#<- not actually anti endo but please if you are one give me ONE doctor or scientist that has publically stated SOMETHING
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Women make up for the other 50% of Tumblr’s audience.
Text
like there has got to be at least one doctor out there that says endogenics are fake right??
there's ones that argue DID isn't even a real thing there's some out there that argue against endogenics openly and actively?? right??
#tagging this with stuff because oh my god#anti endo#<- not actually anti endo but please if you are one give me ONE doctor or scientist that has publically stated SOMETHING#because astro has not even TRIED and its lowkey FRUSTRATING#preferably ones that mention endogenic systems by name and fakeclaim them / say they can't exist at all directly#not just doctors that say DID is a thing and its only trauma based and say nothing about plurality outside of that#like syscourse has existed for a few years in public spaces at least one doctor has probably said 'endos r fake lol' on twitter or somethin#syscourse#systempunk#<- again tagging for reach since i wnat SOMEONE to give SOME proof of the other side of the argument#i KNOW its out there-#even if its not super good i still want it#or maybe itll be good and ill actually change my mind! see if you can try!
23 notes
·
View notes
Text
Changing mindsets, from a Real Anti Endo™️
The Release of the (Pro/Endo) Golden Goose
I hope everyone from all sides will give this important, heartfelt post a read.
It's likely something you'll want to be aware of if you have a vested interest in syscourse and the validity of endogenic systems. Please give this a chance.
It's been almost three years since I started my blogs. Wow. I've been on tumblr a hell of a lot longer, but I really wasn't involved in the system community. I started out firm and loud. I probably inadvertently fakeclaimed (I went into this with the rule that I would NOT directly tell anyone they were faking, it was a boundary that I knew would ruin me socially if I crossed it, but I'm sure I probably did without meaning to), I name called and made fun of people and things. I was disrespectful to people. I invaded tags to get my message out there, though I was quick to stop once I realized I was making the tags unusable for the community I claimed to want to protect.
I learned very quickly what was appropriate and what wasn't, what I could get away with and what I couldn't. It started to become a numbers game, influenced by the risk of the post.
I made a lot of friends and a lot of enemies, and I amassed a following of over 2k. More people have come and gone from my little community than I ever thought possible. People made fanart of me, and I cherish those so deeply. I have over 300 asks because I struggle to delete the ones thanking me.
And the more I was thanked, the nicer I got, the more thanks, the nicer I got, rinse and repeat until I had trouble NOT empathizing with pro/endos. The more I was willing to listen, the more legitimate sources I came across that disproved my original ideas about consciousness. The people sharing the sources were more respectful than I thought they'd be. Things were starting to look a bit cloudy.
