#probably with either a virus/vaccine type each
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was attacked by a cross-site scripting worm deployed by the Internet troll group GNAA on Dec 3, 2012.
Text
Wait..... There's nothing stopping me from giving the QSMP eggs their own Digimon.
...
Hey digimon fans-
#are there any digimon fans here? Probably not#Do I want to create some? yes#Okay but if I assign an egg a digimon that is gonna be FUN#Dapper and pomme need to match of course#probably with either a virus/vaccine type each#or an angelic/demonic digimon#oooohoohoo I want to do this so bad#I'm sure everyone has given them pokemon before. But these kids would THRIVE in a digimon setting#pspspspspsps everyone go watch Digimon Adventure from 1999. And Digimon Adventure 02. And Tamers. And-#okay im done LMAO#not a poll#qsmp#qsmp eggs#Digimon is my roman empire
25 notes
·
View notes
Note
Hi! This is kind of a weird question but how/why was influenza (and other diseases that we have vaccines for now) so deadly 100-200 years ago? Obviously vaccines help tremendously, and probably immunity over time, but are there other reasons that the flu was a much bigger deal a century ago? Sorry if this is oddly specific, but my current project is historical. Thank you!
This is a very interesting question and there are a couple of different ways of looking at it.
Let's start with influenza:
[Note: it's surprisingly difficult to get good worldwide flu data, so I'm going to use US numbers for the purposes of this post.]
I think the first thing to understand is that unlike many other infectious diseases, influenza is substantially different every year. That means that the immunity that you build in 2017 from either the flu or the flu shot won't necessarily help prevent you from getting the flu in 2023. By then it will be a different enough virus that your previous immunity won't be as helpful. Though it might make it a little milder. But keep reading, I'll give you some fun facts to share at parties:
We name flu (A) viruses based on two different proteins on the surface of the virus. The proteins are "H" and "N". There are 16 different "H" proteins, and 9 different "N" proteins that we currently know of. The combination of the two forms the "name" of a particular flu virus. Think H1N1, or H5N6, or any other combination. Each combination has their own attributes, which contributes to how infectious or deadly they are in any given year. And which ones circulate are different every year.
Just mathematically, that's a lot of substantially different flu viruses. Hundreds of them, in fact. And you have to build immunity to each one individually. You could, say, build immunity to H2N5, but that would do little to save you from next year's H4N3. And not only that, but within a single type there are many smaller variations. For example, say you got H5N3, but then it went and mutated. If you then got exposed again, you might have some immunity to new!H5N3, but it could also be just different enough that you still get sick.
Like I said above, different types of flu virus are deadlier or spread faster than others. H5N1 (a type of avian flu with a human mortality rate of 52%) is terrifyingly deadly but fortunately doesn't spread particularly well, while H1N1 (the star of both the 1918 and 2009 flu seasons) spreads rapidly and kills primarily young adults (weird, since flu usually kills babies and old people).
This is why in 2009 we did the whole "close the schools vaccinate the teens hide the president" routine. Because if it was *that* H1N1 we were all about to be screwed in ways we had never experienced before. Fortunately it wasn't, but thank goodness we did it. Also if you got vaccine #2 in 2009, you are also protected against the 1918 strain of H1N1. You're gonna be a hit at parties with that one.
Now, if you look at only deaths (not the best measure, but one with some emotional punch), within the last decade alone we have years where 12,000 people died of flu in the US (2011-2012) and years where that number is as high as 61,000 (2017-2018). These numbers are similar throughout recent history (relative to population), but then you get years like 1968 (where 100,000 people died in the US) and 1957 (where 116,000 died), and then sometimes you get these wild whopping years like 1918 where 675,000 died (equivalent to 1,750,000 people dying in today's US population). These fluctuations have happened since Hippocrates was around, and probably long before that, and there's really nothing to suggest it's getting any milder in any statistically significant way.
Now, outside of these natural fluctuations, we do have some ways of driving down these numbers. We do have a vaccine. It is different every year, based on our prediction of what the most likely or dangerous types of flus will be this year. Fortunately, you do get to keep this immunity for some time, so you can look at the flu vaccine as a personal collection of different flu viruses you have immunity to- you can collect 2-3 different ones every year in one shot and you didn't even have to catch them!! Yay! Unfortunately, since we never reach herd immunity with the flu vaccine, and we can't perfectly predict and incorporate all the strains that will circulate in a given year, while you do get some protection, it's not ever perfect. But it *is* still worth it.
We also have other feats of modern medicine as backup to the flu vaccine. We have oxygen, antiviral drugs like tamiflu, immune modulating drugs, and technology like ventilators to help keep people alive in ways we would not be able to in previous generations. So that's also an advantage. Unfortunately, these don't always work either, and we are still at the whim of those yearly fluctuations in influenza virus deaths.
And really, if you ask any epidemiologist, covid is just a little trial run for the next Big One. Which is both extremely likely to be a flu virus and which we're statistically overdue for.
TL;DR: The flu isn't getting milder so much as it varies wildly in severity every year. The next major flu pandemic is probably going to be in our lifetimes, so start collecting your flu immunity now if you haven't yet. New collections drop every August and are available until April. Get em' while they're hot. This year's included a 2009-like strain of H1N1 and a delightful H3N2 number from Hong Kong.
As for All the Other Vaccine Preventable Illnesses:
*ahem*
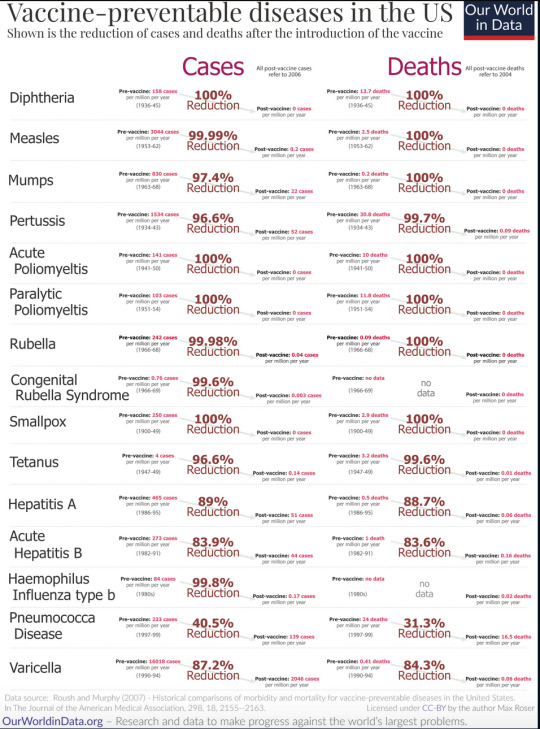
Yes, it's vaccines. It's obviously vaccines. Its basically only vaccines. Anyone who has ever told you it's not vaccines is lying. No other major discovery of modern medicine has ever saved as many lives, prevented as many disabilities, and created as many opportunities for a life well lived as vaccines have. No antiviral drug, no antibiotic, no ventilator can even hold a candle to vaccines. The answer is f*cking vaccines*.
I hope I have made myself clear.
Enjoy this table:
*Yes I do have a masters degree in public health and am a registered nurse that interacts with the public regularly, how did you know?
-Ross @macgyvermedical
7K notes
·
View notes
Text
Sick
Relationships: 10th Doctor x reader (Not an established relationship)
Summary: the Doctor and you find yourselves on a spaceship in desparate need of repair and you are determined to help the crew (Kaisa, Lincoln and Bressa), but then the ship also gets highjacked. And on top of that, you fall sick.
Warnings: you're in mortal danger but that's it
You were standing by the big metal desk in the middle of the room, reading the numbers to Kaisa so he could type them in.
The digits kept swimming in your vision. They were blurry, everything was blurry, but they also kept moving. And when did it get so hot? You wiped the sweat from your forehead while trying to breathe deeply. You knew that if you looked up from the pad, the room would be spinning. The worst part was the tiredness. It coiled through your limbs and made them so heavy you could hardly move them. The effort to keep connecting letters and sounds, keep connecting thoughts hurt.
You closed your eyes for a second and the ship tilted so far you lost your balance. You stumbled back, eyes flying open and arms trying to reach out for something to hold onto.
Suddenly there were strong hands on your shoulder and the small of your back, steadying you. You looked up and recognized the dark orange skin and curly brown hair that was greying at the edges. Kaisa had caught you.
"Are you alright?" his gruff voice came to you.
"Yeah, yeah l'm okay." That sounded weak even to your own ears. "The ship just tilted."
"The ship's fine, love," he answered in confusion. You could see furrowed eyebrows, and then his dark golden eyes. You couldn't make out the wrinkles around them, or the lines on his forehead. Everything was blurry.
He put one hand around you to hold you up, then felt your forehead with the other. It was blessedly cold and you leaned into it with a sigh. "I think humans aren't supposed to be this hot," his worried voice came then.
You could hear Lincoln and Bressa turn around and step closer. You would have cracked a joke about drinks first if you weren't about to ask to sit down from exhastion. But you all had a job to do.
"I'm okay," you tried to reassure him. "Let's just get back to-" As you stepped away from Kaisa to shake his hands off, the ground rushed up and you barely caught yourself on the table. His arms were back, supporting you, before you could fall further. Shit.
"You're sick," Kaisa confirmed with a voice full of worry. He gently pulled you from the table and towards the wall. "Here, sit down," he told you softly and manouvered you to a stack of crates. He helped you sit on one and you rested your head on the taller pile.
"Thanks," you breathed gratefully and closed your eyes.This is nice.
On the other side of the room you could just hear Bressa order Lincoln, "Go get the Doctor. Tell him y/n's sick." Her voice was grave.
~
The Doctor had just recalibrated the fiberlinks of the navicomputer and was well on his way of taking apart the integral protonic bond when Lincoln reached him. The Doctor didn't even pull his head out of the ship's innards, much less stood up. "What is it?" He didn't have time for this.
"Your friend," the young man's distressed voice came. "She's sick."
That made worry explode in his chest. Ice spread through his veins as he hurriedly pulled himself out of the wiring. He hit his head on the way but that didn't matter, not when y/n was-
"What did you say?" the Doctor demanded in a low voice, eyes scanning the Tirellian crewmate.
"Y/n is sick." The Doctor marked every blink, every twitch, every line. He did not like the worried frown on Lincoln's face. He had gotten his answer.
The Doctor put the sonic back in his inner pocket and demanded, "Where is she?", voice forcibly calm but unrelenting. He picked up his coat as the young man turned to show the way, and off they went.
~
When your eyes were closed, you could almost pretend you were fine, but the fever, the heat in your skin was killing you. The box on your cheek and forehead had warmed up and provided no more relief.
You could feel even the darkness around you spin if you tried to think.
~
The Doctor ran into the room after Lincoln, trench coat billowing around him.
"Where is she?" he demanded in worry with his gaze searching the room.
"Over here." Kaisa stood up from behind the large metal table and pointed at the stack of crates beside the wall. He stepped back towards the others as the Doctor came to kneel before you with his coat scraping the floor. His hands hovered just inches above your skin.
"Y/n," he breathed quietly while looking you over. His hand settled on your arm. Scarlet cheeks, sweat - fever, eyes closed, leaning on the crate - exhausti-
You tiredly opened your eyes but you didn't lift your head. "Doct'r." The regret was already in your voice. "'M sorry. I should've-" Should have known the signs, should have slept more, should have eaten-
"You have nothing to be sorry for," he murmured softly, shaking his head. He rubbed your arm, his expression gentle and reassuring.
He took your hand and found your pulse point, which made butterflies flutter in your stomack despite the sickness. Then he lifted his other hand to your cheek. It was cold so you leaned into it, your eyes closing in content. You breathed deeply but it seemed like there was never enough air.
"You've definitely got a fever, about 39 degrees," he continued in that same soft tone. "And your heart is speeding up. How're you feeling?"
"Evr'thin's spinnin'," you told him tiredly, words a bit slurred. You tried to remember, but the things you were trying to describe made it hard to do that. "Couldn't stand up, Kaisa caught me. Couldn'read anymore, evr'thing was blurry'n moving. My head hurts, my eyes hurt, ever'thing hurts. An'l'm tired," you sighed. "I wanna go t'sleep."
"You will, l promise you will, but you need medicine first," he told you gently yet firmly. "It's the virus Tem, from Polon. We were there about four days ago, it's quite common for the planet, but it's dangerous." His brown eyes were full of worry. "If it's left untreated, as yours was, it can be deadly." He left the sentence hang in the silence after it.
You tried to shake your head but the motion caused more pain and you stopped. "So l'll get the meds and ll'l be fine," you told him tiredly. It didn't seem like much of a problem. You faced death on a daily basis, so what was a little virus?
"What do we do?" Kaisa stepped closer and looked down at the two of you, eyebrows furrowed in worry and hands crossed in front of his chest.
The Doctor moved closer and took you by the shoulders. "C'm on." He smiled encouragingly as he gently helped you stand up. You didn't like it, but the solution to this situation probably required moving.
You leaned against him and put your head on his shoulder as he helped you stay upright. The spinning did not help your stomack.
