#suffer similar consequences from being on the frontlines for such a long time
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
When “GIF” was named word of the year in 2012, Oxford Dictionaries U.S.A. credited Tumblr for pushing the word.
Text
was discussing the living situations of the landau siblings last night and whilst gepard technically resides in an apartment in belobog he spends as much time as humanly possible alternating between the frontlines and the barracks. there isn’t much of him to be find there, it’s relatively modern ( by belobogs standards ) but there’s something very impersonal about it. serval left their fathers estate as soon as she could and gepard stayed as long as he could because it was what was best in his eyes. if he is at the epicentre of their fathers expectations serval has her freedom and lynx can live a life unburdened by their family name. I do believe after he leaves it’s quite possible that Lynx might stay with serval.
#he suffers from chronic nightmares and doesn’t sleep soundly on his own very often#he’s prone to bouts of insomnia but many of the soldiers#suffer similar consequences from being on the frontlines for such a long time#so they all sorta band together and look out for each other#ooc.
7 notes
·
View notes
Text
“How long, God?” said Habakkuk.
This is it! COVID19, and a week of isolation (among other things, as you would soon find out) has led me to this: A BLOG! So keep your Pickpocks and Sneepchats – I am a man of culture!.. who will now rant his heart out like an everyday highschooler. But trust me, with a title like that? You know it’s about to get... juicy. To prelude how this’ll go, let me just say, before everything else, “let’s stay calm”. That sounds silly, because never in the history of calming down has anyone calmed down when told to calm down, but trust me, there’s a point to all this. And my hope is that we can all reason with each other, see where other people are coming from, and, God-willing, be able to understand each other a little better.
This will also be shared on Facebook, and with that, I urge people to ENGAGE in civil conversation with people who differ in beliefs and opinions. I’m not a fan of echo chambers where everything you hear is everything you agree with. Read about confirmation bias if you have extra time. I’m sure we all do.
Oh, by the way, this is going to be about politics. Remember when I said it’s about to get juicy?
Keep in mind, this is a blog, not a sermon. I’m no pastor, I’m just a person with words, and a LOT of frustrated questions. I write all these knowing that at some point, I could be wrong, as I am always prepared to be. Not the first time as well, but take it as “I am willing to be wrong in public, so as to be an example to others”.
And with that, let’s dive right in:
“Everyone must submit himself to the governing authorities, for there is no authority except that which God has established. Consequently, he who rebels against authority is rebelling against what God has instituted, and those who do so will bring judgment on themselves.”
If this is your first time reading those words in that order, congratulations, you are now acquainted with the first few words of Romans chapter 13. These words are set in stone, and by all means, uncontestable.
But let’s move over to the book of Habakkuk, where that question in the title came out. To summarize, Hab’s just going ham– laments of violence everywhere, evil deeds being done in broad daylight, the law paralyzed, the wicked outnumber the righteous, justice perverted, you know, a bygone age. Whatever do you mean it sounds eerily familiar and similar to current world events? That’s crazy-talk.
(A small spoiler on how that book ended: Habakkuk’s fine. So that’s a relief.) Alright, hear me out: is there a way to respectfully prod government leaders to action? The common argument against that is “don’t say anything bad or disrespectful of them, they are anointed leaders” (see Romans 1 above). And I must confess that I am guilty of political satire (because that slogan in the congress? Comedy gold! Imagine them pasting that thing together with Elmer’s glue. And the Enrile memes? Never not funny– that man is Jurassic!) Guilty as charged, humor has always been my defense mechanism. But besides that is a desire for accountability. I follow the rules and pay my taxes just like everybody else – granted, I have never voted. Although, I sleep soundly at night knowing I did not put anybody in power, regardless of what you think of our leaders.
But tell me what you think of my stance: I treat the government as I would my uncle. He’s there as an authority figure over me, I wish we hung out more, I get a few laughs making fun of him from time to time, I get a few gifts once in a while, the works. Now say he’s driving, and I’m a passenger in the car, and he’s a bit... inebriated. Head swaying, cross-eyed, shlurs hish wordsh shomething like thish.
Don’t I get a say in the matter? I mean, to go full-circle, the law is about to disobey the law! Yes, pray for safety, but to stay silent on the off-chance he gets offended and go “Shumunod ke neleng kashi!”? (”Jush do ash i shay!” for all my English-speaking friends) Or, say that he started smoking, which situationally, is more or less higher risk. Is it wrong for me to tap him on the shoulder and ask him to stop?
I know I’m not alone in saying this: taking part in speaking out is one of the few ways we can demand accountability and be involved in this democracy. Say what you will of that form of government, Winston Churchill definitely did. He said, “democracy is the WORST form of government, except for all other forms that have been tried from time to time.” I thank God for the freedom to express our faith – that’s democracy and not a divine monarchy, where our leaders are infallible royal deities who could do no wrong and immune to criticism.
We are not about to write signs, print tarpaulins and protest in the streets – that isn’t the way, at least for me and others I know. I have been labeled a rebel, while others I know have been called worse, but I think rebellion starts when you stop following the law, evade your taxes, resort to violence, speed through a red light – you can even consider calling politicians names as rebellion. (though to call Enrile REALLY old is not really an insult – it’s an observation.)
Again, this is a blog, not a sermon. Feel free to disagree or try to change my mind, I still love you <3. And remember: Echo chambers only cultivate confirmation bias.
You may say, “but this isn’t about you, man” And to that, I say I know, and I hope that it wouldn’t be about me, because that’s Ad Hominem If I ever heard one.
Now, on a serious note: people are dying out there. We all have friends in the frontlines that are tackling this pandemic face-to-face, and to hear about face masks paid for by hospitals in full, but going to politicians’ pockets is nothing short of infuriating. Billions took out of the budget that could’ve been used to help, VIP testing for senators with the gall to take time writing that slogan, time that could’ve been used to help out the needy. Forgive me for being frustrated to the brim, I’m not the type to go lalalala, I’m not hearing this. This will not destroy us, and like Habakkuk, it will end well. But to sit tight and say “at least I’m safe” while others are suffering doesn’t sit well with me. I pray I never lose sympathy. If anything I pray for more compassion to move and lend a helping hand. I’ll end with my favorite Bible phrase: “The Lord is good, and His love endures forever.” But the politicians? I have some opinions. I’m about to get attacked, aren’t I?
1 note
·
View note
Photo

A Federal Heroes Compensation Fund
The latest news about Workers Compensation in Ontario California... A Federal Heroes Compensation Fund: The COVID-10 pandemic has the potential of generating an enormous number of occupational illness claims from health care workers [HCW] and first responders [FR]. Several governmental leaders have called for a nationalized workers' compensation benefit program to handle the surge of claims. The ability of the patchwork of individualized state programs to handle the potential monumental surge of claims has come into question. The efficiency and effectiveness of a multitude of non-integrated and stand-alone schemes of workers' compensation will be challenging. The fractionalized handling by multiple jurisdictions will produce an inconsistent and erratic benefit delivery solution that will impact the strategy to provide the best public health initiative nationally to cope with the COVID pandemic.Federal Government Will Provide a Uniform ProgramTypical federal benefits provide a uniform national solution. Issues as to exposure and casual relationship can be standardized across all claims. Fiscal stability of the states and insurance companies can be obtained through federal administration and financing of both administration and delivery, without regard to state budgets and insurance carrier premium dollars. Integration with collateral benefit programs such as Medicare and Medicaid can be fashioned in an integrated solution. State unemployment, pension and supplemental benefits can be applied, setoff and recovered on a common basis thorough a nationalized central Federal agency management.State Programs StressedThe state workers compensation structure will be seriously stressed to handle the growing number of potential claims. HCW and FR are experiencing increased rates of COVID-19 illness and fatalities. The workers are fulfilling their heroic frontline roll in the battle against the disease and enduring enhanced risk that threaten: themselves, their families, health care facilities and the community at large.Workers' compensation insurance carriers are not prepared for these unanticipated catastrophic losses. Premium coverage for this type of “once in an 100 year event” has not been calculated into the rates. The losses are not backstopped by other revenue sources. The economic consequences to the already monetarily and administratively challenged state budgets could be severe and could result in state and local public and private entity bankruptcy. State are overwhelmed in processing unemployment benefits.The fractionalized state programs are not equipped to handle the adjudication and administration of the exponential volume of potential claims and multitude of complicated legal issues. Legal jurisdictional issues over state-wide partnerships alone will lead to complicated and prolonged litigation. As states and other local public entities enlist armies of volunteers from all over the nation, to go to specific epicenters of disease, questions over jurisdiction will arise. The extra-territorial and intra-territorial claims involve complex legal issues that will require duplicative litigation efforts. Additionally, the benefit programs throughout the United States are not equal and will create a wide disparity of benefits. Volunteers may choose to work in a jurisdiction offering the best benefit package instead of where the actual need exists for trained staff.Federal Government Has Done This BeforeIn the past the federal government has stepped up to the plate and similar fact situations and helpful and has provided a uniform federally-based workers compensation program that can't be managed in a uniform, efficient, equitable and summary nature.Examples of the programs are: James Zadroga 9/11 Health and Compensation Reauthorization Act; James Zadroga 9/11 Health and Compensation Act of 2010; Ray Pfeifer, and Luis Alvarez Permanent Authorization of the September 11th Victim Compensation Fund Act; Smallpox Emergency Personnel Protection Act of 2003 [SEPPA]; and Energy Employees Occupational Illness Compensation Program Act of 2000.Proposed “Heroes Fund”NY Governor Andrew Cuomo has called for a COVID-19 fund to compensate frontline workers of he pandemic. He said, “U. S. Senator Chuck Schumer (D-NY) unveiled, a COVID-19 “Heroes Fund,” proposal to reward, retain, and recruit essential workers. The Schumer-led, proposed “Heroes Fund” consists of two major components: a $25,000 premium pay increase for essential workers, equivalent to a raise of $13 per hour from the start of the public health emergency until December 31, 2020, and a $15,000 essential worker recruitment incentive to attract and secure the workforce needed to fight the public health crisis.NY Governor Andrew Cuomo said, “All those essential workers have to get up every morning to put food on the shelves and go to the hospitals to provide health care under extraordinary circumstances.” He urged the Federal government to pay frontline workers “hazard pay” for risking their lives while working during the COVID-19 pandemic. “This crisis is not over yet, and as long as these workers continue to work and expose themselves to the virus, they should be properly compensated.”US Senator Chuck Schumer stated, “And this proposed ‘Heroes Fund' would provide premium pay to these essential workers—the doctors and nurses, grocery store workers, transit workers, and more who are central to fighting this crisis—and would establish an incentive system to retain and recruit the workforce needed for the long months to come. Essential frontline workers sacrifice daily for our collective health and well-being, and I, along with my colleagues, are fully committed to supplying these heroes the financial support they deserve.” Healthcare workers and first responders are the soldiers in the war against the covert epidemic. The nation should meet its legal and moral responsibility to adequately compensate them for injuries occurring in their efforts to defeat the virus. Congress should draft and pass and mediately a federal workers compensation fund that will provide adequate benefits and efficient and remedial nature to the nations healthcare workers and first responders. The president should support this effort, to help the "soldiers and the war for the Nations health,” and signed Federal legislation to assist these individuals who have fought so hard to save the nation.As the first wave of the pandemic continues to surge across the nation and world, it is incumbent upon the Congress to insure the existence of an adequate and uniform benefit program is in place.The battle against COVID-19 will be long and tedious. The nation must provide a uniform, remedial and efficient benefit program to protect our HCWs and FRs and protect their families. This is national effort and should not put one state conflicting against another. The time for Congress to enact a Federal Heroes Compensation Fund is now.Related information:Is the workers' compensation system ready for the 2019-nCoV [coronavirus] virus? Live UpdatesGovernor Murphy Signs Legislation to Expand Family Leave Protections During COVID-19 Outbreak 4/22/20More than 9,000 U.S. health-care workers have been infected with the coronavirus Wahington Post 4/14/2020The Coronavirus Preparedness and Response Supplemental Appropriations Act, [CPRSAA] 2020 (March 6, 2020)CDC Coronavirus Guidance Sets a Standard for Employer Responsibility and Liability 2/28/2020New Jersey Benefits and the Coronavirus (COVID-19): What Employees Should Know 3/17/2020OSHA Steps Backwards on COVID-19 Occupational Exposures 4/12/2020...Jon L. Gelman of Wayne NJ is the author of NJ Workers' Compensation Law (West-Thomson-Reuters) and co-author of the national treatise, Modern Workers' Compensation Law (West-Thomson-Reuters). For over 4 decades the Law Offices of Jon L Gelman 1.973.696.7900 [email protected] has been representing injured workers and their families who have suffered occupational accidents and illnesses.Blog: Workers ' CompensationTwitter: jongelmanLinkedIn: JonGelmanLinkedIn Group: Injured Workers Law & Advocacy GroupAuthor: "Workers' Compensation Law" West-Thomson-Reuters https://bit.ly/2zuaKSM #workerscomplawyerie #inlandempire #lawblog #workinjurylawyer
