. Furthermore, I want to make it clear that I have no intention of stigmatizing people with personality disorders by associating them with villains. A personality disorder does not determine someone's character or make them a bad person. Some characters may be evil because of the choices they make, not as a result of their mental conditions.
Since you didn't ask about anything specific, I'll just give some headcanons on Vs since I think about them the most.
> Vs are not a polycule, it's VoxVal + Velvette because she would never touch any of these losers. What's more, Vox and Val are extremely sexist (I mean it's kinda canon, we heard how they speak about women) so if she had sex with any (or both) of them, she would no longer be one of the boys and become one of the bitches.
> Vox has NPD, Val has BPD, Vel has APD.
> Vox is continuously overstimulated because he's constantly connected to his web. That's why snaps so easily and sometimes goes through 5 stages of grief in 5 seconds. He could disconnect (and sometimes he does) but he's too much of a control freak to not lurk constantly.
> During his life on earth, Valentino had a terrible, toxic father. Very much machismo who abused him relentlessly for being queer. (Not that I want to make him sympathetic, I just think that evil people are often miserable before they become evil.) Because Val is very queer, not just "man occasionally fucking other men", he's always been loud and proud pansexual and gender non-conforming. He wasn't some kind of activist, very concerned about queer issues, he just refused to stay in the closet out of spite, and because it made men around him uncomfortable. He just enjoyed being perceived as a deviant. It was one of the things that eventually got him killed.
> Vox is like a hardcore sadist. He cuts people open just to feel powerful.
> During his life on Earth, Vox used to be extremely homophobic because his bisexuality was threatening to his masculinity. He's also the embodiment of toxic white masculinity from the 50's. He actually did some personal growth in Hell, eg. He gave up racism, homophobia, transphobia, and most other -phobias, and now he despites everyone rather equally. He just bullies women more because misogynistic violence is a low-hanging fruit.
> So with Velvette I had some fun because she manifested in Hell not so long ago and happened to be as powerful as other Vs, who had much more experience and souls collected. So I assumed she must be completely deranged. I came up with the idea that she used to be a toxic influencer who built a cult-like following around her. She weaponized it against multiple people, ruining lives, and manipulating kids into committing crimes or even suicides. Her methods are very fine, Vox and Val have nothing on her when it comes to cruelty.
> Velvette is not misogynistic per se but she despises weak women who can't fight for themselves. That's why other Vs behavior don't bother her, she doesn't feel threatened by their aggression.
> Angel Dust has BPD and an eating disorder. That's why he fell for Valentino so terribly, to trust him with his soul. He used to think that Valentino is the only person fucked up enough to truly love him as damaged as he'd been. (More hc about Val and Angel here). Actually Val has a very similar backstory to him - a queer, gender non-conforming man in a very masculine environment (I'm not sure how canonic is Angel working for the Italian Mafia at this point but I stick to it until proven otherwise).
Other headcanos about Vox and Val ❤️🩵
#hazbin hotel#valentino#vox#Velvette#VoxVal#angel dust#Huskerdust#headcanon#ask#vox hazbin hotel#valentino hazbin hotel#hazbin hotel velvette
236 notes
·
View notes
Text
a lot of people like to begin and end their research into the possibility of endogenic systems existing by merely aggressively pointing to the DSM5 definition of dissociative identity disorder and using this to make some complex claims like:
"dissociative identity disorder is only ever formed by early childhood severe trauma, and so if you don't experience disordered symptoms of plurality, you don't have dissociative identity disorder, therefore you can't be a system."
however, if you ever bothered to look more into psychological literature, as you should before making grandiose sweeping opinionated claims with insufficient research backing, you'd know that the experience of plurality is actually, within the psychiatric community, discussed heavily.
there are plenty of paradigms where you can find things analogous in description to nondisordered, therapist-endorsed plurality, including therapeutic methods of engaging with oneself as plural as a means of Improving oneself: for example, Schema Therapy (often utilized with borderline patients and people with personality disorders), and Internal Family Systems (often utilized in general types of patients, whether or not they were severely traumatized as a child or even as an adult or adolescent)
as a side note, it's very anti-intellectual to have rabidly-held opinions that you bully people online about without even bothering to do a ton of research, especially into perspectives from academics that disagree with your personal very online opinions. any serious practicioner of psychology would be one who is open-minded and seeking to not Confirm a Theory but to learn and form new ideas based on what their clients can teach them.