"Polonians have a vaccine, but it's far too late for that. You though, you three come from Kristella, is that right?" the Doctor looked around the room.
"Yeah," Kaisa nodded.
"So you receaved the whole med package there, including the VC five-six-o-nine."
"Yes."
"Good," he nodded, "bless the Kristellan med care. Your immune system knows the virus so you're not in danger. But you," he looked down at you, gritting his teeth, "are."
Well, that was a bit obvious.
He looked back up at Kaisa. "I want you to get her to the med bay. Give her Triskel two point three with a lot of water, she needs to stay hydrated, and then two shots of Amino when that's down, got it?"
"Yes," the large sailor nodded and stepped closer to take you. "And don't 'Got it' me, young man."
The Doctor opened his mouth to explain the whole Time Lord age thing when-
"I don't wanna go," you mumbled into his chest, pressing yourself closer. The room was spinning, you couldn't see well and you could barely stand. The thought of leaving him (he meant safe and good and you needed him) on this ship where anything could happen to you or him (who would look after him if not you?) made you want to sob.
He pulled away enough to look at you but still hold you. His eyes were soft. "I know," he told you gently and then frowned at the thought of letting you go, "l don't like this either." Every instinct in him flared against leaving you while you were sick and in need of him. He was Gallifreyan, and he protected what was his, even if you didn't know. "But you need medicine, and they need help rewiring the ship," he put it plainly. "I have to stay, and you have to go."
You nodded even though it hurt. He pulled you closer and for a moment, you just held each other.
"Stay safe," you said into his shoulder, almost an order. "Not a hair out of place, you hear me?"
You could feel him smile at the familiar tone. "Yes, ma'am."
It was time to go. You slowly let go of the Doctor as Kaisa came closer. He slung a hand around your waist while you put yours around his shoulders. It worked well, you could stay upright and move at the same time.
Then the whole ship shook like it was being torn apart and you were thrown against the table while Lincoln yelled in surprise. The Doctor and Kaisa kept you stable and unharmed between them, but the room looked like it had survived an earthquake.
"Are you alright?" The Doctor was franctically looking you over for injuries.
"What the hell was that?" demanded Bressa.
~
Kaisa didn't know what to do. You and him were locked in one of the main storage rooms, and they hadn't even let you get medicine. The large Risonians, two out of six who had highjacked the ship, simply came into the med bay and dragged you out before he could find anything to help you. You hadn't even gotten water.
All he could do was put his jacket under your head when you couldn't sit up anymore and hold your hand as you slipped into a restless sleep.
Then he noticed the computer log in the corner behind the crates. He could rewire it, send an altering pulse through the system... He looked at you as your head turned from one side to the other as you gasped for breath, mumbling nonsense in your sleep. Your fever was rising.
"Right then, love. I'm going to get help."
~
When the Doctor noticed Kaisa's message beeping under the log, he'd been momentarily confused. He'd made it very clear to the Risonians that you needed medicine and that he would do anything to make sure you got it, so why would they-
A second later, a pair of the hijacking crew came marching into the room with guns drawn. The Commander was as shocked as him when two of her people turned against her.
This was bad.
~
The Doctor walked into the storage room with his hands behind his head, with Bressa and Lincoln behind him. What remained of the Risonian crew had been locked into a separate room, to keep you all separated. His eyes immediately scanned the space for you.
When he turned the corner behind a high stack of crates, his hearts lurched. You were unconscious, lying on the floor with Kaisa holding your hand.
The Doctor was by your side in a second. Your skin was pale, but your cheeks were scarlet and your forehead glistened with sweat. You were mumbling in your sleep, your breaths laboured. Your head was turning restlessly in the throes of a fever dream. He took your warm hand and held it tightly.
"She was asking for you," Kaisa told him softly, eyes still trained on your face.
"What?" The Doctor's gaze flew to the larger man in confusion.
Kaisa looked up at him, "She was asking for you." He searched his eyes, for what, the Doctor didn't know. "Even after she couldn't answer me anymore, she kept asking for you in her sleep."
The Doctor felt like a hand had squeezed his hearts. It happened again, he did it again, you were in danger and it was his fault. He looked down at your closed eyes and scarlet cheeks. You were helpless, you needed him, and he couldn't do anything.
He brought your hand to his cheek and held it there with his palm as he closed his eyes. He needed you to live, he needed you to be alright. You had to be.
"Doct'r," your voice was barely a whisper.
His eyes flew open and he stared down at your still sleeping form. You turned your head to the side and, "Doct'r," again his name.
It lit a blazing fire in his chest. That was it. That was it, he was getting you out. He was getting all of you out because that was what he was going to do and the universe would bloody listen. He was the Doctor, and you were his. He was not losing you, not ever.
They'd taken the sonic but he was, for all intents and purposes, in a supply closet. Time to find out exactly which supplies he had.
#doctor who#doctorwho#doctor who x reader#doctorwho x reader#the doctor x reader#tenth doctor x reader#10th doctor x reader#the doctor#tenth doctor#10th doctor#doctor who fanfiction#doctorwho fanfiction#reader insert
411 notes
·
View notes
Text
My Experience with the Covid Vaccine
Hi Everyone! I’ve been receiving a lot of questions about my experience with the Covid vaccine and I figured it would be best to just make a post where I can answer everyone’s questions all in one place. I will be going over a couple of different things here from how I was able to get the vaccine, my reaction to the vaccine, the ethics behind the vaccine (for my Catholic, Christian, Pro-Life friends-- you can ignore this section if you are none of those things), how the vaccine works, and why you should get the vaccine. I will try my best to make everything here as honest as I can in terms of my experience and I will link you to sources for my more scientific facts. I know that there is a lot of misinformation out there and fear regarding the vaccine and I hope to put all that to rest.
So let’s start this off with how I was able to get the vaccine. For those of you who don’t know I am a healthcare worker. I work in EMS as an EMT. I was lucky enough to have the option for either the Moderna or the Pfizer vaccine. My company offered us the Moderna vaccine, but the local hospital in our area (which was offering the Pfizer Vaccine) had some extra vaccines and were generous enough to share those vaccines with us. My company wouldn’t receive their shipment for another week or two and I wanted to get my dose as soon as possible, so I decided to get my dose through the local hospital. Which is how I ended up with the Pfizer one.
Many of you asked about my reaction to the vaccine. I have had both doses now and my reactions to both were very different. These were MY reactions. I know people who had different reactions than me, so just because it happened to me does not mean it will happen to you. Everyone is different and can experience things on their own. For my first dose I didn’t have any reactions. I just had the sore arm that comes with any vaccination. They are injecting it directly into your muscle so you are going to be sore. That is normal and you shouldn’t be worried. It feels kind of like a charlie horse or like you worked out really hard at the gym, but only in that one spot. Just ice it or throw on a heat pack or take a tylenol and power through. You did a good thing for yourself and your community. About 18 days later I had my second dose of the vaccine. This dose is larger and is needed in order for you to have the immunity to the virus. DO NOT MISS YOUR SECOND DOSE. I made the mistake of getting this shot while on duty lol. I had started my day with some normal back and neck pain that I attributed to regular heavy lifting of patients and a car crash I had a month prior. About 4 hours after getting my vaccine I started feeling VERY achy in both my back and neck. I thought nothing of it because I started the day with that pain and figured it was just because we had lifted some heavier patients. About an hour later I started getting the chills and the weakness. I was just feeling off and not quite myself. As the night progressed I ended up getting a low grade fever, nausea (luckily I had zofran on hand), a cough, dizziness, and I was diaphoretic (sweaty). I just really didn’t feel very good. I powered through my shift where I got off at 0700 and went home the next morning where I was able to sleep it off. By noon I was back to my regular self with only the sore arm. My reaction to the vaccine from start to finish was probably only about 15 hours. Yea that reaction sucked and I really did not feel too great, but would I do it again if it meant protecting myself and others from Covid? Hell yes!
The process for getting the vaccine may differ at each distribution site in terms of registration, but there are a few things that are going to stay the same. It started off with me registering on the website and answering some basic questions. Such as “are you a healthcare worker?” “have you been exposed to Covid without PPE?” “Are you Pregnant?” “Are you over 16?” “Do you have any allergies?” etc. Common questions that get asked in the current medical setting. I then had to register for an appointment time and show them my ID to prove I am who I am. After answering those questions I was sent off to wait for the first available person to administer my vaccine. Each table is sanitized after each person. I went over and got my shot. Went and filled out my vaccination card and had it signed off by someone then I went to sit in the waiting area for 15 minutes. That part is mandatory for everyone in case there is a reaction to the vaccine. WHICH IS EXTREMELY RARE. If you are a person who has many allergies then it is recommended you wait 30 minutes instead as it can sometimes take 30 minutes for a reaction to develop. Luckily there are healthcare providers all around so you are in good hands :) The whole process was so simple and I made friends with everyone else who was there getting their shots. We were bonding over our combined 5G super coverage. It was glorious.
How does the vaccine work? The Covid 19 Vaccine is a newer type of vaccine. It is something called a mRNA vaccine. mRNA Vaccines are different from our traditional vaccines as they don’t have a weak or inactive version of the virus or bacteria in them. What it does is it teaches the cells in our body how to fight off the virus by creating a protein to trigger our immune systems into action and fight off whatever shouldn’t be there. After the protein in our cells is created it gets displayed for our body to realize that it doesn’t belong. Our immune system then starts creating antibodies to fight off this unknown and very unwelcome protein. After our body has created these antibodies it deletes the protein out of existence as if it never existed leaving only the antibodies to protect us later down the line in case we do end up catching Covid (you can read more on this here https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/mrna.html) . I think mRNA vaccines are going to be the future. They are more effective and way cooler in how they work. How did this vaccine come out so fast you ask? It was obviously planned by the government right? Wrong. Stop with the conspiracy theories ya wackos. mRNA vaccines had been in the works for YEARS. China had successfully identified the protein on the outside of the virus and sent that information to the labs across the world (pfizer and Moderna) to get started on a vaccine. They were able to crank one out and start the testing on animals, then people. After the trials they were able to approve these vaccines for distribution across the world (https://www.health.harvard.edu/blog/why-are-mrna-vaccines-so-exciting-2020121021599). So basically the vaccine is cool and in no way a conspiracy.
Now for all of my Catholic, Christian, and Pro-Life friends. Is it ethical to receive the vaccine. In short, yes. For those of you who are still reading this part the reason this is a big issue for my Catholic, Christian, and Pro-Life friends is because past vaccines have used stem cells from an aborted baby. This is not meant to start a pro-life/pro-choice debate. Any of that on this post will be shut down immediately. For us as Catholics and as people who are pro-life it can be seen as a morally gray area due to the fact that a life has been taken and each human being has inherent dignity and value from conception to natural death. Now on to why we are able to receive the vaccine. Both the Moderna and the Pfizer vaccines were made using the mRNA technique. Which basically means there is no fetal tissue in them. Now where people are getting confused. While the vaccines do not use fetal tissue in them, they still tested them on a morally compromised cell line. Now the reason we are able to receive these vaccines still is because while neither of these vaccines is remote from evil there were no other options for us to keep the population as a whole safe. If you are still concerned about it we are so far removed from the act of the abortion that we cannot be held accountable for the actions that took place that day. This is a very very shortened version and if you would like to keep reading then you can do so here https://www.catholic.com/audio/cot/covid-19-vaccines-and-the-usccb?fbclid=IwAR2xRPbNxiCdsc1ISeb6u_D-YHjyoCrQlT3oTI4QZdeU1z9LZ6eGtbqrrKw. We should be getting this vaccine to protect those of us who are unable to receive it.
This post was not meant to be political in any way. I wanted to help you all understand why this vaccine is so important and put your minds at ease. Remember, the reasons vaccines work is because of herd immunity. Which means if the majority of us as a community get the vaccine then it will help to keep those who can’t get it (the pregnant, breastfeeding, immunocompromised, etc) safe and better protected from the virus. So please do your part. Social distance, wear your mask, wash your hands, get your vaccine, and look out for your neighbors. We are all in this together.
97 notes
·
View notes
Link
Politicians and pundits often like to compare the COVID-19 pandemic to a war. Nothing in most of our lifetimes has had the society-changing impact of the COVID-19 pandemic — and this kind of feels like the way that our parents say their parents described the Great Depression or World War II.
But World War II ended in a singular moment. Treaties were signed and people rushed into the streets in jubilation. The COVID-19 pandemic, which has plagued our lives for the last 14 months, won't end in a singular moment. There'll be no major "pandemic peace treaty," no all-out party. Perhaps, at best, there'll be a bunch of little ones. And that forces us to ask: How will this end?
The virus isn't going to disappear.
Our vaccines are incredibly safe and effective. For those who are vaccinated, they are a ticket back to "normal" life. Indeed, though rushed and poorly messaged, the CDC's guidance allowing vaccinated people to go unmasked both indoors and outdoors is based in strong science. Evidence has demonstrated that the risk of serious infection in the real world is astoundingly low, and that the viral load in the nasopharynx of vaccinated people is lower — likely explaining the reduced risk of transmission.