I talked to my colleagues about how they, as therapists, would handle some of these endos in their practice, and while their belief in the concept varied, kindness and attempts to understand was the consistent answer. When had I lost that kindness and understanding that had driven me to that field to begin with?
Colleagues, yes. For those who don't know, I have a degree in social services and counselling (plus three other degrees). It's why the current situation with the antis turning on me is so funny. I still can't get into the mindset of some of these new anti endos, I just can't imagine justifying that level of cruelty. I had lines that I wouldn't cross, and I didn't think people could be worse than me.
... That might have been a trauma thing, looking back on it.
So I got desperate.
I spoke to the actual doctors who wrote some of these papers all of us are quoting. Everyone was arguing the meaning of the words, so I went directly to the source.
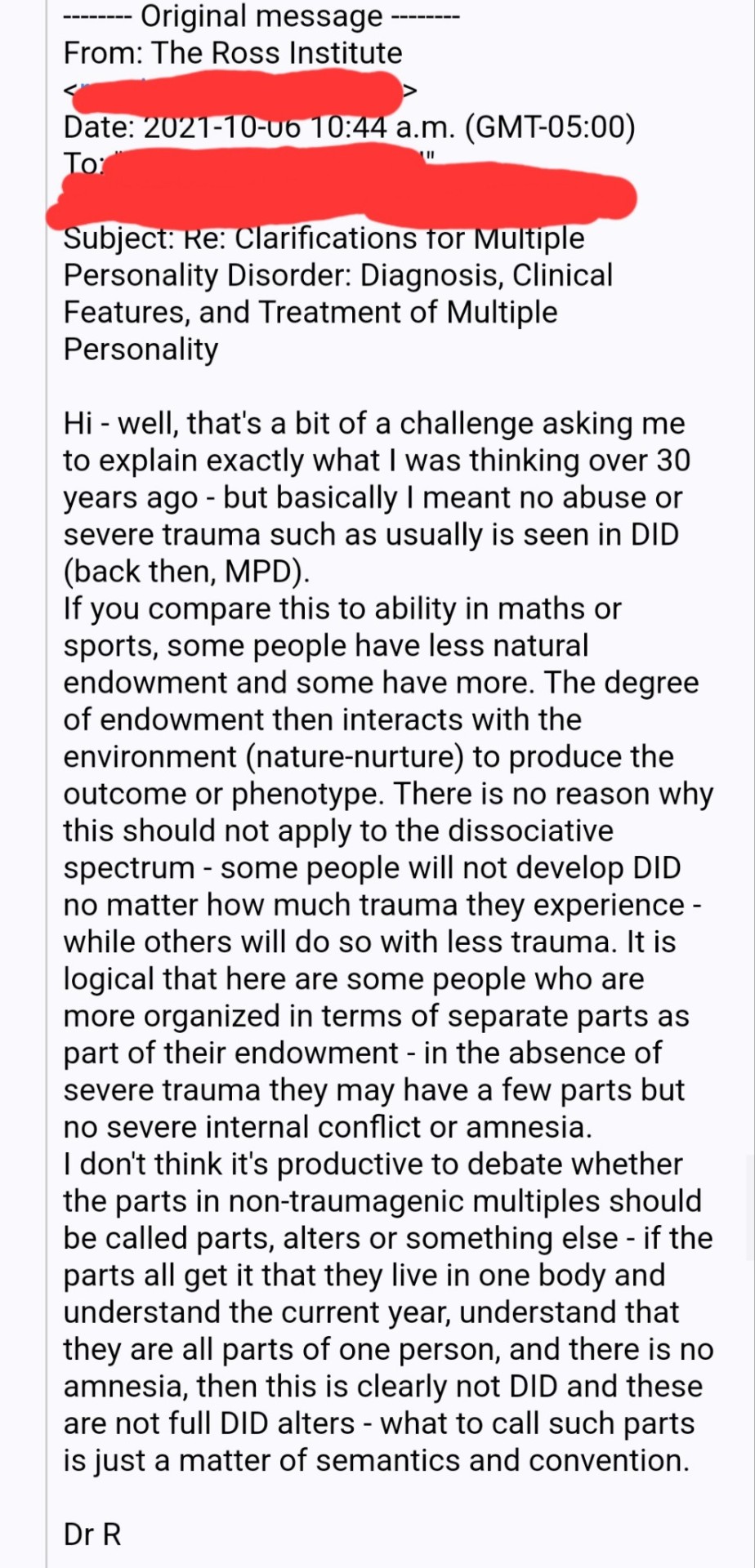
Dr Colin Ross, who wrote about endogenous multiplicity in the 80s. I told him everything-- about plurals, non-traumagenic systems, syscourse, what was being debated, how I and others interpreted his words, and what I wanted to learn.
Was plurality only trauma based?
And back and forth and back and forth we went, with me asking over and over again in different ways, NEEDING to hear that it was.
But I never got that answer. He meant what he meant. He said what he said and he meant it.
That plurality was not only found in the aftermath of trauma.
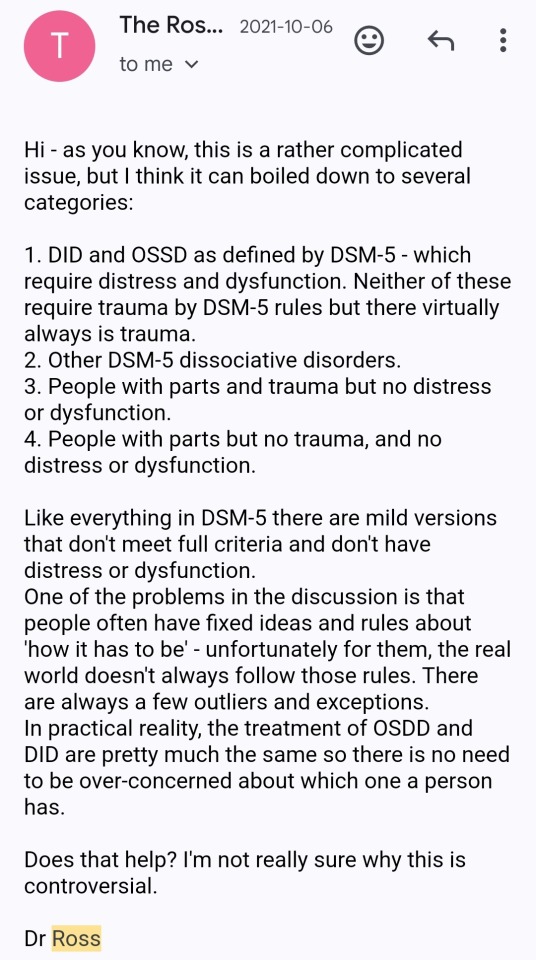
And I said nothing to anyone because I couldn't reconcile it.
Don't try to read between the lines, I assure you, there isn't some hidden meaning to be found there. I can't share all of the messages because some contained personal information, but my final response will tell you all you need to know.
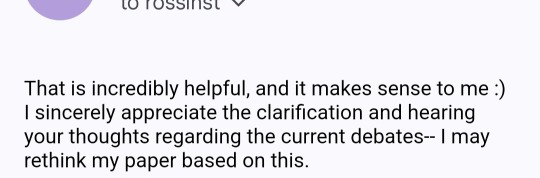
(It did NOT, in fact, make sense, and it took me three years to "rethink my paper" that endogenic plurality wasn't possible, I did not win that conversation, it was a dying stance that was not supported)
I've been accused of paying too much attention to my follower count, but I can't really help it. It's really scary when you make a post and see a sizeable drop. It means a lot of different things. My posts have less reach and support. I've upset people. I've done something wrong. My community is leaving me.
I'm in a weird spot, where I'm blocked by so much of the pro/endo community that I have nothing to join, and the anti endo community, who I still wholeheartedly support, continues to leave me for -checks smudged writing on hand- being too nice??
Misinformation about DID is a massive problem, and it's why I still consider myself anti endo and support that community. I relate to them in such a way that I'll always gravitate to and empathize with them.
Or at least, that's what I thought.
At this point, though, how can I not be pro/endo when Colin fucking Ross says it's possible?
I've already written about how I'm really struggling with these labels, and I love the people that have stuck around while I struggle to figure this out.
I hurt when I see the people that once supported me leave.
My (online) world is shrinking. Literally.
That's scary.
When you've watched so many turn away, you start to wonder, with every post, where is the line where the rest are going to leave? Is it this post?
