#or Cosmo Kramer talking about anything
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Users from the US are the majority of Tumblr visitors.
Text
Has this romance novel ad pop up while I was looking at gifs from Seinfeld and honestly took a moment to realize it wasn’t from Seinfeld.
#Why does it have the exact cadence of somebody from Seinfeld talking about like a Twix bar or something#ETA: Upon further analysis this is either: George Costanza talking about a Twix bar#Jerry Seinfeld talking about George Costanza talking about a Twix bar#or Cosmo Kramer talking about anything
16 notes
·
View notes
Text
Seinfeld Characters If They Hid In Walmart For 24 Hours (together)
Featuring: Cosmo Kramer, Jerry Seinfeld, Elaine Benes, George Costanza, Newman, Kenny Bania
~•~

Cosmo Kramer
• It would definitely be his idea
• He would get caught first
• Run around the store and try on clothes and shoes and have a fashion show
• Would for sure hide in one of those big tubs and struggle to get out
• Would dance in front of the security cameras
• Would get banned and escorted out

Jerry Seinfeld
• Would be opposed to the idea because he wouldn’t want to break the law (but he would cave in eventually)
• Would most likely hide in a metal shelf or even in the back, near the employee’s break room
• He would say jokes into the security cameras
• Would talk to himself as he hides 
• Be one of the last ones caught
• Would get banned (honestly everyone except Bania)

Elaine Benes
• Would want to do it just because she’s bored
• Definitely wants to do a fashion show alongside Kramer
• Would hide with Jerry in the metal shelf or hide in the metal toy bin under all of the toys
• Would be the second person to get caught
• Would most likely giggle to herself as she hides
• Would fall out of her hiding place attracting attention
• If a kid passed by, she would try and scare them (George and definitely Newman would do this as well)
• Would try to flirt with the cops if they were called and arrested her

George Costanza
• Would only do it because he has nothing better to do
• Would capture the attention of many kids and some adults
• Definitely try and hide inside of a plastic tub but would either get stuck or uncomfortable
• Would talk to himself
• Would walk around the store to memorize everything and because he’s bored
• Would be the first one to find a spot to hide in
• Would complain if he got caught and argue with the worker or security guard
• Would stutter if confronted by a worker

Newman
• Would giggle and laugh as he runs around the store
• Dance in front of the cameras with Kramer
• Would try and scare kids by throwing objects at them or turning toys on (activating them, please know what I’m talking about)
• He would definitely jump into the toy bins laughing manically
• Would be one of the first few people caught
• He would definitely open the food and drinks (and not replace them)
• Would definitely get banned from the store after he gets caught (and arrested)
• Would definitely sneak into the back room (the employees’ break room) and read their mail

Kenny Bania
• Would be the last one caught
• Would try and hide with Jerry
• He’s a small motherfucker so he’d fit into practically anything
• Would wear clothes that matched the hiding spot (example: Black clothes with a black shelf)
• Would offer to get food (some Walmarts have restaurants inside)
• Would pick out items and pay for them before the store closes
• Would try and keep a low composure so he wouldn’t be suspicious
• Wouldn’t get banned but a reprimand (at least he paid)
#shifttok#shifting realities#seinfeld#george costanza#Newman#jerry seinfeld#Elaine Benes#cosmo kramer#Kenny Bania#imagines
5 notes
·
View notes
Note
HI HEY I am bursting into your ask box like Cosmo Kramer busts through his neighbour's door. I'm working quite irregularly through my backlog atm and regret that it's taken this long to get asks to you BUT I submit for your kind consideration the following OC Interview Asks to pass on to Yara my beloved :D (also I send her (and naturally you as well!) an excited wave and like seven thousand cool rocks)
16. Describe your perfect day 21. Describe your ideal partner 31 (freebie)- Tell me about your ideal house. Would it be big? What kind of colours/styles/things would you keep in it?
*first time trying to write her speaking, so sorry if it’s clunky and took a long while! She can be kind of verbose sometimes, Also, small text is quiet mumbling to herself, and bold is louder/more rushed excited speech. Tak tak tak is equivalent to “yes yes” “so” or “well well well”. Yolki-Palki (fir trees-sticks) is a euphemism for “fucking hell”. Sbornaya solyanka (solyanka soup with everything on hand) is an equivalent of “hodgepodge”.
Yara lifts her arm halfway up, more akin to one lifting their hand to ask a question than a wave, and smiles at you. She seems to be hard at work fiddling with something rather small, all the while throwing uncertain ~~bashful~~ glances at the formidable pile of rocks. She takes a deep breath.
“It’s good to see you, Plant. Tea? I have a great fruit one right-“ she seems unsure of how to approach the gift, giving off a slight deer-in-the-headlights feeling, albeit a distinctly pleased one “O - for me? Thank you. I didn’t expect such an addition to my collection- oh, you should see it when it gets organized!” The latter part of the sentence is significantly louder and faster than the rest as she claps her hands together “I’ve acquired a lot of new specimens from my last trip to Orzammar, even got my hands on some very curious raw lyrium…” she gives you a conspiratorial but overly exaggerated wink. She might not be very good at winking “of course, it is not to come into contact with anything, but it’s fascinating..!”
16) “Ah! My perfect day? Tak tak tak.. “ she drums her fingers on the table introspectively before reaching for a journal and leaning back, the next words coming out in a mumble “That’s a lot to fit into 24 hours… or, are you talking daytime? 12 hours, then? A perfect day… perfection is a bit of a difficult concept… Well, Zev would need to be there, of course, and Mishka should come too, and it would need to be somewhere nice - no, that’s too cold, and that’s a bit crowded, and I don’t think they allow dogs after last time- I think the gardens near the central market would do fine, they got some new plants - some quite toxic too ! - and there is the duck family and some of the people who come there are really weird! (Is probably firmly cemented in the neighborhood as one of said people, but the irony is lost on her) Yes, I think he’d like that. That and the more interesting shops…oh, and the fruit tarts! No, Mishka, my perfect day doesn’t include you eating the ducks! You can always make your own list!” The Mabari peeks over her shoulder, and sighs dramatically. He doesn’t have opposable thumbs. “Alright, we can stop by for some treats and take a few toys…Plus, I think this alleyway is quite infamous for murders lately, so that’s always fun!! To solve I mean. Or commit. Both is good..” she grins to herself ……at this point, it looks like she’s building a schedule. There is a murder slot. It’s a pretty big one. Mishka seems pretty excited about it.
21) “Oh, I already have one! Elvhen, Antivan, about 165 centimetres…no, that doesn’t seem right, I mean… that’s not..” There is a period of silence as her face appears to take on a grim expression, offset only by its clear shift to a bright red hue as she glances towards the other room. “He’s perfect, but I’m not sure how to put it into words. I haven’t ever thought about that kind of thing… he’s … he’s fun, and smart, and skilled in a scary amount of things, and takes things lightly and in stride. and …he cares, y’know? I s’pose that’s what caught me off guard the first time.” She fiddles with the knife in her hands some more, contemplating her answer “His position was complete garbage, y’see, but he still tried to have the best time he could, and he was very… straightforward in some ways…. Kind, even. T’ be honest, I didn’t get that at all” she chuckles, desperate to hide her embarrassment “Especially towards me. Other people I can understand, admire, even, but he just… spoke his mind when it counted, consequences be damned, and made sure everything was alright, despite everything… I know the feeling, and the conditions, and it’s hard to care about anything , much less so others. I’m … unsure of whether that answers your question.” She now seems genuinely amused. “Yolki-palki, leave it to moi to fall for an assassin’s kindness of all things. He made such a funny face when I told him, too… in my defence, the ~seduction~ went right over my head the first time and he’s wonderful and really should’ve seen it coming..”
31) “I’d say the place is pretty big.. it’s got a solarium, and a library, and some Knick knacks we picked up on the road..” it is unclear if she means the move, the travelling, or their journey through Ferelden as the road, but by the looks of it, it is a bit of everything. Weaponry and gems, among other things, appear as exhibits visible almost everywhere throughout the house. A wide smile precedes her next words “ a garden, too, and we’ve even managed to start up something of a brewing business. Plenty of room for ingredients. Style wise, well, it’s a sbornaya solyanka to be sure. We haven’t changed too much” she shifts in her seat. While the place does appear to house quite a few out-of-place items seemingly either handmade or closer to the Renaissance styling, both older and newer, clearly added in rather recently, the home appears to have been designed in a pretty consistent Gothic styling. “- it was a gift from an … old benefactor.”
After adding a few finishing touches, Yara sets a whittled figurine of a serpent down on the table , sliding it towards you :)
#badart rambles#my oc#oc#oc:yara#ask!!#lore#/has yet to learn writing Zev as a person with actual social skills#writing Yara is a bit tricky bc I’m a more unfamiliar setting for 21 she’d just point to Zev XD#but in a less formal one it’s more stream of consciousness#but even then if you take away the mumbly bits her speech can be a bit confusing#communicating… is hard#/cries bc tumblr crashed at 31 and erased my answer#thank u so much for the ask!! >:d#congratulations! you acquired Snake! :-)#also v slowly working through some stuff rn so I’ve been slow but… aaaaa?#something is up with my ability to view the posts I’ve saved#;-; I normally archive posts I wanna get back to in my likes as a queue#but now I can’t remove the ones I covered (like art accs I wanna look up)#and I can’t find anything and my order is gone T-T my orderrrrrr#Yara lore
7 notes
·
View notes
Link
Jerry's eccentric neighbor and Seinfeld's moocher, Cosmo Kramer is a well-known character in sitcom history. Widely recognized for his harebrained schemes and physical comedy gags, he stole the show nearly every time he dashed into Jerry's apartment. However looking back, some classic Kramer moments on Seinfeld don't really hold up. In other words, the writers didn't do him justice and could have easily avoided tone-deaf writing in favor of a more coherent character.
RELATED: Seinfeld: 10 Times Kramer Was The Most Hated Character On The Show
Here are ten Cosmo Kramer quotes that are no longer politically correct and therefore seen as unacceptable today.
10 "Well, You're As Pretty As Any Of Them, You Just Need A Nose Job."