Yet, some people aren't getting vaccinated. And worse, the distribution of vaccinations isn't even. If, for example, unvaccinated people were evenly distributed in the population, the probability that they would be exposed to the virus if 70% of eligible people were vaccinated would be quite low. After all, 70% of the people around them would be vaccinated and therefore far less likely to pass the virus on. That's how herd — or community — immunity works. The problem though is that just like the virus itself, the behavioral scourge of vaccine rejection spreads from person to person in localized communities. So those who are unvaccinated are more likely to live among others who are unvaccinated, increasing their collective probability of infecting each other.
The likely scenario is that while communities with high vaccine uptake will get to a point where outbreaks are small, self-delimited, and rare — other communities that remain poorly vaccinated will continue to experience larger, more common, and more deadly outbreaks. And the virus will remain a looming concern in the U.S.
The other issue is viral evolution. New seasonal variants will likely spread among us every fall and winter akin to seasonal flu, which kills tens of thousands of Americans every year. Some COVID seasons will be milder, some far deadlier. And just like the flu, we'll likely need annual boosters against it.
Some things change.
But the virus isn't the pandemic's only ingredient — just the foundational one. For people who never got sick, COVID-19 still changed their lives. There is, of course, no singular pandemic experience. For millions of low-income "essential" workers, the pandemic meant fearing every day that you might be infected at work, or worse, bring the virus home with you to infect someone you love. For millions of healthcare workers, the pandemic meant watching your patients die without their loved ones as you struggled to manage the overflow. For others privileged enough to work from home, the pandemic meant endless days of Zoom calls while your kids tried to learn across from you at the dinner table.
As I wrote previously, work from home is going to be a much more common feature of American life. Small businesses, major corporations, and even some government agencies have found that their workers are surprisingly productive from home — and have reconsidered plans to come "back" to work in the office. And workers themselves have found they like using their own bathroom and eating out of their own fridge at lunch.
Indeed, as many workplaces begin to plan to come back to the offices, workers are pushing back. After Apple CEO Tim Cook sent a note to Apple employees requiring them to be back in the office on Mondays, Tuesdays, and Thursdays beginning in September, Apple employees circulated a letter in response:
"We ask for your support in enabling those who want to work remotely / in location-flexible ways to continue to do so, letting everyone figure out which work setup works best for them, their team, and their role — be it in one of our offices, from home, or a hybrid solution. We are living proof that there is no one-size-fits-all policy for people. For Inclusion and Diversity to work, we have to recognize how different we all are, and with those differences, come different needs and different ways to thrive. We feel that Apple has both the responsibility to recognize these differences, as well as the capability to fully embrace them. Officially enabling individual management chains and individual teams to make decisions that work best for their teams roles, individuals, and needs — and having that be the official stated policy rather than the rare individual exceptions — would alleviate the concerns and reservations many of us currently have."
Other companies, like Dropbox, have preempted this demand simply by offering work from home options permanently.
Beyond employee preference, companies attempting to go back to a brick-and-mortar office space will face the question of risk tolerance. As we well know, some eschewed any sort of pandemic protection — be it a mask or a vaccine — from the jump. Others, despite being fully vaccinated, remain hesitant to share enclosed space. How to navigate lower risk tolerances remains a serious challenge. Part of making workplaces safe may mean mandating vaccines, which has prompted serious pushback in the courts of law and public opinion by anti-vaxxer activists who want to use the pandemic as another line of attack. Navigating these challenges is, in part, what is pushing more and more employers to offer alternative working arrangements. Needless to say, some alterations to working conditions because of the pandemic are likely here to stay.
Other things stay the same (again).
Some pandemic experiences were universal. For children, the pandemic has been a catastrophe. Not only has learning lagged, but children have been robbed of valuable socialization and milestones. Indeed, the consequences have been far worse for poorer students, disproportionately children of color, for whom access to quality WiFi and reliable computers are limited. All indications suggest that kids will be back to school in the fall as vaccinations among teachers and students press on.
Access to other people and the venues in which we enjoyed their company was limited if available at all. Restaurants, concert venues, theme parks, theaters — even stores and shopping malls — had limited access.
But that's changing. Prompted by the CDC's new guidelines for vaccinated people, many of these venues have rushed to reopen, and Americans are slowly but surely taking advantage. Flight traffic is increasing. Last week, LAX, one of the country's busiest airports, logged a 2021 record. And businesses can't hire people fast enough to accommodate their needs.
Though worries about COVID-19 exposure — particularly for children who cannot yet be vaccinated — persist. Yet as cases continue to fall, and vaccines are approved for younger and younger children, these, too, will subside.
The doomsday scenario.
But there remains a possibility that experiences of the pandemic we haven't had since last fall come crashing back. Cases climb, hospitals fill up, and thousands more Americans die. And that's a resistant strain.
We've now identified several variants of the virus that are more transmissible, and some more deadly, than the original garden-variety ("wild type") virus we experienced through most of 2020. Thankfully none of them have fully evaded our vaccine-mediated immunity. Yet.
Every single unvaccinated person presents an evolutionary opportunity for the virus. And even as the U.S. and other high-income countries approach a virus-stifling level of vaccination, the rest of the world continues to lag. Some countries have yet to get their first vaccines. New variants with frightening capabilities continue to emerge in these countries. Indeed, last week a new variant with aspects of the Alpha variant and the Delta variant emerged in Vietnam. So even as vaccine manufacturers roll out boosters to protect against the growing plethora of new variants, a doomsday scenario, where a more transmissible, lethal variant evolves, becomes more likely.
And so, we can't take for granted that this is a truly global pandemic. And until the rest of the world receives what they need to "end" this pandemic, we won't see our end either.
***
Dr. Abdul El-Sayed is a physician, epidemiologist, public health expert, and progressive activist who served as Detroit's health director and ran for governor in 2018. He is the author of Healing Politics: A Doctor's Journey Into the Heart of Our Political Epidemic and Medicare for All: A Citizen's Guide, as well as the newsletter The Incision. Get more at incision.substack.com.
21 notes
·
View notes
Text
Not Undertale related
I re-read the document with info on that Left 4 Dead alternate universe I made and I decided I’d share it here despite it not at all being Undertale related. I’ll put it under the cut if you’re interested! Warning, it’s long as hecc! And I mean... HECCIN long
Imagine the L4D universe after the remaining humans and military regained their foothold to fight the infected, and save themselves. Imagine they were aware of Carriers. Imagine this world wouldn’t just kill off the Carriers, and would treat them like humans (For the most part at least). They would create settlements completely divided, Carriers to their district, uninfected to theirs. The military would have a large amount of influence in these cities. The Carrier district would essentially be slums, or at least extremely poor. They would need to become self-sufficient, as the rest of humanity didn’t care for them or even wished for them to die out. These districts would be encased in walls. Some Carriers would say it’s better than being dead. Others would disagree.
Now, imagine Carriers went beyond simply being asymptomatic. What if Carriers did mutate? Rather than being simple common infected Carriers, what if (Based on the way the virus mutates depending on certain circumstances), the conditions for the virus to mutate into a specific special infected (Boomer, Smoker, Hunter, etc.) were met, but the Carrier didn’t turn? A new advanced special infected. Still retaining their sentience, still technically human, but much stronger. The military wouldn’t just leave them alone, they’d use them. This would implement Project Carrier. Any special infected Carriers would be rounded up and enlisted in the military. The better they did, the better the Carrier district did. They would, not only receive personal benefits, but would help the Carrier district receive better supplies. Medical supplies, food (as I imagine the Carrier districts would often be low on food), even improved living conditions. Carrier Soldiers would also be used in medical research to create a vaccine to combat the virus.
Despite this, Carrier Soldiers were seen as traitors to their kind, infected that needed to be killed by others, and experiments to the military. They’d be under constant surveillance to ensure they didn’t step out of line. Special infected were already smart enough to outsmart an unprepared soldier (Not that the military would admit that), and a Carrier Soldier was just a mutated human. If they weren’t kept on a tight leash, they could easily overthrow the military with enough careful planning. Thankfully, there were very few special infected Carriers.
This brings in all the technical stuff that I might get wrong.
The percentages of special infected to regular infected have been confirmed by in-game lore:

Special infected percentages are very low, the highest being 9% (The Hunter), (with Witches being unlisted due to either exceedingly low numbers or inability to safely study), which would mean that most special infected Carriers (Hereby called Special Carriers or SCs), would be Hunters most commonly. Of course I’ll write down theoretical abilities for each type of SC. Unfortunately there’s no information I could find that stated how many survivors were actually Carriers. Of course the in-game playable characters, but that would only amount to 8 (12 if you count the characters exclusive from the L4D survivors) out of all of the encountered NPCs, which of course I could use as a base if it weren’t for “The Sacrifice” comic, which showed the survivors heading to Millhaven and seeing a large amount of bodies being burned. It’s implied that these bodies were Carriers, but it’s also possible that they were simply people who died in millhaven or even common infected that were killed. This skews the numbers a fair bit, so I will use the original 8 survivors and NPCs listed in the wiki.
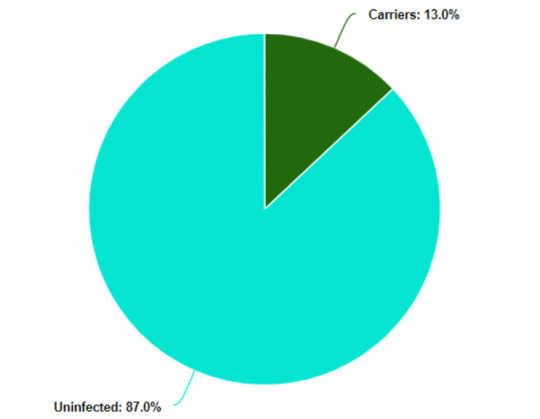
Rounding numbers up, Uninfected survivors would make up about 87% of the population while Carriers would be 13%. Based on the comics, Carriers are primarily male and the only female survivors would be the daughters of male Carriers. Since there are only 2 female survivors out of the 8, that would make a 25% chance of a female Carrier. This will become important later. Maybe.
Since we have a rough percentage of how many survivors would be Carriers, how many of them statistically would be SCs? Well thanks to more math, I have that answer. Using the two previous charts, I was able to make this fancy new chart.
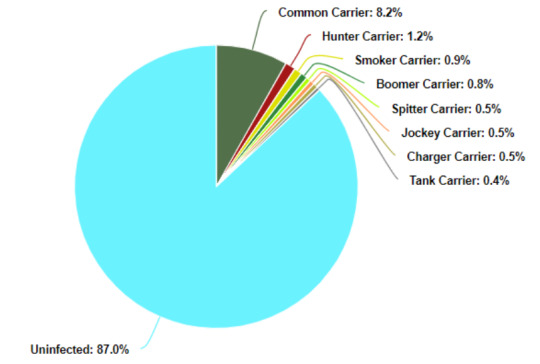
Again, due to a lack of data, Witch Carriers can’t be calculated accurately. However. We know that there is a rough percentage of 25% of Carriers being female, (Well, we don’t know that but let's assume it’s true). It can also be observed that some of the special infected seem to be gender restricted. Hunters, Smokers, Chargers, Jockeys, and Tanks all seem to be male restricted with Spitters being female restricted. (The Boomer is the only exception to this rule). If we subtract half of the percentage of Boomers (To make it simple) and the percentage of Spitters, we get a 24.1% of presumably Common female Carriers.
This is where it comes mostly up to assumptions and hypotheses.
We know that the Witches are just as, if not rarer, than Tanks which make up only 3% of all infected, and only roughly 8% of all Special Infected. We only see the Tank about 1-2 times (though 2 is rare on Expert) per level in L4D, and the Witch, (Excluding the Sugar Mill), has the same spawn-rate. This would make their rarity at least equal to that of the Tank. This would make both the Tank and the Witch roughly 4% of the Special Infected population, and 0.7% of all Infected. Now normally I’d assume that it would be easy enough to put the percentage of Witch Carriers into the chart, but the problem arises with the percentage of female Carriers, which, as you recall, is only 25% with 0.9% already being accounted for as Spitters and Boomers. It’s highly likely that the majority of the remaining 24.1% are Common Carriers, due to the circumstances required to become a Special Infected. Becoming a Witch infected is highly assumed to be a result of an altered mental state, (Loss of sanity or Depression), which is far different from the other infected. All the other infected seem to have a physical condition met in order to become said Special Infected, (Health problems, excess of certain chemicals, etc.).
Now of course you could say, “Well everyone just went through the apocalypse, wouldn’t they all be hella depressed?”, and I would say “Yeah probably.”. However, there is a difference between feeling depressed and clinical depression. It would be a bit far-fetched to assume that all Witches were diagnosed as clinically depressed, but I believe it would make more sense due to the fact that every person can experience depression, but not every person is clinically depressed. Otherwise, I believe there would be a much higher rate of Witch infected if the cause was simply depression on it’s own.