it's also quite offensive towards survivors of psychiatric abuse to insist upon the psychiatric system of diagnostics as the end-all-be-all of one's existence, and it smells like major bootlicking to only ever allow oneself and others to be ~valid~ If an authority confirms it. it's not like the DSMs are these perfect encapsulations of everything ever that could happen psychologically, things are added and removed all the time, and those actions often accrue significant behind-the-scenes debate in the academic sphere, where people with write papers on why they think something should or shouldn't be there. remember, the DSM is simply supposed to be a Tool that Guides clinicians in order to help them distinguish certain phenomena from others, but at the end of the day not only is it Not supposed to focus on nondisordered manifestations of behaviors, but it's also not made to reductively simplify any active debate in psychiatry merely because one thing is canonized a certain way, just so you can be Right Online™
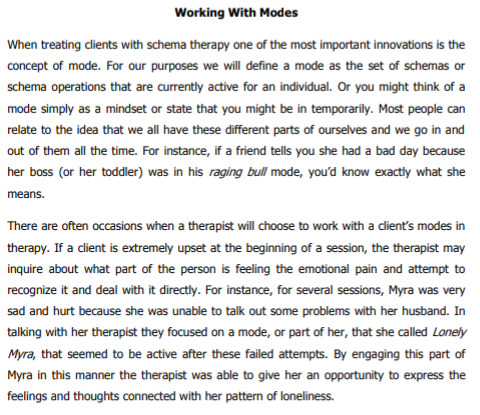
anyway. in schema therapy, schemas are said to be parts of people that hold certain typified negative self-belief systems, and patients are encouraged to both label them and speak to or as them, in order to convince their parts of new and more healthy or productive modes of thinking, rather than getting triggered into letting the schema take over and give them negative thoughts and emotional issues.
these parts are understood within the literature to be natural to everybody, because everyone compartmentalizes into belief + emotional structures like these; what makes them 'not dissociative identity disorder' is merely the fact that these parts do not cause amnesia when taking over the core self, and that they are often identified as 'parts' of the primary person, rather than fully separated other people with distinct consciousnesses. nonetheless, this is one of many examples of the parts work methodology wherein the self is casually understood to be multiple or have subpersonalities or parts within psychological literature, and that fact is then taken towards the conclusion of using this experience in a healing-oriented way.
here is an example of schema therapy, an excerpt of A Client’s Guide to Schema Therapy by David C. Bricker, Ph.D. and Jeffrey E. Young, Ph.D. who are from the Schema Therapy Institute;
moving on, there is my other example: internal family systems. in IFS, clients are encouraged by their practitioner to personify and then actively dialogue with their various emotional states and common modes, and also to look for particular styles of parts already well-known by the IFS paradigm such as 'firefighters' and 'managers,' which are two different kinds of protector parts. with IFS becoming popularized nowadays, more and more laypeople are now becoming comfortable with the idea that they have psychological parts, which can be parts of their personal Self or parts that exist within them and hold certain emotional functions, despite perhaps not experiencing the typical heavy dissociative states definitive of disordered types of multiplicity like DID.
here are some excerpts from a book called The Others Within Us, by Robert Falconer, with a foreword by Dick Schwartz, the founder of IFS, as well as many high praise reviews from members of the psychiatric community for his writing, which breaks new grounds and is very in-depth and thorough.
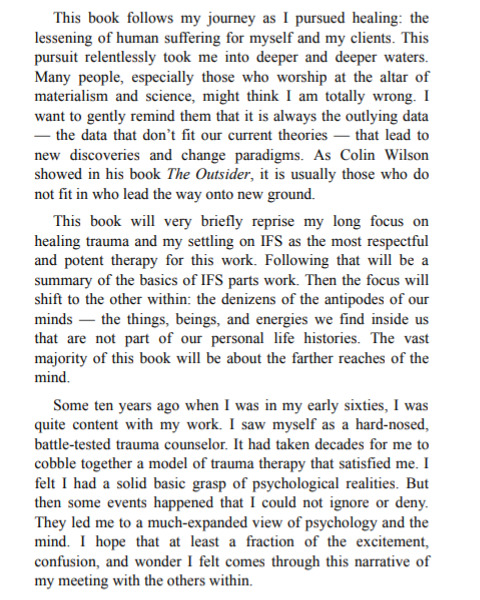
here he discusses needing to have an open mind towards phenomena that are not well-studied yet, and learning to humble himself in order to do so even as a trained clinical trauma counselor in his 60s and 70s at the time of studying and eventually writing this book.
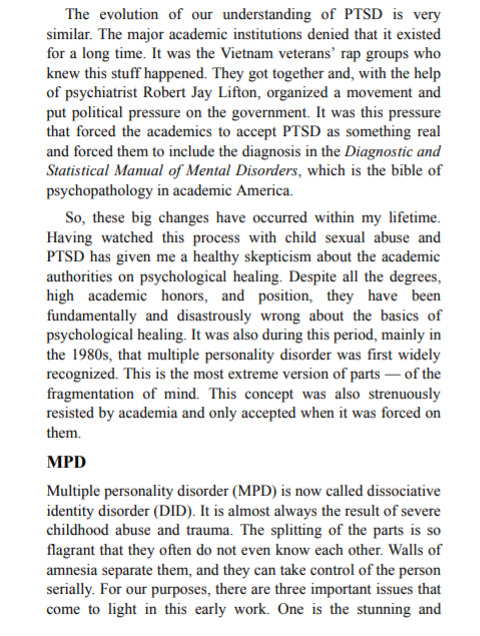
first of all, take note of his discussion of the contestation of even PTSD when they were trying to get it canonized in the DSM. an entire movement including political pressure had to be formed just to get ptsd into the literature. nowadays nobody on this website would (hopefully) contest the validity of ptsd as an experience people could have, but back then, people had to hold their ground against the psychiatric system and even the government just to prove that their experiences deserved to be taken seriously. don't think that this was the olden days either, because the academic world still tends to hold tight to its current state and not be welcoming towards experiences outside its own paradigms, so its good to keep in mind that there are histories and politics going into the making of all this psychological literature, with more room yet for even further and more uncommon experiences to be discussed.