Early on in season three, George went out with a woman named Audrey who in the first place was way out of his league. But, because he was overly concerned with looks and had a superficial understanding of beauty, he couldn't get himself to stop thinking about her nose.
Later the same day at Jerry's, Kramer made an off-hand remark about Audrey needing a nose job and sugarcoated it with, "well, I was just trying to help out." Audrey was humiliated, Jerry and George were stunned and Elaine was the only one who rebuked Kramer for his offensive remark. Unsolicited comments of such nature are hurtful, and, no matter what the intention is, they lead to shame and humiliation, like in Audrey's case.
9 "I Mean, What Am I Supposed To Tell Him? How Much There Is For Him To Live For? Why Should I Lie To Him?"

Newman made his first-ever appearance as a voice-over character in the episode "The Revenge." He was unemployed, single, and, from what's seen in the episode, he didn't have a helpful friend, either.
Kramer dashes into Jerry's apartment to tell him he doesn't want anything to do with their Newman anymore because of his attitude. The men discuss their neighbor's misfortunes at length, and yet, none of them take an active interest in him. All warning signs must be taken seriously, and Jerry and Kramer should have proceeded to help Newman to get the assistance he needed.
8 "You're Getting Heavy. Yeah. You Look Like You've Put On 5... 10 Pounds."

All hell breaks loose in season five's episode "The Non-Fat Yogurt" when the gang suspects the new yogurt shop is making misleading claims about the fat content in their yogurt. The troublemaker of the gang, Kramer points out Elaine's weight gain rather insensitively. As Jerry stands up to object, Kramer shows little care for his feelings and adds, "I'll tell you something else. You're looking a little chunky yourself, buddy."
RELATED: Seinfeld: 10 Most Shameless Things Kramer Ever Did
Although Cosmo's observation turns out to be true, making crude remarks about people's weight is never okay and he should have been careful with his words.
7 "She Changed Her Hairstyle. It's Terrible. No, We're Done."

Season six's "The Kiss Hello" is another instance of how superficial Kramer's personality was. As soon as his girlfriend Wendy changed her hairstyle, he ended things with her and never looked back again.
Kramer was a fickle person who was more concerned with the outward appearance of the girls he dated than he should have been. This time around, however, he cranked his superficiality up a notch and ended things because his girlfriend had her hair cut.
6 "You Know... Get Out."
Of all the people in the City, Kramer was the only one the Soup Nazi seemed to respect. Their friendship meant he could drop in any time and keep Yev Kassem entertained with his rambling stories of the day. Kramer praised the Soup Nazi's strict ordering mechanism and helped him bully people who were unaware of the same.
Kramer had no business ordering a part-Spanish man out of the Soup Nazi's restaurant. Instead of standing up for the guy and asking his good friend, Yev to cut him some slack, Kramer ordered him to leave the premises.
5 "I'm Gonna Capture This."

Seinfeld's finale disappointed fans on many accounts, one of which was Kramer filming a carjacking victim in the fictional town of Latham, Massachusetts.
RELATED: Every Seinfeld Finale, Ranked
It was Kramer who had jumped up and down the plane and caused it to crash land in the first place. As the gang made their way into the town to recover from the shock of the crash landing, they witnessed a helpless boy getting mugged at gunpoint. Kramer turned on his camcorder and started to film the robbery. The rest of the gang followed his lead and made cruel jokes about the boy. They were put in jail for violating the Good Samaritan Law, and their trial turned into a media circus.
4 "And You Must... You Look Exactly Like Jerry. You Don't See This? Oh, You're Like Twins. This Is Eerie."

Quite shockingly, this was first thing that came out of Kramer's mouth when he met George's new girlfriend Janet in "The Cartoon." Everyone looked visibly uncomfortable, but, surprisingly, Janet took it all in her stride. While she didn't seem to mind the unpleasant remark, George was visibly upset—but that didn't deter Kramer from suggesting George was secretly in love with Jerry while everyone stared at him in disbelief.
3 "We'll Kidnap The Dog, We'll Drop Him Off Upstate."

In "The Engagement" when a loud Yorkshire Terrier kept her up all night, Kramer, the vile rogue suggested they kidnap it and drop it off upstate. He enlisted Newman's help, and together they rode in a rental car to commit the crime.
After driving for a while, Kramer abandoned the dog in Monticello at a stranger's doorstep. But, before he walked off, the dog tore a tag off his shirt. It found its way back to the owner, and the three dognappers were traced in no time. However loud this dog may have been, dognapping is not only inexcusable but a felony as well.
2 "You Know How There's Some People You Worry About Whether You're Going To Hurt Their Feelings? With Her, I'm Looking Forward To It. I'd Like To Get It On Video, Watch It In Slow Motion And Freeze Frame It."

...says Kramer in season three's "The Dog" while badmouthing his girlfriend, Ellen to Jerry and Elaine. She wasn't made out to be a nice person, but since when did it become okay to trash-talk a partner much less make a big speech about looking forward to inflicting pain on them?
Kramer's backbiting encouraged Elaine and Jerry to name-call Ellen as well. Confiding relationship problems in friends is one thing, but making a boastful remark about hurting one's partner is quite another.
1 "Hey! Stay Away From The Chicken. Bad Chicken. Mess You Up."

Season eight's "The Chicken Roaster" is a prime example of Kramer's uncivilized behavior. In the episode, Kenny Rogers Roasters sets up a chicken place right across the street from Kramer's place. A menacing red light comes off of its chicken sign, beams straight through Kramer's window and his apartment becomes a "red planet" of a hot mess.
Now, Kramer does go down to the restaurant to complain, but, after they dismiss him, he schemes to put the place out of business by "takin' it to the streets." He hangs a bad chicken banner from his window and drives the customers away. Come to think of it, there were plenty of civilized ways to resolve the conflict, and it was uncouth on Kramer's part to yell out his window and scare people like that.
NEXT: Seinfeld: 10 Ways Kramer Got Worse & Worse
Seinfeld: Ten Kramer Quotes That Haven't Aged Well | ScreenRant from https://ift.tt/2RBPqUN
0 notes
Text
Kelsi Likes Seinfeld
Go to the bottom of this post to see all of my Seinfeld recommendations including books, merch, articles, and more!
There was an echo issue with my audio in the segments while I am on camera. I am working to fix the issue if there is any way to, but until then here is the video if anyone still wants to see it:
youtube
Recently, I decided to start a weekly show called “Kelsi Likes.” The title is an anagram! Each episode is about a different topic with only one thing in common…that I LIKE it!
I’ll be doing episodes on wrestling, cartoons, my favorite movies, horror, my love of Halloween, tv shows, characters, my love for the 90s and so much more!
But this episode is about one of the most iconic television shows of the 90s...
Seinfeld, “the show about nothing,” that was actually about everything and anything!

Even if Seinfeld wasn’t your favorite show in the nineties or if you never cared to watch it at all, no one can deny that it has had a huge impact on the current social and television landscape. Seinfeld played a huge role in television history, in academic television analysis and in society itself by becoming a massively influential, cultural phenomenon.

In college, I wrote a paper titled “The Evolution of the Television Industry in the 1990s.” Seinfeld was one of the specific shows I analyzed and wrote about to prove my thesis: “television of the nineties was revolutionary and stands out from previous decades.”
Here are a few excerpts from the paper:
Hailed as “the best sitcom of all time” is NBC’s Seinfeld, which first aired in 1989 and ended in 1998. The show follows Jerry, Elaine, George and Kramer as they go through everyday life making fun of and analyzing everything and anything. Famously described as “a show about nothing,” Seinfeld’s striking appeal is the wonderful comedy writing and revolutionary idea of having a show that revolves around quirky, but regular, people and their daily encounters. TV Guide describes the show this way:
As put forth by the series itself, Seinfeld was a comedy about nothing.But in reality it was about the very worthy subject of modern manners-waiting interminably for a table at a Chinese restaurant, for instance...and it addressed these issues with all the acute observation and satirical brilliance of a Restoration comedy. It’s just that the manners of Jerry, George, Elaine and Kramer were often atrocious. (Lasswell, 235)
Nothing overly monumental happens to the main characters, but it’s the writing, the acting, and the premise of “nothing” that made this sitcom stand out above all others. It’s original. Even today, over twenty years after the show has ended, it’s still widely considered “the best” sitcom of all time.
This show can be said to have single handedly defined nineties television and the uniqueness of the era. Entertainment Weekly describes Seinfeld as
...that brilliantly self-reflective series about a stand-up comic and his three pals, [and it] went on to become the defining sitcom for the ‘90s. In its eight years on the air, Seinfeld changed the tone of TV, our Thursday-night plants, the way we talk. It spawned enough imitators to fill Yankee Stadium, boosted sales of Jujyfruits and Binaca, and even made medical history--a journal reported that a Massachusetts fan laughed so hard, he kept fainting. It made a mint for NBC--and not a junior one either. (Gwinn, 11)
Always challenging TV “Political Correctness,” Seinfeld addressed countless topics that had never been discussed on television before.
Over the years, the quartet broke tube taboo after taboo, mocking deaf people, cancer, football-shaped goiters, and mental retardation. Even masturbation and oral sex slipped onto the airwaves, thinly disguised with masterful euphemisms. Not exactly safe, family, Tony Danza-type television. But it was precisely Seinfeld’s shocking deviations from formula that separated it from the sea of tapioca. The show gave us a peek at our Jungian dark shadow. It let nothing--not feelings, not death--get in the way of a punchline. (Gwinn, 11)
Overall, Seinfeld was a step in the opposite direction of the regular family-friendly sitcoms such as The Cosby Show and Happy Days that had aired in previous decades. This, however, is exactly why Seinfeld was able to flourish and succeed. In effect, the 90s television audience was left with a new type of comedy that has not since, one could argue, been matched in quality and content.