A study in 2016 showed that about 10.4% of women were found to have depression. (Yeah outdated, I’m sure the number is higher now, but we’re using this one). This can be applied to our charts, however there is no way to tell how much of this percentage lies within the Carrier community. Majority of this percentage is certainly within the Uninfected community, purely based on the low percentage of women within the Carrier community. Only 3.25% of women would be Carriers in this scenario, leaving over 96% of women uninfected. Because of this, statistically, we can assume next to none of the Carrier women are clinically depressed. To keep things simple, I’m going to go with the assumption that less than 0.1% of Carriers become Witch Carriers.

Now that we have all of the statistics out of the way, what exactly would these SCs be like? How extensive are the mutations? I have theories! I’ll continue that in the next post though, since this is already long as hecc... Their abilities are a lot more interesting, so stay tuned!
#Not undertale#Still interesting though!#To me at least...#Maybe that's because it's my au#Left 4 Dead#l4d#Alternate universe#Luna's rambles#Luna's writing#Project Carrier
9 notes
·
View notes
Text
COVID-19 : The past, the present and the future
11th of march 2020 - a day that will go down in history books marking the start of one of the deadliest pandemics in the history of mankind. COVID-19 : CO for corona, VI for virus, D for disease and 19 for when the outbreak was first identified. December 2019, Wuhan saw the occurrence of the first case of a highly infectious, often fatal respiratory virus. It proliferated faster, killing thousands and spreading all over the world.As of present day more than 168 million cases have been recorded along with about 3.51 million people losing their life to this disease.
WHAT IS COVID-19 ?
Contrary to popular opinion, coronavirus is not a new type of virus. Coronaviruses are a category of closely related RNA viruses that infect birds and mammals. In humans and birds, they cause upper-respiratory tract infections which may be of varying degree from minor to fatal. The earliest case of coronavirus infection dates back to North America in the late 1920s.
When an acute respiratory infection of domestic chickens emerged.This infection was characterised by breathlessness and gasping and high mortality rates. Human corona viruses were first identified in the 1940s and new coronaviruses have been discovered since then which includes the SARS-CoV-2 (virus that causes Covid-19) in 2019. Most human coronaviruses originate from bats. There are seven known human coronaviruses that cause respiratory illnesses. But COVID-19 is caused by a new virus that has not been observed in humans before.
BACKGROUND :
The exact origin of the virus to this day remains unknown. The first outbreak is believed to be in Wuhan, Hubei , China in late 2019. Most early cases are related to the people who consumed meat in the Huanan Seafood Wholesale Market in Wuhan. However it's possible that the spread had been going on long before this incident.
A lot of conspiracies surround this topic from people believing that this is a man made virus and leaked from a laboratory. However nothing concrete can be said as of now. America’s top infectious disease expert Dr.Anthony Fauci says that he is not convinced that the virus is natural. Many scientists have again called for an in depth investigation. American Intelligence agency has reasons to believe that The Wuhan Institute Of Virology, Chinese Academy of Sciences has some relations to the virus although there is no concrete proof as of present time.
HOW DOES THE VIRUS SPREAD : TRANSMISSION
Covid-19 is an air-borne, droplet infection that enters the body from the respiratory tract. While speaking, breathing, talking the infected person may release droplets that enter the atmosphere and can be breathed in by a non-infected person resulting in a successful transmission of the virus. The probability of transmission depends on the time of interaction, their relative proximity although researchers prove that infection can occur over long distances particularly indoors. Small airborne particles tend to stay in the environment for longer periods of time while larger droplets either fall on surfaces or stay suspended for a while. In poorly ventilated areas, the droplets stay in the sir for minutes or hours. In september 2020, it was established that on an average an infected person spreads the disease to one to three people. Covid-19 spreads in clusters hence “ super-spreader events” have a huge role in the transmission.
Surface transmission i.e. spread through touching contaminated surfaces is also a likely yet rare possibility. The virus is not known to spread from animal carriers, faeces, urine, breast milk, water etc.
ASYMPTOMATIC CARRIERS
In medicine, any person who tests positive for the disease but fails to show any symptoms is termed as an asymptomatic carrier. When someone gets infected with the virus, it takes about five days to even two weeks to produce symptoms varying from mild to dangerous ones.
Current research suggests that most of the transmission occurs from symptomatic people and not from asymptomatic people. However a vast majority of people are asymptomatic. The reason is yet unknown
WHAT ARE THE WAYS TO END THE PANDEMIC
The WHO is likely to declare the pandemic as over when the infection is contained and the transmission rates drop around the world.
The governments around have 3 main options : Race through it, Delay and vaccinate, or coordinate and crush.
Race through it : In this the global governments do little to nothing to contain the spread of the infection therefore exposing people to the virus.The results of this would be ghastly; millions of people with compromised immune systems will die around the world, health care systems will collapse. In a couple of months most of the people would have been infected and either survived or died. Around this point herd immunity will kick in resulting in the virus to fizzle out as it can no longer find new host bodies.
Delay and Vaccinate: In this the global governments give researchers time to study the virus to produce vaccines and effective ways of treating the infected. They employ methods like masking, planned lockdowns and contact tracing to reduce the spread of the virus. However the virus will spread slowly leading to hundreds of thousands of deaths. And in about a year or so many vaccines would have been developed and after vaccinating about 50-90% of the population the pandemic will end.
Coordinate and crush : The principle here is to starve the virus around the world but instead of each leader acting according to their own jurisdiction, everyone will coordinate and work together treating the world as a huge family. With a combination of social distancing, restricted travels, social distancing the pandemic could be ended with minimum life loss and in a considerably small amount of time.
The best way is to delay and vaccinate with as much global cooperation as possible. It is a tried and tested winner amongst the methods. It's slow, steady and reliable. Even if the herd immunity kicks in before the vaccination is done and the pandemic starts to fizzle away. It may resurface later and vaccination will protect people and from the situation ever escalating further.
WHAT IS A VACCINE ?
Vaccine is a biologically prepared typically containing an agent that resembles the pathogen.
The antigen is prepared from the weakened or the dead form of the disease-causing microorganism or its toxins or the surface proteins. The basic principle of it is that the vaccine works as an antigen stimulating an immune response leading to the formation of antibodies.
The body recognises the agent as a threat, destroys it and further recognises the agent and destroys any microorganism that associates with it in future.
HOW WILL THE VACCINE HELP END THE PANDEMIC ?
Vaccination is critical for reaching the herd immunity threshold which will help us go back to normal life.
Herd immunity or mass immunity is an indirect form of protection from an infectious disease produced when enough people become immune to the disease either through the mode of vaccinations or through getting infected.
This helps us disrupt the chain of transmission since the people who are immune to the disease are unlikely to transmit it further.Some of its effects are that it helps us protect those who can't get vaccinated due to underlying medical conditions or are unable to develop immunity.
Even help us protect our young ones who can't be administered a lot of vaccines.
Herd immunity acts as a method of creating evolutionary pressure and encourages viral evolution. If herd immunity is reached and can be retained for a long period of time, it would eventually lead to the eradication of the disease as a whole. For example- smallpox etc.
Keep hope all this shall pass too.
@influencedgenetics
9 notes
·
View notes
Text
Fubar Part I
Written by Dante Augello. America has reached a point that is unrecognizable to me or anyone I know has ever experienced. I have mentioned this before, but I downplay how unprecedented all this is in my mind. Living in Los Angeles I might see more of this than many. Obviously, we are all experiencing these things though. After the country has been in various stages of the shutdown we are agitated, depressed, and radicalized possibly more than any time than I have ever seen.

I've tried to be optimistic, but it’s difficult as I’m sure most people know. Coronavirus cases are higher in Los Angeles than they have ever been by more than triple from when Los Angeles started to open. Protests over police brutality are ongoing in Los Angeles and throughout the country. The national guard was called in recently, driving around the city with M 4s and active denial systems mounted on their Humvees, speeding from protest to protest, and creating an ominously oppressive vibe all over my neighborhood.
“People are buying guns more than ever for fear of economic and social collapse”
There is a 6 block radius being occupied in Seattle called an “autonomous zone” where they claim to no longer use money and that they do not want police to enter the area. All in response to George Floyd’s death. Talk of defunding or completely getting rid of certain police departments are being put into action all over the country as well, which could have very interesting effects. People are buying guns more than ever for fear of economic and social collapse, so much so that complaints of the highly complicated, expensive, and bureaucratic gun laws of California are starting to anger people of all political parties.

Some of these issues will prove benign, however, others are capable of literally causing some type of civil war. With this much unrest and people out of work, its a perfect environment for such events to spiral out of control. However, I am not a fear monger. I do think we will come out of this, maybe not unscathed but relatively so, for this kind of turmoil is not only scary but exciting. These events bring a crackle of life to the changes in policy and governmental organizations that could be made. Changes that could positively affect this country for the entirety of its existence. However short it seems it may be.
First of all Covid 19 is not going away any time soon. Now that the government is steadily opening up Los Angeles and the rest of the state, coronavirus is rapidly increasing transmission. Not only in California too, but many states have seen higher rates than they ever have before. Masks seem to do little to help the incessant spreading as well, so it seems odd to put so much emphasis on keeping them on at all times, unless indoors. The only time it really makes sense for outdoor use of a mask is in large crowds, but UV light from the sun tends to kill any free-floating viruses almost immediately. Also, getting a 1000 dollar fine for not wearing a mask outside is truly preposterous. However, Until there is more research, it's probably better to keep them on if only to avoid the ticket.

Thousands every day are being diagnosed with coronavirus and unfortunately, we are coming up onin Fall in a few months, which could very well mean a second wave. In hindsight, we should’ve closed earlier, and at this point, it seems we made another huge mistake by opening too early. Nonchalantly murdering an unarmed black man on camera was another momentous disaster, which rightly caused a large amount of angry protesters to huddle in groups screaming and chanting all day spreading the disease much much more. However, we have found some promising things out about this virus. It's not nearly as deadly as we thought it was going to be thankfully, and with proper nutrients, sleep, and exercise it’s doubtful it will cause many problems for you.
Also, vaccines that may work well are being tested regularly. Unfortunately, we do not know that much about it, mostly because it is so new to causing humans sickness, which leaves the possibility of recurrence unknown. we also don’t know how often this virus will mutate. If it mutates regularly and if it's like the flu, that could mean that there will be another Coronavirus outbreak every year just like the flu. This would cause just as much damage or more than the flu does, and that would be on top of the damage the flu already causes. What we are seeing right now is all our efforts being flushed down the toilet. The government has screwed us by closing too late and in turn completely destroying the economy, and now they are opening too early. Similarly destroying the progress we had made trying to get rid of the virus. At this point, it seems it could have been better to not close at all, but that depends on our priorities. Protecting the population with weaker health, or protecting the economy. Unfortunately at this point, we haven’t done much of either by constantly switching our strategies, essentially canceling each other out.

4 notes
·
View notes
Text
He’s going to get us all killed.

May 11, 2020
On numerous occasions in the last four years, provisional president Darnold Trump has come close to dragging us into a murderous war — with Iran, with Venezuela, with China, with any country whose leader didn't flatter him sufficiently. And we're all aware of how his cruel policies and thoughtless utterances have endangered thousands of immigrants, women, Jews, the poor and people of color throughout the nation.
However, in the midst of a nationwide pandemic, Trump's laziness, ignorance and fixation on getting reelected whatever the consequences constitute a deadly threat to the existence of each and every American. Ignoring the informed warnings of federal health officials, he repeatedly advocates to "reopen America," even while admitting many people will die as a result. He's still pushing the potentially dangerous drug hydroxychloroquine. And has even suggested injecting people with disinfectants as a COVID-19 treatment. All of which simply demonstrates his utter disregard for the lives of anyone not named Trump.
But he's also applied more indirect measures to ensure as many people as possible die of COVID-19. Like crippling the World Health Organization by cutting off its funding (the US is by far its biggest donor). Currently, this agency of the UN provides technical assistance to health workers caring for COVID-19 patients, as well as guidance to the public on how to protect themselves. But someone (probably a Faux News idiot) told Trump it was too "China-centric." So no funding for them.
Then there's the EcoHealth Alliance, a 45-year-old organization that works across borders to support medical research of all types. Trump evidently found out it gave some money to a lab in Wuhan, China for research into how SARS-CoV-2 — the coronavirus causing the current pandemic — moved from bats to humans. Right-wing politicians and media accused this lab (without any evidence, naturally) of letting the virus escape. So no funding for them, either.
These two organizations are making possible the research necessary to identify this lethal virus, sequence its genetics, determine its source, uncover how it works, and figure out how to fight it. Without them, we'll likely not have a coronavirus vaccine or treatment any time soon. And a lot more people will die unnecessarily.
Trump's maladministration has clearly embarked on a policy designed to kill American citizens by the thousands in the name of the US economy and (more importantly) Trump's reelection. Appallingly, his supporters seem perfectly fine with this. Maybe the Republican Party should add "bring back human sacrifice" to their 2020 platform.
10 notes
·
View notes
Text
The Fauci Files
At 79 years old, Dr. Anthony Fauci — who has served as the director of the National Institute of Allergy and Infectious Diseases (NIAID) since 1984 — has yet to come out with the “Big One” — a vaccine or infectious disease treatment that will allow him to retire with a victory under his belt.
