#the con has good masking and vaccination policies but the risk is still there. and also Public Transit
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has a low social media market share in South America.
Text
what if i went to a furry convention in 2 weeks. i probably won't but what if i did
#ray speaks#it would take 2 hours to get there by public transit :(#and i'd have to talk to my parents about going kjdgfhkghfd#annnnd there would be Crowds and it'd be stressful & also idk if i wanna risk getting c*vid for this.#the con has good masking and vaccination policies but the risk is still there. and also Public Transit#siiiigh#lots of reasons Not to go but mannnn i'm still tempted#pre-registration is closed so at least i cant impulse buy a pass Now. but they're reopening registration next week...
9 notes
·
View notes
Text
Thoughts on the Reopening of Schools

Hello, friends and families…! In this blog post I will NOT tell you if it is OK for your child to return to school for remote, in-person, or hybrid learning. Any article that gives you specific advice about this may be well intentioned, but will rarely apply to your individual situation, and will be based on information that is going to be out of date by the time you read it.
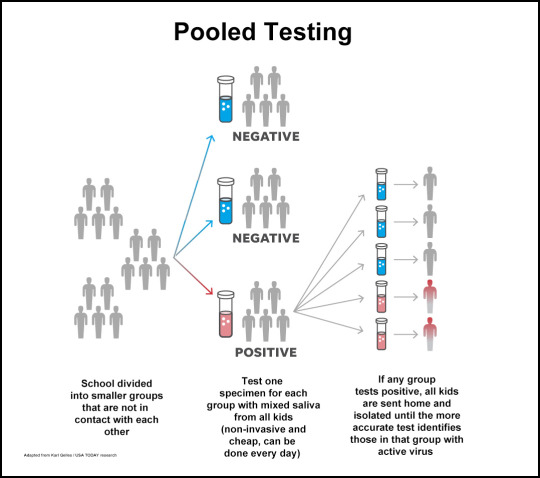
I AM, however, going to review some important points to keep in mind when you juggle the pros and cons of any individual decision that you make for your family, and I think that will be helpful. Just like deciding about surgery, it will ALWAYS come down to weighing the risks and benefits of any given path. When I’m helping parents decide about an operation, I often hear “we just want what’s best for our child”. But it’s very rare that a situation is clear enough so that there is only one reasonable choice. The decision almost always comes down to balancing personal risk tolerance and a wide range of intangibles. That’s why it’s not usually my job to tell my families WHAT to do, but to help them understand the tradeoffs so that they can make those decisions themselves. With that said, here are some things to keep in mind when you are making a decision about school in the era of COVID-19. 1) I probably don’t have to tell you this, but any official recommendation, government regulation or organizational decision about school reopening is NOT only considering the medical aspects of the situation. Economic, political, parenting, regional and developmental concerns are always going to be a big part of what you are told, and that’s reasonable. From a purely medical point of view, the “safest” thing to do would for everyone to stay in full lockdown until a vaccine arrives, but virtually no one is seriously recommending that. So don’t discount those factors, but be aware of their impact and relative importance. 2) Most people making these decisions are working in good faith, and trying to get the best possible outcome. It’s easy to vilify school administrators and other parents by assuming the worst underlying motives. But the majority of people who actually have the responsibility of making community decisions are trying to strike the right balance. Give them the benefit of the doubt, hear them out and consider the tradeoffs that they are dealing with before forming your own opinions. Be open to new strategies to minimize school risks. For example, one such idea is pooled saliva testing which is to be used by the SUNY system. This is much cheaper and less invasive than traditional testing methods, and it will allow schools to rapidly shut down new outbreaks before they spread widely in the community.
