Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by medhumans and here's what we found interesting.
Average Info
Notes Per Post
562K
Likes Per Post
251K
Reblog Per Post
310K
Reply Per Post
45
Time Between Posts
2 months
Number of Posts By Type
Photo
5
Quote
5
Text
2
Link
5
Last Seen Tumblr Blogs





Fun Fact
Tumblr was the first site to host the blog for President Barack Obama in 2011.
Photo







This Comedian Nails Why The Mental Illness + Creativity Connection is Ridiculous
185K notes
·
View notes
Quote
1. Trauma permanently changes us. This is the big, scary truth about trauma: there is no such thing as “getting over it.” The five stages of grief model marks universal stages in learning to accept loss, but the reality is in fact much bigger: a major life disruption leaves a new normal in its wake. There is no “back to the old me.” You are different now, full stop. This is not a wholly negative thing. Healing from trauma can also mean finding new strength and joy. The goal of healing is not a papering-over of changes in an effort to preserve or present things as normal. It is to acknowledge and wear your new life — warts, wisdom, and all — with courage. 2. Presence is always better than distance. There is a curious illusion that in times of crisis people “need space.” I don’t know where this assumption originated, but in my experience it is almost always false. Trauma is a disfiguring, lonely time even when surrounded in love; to suffer through trauma alone is unbearable. Do not assume others are reaching out, showing up, or covering all the bases. It is a much lighter burden to say, “Thanks for your love, but please go away,” than to say, “I was hurting and no one cared for me.” If someone says they need space, respect that. Otherwise, err on the side of presence. 3. Healing is seasonal, not linear. It is true that healing happens with time. But in the recovery wilderness, emotional healing looks less like a line and more like a wobbly figure-8. It’s perfectly common to get stuck in one stage for months, only to jump to another end entirely … only to find yourself back in the same old mud again next year. Recovery lasts a long, long time. Expect seasons. 4. Surviving trauma takes “firefighters” and “builders.” Very few people are both. This is a tough one. In times of crisis, we want our family, partner, or dearest friends to be everything for us. But surviving trauma requires at least two types of people: the crisis team — those friends who can drop everything and jump into the fray by your side, and the reconstruction crew — those whose calm, steady care will help nudge you out the door into regaining your footing in the world. In my experience, it is extremely rare for any individual to be both a firefighter and a builder. This is one reason why trauma is a lonely experience. Even if you share suffering with others, no one else will be able to fully walk the road with you the whole way. A hard lesson of trauma is learning to forgive and love your partner, best friend, or family even when they fail at one of these roles. Conversely, one of the deepest joys is finding both kinds of companions beside you on the journey. 5. Grieving is social, and so is healing. For as private a pain as trauma is, for all the healing that time and self-work will bring, we are wired for contact. Just as relationships can hurt us most deeply, it is only through relationship that we can be most fully healed. It’s not easy to know what this looks like — can I trust casual acquaintances with my hurt? If my family is the source of trauma, can they also be the source of healing? How long until this friend walks away? Does communal prayer help or trivialize? Seeking out shelter in one another requires tremendous courage, but it is a matter of life or paralysis. One way to start is to practice giving shelter to others. 6. Do not offer platitudes or comparisons. Do not, do not, do not. “I’m so sorry you lost your son, we lost our dog last year … ” “At least it’s not as bad as … ” “You’ll be stronger when this is over.” “God works in all things for good!” When a loved one is suffering, we want to comfort them. We offer assurances like the ones above when we don’t know what else to say. But from the inside, these often sting as clueless, careless, or just plain false. Trauma is terrible. What we need in the aftermath is a friend who can swallow her own discomfort and fear, sit beside us, and just let it be terrible for a while. 7. Allow those suffering to tell their own stories. Of course, someone who has suffered trauma may say, “This made me stronger,” or “I’m lucky it’s only (x) and not (z).” That is their prerogative. There is an enormous gulf between having someone else thrust his unsolicited or misapplied silver linings onto you, and discovering hope for one’s self. The story may ultimately sound very much like “God works in all things for good,” but there will be a galaxy of disfigurement and longing and disorientation in that confession. Give the person struggling through trauma the dignity of discovering and owning for himself where, and if, hope endures. 