He failed to create a successful vaccine for AIDS, SARS, MERS and Ebola. A COVID-19 vaccine is essentially his last chance to go out in a blaze of glory. As evidenced by his history, he will stop at nothing to protect Moderna’s COVID-19 vaccine and Gilead’s antiviral Remdesivir.
He even threw tried and true pandemic protocols out the window when COVID-19 hit, turning into an unquestioning spokesman for draconian liberty-stripping measures instead. To echo a question asked by Dr. Sal Martingano in his article,1 “Dr. Fauci: ‘Expert’ or Co-Conspirator,” why are we not questioning this so-called expert?
Fauci ‘Has Been Wrong About Everything’
The risk we take when listening to Fauci is that, so far, he’s been wrong about most things. In a July 14, 2020, “Opposing View” editorial in USA Today, White House adviser Peter Navarro, director of the Office of Trade and Manufacturing Policy, stated that Fauci “has been wrong about everything that I have interacted with him on.”2 According to Navarro, Fauci’s errors in judgment include:3
• Opposing the ban on incoming flights from China in late January 2020.
• Telling the American people the novel virus outbreak was nothing to worry about well into February.
• Flip-flopping on the use of masks — first mocking people for wearing them, and then insisting they should. In fact, mid-July, he suddenly urged governments to “be as forceful as possible” on mask rules.4
• Claiming there was only anecdotal evidence supporting the use of hydroxychloroquine, when the scientific grounds for it go as far back as 2005, when the study,5 “Chloroquine Is a Potent Inhibitor of SARS Coronavirus Infection and Spread,” was published in the Virology Journal.
Fauci should have been well aware of this publication. According to that study,6 “Chloroquine has strong antiviral effects on SARS-CoV infection of primate cells. These inhibitory effects are observed when the cells are treated with the drug either before or after exposure to the virus, suggesting both prophylactic and therapeutic advantage,” the study authors said. In other words, the drug worked both for prevention and treatment.
As noted by Navarro, more recent research found hydroxychloroquine reduced the mortality rate among COVID-19 patients by 50% when used early.
Interestingly, in a March 24, 2020, interview7 with Chris Stigall, Fauci did say that — were he to speak strictly as a doctor treating patients — he would certainly prescribe chloroquine to COVID-19 patients, particularly if there were no other options.
Then, in August, he flipped back to insisting hydroxychloroquine doesn’t work,8 even though by that time, there were several studies demonstrating its effectiveness against COVID-19 specifically.
So, it appears Fauci has had a hard time making up his mind on this issue as well, on the one hand dismissing the drug as either untested or ineffective against COVID-19, and on the other admitting it would be wise to use, seeing how the options are so limited.
Navarro continues:9
“Now Fauci says a falling mortality rate doesn’t matter when it is the single most important statistic to help guide the pace of our economic reopening. The lower the mortality rate, the faster and more we can open. So when you ask me whether I listen to Dr. Fauci’s advice, my answer is: only with skepticism and caution.”
Fauci Has Done Nothing to Help Unite the Country
While Fauci claims to be exasperated by how political the pandemic has become,10 Robert F. Kennedy Jr. pointed out in an August 2, 2020, Instagram post11 that Fauci himself is, at least in part, part of the problem, as his double standards on hydroxychloroquine have done much to polarize and divide the nation:
“Fauci insists he will not approve HCQ for COVID until its efficacy is proven in ‘randomized, double blind placebo studies.’ To date, Dr. Fauci has never advocated such studies for any of the 72 vaccine doses added to the mandatory childhood schedule since he took over NIAID in 1984. Nor is he requiring them for the COVID vaccines currently racing for approval.
Why should chloroquine be the only remedy required to cross this high hurdle? HCQ is less in need of randomized placebo studies than any of these vaccines since its safety is well established after 60 years of use and decades on WHO’s listed of ‘essential medicines.’
Fauci’s peculiar hostility towards HCQ is consistent with his half century bias favoring vaccines and patent medicines. Dr. Fauci’s double standards create confusion, mistrust and polarization.”
In a June 10, 2020, article,12 Global Research also questioned Fauci’s many attempts to disparage the drug for no apparently valid reason; even promoting the fake (and ultimately retracted) Lancet study that claimed to show hydroxychloroquine was dangerous. At the end of the day, who benefits? Well, certainly it benefits the drug and vaccine industries, which seems to be where Fauci’s loyalties lie.
Fauci’s Bias Is Hard to Miss
While Fauci is not named on the patents of either Moderna’s vaccine or Remdesivir, the NIH does have a 50% stake in Moderna’s vaccine,13 and the recognition that would come with a successful vaccine launch would certainly include Fauci.
He also has lots to lose — if nothing else, his pride — if Remdesivir doesn’t become a blockbuster, as his NIAID is sponsoring the clinical trials.14 The NIAID also supported the original research into Remdesivir, when it was aimed at treating Ebola.15
His bias here is clear for anyone to see. April 29, 2020, he stated16 Remdesivir "has a clear-cut and significant positive effect in diminishing the time to recovery." How good is that? Patients on the drug recovered in 11 days, on average, compared to 15 days among those receiving a placebo. Overall, the improvement rate for the drug was 31%.
Meanwhile, research17 now shows hydroxychloroquine reduced mortality by 50% when given early, and many doctors anecdotally claim survival rates close to 100%. This still isn’t good enough for Fauci, who continues insisting hydroxychloroquine is a bust.18
His stance on these two drugs certainly doesn’t make sense based on the data alone. But it does make sense if he wants (or has been instructed) to protect the profits of Remdesivir.
As director of NIAID, which has been part of Remdesivir’s development from the start, why wouldn’t he want to see it become a moneymaker for the agency he dedicated his career to? It also makes sense when you consider his primary job is to raise funds for biodefense research, primarily vaccines but also diagnostics and drug therapies.19,20
Fauci Doubts Safety of Russian Vaccine
Early in August 2020, Russia announced they would begin vaccinating citizens with its own COVID-19 vaccine, despite not finishing large-scale human trials.21 The announcement drew skepticism from American infectious disease specialists, including Fauci, who said he has “serious doubts” that Russia’s COVID-19 vaccine is actually safe and effective.22
Fauci conveniently ignores the many failed attempts to create other coronavirus vaccines over the past two decades, including vaccines against SARS and MERS.
He’s probably right on that point. It’s hard to imagine you can prove safety and effectiveness in a mere two months of trials. But the fast-tracked vaccine efforts of the U.S. and EU are hardly bound to be significantly better, considering the many shortcuts that are being taken.
Fauci Ignores Two Decades of Failed Coronavirus Vaccines
Despite being in a position to know better, Fauci conveniently ignores the many failed attempts to create other coronavirus vaccines over the past two decades, including vaccines against SARS and MERS. A paper23 by Eriko Padron-Regalado, “Vaccines for SARS-CoV-2: Lessons From Other Coronavirus Strains” reviews some of these past experiences. As noted in the Conservative Review:24
“Since their emergence in 2003 and 2012 respectively, no safe and efficacious human vaccines for either SARS-Cov1 or MERS have been developed.
Moreover, experimental non-human (animal model) evaluations of four SARS-Cov1 candidate vaccine types, revealed that despite conferring some protection against infection with SARS-Cov1, each also caused serious lung injury, caused by an overreaction of the immune system, upon viral challenge.25
Identical ‘hypersensitive-type’ lung injury occurred26 when mice were administered a candidate MERS-Cov vaccine, then challenged with infectious virus, negating the ostensible benefit achieved by their development of promising … ‘antibodies’ … which might have provided immunity to MERS-Cov.
These disappointing experimental observations must serve as a cautionary tale for SARS-Cov2 vaccination programs to control epidemic COVID-19 disease.”
NIAID Safety Controversies and Ethics Violations
When recently asked for a rebuttal to criticism of his leadership during the pandemic, Fauci replied, “I think you can trust me,” citing his long record of service in government medicine. However, that long service record is fraught with ethics and safety lapses.
For example, in 2005, NPR reported27 the NIH tested novel AIDS drugs on hundreds of HIV-positive children in state foster care during the late 1980s and90s without assigning patient advocates to monitor the children’s health, as is required by law in most states.
Fauci was appointed director of the NIAID in 1984. The AIDS research was part of his research portfolio, and the AIDS research division reported directly to him, so these violations occurred on his watch.28 In 2008, two NIH biomedical ethicists published a paper on the controversial practice of using wards of the state as guinea pigs, noting:29
"Enrolling wards of the state in research raises two major concerns: the possibility that an unfair share of the burdens of research might fall on wards, and the need to ensure interests of individual wards are accounted for ... Having special protections only for some categories is misguided. Furthermore, some of the existing protections ought to be strengthened."
Under Fauci, the NIAID became the largest funder of HIV/AIDS in the world.30 Despite that, numerous articles over the years have discussed how AIDS activists have been less than satisfied with Fauci and the NIAID.31,32,33 A 1986 article stated:34
“If Fauci were less intent on amassing power within the federal health bureaucracy … he would have left AIDS treatment research with the NCI, where it began, relying on that institute's proven expertise in organizing large, multisite clinical trials for cancer therapies."
A July 23, 2020, article in Just the News lists several other safety and ethics problems that Fauci has been involved in through the years, including conflict of interest violations in vaccine research.35
Just the News also interviewed NIAID chief of ethics and regulatory compliance Dr. Jonathan Fishbein, whom the NIAID was forced to reinstate in 2005 after it was determined that Fishbein had been wrongly fired in retaliation for raising concerns about lack of safety in some of the agency’s research:36
“Fishbein said … Fauci failed to take responsibility for the managers and researchers working below him when signs of trouble emerged, allowing problems to persist until others intervened. ‘Fauci is all about Fauci,’ Fishbein said. ‘He loves being the headline. It’s his ego.’”
Fauci’s Connections to Wuhan Lab
By now, you probably also know that the NIAID funded gain-of-function research on coronaviruses at the Wuhan Institute of Virology. As reported by Newsweek:37
“In 2019, with the backing of NIAID, the National Institutes of Health committed $3.7 million over six years for research that included some gain-of-function work. The program followed another $3.7 million, 5-year project for collecting and studying bat coronaviruses, which ended in 2019, bringing the total to $7.4 million.”
This money was not given directly, but rather funneled to the Wuhan lab via the EcoHealth Alliance. According to a recent report by The Wall Street Journal,38 the NIH is now insisting EcoHealth Alliance submit all information and materials from the Wuhan lab before it’s allowed to resume funding.
Fauci is a longtime proponent of dangerous gain-of-function research. In 2003, he wrote an article39 published in the journal Nature on how “the world needs new and creative ways to counter bioterrorism.”
“We will pursue innovative approaches for modulating innate immunity to induce and enhance protection against many biological pathogens, as well as simple and rapid molecularly based diagnostics to detect, characterize and quantify infectious threats,” Fauci wrote.
“These are lofty goals that may take many years to accomplish — but we must aspire to them. Third, we must enormously strengthen our interactions with the private sector, including biotechnology companies and large pharmaceutical corporations.
Many biodefence-related products that we are pursuing do not provide sufficient incentives for industry — the potential profit margin for companies is tenuous, and there is no guarantee that products would be used.
Therefore, we will seek non-traditional collaborations with industry, for example guaranteeing that products will be purchased if companies sign up … so that we can quickly make available effective vaccines and treatments …”
With that, there can be little question about which team Fauci is on. He’s on the side of drug and vaccine makers, and has been for decades. There’s no money to be made by either the agency or its private collaborators from natural products such as vitamin D, vitamin C, quercetin or its drug equivalent, hydroxychloroquine. All of these are dirt-cheap and off patent.
Prediction Track Record = Null
Fauci’s predictions for COVID-19 mortality have also turned out to be as inaccurate as all of his previous predictions. In 1987, he predicted heterosexual infection of HIV/AIDS would rise to 10% by 1991. It never rose above 4%.
He predicted the bird flu would result in 2 million to 7 million deaths. In the end, the avian H5N1 flu killed 440 worldwide. He sought billions of dollars to combat the threat of Zika, a virus that fizzled without making much of an impact anywhere.40
When you look at his track record, you realize he’s predicted “nightmare” scenarios for decades, none of which have materialized. Last but not least, Dr. Fauci serves on Bill Gates leadership council.
1 note
·
View note
Text
Stream of Consciousness Texts That I Sent to A Large Grouptext of Friends at 2 AM Again Like The Unhinged Woman I Am: Coronavirus and Chronic Illness Edition
——————-
My dad started talking about giving my brother hope about the school year and going back to school, and I’m realizing that’s probably happening before the vaccine (which will likely come out around January). What the heck am I gonna do? Do I need to move out? Schools are gonna be where this thing spreads. My brother will bring it home, I don’t know what I’m going to do about it?