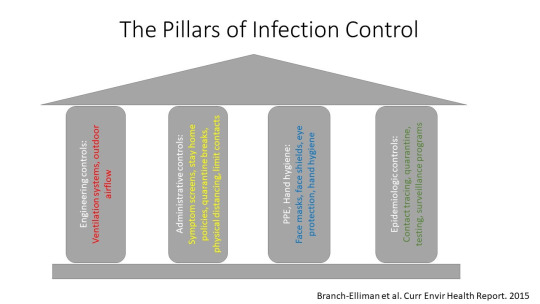
3) There are a large number of controls - administrative, infrastructure / engineering, epidemiological and personal - that can be incorporated into an in-person reopening plan. It’s beyond the scope of this email to discuss them all, but here is a good summary. Not every school needs to adopt every possible control, but this should give you an idea about the kind of things that you might be asked to consider. Try to understand the goals that are reasonable for your child's particular situation, taking into account the time, place and current community infection rates. Keep this passage in mind:
“Given the uncertainty, reliance on an effective vaccine to solve the return-to-school problem is unrealistic, and other strategies that may at first glance seem too difficult or too expensive must be developed and implemented. If the position adopted by society is: ‘not until it is completely safe,’ then we have to recognize that the kindergarteners who left their elementary schools in March of 2020 may never see the inside of those buildings again. This is not feasible. Thus, we really need to shift the conversation from ‘perfectly safe’ and ‘only if there is vaccine’ to ‘how can we do this as safely as possible?’ and ‘what resources do we need in order to achieve this common goal?’“
4) The people who know more about COVID-19 than anyone else in the world never heard of it 8 months ago. This is a new virus, and we are learning about it daily. Beware of anyone who is absolutely certain, who doesn’t qualify their advice with words like “as best as we know right now”, or who makes definitive statements about the long term effects of infection. Watch out for people trying to score cheap political points by comparing someone’s prior and current statements, and claiming “hypocrisy” or “flip-flopping”. For something new like this, it is always important to follow current developments and continually refine policy and practices. Don’t be like the guy that Stephen Colbert was describing when he said: "He believes the same thing Wednesday that he believed on Monday, no matter what happened on Tuesday.” 5) Having accurate, current data about the number of local infections is CRUCIAL in running any sort of school plan, and that has to be monitored regularly. Plans for in-person education can change overnight - you can see that with the early opening and reclosing of several college campuses. As schools open, we are getting new data about the rate of infection in children, which must be watched closely as this process continues. Some recent information suggests that infection rates are actually rising faster in children than in adults. However, this data set covers all patients under ager 18. There is other evidence that toddlers have exceptionally low infection rates, despite being - as this article describes them - "mask licking germ bombs". 6) The American Academy of Pediatrics has a document outlining its recommendation for school reopening. In general, they recognize that there are serious downsides to remote learning including the challenges of effective teaching, the loss of the social aspects of school, and the inherent inequality of online classes, especially for underserved communities. So if in-person education can be done safely, that's better for kids. But they also stress the point that there is no one single answer for all times and places. Increasing evidence that children can be asymptomatic for weeks and spread the virus has to be incorporated into any school plan. While the AAP’s initial recommendations strongly advocated for in-person classes, these recommendations have been revised as it has become clear that more study is needed. This passage is from these guidelines:
“To be able to open schools safely, it is vitally important that communities take all necessary measures to limit the spread of the SARS-CoV-2. School policies must be flexible and nimble in responding to new information, and administrators must be willing to refine approaches when specific policies are not working…the AAP strongly advocates that all policy considerations for the coming school year should start with a goal of having students physically present in school. Unfortunately, in many parts of the United States, there is currently uncontrolled spread of SARS-CoV-2. Although the AAP strongly advocates for in-person learning for the coming school year, the current widespread circulation of the virus will not permit in-person learning to be safely accomplished in many jurisdictions.”
7) As parents, we are used to meticulously planning our children's lives far into the future. COVID-19 has shown us again and again that this is not always possible. Of course, we still need to anticipate challenges and make decisions, but we need to be much more comfortable with contingencies and accept the fact that things can change rapidly due to forces beyond our control. As the old joke goes: "How do you make God laugh? Tell him your plans." 8) The mitigation practices that have helped us get the virus under control in New York City over the past few months are vital, and need to be continued, especially as schools reopen and socialization outside of school increases. Masks work. Hand hygiene works. Social distancing works. Our overall rate of positive test results has recently stayed around or below 1%. Unfortunately, there is no book that will tell you exactly what to do in every situation - we all use judgement in deciding what to do when. Masks work, but most people don't wear them inside with their immediate family members who are taking precautions when away from home, or when eating at an outdoor restaurant with adequate separation from other tables. On the other hand, for example, we might wear them when outside with a more distant family member who has been traveling from areas with a higher infection rate. Even if your family remains vigilant, if your child spends a significant amount of time indoors and/or without masks with someone from another family who isn’t so careful, you can reverse all of those hard won gains. Ideally, your child's social life will be built around families that share your concerns and attitudes, so that you can safely maintain the socialization that is so vital for healthy cognitive and emotional development. As infection rates have fallen, so has our attention to detail. The virus isn’t gone, and the cold weather will probably make transmission more likely. Stay strong, watch the numbers, listen with an open mind, and take care of each other. And as always, I’m happy to chat or email with any of you about your individual concerns. Best, Mike Rothschild
1 note
·
View note
Text
In Response to Golden State Fur Con’s Relaxed Safety Rules Regarding COVID-19
Update: In response to the criticism, Golden State Fur Con held a poll on whether it should require (the previous policy) or only recommend vaccination and face masks and subsequently decided to revert to the previous policy. The convention was held with that previous policy in place.