1 note
·
View note
Text
Facing Two Fronts: COVID-19 amidst the Yemeni Civil War | CSPPS
See on Scoop.it - COMPARE RISK COMMUNICATION
Facing Two Fronts: COVID-19 amidst the Yemeni Civil War CSPPS Coordinated Response to Support Local Action during COVID-19: an interview with Yemen’s CSPPS Member Youth Without Borders Organization for Development (YWBOD) At times of acute crisis, it is easy to lose sight of the bigger picture. A global pandemic, like the one we are facing today, is a perfect example of where our natural response is to focus solely on the aspects which are most acutely affected: a nation’s healthcare system and its economy. However, the trickle-down effect of COVID-19 can seriously affect other crucial areas of life, particularly peace and conflict. CSPPS has launched this series of articles, which zooms in on the role of civil society in supporting local response action. Via interviews with frontline responders, we discuss the short-term and long-term effects COVID-19 is having on prospects for peace and stability in their countries. “Our world faces a common enemy: COVID-19. The virus does not care about nationality or ethnicity, faction or faith. It attacks all, relentlessly … Let’s not forget that in war-ravaged countries, health systems have collapsed. Health professionals, already few in number, have often been targeted. Refugees and others displaced by violent conflict are doubly vulnerable. The fury of the virus illustrates the folly of war.” (UN Secretary-General’s Appeal for Global Ceasefire, 23 March 2020) Once the magnitude of the current pandemic became clear, so did the fact that those in a state of ongoing conflict will be impacted most severely. Following the appeal by UN Secretary-General António Guterres, the Saudi-backed coalition declared a two-week unilateral truce on April 8th in an attempt to contain the devastating impact of COVID-19 in an already war-torn Yemen. However, this has not been upheld. Instead, conflict has spiked over the past weeks, leading to multiple deaths on top of the already towering death toll. And although the Saudi coalition announced a month-long extension of their unilateral ceasefire on April 24th, scepticism about their actual compliance to this statement cannot be said to be unfounded. The Yemeni Civil War has been ravaging the country since March 2015, after Houthi opposition forces overran the capital Sana’a in 2014, which prompted an international response, led by Saudi Arabia in support of current Yemeni President Abdrabbuh Mansur Hadi. The Saudi response to the Yemeni situation can only be described as abhorrent: civilians, young children, nobody has been spared in this struggle for power. A draft of the 2017 UN report on children and armed conflict condemned the Saudi coalition, stating: “In Yemen, the coalition’s actions objectively led to the listing for the killing and maiming of children, with 683 child casualties attributed to this party, and, as a result of being responsible for 38 verified incidents, for attacks on schools and hospitals during 2016.” The struggle over control of the nation has left approximately 80% of the population relying on humanitarian aid and has led to more than 100,000 casualties due to the violence, of which 12,000 are civilian. Additionally, more than 85,000 people are said to have died from famine as a direct consequence of the war. All the while, the country suffers from the worst epidemic of cholera in modern history, making the Yemeni situation the world’s worst humanitarian crisis. A looming pandemic over this already dire situation only intensifies the need for a sustainable peace. For the third article in this series, the Secretariat of the Civil Society Platform for Peacebuilding and Statebuilding (CSPPS) discussed the reality of the ceasefire in Yemen in light of COVID-19 with Maged Sultan, member of CSPPS and Chair of the Youth Without Borders Organization for Development (YWBOD) in Yemen. “In spite of the pandemic spreading all over the world, the warring parties in Yemen pay no attention to work together to face this crisis. Instead, the violence and armed conflict continue, and each party is trying to gain more political and military victory over the other.” Despite the ceasefire declared by the Saudi- and United Arab Emirates-led coalition, which promised to stop airstrikes for two weeks, the opposing Houthis have come with unreasonable conditions from their end and have called the declared ceasefire a “ploy”, Sultan explains. Both parties have since continued their struggle for power. Since the failed call for a nation-wide ceasefire, Sultan states, “the Houthis have escalated violence against the forces of the internationally recognised government in Ma’rib, the north of Yemen, and they could gain some more geographical areas and military camps there. Also in Al-Jawf, violence continues, and the internationally recognised government forces continue to try to restore some of the areas lost to the Houthis. Just two days ago, they managed to regain one of the military camps there.” “The Houthis have escalated violence against the forces of the internationally recognised government in Ma’rib, the north of Yemen, and they could gain some more geographical areas and military camps there. Also in Al-Jawf, violence continues, and the internationally recognised government forces continue to try to restore some of the areas lost to the Houthis. Just two days ago, they managed to regain one of the military camps there.” The Houthis are imposing a ban on travel in Taiz, and conflict has soared since the start of the pandemic. In a similar manner, the Southern Transitional Council (STC), which seeks to separate the South of Yemen from the rest of the nation, continued to exercise its power over Aden, undeterred by the Riyadh Agreement struck last November. By issuing decrees of curfew and other measures, supposedly to contain the spread of COVID-19, the STC had found additional means of asserting its control over the region. On April 26th, this escalated into a declaration of self-rule, completely shattering the Riyadh Agreement and, with it, any prospect of imminent peace. The independent control over the Southern governates only further jeopardises the possibility of an upheld, nation-wide ceasefire in Yemen, bringing the state of the nation to a political as well as military boiling point amidst COVID-19. “I just want to say again: the warring parties in Yemen did not respond positively to the global spread of the virus. Instead, they take this matter as a means of gaining more political or military control.” On April 10th, Yemen’s first case of COVID-19 was confirmed in Hadhramaut, sparking panic amongst its incredibly fragile population. To illustrate the extent of this fear, Sultan told us of the many posts on social media that circulated after the announcement of the case, calling for the patient to be killed in order to spare the rest of the population. In a society where the majority of the population owns weapons, a scare like this can easily escalate, or result in a much faster spread of the virus when suspected cases are withheld out of fear of the repercussions. Misinformation and fear amongst a fragile population, as we have seen in our second article on the Liberian context, will undeniably worsen any status quo. In this context, amidst the world’s worst humanitarian crisis, a global pandemic could very well be the final blow to whatever is left of the Yemeni nation. “The majority of the population (more than 70%) depends on daily earnings, aside from the exorbitantly high percentages of poverty and unemployment across the country. A curfew will take away those daily earnings, and there are no alternatives provided, not by the government, nor by other actors. What will such people do? Robberies and other crimes are the expected consequences, which poses a real threat to national cohesion and communal peace.” Sultan recalls a meeting he had with security forces two days before our conversation, in which he asked what procedures were being put in place to prepare emergency security teams in the event of the virus spreading within the city. “Nothing”, was their response, “there are security teams in place, but they are not prepared to work effectively within the COVID-19 situation. Most likely, policemen will run away out of fear of infection, rather than enforce peace.” As regards gender-based violence especially, Sultan foresees a surge once a nation-wide curfew is imposed. “Once men and women will be confined at home, there will be an increase in domestic violence. This is exactly what happened in 2015, at the beginning of the war: because people were forced to stay at home, the terrible economic situation and the lack of awareness surrounding gender equality, a lot of gender-based violence occurred. On the other hand, if security provisions will fail out of fear amongst the security forces, we can expect to see an escalation of cases of rape and sexual harassment on the streets as well.” As no security institution is working adequately at the moment, especially not with the looming pandemic, local insecurity and conflict are on the rise. Sultan, as Chair of the Youth Without Borders Organization for Development and member of CSPPS, has therefore initiated a peacebuilding project, in collaboration with the local police and communities. In Taiz, they install security cameras in some high-risk areas which are directly connected to a server based in the police station, to reinforce whatever sense of security there is left. Additionally, they engage in the distribution of masks and hand sanitizer, and have started public sensitisation campaigns, as have other civil society organisations across Yemen, to raise awareness about social distancing and other precautions to avoid infection. In order to support the faltering healthcare system (only half of Yemen’s healthcare facilities are still fully functional, and there are only 500 ventilators available in the whole country), YWBOD is providing logistic and medical requirements like oxygen tanks and hand sanitizer to two emergency units, but this effort does not suffice as challenges are mounting nation-wide. As UN Secretary-General Guterres put it in his most recent appeal on April 23rd: “The COVID-19 pandemic is a public health emergency – but it is far more. It is an economic crisis. A social crisis. And a human crisis that is fast becoming a human rights crisis.” “People – and their rights – must be front and centre. …. We have seen how the virus does not discriminate, but its impacts do – exposing deep weaknesses in the delivery of public services and structural inequalities that impede access to them. We must make sure they are properly addressed in the response.” (Secretary-General of the United Nations, 23 April 2020) Upon the question whether Guterres’ appeal for a global ceasefire has been fruitful so far, Sultan states: “As the world is busy with the coronavirus, the conflicting parties of Yemen abuse the situation in their favour, rather than taking actions and measures which can bring solutions to the virus.” Sultan urges for the Riyadh Agreement to be enforced, and for the international community to put further pressure on all the warring parties, whether local or international. “Especially amidst COVID-19, a nation-wide ceasefire to solve this immense humanitarian crisis should be the priority of everyone involved. This, however, requires voices from inside the country, as well as real pressure from the global level. In order to do so, we need to meet the urgent needs of a ceasefire, mobile resources as well as joint efforts to fight COVID-19 from a holistic perspective.” The international community has an obligation to protect and respect human rights, not least the rights of the most vulnerable. More than 6.7 million Yemenis, an unprecedented figure, were already in need of assistance before the COVID-19 outbreak. The pandemic can only worsen their predicament. In his recent briefing to the United Nations Security Council, UN Special Envoy for Yemen Martin Griffiths painted a picture of the current situation, saying that “Yemen cannot face two fronts at the same time: a war and a pandemic. And the new battle that Yemen faces in confronting the virus will be all-consuming. We can do no less than stop this war and turn all our attention to this new threat.” Facing two fronts, Sultan calls upon the international community, including the International Dialogue on Peacebuilding and Statebuilding, of which CSPPS is part, to support the call for a true ceasefire. Yemen needs a nation-wide ceasefire, to be upheld, respected and supported by all stakeholders. As CSPPS, we support Sultan in his plea, and call for a global community in which members hold each other accountable for their actions, and the devastating consequences thereof. The urgency is undeniable. Amidst this global pandemic, especially when it threatens those who have already lost so much, there is simply no more time left to lose. The time to act on peace is now. Article by Charlotte de Harder - CSPPS
0 notes
Text
New story in Health from Time: As U.S. Braces for Coronavirus to Spread, Hospitals Worry About Shortages
As doctors in the U.S. have watched Italy’s health care system buckle under the sudden strain of the coronavirus, the magnitude of the problems that could be heading their way have begun to sink in. The crises Italian medical staff have been reportedly facing — overwhelming conditions, choosing which patients get treatment, and desperately working to expand their manpower — are all things that hospitals in the U.S. could encounter if the virus continues on its path, doctors say.