second of all, note that he says that to clinicians working even with people with MPD/DID, it became apparent that the parts structure could be normal for people, beneficial, and even healthy, and that it was simply the severely dissociative aspects of it that they would work to heal, rather than viewing the entire experience of plurality as inherently disordered or solely a product of trauma.
i hope its clear by now that there's a lot of discussion surrounding this issue, but that plenty of it involves the normalization of nondisordered plurality, that plurality can be even healthy and a good, therapist-approved means of self-exploration for people, and that you should not cherry-pick literature while using intellectually dishonest argument techniques online.
endos are valid imho. i myself am a dissociative system, but at least i don't claim that my opinion is the standard opinion based on just that, i actually try to do my research. hopefully this was interesting to you, and please don't discourse on my post. kthxbai
#syscourse#dissociative identity disorder#did system#traumagenic system#endogenic system#actually multiple#original post
20 notes
·
View notes
Text
Hey, so I know people want to help their friends and stuff, but it can actually be really harmful when someone has told you that they don't have an illness or disorder, and you continuously push the idea that they do, in fact, have that illness or disorder. Some illnesses and disorders share a lot of symptoms! PTSD and Autism are a great example because even clinicians can misdiagnose these for one another, meaning your average Joe would have a difficult time trying to diagnose, say, their friend without proper training and education.
Suggesting something is perfectly fine, but as I mentioned, pushing your diagnosis of someone else onto them, especially when they seem very resistant and disagree, is not always helpful or respectful. Sure, someone may be in denial of a diagnosis; that is their problem, and they will need to come to terms with it on their own. Suggesting someone might have something, especially if they ask for your advice or opinion, is more than ok - in fact, I encourage getting second opinions if you're unsure about something - but please do not force what you've decided is the truth onto someone who is extremely unwilling. If the same were repeatedly done to you, you may not appreciate it either.
Obviously, it is more than ok to want to help a loved one get the treatment and diagnosis that they need, but please, PLEASE remember that you are also most likely not a clinician/physician, and while self-diagnosis is totally valid and understandable, diagnosing someone else is a little bit not.
#reminder#i have had people do this to me constantly#when i know they are mistaking something for something else#you know your own body and mind better than anyone#please trust others to know themselves at least somewhat as well#and if they are in denial then that is not your problem to solve#just felt this needed to be said because this has happened multiple times now#and I'm a little exhausted from it now
22 notes
·
View notes
Note
do you have opinions on cbt
Hahaha everyone has opinions on CBT. For the radical queer trauma therapist circles I run in I’m actually pretty pro-CBT. For the average person involved in mental/behavioral health, I’m probably anti-CBT.
[For context, Cognitive Behavioral Therapy is a famously evidence based type of therapy which works by targeting thoughts/cognitions. It theorizes that thoughts cause behaviors which cause feelings which cause thoughts all around and around in a spiral of doom for which the easiest intervention is targeting the thoughts. It can be very regimented, hence it’s easily studied, hence why it’s so “evidence based.” You basically identify “cognitive distortions” like catastrophizing (I failed my exam and so I’m going to fail out of school and live in a cardboard box) and reality-check them (it’s one exam in one class and I can still pass the class if I get a decent grade on my final). You also identify the thought/feeling/behavior spiral (thought=I failed -> I will be homeless, feeling=fear, shame, behavior=avoiding the professor and anything associated with the class.) It’s definitely bigger and more complicated than that, but you get the idea.]
For a lot of people with anxiety and with OCD especially, it can be so life changing.
For a lot of people, especially people who are trauma survivors or whose presenting problems are connected to trauma, it can feel like gaslighting.
(Fun fact! Part of the reason TF-CBT (trauma focused CBT) has such solid evidence behind it is that it ignores the wild survival bias in its studies. People who have a lot of trauma or really intense PTSD tend to drop out. Those who stay mostly have success with it and provide happy little data points)
I think certain parts of CBT can be so useful – noticing thoughts, identifying cognitive distortions, checking in with reality – and I think using the triangle with clients (the little triangle of “thoughts,” “emotions,” “behaviors”) can be super useful, and I do it fairly often.
Personally, I find a lot of my clients can do (most of) the mental/cognitive work on their own – what they really need help with from a trained professional is actually a felt sense of safety and emotional processing which require therapeutic flexibility and other modalities -- and a longer period of work.
Some people like a very concrete, structured approach, especially if they’re new to therapy or skeptical of the value of therapy. Also, a lot of people only can access therapy for a short time and a lot of people only want to be in therapy for a short time, and you can make changes quickly with CBT. Also, from the therapist end, there are a million free CBT trainings and workshops you can do vs. most other modalities where you have to pay $1000s for trainings (on top of getting a graduate degree).
Insurance companies and payers in general LOVE CBT because it’s structured, evidence-based, and short-term. You also require clients to do homework, which is basically like extra therapy time you don’t have to pay the clinician for. You can also train people in it pretty easily. I think it’s important to understand *why* CBT is held up as the best/standard therapy type now, and it has a lot less to do with CBT itself and more to do with service provision and structural factors around paying for therapy and with what can be effectively researched.
