
Sideblog for text-heavy DID posts. I also have CPTSD, Conversion Disorder /FND, and complex chronic pain.
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by ophidahlia-did and here's what we found interesting.
Average Info
Notes Per Post
423K
Likes Per Post
232K
Reblog Per Post
191K
Reply Per Post
814
Time Between Posts
3 days ago
Number of Posts By Type
Text
11
Note
1
Photo
4
Video
1
Last Seen Tumblr Blogs





Fun Fact
Tumblr.com rank in the US is 25.
Text
absolutely cursed
I found some Chicago Bears Nesting dolls Mercari



345 notes
·
View notes
Text
turned on the San Diego Zoo live ape cam and theres an orangutan walking around wearing a cloak
25K notes
·
View notes
Note
Hi! I'm was another anon but I just realised a much better wording to my question. How do you handle having to trust a therapist? Individually or as a system... So sorry for bringing this to you twice if this is a bad topic. Good luck out there
I appreciate you rephrasing your question. More general questions without specific examples are easier for me to answer.
I think building trust really just takes time. You need to build positive experiences that prove to yourself (and all parts of your system) that you are safe and that your therapist is a safe person.
I think that it can help to identify which parts of your system are struggling with trust so that you can discuss their concerns directly. We made a list of concerns and brought it too therapy. We invited concerned parts to be present in therapy until they felt comfortable enough to relax. We check in with them frequently and ask “Is it okay to share this? Are we going too fast? Is this topic alright?”
When our therapist wanted to work with a part that was inaccessible because the system didn’t trust her to work with them, we started building trust and proving to the system that it was safe. We directly told our therapist, “We’re not ready for you to talk to that part yet. We want to start with someone else.” So we used the same techniques with a part who was holding a less upsetting trauma memory, and we showed the whole system that the techniques worked, and that it was safe to interact with our therapist. We did this a few times, gradually building up to allowing access to the part everyone is afraid to work with.
15 notes
·
View notes
Text
person: are you out of your mind?!
me, dissociating: quite literally, yes, i am
29K notes
·
View notes
Text
Feeling pretty comfortable reclaiming "crazy" as a slur tbh ("mad" also). Even years after getting diagnosed correctly I still have little control over switches, so much identity confusion, so much "made" actions/feelings/thoughts, my physical health & mental state are both extremely unpredictable & unstable over days, weeks, & even months. Combine D.I.D. with Conversion Disorder, CPTSD, complex chronic pain, and all the other very uncommon components & marginalizations of my situation (being trans, a power wheelchair user, extremely poor, a practicing pagan, etc etc just edges me further out onto the fringes of society)... "crazy" just feels like my normal now. Like, I still have apparent physical injuries just appear out of nowhere and it's nearly impossible to determine that they're really conversion symptoms and not actually organic. It feels like even my body itself is crazy, to say nothing of my mental states.
Saying I'm crazy is like, anything but a diagnosis. Crazy, for me personally, isn't experiencing things that aren't real, which is how most people (especially neurotypicals) think of it, it's experiencing things which most other people can't comprehend as being real. It's not lacking a grasp on reality, it's other people not being able to grasp my reality. It's existing somewhere outside the general consensus reality. "Crazy" is a box people put you in when they can't imagine you fitting in any of the tidy, neatly labelled boxes they have for people because your lived reality threatens to overturn their little epistemological taxonomy.
Well, I'm keeping the box and I'll going at it with the markers and box cutter and duct tape and they can't stop me lol. I always loved the Mad Pride movement/counter-culture for so many reasons, and over time I guess those reasons have finally become as personal as they are political.
(Neurotypicals do not interact with this)
#Mad Pride#Crazy slur#Slur#Slurs#Tw#actually dissociative#actuallydissociative#actually did#If other folks have a different understanding of what it means to be crazy thats fine#Its political but it's also very personal
46 notes
·
View notes