I am so confused right now.
Earlier today, Golden State Fur Con, a furry convention set to take place on 8-10 April in Los Angeles, decided to drop their requirements for attendees to be vaccinated against COVID-19 and wear face masks during the convention, reducing them to recommendations. They cite the latest county public-health order which took effect today and reduces the requirements for "mega events" (events with large numbers of people) to recommendations.
There are a few possibilities I can think of for why this happened.
The organizers decided to do this voluntarily to align with government restrictions: Okay, I can understand wanting to ease restrictions related to COVID-19. But many events have imposed stricter requirements than the government's, so the organizers could still keep the previous requirements. I can respect people's choices to attend or not attend based on these restrictions, but making this change only a week before the event, when people's plans have been set and costs have been paid, makes this choice much more difficult. I ask the event organizers to please reconsider if they can.
The government does not allow events to impose further requirements related to COVID-19: I don't think this is the case here. Obviously, if the county (and the state) recommend that "mega events" verify vaccination status or a negative viral test, then events can choose to do that even if it's not required by the government. Nothing I can find in the county or state orders indicates that events cannot impose even stricter requirements if they so choose. Similarly, the county suggests that event hosts may require everyone to wear masks, again, even if it's not required by the government.
The organizers have some contractual obligation not to impose further requirements related to COVID-19: This is a possibility that was mentioned on Telegram, but to my knowledge this has not been confirmed. This seems somewhat plausible but in my mind this raises more questions than it answers.
This is an April Fools' Day joke: Hahaha, they got me good... This is in incredibly poor taste. They should've gone with the "fork fandom" thing that everyone else is doing today. (Maybe post a picture with fifty forks or something based on the theme.)
If you are still planning to attend, I highly recommend that you continue to adhere to the previous requirements. Get vaccinated (and boosted) if you can, and wear a face mask. Also consider getting tested before and after the convention to reduce your risk further.
0 notes
Photo

Vaccine hesitancy in Pakistan heightens risk of COVID resurgence
Vaccine hesitancy in Pakistan heightens risk of COVID resurgence

Islamabad, Pakistan – Pakistan’s success at managing the coronavirus pandemic – with relatively low rates of severe disease and death – and distrust of government-led and foreign-funded public health initiatives has driven vaccine hesitancy, which could put the country’s fragile gains against COVID-19 at risk, say experts and officials.
Since the pandemic began, Pakistan, a country of 220 million people, has registered more than 586,000 cases of the virus, with 13,128 deaths, as per government data.
Its current case-fatality rate of 2.2 percent is comparable to countries such as France and Canada – and is slightly higher than the United States – but is extremely low when its very low rate of testing is accounted for.
Pakistan conducts 0.18 tests per 1,000 people, compared with 4.62 per 1,000 in France or 2.76 per 1,000 in the US, as per government data.
In February, the country opened up vaccinations for hundreds of thousands of front-line healthcare workers across the country, with the arrival of more than 500,000 doses of the Chinese Sinopharm vaccine donated by the Chinese government.
Almost immediately, however, the campaign hit a snag.
“Even in the healthcare community, people thought that taking the vaccine might be harmful,” says a senior health official involved in vaccination efforts in Sindh province, which saw some of the worst of Pakistan’s COVID-19 pandemic.
The official spoke on condition of anonymity.
While thousands of healthcare workers registered themselves for the vaccine, initial rates of vaccination were slow, with doctors saying they were concerned about possible side-effects or reactions to the vaccine.