I’m reading Richard Schwartz’s “No Bad Parts” right now about Internal Family Systems therapy, and I’m now thinking of CBT within that framework. Basically, CBT is an effective part of the overall therapy system but it’s being asked to do too much, and so is overfunctioning and causing problems. We really should just let it settle into its own niche.
It’s not my therapy niche! But it has a place.
(If you were asking about Cock and Ball Torture therapy that would probably fall under the category of “experiential” therapy. Not sure it’s really been studied, but I’m sure there would be enthusiastic participants.)
48 notes
·
View notes
Text

Random Headcanon: Even prior to relying so heavily on tactile methods due to lack of vision, Eden was exceptionally skilled at myofascial trigger point release / injections and was probably gently herded into a DO degree instead of an allopathic school both due to this and his nontraditional + ruralmed background.
This also means he gives a killer neck and back massage and he will sit / kneel on your back to reach if he needs leverage.

#| clinician's opinion :: facts |#| also means if Eden had lived / been allowed to finish his schooling he would have been a classic rural med doc#putting out fires with no resources and accepting barter when insurance won't cover#can't change my mind |
2 notes
·
View notes
Text

Eden is not often too bitter about losing his vision - he also died and it didn't really take, so he feels he could be worse off. Maybe it will come back eventually, missing eye notwithstanding.
However.
Sometimes ' I have no idea what [ friend / loved one ] looks like ' hits him really hard.
1 note
·
View note
Text
I have opinions about a post (https://www.tumblr.com/justanothersyscourse/715275783016448000/looks-like-the-tulpa-studies-might-finally-be).
🗝️🏷️ psychosis, invalidation, syscourse? (It’s a link to an anti-endo review of a study, with my endo-neutral commentary)
The reblog options makes it huge, and I care more about the bottom highlighted part. I look forward to finding the whole study, but I want to share strategies I use for reading academic papers.
Things to keep in mind:
Clinicians and researchers typically don’t have lived experience. They can learn from formal education or people who do have whatever they’re looking at, but can take many years to communicate in community (system-specific social settings) spaces effectively, if they ever get to that point.
Language develops separately in different contexts. There are barriers on both sides that prevent conversation; psychologists don’t know community terms, and the community doesn’t know how to decode academic phrasing.
Some researchers are snooty. There are professionals that approach community members believing they are lying, wrong, or confused. Words like “experience” and “feel” are used, both to make the professional appear more neutral and to imply unreality. Plenty of papers on DID also say things like “The patient experiences herself as a young child” when admittedly describing what the community calls “littles”.
This doesn’t mean that the study will prove anything either way. I haven’t seen the abstract, but it looks like they’re trying to reject or fail to reject that tulpas (among other audial experiences) are symptoms of psychosis. I can’t really tell what their base hypothesis was, but science doesn’t actually prove anything; it explains, it experiments, it observes, but it cannot definitively say that something is fact. Even things we’re pretty sure about, like gravity, can’t be known for certain. I have no personal investment in this study either way, but I do believe that harassing people is not okay — including people who are spreading harm. I have yet to see an endogenic system cause harm solely due to their identity as endogenic. Misinformation and poor etiquette suck, but there are methods to try before harming people back.
🗝️🏷️ same but also mild RAMCOA mention
(I also don’t understand why the willing creation of other selves is bad aside from the name “tulpamancy”, especially as a member of a traumagenic system that still splits somewhat intentionally. Is it different cause we were forced to do it? Or just because we have trauma? I will not accept being called bad for surviving as a small child, so why are they different?) - 🪡
49 notes
·
View notes
Note
DROP YOUR DX FOR VOX !!!!! Please and thank you.
I would like to preface all my posts on headcanons related to psychology and mental illness with a disclaimer: diagnosing mental conditions, especially personality disorders, can be extremely challenging. It's a complicated process that relies heavily on a psychologist's interpretation of facts, making it susceptible to biases. Personality disorders cannot be diagnosed based on surface-level observations and are not just labels that we can assign to people like in the case of MBTI. Additionally, I am not a clinician with any expertise in diagnosing people. Therefore, the following post should not be taken as a reliable professional opinion. It's simply my interpretation of the internal mechanisms that may be responsible for the behavior of certain characters in my fan fiction. Furthermore, I want to make it clear that I have no intention of stigmatizing people with personality disorders by associating them with villains. A personality disorder does not determine someone's character or make them a bad person. Some characters may be evil because of the choices they make, not as a result of their mental conditions.

(I've already posted some stuff here so I'm not going to repeat myself.)
Okay, so, Vox has Narcissistic Personality Disorder (NPD). It's crucial to distinguish this from "common narcissism" (people often described as "narcissists" by others just because they are egotist assholes; kinda ableist, you shouldn't do it because it's extremely stigmatizing towards people suffering with actual NPD) . While those individuals typically function well, those with NPD exhibit all the traits – grandiosity, egocentrism, attention-seeking, intense power fantasies – but as it's a disorder, these traits lead to inflexible and maladaptive patterns of behavior and cognition.