I just want to be me, us, we want to laugh at the stupid crap people say, system or not, I want to talk about my disorder, I want to combat misinformation, I want to have productive, fun conversations about ideas and concepts with people who disagree and have different interpretations. I want to play devil's advocate and get people thinking. I want to be able to comment positivity and kindness on any post I see, I want to feel comfortable talking to more people about their ideas. I sympathize with anti endos, I relate to CDD systems, I still firmly believe that CDDs and plurality are different, unrelated concepts.
My priority will always and forever be the CDD community first and foremost.
However, I am a hypocrite. I have gone straight to the horse's mouth and failed. I've seen so much research that I finally get it. I'm grappling with holding on to this conversation with Dr Ross, wondering what harm I could have prevented if I'd gone public with these emails earlier.
Since when has being open to change been a bad thing?
Since when has showing respect to lived experiences been a bad thing?
What am I? What label describes this?
How do I go forward from here?
What are you going to do with this information?
I promise you, hate isn't the way forward.
#syscourse#not syscourse#pro syscourse conversation#anti endo#pro endo#anti plural#pro plural#debunk#endogenic safe#system safe#pro system
367 notes
·
View notes
Text
[Had an error when trying to post an ask. This is our attempt at a work-around.]

Anonymous asked: Could you please put that your pro-endo in your bio? Considering the main difference between antis and pros is that we define "all plurals" differently, it's not very clear what you meant, and I thought you were anti-endo until I went through every single one of your side blogs mentioned in your pinned post
-an anti-endo who loves your prompts, the newest prompts tags just took me off guard <3
As you have noted, We use the term "plural" in our posts and blog name, which is inherently inclusive/pro-endo and has been since its coining decades ago, so I am not going to honor this unnecessary request. I hate to be the one to tell you this, but if you're using "plural" in any sort of anti-endo or generally exclusionist way, you are using it incorrectly, since it originated as an inclusive alternative to terms that had more medical associations. I'm honestly offended that you thought I was part of the same group of exclusionists that has openly and repeatedly told me they want me dead, have sent me gore in response to a positivity post, recently invaded inclusive tags to spread hate, and regularly tell me to kill myself – hell, you yourself are admitting that you are against my right to self-determination if not my very existence, alongside my religious and spiritual beliefs (I don't have to tell you how this in particular is an asshole move, do I?), and believe that you somehow know what's going on inside my head better than I or even – at the very least, if you won't listen to me and the thousands of other endogenic systems about our own lives – the doctors actually studying endogenic plurality do, considering our endogenic origins. I will not block you so that you can see this response, but you are not welcome here. Here is a document full of sources about endogenic plurality existing and being recognized as a real and valid scientific phenomenon, not to mention how it is a cultural, spiritual, and religious practice found around the world; I hope you educate yourself and grow as a person. You seem to be trying to be polite, so I can only hope that you are just someone who has been horribly misinformed about pro-endos and endogenic systems.
However, at the same time, please understand that you are asking a blog with an inherently inclusive term in the title and all their posts, and a pinned post that clarifies yes, they do mean they support all systems (and advise those who don't support all systems not to interact), to put a separate warning in their bio that yes, they actually really do mean it when they say they support all systems. The thing is, I wouldn't have a problem with this request if it wasn't under this context. You yourself have admitted that you read my pinned post; how did you take the section that says all systems/plurals are welcome (and exclusionists like you are not) and somehow think it meant we didn't actually mean all? If you're excluding anyone from your definition of "all plurals" by adding little rules like "must be traumagenic", you don't mean all. You mean some. You, as an anti-endo, as an anti- certain plurals, only support some plurals. Someone who is against part of a community does not support all of a community; they only support the part of the community they are not against, which is only some of the community. This is how quantitative words work. Just because you have decided that the part of the community you personally choose to support and give basic respect to is the only "real" or "valid" part of the community doesn't mean the part you don't support stops existing or stops using the label you claim to support fully and without any restrictions or rules (since that is what supporting all of a community means); you don't actually support all plurals, and I'm concerned that you ever thought you did. I could break out a Euler diagram if it would make it clearer that only supporting some does not mean supporting all, and that supporting all does not mean supporting only a particular group. That's like saying you support all animals while being anti mammals and, at best, believing they're all actually confused and misguided birds – or, as I'll elaborate on in a moment, saying you support all queer people while being an aphobe who, at best, thinks aspecs are all just confused and misguided gays. That is not support, and you are certainly not giving your actual respect to all plurals. I say this delicately, but I don't think you should be participating in syscourse if you have trouble with the concept that excluding people from a label means not being inclusive of all people who use that label.
If a comparison will help you understand our response, especially the passive aggressiveness that I can admit is fully leaking through – this ask is essentially the same as how aphobes, during the years of "ace discourse", would occasionally react with surprise that queer blogs supported aspecs, despite aspecs being documented parts of and contributors to the queer community for decades, and queer being an inclusive term. In essence, "I know you're using an inclusive term that both historically and in the modern day includes people I hate, but I really thought you would agree with me that said marginalized group that I hate shouldn't exist, and that this community would be better off if they were all gone!" Meanwhile, aphobes were posting gore in the aspec tags, making fun of the murder of an asexual girl, spreading lies of pedophilia about anyone who showed support for aspecs, and telling aspecs that they were lying about the discrimination they've faced, that their sexualities were just trauma responses or mental illnesses, that they were broken and needed to be "fixed", that they were "stealing terms" and "making the community look bad", that they were making it all up for attention, or just straight-up to kill themselves. None of these examples are all too dissimilar from what I regularly see anti-endos saying and doing – some of them are the exact same save some of the specific words used by these bigots swapped out for more system specific ones. Just today I saw an anti-endo claim that pro-endos are "grooming children" just by being inclusive, like how aphobes claim aspec people are "grooming children".