“For me it flipped from, ‘This is a real concern, I wonder what’s going to happen’… to ‘Holy cow, I think we’re in trouble,’” says Laurel Fick, a residency director and an internal medicine physician at Ascension St. Vincent Hospital Indianapolis hospital, when she realized how grim the situation in Italy had grown.
As of Monday, the U.S. had more than 4,000 confirmed coronavirus cases, according to Johns Hopkins University, only a fraction of the approximately 28,000 cases in Italy. But the slow start of rolling out testing has made it impossible to know exactly how widespread the pandemic actually is in the U.S. What is clear is that the rate at which cases are increasing is similar to Italy’s trajectory. The Surgeon General said Monday that the U.S. is two weeks behind Italy.
“When you look at the projections, there’s every chance that we could be Italy,” U.S. Surgeon General Jerome Adams told Fox News on Monday.
As health care professionals watch the potential future unfold across the Atlantic, they are growing increasingly anxious that the novel coronavirus, which is particularly dangerous for the elderly and people with underlying medical conditions, could overrun the American healthcare system. As public officials and businesses try to enforce social distancing to slow the spread, hospital staff say they are concerned about shortages of specialized equipment like ventilators, hospital beds, masks and personnel. If the system grows too stretched, they worry they may ultimately have to ration health care.
For now, hospitals can only prepare for the worst. One estimate reportedly presented by the American Hospital Association predicts there could be 96 million cases of coronavirus in the U.S. in the next couple of months, with 1.9 million intensive care unit admissions, 4.8 million hospitalizations, and 480,000 deaths associated with the virus.
“We are not ready. We are not ready virtually anywhere in the country for that kind of onslaught on our health care system,” says Irwin Redlener, director of the National Center for Disaster Preparedness at Columbia University.
For instance, Redlener estimates that there are 95,000 intensive care beds in the country, but “even in the moderate attack rate of the coronavirus,” he believes there could be a need for more than double that number. He also believes the U.S. has only a “fraction” of the mechanical ventilators that could be needed, a device that will be crucial for a virus that aggressively attacks the lungs and for which there is no good substitute. A 2010 survey estimated that there were likely around 62,000 mechanical ventilators in U.S. hospitals.
The Trump Administration has slowly begun to publicly recognize the gravity of the situation hospitals and medical staff are facing. Health and Human Services Secretary Alex Azar acknowledged during a White House briefing on Sunday that a “pandemic like this runs the risk of exceeding our health care system capacity.”
In a sign of how difficult these resources are to come by as the pandemic spans the globe, Trump held a call with governors on Monday telling them they should seek crucial equipment on their own, according to a New York Times report. “Respirators, ventilators, all of the equipment — try getting it yourselves,” Trump reportedly said. “We will be backing you, but try getting it yourselves. Point of sales, much better, much more direct if you can get it yourself.”
Some of these supplies are available in the federally managed, secretive Strategic National Stockpile (SNS), which distributes supplies during crises like this one. On Sunday, Azar said there are “thousands and thousands” of ventilators available in the SNS, but cited national security reasons for not disclosing specific numbers of the supplies available.
Knowing their facilities cannot handle experts’ worst-case scenarios, doctors have been aggressively calling for social distancing to “flatten the curve,” or slow the rate at which the population gets infected and therefore keep the health care infrastructure from being overwhelmed. On Sunday, the Centers for Disease Control put out new guidelines recommending events with 50 or more people be cancelled for the next eight weeks, as well as events of any size where social distancing could not be incorporated.
By Monday, Trump was urging people to avoid gatherings of groups of more than ten. Several cities have now started cracking down on social life, closing restaurants and bars and asking residents to “shelter in place,” and businesses across the country have sent employees to work from home.
“I actually worry that there are a lot of individuals who are not taking it seriously,” says Avital O’Glasser, medical director for the Preoperative Medicine Clinic at Oregon Health & Science University in Portland. “I worry about the banter that people are still saying, ‘I’m going out to bars. I want to go celebrate St. Patrick’s Day. This isn’t going to affect me. I’m young and healthy. Why do I have to isolate myself?’”
If the country is unable to reduce its infection rate, the nation’s health care infrastructure will not be able to cope, and it could result in a decline of adequate care both for coronavirus patients and people suffering everyday health issues, complications or trauma, experts across the country worry.
On Friday, the American College of Surgeons released guidance on minimizing, postponing, or cancelling elective operations in the midst of the pandemic. The Surgeon General also tweeted for hospitals to consider stopping elective procedures, citing the tax it would put on personnel needed for coronavirus response. If there aren’t enough resources to provide proper continuing care to people with chronic illness, medical professionals say that in itself may also have long-term consequences in the health care system.
And while medical professionals are thinking that far ahead, they have more urgent advice. “If we don’t keep that curve flat, and try to keep the critical cases down to a minimum, we’re going to get to a point where we just don’t have enough resources,” says John Hick, medical director for emergency preparedness and emergency physician at Hennepin Healthcare in Minneapolis.
Hick worries about the number of ventilators available, as well as the number of extracorporeal membrane oxygenation, or ECMO, systems, which function like an external blood pump. “So that’s kind of what we’re wrestling with right now — in addition to just space and the staffing,” he said.
He also pointed to appropriate hospital beds as something difficult to work around, describing how unrealistic it would be, for example, to place an 80-year-old patient on a makeshift cot. “Their skin breaks down. A lot of times we have to position those patients differently in order to ventilate them appropriately,” he said. “There’s just no substitute for a good, quality hospital bed.”
Hospitals are also increasingly concerned about the short supply of the personal protective equipment (PPE) used to keep health care workers safe and healthy, like gowns, N95 respirators, surgical masks, gloves and eye protection.
“We’re seeing significant shortages of personal protective equipment and [a] shift to having to really conserve personal protective equipment to make sure that our nurses, physicians and others are adequately protected,” says Paul Biddinger, Vice Chairman for Emergency Preparedness in the Department of Emergency Medicine at Massachusetts General Hospital. “Every health care system has been having to very carefully determine how they allocate and use their PPE so that they try to preserve it to protect the workforce.”
As an increasing number of first responders are likely to come in contact with and contract coronavirus — and therefore be unable to continue working themselves — staffing could become a major problem. Facing furloughed workers, or workers simply exhausted after endless hours on the job, trained professionals out of the workforce may be looked to as standby substitutes. Health care professionals who are not normally considered frontline workers are also figuring out how they can jump in and get involved in the fight.
“I think we’re having to all get comfortable with the idea of practicing outside of our comfort zone,” Fick says. “I’m an internal medicine physician, I’m trained in critical care for my residency, but that was 10 years ago. I haven’t operated a ventilator in 10 years, but I’m preparing to rapid-fire relearn that skill in the event that I have to use that.”
from Blogger https://ift.tt/2wg35pI via SEO Services
from WordPress https://ift.tt/38RuEDa via IFTTT
0 notes
Link
As doctors in the U.S. have watched Italy’s health care system buckle under the sudden strain of the coronavirus, the magnitude of the problems that could be heading their way have begun to sink in. The crises Italian medical staff have been reportedly facing — overwhelming conditions, choosing which patients get treatment, and desperately working to expand their manpower — are all things that hospitals in the U.S. could encounter if the virus continues on its path, doctors say.
“For me it flipped from, ‘This is a real concern, I wonder what’s going to happen’… to ‘Holy cow, I think we’re in trouble,’” says Laurel Fick, a residency director and an internal medicine physician at Ascension St. Vincent Hospital Indianapolis hospital, when she realized how grim the situation in Italy had grown.