NPD has its roots in intense feelings of shame, low self-compassion, and self-loathing. In my interpretation, Vox has always felt inadequate. His father inherited an enormous amount of money, establishing a media conglomerate in the 20's. Vox's mother, captivated by the world of movies, used them to escape her reality as a trophy wife. Despite her dreams of becoming an actress, Vox's father, possessive and protective, prevented her entry into the entertainment industry. As a compromise, he made their son a child actor, with the condition that it would be temporary. When Vox grew older, he was expected to transition to learning business and other skills, ultimately to take over the family's empire.
So, Vox was never enough for either of his parents. His father thought of him as annoying and unserious due to his talkativeness and exaggerated behaviors, attributing it to growing up surrounded by actors. As for his mother... Vox turned out to be a terrible actor, struggling to convey emotions that weren't bombastic and over-the-top. Being a teenager is humiliating enough, but imagine being a teenager bad at something and forced to do it for a worldwide audience, when the whole production crew is annoyed with you. Fortunately, he grew up to be devilishly handsome (not to be a simp, I just believe someone must be handsome to endure the ethereal punishment of having their face swapped for a TV screen) and entertaining, leading them to make him a TV host and media personality.

Anyway, NPD is all about creating a perfect self and projecting it to the world when you're deeply ashamed of your true self. It means that, no matter what you're doing, you're constantly concerned about how it looks to other people. You constantly play an exhausting game, trying to win gold stars of social admiration for every-fucking-thing, guided by superficial ideals of wealth, perfection, beauty, and, above all, power. One reason Alastor's existence bothers Vox so much is the fact that he cannot comprehend the idea of someone choosing radio over his "objectively better and correct" medium. Vox lacks the ability to understand nuanced sentiments, which ironically makes him thrive in Hell. In this anarchocapitalist, lawless society, survival of the fittest prevails, and this is a game he excels at playing.

Generally, the best approach for individuals with NPD is to pull them out of delusional thinking by confronting their beliefs about the world and themselves with reality (it should be performed by qualified therapist, especially when someone hasn't completed any kind of therapeutic process yet). However, in Hell, Vox's behavior was no longer in violation of social norms; on the contrary, it was highly rewarded. Consequently, he completely lost his shit, became unhinged, and began acting on all his previously suppressed urges. He finally fulfilled all narcissistic power fantasies and became (almost) untouchable. Now, he's ready to kill anyone who questions him, seeing it as threatening to his fragile image of the perfect self.

He exhibits strong bipolar tendencies. Most of the time, he's power-tripping in a semi-maniacal state. Periodically, he undergoes deep, depressive episodes, locking himself up in his apartment and avoiding interaction.
Constantly guarding this fragile image of the perfect self that he built is exhausting. The bigger this image gets, the more fragile it becomes, like a house of cards. And guarding it becomes more and more exhausting. But there's nothing scarier than the idea of the facade falling apart and people seeing him as he is: imperfect and vulnerable, damaged and ashamed, rotten and evil. Deep down, he knows he's unlovable, and it hurts. He knows that true love exists; he craves this ultimate form of admiration and devotion, but it requires vulnerability and honesty, which he's not capable of. He's only vulnerable with Valentino, and only occasionally when he's intoxicated or when Val fucks every last thought out of his body. He's very much a controlling top insecure about his masculinity, so the latter happens rarely.

Also, drugs. Oh, do this man enjoy some coke. Other drugs and booze, not so much; they make him feel less in control. But getting coked up, going out, causing a scene, killing some poor souls, and relishing this feeling of being completely untouchable? Feels so good.
When it comes to Alastor, he hates him because he's jealous. Despite all his efforts—building a perfect persona, a perfect company, perfect entertainment—this stinky, outdated, and boring radio demon gets so much attention and admiration that should be his. Moreover, he feels that Alastor can see right through his bullshit. He's so paranoid about it that he's almost certain Alastor knows about his childhood traumas, about his death, about all his truths, and could one day broadcast it for all people of Hell to hear. So, he needs him dead.
Note: these headcanons (especially Vox's past) are very important part of my fanfiction. Please feel free to use them in your fics but I'll appreciate if you tag me 🩷
Velvette hc | Valentino hc | Vees + Angel hc | VoxVal hc
#vox#vox hazbin hotel#Valentino#valentino hazbin hotel#voxval#staticmoth#headcanon#character analysis#ask
337 notes
·
View notes
Note
I’m currently on Dr Lorimer’s (GenderCare) waiting list for an assessment for a diagnosis of gender dysphoria and then hopefully top surgery. This goes for anyone who can refer for surgery, but it’s stated on his website that you have to be “psychically and psychologically stable” to be referred.
I’ve currently been diagnosed with borderline traits, but my psychiatrist and I are discussing a full diagnosis of BPD. I have numerous diagnosed anxiety disorders as well, along with ASD.
What’s the likelihood of me being refused treatment for being “psychologically unstable”? I’ve been fully socially transitioned for 3 years straight, no waverings in my opinion that I am trans. I know for a fact that my other mental health diagnoses have no bearings on what treatment I want, but I’ve had such bad experiences with healthcare professionals in the past that I have an unwavering anxiety I will be refused treatment.