I also asked some friends and family what Seinfeld meant to them.

My friend Trace (who has a UCF podcast: @UCF_Knightline) described Seinfeld like this:
Well written and witty, the scenarios the characters found themselves in were absurd, yet relatable. Who hasn't lost their car in a parking garage or struggled with someone who is a close talker? The terms seeped into our public consciousness and decades after its debut, the show is still as relevant as ever.
When I discovered Jerry Seinfeld, simply put, his poke at little things made me laugh. My enjoyment of his comedy made me want to check out his new show. Seinfeld's core characters weren't written to be like-able, yet proved to be enduring and, ironically, quite like-able.
My 14- and 15-year old nephews have only recently discovered Seinfeld through syndication and laugh out loud as I did when I first watched the episodes during their original run and dozens of times since.
It was billed as a show about nothing, yet became a show about anything and everything and remains my favorite show of all-time. No matter when I tune in, be it a few minutes in or only with a few minutes left, I watch and laugh and yell out the lines and ... yada, yada, yada all over again!
My co-host of my wrestling podcast, Paul, gave me a list of his favorite Seinfeld episodes!

My dad, Donald, also gave me a list of his favorite episodes and had this to say about the show:
Favorite Episodes for the Show’s Lead Characters:
Jerry (Possibly the most innately funny lead of a sitcom of all time) = With 180 shows to choose from? Maybe The Puffy Shirt, Season 5.
George = A three-way tie between The Marine Biologist, The Opposite, and the “I was in the pool!” Hamptons episode, all Season 5.
Elaine = The Bizzaro Jerry and The Little Kicks, both Season 8.
Kramer = Any and all of his appearances since the Seinfeld pilot (there were only two episodes in which he didn’t turn up: The Chinese Restaurant and The Pen). If I had to choose one favorite, it would probably be The Merv Griffin Show (Season 9); Also love any of the episodes that feature a Kramerica Industries venture, i.e., the NYU intern assisted oil bladder system (The Voice, Season 9), and his other various “Eureka!” ideas like Make Your Own Pie pizza restaurant or his PB&Js sandwich shop, the Coffee Table Book about coffee tables, The Beach cologne, ketchup and mustard in the same bottle, and the aforementioned male brassiere twist. Should I also include the co-created homeless person powered Rickshaw endeavor, Jerry’s imagining of a future Kramer’s car periscope invention, and possibly the roll-out tie dispenser? Cosmo’s umbrella corporation far outdistances George’s more pedestrian and fictional Vandelay Industries that was made up for extending Costanza’s unemployment benefits as a would be latex salesman.
Hardly a day goes by in my life that doesn’t include an occurrence or interaction within it that I can someway, somehow relate to a Seinfeld episode. Guess that does it for now, gotta go watch some Seinfeld reruns. It NEVER gets old, kinda like watching the movie “Jaws”. So Kelsi Likes, “you’re going to need a bigger list.” LOL
Lots of people on Twitter also weighed in and tweeted about their favorite episodes:









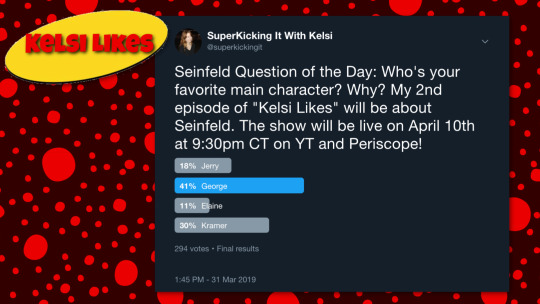
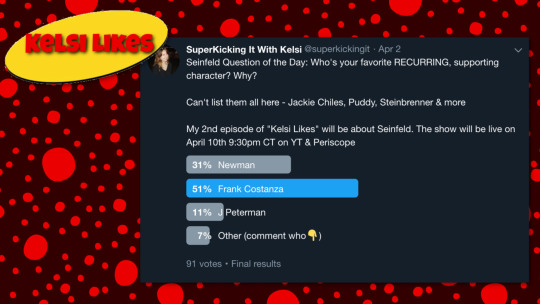
I also put out a number of Seinfeld-related polls on Twitter:
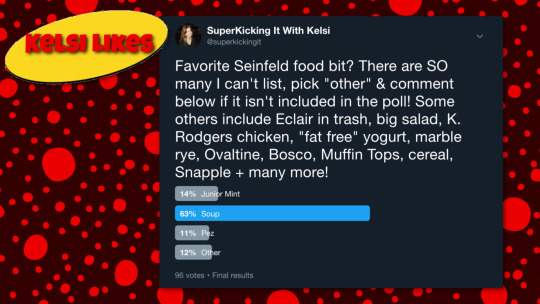

The last poll shown above references Seinfeld food bits, and there is actually a massive amount of food references throughout the entire run of the show! I found this fun article/list that compiles all the references and includes episode numbers and descriptions: Complete Food Tour of Seinfeld by Moze Halperin and Jillian Mapes from flavorwire.com

“Kelsi’s Kountdown” - My Favorite Seinfeld Quotes
The sea was angry that day my friends…
HELLO NEWMAN
SERENITY NOW!
These Pretzels are Making Me Thirsty
No Soup for You

Honorable Mentions:
GET OUT
Just pop the top, and toss the stump
TURN PIMP…I’M NOT A PIMP!
Jambalaya
You son of a bitch bastards
Schmoopy! No you’re schmoopy!
Yada yada yada
CABLE BOY…What have you done to my little cable boy?
I was in the pool.
Oh, No, I'm so sorry. It's the MOOPS. The correct answer is The MOOPS.
Here’s to feeling good all the time!
Believe or not answering machine message
You’re living in the past, man. You’re hung up on some clown from the 60s, man!
Well HELLLOOOO
Just Take One Dip and END IT!
Shut up ya old bag
You’re an anti-dentite!
If this wasn’t my son’s wedding day, I’d knock your teeth out you anti-dentite bastard

In the video at the top of the blog post I also talk about my most underrated Seinfeld episode list as well as my favorite Newman episodes.
“Kelsi’s Kountdown” - My Favorite Seinfeld Episodes:
The Chicken Roaster (1996 – Season 8)
The Bris (1993 – Season 5)
The Soup Nazi (1995 – Season 7)
The Little Kicks (1996- Season 8)
The Rye (1996 – Season 7)

In the video, I also recommended a number of books, articles, and Seinfeld-themed merchandise.
Here is what I recommended (including links!):
The book “Seinfeldia”: A very comprehensive look at behind-the-scenes facts and information about the show. You can buy it anywhere, including Amazon.
The Complete Series on DVD: Includes AMAZING, in depth bonus features, including interviews with the cast and creators, that will keep you entertained for hours.
Factinate Article: Includes a lot of very interesting facts and tidbits about the show
The book “Seinfeld Trivia”: Available anywhere, including Amazon
A Rolling Stone Article: Lists and describes the 100 Best Seinfeld characters

TwentyTwoWords.com Article: A visually appealing article that lists the best quotes and includes stills from the show.

Festivus! The Book: About the Festivus holiday tradition referenced on the show.
Seinfeld Funko Vinyl Idolz: Awesome figurines that can be displayed. I own all of the figures seen in the picture below except for Puddy.