8. Love shows up in unexpected ways. This is a mystifying pattern after trauma, particularly for those in broad community: some near-strangers reach out, some close friends fumble to express care. It’s natural for us to weight expressions of love differently: a Hallmark card, while unsatisfying if received from a dear friend, can be deeply touching coming from an old acquaintance. Ultimately every gesture of love, regardless of the sender, becomes a step along the way to healing. If there are beatitudes for trauma, I’d say the first is, “Blessed are those who give love to anyone in times of hurt, regardless of how recently they’ve talked or awkwardly reconnected or visited cross-country or ignored each other on the metro.” It may not look like what you’d request or expect, but there will be days when surprise love will be the sweetest. 9. Whatever doesn’t kill you … In 2011, after a publically humiliating year, comedian Conan O’Brien gave students at Dartmouth College the following warning: “Nietzsche famously said, ‘Whatever doesn’t kill you makes you stronger.’ … What he failed to stress is that it almost kills you.” Odd things show up after a serious loss and creep into every corner of life: insatiable anxiety in places that used to bring you joy, detachment or frustration towards your closest companions, a deep distrust of love or presence or vulnerability. There will be days when you feel like a quivering, cowardly shell of yourself, when despair yawns as a terrible chasm, when fear paralyzes any chance for pleasure. This is just a fight that has to be won, over and over and over again. 10. … Doesn’t kill you. Living through trauma may teach you resilience. It may help sustain you and others in times of crisis down the road. It may prompt humility. It may make for deeper seasons of joy. It may even make you stronger. It also may not. In the end, the hope of life after trauma is simply that you have life after trauma. The days, in their weird and varied richness, go on. So will you.
Catherine Woodiwiss, “A New Normal: Ten Things I’ve Learned About Trauma” (via thepeacefulterrorist)
It is such a pleasure and a gift to read this right now, to remind myself that all of us who have suffered trauma of any form will and do live on.
(via md-admissions)
46K notes
·
View notes
Text
the worst thing you can say to someone is ‘you’re too sensitive’ because that’s basically saying ‘you feel things more deeply and fully than I do and this inconveniences me because now I have to be more mindful of my own actions’
you’re not too sensitive, the world is just callous and stubborn. sensitivity doesn’t make you weak and callousness doesn’t make you strong.
273K notes
·
View notes
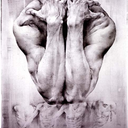
Photo



Device may allow sensations in prosthetic hands
To the nearly 2 million people in the United States living with the loss of a limb, including U.S. military veterans, prosthetic devices provide restored mobility, yet lack sensory feedback. A team of engineers and researchers at Washington University in St. Louis is working to change that so those with upper limb prosthetics can feel hot and cold and the sense of touch through their prosthetic hands.
Daniel Moran, PhD, professor of biomedical engineering in the School of Engineering & Applied Science and of neurobiology, of physical therapy and of neurological surgery at Washington University School of Medicine in St. Louis, has received a three-year, nearly $1.9 million grant from the Defense Advanced Research Projects Agency (DARPA) to test a novel device developed in his lab that would stimulate the nerves in the upper arm and forearm. If it works, upper-limb amputees who use motorized prosthetic devices would be able to feel various sensations through the prosthetic, which would send sensory signals to the brain.
DARPA is already funding the “Luke Arm,” a high-tech bionic limb created by DEKA Research. The prosthetic is named for “Star Wars” character Luke Skywalker, who received a prosthetic after losing his right hand in an epic battle with Darth Vader. It is designed to help servicemen and women and veterans who had upper limb amputations. While the advanced prosthetic arm allows users to perform six different grips, such as picking up small objects, it does not provide users with the sense of touch and orientation of a natural hand.
Moran, whose expertise is in motor neurophysiology and brain-computer interfaces, and his team have developed an electrode designed to stimulate sensory nerve cells in the ulnar and median nerves in the arms. The ulnar nerve, one of three main nerves in the forearm, is the largest nerve in the body unprotected by muscle or bone and is connected to the ring finger and pinkie finger on the hand. It’s the nerve that is stimulated when a hit to the elbow triggers the “funny bone.” The median nerve in the upper arm and shoulder is connected to the other fingers on the hand, so together, the two nerves control movement and sensations including touch, pressure, vibration, heat, cold and pain in all of the fingers.