Text
It is okay to not be diagnosed officially. Sometimes things get in the way. Like lack of funds, or a lack of emotional support. Maybe you're in a dangerous place. Maybe you cannot handle the official diagnosis. Because there is such a big stupid difference between knowing for a fact you have it and having the paperwork in front of you to confirm your suspicions. It can be an emotional process that can make or break you.
So, take your time. Get your diagnosis when you're ready. I love and support you 💙
115 notes
·
View notes
Text
The theory of structural dissociation
Here’s a post where I explain the theory of structural dissociation. All information is taken from The Haunted Self: Structural Dissociation and the Treatment of Chronic Traumatization by Van der Hart, Nijenhuis and Steele (2006).
I am not a professional and am only repeating things I’ve read. The reason I’m making this post is because I (and others) refer to the theory of structural dissociation regularly, so having a clear post about it seemed like a good idea!
Before explaining the different ‘levels’ of structural dissociation, I’ll shortly explain the terms ANP and EP. ANP stands for Apparently Normal [Part of the] Personality, whereas EP stands for Emotional [Part of the] Personality.
Very broadly stated, ANP parts are focused on functioning in the daily life and distanced from anything trauma-related; in DID ANP’s can be completely unaware of any trauma. EP’s are more trauma-related; often ‘containing’ very intense, trauma-related emotions, memories, actions, beliefs et cetera.
However, it’s important to mention that the ANP/EP distinction is not black/white. Some EP’s can help out in daily life, ANP’s can still have emotions, stuff like that. Especially once there are multiple parts and more elaborated parts, the ANP/EP distinction becomes blurry. For instance, I wouldn’t be able to define for all of us whether they’re ANP or EP.
Okay. Back to the theory of structural dissociation. Two more important terms: elaboration and autonomy of parts. Please check out this infographic by @clever-and-unique-name on the elaboration of parts! Simply put, elaboration is about the degree to which a part has its own traits (e.g. name, internal appearance, skills, beliefs, …) and autonomy is about the degree to which a part feels they are their own self and the degree to which they can take executive control (aka ‘switch out’).
The theory of structural dissociation distinguishes between three ‘levels’ of structural dissociation:
Primary structural dissociation. This is the most ‘simple and basic’ trauma-related division of the personality: a single ANP and a single EP. In this case, the EP is unelaborated and not very autonomous in daily life. Primary structural dissociation often occurs after a single traumatizing event.
Secondary structural dissociation. When traumatizing events keep happening and keep being overwhelming, further division of the EP can happen while the ANP remains intact: in this situation someone will have one ANP and multiple EP’s. The EP’s can be more elaborated and autonomous than in primary structural dissociation, but are typically less elaborated and autonomous than in tertiary structural dissociation.
Tertiary structural dissociation. The difference between this level and secondary structural dissociation is that in tertiary structural dissociation, the person has more than one ANP and multiple EP’s. This can happen when inescapable aspects of daily life have become associated with past trauma, or when the functioning of the existing ANP(’s) is so poor that normal life becomes too overwhelming - causing a new ANP to develop. In this level, it’s common for several ANP’s and EP’s to be more elaborated and autonomous than in secondary structural dissociation.
In severe cases of secondary and in all cases or tertiary dissociation, more than a single part may have a strong degree of elaboration (e.g. names, ages, genders, preferences) and emancipation (perceived separation and autonomy). This is not usually observed in primary structural dissociation, and neither in most cases of secondary structural dissociation.
According to the authors of The Haunted Self, the levels of structural dissociation and various diagnostic labels relate as follows (they categorize more diagnoses in the book, I’m only naming the ‘relevant’ ones right now):
PTSD = primary structural dissociation
Trauma-related BPD, CPTSD, OSDD = secondary structural dissociation
DID = tertiary structural dissociation
Please keep in mind this is a proposed relationship between structural dissociation levels and DSM diagnostic labels. Many survivors experience structural dissociation without the elaboration and emancipation of some dissociative parts found in DID.
Based on this description of the theory it may seem easy to figure out ‘where you are at’, but personally I believe it’s not. That’s why I, for myself, hold onto the idea that dissociation is a spectrum. These categories help a lot, but there are no hard walls in between. Maybe someone with PTSD from a single traumatic event can have two EP’s. Maybe someone with CPTSD can have black-out amnesia but no elaborated parts. Maybe someone with OSDD can have more elaborated parts (that’s me).
A last important note is that, once you’re in a ‘higher’ level, you can also have the parts associated with lower levels. Simple example: someone with DID can also have very simple, one-dimensional, unelaborated EP’s.
I think that’s plenty information for now. Let me know if I made a mistake, missed something big, or if you have any questions.
- Sae
439 notes
·
View notes
Text
Child Parts
“Child parts, or vulnerable parts, carry intense and unmodulated feeling states such as longing, fear, sadness, abandonment, need, hopelessness, and shame. These parts often represent either the normal feelings that were not tolerated in the family and had to be dissociated, such as the longing for nurturance, or traumatic dissociated feelings such as terror. These young parts can also hold a full range of physical sensations, such as pain, shakiness, agitation, coldness, or intense hunger.