I wish I were healthy so the prospect of living on my own wouldn’t be so scary. I’m so weak and exhausted, I feel like making three meals a day, doing my own laundry and cleaning, and somehow handling groceries (I guess Shipt and sanitizing them myself) would be too much for me to do alone with my limited energy. And that’s not even taking into account factors like what to do in flares when I’m BEYOND sick like can’t get out of bed, or finding a place safely, or not losing my mind alone. I don’t know, I haven’t really thought about this.
I just want to be healthy, guys.
It’s so upsetting because this could’ve been over months ago if the majority of people took it seriously quickly. If everyone stayed inside for just two frickin weeks we could’ve been fine. But now some of us may have to do it for a year because this stupid country isn’t even compassionate enough to sacrifice two gotdang weeks for the weakest of us. And I’m one of the lucky ones, able to stay in like this for maybe a year! Others just die! I’m frustrated that this is a situation in the first place, and I’m frustrated that I’m sick enough that it still could kill me even months after people have stopped caring. I never asked for this. I’ve done everything I can to be healthy. I spend more time trying to improve my health than any one of you and yet I’m the one still sick at the end of the day with very few improvements. I’m so tired.
I would be tired even without Covid, but this is just highlighting the inequity in disability. It’s highlighting the privilege many have of being able to NOT worry about health, about doing nothing to stay healthy and still having infinitely more energy than someone working hard on health and getting nowhere. God I wish I could be as carefree as those spring breakers hanging out in crowds on the beach for no reason other than they can and they don’t care. I wish I didn’t have to care. I still would, but I wish it wasn’t forced upon me. I hate that even if individuals have basic empathy (which of course many don’t), our system lacks it. This country makes me sick. Literally.
I wish I could just fly to another country with low Covid numbers (one that allows flying in if you obey their mandatory quarantine), quarantine for two weeks, then start over. I’m sick of this country anyway. Unfortunately, that would require me to be in a US airport and in a US airplane, so I can’t even do last resort stuff.
And I doubt anyone has the same level of quarantine we’re doing here- no outside cooked food, just cookable groceries. Thoroughly sanitizing everything that comes in. Not even leaving the house for work or grocery shopping. And most importantly the fact that I’ll be doing it until I’m positive it’s safe, which will probably be until there’s a vaccine.
I guess I’ll just super-quarantine in my own house. Stay six feet away from everyone. Everyone wearing masks at all times. No touching anything that anyone else might touch. I don’t know, it just seems daunting to know that many months from now things will not only have not improved for me, but will have gotten worse. Especially since this whole thing was entirely preventable- I wish Cheeto in Chief had an ounce of compassion. I wish he was punished with the disease- even if he had survived it might’ve taught him it was real and dangerous early on. I wish my life mattered to this country, this system, and to millions of people here. I mean, if you knew someone would die if you didn’t simply stay in your house for two weeks, wouldn’t you do it? I can’t believe that same logic doesn’t apply to lives like mine for so many people.
Anyway, what do I have to look forward to when all this is over? Shopping? Restaurants? Seeing friends maybe once a week? Petty. It’s all petty. I wasn’t working toward anything before this except for health, and that’s not going to be fixed because I can’t even get any blood tests right now, let alone have doctors do any in-person appointments and important checks like MRIs, X-rays, CT scans. Everything put on hold and nothing on the other side. You all have jobs and education and lives outside of the house- I really don’t. I mean, I had a part time job but it’s not like it’s working toward something, and I may have lost it in the pandemic anyway. You have jobs and new houses and apartments and boyfriends and education and children and energy to do pretty much anything you need to do and exciting or productive lives to live. What do I get when I come out of this? Probably just a bunch of cavities to fill because this happened when Sjögren’s Syndrome started melting my teeth and they can’t do much without more tests. I really have nothing to look forward to- that’s part of why this has been easy (I’m not missing much) but it’s also why thinking ahead proves to be just... disturbing. I try to stay positive but my day to day life has felt pointless for a long time, and in the short term that doesn’t matter, but god it’s a terrible thing to confront when I recognize that my only two options in a few months are going to be stay inside and feel sick OR leave my house and feel sick, and either way I don’t get anything done or really work toward anything except feeling ok, which I may never. I may never feel ok! I miss feeling like I have purpose. I still have ambition but it’s undirected because honestly I don’t think I have the energy to do any of the stuff I used to picture myself doing. So I don’t know what I want to happen here. Honestly this virus and my quarantine could go on for years and I would feel the same as I do now. I felt stuck long before the quarantine, because I’m not stuck in this house, I’m stuck in my own weak body.
And I’m sure this is disturbing to read because I’m kinda mildly fine most of the time and optimistic and positive and all that, and I know I blow up probably once a week at this point so maybe it doesn’t even seem that way anymore??? At least I still act that way in person, lucky you guys get to read my terrible rants. But I just want someone to see this, you know? I want someone to know that me being positive isn’t an accident, that it’s hard work against the mountain of garbage being thrown at me mostly by MY OWN BODY. It’s terrible in concept. I’m actually feeling fine right now mentally but I need someone to know the concepts I’m wrestling with: the fact that my worst enemy is me and it’s by no fault of my own. I was dealt a bad hand. Even in the very best of circumstances, without Covid, I’m living a pretty unfulfilling life. Sickness makes it hard enough- to be at higher risk of death or permanent damage in addition to that is just cruel. I just wish I could project this into everyone’s brain so they could understand why it matters so much that people freaking care about each other enough to protect each other from having even more difficult lives- or even deaths. I want to survive!!!! I’m clawing at the walls of suffering until my fingernails bleed!!! I keep it in my head that I’m gonna get out of this pain someday even if that’s not necessarily true!!! All I want is to live and to live well. I just want to live well. I’m happy to live and to survive so it’s gotta get better someday. I just wish the world cared a little bit more. I wish I had something tangible and fulfilling to look forward to. In this moment, I can be happy and read a book or watch TV, but I wish the other type of happiness was a factor in my life again, the sense of fulfillment and accomplishment. Sickness has taken so much from me.
1 note
·
View note
Text
Worth Any Risk, chapter 3
Description: Shortly after Ethan’s return to Edenbrook, he tries to pick up where he left off as if nothing happened. When MC becomes gravely ill, he is reminded that there some things worth any risk.
My MC is named Olivia House.
Ethan monitored Olivia closely, hoping that this was just a harmless bug. But his experience as a doctor told him to never assume the least, to always be prepared.
A couple hours after Olivia fell asleep
again, a shudder went through her body. It was enough to startle her awake. She winced at the ache that radiated through her.
“Rookie? How are you feeling?”
“Terrible.” When Ethan handed her the thermometer, Olivia checked her temperature. “102.5.”
That made Ethan frown. “It’s gone up a degree and a half in two hours with acetaminophen.”
Olivia’s stomach rolled uncomfortably. Feeling bile rise in her throat, she pressed her lips shut tightly. Fortunately there was a trash bin nearby and Ethan grabbed it quickly, all too familiar with the signs of imminent vomiting. Moments later, Olivia retched, emptying the contents of her stomach into the bin.
Ethan put his hand on her back, running his mind to try to narrow down the causes. A stomach virus wouldn’t account for the rapidly rising fever. Vomiting wasn’t particularly common with the flu.
Olivia shuddered when she leaned back. She took a sip of water, trying to rinse out the bitter taste. “I don’t think I’ve ever felt this sick… everything hurts.”
“Be more specific. You know this, Rookie. We need to figure out what’s wrong before we land.”
She let out a tired chuckle. “They say doctors make the worst patients.”
“We do.” She cringed as she rolled her shoulders, trying to work the kinks out of her neck.
“Hang on…” Ethan placed his hands on either side of her neck, gently turning her head in each direction. His heart skipped a beat when he felt resistance. “Your neck is stiff.”
“I’ve been sleeping all day on a plane.”
“Hmm.”
Olivia’s face paled. “You have an idea.”
“I need to look at your back.”
Nodding, Olivia scooted to the edge of her seat and leaned forward. Ethan lifted her shirt, feeling his stomach drop when he saw a reddish-purple rash dotting the small of her back.
Olivia frowned. “Ethan? You’re… not saying anything…”
Ethan let out a deep breath, trying to remain calm for her sake. He couldn’t lie or sugarcoat it, but there was no sense in causing even more panic than necessary. “Olivia…. I think you have meningitis.”
It took a long moment to register his words. Her face fell. “How could I have contracted it? I’ve had all the vaccinations, I haven’t had patients with it…”
“Sometimes it can be more resistant. Symptoms usually begin a few days after exposure, so you could have been exposed to it at the airport or in Auckland.”
Olivia closed her eyes, combing her mind for everything she learned about meningitis in medical school. “Meningitis usually starts with a fever that rises quickly… stiff neck…” As she rattled off symptoms, the more her heart pounded. “It can kill in 24 hours.”
Ethan grabbed her hand. “We’re not at that point yet. Someone on this flight is bound to have antibiotics of some sort. Probably not the specific type we need, but anything is better than nothing. We need to focus on slowing down the progression of the illness until we land.”
Olivia didn’t look convinced. “We don’t land for another fourteen hours…”
“Not if I can help it. We can try to land somewhere along the way and you get stable enough before we go to Edenbrook.”
“And how long would that be?”
“...I don’t know. But I do know that I’m going to see if there are any antibiotics whatsoever on this plane. You need intravenous steroids and corticosteroids. I don’t expect to find those, but I’ll use whatever I can find for now.”
Olivia forced a weak smile. “Look at you, taking medicine from random strangers. But… you shouldn’t be
near me. If I have meningitis, you could contract it.”
Ethan shook his head. “I’ll take the preventative antibiotics when we get back to Edenbrook. I’m not leaving you alone.”
The younger doctor sighed. “Stubborn as always.” She closed her eyes as Ethan left, undoubtedly to interrogate random passengers for any antibiotics they may have in their possession.
She dozed off, only to wake up a few minutes later when she heard Ethan return to his seat next to her.
“Did you find anything?”
His face fell. “Only amoxicillin. It’s not going to have a strong effect, but it’s worth seeing if a larger dose can at least lessen the symptoms.”
Olivia nodded weakly. “I’m willing to try anything at this point.” She picked up her water bottle and let Ethan help her sit up. She swallowed several tablets with a swig of water.
“I asked the attendant to have this section of the plane evacuated. Now the bathroom There aren’t many people on this flight, but you don’t need everyone making a spectacle out of you.”
“Thank you… I don’t really want my uncontrollable puking to be a performance.” Olivia pulled Ethan’s warm sweater tighter around herself.
“Your temperature must be rising again.” His face knitted with concern as he pressed his palm against her forehead. “You’re burning up.”
Even though she was shivering, Olivia felt sweat beading down her face. “It’s climbing fast…” Her voice wavered. “If I’m not dead before we land, there could be serious complications…” When tears stung her eyes, she quickly tried to blink them back.
She had to stay calm. Panicking would only worsen her situation. But she knew that without treatment soon, her chances weren’t in her favor.
“Stop that,” Ethan chided. “You’re not dying on my watch. Yes, there is a significant risk of complications. But we’re going to focus on making sure you survive. And you will.”
Olivia forced a watery smile and rubbed at her eyes. “You sound sure.”
Ethan absently touched her cheek. Whether he was making his promises to her or himself, he didn’t know. He knew that if she didn’t get treatment soon, she could be dead in a matter of hours. He just hoped that they would land far before that time came.
“I’ll do whatever I can to make sure you’re around to irritate me for years to come, Rookie.”
She swallowed hard and closed her eyes when a painful tremor went through her. “I… I don’t think I’ve ever been this scared…”
Ethan’s chest constricted at the fear in her voice. “I know… I haven’t, either,” he admitted softly. She was the one who could be dying, and all he was doing was making promises he couldn’t keep in an attempt to ease his own fear.
At that, Olivia opened her eyes. “How? You’ve seen it all…”
His face fell. “It’s… it’s different when it’s someone I care about.” Ethan swallowed the lump in his throat. “It’s why they don’t let doctors treat their family or friends. Their fear affects their judgment.”
Olivia reached for his hand. He let her take it and squeezed gently. She closed her eyes again, letting a stray tear escape. As Ethan wiped it away with his free hand, she leaned into his touch, longing for comfort.
“I’m right here…” Forgetting any boundaries he had insisted on having, Ethan smoothed her hair back. “I want you to rest. I’ll keep an eye on you.”
He couldn’t lose her.
Chapter 4
Tags: @isabella-choices @peekaboochu @foulcroissantknightpalace @teamdrake27 @edgiestwinter @samara-rani @drakewalkerfantasy @perriewinklenerdie @drakesensworld @msjpuddleduck If I missed anyone, or you’d like to be added or removed, please comment.
#open heart fanfiction#ethan ramsey#ethan ramsey x mc#choices: stories you play#choices: open heart#open heart#ethan ramsey fanfiction
86 notes
·
View notes
Note
I think I still got sick with the flu even after I got the vaccine last time. So I don't want to get it again. Why is everyone blogging to get the vaccine?
Ah the good old flu vaccine. Good question, thanks for asking!