Can anyone with a personality disorder share their experience of going through the trans healthcare conveyer belt? With any gender specialist. The PD is mostly what I’m worried about, considering the stigma around it. Would it be wise to hold off on getting the full PD on my record until after I get surgery? All of my diagnoses are on my GP record so they’re not hard to hide anymore.
Thank you!
Hi Anon,
This is just a general statement that clinicians make when diagnosing GD.
Everyone is assessed for their mental stability and understanding of GD.
All they are looking for is stability in your feelings of GD and what detrimental impact this has had on your life. As long as you can express your unwavering feelings of GD and talk about the ways in which you have changed your life to live in your chosen gender and the positive impact this has on you, you should be fine.
Always be truthful about your mental health with your clinician, as covering up things will later trip you up and may result in them questioning your ‘capacity’ to go through treatment.
2 notes
·
View notes
Text
Carl Gustav Jung (1865-1961) was a Swiss psychiatrist and psychotherapist who founded analytical psychology. Jung proposed and developed the concepts of extraversion and introversion; archetypes, and the collective unconscious. The central concept of analytical psychology is individuation - the psychological process of integrating the opposites, including the conscious with the unconscious, while still maintaining their relative autonomy. Jung considered individuation to be the central process of human development. Though he was a practising clinician and considered himself to be a scientist, much of his life's work was spent exploring tangential areas such as Eastern and Western philosophy, alchemy, astrology, and sociology, as well as literature and the arts. Jung's interest in philosophy and the occult led many to view him as a mystic, although his ambition was to be seen as a man of science.
[..] It is a common and totally unjustified misunderstanding on the part of scientifically trained people to say that I regard the psychic background as something "metaphysical," while on the other hand the theologians accuse me of "psychologizing" metaphysics. Both are wide of the mark: I am an empiricist, who keeps within the boundaries set for him by the theory of knowledge.
[..] As a psychologist, I am not qualified to contribute anything useful to the question of the physical reality of Ufos. I can concern myself only with their undoubted psychic aspect, and in what follows shall deal almost exclusively with their psychic concomitants.
[..] To believe that Ufos are real suits the general opinion, whereas disbelief is to be discouraged. This creates the impression that there is a tendency all over the world to believe in saucers and to want them to be real, unconsciously helped along by a press that otherwise has no sympathy with the phenomenon. This remarkable fact in itself surely merits the psychologist’s interest. Why should it be more desirable for saucers to exist than not?
[..] I know that, just as before, my voice is much too weak to reach the ear of the multitude. It is not presumption that drives me, but my conscience as a psychiatrist that bids me fulfill my duty and prepare those few who will hear me for coming events which are in accord with the end of an era. As we know from ancient Egyptian history, they are manifestations of psychic changes which always appear at the end of one Platonic month and at the beginning of another. Apparently they are changes in the constellation of psychic dominants, of the archetypes, or "gods" as they used to be called, which bring about, or accompany, long-lasting transformations of the collective psyche.
This transformation started in the historical era and left its traces first in the passing of the aeon of Taurus into that of Aries, and then of Aries into Pisces, whose beginning coincides with the rise of Christianity. We are now nearing that great change which may be expected when the spring-point enters Aquarius. It would be frivolous of me to try to conceal from the reader that such reflections are not only exceedingly unpopular but even come perilously close to those turbid fantasies which becloud the minds of world-reformers and other interpreters of "signs and portents." But I must take this risk, even if it means putting my hard-won reputation for truthfulness, reliability, and capacity for scientific judgment in jeopardy. I can assure my readers that I do not do this with a light heart. I am, to be quite frank, concerned for all those who are caught unprepared by the events in question and disconcerted by their incomprehensible nature. Since, so far as I know, no one has yet felt moved to examine and set forth the possible psychic consequences of this foreseeable astrological change, I deem it my duty to do what I can in this respect. I undertake this thankless task in the expectation that my chisel will make no impression on the hard stone it encounters.
[..] Certain objects are seen in the earth’s atmosphere, both by day and by night, which are unlike any known meteorological phenomena. They are not meteors, not misidentified fixed stars, not "temperature inversions," not cloud formations, not migrating birds, not aerial balloons, not balls of fire, and certainly not the delirious products of intoxication or fever, nor the plain lies of eyewitnesses. What as a rule is seen is a body of round shape, disk-like or spherical, glowing or shining fierily in different colours, or, more seldom, a cigarshaped or cylindrical figure of various sizes. It is reported that occasionally they are invisible to the naked eye but leave a "blip" on the radar screen.
The round bodies in particular are figures such as the unconscious produces in dreams, visions, etc. In this case they are to be regarded as symbols representing, in visual form, some thought that was not thought consciously, but is merely potentially present in the unconscious in invisible form and attains visibility only through the process of becoming conscious. The visible form, however, expresses the meaning of the unconscious content only approximately. In practice the meaning has to be completed by amplificatory interpretation. The unavoidable errors that result can be eliminated only through the principle of "waiting on events"; that is to say we obtain a consistent and readable text by comparing sequences of dreams dreamt by different individuals. The figures in a rumour can be subjected to the same principles of dream interpretation. If we apply them to the round object – whether it be a disk or a sphere we at once get an analogy with the symbol of totality well known to all students of depth psychology, namely the mandala (Sanskrit for circle).