People using arm prosthetics have to rely on their vision to use them properly, Moran said. To pick up a cup of coffee, they have to be able to see the cup, place the fingers of the prosthesis around it and lift it. They are unable to feel whether the cup is in their hand, if the cup is hot or cold, or if they are about to drop it. By enabling the ability to feel, users will have more control over the prosthesis.
Moran’s team includes Harold Burton, PhD, professor of neurobiology and Wilson (Zach) Ray, MD, assistant professor of neurological surgery, both at the School of Medicine; and Matthew MacEwen, who graduates this month with an MD/PhD and who worked on this project for his dissertation. The team developed a macro-sieve peripheral nerve interface designed to stimulate regeneration of the ulnar and median nerves to transmit information back into the central nervous system.
Ray will implant the device — which is made of an ultrathin, flexible material similar to a soft contact lens and is about one-eighth the size of a dime — into the forearms of anesthetized nonhuman primates. The research team will then determine the amount of sensory information that is encoded by providing low levels of stimulation to small groups of nerves. The device, which looks like a wagon wheel with open spaces between the “spokes,” allows the nerve to grow. Ray also will implant a small cuff electrode, the current standard of care, to compare the performance.
Once implanted, Moran and the team will train the nonhuman primates to play a joystick-controlled videogame, in which the team will give them cues as to where to move the joystick by stimulating specific sectors in the ulnar and median nerves so it feels as if someone is touching them, Moran said. Their reward for advancing through the various stages of the game successfully is fruit-flavored juice.
“We want to determine what they can perceive through artificial stimulation of the nerves,” Moran said. “If we stimulate a particular sector of the nerve, that tells them to reach to a specific target. Using very low levels of stimulation (i.e. sensation), we want to figure out how many different nerve sectors we can independently encode with a unique target location.”
Keep reading
132 notes
·
View notes
Quote
You can’t just switch off your feelings because the other person did.
Sophie Kinsella (via onlinecounsellingcollege)
8K notes
·
View notes
Link
0 notes
Link
0 notes
Link
so necessary and so relevant
0 notes
Text
my apologies
for the years of silence. loss and its aftermath had swept me away. i am back now, albeit with eyes wider and more weary.
0 notes
Quote
It isn’t reasonable to ask that we achieve perfection. What is reasonable is to ask that we never cease to aim for it.
Dr. Atul Gawande, “Complications: A Surgeon’s Notes on an Imperfect Science” (via classicalconditioning)
286 notes
·
View notes
Quote
“Miraculously recover or die. That’s the extent of our cultural bandwidth for chronic illness.”
S. Kelley Harrell (via chronicillnessmemes)
657 notes
·
View notes
Photo


Artist Bobby Baker, who has faced both breast cancer and borderline personality disorder, chronicles both her physical and mental recovery through these whimsical, insightful drawings. Despite some of the pain and vulnerability she shares in her work, Bobby says, “I can’t help being funny. I have always made people laugh.” You can see more of Bobby’s drawings in the book Diary Drawings: Mental Illness and Me.
145 notes
·
View notes
Link
Tweeting Cancer, by Meghan O’Rourke The New Yorker, January 13, 2014
"… What Adams is doing is not new—it is not even new in our time. But it is less filtered and more immediate than ever, and surely this is part of what’s at stake here: a lingering concern that dying perhaps deserves...
4 notes
·
View notes
Photo

Abraham Verghese, MD, MACP, opened the 2012 Joint Meeting of the American Ophthalmology Assn with a talk about where meaning resides in medicine—the human touch. It’s a powerful, old-fashioned tool that modern medicine is in danger of losing, he said.
Dr. Verghese is professor for the Theory and Practice of Medicine at Stanford University Medical School and senior associate chair of the Department of Internal Medicine. He is also the author of three best-selling books: two memoirs and a novel. He began his discussion by examining Sir Luke Fildes’ famous painting, The Doctor (1891). It’s an iconic image that has influenced public perceptions of medicine over time and has been used to articulate different points of view about medical care.