As of Monday, the U.S. had more than 4,000 confirmed coronavirus cases, according to Johns Hopkins University, only a fraction of the approximately 28,000 cases in Italy. But the slow start of rolling out testing has made it impossible to know exactly how widespread the pandemic actually is in the U.S. What is clear is that the rate at which cases are increasing is similar to Italy’s trajectory. The Surgeon General said Monday that the U.S. is two weeks behind Italy.
“When you look at the projections, there’s every chance that we could be Italy,” U.S. Surgeon General Jerome Adams told Fox News on Monday.
As health care professionals watch the potential future unfold across the Atlantic, they are growing increasingly anxious that the novel coronavirus, which is particularly dangerous for the elderly and people with underlying medical conditions, could overrun the American healthcare system. As public officials and businesses try to enforce social distancing to slow the spread, hospital staff say they are concerned about shortages of specialized equipment like ventilators, hospital beds, masks and personnel. If the system grows too stretched, they worry they may ultimately have to ration health care.
For now, hospitals can only prepare for the worst. One estimate reportedly presented by the American Hospital Association predicts there could be 96 million cases of coronavirus in the U.S. in the next couple of months, with 1.9 million intensive care unit admissions, 4.8 million hospitalizations, and 480,000 deaths associated with the virus.
“We are not ready. We are not ready virtually anywhere in the country for that kind of onslaught on our health care system,” says Irwin Redlener, director of the National Center for Disaster Preparedness at Columbia University.
For instance, Redlener estimates that there are 95,000 intensive care beds in the country, but “even in the moderate attack rate of the coronavirus,” he believes there could be a need for more than double that number. He also believes the U.S. has only a “fraction” of the mechanical ventilators that could be needed, a device that will be crucial for a virus that aggressively attacks the lungs and for which there is no good substitute. A 2010 survey estimated that there were likely around 62,000 mechanical ventilators in U.S. hospitals.
The Trump Administration has slowly begun to publicly recognize the gravity of the situation hospitals and medical staff are facing. Health and Human Services Secretary Alex Azar acknowledged during a White House briefing on Sunday that a ���pandemic like this runs the risk of exceeding our health care system capacity.”
In a sign of how difficult these resources are to come by as the pandemic spans the globe, Trump held a call with governors on Monday telling them they should seek crucial equipment on their own, according to a New York Times report. “Respirators, ventilators, all of the equipment — try getting it yourselves,” Trump reportedly said. “We will be backing you, but try getting it yourselves. Point of sales, much better, much more direct if you can get it yourself.”
Some of these supplies are available in the federally managed, secretive Strategic National Stockpile (SNS), which distributes supplies during crises like this one. On Sunday, Azar said there are “thousands and thousands” of ventilators available in the SNS, but cited national security reasons for not disclosing specific numbers of the supplies available.
Knowing their facilities cannot handle experts’ worst-case scenarios, doctors have been aggressively calling for social distancing to “flatten the curve,” or slow the rate at which the population gets infected and therefore keep the health care infrastructure from being overwhelmed. On Sunday, the Centers for Disease Control put out new guidelines recommending events with 50 or more people be cancelled for the next eight weeks, as well as events of any size where social distancing could not be incorporated.
By Monday, Trump was urging people to avoid gatherings of groups of more than ten. Several cities have now started cracking down on social life, closing restaurants and bars and asking residents to “shelter in place,” and businesses across the country have sent employees to work from home.
“I actually worry that there are a lot of individuals who are not taking it seriously,” says Avital O’Glasser, medical director for the Preoperative Medicine Clinic at Oregon Health & Science University in Portland. “I worry about the banter that people are still saying, ‘I’m going out to bars. I want to go celebrate St. Patrick’s Day. This isn’t going to affect me. I’m young and healthy. Why do I have to isolate myself?’”
If the country is unable to reduce its infection rate, the nation’s health care infrastructure will not be able to cope, and it could result in a decline of adequate care both for coronavirus patients and people suffering everyday health issues, complications or trauma, experts across the country worry.
On Friday, the American College of Surgeons released guidance on minimizing, postponing, or cancelling elective operations in the midst of the pandemic. The Surgeon General also tweeted for hospitals to consider stopping elective procedures, citing the tax it would put on personnel needed for coronavirus response. If there aren’t enough resources to provide proper continuing care to people with chronic illness, medical professionals say that in itself may also have long-term consequences in the health care system.
And while medical professionals are thinking that far ahead, they have more urgent advice. “If we don’t keep that curve flat, and try to keep the critical cases down to a minimum, we’re going to get to a point where we just don’t have enough resources,” says John Hick, medical director for emergency preparedness and emergency physician at Hennepin Healthcare in Minneapolis.
Hick worries about the number of ventilators available, as well as the number of extracorporeal membrane oxygenation, or ECMO, systems, which function like an external blood pump. “So that’s kind of what we’re wrestling with right now — in addition to just space and the staffing,” he said.
He also pointed to appropriate hospital beds as something difficult to work around, describing how unrealistic it would be, for example, to place an 80-year-old patient on a makeshift cot. “Their skin breaks down. A lot of times we have to position those patients differently in order to ventilate them appropriately,” he said. “There’s just no substitute for a good, quality hospital bed.”
Hospitals are also increasingly concerned about the short supply of the personal protective equipment (PPE) used to keep health care workers safe and healthy, like gowns, N95 respirators, surgical masks, gloves and eye protection.
“We’re seeing significant shortages of personal protective equipment and [a] shift to having to really conserve personal protective equipment to make sure that our nurses, physicians and others are adequately protected,” says Paul Biddinger, Vice Chairman for Emergency Preparedness in the Department of Emergency Medicine at Massachusetts General Hospital. “Every health care system has been having to very carefully determine how they allocate and use their PPE so that they try to preserve it to protect the workforce.”
As an increasing number of first responders are likely to come in contact with and contract coronavirus — and therefore be unable to continue working themselves — staffing could become a major problem. Facing furloughed workers, or workers simply exhausted after endless hours on the job, trained professionals out of the workforce may be looked to as standby substitutes. Health care professionals who are not normally considered frontline workers are also figuring out how they can jump in and get involved in the fight.
“I think we’re having to all get comfortable with the idea of practicing outside of our comfort zone,” Fick says. “I’m an internal medicine physician, I’m trained in critical care for my residency, but that was 10 years ago. I haven’t operated a ventilator in 10 years, but I’m preparing to rapid-fire relearn that skill in the event that I have to use that.”
0 notes
Link
As doctors in the U.S. have watched Italy’s health care system buckle under the sudden strain of the coronavirus, the magnitude of the problems that could be heading their way have begun to sink in. The crises Italian medical staff have been reportedly facing — overwhelming conditions, choosing which patients get treatment, and desperately working to expand their manpower — are all things that hospitals in the U.S. could encounter if the virus continues on its path, doctors say.
“For me it flipped from, ‘This is a real concern, I wonder what’s going to happen’… to ‘Holy cow, I think we’re in trouble,’” says Laurel Fick, a residency director and an internal medicine physician at Ascension St. Vincent Hospital Indianapolis hospital, when she realized how grim the situation in Italy had grown.
As of Monday, the U.S. had more than 4,000 confirmed coronavirus cases, according to Johns Hopkins University, only a fraction of the approximately 28,000 cases in Italy. But the slow start of rolling out testing has made it impossible to know exactly how widespread the pandemic actually is in the U.S. What is clear is that the rate at which cases are increasing is similar to Italy’s trajectory. The Surgeon General said Monday that the U.S. is two weeks behind Italy.
“When you look at the projections, there’s every chance that we could be Italy,” U.S. Surgeon General Jerome Adams told Fox News on Monday.
As health care professionals watch the potential future unfold across the Atlantic, they are growing increasingly anxious that the novel coronavirus, which is particularly dangerous for the elderly and people with underlying medical conditions, could overrun the American healthcare system. As public officials and businesses try to enforce social distancing to slow the spread, hospital staff say they are concerned about shortages of specialized equipment like ventilators, hospital beds, masks and personnel. If the system grows too stretched, they worry they may ultimately have to ration health care.
For now, hospitals can only prepare for the worst. One estimate reportedly presented by the American Hospital Association predicts there could be 96 million cases of coronavirus in the U.S. in the next couple of months, with 1.9 million intensive care unit admissions, 4.8 million hospitalizations, and 480,000 deaths associated with the virus.
“We are not ready. We are not ready virtually anywhere in the country for that kind of onslaught on our health care system,” says Irwin Redlener, director of the National Center for Disaster Preparedness at Columbia University.
For instance, Redlener estimates that there are 95,000 intensive care beds in the country, but “even in the moderate attack rate of the coronavirus,” he believes there could be a need for more than double that number. He also believes the U.S. has only a “fraction” of the mechanical ventilators that could be needed, a device that will be crucial for a virus that aggressively attacks the lungs and for which there is no good substitute. A 2010 survey estimated that there were likely around 62,000 mechanical ventilators in U.S. hospitals.
The Trump Administration has slowly begun to publicly recognize the gravity of the situation hospitals and medical staff are facing. Health and Human Services Secretary Alex Azar acknowledged during a White House briefing on Sunday that a “pandemic like this runs the risk of exceeding our health care system capacity.”
In a sign of how difficult these resources are to come by as the pandemic spans the globe, Trump held a call with governors on Monday telling them they should seek crucial equipment on their own, according to a New York Times report. “Respirators, ventilators, all of the equipment — try getting it yourselves,” Trump reportedly said. “We will be backing you, but try getting it yourselves. Point of sales, much better, much more direct if you can get it yourself.”
Some of these supplies are available in the federally managed, secretive Strategic National Stockpile (SNS), which distributes supplies during crises like this one. On Sunday, Azar said there are “thousands and thousands” of ventilators available in the SNS, but cited national security reasons for not disclosing specific numbers of the supplies available.
Knowing their facilities cannot handle experts’ worst-case scenarios, doctors have been aggressively calling for social distancing to “flatten the curve,” or slow the rate at which the population gets infected and therefore keep the health care infrastructure from being overwhelmed. On Sunday, the Centers for Disease Control put out new guidelines recommending events with 50 or more people be cancelled for the next eight weeks, as well as events of any size where social distancing could not be incorporated.
By Monday, Trump was urging people to avoid gatherings of groups of more than ten. Several cities have now started cracking down on social life, closing restaurants and bars and asking residents to “shelter in place,” and businesses across the country have sent employees to work from home.