ScreenRant Article: Written by Sean Harrigan this lists the best 15 Minor Seinfeld Characters

0 notes
Text
The Least Likely Style Influencer Of The Year Is The DILF
https://fashion-trendin.com/the-least-likely-style-influencer-of-the-year-is-the-dilf/
The Least Likely Style Influencer Of The Year Is The DILF
As you’ve probably heard by now, your old man is trending hard this year. Ever since Balenciaga sent real dads with their real kids down the catwalk, there has been a new and unexpected fashion tribe, the DILF.
For those who thought the acronym had another meaning, allow us to correct you. DILF – as far as we’re concerned – stands for ‘Dads In Latest Fashions’. Okay, you might quibble on the term ‘latest’. The fashions we’re talking about are synonymous with styles now a quarter of a century old: relaxed, stonewash denim, sensible jackets, dad caps and more. Which raises a question:
How have fathers, once synonymous with lame fits and sadsack style, become fashionable?
Some commentators have suggested that the DILF look came about from cash-strapped millennials hankering after the stability embodied by the suburban dads of their childhood, with their big houses, sensible cars and retirement savings. What once was boring has become aspirational.
That may be true, but there are other, more prosaic reasons. “Fashion is cyclical,” says Jess Punter, a menswear stylist and writer. “The shapes and styles that the dad trend has resurrected are from the early nineties. It’s also comfortable and practical.”
Dads dress for function, not form; the outdoorsy brands they favour, such as Patagonia and the North Face, tend to be eco-conscious, thereby bestowing wokeness on their wearers. (Patagonia sued the Trump administration for shrinking US national parks.)
Then there’s the simple fact that a DILF’s uncoolness is precisely what makes it cool. If everybody was rocking it then it wouldn’t be a swerve. “It’s pointing the finger at fashion, which has created this anti-fashion phenomenon,” says James Lawrence, head of menswear design at ASOS. “It’s fun and shouldn’t be taken too seriously.”
Finally, the DILF look is chaotically, eye-catchingly eclectic. “It’s created a great way of clashing different styles from different genres together and making them all work,” continues Lawrence. Because if there’s one thing dads don’t have time to think about, it’s putting together coherent outfits. Forget Steve McQueen: it’s dads who have truly effortless style.
Key Pieces From The DILF Trend
Dad Cap
The origins of the dad trend can be traced back a couple of years to the sudden ubiquity of the kind of simple cotton-twill baseball caps that are sported on peewee game touchlines everywhere.
Cheap and logo-friendly, they’ve long been a streetwear mainstay, but became an unlikely fashion must-have when Balenciaga created its own version, embroidered with the house’s name, that retailed for $285. Peak dad style.
Dad Jeans
Loose, pleated trousers are a viable legwear option for giving off dad vibes, but high-waisted, straight-legged jeans are the definitive, combining the robustness of denim with the roominess of joggers (plus the ability to bend over and squat down – crucial with kids).
Look no further than original Levi’s 501s: regular jeans for a regular guy. And none of your raw indigo denim here: if they’re not stonewash then they won’t wash.
Chunky Trainers
“The chunky trainer is definitely the footwear big deal of the season and epitomises ‘dad style’ for its ugliness, and how it’s worn with everything,” says ASOS’ Lawrence.
Again, the likes of Balenciaga have their coveted high-fashion takes, such as the Triple S (which presumably stands for “Sell like Shit off a Shovel”). But for a more authentically dad option that won’t set you back a cool $800, cop something like a New Balance 990.
Technical Jacket
“An oversized tech jacket is also key as it adds an element of ‘trainspotter’ to the anti-fashion look,” continues Lawrence. “Wear it over everything from tailoring to sportswear, just like your dad’s favourite jacket.”
The North Face, maker of the on-point Nuptse, is a frequent collaborator with Supreme. Meanwhile Helly Hansen is coming back, which will make anyone who can remember it from the first time around feel old.
Half-Zip Fleece
It’s a toss-up between this and the mock turtleneck. But few pieces or fabrics are as DILF-friendly as a half-zip fleece. Because of that, it has languished unloved on the racks at hiking stores, which is a shame: it’s warm but not bulky, making it ideal for layering under your technical jacket and doubling as outerwear (albeit not waterproof) for those awkward in-between days. This is one time when getting fleeced is a good thing.
How To Dress Like A DILF
Look To Jerry And The Tastemakers
“Watch reruns of Seinfeld for style inspo,” suggests Punter. (It’s on Amazon Prime.) With his baggy blazers, blousy shirts tucked into stonewashed jeans and chunky Nikes, the eponymous stand-up in his nineties prime could have stepped off the Balenciaga runway – all he needs is a kid.
Don’t sleep on the surprisingly steezy George Costanza or indeed Cosmo Kramer, who has a nice line in floral Cuban collar shirts.
Jerry Seinfeld
Weigh Up The Situation
If you’ve succumbed to middle-age spread or sympathy baby weight then trying to jump on the Balenciaga bandwagon will do you a fat lot of good. “Like all fashion trends, dad style looks best on lean male models,” says Punter. And svelte, selectively casted fathers in fashion shows.
“Sadly you won’t pull it off if you have a dadbod – man boobs and paunches are too real.” Maybe try and fit in a few pull-ups next time you go to the playground.
Don’t Kid Yourself
This brings us to the salient point: the DILF look as modelled on the catwalk is not actually for dads at all. “It’s about ‘elevated’ pieces from labels like Balenciaga that score fashion points, not something that can be picked up in a supermarket,” continues Punter. “If you are an actual dad, I also recommend not spending £700 on a pair of trainers – you have mouths to feed.” ASOS’ Lawrence echoes as much: “Don’t do it if you are a dad.”
What If You’re Not A DILF, Just A Dad?
So what do you do if you are not a fashion-conscious young scenester and just a dad trying to stay stylish? Some recommendations:
A bit of extra room in the thigh is entirely welcome, but denim should taper down to your ankles and hug your hips, not your belly button. Leave the dad jeans to childless Gen Z-ers (who basically are children).
A technical jacket is a watertight outerwear choice, but take a rain check on anything with big logos, bright or oversized. You’re too old to be ‘playing with silhouette’, or indeed anything except your kids.
Sidestep ‘ironic’ chunky trainers in favour of sleeker classics (Stan Smiths, Converse, Vans) or modern, Flyknit-type styles: in short, the middle of the spectrum between ‘sneakerhead’ and ‘Obama’s Asics’.
Excepting obvious fails, what divides good dad style from bad is often effort, or lack thereof. Stay in good shape, get a regular haircut, clean and press your clothes. You want to look crisp, not be covered in bits of one.
0 notes
Photo