The flu is caused by the influenza virus, and there are 4 types, A, B, C, and D. But human influenza virus A and B are what cause people to get sick every winter. Influenza A is sub-typed based on two proteins on its surface - hemagluttinin (H) and neuraminidase (N), and then further broken down again by strains - that’s why you might have heard something like “back in 2009, the H1N1 caused a pandemic.”
As the virus keeps replicating, it goes through genetic changes, something called antigenic drift. As these changes accumulate, the more different the next strain is from the last ones. So your body might not have immunity against the vaccination you got a year or two ago. Which is also why each year the vaccine needs to be reviewed and/or updated to reflect the changed virus.
It’s possible you acquired the virus a few days before you got your shot, so when you got sick, you attributed it to getting your shot. Or you got sick within the 2 weeks after the shot - it usually takes your body about 2 weeks to develop immunity and protection.

It’s also possible you got sick with another more common virus, a rhinovirus, which causes the common cold. The symptoms are similar and there are no vaccinations for those, and no, you can’t get antibiotics for them either.

The vaccination is especially important for those at high risk - children, older adults, pregnant women, and those people with chronic conditions. It can save you a trip to the ER!
I mean, the influenza virus is probably some kind of mutant zombie virus just trying to take over the human population and the world (amiright Doc @cranquis?) So get your shots, and let’s put off the apocalypse a bit longer, at least…

704 notes
·
View notes
Text
We hear it every year, year after year…”This is going to be the worst year for ticks yet.” It seems to get worse every year. If this is unfamiliar to you, you might be fortunate enough to live in an area where the concern is not so prevalent. In the northeastern United States, however, you’d be hard pressed to find a group that hasn’t expressed concern.
Why ticks?
These tiny vile creatures spread several diseases, most commonly Lyme Disease. Since May is Lyme Disease Prevention Month let’s work to understand HOW Lyme is transmitted. We’ll also explore some steps we can take to keep ourselves and our animals (horses, dogs, cats) safe.
In 2017 nearly 30,000 cases of Lyme disease were diagnosed and another 13,000 were suspected as “probable.” Most of these cases originated in the northeastern United States as seen in the map below thanks to CDC.gov. The chart following shows the upward trend of Lyme disease throughout the years.
Cases confirmed in the United States 2017. Courtesy of CDC.gov
Cases of Lyme Disease in the United States 1997-2017 courtesy of CDC.gov
Ticks are arachnids, or eight-legged creatures, that thrive in deep grass and wooded areas. Often areas where our horses enjoy, of course. There are several different species of tick and they all have different life cycles, feeding habits, and habitats.
What is a bit more alarming is a new tick to the United States called the Asian Long-horned tick, which can reproduce without a mate. The video below talks briefly about it.
youtube
Most of the time when we think of ticks we think of the most common threat; the deer tick/black-legged tick. The deer tick is often the source of Lyme disease along with several other illnesses including Anaplasmosis, Powassan, and Tick-Borne Relapsing Fever. Blade suffered from anaplasmosis in 2017 (Blade’s Got the Blues and Equine Affaire).
The deer tick begins its life cycle as an egg laid by the females in springtime. By summer the larva emerges from its egg and waits for a host. Hosts are typically birds and small rodents.
Freshly hatched ticks they are free of the bacteria that causes Lyme disease. Only when they feed on their hosts do they pick up the pathogens. In the United States the bacteria transmitted is either Borrelia burgdorferi or Borrelia mayonii. Across the pond in Europe and Asia you are more likely to find Borrelia afzelii and Borrelia garinii.
The birds and rodents that feed tick larva carry these species of bacteria without illness; they are simply hosts. By fall the tick falls from its host and enters its nymph stage. The nymphs are barely visible to the human eye. These critters lay dormant through the winter but by April/May they begin to emerge again. They wait for a host to walk by so they can catch a ride. Using their barbed mouth parts, the tick digs in for a blood meal. The pathogen inside the tick enters the salivary glands and can be released through the tick’s saliva. These hosts include us and our loved ones. Nymphs are often the cause of Lyme disease since they are small and difficult to spot.
By fall the nymphs become adults looking for new hosts. At 45°F they seek wooded areas to survive the winter. When they emerge again in spring they continue to look for hosts and mate. A single female tick can lay 3000 eggs! After a two-year life cycle the new batch of larva hatches and begins the cycle again.
As you can see, we can become infected by both the nymphs and the adult ticks. The more hosts carrying the bacteria, the more likely it is to spread to us.
The hallmark sign of Lyme disease is the bullseye, a circular rash around the bite. Symptoms may appear weeks after the bite. This appears in a majority of cases…but what of our equine friends?
Horses suffering from Lyme Disease may have subtle symptoms. They might be off mentally, emotionally, and physically. They may be sore or lame, lethargic, grumpy, neurological, or have a low-grade fever. Lyme is known to mimic other issues so a vet is critical in ruling out other problems. Lyme will also elude testing, as there are many cases of Lyme that appear negative on test results.
I’m even learning that Lyme can be a cause for some headshaking in horses. Headshaking is not commonly listed as a symptom nor have any of my vets over the past two years suggested the possibility. This is, however, something I plan on looking into after this research. As you may know from past articles, Blade developed headshaking about 18 months ago (shortly after his run with anaplasmosis). Though our tests were negative it could have been one of those instances with a false negative.
Once Lyme has been diagnosed (or suspected) there are a few treatment options.
The most common treatment is called Doxycycline, an ingestable antibiotic often given in a powdered form with food. A similar drug is called Naxcel. Despite their popularity with horse-owners they only happen to be 50% effective.
The most effective treatment is more pricey… a study in 2005 reported 100% effectiveness. The reoccurrence levels were considerably lower in the study as well. What’s this treatment you ask? Daily intravenous oxytetracycline. My vet once called it the “gold standard.” The reason most horse-owners don’t opt for this treatment is the administration. Having a vet visit and administer the shot every day for 3-5 days is pricey so most horse owners use the Doxy.
If I remember correctly I paid somewhere around $450 for three daily IVs of Oxytet for Blade.
So what are some ways we can prevent this problem from happening in the first place? As the Benjamin Franklin saying goes, “An ounce of prevention is worth a pound of cure.”
Lyme vaccines for horses are not available yet. Studies have shown some effectiveness using canine vaccines on ponies, but it is still far too early. There are no studies out (yet) showing the safety of this methodology. Until we have vaccines we are tasked with the footwork that we should be doing anyway.
Checking for ticks often is the first thing you should be doing. Check yourself, check your dogs, check your cats, check your horses. It takes 24 hours for a biting tick to transmit the disease. I tend to find most ticks under the cheek, the neck, the chest, and the barrel (especially up behind the back legs).
There are a lot of Facebook experts who have tips, tricks, and endless opinions on tick removal. The simplest thing you can do is use a good pair of tweezers and pull the tick up slowly and steadily so you remove the whole bug. Another useful tool can be found in most pharmacies and pet stores. The tick twister. This little hooklike tool comes in a couple sizes (at least mine had 3 sizes in the package). When you find a tick you slide the bug between the openings at the end so it becomes wedged. From there twist and pull gently. I have successfully removed many ticks using this tool and I love it. After a tick is removed you may choose to save it in a plastic bag for testing. Apply alcohol or antibiotic ointment to the affected bite wound to be safe.
Since ticks prefer wooded areas, you can try to stay out of these areas. That’s easier said than done if you enjoy the outdoors.
Keeping the grass and pasture mowed can be helpful.
Removing piles of leaves and moist ground cover is an excellent way to prevent ticks. That leftover hay pile? Let’s get rid of it!
Keeping down the rodent population could be useful. Non-poison rodent traps, barn cats, and proper food storage go a long way.
Chickens and guinea hens love to eat ticks!
DEET and permethrins are of course some good chemicals that have proven efficacy for the prevention of ticks and other pests. Some people use them others don’t. That’s your choice to make. There are many products on the market including fly sprays, spot-on applications, and even wipes.
I have had mediocre success with feed through pest repellant. The more I use it the less effective it seems to be (though the first year seemed to make a big difference).
If you are opposed to chemicals more research has been finding useful essential oils that are as effective as the CDC recommended products. The key to the best product is perfecting the volatility ratio of oils. High volatility essential oils disperse into the air faster. This helps by preventing ticks from attaching in the first place. Lower volatility oils will disperse into the air more slowly and have a longer lasting effect. Check out the Tisserand Institute’s “Tick Talk” (link below) for more information on these oils. I’ve also shared with you their formulation for DIY tick repellant.
Credit to Tisserand Institute
The thought of ticks and the disease they spread makes my head hurt. Lyme disease is rarely fatal but it does lead to some frustrating and debilitating complications.
Other diseases like Powassan are rarer but a lot more deadly; this virus is associated with brain swelling. Here in New York we are already beginning to hear reports of Powassan virus. One group has found 25-50% of deer in the Adirondacks are positive for the virus and it only takes 15 minutes for the tick to transmit the virus to humans.
Whether Lyme, Anaplasmosis, or Powassan we can take steps to stay healthy and prevent ticks from biting. It may take some time and effort but it’s completely worth it.
What are some of the methods you use to keep ticks at bay?
REFERENCES AND FURTHER READING
http://ssequineclinic.com/pages/services_lyme.html
https://ker.com/equinews/lyme-disease-horses/
https://equusmagazine.com/management/protect-against-lyme
https://www.vet.cornell.edu/animal-health-diagnostic-center/testing/protocols/lyme-multiplex-horses
https://igenex.com/ticktalk/2018/01/01/a-closer-look-at-the-different-types-of-ticks-and-how-to-identify-each/
https://www.cdc.gov/lyme/stats/graphs.html
http://www.aldf.com/deer-tick-ecology
https://www.cdc.gov/ticks/life_cycle_and_hosts.html
https://www.cdc.gov/lyme/index.html
https://www.lymedisease.org/get-involved/take-action/lyme-awareness-month/
https://tisserandinstitute.org/tick-talk-2/
https://www.adirondackdailyenterprise.com/news/local-news/2019/02/powassan-virus-on-the-up-tick/
What Ticks Me Off We hear it every year, year after year..."This is going to be the worst year for ticks yet." It seems to get worse every year.
#Animals#Family#Health#Horse#horselover#Horses#LymeDisease#LymeDiseasePreventionsMonth#Prevention#TheGreenHorseman#Ticks
1 note
·
View note
Text
Science and Chemistry Classes
Expert discusses the spread of omicron
by University of Waterloo
12/01/2022
Everyone needs to do their part, wearing appropriate masks, staying home if they're symptomatic or told that they're going into isolation, and getting whatever dose of vaccination they're eligible for as soon as they can.
Before becoming the President and Vice-Chancellor of the University of Waterloo last year, Vivek Goel supported Canada's response to the pandemic as a member of the Federal COVID-19 Immunity Task Force. He also served as scientific advisor for the CanCOVID Network, which is a national network of researchers in the areas of health, science and policy created to promote collaboration on COVID-19 research. As we face omicron, the latest variant of concern, Dr. Goel discusses the ways it has changed the pandemic, its impact on society, and what to do about it.
We hear omicron isn't as severe or as deadly as previous variants, but there has been explosive growth in hospitalization. Can you help us make sense of that?
I think it's important to think about the impact of the virus as opposed to the severity of the virus. The impact of the virus on the population is driven by a number of factors. One of them is how fast it goes from one person to the next, how transmissible it is. The second is how bad the disease hits each person it infects—the virulence of the virus—and the degree of protection each individual has from either getting the disease and/or the severity of the disease if they do get it, and that's their prior immunity.
And so, when we talk about comparing omicron to the delta variant, or the alpha variant before that, or the original wild-type variant, which was first detected in Wuhan, you can't just say: "Is it more severe or not?" because it's comparing all these different characteristics at once. And the evidence is still evolving.
What we do know is that the impact of this particular variant, the omicron variant, is less than the impact of delta at the individual level. But that is in large part because of the prior immunity that our population has. And there is some evidence to suggest that the virulence of the virus—the degree of disease that it causes in people who are infected—is also less than that of the delta variant, the one that just came immediately before. But the amount of that is still being established. There are some people who are saying that the virulence is probably still about the same as the original wild-type variant.
What is different about omicron?
Where the omicron variant clearly has as an advantage is its transmissibility. Each person it infects is going to infect many more people. And again, the numbers vary, but it's probably about at least two to three times more than delta, and two to three times delta was two to three or more times than alpha. And alpha was more than the original.
So, it's many times more transmissible than the original virus that we saw back in late 2019, and that spread around the world in the beginning of 2020, and probably causes about the same severity of disease in each person that it infects. If we can think back to the early days, when it was first appearing in Italy or New York, and we saw ICUs being overrun, if we had had this virus back then we would have had total devastation throughout the world because it is many times more transmissible but can still cause severe disease in those that don't have prior immunity.
The reason we're talking about it having less severity, or being "mild," is because since the beginning of 2020, we have started to build up population immunity, and it's built up in two ways. One, people have become infected with the disease. And we've got the vaccines, allowing people to be protected against infection to a certain degree. But more importantly, vaccines have allowed people to be protected from having really bad consequences if they do get infected.