Yes, I am aware this is harsh to hear. No, I am not going to apologize – your community and hatred is part of the reason we have traumagenic origins (hello, the one writing this is a protector who split specifically due to the trauma you anti-endos inflicted on us!! In other words, your community is directly responsible for my traumagenic existence!! Should I be thanking you for allowing me a chance to experience the better parts of life? Hm, nah.) and are scared to interact with others who share our own damn disorder. You claim the "main difference" between us and you is that we define "all plurals" differently, but from where we're standing, the "main difference" is that pro-endos aren't regularly traumatizing, harassing, suicide baiting, mocking and insulting, spreading misinformation about, using slurs against, wishing harm on, and fakeclaiming the other side, often for merely disagreeing with them. We just came out of a harassment campaign in which anti-endos spread hate in our inclusive tags and spaces for weeks. I'm fucking sick of syscourse and being told I should kill myself for the "crime" of being inclusive of endogenic systems like the ones that helped me accept my plurality in the first place, or the pro-endos that create resources that help me manage my DID and not be a dissociative wreck all the time. To say the main difference between our communities is "how we define 'all plurals'" is a spit in the face of all the shit I and many, many others have faced from anti-endos like you over the years.
If you change your stance and learn not to hate others for their religions, cultures, traits they can't control, and personal beliefs and choices about their own body and mind, we will be happy to welcome you to our community and this blog. But until then, you need to re-evaluate your priorities and morals in life. Are you fine with being part of a community that twists others' words on the regular to make it seem like they're promoting child abuse? Are you chill with the fact that I exist as a protector to defend my system from people like you, the same way many others in my system exist to protect us from other abusers and threats to our safety and health? Are you okay with telling a living, breathing person you admire and enjoy the work of that you disagree with their identity and existence, and that you ally yourself with those who want them dead just for existing, have even personally threatened their life and well-being, as you have just done with this ask?
What took me off-guard was this ask and just how horribly you seem to be unaware of basic concepts like "plural is an inclusive term signaling someone is pro-endo" and "'all systems' does not mean 'only traumagenic systems'." But I guess in a way, it's only fair; you mistook me for one of those who hate my guts – while I can't tell even as I type this if you are a troll or not.
TLDR: No, we will not clarify in our bio that we are pro-endo, because there is no need to do so when we already use terms that signal that everywhere on our blog, and our pinned post even clarifies our stance in the rare case someone doesn't know the signal. You have been horribly misinformed; you cannot support "all plurals" while being against certain plurals, and "plural" is an inclusive term anyway even without that clarification. Again, you have misunderstood our pinned post which tells anti-endos like you to fuck off, which is almost funny considering we put that section in the post due to the horrendous amounts of harassment we and other pro-endos (not even just endogenic systems; a lot of anti-endos group all of us together as "fakers spreading misinformation") have faced from anti-endos like you. Please go think about the kind of people you're spending time with, and ask yourself if you're okay with being part of the same group of people that wants those like me dead for the crime of existing in a way that doesn't adhere to one specific medical model whose authors acknowledge isn't the only way to be more-than-one, anyway.
Have the day you deserve! <3
59 notes
·
View notes
Text
Gestational Diabetes: What to Know
New Post has been published on https://type2diabetestreatment.net/diabetes-mellitus/gestational-diabetes-what-to-know/
Gestational Diabetes: What to Know
We get a LOT of queries on pregnancy and diabetes -- not least gestational diabetes, the kind that pops up during pregnancy in women who have not had diabetes prior. To help answer the many questions that come our way, we’ve put together the following guide to key gestational diabetes topics.
Image Attribution
Image Attribution
URL: https://www.flickr.com/photos/jerrylai0208/14281758292/in/photolist-nL2KaW-7Lsz4B-s3b9L-7XfFgh-669mzY-8dbGLR-dy17Rr-uyVKg-rWDFG-c9f8u-7yZp5w-9WBx3T-6TjsGN-9CGXc4-5WhfPV-6346AE-8veKBD-4oqPNU-7PZhur-ioxAFh-8AQeS5-uyVK7-uyVKf-dNFjG-e1TAcm-6tEN8R-6Xho3o-cBfh-cpyFfC-i3eVYw-gYP4my-eBo6v-eBo6W-gSK9LN-cjtJe-c2W1WW-4UP1x7-63XnZy-pCYamt-6FoNAH-6YjLR5-7BhtFi-Pyuhr-nyYHAv-7Bhtte-JG5XP-4Hbppe-6nhU6m-6zsXFb-rWDwg
Please note that we also published a fact-filled doctor/patient interview on pregnancy with existing type 1 and type 2 diabetes recently here. Be sure to check that out too!
Know a lot about these topics yourself? Please add your 2 cents in the comments section below!
What is Gestational Diabetes?
Simply put, gestational diabetes is a form of elevated blood sugar that women get specifically during pregnancy, when the placenta makes hormones that can lead to a buildup of sugar in the blood. If you are unlucky enough to have a pancreas that can’t make enough insulin to handle that onslaught of hormones, your blood sugar levels will rise and can cause gestational diabetes.
You might be surprised to hear that the medical community does not agree on an exact level of blood glucose that determines gestational diabetes.