Child parts often function at the developmental level of early childhood or even infancy, with some being preverbal. These parts’ cognition is often undeveloped, both because of their developmental stage and because of their trauma exposure and lack of adequate support or nurturance. Even when these parts become calm enough to think, their early narratives about the trauma are often fragmented, primitive, and/ or missing.
(…)Child parts can be very fearful and dysregulated; however, they can also be highly creative, playful, and spontaneous. When they are cared for, usually by the therapist initially and then eventually by the adult self of the client, they can feel a greater sense of safety and connection, including feelings of adoration or love. With an increased sense of security, they may also be able to grieve their losses and experience sadness and empathy.”
“Treating Adult Survivors of Childhood Emotional Abuse and Neglect: Component-Based Psychotherapy” (p. 151), by Hopper, Grossman, Spinazzola, Zucker
540 notes
·
View notes
Video
You have no idea how long I looked for this
163K notes
·
View notes
Text
The theory of structural dissociation
Here’s a post where I explain the theory of structural dissociation. All information is taken from The Haunted Self: Structural Dissociation and the Treatment of Chronic Traumatization by Van der Hart, Nijenhuis and Steele (2006).
I am not a professional and am only repeating things I’ve read. The reason I’m making this post is because I (and others) refer to the theory of structural dissociation regularly, so having a clear post about it seemed like a good idea!
Before explaining the different ‘levels’ of structural dissociation, I’ll shortly explain the terms ANP and EP. ANP stands for Apparently Normal [Part of the] Personality, whereas EP stands for Emotional [Part of the] Personality.
Very broadly stated, ANP parts are focused on functioning in the daily life and distanced from anything trauma-related; in DID ANP’s can be completely unaware of any trauma. EP’s are more trauma-related; often ‘containing’ very intense, trauma-related emotions, memories, actions, beliefs et cetera.
However, it’s important to mention that the ANP/EP distinction is not black/white. Some EP’s can help out in daily life, ANP’s can still have emotions, stuff like that. Especially once there are multiple parts and more elaborated parts, the ANP/EP distinction becomes blurry. For instance, I wouldn’t be able to define for all of us whether they’re ANP or EP.
Okay. Back to the theory of structural dissociation. Two more important terms: elaboration and autonomy of parts. Please check out this infographic by @clever-and-unique-name on the elaboration of parts! Simply put, elaboration is about the degree to which a part has its own traits (e.g. name, internal appearance, skills, beliefs, …) and autonomy is about the degree to which a part feels they are their own self and the degree to which they can take executive control (aka ‘switch out’).
The theory of structural dissociation distinguishes between three ‘levels’ of structural dissociation:
Primary structural dissociation. This is the most ‘simple and basic’ trauma-related division of the personality: a single ANP and a single EP. In this case, the EP is unelaborated and not very autonomous in daily life. Primary structural dissociation often occurs after a single traumatizing event.
Secondary structural dissociation. When traumatizing events keep happening and keep being overwhelming, further division of the EP can happen while the ANP remains intact: in this situation someone will have one ANP and multiple EP’s. The EP’s can be more elaborated and autonomous than in primary structural dissociation, but are typically less elaborated and autonomous than in tertiary structural dissociation.
Tertiary structural dissociation. The difference between this level and secondary structural dissociation is that in tertiary structural dissociation, the person has more than one ANP and multiple EP’s. This can happen when inescapable aspects of daily life have become associated with past trauma, or when the functioning of the existing ANP(’s) is so poor that normal life becomes too overwhelming - causing a new ANP to develop. In this level, it’s common for several ANP’s and EP’s to be more elaborated and autonomous than in secondary structural dissociation.
In severe cases of secondary and in all cases or tertiary dissociation, more than a single part may have a strong degree of elaboration (e.g. names, ages, genders, preferences) and emancipation (perceived separation and autonomy). This is not usually observed in primary structural dissociation, and neither in most cases of secondary structural dissociation.
According to the authors of The Haunted Self, the levels of structural dissociation and various diagnostic labels relate as follows (they categorize more diagnoses in the book, I’m only naming the ‘relevant’ ones right now):
PTSD = primary structural dissociation
Trauma-related BPD, CPTSD, OSDD = secondary structural dissociation
DID = tertiary structural dissociation
Please keep in mind this is a proposed relationship between structural dissociation levels and DSM diagnostic labels. Many survivors experience structural dissociation without the elaboration and emancipation of some dissociative parts found in DID.
Based on this description of the theory it may seem easy to figure out ‘where you are at’, but personally I believe it’s not. That’s why I, for myself, hold onto the idea that dissociation is a spectrum. These categories help a lot, but there are no hard walls in between. Maybe someone with PTSD from a single traumatic event can have two EP’s. Maybe someone with CPTSD can have black-out amnesia but no elaborated parts. Maybe someone with OSDD can have more elaborated parts (that’s me).
A last important note is that, once you’re in a ‘higher’ level, you can also have the parts associated with lower levels. Simple example: someone with DID can also have very simple, one-dimensional, unelaborated EP’s.
I think that’s plenty information for now. Let me know if I made a mistake, missed something big, or if you have any questions.
- Sae
439 notes
·
View notes