In the first two weeks after vaccinations began, only 32,582 front-line healthcare workers in Sindh, out of an eligible 78,000, had gotten their first jab of the vaccine, as per government data. In other provinces, the situation was even worse.
“Initially, people did not get vaccinated and a lot of people were concerned about reactions ,” says Dr Ahmed Zeb, a physician in the northwestern city of Peshawar, which saw hospital intensive care units overflowing in June, during Pakistan’s first peak of coronavirus cases.
Dr Faisal Sultan, Pakistan’s health minister, says the hesitancy has been driven by healthcare workers “over-analysing the data”.
“That is a hazard in today’s world, with a number of vaccines available and people looking at all the pros and cons and analysing efficacies, and sometimes losing sight of the fact that for the individual the most important number to remember is the protection against severe disease,” he told Al Jazeera.
“And all the licenced vaccines protect against severe disease in the 90 percent .”
So far, a month after vaccinations began, Pakistan has only administered 197,000 doses of the vaccine, or 0.09 vaccinations per 100 members of the population, putting it almost dead last in countries where vaccination data is available, according to the Our World In Data dataset.
Moreover, as the vaccination programme moves towards getting senior citizens their jabs, the lack of public buy-in is clear.
Only 240,000 out of an estimated eight million citizens over the age of 65, or three percent, have so far registered to receive the vaccine in the next phase, according to government data.
Why the hesitancy?
So what is driving this hesitancy and could low rates of vaccination drive a later resurgence of the coronavirus?
Dr Faisal Mahmood, head of the infectious diseases department at the Karachi-based Aga Khan University Hospital, says there are “many reasons” for the hesitancy but one stands out.
“In a small survey I did, the most common reason concerns regarding safety,” he says. “There is an inherent fear in some to get the vaccine, in some fuelled by distrust of the data, or perhaps due to ‘news’ received from social media.”
Pakistan is currently administering doses of the Chinese Sinopharm vaccine, with 14.6 million doses of the Oxford-AstraZeneca vaccine due to arrive in two batches in March and between April and May through the global COVAX initiative.
The country has also approved the use of the Russian Sputnik V vaccine.
All three vaccines have passed peer-reviewed phase III clinical trials and are in use in at least 10 countries collectively, according to medical journal The Lancet.
“We always have vaccine hesitancy in Pakistan,” says Dr Wajiha Javed, the head of public health at the multinational pharmaceutical company Getz Pharma’s Pakistan division.
“People don’t understand scientific data, if it gets in the hands of people who are not educated enough to understand it .”
Dr Javed said that qualified doctors in her own company had refused to take the vaccine “because they don’t have good information”.
Rumours of the vaccine’s safety were not helped by the provincial health minister in Punjab province, the country’s largest, saying during a press conference that citizens took the vaccine “at their own risk”.
By the end of February, levels of vaccine uptake by healthcare workers were so low that Sindh’s health minister ordered all government healthcare workers to take the vaccine or face disciplinary action, with similar orders given by directors at main government hospitals.
According to the country’s health ministry, meanwhile, there has not been a single case of serious side-effects from the vaccine reported in Pakistan since vaccinations began.
The concerns around safety alone, however, may not be enough to fully explain the hesitancy, says Maha Rehman, a data analytics specialist and member of faculty at the Lahore-based LUMS University.
“Efficacy data alone is not enough to scepticism around the vaccine rollout,” she says. “The overall level of trust in the health service provider is critical.”
Pakistan consistently ranks low on global healthcare indicators such as access to healthcare and child mortality.
It is one of two countries in the world where polio remains endemic and faces a number of other health challenges.
“People don’t really trust the government,” says Rehman.
“They don’t trust what vaccine they will get, will it be a trial, will it be a placebo? There needs to be an active policy shift that everything is being done very, very transparently.”
Health Minister Sultan says that concern may not be relevant, pointing out that vaccines have been developed by international companies and are being administered worldwide.
“At the end of the day, people do know that the vaccines have not been made in a backroom by anyone, they have been made by leading entities in advanced countries who used their technological muscle billions of dollars,” he says.
That, however, opens a different kind of distrust, say experts.
“There is this conception that it is foreign-funded, so there must be some other agenda, why can’t our own government look into it?” says Dr Javed, explaining a trend that has driven the country’s challenges in eradicating polio.
Polio vaccine refusals in Pakistan have grown because of misinformation about the foreign-funded vaccination programme being harmful to children’s health.