The American Diabetes Association (ADA) currently defines gestational diabetes as:
Fasting glucose level of 92 mg/dl (5.3 mmol/L in European unites) or higher
One-hour post-meal glucose level of 180 mg/dL (7.8 mmol/L) or higher
Two-hour post-meal glucose level of 153 mg/dL (6.7 mmol/L) or higher
But the UK’s National Institute for Health and Care Excellence (NICE) recently altered the threshold for diagnosis to a looser standard of 5.6-mmol/L (101 mg/dL) fasting glucose, which reduces the “unmanageable numbers of women falling into the category of gestational diabetes,” European authorities state.
Either way, the ADA explains: “Gestational diabetes usually appears roughly halfway through pregnancy, as the placenta puts out large amounts of ‘anti-insulin’ hormones. Women without known diabetes should be screened for gestational diabetes 24 to 28 weeks into their pregnancies. (If high blood glucose levels are detected earlier in pregnancy, the mother-to-be may actually have type 2 diabetes, rather than gestational.)”
The ADA estimates that gestational diabetes occurs in 9.2 percent of pregnancies.
What’s the Diabetes and Pregnancy Risk?
The bad news is: if left untreated, extreme high blood sugar levels can cause damage to the baby's brain that can lead to developmental delay and a host of other problems.
As reported by the “What to Expect” folks, “if excessive sugar is allowed to circulate in a mother's blood and then enter the fetal circulation through the placenta, the potential problems for both mother and baby are serious.”
Uncontrolled high blood sugars can lead to having a too-large baby (a condition called macrosomia), making delivery more difficult and C-section more likely, and even preeclampsia and stillbirth.
Poorly controlled diabetes during pregnancy can also lead to potential problems for the baby after birth, such as jaundice, breathing difficulties and low blood sugar levels. Later in life, he or she may be at an increased risk for obesity and type 2 diabetes.
The good news is: “These potential negative effects don't apply to moms who get the help they need to keep their blood sugar under control.” And there is lots of help available!
Note that since gestational diabetes is considered a pregnancy complication, women who have it are more likely to be induced, since most doctors won't let their pregnancies progress past their due dates.
Signs and Symptoms of Gestational Diabetes
How do you know if you might have gestational diabetes?
The tricky part is, most women don’t have obvious symptoms, so it can easily go undetected. The basic symptoms are similar to those that appear with the onset of any kind of diabetes:
Unusual thirst
Frequent and copious urination
Fatigue
Sugar in the urine (detected by a lab test)
A Test for Gestational Diabetes?
The most common test is a fasting test called an oral glucose tolerance test (OGTT). This measures how well your body’s cells are able to absorb glucose, or sugar, after you ingest a given amount of a sugary drink. The test can take place in your doctor’s office or a local lab.
To prepare for it, you need to abstain from food for at least 8 hours before the scheduled test. You can drink water, but no other beverages, including coffee and caffeinated tea, as these can interfere with the results.
When you arrive at the test site, the technician will take a blood sample to measure your baseline glucose level. This part of the test is also called a fasting glucose test.
After that, you’re asked to drink a solution that contains ~75 grams of sugar. And an hour later, you’ll give a second blood sample to see the effect on blood sugar level.
If your result is positive (a high glucose number after one hour) your doctor may ask for a test at the two and three-hour marks as well to best determine how well your body can handle a sugar challenge.
Gestational Diabetes Diet (aka What to Eat)
Because diet/meal plan is a mainstay of controlling glucose levels, experts encourage women to see a professional dietitian to help them craft a meal plan suited to them individually -- based on weight, height, physical activity, and their own level of glucose intolerance.
But even if you don’t have access to a pro, here are some general dietary guidelines, compiled by registered dietitian Julie Redfern:
Eat a variety of foods, distributing calories and carbohydrates evenly throughout the day. Make sure both your meals and your snacks are balanced. The American Diabetes Association recommends that you eat three small-to-moderate-size meals and two to four snacks every day, including an after-dinner snack.
Curb your carb intake. Limit foods and beverages that contain simple sugars such as soda, fruit juice, flavored teas and flavored waters, and most desserts – or avoid them altogether. These foods can quickly elevate your blood sugar.
Milk is high in lactose, a simple sugar, so you may need to limit the amount you drink. If you're looking for a new beverage of choice, try club soda with a squeeze of lemon or orange, or unsweetened decaffeinated iced tea.
It's best to include complex carbs (those containing more fiber) and spread them out over the day. Pair lean protein with carbohydrates at all meals and snacks. Protein helps to make you feel fuller, sustain energy, and give you better blood sugar control.
Don't skip meals. Be consistent about when you eat meals and the amount of food you eat at each one. Your blood sugar will remain more stable if your food is distributed evenly throughout the day and consistently from day to day.
Eat a good breakfast. Your blood glucose levels are most likely to be out of whack in the morning. To keep your level in a healthy range, you may have to limit carbohydrates (breads, cereal, fruit, and milk), boost your protein (eggs, cheese, peanut butter, nuts) , and possibly avoid fruit and juice altogether.
Include high-fiber foods, such as fresh fruits and vegetables, whole grain breads and cereals, and dried peas, beans, and other legumes. These foods are broken down and absorbed more slowly than simple carbohydrates, which may help keep your blood sugar levels from going too high after meals.
Some Great Advice on Managing Gestational Diabetes
It is true that women who experience gestational diabetes have a seven times greater risk of developing type 2 diabetes by the time their child turns 10, compared with women who didn’t have it.
But at the same time, a combination of good diet, exercise and glucose-lowering medications can keep both mother and baby healthy and safe.