Marvel Age Vol. 1 No. 124 (May 1993)
Crossovers!
In other entertainment media, this refers to bringing an audience that likes one genre (like country-western music) to another, hybrid genre (country-western-rock) usually through the strength of a given performer's performance. This broadens their base of appeal, giving the artist a more mainstream audience. Hip-hoppers dream of crossing over and attracting a pop audience. Action stars like Jean-Claude Van Damme dream of crossing over and attracting more women to his pictures. In comics, the term has a different meaning. Crossovers are done within the same genre, and the one doing the crossing over is not the artist or the work, but the characters in the story.
Imagine Clive Barker characters making guest appearances in Stephen King's books. Imagine the kid from Home Alone meeting Problem Child. We occasionally see some of this. Seinfeld's Kramer did a guest shot as Kramer on Mad About You earlier this TV season. On the rarest occasions you'll even get genre-crossovers on TV, the classic example being when a few doctors from the dramatic series St. Elsewhere showed up on Cheers.
But when it comes to character crossovers, the comics medium in the champion, Marvel is the champion's champion, and there's no end in sight as long as you readers demand we keep doing them. Make no mistake, the vast majority of you do demand them, and they still do their magic, attracting readers to try a certain title they ordinarily would not buy. And crossovers can still be a lot of fun for us creative-types, too.
Industry jargon time. There are two different types of crossovers. A closed crossover is conceived of as involving specific titles where each title is equally important in advancing the storyline. Recent examples are "Operation: Galactic Storm," in seven different AVENGERS titles; "Dead Man's Hand" in NOMAD, DAREDEVIL and PUNISHER; and "X-Cutioner's Song" in the core X-titles. An open crossover is one which has a basic storyline told in one major series, but its ramifications and complications can play out in any title that chooses to get involved. Recent examples include the INFINITY trilogy (GAUNTLET, WAR, and CRUSADE); "Inferno" in X-MEN and "Acts of Vengeance" in AVENGERS.
The merits and demerits of the two types of crossovers? Open crossovers are more difficult to coordinate, due to the greater number of titles usually involved. On the other hand, they are more creator-friendly: no one is barred from participating ("Sorry, fella, this crossover is closed."). Open crossovers also enable the readers to pick and choose which tie-in issues of which they wish to partake. They pick up the key elements of the story by reading the keystone series, and the rest is just gravy.
Tom DeFalco has a theory that every other open crossover has lots of participants. Writers and artists get involved one year, discover all of the coordination headaches involved, vow to never do it again, and so pass up the chance to participate the next year. Months later, they get their sales incentive checks, realize the benefits and, forgetting the aggravation, agree to participate in the next one, having missed the intervening event. So it goes, year after year, according to the Chief.
The merits and demerits of a closed crossover? Each part of a closed crossover is essential, so to buy one is to commit to buying them all, or else the storyline is not going to be intelligible. They're creator-unfriendly, not allowing others to jump in if they have an inclination. Taken as a whole, they are probably more coherant, since more centralized scrutiny is given to every integral part. Participation in a closed crossover is probably a better sales boost for a title, since every part of a closed crossover is equally important to the advancement of the storyline.
In a crossover, there's usually one editor who's in charge of the whole magilla, and that's the person who's the regular editor of the main title character around whom the crossover revolves. The editor in charge, of course, has a supervisor (one of the executive editors) to look over everything in an advisory capacity, but the editor in charge has to do all the hands-on work: distributing the rough outline to everyone involved, answering continuity questions, and reviewing all the tie-in plots to make sure they conform to the details of the overall storyline.
Sound complicated? I'm not done yet. All the participating editors of the crossover must also submit their book's plots to the other participating editors if there's so much as a cameo of a given editor's character in their story. And once the art is done, photocopies of the artboards must also be distributed to fellow editors in the crossover so they can make certain that costume details and so forth are consistent. We're talking major league coordination here, folks, and it's never any wonder to me that try as hard as we might, there is always a detail that is a little off in one title or another.
I've initiated major storylines in closed crossovers. I've participated in open crossovers whose premises I had nothing to do with. I've read and supervised crossovers for which I had no input or participation. Let me bend your attention span a bit with some of my specific experiences.
"Operation: Galactic Storm" was based on a plot germ growing out of my QUASAR continuity. Quaze is supposed to be the Protector of the Universe. What would happen, thought I, if some aliens wanted to enlist his aid in a war with some other aliens? How would he decide which side to assist? Would he try to prevent the whole thing from happening, or would he turn his back on the whole murky affair? Well, when Bob Harras, Fabian Nicieza, and I were casting around for premises big enough to involve all the AVENGERS titles, I offered my QUASAR idea. Obviously, if the war infringed upon Earth in some way it could be "opened up" beyond the QUASAR title. Bob, Fabe, and I then thrashed out a raw outline of key events in each of the nineteen (ulp!) chapters that comprised the crossover. This took a lot of lunches.
Then we held an AVENGERS summit meeting with all the writers and editors, in order to debug and flesh out the outline. The writers were required to cover the events that were slotted for their issues of the storyline, like it or not. In most cases, there was plenty of room for the individual writers to make their portions uniquely their own, but it was still a far greater imposition upon their titles than usual. The net result, in my opinion, was pretty successful.
Last year I also participated in the open crossover INFINITY WAR. I had nothing to do with the basic premise-- the extent of my influence on the core storyline was "Since this story's so darn cosmic, and Quasar has a unique role in the cosmos, make sure he's got something special to do, please." And so he did. Writer Jim Starlin had the mad Titanian Thanos choose Quasar, of all the assembled multitude, to wield the Ultimate Nullifier. Unique enough for me. And when I wrote my tie-ins, I was obliged to deal with events in the limited series. In one issue, Quasar's role was to "find Eternity." I relished this, since I have long been interested in exploring the means by which omnipotent abstract entities acquire humanoid forms. I used my assignment to do a real offbeat story. I was happy.
For my second crossover issue, I was a little more hamstrung. My issue came between two issues of WAR and, at the beginning of the second issue, Quas was in exactly the same predicament he was in at the end of the first. I had an issue of QUASAR where he couldn't do anything! I managed to get around this as best I could by having Q go on a fact-finding quest that no one knew he went on. Whew. Then for my third crossover issue, Quas got nullified in WAR and never came back in the course of the story(!). Obviously, I had to tell what happened to him after he got nullified, and bring him back to life. This challenge was compounded by the fact that, in his own series, Quasar had already spent a few recent issues being "dead," so it was incumbent upon me to make this new experience as different from the previous one as possible. Truth to tell, I would never have chosen to do another "after death" storyline in the course of the book if I hadn't been obliged to. I now find that having had a character come back from the dead twice makes the threat of corporeal harm pretty empty.
So that's my side of the story on the subject of crossovers. They sometimes seem like a necessary evil, and sometimes like an unnecessary good! I would be interested to hear from you what you think our best and worst coordinated mass crossovers have been (I have my own theories). But as long as the idea of crossing over from one title to another remains a way to boost interest among you readers, we're going to keep doing it. And hey, maybe one time we'll get it absolutely right.
Source: Internet Archive
(image via Trusty Plinko Stick)
0 notes
Text
Fixing the 5 Percent
An oversized poster of the Seinfeld character Kramer watches over Phil Rizzuto’s daily routine. When Rizzuto, named for the famous New York Yankees shortstop, swallows his 6 a.m. pills, Kramer is looming over him, looking quizzical. Same for the 9 a.m., noon, 6 p.m., and midnight doses, each fistful of pills placed in a carefully labeled Dixie cup. “I live on medication,” he says.
Listen to the audio version of this article:
Download the Audm app for your iPhone to listen to more titles.
Rizzuto’s daily life in Haverhill, Massachusetts, is a litany of challenges: His aides have to hoist his paralyzed legs from his bed to his motorized wheelchair and back again; keep the bag that collects his urine clean; tend to the gaping wound on his backside, which developed when he was left to lie still in bed too long; and help him avoid the panic that could claim anyone in his situation—that last one is particularly difficult since Rizzuto’s obsessive-compulsive disorder drives him to want to do everything for himself.
After more than a year of emergency and rehabilitative care following a devastating car accident, Rizzuto moved into a YMCA-run housing complex in this gritty New England town. But he still endured constant medical emergencies. “I was back and forth and in and out of the hospitals so much, it was like I didn’t know I had an apartment here,” the 56-year-old says, sitting in his small studio. His open wound kept getting infected; his diaphragm, weakened by his injury and his inability to quit smoking, left him gasping for breath; his urine-collection bag slipped out; his demons kept getting the better of him. The government eventually covered the cost of his care, but the relentless need for medical attention was exhausting and demeaning.
Then he opted into a Massachusetts health-care program called One Care that focuses on people with complex medical needs who are on Medicare. One Care provides 71 hours of aide support a week, a twice-weekly visit from a massage therapist, twice-monthly psychiatric care, a wheelchair support group, and a nurse practitioner who oversees and coordinates Rizzuto’s care. If he struggles between visits—or just wants to talk—she’s available by phone, even on weekends and after hours. Now, his life has a routine and a discipline that keeps emergencies at bay. “The difference it’s made …” he says, unable to fully express his gratitude. He estimates his hospital visits have dropped at least 75 percent since the One Care program took charge of his health. “I would hate like hell to not have them.”
The program that has helped Rizzuto is part of a nationwide movement to improve care for people struggling with very complicated medical needs—so-called super-users—the 5 percent of patients who account for about half of the country’s health-care spending. (Surgeon and New Yorker writer Atul Gawande outlined the problem and one solution in a definitive 2011 piece about the Camden Coalition of Healthcare Providers.) Some of these super-user programs say they provide cost savings of as much as 20 to 40 percent after a few years, as well as provide the kind of advantages offered to Rizzuto: fewer stressful hospital visits, better mental and physical health, and the satisfaction of being treated like a person instead of a package of problems. The program accomplishes this by shifting the focus of medical care. Instead of responding to complications, the care team tries to prevent them. “You can’t even get to the medical issue until you’ve figured out: Do they have a place to sleep, do they have housing they’re not going to lose, do they have food in their refrigerator, do they have a refrigerator?” says Christopher Palmieri, the president and CEO of the nonprofit Commonwealth Care Alliance, which manages 80 percent of One Care patients.