‘What difference does it make?’
In addition to hesitancy around the vaccine itself, doctors say there is also a sense of indifference among the general public regarding the virus, given Pakistan’s relatively low number of deaths and cases of severe disease from COVID-19.
“There is a sense of why should we get it, what difference does it make, corona is not a major issue,” says Dr Adnan Khan, a public health researcher and infectious disease specialist. “Mostly it is indifference, that what’s the need to for getting the vaccine when corona was not that big a deal.”
Khan said that when he got the first dose of his vaccination last week, none of the staff who administered the injection to him had gotten the jab themselves, despite being eligible.
“Even now, I still run into people who say that what is this corona that you are talking about? I still wear my mask and I am probably the only person who is wearing a mask in an overwhelming majority of situations.”
During the country’s first peak of coronavirus cases in June, Pakistan saw cases rising by more than 6,000 each day, with daily deaths peaking at 155 on June 19.
At the time, intensive care units in main cities were beginning to turn patients away for a lack of ventilators.
As cases subsided, however, so did social-distancing measures and government-mandated restrictions on gatherings.
The country’s second peak hit in late November, and appeared to be shallower and more sustained, with cases still not back down to the levels seen in between the peaks.
The slower rate of cases and deaths, say experts, has led to public indifference regarding the seriousness of the virus.
“There are people who don’t even believe in COVID here, so how would you find people to take the vaccine?” asked the senior Sindh health official.
The risks created by the rates of vaccination remaining low, however, are very real.
“The risk to Pakistan or any country where the vaccination rates remain low is that here will be chances of a resurgence and the resurgences will impact our businesses ,” says Health Minister Dr Sultan.
“Our ability to resume normal is heavily dependent on having community-level immunity and the best way to get that is to get vaccinated.”
Dr Mahmood, the infectious disease specialist, agrees, although he also stressed that vaccines were not a silver bullet for the pandemic and that continued social-distancing restrictions were required.
“Without the vaccine, we will always be under the threat of more surges,” he said. “That is not to say that this is not possible even with the vaccine, however, the chances do drop.”
Momentum picking up
For the government, the issue of the slow vaccine distribution is more a question of time and momentum than one of serious vaccine refusal.
“The hesitation is based on doctors and nurses looking and asking each other whether their peers and opinion leaders have taken the vaccine,” says Dr Sultan.
“This is not strange, it happens in every country and is happening in Pakistan as well.
“Gradually we are seeing a good pick up of it. And we are seeing that as well.”
This week, daily vaccination numbers went up to about 15,000 per day countrywide, from 3,000 per day earlier in the campaign, according to government data.
Doctors, too, say they are beginning to see the campaign pick up momentum.
“Once people started getting the vaccinations and they saw that people are not suffering side effects ,” says Dr Zeb, the physician in Peshawar.
“The awareness is getting better and the number of people who are getting vaccinated is increasing.”
Zeb, who works with a doctors’ union, said his organisation’s data showed that only 36 healthcare workers were vaccinated in the first four days of the campaign in Peshawar but that there were currently between 70 and 80 doctors being vaccinated each day at his hospital alone.
As momentum for vaccinations picks up, Pakistan’s challenges may shift from being demand-side to supply-side.
Currently, the country has confirmed supplies of roughly 15.85 million doses of the Sinopharm and Oxford University-AstraZeneca vaccines (both requiring two doses per person) arriving through Chinese government grants and the COVAX initiative by the end of May.
In a country of 220 million, that will not be near enough to cover enough of the population to establish herd immunity.
“By the end of the year, our estimate is that about between 45 to 50 million people,” says Health Minister Sultan.
“We will get those from whatever entities make it available, largely COVAX and then whatever .”
Pakistan’s government has also authorised the private sector to acquire government-approved vaccines for sale, although no company has yet been able to do so due to a shortage of global vaccine supplies.
“If someone wants to buy it separately, we will not stop them, that path is available,” says Sultan.
“We will control the prices, but the price control will be reasonable.”
Others in the sector, however, are sceptical that the distribution of vaccines will remain equitable if there is a shortage of free government vaccines and an open private market.
“The haves will have it and the have-nots will not be able to afford it,” says Dr Javed.
Read full article: https://expatimes.com/?p=18763&feed_id=36276
0 notes