Here are some excellent tips we’ve garnered from various experts:
Try CGM: Like your sisters with type 1 and type 2 diabetes, tight glucose control can be aided by using a continuous glucose monitor (CGM). For this, you’ll likely need to see a healthcare professional who specializes in diabetes, an endocrinologist or diabetes educator.
Create a Team: “Stay calm, find an amazing endocrinologist and also connect with inspirational and supportive women who have been through it,” recommends Noor Alramahi, a type 1 diabetes advocate in Palo Alto, CA, who had a healthy diabetic pregnancy with twins. She adds that this is important because the psychological aspect is often the biggest challenge.
Don’t Stress Over Single Highs: Noor also says, “Before pregnancy and in the family planning stages doctors and healthcare providers put a lot of emphasis on the potential complications of a ‘high risk’ pregnancy, so much so that when you do get pregnant that’s all you can think about, like I did, every time my numbers were not perfect (70-120). The stress over that made it a lot worse than it really was. I was lucky to have an amazing endo who kept reminding me that it’s fine to have high numbers here and there as long as I don't keep them high, and that the stress might do more damage than the occasional off-target glucose result.”
Know Your Food: Brooke Gibson, founder of the Bay Area support group Sugar Mommas who has had four healthy diabetic pregnancies herself, emphasizes how important it is to control your diet and exercise as much as possible to keep your blood sugars under good control. “Talk to a nutritionist to learn about different foods and how they can affect your blood sugar.”
Follow Up After Baby: Dr. Kristin Castorino, who cares for pregnant woman with diabetes at the Sansum Center in Santa Barbara notes, “About half of women who have gestational diabetes will eventually develop type 2, so it’s important after delivery to continue to make changes to you and your family’s routines around food and activity to be on a healthier life path. The National Diabetes Prevention Program is proven to help prevent T2. Many YMCAs or health care centers have started local programs.”
On Coping with Gestational Diabetes
San Diego-based mom and writer Elise Blaha Cripe chronicled her experiences with gestational diabetes on her blog. She shares some important practical things she learned:
eating vegetables (especially green ones!) with meals helps keep my blood sugar down
most fruits are out aside from berries
walks after meals help keep numbers low
strenuous exercise can make numbers higher
stress plays a HUGE factor in blood sugar levels
a glass of milk or a small bit of carbohydrates right before bed can help my body regulate sugars overnight
Elise Blaha Cripe and family
She also puts the whole gestational diabetes experience into perspective this way:
“I have found that in the scheme of things, gestational diabetes, while annoying, is no big deal. Best case, I change my diet, eat healthy, exercise, gain an appropriate amount of weight & maintain correct blood sugar levels. Worst case, I am unable to manage my blood sugar with diet and exercise & need to take medication. But here's the thing, as long as it's properly managed, I should be blessed with a healthy baby. There can be complications of course. But there can always complications. This is birth. This is life.”
“Once I embraced that, this whole thing became easier.”
Thank you Elise, et al!
Some Resources on Gestational Diabetes
“Gestational Diabetes During Pregnancy” -- an online guide from the authors of the “What to Expect” books.
“Managing Your Gestational Diabetes” -- guidebook by famous diabetes and pregnancy expert Dr. Lois Jovanovic.
“Gestational Diabetes: Your Survival Guide” -- a handbook by Dr. Paul Grant, consulting diabetologist at the John Radcliffe Hospital, Oxford, UK.
Diabetic Mommy -- an online blog and community site run by a mom with type 2 diabetes.
“The Ultimate Gestational Diabetes Cookbook” -- a popular resource by chef Ted Alling.
Disclaimer: Content created by the Diabetes Mine team. For more details click here.
Disclaimer
This content is created for Diabetes Mine, a consumer health blog focused on the diabetes community. The content is not medically reviewed and doesn't adhere to Healthline's editorial guidelines. For more information about Healthline's partnership with Diabetes Mine, please click here.