Despite its successes, this care movement, which doesn’t go by any catchy name—one doctor gave it the clunky title “high-impact, relationship-based primary care”—is scattered among a handful of states and is advancing only very slowly across the country. There is general agreement that these programs must address a range of social and pragmatic needs, like transportation, housing, nutrition, isolation, emotional well-being, and medical problems. But the details of each program are different. “Everyone’s trying their home brew,” says Dr. Harlan Krumholz, a cardiologist and health-care researcher at Yale University and Yale-New Haven Hospital.
The one thing all of the super-user care programs have in common is a mantra that could have come from Cosmo Kramer himself: Stay the hell out of the hospital. Hospitals, these folks argue, often make sick people sicker. They’re sources of infection to vulnerable patients. They’re disorienting. They run costly tests and look for issues that are better left alone. Super-users, says Krumholz, “represent a failure of the system.”
Medical care is dangerous,” says Dr. Rushika Fernandopulle, the co-founder and CEO of Iora Health, a leading practitioner of a more holistic approach to health. Fernandopulle says a big part of his company’s business model involves fighting to keep people out of the hospital—not just because it’s expensive, but because the care they will get puts them at higher risk for other problems. Medicare patients saw roughly a 40 percent drop in hospitalizations after Iora took over their care, Fernandopulle says.
For Fernandopulle, one patient in particular illustrates this phenomenon of snowballing medical care. That patient was an 80-year-old woman, fairly healthy but with hypertension and arthritis, who one day saw red in the toilet after urinating. She told her primary-care doctor, who sent her to a urologist; the urologist worried it might be cancer and ordered a catheter inserted. Before the procedure, a nurse asked the octogenarian if she ever felt weak or dizzy. (Of course she did—think about it.) When the woman said yes, a heart monitor was ordered: It showed a dip in her overnight heart rate. A cardiologist then scheduled the woman for a pacemaker.
“This is what I mean by the vortex,” Fernandopulle says, noting that inserting a pacemaker would be risky and provide no clear benefit. The woman’s condition might be explained in a much more low-tech way: a beet salad, for example, could be the culprit behind the red pee, and a prescribed medication might trigger the heart irregularity. “I called the cardiologist and politely declined the pacemaker for this patient,” Fernandopulle says. Part of the problem is that, while each doctor gets paid for each procedure he or she performs, usually no one gets paid for taking a step back and using common sense to think about what would genuinely help the patient.
“The health-care system as a whole is out of balance,” says Dr. Donald Berwick, the former head of the Centers for Medicare and Medicaid Services under President Obama. “We put far more into hospital care than we do keeping people from having to be in the hospital.” Hospital stays cost more than anything else in the health-care system; an average inpatient admission runs nearly $2,000 a day, and an intensive-care stay can easily cost $7,000 a day. In 2012, a typical hospital stay topped $10,000, according to the federal Agency for Healthcare Research and Quality. Caring for an Iora patient, on the other hand, typically costs about $3 a day and can reduce hospitalizations by 40 to 50 percent, Fernandopulle says. All of the physicians and advocates we interviewed who support this type of high-needs care are quick to note that their goal isn’t to deprive people of medical care. If someone doesn’t get needed heart surgery, they will end up in worse shape; no one will benefit. Their aim is appropriate, Goldilocks care: not too much, not too little.
Cory Sevin, a senior director with the Institute for Healthcare Improvement, a policy center in Cambridge, Massachusetts, says providing more appropriate treatment is also better for the caregiver. Kim Tremblay, a nurse practitioner with the Commonwealth Care Alliance, says that while the work is intense, she has enjoyed managing Rizzuto’s health team for three years and watching him slowly improve. “We give a lot to these patients,” she says. “We get a lot back.”
The model hinges on establishing strong, trusting relationships—but that doesn’t always come easily. “Some patients jump on board; sometimes it takes six months to establish a connection,” Tremblay says, recalling one patient who refused to talk to her for nearly five months before finally accepting help. She has become profoundly invested in her patients’ care. “Every time we send someone to the hospital, it’s stressful,” for both the patients and caregivers, Tremblay says. “We send someone in [and] we kind of shudder, Are they going to come out better?”
One big challenge to providing care for patients with complex needs is finding them. Commonwealth Care, for instance, has struggled to identify people who will benefit from its program. Any Massachusetts resident who receives both Medicare and Medicaid is eligible to join One Care. Commonwealth Care Alliance, which serves most of these patients, had to hire extra staff to track down potential clients. When Commonwealth Care started four years ago, 43 percent of these potential clients were considered “unreachable,” for reasons like having an unknown address. Today, that rate has shrunk to 32 percent.
Why is it so hard to track down needy patients? Some people are so isolated and disengaged that they’re largely invisible. Others patients are expensive and challenging today but might soon recover. And still others are doing fine now but might have a setback that throws them off balance for months. In fact, 60 to 80 percent of patients who are super-users now won’t be a year from now, Sevin says, and different people will be.
There are also people who will be perennially expensive—because their disease requires a costly drug, for instance. And there are those who will be expensive for a short time—say, for the few months after an organ transplant. There’s no point in wasting time trying to bring either group’s medical expenses down.
Fernandopulle says the only effective way to identify people at risk for super use is to ask them two questions: “How do you think your health is?” and “How confident are you in managing your health?”
“If they answer, ��Poor, poor,’ they are at huge risk,” he says.
On a recent sweltering day, Rizzuto met his wheelchair support group at a small zoo in suburban Boston. Keeping cool in the above-90-degree heat wasn’t easy for Rizzuto. Paralysis robs people of their ability to regulate body temperature. One of Rizzuto’s aides, Bill Regan, came prepared with water, ice packs, sandwiches, and a spray bottle that he frequently spritzed on Rizzuto’s face and legs.
Rizzuto says these interactions with other people in wheelchairs help lift his mood, though on this trip he seemed more focused on watching a brown bear, several snakes, and tiny, hyperactive cotton-topped tamarins. He never could have made it around the zoo without a motorized wheelchair—though it took Rizzuto a year to convince the state to buy it for him. One of the first things One Care does when signing on a new client is to assess the person’s equipment needs, Tremblay says.
One Care is a partnership between Massachusetts’s Medicaid agency and the federal Centers for Medicare and Medicaid, and it focuses solely on patients ages 21 to 64 with multiple, complex medical and behavioral issues. (An older program, Senior Care Options, takes the same approach for patients over 65.) Most of Commonwealth Care’s 13,500 One Care clients earn less than $20,000 a year; some are homeless; the majority of them have a serious mental illness or substance-use disorder, as well as multiple other chronic health conditions.
This high-touch care approach is beginning to save money, says Palmieri. A report last year by the Commonwealth Fund found that among 4,500 members of One Care, patients enrolled for 12 continuous months had 7.5 percent fewer hospital admissions and 6.4 percent fewer emergency-room visits. For those enrolled in the program for at least 18 months, hospital admissions dropped 20 percent, the study found.
Although each model of high-touch care is different, the basics are the same: focusing on prevention, ensuring basic needs are met, reducing unnecessary treatment, and building relationships with patients. At Stanford University, for example, one young man with severe anxiety and obsessive-compulsive disorder required constant reassurance (in addition to his multiple medications) from doctors and emergency departments. In a traditional care system, emergency-room staff might roll their eyes and quickly send him on his way. Instead, Dr. Alan Glaseroff, the co-founder of Stanford’s Coordinated Care program to treat high-needs university employees and their family members, gave the 19-year-old his phone number. At first, whenever his anxiety or OCD took control, the young man called Glaseroff or another care coordinator as many as seven times a day.
But slowly, over the course of three years, the man learned to think before he called. If he saw spots in his eyes, he’d wait for a few minutes to see if they went away. He was taught to use mindfulness techniques, and if the symptom persisted, he would run through a checklist to see if it was really something to be concerned about. He ended up calling the clinic every two to three weeks, rather than multiple times a day, and learned not to lean on the clinic’s staff for minor issues. “Now, he hardly needs us,” Glaseroff says.
Creating viable long-term plans like this means far fewer emergencies. In fact, in its first three years, the Stanford program cut emergency-room visits for its 253 patients by 59 percent, hospital admissions by 29 percent, and total cost per patient by 13 percent, says Glaseroff, who teaches this model of care in two-day workshops across the country. According to the study, the Stanford practice saved the university $1.8 million and now has nearly twice as many patients.
The secret to the cost-savings, Glaseroff says, is for patients to use hospitals and doctors only when absolutely necessary and to rely for most of their care on empathetic—and relatively inexpensive—medical assistants, who check in with each patient about once a week. In the past four years, in an industry known for its high burnout and turnover, not one of his practice’s care coordinators has left, Glaseroff says. “They’re not allowed to diagnose and treat, but they’re really good at the people stuff,” he says. “The core is being given responsibility for people, not for tasks.”
Patients in the program have responsibilities as well as rights, Glaseroff says. They are expected to show up for their medical appointments and to come on time out of fairness to others. They’re told to call the clinic if they can before heading to the emergency room and then wait a few minutes for a call back, Glaseroff says. They are expected to do their part to engage with their care coordinator, even if the medical system hasn’t always treated them well in the past. “It’s patient self-management—what people do within their chronic illness 365 days a year—that matters the most,” he says.
For the high-touch model to work financially, large numbers of patients have to stick around long enough to recoup the upfront investment in their care. Today, there are only a few pools of people stable enough to sustain this model: people who work for major employers, like Stanford University, and those insured by the federal government.
Iora provides health care to workers at large, stable employers like the Dartmouth College Employees, the New England Carpenters Benefits Fund, a union trust, and members of Medicaid Advantage plans, like Humana and Tufts Health Plan. This gives them a big group of customers with high needs and the corporate muscle to avoid being pushed around by hospitals that don’t want to lose patients, Fernandopulle says.