What we're seeing with omicron is the vaccines are less protective against infection with omicron than they were for delta and the earlier variants. But they still protect against being hospitalized or needing to go into the ICU and go onto a ventilator, and they protect against death. What's happening right now is we're seeing a very rapid spread of this particular variant because the prior immunity, either from disease or from the vaccines, does not protect to the same degree against the transmission.
So we're seeing the cases in vaccinated people, but we're not seeing vaccinated people being hospitalized at the same rate, or needing intensive care, or having the unfortunate consequence of passing away. That's why we can wind up with a situation where we'll have a headline saying, "It's not as severe, it's not as deadly." That's in large part because of this prior immunity that we've built up, especially from vaccines.
What does this all mean on a larger scale?
Even if we believe it is "mild," it's still having devastating consequences for us as a society. And that's because of a couple of things. One, because it is spreading as a disease and even in vaccinated populations, it is spreading to many people all at the same time. That results in a lot of absenteeism, either because people have been infected, or because they've been exposed and they're asked to go into isolation as a result of that.
The other consequence for the health system is that because it's infecting so many people all at once, there's still going to be a certain proportion hospitalized. And even if that proportion is very small, a fraction of one percent, when you have millions of people infected at the same time, that very small percentage multiplied by that many people at the same time, results in a lot of people having to go to hospital.
The final thing I'll just say on this is we still have 10 to 15 percent of people who haven't been vaccinated or haven't had their two doses. There's a certain fraction of those that are children under five, for whom we still don't have vaccines approved, and the children five to 11, for whom the vaccine was just approved a few months ago, and so they're still in the process of getting vaccinated.
So, again, omicron spreading into that population is going to result in a higher rate of hospitalization, because even though COVID has been generally milder in children, as it starts to spread so fast, there are just going to be so many children being infected at the same time, we will start to see hospitalizations rise in that population. And then we have adults who have not been fully vaccinated. Unfortunately, what we are seeing in our hospitals right now is the vast majority of people being hospitalized and almost all the people needing to be in intensive care and having to have ventilators are the unvaccinated.
What can members of our community do?
Make sure you continue to follow public-health precautions. Over these next few weeks, we do need to hunker down and limit our daily contacts so we reduce the amount of transmission. We need to ensure we don't further overwhelm our health-care system and that we're able to maintain our essential services.
0 notes
Text
Coronavirus: How to stay safe on a flight
New Post has been published on https://www.travelonlinetips.com/coronavirus-how-to-stay-safe-on-a-flight/
Coronavirus: How to stay safe on a flight

Holidays have now resumed under the government’s traffic-light system, particularly in light of the lifting of quarantine for amber-list arrivals who’ve been fully vaccinated.
As more people find themselves leaving on a jet-plane for pastures new, they may find it’s a very different experience compared to pre-Covid times.
From social distancing and wearing masks at the airport to limited food on aircraft, measures aimed at minimising the spread of coronavirus are now common.
But just how risky is flying? And is there any way to guarantee safety? Here’s everything you need to know.
How should I get to the airport?
Before you even arrive at the airport, there’s the getting to the airport bit to consider.
Public transport carries a greater risk of coming into contact with new people – and therefore a greater risk of coming into contact with coronavirus – than travelling by car.
However, as The Independent’s esteemed travel correspondent, Simon Calder, would point out, driving or getting a taxi carries its own risks: road traffic accidents claim around 1,800 lives in the UK every year.
Essentially, every mode of transport carries some kind of risk. But if your main concern right now is catching Covid-19, a car is probably the best way to go (being sure to wear a mask, keep the window open and wash/sanitise your hands before and afterwards if you’re catching a cab). If travelling by public transport, mask-wearing is still recommended in the UK.
How can I stay safe at the airport?
At the airport itself, new measures are now widespread, such as social distancing and mandatory face coverings for passengers and staff.
Although travellers often fixate on planes as a hotbed of germs, the airport is potentially a much more risky proposition, bringing together people from all over the world.
Keeping your distance from those outside your household, regular hand washing or using hand sanitiser, and wearing a mask are the most important steps to take. But there are other ways to limit contact with others too: check in online and print off your boarding pass in advance where possible.
When it comes to luggage, there are two opposing stances to consider.
The Department for Transport (DfT) last year recommended that passengers check in all baggage, saying: “This will speed up boarding and disembarking and minimise the risk of transmission.”
However, Ryanair had a different take, arguing that taking hand luggage reduces the number of hands your bag passes through by a substantial amount, cutting out various baggage handlers on either side of the journey.
Airports empty as Coronavirus affects aviation industry
Show all 11
1/11Airports empty as Coronavirus affects aviation industry
Airports empty as Coronavirus affects aviation industry
Ben Gurion International airport, Israel
Reuters
Airports empty as Coronavirus affects aviation industry
Daxing International Airport, Beijing
AFP via Getty
Airports empty as Coronavirus affects aviation industry
Taoyuan International Airport, Taiwan
EPA
Airports empty as Coronavirus affects aviation industry
Noi Bai International Airport, Vietnam
AFP via Getty
Airports empty as Coronavirus affects aviation industry
Haneda Airport, Tokyo
Reuters
Airports empty as Coronavirus affects aviation industry
Changsha Huanghua International Airport, China
Reuters
Airports empty as Coronavirus affects aviation industry
Shanghai Pudong Airport in Shanghai, China
EPA
Airports empty as Coronavirus affects aviation industry
Daxing International Airport, Beijing
AFP via Getty
Airports empty as Coronavirus affects aviation industry
Haneda Airport, Tokyo
Reuters
Airports empty as Coronavirus affects aviation industry
Shanghai Pudong Airport in Shanghai, China
EPA
Airports empty as Coronavirus affects aviation industry
Noi Bai International Airport, Vietnam
AFP via Getty
The airline’s CEO Michael O’Leary told The Independent last summer: “We’re recommending passengers do exactly the opposite [of the DfT advice]: maximise carry-on bags and minimise checked-in bags. Even though, clearly, we make more money out of checked-in bags.
“Our logic has always been that checked-in bags are handled by eight pairs of hands, from the check-in desk to the boarding gate, all the way through to the arrival airport as well – whereas a carry-on bag the passenger keeps with them at all times.”
Avoiding checked-in luggage also means you don’t have to congregate around the baggage carousel with lots of other people after your flight. This means you’re better able to follow the DfT’s other piece of advice: “Leave the airport as quickly as possible.”
There are risks either way – but airlines have made it very clear they will not be reducing their, at times hefty, rates for checking in a bag.
Elsewhere, trays at security are often a hotbed of bacteria at airports as they pass through so many different hands each day. (A study conducted in 2016 even suggested the trays are home to more respiratory viruses than public toilets.)
After you’ve gone through security and removed your items from the trays provided, ensure you sanitise or wash your hands as soon as possible, being sure not to touch your face in the meantime.
How can I stay safe on the aircraft?
On board the aircraft, the DfT advises passengers to: remain seated as much as possible; follow instructions and guidance from crew; use contactless payment where possible; be aware there is likely to be reduced food and drink service; and make the cabin crew aware if you become ill.
Most airlines will require you to wear a mask onboard when not eating or drinking, and will provide hand sanitiser.
In England, Scotland and Wales passengers must wear a face covering onboard the aircraft; in Northern Ireland the measure is “recommended”. (Some airlines are very specific about which types of masks they deem acceptable – check the rules before you fly.)
If you’re flying short-haul, going to the toilet just before boarding could help eliminate the need to go while on the aircraft, meaning less movement around the cabin and less chance of coming into contact with a coronavirus carrier.
This may seem like hair splitting, but studies have shown that those who move a lot around the cabin are more likely to pick up a bug.
In a 2018 study tracking the “behaviours, movements and transmission of droplet-mediated respiratory diseases during transcontinental airline flights”, a research team led by Atlanta’s Emory University found that those in window seats had far fewer encounters with other passengers than people in other seats.
This is due in large part to the fact that those by the window were less likely to get up from their seat, with just 43 per cent moving around the aircraft compared to 80 per cent of people in aisle seats – meaning they were less likely to come into contact with potential virus carriers.
One of the study’s diagrams showed the likelihood of travellers coming into contact with one designated infectious passenger based on where they’re sitting. Other than those sitting on the same row as patient zero, all window seat passengers had a five per cent or less chance of coming into contact with them. Most had a 0-1 per cent probability, far lower than their middle and aisle seat counterparts.
Opting to take a window seat could, therefore, lower your risk of catching something – but the most important thing to remember is that the less you move around the plane, the lower the likelihood of you coming into contact with a virus carrier.
Are planes more dangerous than other modes of transport because of the air circulating?
Like other modes of transport and all enclosed spaces, there is a risk of virus transmission.
One medical report, released in November 2020, found that a passenger who had tested negative for coronavirus before a flight went on to infect four others during the journey.
A total of seven passengers sitting in relatively close proximity to one another ultimately tested positive for Covid-19 following the flight, stated the report from New Zealand’s Institute of Environmental Science and Research.
Another study suggested that the risk of catching coronavirus on long-haul flights is “real” after a single passenger infected 15 others on the same plane – although this did occur before masks were being widely used. The unnamed businesswoman, 27, flew from London to Vietnam during the early days of the pandemic, on 1 March 2020. She had a sore throat and a cough before boarding the 10-hour service, and tested positive for Covid-19 a few days later.
However, previous research has highlighted that the risk of catching something on a plane is pretty low in general.
The probability of actually being infected by “patient zero” was just 0-1 per cent for the vast majority of all passengers, apart from those sitting on the same row or across the aisle, according to the 2018 study mentioned earlier.
What a flight looks like in lockdown
Many travellers have the misconception that they are more likely to get ill after a flight because they presume the “same air”, carrying every passenger’s sniffle, sneeze or cough, is getting recycled and pumped around the aircraft.
In fact, modern jets have very advanced air filtration systems, making transmission via the air you breathe onboard extremely unlikely.
David Nabarro, WHO special envoy for Covid-19, previously said that air travel is “relatively safe” when it comes to the spread of coronavirus.
“The one good thing about aeroplanes is that the ventilation system includes really powerful filters which means that in our view they are relatively safer,” he told BBC News.
“Given the excellent ventilation system on modern commercial aircraft and that the main method of transmission [of respiratory infections] is by direct contact and/or airborne droplet, most risk is isolated to those passengers sitting in the same row or that behind or in front of someone sick,” Dr David E Farnie, medical director of Global Response Centre for MedAire Worldwide, told The Independent.
The International Air Transport Association (IATA), which has done extensive research on the topic of air transport and communicable diseases, backs up the assertion that people onboard an aircraft are no more likely to fall ill than anyone in a confined space.
Its fact sheet on Public Health Emergency Preparedness highlighted the importance of modern air filters on planes, which “have a similar performance” to those used to keep the air clean in hospital operating rooms and industrial clean rooms.
“Hepa (high-efficiency particulate air) filters are effective at capturing greater than 99.9 per cent of the airborne microbes in the filtered air.”
The modern cabin air system delivers around 50 per cent fresh air and 50 per cent filtered, recirculated air.
“Air supply is essentially sterile and particle-free,” says IATA. Research published by IATA in October 2020 suggested that catching coronavirus on a flight was less likely than being struck by lighting.
It found that between January and July 2020 there were just 44 cases where coronavirus was thought to have been transmitted during a flight. This number included confirmed, probable and potential cases.
At the same time, the industry association said that 1.2 billion passengers travelled by air in that time, representing a one in 27 million probability of catching Covid-19 on a flight – significantly less than the chances of being struck by lightning, which is around one in 500,000 according to the US Centers for Disease Control and Prevention.
In essence, getting on a plane carries a similar risk to entering any confined space with others – there is no way of eliminating the danger completely, so masking up and being diligent about your personal hygiene is your best bet.
What are airlines and airports doing to maximise safety?
A host of measures have been introduced by the aviation industry since the pandemic started.
Most airlines have reduced their food and drink offering, plus are demanding contactless payment onboard. They are also doing much more regular deep cleans and cabin disinfection – for some carriers this will be undertaken daily, for others it will be done after every single flight.
A process called ‘fogging’ has also been rolled out by some airlines. It involves spraying a high-grade disinfectant through a fog machine throughout the cabin – this aerosolises the disinfectant and means it sticks to all surfaces, including seats, trays, ceiling, floors and bathrooms.
Other carriers have adopted Ultra Violet cleaning technology. Qatar Airways, for example, bought six Honeywell UV Cabin Systems, saying the tech “has been shown to be capable of inactivating various viruses and bacteria”.
About the same size as a refreshment trolley, the system features extendable UV arms that can treat seats, surfaces and cabins without using cleaning chemicals.
Numerous airports have made use of similar technology: Heathrow, Doha and Pittsburgh airport are among those that have deployed UV cleaning robots to kill microbes in frequently used areas.
Less tech-heavy methods are also being employed. At Heathrow airport, hundreds of hand sanitiser dispensers have been installed, social distancing and one way systems are in place, perspex screens have been put up and there is anti-viral cleaning of all key passenger touchpoints .
Source link
0 notes