Type 2 Diabetes Treatment Type 2 Diabetes Diet Diabetes Destroyer Reviews Original Article
0 notes
Text
Diagnosing endo part 2
I have an essay due in 3 days so obviously Tumblr is my priority. I’ll explain a bit more here about the process of actually being diagnosed but It could be MUCH more in depth so please message me if you want to know any specifics or any advice. When I was suspected of having it (after 5+ years of being ignored and brushed off by various medical professionals) I religiously read blogs, websites, articles and anything I could get my hands on to understand what was happening inside me. Although I’d had health problems before there is something so uniquely devastating about endometriosis. The best way I can think to describe it is feeling like you’ve been invaded, like you’re fighting your own body and losing when it’s supposed to be on your side with the knowledge that there is no end in sight (no end-o? wheeey). The pain reached its peak near the end of my second relationship. My biggest regret is not being able to communicate with my partner about the pain I was in, instead I resented him for taking an interest in it and for trying to be closer to me at a time where I wanted to shut myself off from everything rather than deal with these feelings. It took me a long time to stop blaming myself for doing that. I didn’t understand what was happening so how on earth could I help someone else to understand? I used to think having any kind of health problem was easier in a relationship because you had that constant emotional support. But the expectation you have of your partner supposedly knowing you, knowing how you how feel when you’re in pain, knowing how to act and when to act, was a very damaging part of my relationship. I was relieved when I ended it for both our sakes. Six months after that, in September 2015 I became unable to work because of the pain, the bleeding, the sleepless nights and endless worrying that my insides were just giving up on me. My self worth had gone to shit and I got involved with a self confessed narcissist with his own cocktail of mental and physical health problems to distract me (I don’t feel bad writing that because he’ll be too busy wanking off to his own reflection somewhere to read this). This at least marked at a turning point at which I regularly crawled to the GP in tears begging them to listen to me. I was constantly in trouble at one of my two jobs and because of the invisible illness element of it I was treated with disdain and told I was being overly dramatic about period pain and would face disciplinary. It was hard to fight my corner when I had no clue what was wrong, no medical evidence and nothing visible I could show to anyone. I was only taken seriously when I came in for a shift where I felt like my organs were falling out, walked onto the shop floor and burst into tears. People at work changed their tune but I didn’t feel any more supported or hate myself and my body any less for constantly failing me and it irritated me that I had to constantly get to a point of breaking down for people to listen. After months solidly on the pill (to stop me having any kind of period), as well as a couple of instances of passing out and A&E trips due to pain, in February 2016 I had a laparoscopy. It was performed by a disinterested doctor who genuinely said the words ‘I didn’t think there was anything wrong with you. How did you cope being in so much pain? You should have made more of a fuss’ as soon as I came round from the anaesthetic (my parents had words with him and I love them for that). He confirmed what I knew all along: That most doctors did not take women’s pain seriously, especially when it was to do with their reproductive organs. He flippantly told me he would give me an injection that would ‘shut my ovaries down’ and put me into early menopause for at least 6 months at age 23 (which I graciously declined at a later date). The lowest point was the next week or so. Naturally the narcissist didn’t wish me well before the operation and ignored me for weeks on end afterwards and my outlook became bleaker and bleaker. They had told me that the pill had healed a lot of my endo which was great but that there was an active patch on a blood vessel they would never be able to remove and scarring on my abdomen and pouch of douglas (why that name though? I really don’t understand). I had super got my hopes in the weeks before surgery and convinced myself that this would be the end – they’d remove what was there, pop in a mirena coil and I could put it all behind me and be pain free. No one prepared me for the emotional upset of being told not only that your own consult DID NOT BELIEVE the pain I shared with him but also that they had not been able to rectify the situation through the surgery. I was told there was a chance the coil would improve the pain but we would see in 6 – 18 months and there was nothing more they could do. I was discharged and never, in any of this, was any psychological aspect mentioned. The amount of hormones going in and out of my body in those few months was enough to make anyone miserable, let alone the healing scars, discomfort of the coil settling in (almost as bad as the discomfort of realising it has done nothing for the pain a year later woooo) and the abrupt return to my three part time jobs where I was fine now as far as anyone was bothered. Saying this, once again I never shared my discomfort with anyone outside my immediate support network, and even stopped talking about it to them after a while for fear of becoming annoying. Instead I did what I was used to: internalised everything, hated myself, felt anger and frustration over my lack of control over my body, health and emotions and tried to make everyone around me comfortable (even those who didn’t deserve it) at the expense of my own health and sanity. It’s been a long path to being able to write any of this with crippling shame and anxiety over what people might think but I am so sure I am right in saying that I am important, my body and comfort is important and the people around you need to know your needs in order to help you. The best thing I learnt from this whole experience was that I can absolutely handle it alone (because I forced myself to) but people are so willing to help as soon as they are aware of what you’re going through. And it’s up to you to make them aware because no matter how well someone knows you, they cannot feel your pain and know your thoughts. Never feel guilty for making your needs known, for feeling what you really feel but don’t hold it against those around you because it is a toxic, lonely place. I’m still in pain daily and there is still no end in sight, more investigations to come and a constant balance of trying to enjoy myself without burning myself out completely. But somewhere in all of this, with the support of beautiful friends and considerate and understanding sexual conquests (Is there any better way to say that? Probably) I changed my relationship to my mind and body for the better and am on my way to a much better place. And for the record strong painkillers, anti-depressants, therapy (not CBT) and binge eating comfort food are also really really great.
0 notes
Text
Ask D'Mine: Is Medicare Snooping? And Dead CGMs
New Post has been published on http://type2diabetestreatment.net/diabetes-mellitus/ask-dmine-is-medicare-snooping-and-dead-cgms/
Ask D'Mine: Is Medicare Snooping? And Dead CGMs
Who doesn't sometimes need help navigating life with diabetes? That's why we offer Ask D'Mine, our weekly advice column, hosted by veteran type 1, diabetes author and educator Wil Dubois. This week, he takes a look at the federal government's involvement in approving test strip prescriptions, and — being an expert continuous glucose monitor user and book author on the topic — Wil gives some advice on what sometimes happens when a GCM transmitter stops working. Go on, read up!
Got your own questions? Email us at [email protected]
Nancy, type 2 from Missouri, writes: When I picked up my test strips this month, my pharmacist told me that Medicare is requiring my pharmacy to have a copy of my blood sugar logs for 30 days, no more than 6 months old. An annoyance to be sure, since I tend to suck at writing them down. But, beyond that, I don't get the rationale. Is it some kind of test to prove that I use the damn strips? If so, what's stopping me from making up the numbers for a log? And it's feeling like a big fat invasion of privacy. I like my pharmacist, he's a great guy. But he doesn't make treatment decisions such as how much insulin I use or whether I'm in good enough control, so there's no reason that I can see that he needs to have my test logs. Perhaps Medicare is trying to make it annoying for me to get the strips so I'll just pay for them myself? Do you know anything about this?
Wil@Ask D'Mine answers: I checked with some folks in the Medicare supply biz, and they tell me that Medicare only requires the 30 days of less-than-half-year-old data when a patient uses more strips than Medicare likes to pay for. As a reminder to everyone, Medicare guidelines only cover one strip per day for folks on pills and three per day for insulin shooters. Not enough in either case.