“I actually worry that there are a lot of individuals who are not taking it seriously,” says Avital O’Glasser, medical director for the Preoperative Medicine Clinic at Oregon Health & Science University in Portland. “I worry about the banter that people are still saying, ‘I’m going out to bars. I want to go celebrate St. Patrick’s Day. This isn’t going to affect me. I’m young and healthy. Why do I have to isolate myself?’”
If the country is unable to reduce its infection rate, the nation’s health care infrastructure will not be able to cope, and it could result in a decline of adequate care both for coronavirus patients and people suffering everyday health issues, complications or trauma, experts across the country worry.
On Friday, the American College of Surgeons released guidance on minimizing, postponing, or cancelling elective operations in the midst of the pandemic. The Surgeon General also tweeted for hospitals to consider stopping elective procedures, citing the tax it would put on personnel needed for coronavirus response. If there aren’t enough resources to provide proper continuing care to people with chronic illness, medical professionals say that in itself may also have long-term consequences in the health care system.
And while medical professionals are thinking that far ahead, they have more urgent advice. “If we don’t keep that curve flat, and try to keep the critical cases down to a minimum, we’re going to get to a point where we just don’t have enough resources,” says John Hick, medical director for emergency preparedness and emergency physician at Hennepin Healthcare in Minneapolis.
Hick worries about the number of ventilators available, as well as the number of extracorporeal membrane oxygenation, or ECMO, systems, which function like an external blood pump. “So that’s kind of what we’re wrestling with right now — in addition to just space and the staffing,” he said.
He also pointed to appropriate hospital beds as something difficult to work around, describing how unrealistic it would be, for example, to place an 80-year-old patient on a makeshift cot. “Their skin breaks down. A lot of times we have to position those patients differently in order to ventilate them appropriately,” he said. “There’s just no substitute for a good, quality hospital bed.”
Hospitals are also increasingly concerned about the short supply of the personal protective equipment (PPE) used to keep health care workers safe and healthy, like gowns, N95 respirators, surgical masks, gloves and eye protection.
“We’re seeing significant shortages of personal protective equipment and [a] shift to having to really conserve personal protective equipment to make sure that our nurses, physicians and others are adequately protected,” says Paul Biddinger, Vice Chairman for Emergency Preparedness in the Department of Emergency Medicine at Massachusetts General Hospital. “Every health care system has been having to very carefully determine how they allocate and use their PPE so that they try to preserve it to protect the workforce.”
As an increasing number of first responders are likely to come in contact with and contract coronavirus — and therefore be unable to continue working themselves — staffing could become a major problem. Facing furloughed workers, or workers simply exhausted after endless hours on the job, trained professionals out of the workforce may be looked to as standby substitutes. Health care professionals who are not normally considered frontline workers are also figuring out how they can jump in and get involved in the fight.
“I think we’re having to all get comfortable with the idea of practicing outside of our comfort zone,” Fick says. “I’m an internal medicine physician, I’m trained in critical care for my residency, but that was 10 years ago. I haven’t operated a ventilator in 10 years, but I’m preparing to rapid-fire relearn that skill in the event that I have to use that.”
0 notes
Link
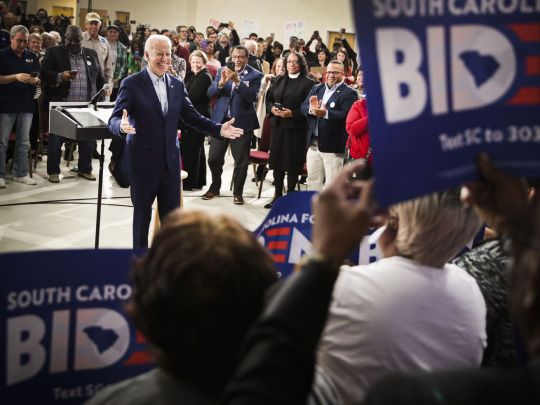
Joe Biden campaigns in Sumter, South Carolina, on February 28, 2020. | Scott Olson/Getty Images
A good night for Biden, a bad one for Bloomberg
South Carolina is the end of the beginning — and it turned out to be a big enough blowout to transform our understanding of the race to come into what really looks like a two-person race between Joe Biden and Bernie Sanders.
First came the traditional two — Iowa’s caucuses and New Hampshire’s “first-in-the-nation” primary. Then came Nevada, moved close to the front of the calendar to give Latino voters more voice in the process, and now, South Carolina, which serves a similar role but for the African-American electorate. None of these states are particularly large or rich in delegates (though South Carolina is the biggest of the four) but they matter because each one stands along on its own day — a beautiful unique snowflake that drives narratives and builds momentum.
Collectively the opening four don’t determine the winner of a nominating contest, but they do drive the shape of the race of the race to come.
But before we head on to Super Tuesday, here’s who won and who lost.
Winner: Joe Biden
Biden won by winning, a pleasingly straightforward and old-fashioned way of winning. His campaign was on the verge of being left for dead after fourth- and fifth-place finishes in Iowa and New Hampshire, respectively, but started a comeback with a second-place finish in Nevada and now delivered in the demographically friendly state of South Carolina.

Sean Rayford/Getty Images
Supporters cheer for Joe Biden in Spartanburg, South Carolina, on February 28, 2020.
The former vice president is still in much worse shape than he was at the beginning of February when he enjoyed a large national polling lead and was only very slightly behind Bernie Sanders in Iowa. At that time it still seemed plausible that Biden might edge out a win in the caucuses and then just roll to a dominant victory. Those days are gone and despite the South Carolina win, Biden is still playing catchup to Sanders in national polls and will likely fall behind in delegates on Super Tuesday.
But he’s stopped the bleeding, his national poll numbers seem to be on the upswing, he retains a deep reservoir of support with black Democrats, and he can make an excellent case that he is far and away the most viable alternative to Sanders. Joe’s back.
Loser: Michael Bloomberg
When Michael Bloomberg started talking about a late entry into the race in early November, I said he was only going to split the moderate vote and help elect Elizabeth Warren.
Since that time, Sanders has clearly displaced Warren as the leading progressive champion, but the basic analysis applies. Right now, Sanders enjoys a roughly 12-point lead over Biden in national polls, but ranked-choice polling shows he’d have a much narrower lead in a two-person race. Bloomberg’s presence in the race, in other words, is meaningfully increasing the odds of the outcome he says he doesn’t want. Dropping out and giving a modest amount of money to a pro-Biden Super PAC would be a reasonably effective “stop Bernie” move, while spending lavishly on his own campaign is helping Bernie.

Joe Raedle/Getty Images
Mike Bloomberg campaigns in Wilmington, North Carolina, on February 29, 2020.
But there was a brief period after Biden’s Iowa swoon when this analysis didn’t seem to apply. Amidst a big panic about the VP’s viability as a candidate, a decent crop of frontline house members and big city mayors (many of whom had benefitted in one way or another from Bloomberg’s largess) endorsed the former New York mayor and he received enough free media coverage to largely stomp on coverage of Pete Buttigieg’s bounce.
The reality that Biden is still here — and still the obvious choice for Democrats who want continuity with the Obama Era rather than a political revolution — deals a fatal blow to the logic of the Bloomberg boomlet. Blessed as he is with a $60 billion fortune, Bloomberg can easily blow $100 million a month on a presidential campaign without breaking a sweat, so nobody can force him out of the race. But he presumably wants to actually be president not just run for president, and it’s increasingly hard to see how that happens.
Loser: Tom Steyer
He’s rich, but not nearly as rich as Michael Bloomberg. He spent big on the 2020 primary, but not Bloomberg big. And unlike Bloomberg, he has no record in office or qualifications to be president.
Nonetheless, Steyer decided to run with his spending concentrated in the early states — South Carolina particularly.

Scott Olson/Getty Images
Tom Steyer campaigns in in Myrtle Beach, South Carolina, on February 26, 2020.
South Carolina was the only one of those early four where there was any evidence of him getting traction, but it all it earned him was a distant third-place finish. There’s no path forward here for Steyer and it’s not clear what he’s doing.
The good news is that unlike Bloomberg, Steyer never really attracted any oppo or criticism from his rivals. Steyer’s pre-campaign political giving was extremely well-regarded and broadly appreciated in progressive circles, and it seems like if he wants to drop out he can go back to being a well-liked benefactor with no real harm done or hard feelings. Still, it’s difficult to understand exactly what was going on here.
Winner: James Clyburn
After the failure of the “party decides” thesis in the 2016 cycle, there’s been considerable skepticism about whether old-fashioned things like endorsements from local elected officials still matter.
The endorsement of Biden by Rep. James Clyburn (D-SC), one of the top figures in the House Democratic caucus, absolutely counted as a big deal by those traditional standards. But did traditional standards count anymore? In South Carolina, at least, it seems that they did — with 47 percent telling exit pollsters his endorsement was a factor in their decision.
Nearly half (!!!) of South Carolina voters said congressman Jim Clyburn’s (D-S.C.) final-week endorsement was an important factor in their vote, according to preliminary exit poll results from Edison Research. Clyburn announced his support for Biden on Wednesday
— Matt Viser (@mviser) February 29, 2020
That’s a win for old-school politics. But specifically because old-school politics seems to be on the way out, it’s also a considerable personal win for Clyburn who has proven himself to be the rare modern-day elected official who is actually someone who voters care about. The mere fact that people say Clyburn swung their vote doesn’t necessarily mean it’s true, of course, but the mere fact that they want to say it is a sign of the esteem for him locally.
Winner: The news cycle
I didn’t love needing to work on the weekend, but the fact is the open primary on a Saturday gave plenty of people the opportunity to vote and once they voted the votes were counted quickly and without a lot of drama.
“State holds election and it’s fine” is not exactly the biggest news in the world, but after the fiasco in Iowa and with the future of caucuses as a whole in question, it’s a nice reminder that there are simple, straightforward ways to hold an election.
And it’s a lucky thing too because this was a Saturday absolutely jam-packed with news. In the morning, the Trump administration signed a deal with the Taliban that should remove US forces from Afghanistan and very likely set the stage for an eventual Taliban victory in their ongoing war with the Afghan government. Concurrently, the United States suffered the first Covid-19 death on American soil and Trump held an afternoon coronavirus press conference in which he began to back off his earlier efforts to downplay the seriousness of the epidemic.
South Carolina is a big story, but it’s not clear how long we’ll be talking about this with so much else going on.
Winner: The contested convention
It would be over the top to call Sanders a “loser” in this outcome — he’s still the frontrunner in delegates and national polls, the most likely nominee, and generally in good shape.
