#we need more ora serratas
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was attacked by a cross-site scripting worm deployed by the Internet troll group GNAA on Dec 3, 2012.
Text
There are so few weird looking women mutants. I was trying to think about it now (not the background only had a name and died type of characters) and it's genuinely pathetically so little. They are almost all painfully humanoid at most with different skin colour and some markings.
This also made me learn that onyxx is a boy I always thought she was a girl I am so heartbroken.
8 notes
·
View notes
Text
All I know is no way Genesis supporters Lycaon and Ora Serrata retain their seats after the Genesis War, and my bet is on White Sword to take the Seat of Stalemate and Death will take the Seat of Law. The whole scene between him and Pestilence where he waxed on about the importance of having their laws and traditions actually mean something was very pointed, especially in light of how hypocritical Ora usually was about seeing herself as above the law.
I don’t know that I see Redroot sitting on the Ring directly as they haven’t even had her available to act as the Voice of Arakko since they moved planets, so I do see her as more likely to be a direct parallel to Doug as the Voice of Krakoa, and don’t quote me but I’m PRETTY sure I remember seeing saying in an interview that one of the Arakkii Five we saw in Year 1000 of Sins of Sinister, and who helped resurrect Storm, would have a younger version who’d take one of the empty Great Ring seats. Bloodroot, Genis Mind-Flayer and Craana are the most likely candidates of those five but my money is on either Genis or Craana to be the new Seat of Dreams as we have yet to see an omega level Arakkii telepath or reality warper like those two. So they each fill a unique niche that would work for the Seat of Dreams.
As for Xilo and Fisher King staying merged, I think it’s likely at least for the time being, and I would not be surprised to see Apocalypse to take the empty Night Seat as I bet anything he was one of the original Night Seats on Okkara.
But I don’t see Apocalypse taking one of the nine Great Ring seats because they’ve put too much emphasis on him not being omega and if they do change the Arakkii precedent of only omegas holding GR seats, that needs to play out rather than just be handwaved as oh we’re not doing that anymore.
I don't know if I've talked about it here before or not, but I'm torn between my two picks for the still vacant Seat of Dreams on the Great Ring of Arakko.
On one hand, we have Apocalypse coming back, and if he doesn't return to Krakoa, I could see him holding this seat, but on the other hand, we have the return of Redroot. With her back in the picture, this would be the perfect opportunity to have Arakko itself sit on the Great Ring, with Redroot acting as it's Voice, as opposed to the unofficial seat it originally had.
Of course, if (That-Which-Was) Xilo stays merged with the Fisher King, that would potentially open up either the Seat of History or the Seat of Nothing, and Arakko could potentially fill the former.
7 notes
·
View notes
Text
Night Seats Revealed!
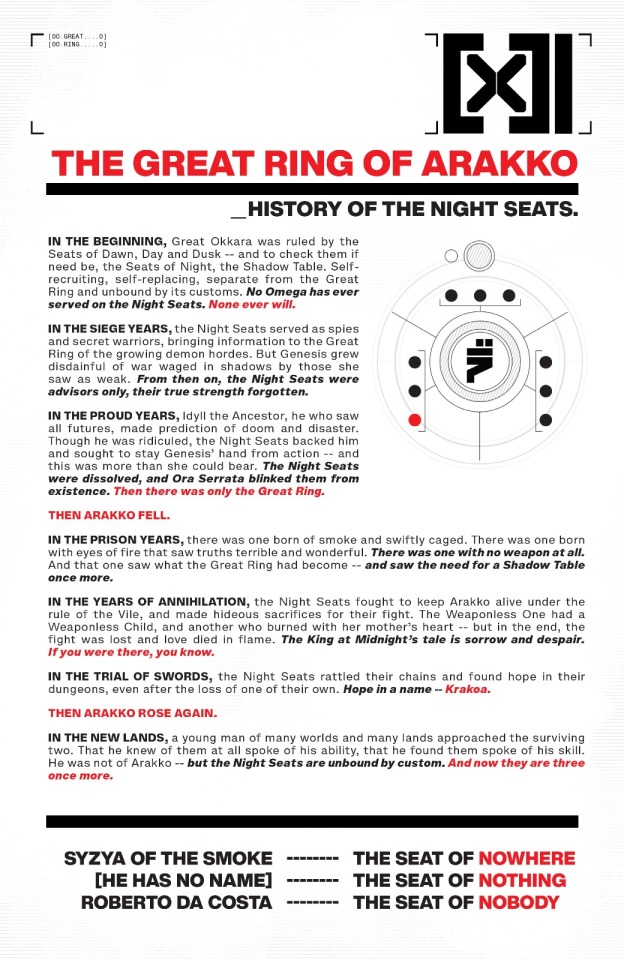
I like the juxtaposition of how the Night Seats check and balance Dawn, Day, and Dusk. It's even more poetic that they're all Non Omega mutants. No Omega has ever sat in the Night Seats and none ever will, just like how no Non Omega has ever sat in the Great Ring and none ever will.