If he loses customers to other insurance carriers in the first year or two, he’ll have all the upfront costs and none of the savings. A five-year time horizon allows Iora to recoup its upfront investment and get ahead of problems—controlling diabetes before it leads to a heart attack, for instance, says Fernandopulle, whose company oversees care for about 20,000 patients in eight states.
Iora and another company with a similar approach, Landmark Health, also provide care to people on Medicare Advantage—a government-funded, privately run program. About a third of people on Medicare now belong to Medicare Advantage programs, which were created by the Affordable Care Act. The Trump administration and Republicans have proposed huge cuts to Medicaid over the next decade. It’s unclear, however, whether such cuts would paralyze efforts at innovation or provide more urgency to reduce health-care spending. “It is a bipartisan issue that the current costs of health care are unsustainable,” Yale’s Krumholz says, “whether driven by empathy for those who are disadvantaged and suffering or by economic imperative.”
But there are also built-in disincentives to this kind of high-touch care. One of the most obvious is that hospitals make money on patients. If they succeed in decreasing readmissions, they also limit their own earnings. Despite efforts to replace fee-for-service care with so-called global payments, “the fact is that currently most health-care systems are still operating in an environment where reducing emergency-department and inpatient use hurts their bottom line,” says Dr. Seth Berkowitz, a primary-care doctor at Massachusetts General Hospital who studies how addressing patients’ social needs improves their health and lowers costs.
Moreover, the model is challenging to scale, because all health care is local. State laws, hospital structures, and needs differ from place to place. What works in Florida doesn’t work in Washington state, and vice versa, notes Fernandopulle, whose frequent-flyer miles attest to his attempts to learn about new markets.
Slowly, though, these scattershot efforts may be coalescing into a larger movement. Fernandopulle says it’s getting easier for companies like his to raise money in the private sector. Other factors seem to be coming together, too. Technology allows health-care companies to more easily identify people at risk of becoming super-users, track their progress, and standardize some of their treatments. There’s broad public consensus, gaining momentum in recent years, that health-care costs need to come down, says Dr. J. Michael McGinnis, the executive officer of the National Academy of Medicine, an advisory body formerly known as the Institute of Medicine. “Now the issue is not whether; it’s how.”
Rizzuto is lucky that he was treated for his 2012 car accident in Massachusetts. If he’d had to recover in neighboring New Hampshire, where someone else’s road rage landed him in a ditch and then in a month-long coma, he’d probably still be making near-weekly trips to the emergency room. The crash left his spine broken in two places and exacerbated his post-traumatic-stress disorder and a concussion that still makes him feel like “I have some scramblage with my brain.”
The paralysis has left him with limited control of the outer three fingers on each hand—restricting his ability to play his beloved guitar—and he can’t breathe deeply enough or with enough control to sing anymore. His core muscles are weak, too, Rizzuto says, explaining why his torso wobbles uncontrollably as he speaks. “I’m so close to being a quadriplegic, it’s crazy,” he says. Rizzuto lifts his t-shirt to reveal small, circular burn marks dotting his chest. He knows he needs to quit smoking—and will have to before his upcoming surgery to close the wound on his back, but it has been a struggle. Rizzuto says he often spaces out with a cigarette between his fingers and doesn’t notice he’s doing himself damage until it’s too late. “There’s just so much to get used to,” he says.
But he has also come to terms with his current life. Despite everything that has happened, he still has his adult twin sons, a daughter, a granddaughter, a safe place to live, and caregivers who really care. And so he goes on living the best life he can. He even hopes to start talking to high-school kids about his experiences. “I’m very fortunate,” Rizzuto says. “I don’t know why. Maybe it’s because I’m supposed to do something with this stupid accident that happened to me.”
from Health News And Updates https://www.theatlantic.com/health/archive/2017/06/fixing-the-5-percent/532077/?utm_source=feed
0 notes
Text
Fixing the 5 Percent
An oversized poster of the Seinfeld character Kramer watches over Phil Rizzuto’s daily routine. When Rizzuto, named for the famous New York Yankees shortstop, swallows his 6 a.m. pills, Kramer is looming over him, looking quizzical. Same for the 9 a.m., noon, 6 p.m., and midnight doses, each fistful of pills placed in a carefully labeled Dixie cup. “I live on medication,” he says.
Listen to the audio version of this article:
Download the Audm app for your iPhone to listen to more titles.
Rizzuto’s daily life in Haverhill, Massachusetts, is a litany of challenges: His aides have to hoist his paralyzed legs from his bed to his motorized wheelchair and back again; keep the bag that collects his urine clean; tend to the gaping wound on his backside, which developed when he was left to lie still in bed too long; and help him avoid the panic that could claim anyone in his situation—that last one is particularly difficult since Rizzuto’s obsessive-compulsive disorder drives him to want to do everything for himself.
After more than a year of emergency and rehabilitative care following a devastating car accident, Rizzuto moved into a YMCA-run housing complex in this gritty New England town. But he still endured constant medical emergencies. “I was back and forth and in and out of the hospitals so much, it was like I didn’t know I had an apartment here,” the 56-year-old says, sitting in his small studio. His open wound kept getting infected; his diaphragm, weakened by his injury and his inability to quit smoking, left him gasping for breath; his urine-collection bag slipped out; his demons kept getting the better of him. The government eventually covered the cost of his care, but the relentless need for medical attention was exhausting and demeaning.
Then he opted into a Massachusetts health-care program called One Care that focuses on people with complex medical needs who are on Medicare. One Care provides 71 hours of aide support a week, a twice-weekly visit from a massage therapist, twice-monthly psychiatric care, a wheelchair support group, and a nurse practitioner who oversees and coordinates Rizzuto’s care. If he struggles between visits—or just wants to talk—she’s available by phone, even on weekends and after hours. Now, his life has a routine and a discipline that keeps emergencies at bay. “The difference it’s made …” he says, unable to fully express his gratitude. He estimates his hospital visits have dropped at least 75 percent since the One Care program took charge of his health. “I would hate like hell to not have them.”
The program that has helped Rizzuto is part of a nationwide movement to improve care for people struggling with very complicated medical needs—so-called super-users—the 5 percent of patients who account for about half of the country’s health-care spending. (Surgeon and New Yorker writer Atul Gawande outlined the problem and one solution in a definitive 2011 piece about the Camden Coalition of Healthcare Providers.) Some of these super-user programs say they provide cost savings of as much as 20 to 40 percent after a few years, as well as provide the kind of advantages offered to Rizzuto: fewer stressful hospital visits, better mental and physical health, and the satisfaction of being treated like a person instead of a package of problems. The program accomplishes this by shifting the focus of medical care. Instead of responding to complications, the care team tries to prevent them. “You can’t even get to the medical issue until you’ve figured out: Do they have a place to sleep, do they have housing they’re not going to lose, do they have food in their refrigerator, do they have a refrigerator?” says Christopher Palmieri, the president and CEO of the nonprofit Commonwealth Care Alliance, which manages 80 percent of One Care patients.
Despite its successes, this care movement, which doesn’t go by any catchy name—one doctor gave it the clunky title “high-impact, relationship-based primary care”—is scattered among a handful of states and is advancing only very slowly across the country. There is general agreement that these programs must address a range of social and pragmatic needs, like transportation, housing, nutrition, isolation, emotional well-being, and medical problems. But the details of each program are different. “Everyone’s trying their home brew,” says Dr. Harlan Krumholz, a cardiologist and health-care researcher at Yale University and Yale-New Haven Hospital.
The one thing all of the super-user care programs have in common is a mantra that could have come from Cosmo Kramer himself: Stay the hell out of the hospital. Hospitals, these folks argue, often make sick people sicker. They’re sources of infection to vulnerable patients. They’re disorienting. They run costly tests and look for issues that are better left alone. Super-users, says Krumholz, “represent a failure of the system.”
Medical care is dangerous,” says Dr. Rushika Fernandopulle, the co-founder and CEO of Iora Health, a leading practitioner of a more holistic approach to health. Fernandopulle says a big part of his company’s business model involves fighting to keep people out of the hospital—not just because it’s expensive, but because the care they will get puts them at higher risk for other problems. Medicare patients saw roughly a 40 percent drop in hospitalizations after Iora took over their care, Fernandopulle says.
For Fernandopulle, one patient in particular illustrates this phenomenon of snowballing medical care. That patient was an 80-year-old woman, fairly healthy but with hypertension and arthritis, who one day saw red in the toilet after urinating. She told her primary-care doctor, who sent her to a urologist; the urologist worried it might be cancer and ordered a catheter inserted. Before the procedure, a nurse asked the octogenarian if she ever felt weak or dizzy. (Of course she did—think about it.) When the woman said yes, a heart monitor was ordered: It showed a dip in her overnight heart rate. A cardiologist then scheduled the woman for a pacemaker.
“This is what I mean by the vortex,” Fernandopulle says, noting that inserting a pacemaker would be risky and provide no clear benefit. The woman’s condition might be explained in a much more low-tech way: a beet salad, for example, could be the culprit behind the red pee, and a prescribed medication might trigger the heart irregularity. “I called the cardiologist and politely declined the pacemaker for this patient,” Fernandopulle says. Part of the problem is that, while each doctor gets paid for each procedure he or she performs, usually no one gets paid for taking a step back and using common sense to think about what would genuinely help the patient.
“The health-care system as a whole is out of balance,” says Dr. Donald Berwick, the former head of the Centers for Medicare and Medicaid Services under President Obama. “We put far more into hospital care than we do keeping people from having to be in the hospital.” Hospital stays cost more than anything else in the health-care system; an average inpatient admission runs nearly $2,000 a day, and an intensive-care stay can easily cost $7,000 a day. In 2012, a typical hospital stay topped $10,000, according to the federal Agency for Healthcare Research and Quality. Caring for an Iora patient, on the other hand, typically costs about $3 a day and can reduce hospitalizations by 40 to 50 percent, Fernandopulle says. All of the physicians and advocates we interviewed who support this type of high-needs care are quick to note that their goal isn’t to deprive people of medical care. If someone doesn’t get needed heart surgery, they will end up in worse shape; no one will benefit. Their aim is appropriate, Goldilocks care: not too much, not too little.
Cory Sevin, a senior director with the Institute for Healthcare Improvement, a policy center in Cambridge, Massachusetts, says providing more appropriate treatment is also better for the caregiver. Kim Tremblay, a nurse practitioner with the Commonwealth Care Alliance, says that while the work is intense, she has enjoyed managing Rizzuto’s health team for three years and watching him slowly improve. “We give a lot to these patients,” she says. “We get a lot back.”