And while obviously having a big loss to Biden by wasn’t Sanders’s first choice of outcome, everyone knows this is not the demographically friendliest state for him. But despite years of hard work and organizing aimed at bolstering his standing in black-heavy southern states, he still came up far short.
Consequently, while Sanders remains in the lead the odds of him scoring a clean victory over Biden have diminished. That means a scenario in which nobody secures a majority of pledged delegates before the convention is now looking more likely.
Loser: Assuming normal voters think like professional activists
Clinton won the 2016 nomination in large part thanks to scoring huge margins with African-American voters in places like South Carolina.
And once it became clear how central black voters were to her support, she started talking about politics in a very particular kind of way — talking about intersectionality, asking “if we broke up the big banks tomorrow ... would that end racism?”, and invoking the phrase “systematic racism.” These are ideas familiar to younger college graduates, often developed by black intellectuals and popular in racist justice activism circles. And since Clinton did, in fact, obtain overwhelming majorities among African-American voters many 2020 contenders essentially tried to imitate this approach.
Suzanna Danuta Walters in The Nation hailed Warren for running “an unapologetically intersectional campaign,” which she certainly did. So did Kirsten Gillibrand and Julian Castro, both of whom ended up dropping out early, with Castro endorsing Warren and becoming a frequently used campaign surrogate.

Drew Angerer/Getty Images
Sen. Bernie Sanders campaigns in North Charleston, South Carolina, on February 26, 2020.
In South Carolina we saw that this approach delivered very meager results with the electorate. Both in the Palmetto State and in national polls, black voters seem split between Biden’s back-to-basics kitchen table economics pitch and Bernie’s democratic socialist pitch with the divisions mostly falling along age lines. The two candidates’ pitches on economic issues are very different, but Biden and Sanders are similar in having some of the weakest claims to wokeness and least explicitly intersectional rhetoric in the field. It’s not that racial issues aren’t important or that the candidates doing well in South Carolina don’t have strong policies on them.
But most voters are working class, not necessarily super-familiar with cutting edge intellectual concepts, and not as siloed in their concerns as activists. There’s a strong market in South Carolina for “similar to Obama” and a smaller, but also pretty strong, market for Sanders’ youth-fueled revolution with very few voters looking to attend a critical race theory seminar.
from Vox - All https://ift.tt/39aRXIZ
0 notes
Text
Trump's finances on health: three losers and a couple of winners
New Post has been published on https://pressography.org/trumps-finances-on-health-three-losers-and-a-couple-of-winners/
Trump's finances on health: three losers and a couple of winners
President Donald Trump’s price range blueprint, out today, includes devastating cuts to fitness research funding and public health packages — at the side of a few vague commitments to release an epidemic reaction fund and keep funding within the fight against HIV.
Finances On Health
Bing Finance
Even as the plan may be too extreme to get Congress’s seal of approval, the White House is signaling a clear desire to intestine some of America’s fitness infrastructure to bolster protection spending and build a wall alongside the USA-Mexico border.
We’ve passed the fitness winners and losers in the budget for you. Right here’s a brief evaluate.
Loser: The National Institutes of fitness The 18 percent reduce to the Department of health and Human Services consists of a $five.eight billion discount for the Countrywide Institutes of health, or approximately a 5th of its finances.
This will decimate the basic and clinical scientific infrastructure in the USA, said Joseph Ross, a professor of medicine at Yale College. Spending on fitness R&D inside the US has already been flagging, and most of the NIH’s budget goes to a military of three hundred,000 outdoor researchers, so a completely large community of researchers would sense the consequences of a price range discount of this length. In line with Matt Hourihan, the director of the R&D price range and Coverage Software for the yank Association for the Advancement of Technology, when the NIH’s budget dropped 5 percent from sequestration cuts, they had to cut around seven hundred individual grants (out of approximately 9,000). With a 20 percent reduce, “We’re likely speaking about [grant] cuts in the loads, if not the thousands,” he informed Vox’s, Brian Resnick.
The cuts would imply less publicly funded Science on things like a way to deal with pain, combat getting old, or create vaccines for diseases like Ebola. “Our [research] confirmed that publicly funded Science carried out at educational research establishments and authorities labs are the supply of the most vital improvements and merchandise that end up transformative therapeutics,” said Aaron Kesselheim, an accomplice professor of drugs at Harvard Medical Faculty. “Deep cuts like This could flip off the invention of the important new therapies of the day after today.”
The price range also calls for “a primary reorganization of NIH’s institutes and facilities to help consciousness resources on the very best precedence studies and training sports.” There’s now not tons element on exactly what this reorganization might appear like, except that the finances propose getting rid of the Fogarty Global Center, a $69.1 million international health Application at NIH that price range four hundred studies and training initiatives involving extra than a hundred US universities and other nations.
The Center has also been analyzing the effect of weather change on disease outbreaks, which may be why it’s a goal. “We do know that international climate exchange is very a great deal associated with the elevated danger of disorder,” stated John Auerbach, president, and CEO of the public fitness nonprofit the Consider for The user’s fitness. “There appears to be a pattern [in the administration] of lowering investment for both studies or packages that cope with local climate change.”
Loser: fitness Services research The administration additionally requires consolidating the Corporation for Healthcare studies and Satisfactory inside NIH. AHRQ became founded to work within the Department of fitness and Human Services, with the assignment of producing proof to make health care safer, better Quality, and extra less expensive.
AHRQ is extremely essential: It’s the handiest US corporation dedicated to studying health delivery, looking at questions like how first-class to deal with returned ache amongst all the potential remedies that are to be had, or reduce the chance of principal line infections so people don’t die Whilst being cared for in hospitals.
Men’s Health
Bringing AHRQ into the NIH at a time when the NIH is dealing with deep cuts may kill it, professionals told me.
“The NIH may not value the AHRQ project,” because it’s comprised especially of organ and disorder-based totally studies institutes, stated Victor Montori, professor of drugs at Mayo Hospital and a senior adviser to AHRQ. “Any finances cuts will prioritize maintaining NIH core packages.”
AcademyHealth president and CEO Lisa Simpson gave a similar prediction. “If NIH is losing 20 percentage of its budget, AHRQ could simply disappear.”
The $500 million block grant would loosen the one’s regulations, however, may additionally genuinely be a conceal for cuts. “What we’ve visible inside the past while block presents are created,” Auerbach said, “they frequently lump collectively one-of-a-kind previously existing packages and then cut them significantly.”
There are other attacks on public fitness in this price range. The Trump plan requires disposing of “programs which might be duplicative or have limited effect on public fitness and nicely-being.” Once more, other than cutting Fogarty, it isn’t clear what those packages can be. The price range does unmarry out fitness professions and nursing training applications, though, “which lack proof that they appreciably enhance the state’s health group of workers” and proposes cutting them through $403 million. That might suggest a discount in education capability for nurses, the state’s frontline fitness vendors. Sarah Frostenson What’s extra, there are dramatic cuts to investment for inexpensive housing, community development, and environmental fitness packages in different businesses. The Trump administration proposed a $6 billion, or 13 percentage, discount within the finances for the Branch of Housing and urban development (HUD).
“We’re nonetheless in the early tiers of knowledge the extent of the significance of housing as a determinant of health — for instance, health risks in condo houses, neighborhood environments for bodily activity, lead publicity, community improvement, clean water, sidewalks,” said University of Minnesota public fitness researcher Sarah Gollust. “And all of those would be highly suffering from cuts to HUD.”
The White House would also reduce $26 billion from the Environmental Safety Business enterprise — a 31 percentage reduction from 2017. This can imperil different crucial public health packages, along with efforts to lessen the danger of lead poisoning and make sure clean ingesting water in communities.
inside the simplest mention of ladies’ health in the price range, Trump could provide $6.2 billion to the WIC Program, which allows states meet the dietary and health wishes of low-income pregnant and postpartum ladies, infants, and youngsters. This represents a $a hundred and fifty million reduce from FY 2016 — and the program was already reduced by means of $273 million the year before that.
Researchers and health officers have long been calling for a federal emergency respond fund for public fitness disasters, similar to FEMA, the Federal Emergency Management Organization.
In public fitness Proper now, every time there may be a risk of an infectious disease spiraling out of Manipulate, officials, and researchers from around the USA head to Washington, DC, to plead for emergency money earlier than Congress. The scramble has performed out with disturbing regularity — for Ebola, H1N1 (also known as swine flu), and Zika.
The price range seems to cope with this by using growing “a brand new Federal Emergency reaction Fund to swiftly reply to public fitness outbreaks, inclusive of Zika Virus ailment.”
“That is probably a very good sign,” said Jennifer Kates, director of worldwide fitness and HIV Policy at the Kaiser Own family Basis. “It seems to be a reputation of that name [by the public health community]. but it’s doubtful in which the funding is coming from.”
The budget doesn’t specify whether it’s a new pot of money, or whether it’s repurposing price range from other things.
Winner: The combat in opposition to HIV and malaria Most of the few guarantees made on health were one to hold the the investment for domestic and international HIV programs.
At the domestic the front, the price range calls for investment for Ryan White HIV/AIDS companies — an “excessive priority” it desires to hold. Ryan White packages offer health care to humans living with HIV who can not get medical health insurance. With $2.three billion in funding in the ultimate budget, it’s the third-largest source of federal money for domestic HIV care after Medicare and Medicaid.
The budget also “presents sufficient resources to keep cutting-edge commitments and all modern-day patient tiers on HIV/AIDS remedy underneath the President’s Emergency Plan for AIDS Remedy.”
PEPFAR is America’s global heath Application to fight AIDS around the world and the largest dedication by any united states committed to an unmarried disease. the program funds each day lifesaving antiretroviral treatment for eleven.five million people, which is equal to the populace of new York and Chicago.
Similarly, the White House would keep investment for malaria packages and meet America commitments to the global Fund, the Global global fitness financing business enterprise.
Trump’s in
But the language in the budget blueprint doesn’t connect dollar quantities to those commitments. the one’s details may additionally come within the very last finances inspiration, out in may.
0 notes
Link
As doctors in the U.S. have watched Italy’s health care system buckle under the sudden strain of the coronavirus, the magnitude of the problems that could be heading their way have begun to sink in. The crises Italian medical staff have been reportedly facing — overwhelming conditions, choosing which patients get treatment, and desperately working to expand their manpower — are all things that hospitals in the U.S. could encounter if the virus continues on its path, doctors say.