Fildes was commissioned to create a piece that would “put on record the status of the doctor in our time.” He drew inspiration from the physician who cared for his oldest son. Despite the tragedy of his son’s death on Christmas Eve, Fildes was so impressed with the physician that he chose to depict “the physician in our time.” In it, the doctor holds vigil by a gravely ill child’s bedside, with the worried parents in the background. None of the new medical instruments—stethoscope, thermometer, ophthalmoscope—of that Victorian era are pictured. It’s just light streaming in, with the doctor focusing singular attentiveness on the child. The public reception was overwhelming, and it was credited with elevating the medical profession.
When President Truman proposed a form of nationalized medical care, the American Medical Association weighed in with its opinion against the legislation by reproducing this image in countless brochures and posters bearing the slogan “Keep Politics out of This Picture.” “It was a very successful campaign that has kept us from socialized medicine,” Dr. Verghese said, as it preyed on parents’ fears that Truman’s plan would mean their child might not get this kind of care.
In Britain, by contrast, the same image was used to celebrate the 50th anniversary of the National Health Service. When asked about the painting, Fildes never mentioned the death of his child, Dr. Verghese said, but “spoke of the dawn breaking and the hope that comes to us all. I believe that it [the painting] is not about the doctor. It’s about you and me putting ourselves in the role of the sick child. What do I want? The attentiveness of the doctor. It speaks to the Samaritan instincts of medicine.”
If The Doctor were painted today, Dr. Verghese said he fears it would depict a doctor attentive to a computer screen instead of the ill child. “The patient in the bed has become an icon for the patient in the computer. I’ve taken heat from Silicon Valley for coining the term the iPatient. The iPatient is getting all the attention, while the patient in the bed is asking ‘Where the hell is everyone, when will I be informed?’ Medicine today has transformed the three-dimensional human being into a two-dimensional image.”
The danger of not being at the bedside is that you will lose the ability to diagnose the low-hanging fruit, and it represents the loss of an important ritual, he said. “Rituals are about transformation. The ritual of one individual coming to another and telling them things they don’t tell their priest or rabbi, disrobing and then allowing people to touch them. That is a ritual of exceeding importance,” he said. “It preserves the personality of the patient and focuses on the body.”
“Ophthalmology is the last bastion of hands-on care,” Dr. Verghese said. “As you go out to the exhibit hall to look at the latest technology, remember that the finest instrument in your possession is your hand. The ability of the hand to heal is what we should be seeking.” The need to preserve the meaning of medicine in the midst of the most extraordinary changes in health care since the 1960s was the common theme among all the Opening Session speakers, including Academy CEO David W. Parke II, MD. At a time of rapid consolidation, EMR adoption and numerous quality of care initiatives, it’s important to measure your professional impact through the people you have helped and the lives you’ve changed, said Dr. Parke. “Remember the narratives—they are why we became doctors in the first place.”
10 notes
·
View notes
Quote
It is easy enough to reiterate these elisions by skipping the grief and moving straight into an academic argument. Maybe it is unavoidable; maybe the elision is the requirement of the academic narrative form. No one who writes about cancer can really escape the ways that language overwrites the helplessness and pain of mortality.
S. Lochlann Jain (2013) Malignant: How Cancer Becomes Us. Endnote 10, Chapter 5. (via fullerenes)
5 notes
·
View notes
Photo









Watch the whole talk here»
Almost 20 years ago, writer Andrew Solomon fell into a deep depression. In this talk from TEDxMet, he speaks eloquently and openly about his struggle with “the family secret we all share,” but that no one wants to talk about. If you are a human or know a human, you have to watch this talk, but — be warned — you might just find yourself in tears.
49K notes
·
View notes
Link
A powerful, must-read first-hand account of The Atlantic editor Scott Stossel’s lifelong battle with (and eventual embrace of) crippling anxiety issues. Anybody who has ever struggled with anxiety, or knows someone who has, will find something of value in this extraordinary and brave essay.
And after you’ve read his essay, please make sure to read the companion piece, This is Anxiety, featuring stories from other Atlantic readers about their own battles with anxieties of all kinds, how they’ve survived, what’s helpful, and what isn’t.
(A big, BIG thank you to The Atlantic for running these pieces, and doing their part to raise awareness and fight the stigma around talking openly about mental illness.)
415 notes
·
View notes