The Night seats therefore represent the people of Arakko more so than even the Seat of All Around Us and Seats of Dusk as they're the "regular folks" that don't have stupid powerful weapons yet still continue to fight in the name of Okkara, and then Arakko. I also like that they're not bound to the customs of the Great Ring and they're really a no-nonsense kinda group. They do what needs to be done free from the biased prejudice of the Omegas serving on the Great Ring.
Which brings me to the point about Genesis. I was surprised to learn that Apocalypse is the more open minded one in the relationship. He accepts the formation of mutant circuits and even encourages it. Survival of the people more so than survival of the individual. It seems when Genesis says she's more fit than him, she embodies the same ideals as him 1000% more hardcore. Here we see that she refuses to acknowledge and even feels insulted by the role that the Seats of Night plays in battle. She doesn't like cold War tactics, she prefers direct "honorable" Combat. She even had Ora Serrata erase them from existence because they disagreed with her.
We haven't had a lot of characterization for Genesis, and the ones we have had of her seems to portray her as being a hardened warrior mother who's proud but also compassionate. But I think it's neat that they break down the stereotype of life giving nurturing Gaia-esque Snow White motherhood character in that she has some fatal character flaws too. She's too proud to listen to her people, those who she deems as weaker than her, and even those who merely disagree with her as we have seen from Idyll. He was an Omega Seer and Genesis should have known this, yet she's too stubborn and proud to acknowledge his prophecy and instead punished the very balancing mechanism for staying her hands.
12 notes
·
View notes
Text
Management of Proliferative Sickle Cell Retinopathy Associated With Retinoschisis in a Tertiary Hospital in Saudi Arabia:A Case Report by Ahmed D

Introduction
Sickel cell disease (SCD) is the most common endemic disease with the prevalence reaching up to 3% [1,2]. The disease results from point mutation of nuclear bases at the sixth position of the beta-globin chain (substitution of glutamic acid by valine results in hemoglobin SS or glutamic acid by lysine results in hemoglobin SC). These two genotypes have different clinical presentations in which HbSS is more common and associated with a severe systemic disease where Hb SC is associated more with SCD proliferative retinopathy, this is probably due to rising in hematocrit level leading to thrombosis formation and occlusion of retinal precapillary arterioles [1,3]. Sickle cell retinopathy develops in the second decade of life rarely to be seen under the age of 10 years [4,5].
The initiating event in the pathogenesis of proliferative retinopathy results from vaso-occlusive events of microvasculature (peripheral retinal arteriolar occlusion) resulting in the production of hypoxia-inducible factor 1 (HIF-1α), basic fibroblast growth factor (bFGF) and vascular endothelial growth factor (VEGF) causing ischemia to the peripheral retina and resulting in neovascularization with characteristic sea fan appearance [6]. The proliferative retinopathy can result in sight-threatening complications.
Goldberg categorized the proliferative retinopathy into 5 stages [7], in which the early stages of proliferative retinopathy; peripheral arterial occlusion (stage 1) or peripheral arteriovenous anastomoses between the perfused and nonperfused peripheral retina (stage 2 ) may not need intervention and spontaneous regression due to auto-infarction can be seen without any complications(8), on the other hand the vision loss is common in late stages (stage 3 sea fan ) due to vitreous hemorrhage (stage 4) and tractional retinal detachment with or without hole formation (stage 5) for that it is very important to screen and manage promptly to preserve the current vision and prevent complications(9).
Currently, there is lacking evidence of optimum management [1], the aim is to induce regression of neovascularization (sea fan stage) and prevent the need for surgical interventions prior to complications [7,10].
Case Report
A 33-year-old female presented to our hospital complaining of floaters in the right eye for one day the other eye asymptomatic, the patient is a case of sickle cell disease no previous history of any ocular or systemic illnesses. A full ophthalmic examination was carried out, Visual acuity was 20/200 OD (Right eye), 20/28 OS (Left eye), intraocular pressure 11 mmHg OD, 12 mmHg OS. For the right eye extraocular muscule motility and anterior segment (sclera, conjunctiva, cornea, iris, and lens) were normal, on posterior segment examination the view was hazy due to mild vitreous hemorrhage, there was partial posterior vitreous detachment and subhyaloid hemorrhage and mild vitreous hemorrhage and sea fan seen at the temporal retina and slightly elevated with associated retinoschisis, the left eye showed sea fan at the far periphery of temporal side also slightly elevated as the other eye.