“For me it flipped from, ‘This is a real concern, I wonder what’s going to happen’… to ‘Holy cow, I think we’re in trouble,’” says Laurel Fick, a residency director and an internal medicine physician at Ascension St. Vincent Hospital Indianapolis hospital, when she realized how grim the situation in Italy had grown.
As of Monday, the U.S. had more than 4,000 confirmed coronavirus cases, according to Johns Hopkins University, only a fraction of the approximately 28,000 cases in Italy. But the slow start of rolling out testing has made it impossible to know exactly how widespread the pandemic actually is in the U.S. What is clear is that the rate at which cases are increasing is similar to Italy’s trajectory. The Surgeon General said Monday that the U.S. is two weeks behind Italy.
“When you look at the projections, there’s every chance that we could be Italy,” U.S. Surgeon General Jerome Adams told Fox News on Monday.
As health care professionals watch the potential future unfold across the Atlantic, they are growing increasingly anxious that the novel coronavirus, which is particularly dangerous for the elderly and people with underlying medical conditions, could overrun the American healthcare system. As public officials and businesses try to enforce social distancing to slow the spread, hospital staff say they are concerned about shortages of specialized equipment like ventilators, hospital beds, masks and personnel. If the system grows too stretched, they worry they may ultimately have to ration health care.
For now, hospitals can only prepare for the worst. One estimate reportedly presented by the American Hospital Association predicts there could be 96 million cases of coronavirus in the U.S. in the next couple of months, with 1.9 million intensive care unit admissions, 4.8 million hospitalizations, and 480,000 deaths associated with the virus.
“We are not ready. We are not ready virtually anywhere in the country for that kind of onslaught on our health care system,” says Irwin Redlener, director of the National Center for Disaster Preparedness at Columbia University.
For instance, Redlener estimates that there are 95,000 intensive care beds in the country, but “even in the moderate attack rate of the coronavirus,” he believes there could be a need for more than double that number. He also believes the U.S. has only a “fraction” of the mechanical ventilators that could be needed, a device that will be crucial for a virus that aggressively attacks the lungs and for which there is no good substitute. A 2010 survey estimated that there were likely around 62,000 mechanical ventilators in U.S. hospitals.
The Trump Administration has slowly begun to publicly recognize the gravity of the situation hospitals and medical staff are facing. Health and Human Services Secretary Alex Azar acknowledged during a White House briefing on Sunday that a “pandemic like this runs the risk of exceeding our health care system capacity.”
In a sign of how difficult these resources are to come by as the pandemic spans the globe, Trump held a call with governors on Monday telling them they should seek crucial equipment on their own, according to a New York Times report. “Respirators, ventilators, all of the equipment — try getting it yourselves,” Trump reportedly said. “We will be backing you, but try getting it yourselves. Point of sales, much better, much more direct if you can get it yourself.”
Some of these supplies are available in the federally managed, secretive Strategic National Stockpile (SNS), which distributes supplies during crises like this one. On Sunday, Azar said there are “thousands and thousands” of ventilators available in the SNS, but cited national security reasons for not disclosing specific numbers of the supplies available.
Knowing their facilities cannot handle experts’ worst-case scenarios, doctors have been aggressively calling for social distancing to “flatten the curve,” or slow the rate at which the population gets infected and therefore keep the health care infrastructure from being overwhelmed. On Sunday, the Centers for Disease Control put out new guidelines recommending events with 50 or more people be cancelled for the next eight weeks, as well as events of any size where social distancing could not be incorporated.
By Monday, Trump was urging people to avoid gatherings of groups of more than ten. Several cities have now started cracking down on social life, closing restaurants and bars and asking residents to “shelter in place,” and businesses across the country have sent employees to work from home.
“I actually worry that there are a lot of individuals who are not taking it seriously,” says Avital O’Glasser, medical director for the Preoperative Medicine Clinic at Oregon Health & Science University in Portland. “I worry about the banter that people are still saying, ‘I’m going out to bars. I want to go celebrate St. Patrick’s Day. This isn’t going to affect me. I’m young and healthy. Why do I have to isolate myself?’”
If the country is unable to reduce its infection rate, the nation’s health care infrastructure will not be able to cope, and it could result in a decline of adequate care both for coronavirus patients and people suffering everyday health issues, complications or trauma, experts across the country worry.
On Friday, the American College of Surgeons released guidance on minimizing, postponing, or cancelling elective operations in the midst of the pandemic. The Surgeon General also tweeted for hospitals to consider stopping elective procedures, citing the tax it would put on personnel needed for coronavirus response. If there aren’t enough resources to provide proper continuing care to people with chronic illness, medical professionals say that in itself may also have long-term consequences in the health care system.
And while medical professionals are thinking that far ahead, they have more urgent advice. “If we don’t keep that curve flat, and try to keep the critical cases down to a minimum, we’re going to get to a point where we just don’t have enough resources,” says John Hick, medical director for emergency preparedness and emergency physician at Hennepin Healthcare in Minneapolis.
Hick worries about the number of ventilators available, as well as the number of extracorporeal membrane oxygenation, or ECMO, systems, which function like an external blood pump. “So that’s kind of what we’re wrestling with right now — in addition to just space and the staffing,” he said.
He also pointed to appropriate hospital beds as something difficult to work around, describing how unrealistic it would be, for example, to place an 80-year-old patient on a makeshift cot. “Their skin breaks down. A lot of times we have to position those patients differently in order to ventilate them appropriately,” he said. “There’s just no substitute for a good, quality hospital bed.”
Hospitals are also increasingly concerned about the short supply of the personal protective equipment (PPE) used to keep health care workers safe and healthy, like gowns, N95 respirators, surgical masks, gloves and eye protection.
“We’re seeing significant shortages of personal protective equipment and [a] shift to having to really conserve personal protective equipment to make sure that our nurses, physicians and others are adequately protected,” says Paul Biddinger, Vice Chairman for Emergency Preparedness in the Department of Emergency Medicine at Massachusetts General Hospital. “Every health care system has been having to very carefully determine how they allocate and use their PPE so that they try to preserve it to protect the workforce.”
As an increasing number of first responders are likely to come in contact with and contract coronavirus — and therefore be unable to continue working themselves — staffing could become a major problem. Facing furloughed workers, or workers simply exhausted after endless hours on the job, trained professionals out of the workforce may be looked to as standby substitutes. Health care professionals who are not normally considered frontline workers are also figuring out how they can jump in and get involved in the fight.
“I think we’re having to all get comfortable with the idea of practicing outside of our comfort zone,” Fick says. “I’m an internal medicine physician, I’m trained in critical care for my residency, but that was 10 years ago. I haven’t operated a ventilator in 10 years, but I’m preparing to rapid-fire relearn that skill in the event that I have to use that.”
0 notes
Text
New story in Health from Time: As U.S. Braces for Coronavirus to Spread, Hospitals Worry About Shortages
As doctors in the U.S. have watched Italy’s health care system buckle under the sudden strain of the coronavirus, the magnitude of the problems that could be heading their way have begun to sink in. The crises Italian medical staff have been reportedly facing — overwhelming conditions, choosing which patients get treatment, and desperately working to expand their manpower — are all things that hospitals in the U.S. could encounter if the virus continues on its path, doctors say.
“For me it flipped from, ‘This is a real concern, I wonder what’s going to happen’… to ‘Holy cow, I think we’re in trouble,’” says Laurel Fick, a residency director and an internal medicine physician at Ascension St. Vincent Hospital Indianapolis hospital, when she realized how grim the situation in Italy had grown.
As of Monday, the U.S. had more than 4,000 confirmed coronavirus cases, according to Johns Hopkins University, only a fraction of the approximately 28,000 cases in Italy. But the slow start of rolling out testing has made it impossible to know exactly how widespread the pandemic actually is in the U.S. What is clear is that the rate at which cases are increasing is similar to Italy’s trajectory. The Surgeon General said Monday that the U.S. is two weeks behind Italy.
“When you look at the projections, there’s every chance that we could be Italy,” U.S. Surgeon General Jerome Adams told Fox News on Monday.
As health care professionals watch the potential future unfold across the Atlantic, they are growing increasingly anxious that the novel coronavirus, which is particularly dangerous for the elderly and people with underlying medical conditions, could overrun the American healthcare system. As public officials and businesses try to enforce social distancing to slow the spread, hospital staff say they are concerned about shortages of specialized equipment like ventilators, hospital beds, masks and personnel. If the system grows too stretched, they worry they may ultimately have to ration health care.
For now, hospitals can only prepare for the worst. One estimate reportedly presented by the American Hospital Association predicts there could be 96 million cases of coronavirus in the U.S. in the next couple of months, with 1.9 million intensive care unit admissions, 4.8 million hospitalizations, and 480,000 deaths associated with the virus.
“We are not ready. We are not ready virtually anywhere in the country for that kind of onslaught on our health care system,” says Irwin Redlener, director of the National Center for Disaster Preparedness at Columbia University.
For instance, Redlener estimates that there are 95,000 intensive care beds in the country, but “even in the moderate attack rate of the coronavirus,” he believes there could be a need for more than double that number. He also believes the U.S. has only a “fraction” of the mechanical ventilators that could be needed, a device that will be crucial for a virus that aggressively attacks the lungs and for which there is no good substitute. A 2010 survey estimated that there were likely around 62,000 mechanical ventilators in U.S. hospitals.
The Trump Administration has slowly begun to publicly recognize the gravity of the situation hospitals and medical staff are facing. Health and Human Services Secretary Alex Azar acknowledged during a White House briefing on Sunday that a “pandemic like this runs the risk of exceeding our health care system capacity.”
In a sign of how difficult these resources are to come by as the pandemic spans the globe, Trump held a call with governors on Monday telling them they should seek crucial equipment on their own, according to a New York Times report. “Respirators, ventilators, all of the equipment — try getting it yourselves,” Trump reportedly said. “We will be backing you, but try getting it yourselves. Point of sales, much better, much more direct if you can get it yourself.”
Some of these supplies are available in the federally managed, secretive Strategic National Stockpile (SNS), which distributes supplies during crises like this one. On Sunday, Azar said there are “thousands and thousands” of ventilators available in the SNS, but cited national security reasons for not disclosing specific numbers of the supplies available.
Knowing their facilities cannot handle experts’ worst-case scenarios, doctors have been aggressively calling for social distancing to “flatten the curve,” or slow the rate at which the population gets infected and therefore keep the health care infrastructure from being overwhelmed. On Sunday, the Centers for Disease Control put out new guidelines recommending events with 50 or more people be cancelled for the next eight weeks, as well as events of any size where social distancing could not be incorporated.