This is not by any means a new invention, for it can be found in all epochs and in all places, always with the same meaning, and it reappears time and again, independently of tradition, in modern individuals as the "protective" or apotropaic circle, whether in the form of the prehistoric "sun wheel," or the magic circle, or the alchemical microcosm, or a modern symbol of order, which organizes and embraces the psychic totality. As I have shown elsewhere, in the course of the centuries the mandala has developed into a definitely psychological totality symbol, as the history of alchemy proves.
[..] In so far as the mandala encompasses, protects, and defends the psychic totality against outside influences and seeks to unite the inner opposites, it is at the same time a distinct individuation symbol and was known as such even to medieval alchemy. The soul was supposed to have the form of a sphere, on the analogy of Plato’s world-soul, and we meet the same symbol in modern dreams. This symbol, by reason of its antiquity, leads us to the heavenly spheres, to Plato’s "supra-celestial place" where the "Ideas" of all things are stored up. Hence there would be nothing against the naïve interpretation of Ufos as "souls." Naturally they do not represent our modern conception of the psyche, but give an involuntary archetypal or mythological picture of an unconscious content, a rotundum, as the alchemists called it, that expresses the totality of the individual. I have defined this spontaneous image as a symbolical representation of the self, by which I mean not the ego but the totality composed of the conscious and the unconscious. I am not alone in this, as the Hermetic philosophy of the Middle Ages had already arrived at very similar conclusions. The archetypal character of this idea is borne out by its spontaneous recurrence in modern individuals who know nothing of any such tradition, any more than those around them.
[..] If the round shining objects that appear in the sky be regarded as visions, we can hardly avoid interpreting them as archetypal images. They would then be involuntary, automatic projections based on instinct, and as little as any other psychic manifestations or symptoms can they be dismissed as meaningless and merely fortuitous. Anyone with the requisite historical and psychological knowledge knows that circular symbols have played an important role in every age; in our own sphere of culture, for instance, they were not only soul symbols but "God-images." There is an old saying that "God is a circle whose centre is everywhere and the circumference nowhere." God in his omniscience, omnipotence, and omnipresence is a totality symbol par excellence, something round, complete, and perfect. Epiphanies of this sort are, in the tradition, often associated with fire and light. On the antique level, therefore, the Ufos could easily be conceived as "gods." They are impressive manifestations of totality whose simple, round form portrays the archetype of the self, which as we know from experience plays the chief role in uniting apparently irreconcilable opposites and is therefore best suited to compensate the splitmindedness of our age.
It has a particularly important role to play among the other archetypes in that it is primarily the regulator and orderer of chaotic states, giving the personality the greatest possible unity and wholeness. It creates the image of the divine-human personality, the Primordial Man or Anthropos, a chên-yên (true or whole man), an Elijah who calls down fire from heaven, rises up to heaven in a fiery chariot, and is a forerunner of the Messiah, the dogmatized figure of Christ, as well as of Khidr, the Verdant One, who is another parallel to Elijah: like him, he wanders over the earth as a human personification of Allah.
Gisela von Frankenberg: Nommo (1981), Blaue Blume (1990)
The present world situation is calculated as never before to arouse expectations of a redeeming, supernatural event. If these expectations have not dared to show themselves in the open, this is simply because no one is deeply rooted enough in the tradition of earlier centuries to consider an intervention from heaven as a matter of course. We have indeed strayed far from the metaphysical certainties of the Middle Ages, but not so far that our historical and psychological background is empty of all metaphysical hope. Consciously, however, rationalistic enlightenment predominates, and this abhors all leanings towards the "occult." Desperate efforts are made for a "repristination" of our Christian faith, but we cannot get back to that limited world view which in former times left room for metaphysical intervention. Nor can we resuscitate a genuine Christian belief in an after-life or the equally Christian hope for an imminent end of the world that would put a definite stop to the regrettable error of Creation. Belief in this world and in the power of man has, despite assurances to the contrary, become a practical and, for the time being, irrefragable truth. This attitude on the part of the overwhelming majority provides the most favourable basis for a projection, that is, for a manifestation of the unconscious background.
Undeterred by rationalistic criticism, it thrusts itself to the forefront in the form of a symbolic rumour, accompanied and reinforced by the appropriate visions, and thus activates an archetype that has always expressed order, deliverance, salvation, and wholeness. It is characteristic of our time that the archetype, in contrast to its previous manifestations, should now take the form of an object, a technological construction, in order to avoid the odiousness of mythological personification. Anything that looks technological goes down without difficulty with modern man. The possibility of space travel has made the unpopular idea of a metaphysical intervention much more acceptable. The apparent weightlessness of the Ufos is, of course, rather hard to digest, but then our own physicists have discovered so many things that border on the miraculous: why should not more advanced star-dwellers have discovered a way to counteract gravitation and reach the speed of light, if not more? Nuclear physics has begotten in the layman’s head an uncertainty of judgment that far exceeds that of the physicists and makes things appear possible which but a short while ago would have been declared nonsensical. Consequently the Ufos can easily be regarded and believed in as a physicists’ miracle.