A plan was made to do pars plana vitrectomy, silicon oil injection, and endo-laser for the right eye if the vitreous hemorrhage did not clear or increased after one week of observation. After one week the patient came with much reduction of the vitreous hemorrhage and improvement of the visual acuity to 20/50 so laser scatter photocoagulation was planned for both eyes extending posterior to the sea fan OU for about 2-3 disc diameters and anteriorly involving all the ischemic retina up to near the ora serrata.
One week Post laser, the visual acuity was 20/50 OD 20/28 OS. In the Follow up two weeks later the patient was satisfied and had no new complaints visual acuity 20/40 OD, 20/28 OS the laser marks darkened and vitreous hemorrhage completely disappeared .
Discussion
The visual loss in proliferative sickle cell retinopathy (PSR) is mainly due to vitreous hemorrhage and tractional retinal detachment, hence the early detection can prevent such complications [9].
The treatment aims to induce regression of stage 3 PSR avoiding possible complications and blindness [11]. One paper on 341 eyes studying the rate of PSR regression between the control groups (47 weeks) and the laser-treated groups (42 weeks) showed no significant difference. This is possible due to the lack of having specific criteria for doing a proper preventive laser and the regression could happen due to auto-infarction of blood vessels [2]. Some clinicians will choose to observe waiting for auto-infarction since the rate is about 32% (12) others may consider treatment, unfortunately the ideal management in sickle retinopathy is not well defined [1].
Photocoagulation is considered the safest method of treatment of neovascularization just like proliferative diabetic retinopathy [11,13]. The laser is indicated in neovascularization more than 60-degrees, other proposed indications to start treatment are spontaneous vitreous hemorrhage, rapid progression, single eye patient, bilateral proliferative cases [14], elevated neovascular fronds and in cases where the fellow eye has been lost from proliferative retinopathy [18]. In our case study, we initiated treatment because the patient had bilateral proliferative with spontaneous vitreous and subhyaloid hemorrhage in one eye and elevated fronds bilaterally Fig 1. On the other hand we did not take a rapid decision to perform a vitrectomy to the more advanced right eye because of the known significant intra and post-operative complications that can occur in those patients from surgical intervention as ocular ischemia , recurrent hemorrhage and elevated intraocular pressure [18]. Fortunately enough, a decrease in vitreous hemorrhage and good fundus view was probable within one week which enabled us to go for scatter laser photocoagulation.
The retina produce vascular growth factors leading to the formation of new vessels, Not just from the ischemic retina but also from 2 mm posterior to ischemic retina hence the laser should be extended posterior to and up to ora Serrata, if we consider scattered laser photocoagulation [15,18]. This is similar to what we did In our case study where we aimed at completely ablating the ischemic retina with a safety zone up to the ora serrate and posteriorly for 2-3 disc diameters, we also extended the treatment circumferentially 2 clock hours on both sides of the ischemic retina extent to be sure that we did not miss any ischemic area.
The specific methods treating PSR are scatter laser (360-degree to the periphery or localized around the new vessels) or feeder vessel laser coagulation [16].One study considered the scatter laser as the preferred method ablating the ischemic retina circumferentially 360-degree [17], another one found that feeder coagulation is comparable to scattered laser in the prevention of VH but with a potential risk of inducing retinal break and vitreous hemorrhage because of the high power settings used in this modality of treatment [2,18]. For unreliable patients it was postulated to do scatter laser 360-degree [16], although there is no clear evidence that the outcome of this technique is any better than the other laser techniques or even observation for spontaneous regression [18]. In our case study we did not go for 360 degree treatment because we did not feel that coagulating healthy peripheral retina will be of benefit particularly that other studies did not find any superiority of such a technique. The mechanism of feeder laser coagulation is direct occlusion [13] and in the scattered laser is indirect ablating ischemic retina decreasing vascular endothelial growth factor VEGF [16]. From our point of view we anticipated that ablating the ischemic retina is a more radical treatment than occluding the neovascularization leaving the ischemic retina untreated with the potential of developing new neovascularization because of the unchecked release of the growth factors from the untreated ischemic retina The preferred laser effect is when the disease is detected early at the periphery before reaching the central retina [17], and the successful treatment is achieved if we avoid the potential complication and morbidity of surgical interventions[11].
Conclusion
Although this is only a case study, yet with the criteria driven from larger studies, we feel that scatter laser is a safe technique with no complications and effective in the management of this proliferative disease when detected at stage 3 and before entering into the more advanced stages 4 and 5 .
For more information about Journal : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/pdf/IJCMCR.SC.ID.00050.pdf https://ijclinmedcasereports.com/ijcmcr-sc-id-00050/
#Proliferative Sickle Cell Retinopathy#Tertiary Hospital#Saudi Arabia#Ahmed D#ijcmcr#clinical studies
0 notes