By Monday, Trump was urging people to avoid gatherings of groups of more than ten. Several cities have now started cracking down on social life, closing restaurants and bars and asking residents to “shelter in place,” and businesses across the country have sent employees to work from home.
“I actually worry that there are a lot of individuals who are not taking it seriously,” says Avital O’Glasser, medical director for the Preoperative Medicine Clinic at Oregon Health & Science University in Portland. “I worry about the banter that people are still saying, ‘I’m going out to bars. I want to go celebrate St. Patrick’s Day. This isn’t going to affect me. I’m young and healthy. Why do I have to isolate myself?’”
If the country is unable to reduce its infection rate, the nation’s health care infrastructure will not be able to cope, and it could result in a decline of adequate care both for coronavirus patients and people suffering everyday health issues, complications or trauma, experts across the country worry.
On Friday, the American College of Surgeons released guidance on minimizing, postponing, or cancelling elective operations in the midst of the pandemic. The Surgeon General also tweeted for hospitals to consider stopping elective procedures, citing the tax it would put on personnel needed for coronavirus response. If there aren’t enough resources to provide proper continuing care to people with chronic illness, medical professionals say that in itself may also have long-term consequences in the health care system.
And while medical professionals are thinking that far ahead, they have more urgent advice. “If we don’t keep that curve flat, and try to keep the critical cases down to a minimum, we’re going to get to a point where we just don’t have enough resources,” says John Hick, medical director for emergency preparedness and emergency physician at Hennepin Healthcare in Minneapolis.
Hick worries about the number of ventilators available, as well as the number of extracorporeal membrane oxygenation, or ECMO, systems, which function like an external blood pump. “So that’s kind of what we’re wrestling with right now — in addition to just space and the staffing,” he said.
He also pointed to appropriate hospital beds as something difficult to work around, describing how unrealistic it would be, for example, to place an 80-year-old patient on a makeshift cot. “Their skin breaks down. A lot of times we have to position those patients differently in order to ventilate them appropriately,” he said. “There’s just no substitute for a good, quality hospital bed.”
Hospitals are also increasingly concerned about the short supply of the personal protective equipment (PPE) used to keep health care workers safe and healthy, like gowns, N95 respirators, surgical masks, gloves and eye protection.
“We’re seeing significant shortages of personal protective equipment and [a] shift to having to really conserve personal protective equipment to make sure that our nurses, physicians and others are adequately protected,” says Paul Biddinger, Vice Chairman for Emergency Preparedness in the Department of Emergency Medicine at Massachusetts General Hospital. “Every health care system has been having to very carefully determine how they allocate and use their PPE so that they try to preserve it to protect the workforce.”
As an increasing number of first responders are likely to come in contact with and contract coronavirus — and therefore be unable to continue working themselves — staffing could become a major problem. Facing furloughed workers, or workers simply exhausted after endless hours on the job, trained professionals out of the workforce may be looked to as standby substitutes. Health care professionals who are not normally considered frontline workers are also figuring out how they can jump in and get involved in the fight.
“I think we’re having to all get comfortable with the idea of practicing outside of our comfort zone,” Fick says. “I’m an internal medicine physician, I’m trained in critical care for my residency, but that was 10 years ago. I haven’t operated a ventilator in 10 years, but I’m preparing to rapid-fire relearn that skill in the event that I have to use that.”
via Blogger https://ift.tt/2wg35pI
0 notes
Link
March 16, 2020 at 08:06PM
As doctors in the U.S. have watched Italy’s health care system buckle under the sudden strain of the coronavirus, the magnitude of the problems that could be heading their way have begun to sink in. The crises Italian medical staff have been reportedly facing — overwhelming conditions, choosing which patients get treatment, and desperately working to expand their manpower — are all things that hospitals in the U.S. could encounter if the virus continues on its path, doctors say.
“For me it flipped from, ‘This is a real concern, I wonder what’s going to happen’… to ‘Holy cow, I think we’re in trouble,’” says Laurel Fick, a residency director and an internal medicine physician at Ascension St. Vincent Hospital Indianapolis hospital, when she realized how grim the situation in Italy had grown.
As of Monday, the U.S. had more than 4,000 confirmed coronavirus cases, according to Johns Hopkins University, only a fraction of the approximately 28,000 cases in Italy. But the slow start of rolling out testing has made it impossible to know exactly how widespread the pandemic actually is in the U.S. What is clear is that the rate at which cases are increasing is similar to Italy’s trajectory. The Surgeon General said Monday that the U.S. is two weeks behind Italy.
“When you look at the projections, there’s every chance that we could be Italy,” U.S. Surgeon General Jerome Adams told Fox News on Monday.
As health care professionals watch the potential future unfold across the Atlantic, they are growing increasingly anxious that the novel coronavirus, which is particularly dangerous for the elderly and people with underlying medical conditions, could overrun the American healthcare system. As public officials and businesses try to enforce social distancing to slow the spread, hospital staff say they are concerned about shortages of specialized equipment like ventilators, hospital beds, masks and personnel. If the system grows too stretched, they worry they may ultimately have to ration health care.
For now, hospitals can only prepare for the worst. One estimate reportedly presented by the American Hospital Association predicts there could be 96 million cases of coronavirus in the U.S. in the next couple of months, with 1.9 million intensive care unit admissions, 4.8 million hospitalizations, and 480,000 deaths associated with the virus.
“We are not ready. We are not ready virtually anywhere in the country for that kind of onslaught on our health care system,” says Irwin Redlener, director of the National Center for Disaster Preparedness at Columbia University.
For instance, Redlener estimates that there are 95,000 intensive care beds in the country, but “even in the moderate attack rate of the coronavirus,” he believes there could be a need for more than double that number. He also believes the U.S. has only a “fraction” of the mechanical ventilators that could be needed, a device that will be crucial for a virus that aggressively attacks the lungs and for which there is no good substitute. A 2010 survey estimated that there were likely around 62,000 mechanical ventilators in U.S. hospitals.
The Trump Administration has slowly begun to publicly recognize the gravity of the situation hospitals and medical staff are facing. Health and Human Services Secretary Alex Azar acknowledged during a White House briefing on Sunday that a “pandemic like this runs the risk of exceeding our health care system capacity.”
In a sign of how difficult these resources are to come by as the pandemic spans the globe, Trump held a call with governors on Monday telling them they should seek crucial equipment on their own, according to a New York Times report. “Respirators, ventilators, all of the equipment — try getting it yourselves,” Trump reportedly said. “We will be backing you, but try getting it yourselves. Point of sales, much better, much more direct if you can get it yourself.”
Some of these supplies are available in the federally managed, secretive Strategic National Stockpile (SNS), which distributes supplies during crises like this one. On Sunday, Azar said there are “thousands and thousands” of ventilators available in the SNS, but cited national security reasons for not disclosing specific numbers of the supplies available.
Knowing their facilities cannot handle experts’ worst-case scenarios, doctors have been aggressively calling for social distancing to “flatten the curve,” or slow the rate at which the population gets infected and therefore keep the health care infrastructure from being overwhelmed. On Sunday, the Centers for Disease Control put out new guidelines recommending events with 50 or more people be cancelled for the next eight weeks, as well as events of any size where social distancing could not be incorporated.
By Monday, Trump was urging people to avoid gatherings of groups of more than ten. Several cities have now started cracking down on social life, closing restaurants and bars and asking residents to “shelter in place,” and businesses across the country have sent employees to work from home.
“I actually worry that there are a lot of individuals who are not taking it seriously,” says Avital O’Glasser, medical director for the Preoperative Medicine Clinic at Oregon Health & Science University in Portland. “I worry about the banter that people are still saying, ‘I’m going out to bars. I want to go celebrate St. Patrick’s Day. This isn’t going to affect me. I’m young and healthy. Why do I have to isolate myself?’”
If the country is unable to reduce its infection rate, the nation’s health care infrastructure will not be able to cope, and it could result in a decline of adequate care both for coronavirus patients and people suffering everyday health issues, complications or trauma, experts across the country worry.
On Friday, the American College of Surgeons released guidance on minimizing, postponing, or cancelling elective operations in the midst of the pandemic. The Surgeon General also tweeted for hospitals to consider stopping elective procedures, citing the tax it would put on personnel needed for coronavirus response. If there aren’t enough resources to provide proper continuing care to people with chronic illness, medical professionals say that in itself may also have long-term consequences in the health care system.
And while medical professionals are thinking that far ahead, they have more urgent advice. “If we don’t keep that curve flat, and try to keep the critical cases down to a minimum, we’re going to get to a point where we just don’t have enough resources,” says John Hick, medical director for emergency preparedness and emergency physician at Hennepin Healthcare in Minneapolis.
Hick worries about the number of ventilators available, as well as the number of extracorporeal membrane oxygenation, or ECMO, systems, which function like an external blood pump. “So that’s kind of what we’re wrestling with right now — in addition to just space and the staffing,” he said.
He also pointed to appropriate hospital beds as something difficult to work around, describing how unrealistic it would be, for example, to place an 80-year-old patient on a makeshift cot. “Their skin breaks down. A lot of times we have to position those patients differently in order to ventilate them appropriately,” he said. “There’s just no substitute for a good, quality hospital bed.”
Hospitals are also increasingly concerned about the short supply of the personal protective equipment (PPE) used to keep health care workers safe and healthy, like gowns, N95 respirators, surgical masks, gloves and eye protection.
“We’re seeing significant shortages of personal protective equipment and [a] shift to having to really conserve personal protective equipment to make sure that our nurses, physicians and others are adequately protected,” says Paul Biddinger, Vice Chairman for Emergency Preparedness in the Department of Emergency Medicine at Massachusetts General Hospital. “Every health care system has been having to very carefully determine how they allocate and use their PPE so that they try to preserve it to protect the workforce.”
As an increasing number of first responders are likely to come in contact with and contract coronavirus — and therefore be unable to continue working themselves — staffing could become a major problem. Facing furloughed workers, or workers simply exhausted after endless hours on the job, trained professionals out of the workforce may be looked to as standby substitutes. Health care professionals who are not normally considered frontline workers are also figuring out how they can jump in and get involved in the fight.
“I think we’re having to all get comfortable with the idea of practicing outside of our comfort zone,” Fick says. “I’m an internal medicine physician, I’m trained in critical care for my residency, but that was 10 years ago. I haven’t operated a ventilator in 10 years, but I’m preparing to rapid-fire relearn that skill in the event that I have to use that.”
0 notes