[..] Should it be that an unknown physical phenomenon is the outward cause of the myth, this would detract nothing from the myth, for many myths have meteorological and other natural phenomena as accompanying causes which by no means explain them. A myth is essentially a product of the unconscious archetype and is therefore a symbol which requires psychological interpretation. For primitive man any object, for instance an old tin that has been thrown away, can suddenly assume the importance of a fetish. This effect is obviously not inherent in the tin, but is a psychic product.
-- C. G. Jung, Ein moderner Mythus: Von Dingen, die am Himmel gesehen werden (1958)
Sunday, December 3, 2023
5 notes
·
View notes
Text
To anyone this helps: I literally do autism research at the place where autism was defined, and I work with people who are consults for the ASD portion of the DSM. I am also autistic.
I can attest that the people who are deep into this research support the fact that autistic people know themselves best. They (and I) are quite supportive of self diagnosis. Current data supports that nearly 3% of people are autistic—that’s a HUGE number. Given the problems with prior diagnostic criteria and the inequitable ways it has been applied for so many decades, it’s entirely reasonable that an extremely large proportion of the population was missed and is on a journey of late discovery.
This isn’t to say never to trust your psychologist/therapist/etc., but unfortunately, clinical practice is often years if not decades behind what the research is screaming from the rooftops. It doesn’t help that autism has been politicized and polarized as a topic, either. But if you find autism resources are helpful for you—use them. Self-diagnose if you have done the research; you know YOU best.
And most importantly, even to the kids self-diagnosing off a single TikTok—there’s probably a reason. They’re probably going through something, and no matter what, the process of learning more about neurodivergence will inevitably lead them to the right place.
So, yeah. Not all of these licensed professionals actually know what they’re talking about on this topic, especially when it comes to adults. And if you’re being shut down by a clinician, don’t lose hope—if it is meaningful to you, seek a second opinion. If you have the means, find a clinician who explicitly states they’re up to date on the current DSM and is aware of disparities in diagnosis—someone remote if you need to. And if you don’t have the means, keep engaging in the autism community. We want you here 💛
a while ago i attended this lecture on autism. guy in the audience said he had many of the symptoms that were presented and asked what should he do to get treatment and possibly a diagnosis. instead of answering his question the psychologist went on a tangent about how “the clinic reigns all powerful over guesswork”, and how actually it has become a trend amongst little children on the internet to claim that they are autistic for cool points, and that this hurts real autistic people. no she didn’t tell him how to get his symptoms looked into, she just made it very clear that to her, aknowledging your own symptoms is bad and evil and hurts the poor real mentally ill people.
an ex-friend of mine, then a psychology major and by now probably a full psychologist, once lectured me on how horrible and bad it was that i told her “i probably have some sort of neurodivergency”, and that if i were her patient she would never give me a diagnosis because “you aren’t like this now, but i know that if you get a diagnosis you’ll use it as an excuse to start treating people badly. that’s just how mentally ill people are.”
same ex-friend was extremely disgusted when she found out that fans sometimes make neurodivergency headcanons for characters that have the same symptoms as they do, and that authors sometimes write books with neurodivergent protagonists in stories that don’t focus on that (ex: she seemed horrified that percy jackson has adhd?)
multiple psychologists i’ve seen on facebook agree that they should refuse to treat patients that say “i’m here because i have symptoms of a disorder and wonder if i have it”, and that a patient should arrive to a psychologist as a blank slate.
school psychologist asked me how i was feeling about my trauma situation and i told him i thought my friends would leave me. instead of addressing the issue he said that that no i didn’t, that i was lying, that i had searched “bpd symptoms” online and now i was faking symptoms because i wanted to have bpd, that he shouldn’t have told me he suspected i had a personality disorder because now look what was happening. no, i didn’t search bpd symptoms online. yes, my friends left me, it was a completely founded belief and not a symptom, let alone a faked symptom.
so the next time you hear someone saying they’re “anti self-diagnosis” i want you to understand what they’re saying. what they’re saying is:
- i don’t want people to be aware of their own symptoms
- i don’t think my patients should have access to any information that doesn’t come from me
- i don’t think neurodivergent people should learn how to cope with their symptoms and live “normal” lives
- i think neurodivergent people should be denied a diagnosis because the moment they get one they will become evil and dangerous
- i don’t think people who don’t look like a stereotype could possibly be neurodivergent, even if they have all the symptoms, so i think they are faking it for attention and should be denied treatment
#trying to stay vague because tumblr is my anonymous space and I like not being perceived lmao#but it is very interesting seeing this huge and growing chasm in research and clinical work#not that all research is perfect but it’s getting better very quickly which is very encouraging actually#neurodivergence babey
102K notes
·
View notes
Text
Eden has two types of crushes they are very soft / tentative affection and ' crushing and so, so mad about it '
3 notes
·
View notes
Text

Eden doesn't think he's a real or entire person because he's not a living person and he doesn't really talk about that unless pressed, and I need to sit down and explore that in threads more often. Ramifications of this include:
Unable to understand when someone puts themself in danger by defending him from a physical threat
Very confused when people ask him for an opinion
Wouldn't be able to recognise his own face in mirrors if he could see
Generalised depersonalisation / ' my physical form feels incorrect / defective ' things
0 notes