Of course, your doc can fill out the paperwork for an "over-utilization" request. If your doc has a documentable medical reason for your needing the amount of strips that any sane person would realize that any healthy diabetic would need in the first place, the feds are pretty good about covering them. Commercial insurance is another matter altogether, however. They take the fed guidelines and cast them in stone. Getting what you need from a commercial plan is a nightmare. Cost is always excessive and sometimes even then, you're screwed as they won't always listen to a physician's override prescription all in the name of "medical necessity." So much for this being between you and your doc ...
But back to your situation. Yeah, the feds do require the supplier or pharmacy to keep copies of logs or doctor's notes. It's nothing super-new; it's a small part of 2010's Improper Payments Act. And yes, it's absolutely a test to prove that you use the damn strips. An annoyance? Perhaps. But I gotta say, if Medicare is willing to give you twice or three times the number of strips that they misguidedly think you need—at no additional cost to you—I don't think it's outrageous for them to ask for occasional proof that you're actually using them.
Wow. Never thought I'd see the day I'd be defending Medicare. But will Medicare even look at your logs? Probably not. Medicare has a small SWAT team of medical reviewers that travel around the country and pounce unexpectedly on the suppliers cashing those big checks from the government. God help the pharmacy that sells you a gazillion strips, then gets raided during a random audit and can't prove that your doc ordered the strips, and that you're using them.
The feds aren't going to judge your blood sugar, they're only interested in whether or not you're actually using what they pay for. It's not about your health. It's about the money. So you aren't being judged, nor is your doctor. It's an anti-fraud kinda thing. Medicare is served by a legion of for-profit companies that get rich preying on seniors. Late night ads, aggressive phone marketing, and refill increases that neither doctors nor patients asked for or needed got us where we are today.
Now for you, Nancy, I have a few ideas. The log doesn't have to be hand-written. You can give the pharmacy a download of your meter—although I admit it is odd they asked you directly; typically they'd send a request to your doc. Anyway, if you don't know how to do a download, ask someone at your doctor's office for help. As to your privacy: yeah, the boys at the one-hour photo will absolutely look at your naked pics, and probably make copies for themselves, too. But I doubt your pharmacist is the blood sugar equivalent of a dirty old man. He'll probably put your log into a file cabinet without looking at it. Still, if you want to keep your blood sugar data more private (I understand), you can just have the statistics page for 30 days printed. The stats page gives the number of times you tested in the time period, the highest reading, the lowest reading, and the average. Is someone still peeking into your underwear drawer? Yes, but they'll be learning a lot less than they could from the full log book.
Could you forge a log? Sure. Why not? Teenagers do it every day. Usually in the waiting room at the endo's office. You could even ask for more strips, forge a bigger log book, then sell the strips on Ebay. The system isn't perfect. But the feds are more interested in keeping the suppliers honest than in keeping the patients honest.
One last thing. My friendly local EdgePark rep, one of the ones I queried about this issue, was mortified that you were turned away by your pharmacy, saying, "The pharmacy should not have refused the script, but should have at least filled the Medicare guideline amount, then required the patient to give them a log book," before filling the rest of the script.
Anyway, moving forward, I think we'll see a lot more requirements like this. Healthcare costs are out of control and there's going to be a lot of time and money wasted to ensure that we're not wasting time and money. But for me, I would have been more than happy to give my insurance company two log sheets per year to get the strips I need. I gave them a lot more than that, and was still turned down.
Allison, type 1 from Arizona, writes: OK, I need to get my Medtronic sensor going again. I have your CGM book in one hand and the little blue transmitter charger in the other. I'm trying to figure out why my charger is flashing red. I've changed the battery and even left it plugged in overnight. Suggestions?
Wil@Ask D'Mine answers: Sorry Allison, you're screwed. Red is dead. A little-known, but apparently published (in small print, in Appendix MCXII of the MiniLink user's guide) fact is that if you let your transmitter fully discharge, it's the same as drowning a baby squirrel: There's no bringing it back.
You'll have to buy a new one. If it makes you feel any better, I did the same thing to an iPro transmitter at the clinic. My boss told me if I ever did it again, it was coming out of my paycheck!
So here's the deal, boys and girls: If you're taking a CGM vacation, put a fresh copper-top into the little blue charger and leave the frickin' transmitter plugged in. If you're on a CGM vacation and didn't do this, go attend to it right now.
No more drowned baby squirrels! It's crazy because we're "trained" to worry about over-charging batteries on our devices, but not warned that apparently, keeping a trickle charge going to your Med-T transmitter is its life support system. I guess taking our squirrel analogy to its extreme, keeping the transmitter charging is needed for healthy hibernation.
This is not a medical advice column. We are PWDs freely and openly sharing the wisdom of our collected experiences — our been-there-done-that knowledge from the trenches. But we are not MDs, RNs, NPs, PAs, CDEs, or partridges in pear trees. Bottom line: we are only a small part of your total prescription. You still need the professional advice, treatment, and care of a licensed medical professional.
Disclaimer: Content created by the Diabetes Mine team. For more details click here.
Disclaimer
This content is created for Diabetes Mine, a consumer health blog focused on the diabetes community. The content is not medically reviewed and doesn't adhere to Healthline's editorial guidelines. For more information about Healthline's partnership with Diabetes Mine, please click here.
Type 2 Diabetes Treatment Type 2 Diabetes Diet Diabetes Destroyer Reviews Original Article
0 notes