Photo

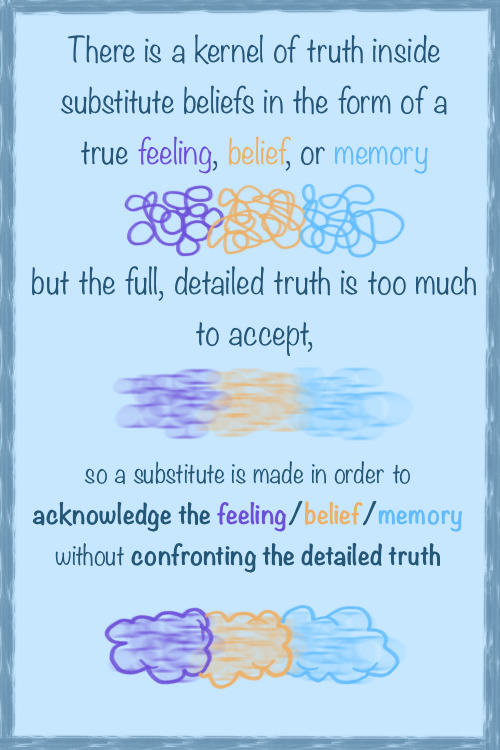
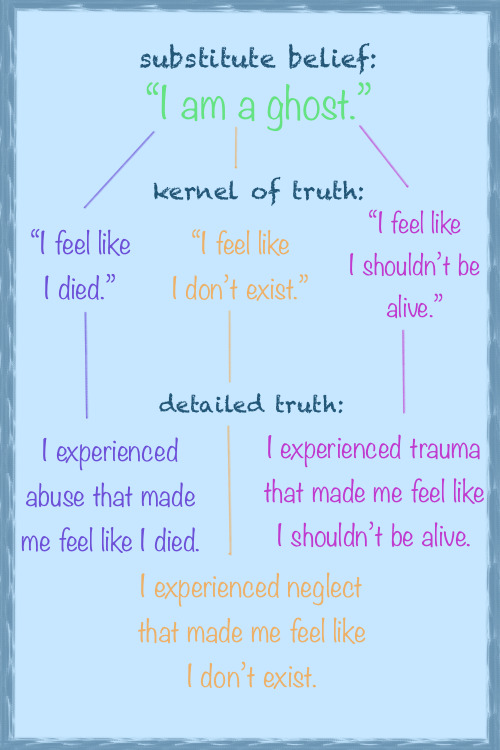

“Substitute beliefs” is an umbrella concept that can be applied to understanding introjects (fictional and real-life), pseudomemories, non-human alters, and more.
It’s important to note that not all substitute beliefs are harmful–they may be comforting, or even feel empowering. You don’t necessarily have to stop being a ghost! That said, it may be worth mentioning in therapy to make sure it’s a healthy belief to engage with.
[Check out my DID/OSDD casually explained masterpost for sources and more infographics!]
5K notes
·
View notes

Text
“In avoiding any situations reminiscent of the past trauma, or any initiative that might involve future planning and risk, traumatized people deprive themselves of those new opportunities for successful coping that might mitigate the effect of the traumatic experience. Thus, constrictive symptoms, though they may represent an attempt to defend against overwhelming emotional states, exact a high price for whatever protection they afford. They narrow and deplete the quality of life and ultimately perpetuate the effects of the traumatic event.” — Judith Lewis Herman
59 notes
·
View notes
Text
I don’t know who needs to hear this, but please let your self cry and feel and hurt. let the pain leave your body. the longer it stays there, the more it will hurt you.
63K notes
·
View notes