The model hinges on establishing strong, trusting relationships—but that doesn’t always come easily. “Some patients jump on board; sometimes it takes six months to establish a connection,” Tremblay says, recalling one patient who refused to talk to her for nearly five months before finally accepting help. She has become profoundly invested in her patients’ care. “Every time we send someone to the hospital, it’s stressful,” for both the patients and caregivers, Tremblay says. “We send someone in [and] we kind of shudder, Are they going to come out better?”
One big challenge to providing care for patients with complex needs is finding them. Commonwealth Care, for instance, has struggled to identify people who will benefit from its program. Any Massachusetts resident who receives both Medicare and Medicaid is eligible to join One Care. Commonwealth Care Alliance, which serves most of these patients, had to hire extra staff to track down potential clients. When Commonwealth Care started four years ago, 43 percent of these potential clients were considered “unreachable,” for reasons like having an unknown address. Today, that rate has shrunk to 32 percent.
Why is it so hard to track down needy patients? Some people are so isolated and disengaged that they’re largely invisible. Others patients are expensive and challenging today but might soon recover. And still others are doing fine now but might have a setback that throws them off balance for months. In fact, 60 to 80 percent of patients who are super-users now won’t be a year from now, Sevin says, and different people will be.
There are also people who will be perennially expensive—because their disease requires a costly drug, for instance. And there are those who will be expensive for a short time—say, for the few months after an organ transplant. There’s no point in wasting time trying to bring either group’s medical expenses down.
Fernandopulle says the only effective way to identify people at risk for super use is to ask them two questions: “How do you think your health is?” and “How confident are you in managing your health?”
“If they answer, ‘Poor, poor,’ they are at huge risk,” he says.
On a recent sweltering day, Rizzuto met his wheelchair support group at a small zoo in suburban Boston. Keeping cool in the above-90-degree heat wasn’t easy for Rizzuto. Paralysis robs people of their ability to regulate body temperature. One of Rizzuto’s aides, Bill Regan, came prepared with water, ice packs, sandwiches, and a spray bottle that he frequently spritzed on Rizzuto’s face and legs.
Rizzuto says these interactions with other people in wheelchairs help lift his mood, though on this trip he seemed more focused on watching a brown bear, several snakes, and tiny, hyperactive cotton-topped tamarins. He never could have made it around the zoo without a motorized wheelchair—though it took Rizzuto a year to convince the state to buy it for him. One of the first things One Care does when signing on a new client is to assess the person’s equipment needs, Tremblay says.
One Care is a partnership between Massachusetts’s Medicaid agency and the federal Centers for Medicare and Medicaid, and it focuses solely on patients ages 21 to 64 with multiple, complex medical and behavioral issues. (An older program, Senior Care Options, takes the same approach for patients over 65.) Most of Commonwealth Care’s 13,500 One Care clients earn less than $20,000 a year; some are homeless; the majority of them have a serious mental illness or substance-use disorder, as well as multiple other chronic health conditions.
This high-touch care approach is beginning to save money, says Palmieri. A report last year by the Commonwealth Fund found that among 4,500 members of One Care, patients enrolled for 12 continuous months had 7.5 percent fewer hospital admissions and 6.4 percent fewer emergency-room visits. For those enrolled in the program for at least 18 months, hospital admissions dropped 20 percent, the study found.
Although each model of high-touch care is different, the basics are the same: focusing on prevention, ensuring basic needs are met, reducing unnecessary treatment, and building relationships with patients. At Stanford University, for example, one young man with severe anxiety and obsessive-compulsive disorder required constant reassurance (in addition to his multiple medications) from doctors and emergency departments. In a traditional care system, emergency-room staff might roll their eyes and quickly send him on his way. Instead, Dr. Alan Glaseroff, the co-founder of Stanford’s Coordinated Care program to treat high-needs university employees and their family members, gave the 19-year-old his phone number. At first, whenever his anxiety or OCD took control, the young man called Glaseroff or another care coordinator as many as seven times a day.
But slowly, over the course of three years, the man learned to think before he called. If he saw spots in his eyes, he’d wait for a few minutes to see if they went away. He was taught to use mindfulness techniques, and if the symptom persisted, he would run through a checklist to see if it was really something to be concerned about. He ended up calling the clinic every two to three weeks, rather than multiple times a day, and learned not to lean on the clinic’s staff for minor issues. “Now, he hardly needs us,” Glaseroff says.
Creating viable long-term plans like this means far fewer emergencies. In fact, in its first three years, the Stanford program cut emergency-room visits for its 253 patients by 59 percent, hospital admissions by 29 percent, and total cost per patient by 13 percent, says Glaseroff, who teaches this model of care in two-day workshops across the country. According to the study, the Stanford practice saved the university $1.8 million and now has nearly twice as many patients.
The secret to the cost-savings, Glaseroff says, is for patients to use hospitals and doctors only when absolutely necessary and to rely for most of their care on empathetic—and relatively inexpensive—medical assistants, who check in with each patient about once a week. In the past four years, in an industry known for its high burnout and turnover, not one of his practice’s care coordinators has left, Glaseroff says. “They’re not allowed to diagnose and treat, but they’re really good at the people stuff,” he says. “The core is being given responsibility for people, not for tasks.”
Patients in the program have responsibilities as well as rights, Glaseroff says. They are expected to show up for their medical appointments and to come on time out of fairness to others. They’re told to call the clinic if they can before heading to the emergency room and then wait a few minutes for a call back, Glaseroff says. They are expected to do their part to engage with their care coordinator, even if the medical system hasn’t always treated them well in the past. “It’s patient self-management—what people do within their chronic illness 365 days a year—that matters the most,” he says.
For the high-touch model to work financially, large numbers of patients have to stick around long enough to recoup the upfront investment in their care. Today, there are only a few pools of people stable enough to sustain this model: people who work for major employers, like Stanford University, and those insured by the federal government.
Iora provides health care to workers at large, stable employers like the Dartmouth College Employees, the New England Carpenters Benefits Fund, a union trust, and members of Medicaid Advantage plans, like Humana and Tufts Health Plan. This gives them a big group of customers with high needs and the corporate muscle to avoid being pushed around by hospitals that don’t want to lose patients, Fernandopulle says.
If he loses customers to other insurance carriers in the first year or two, he’ll have all the upfront costs and none of the savings. A five-year time horizon allows Iora to recoup its upfront investment and get ahead of problems—controlling diabetes before it leads to a heart attack, for instance, says Fernandopulle, whose company oversees care for about 20,000 patients in eight states.
Iora and another company with a similar approach, Landmark Health, also provide care to people on Medicare Advantage—a government-funded, privately run program. About a third of people on Medicare now belong to Medicare Advantage programs, which were created by the Affordable Care Act. The Trump administration and Republicans have proposed huge cuts to Medicaid over the next decade. It’s unclear, however, whether such cuts would paralyze efforts at innovation or provide more urgency to reduce health-care spending. “It is a bipartisan issue that the current costs of health care are unsustainable,” Yale’s Krumholz says, “whether driven by empathy for those who are disadvantaged and suffering or by economic imperative.”
But there are also built-in disincentives to this kind of high-touch care. One of the most obvious is that hospitals make money on patients. If they succeed in decreasing readmissions, they also limit their own earnings. Despite efforts to replace fee-for-service care with so-called global payments, “the fact is that currently most health-care systems are still operating in an environment where reducing emergency-department and inpatient use hurts their bottom line,” says Dr. Seth Berkowitz, a primary-care doctor at Massachusetts General Hospital who studies how addressing patients’ social needs improves their health and lowers costs.
Moreover, the model is challenging to scale, because all health care is local. State laws, hospital structures, and needs differ from place to place. What works in Florida doesn’t work in Washington state, and vice versa, notes Fernandopulle, whose frequent-flyer miles attest to his attempts to learn about new markets.
Slowly, though, these scattershot efforts may be coalescing into a larger movement. Fernandopulle says it’s getting easier for companies like his to raise money in the private sector. Other factors seem to be coming together, too. Technology allows health-care companies to more easily identify people at risk of becoming super-users, track their progress, and standardize some of their treatments. There’s broad public consensus, gaining momentum in recent years, that health-care costs need to come down, says Dr. J. Michael McGinnis, the executive officer of the National Academy of Medicine, an advisory body formerly known as the Institute of Medicine. “Now the issue is not whether; it’s how.”
Rizzuto is lucky that he was treated for his 2012 car accident in Massachusetts. If he’d had to recover in neighboring New Hampshire, where someone else’s road rage landed him in a ditch and then in a month-long coma, he’d probably still be making near-weekly trips to the emergency room. The crash left his spine broken in two places and exacerbated his post-traumatic-stress disorder and a concussion that still makes him feel like “I have some scramblage with my brain.”
The paralysis has left him with limited control of the outer three fingers on each hand—restricting his ability to play his beloved guitar—and he can’t breathe deeply enough or with enough control to sing anymore. His core muscles are weak, too, Rizzuto says, explaining why his torso wobbles uncontrollably as he speaks. “I’m so close to being a quadriplegic, it’s crazy,” he says. Rizzuto lifts his t-shirt to reveal small, circular burn marks dotting his chest. He knows he needs to quit smoking—and will have to before his upcoming surgery to close the wound on his back, but it has been a struggle. Rizzuto says he often spaces out with a cigarette between his fingers and doesn’t notice he’s doing himself damage until it’s too late. “There’s just so much to get used to,” he says.
But he has also come to terms with his current life. Despite everything that has happened, he still has his adult twin sons, a daughter, a granddaughter, a safe place to live, and caregivers who really care. And so he goes on living the best life he can. He even hopes to start talking to high-school kids about his experiences. “I’m very fortunate,” Rizzuto says. “I don’t know why. Maybe it’s because I’m supposed to do something with this stupid accident that happened to me.”
Article source here:The Atlantic
0 notes
Text
Gucci and the TV stand
By Rivy
Sophomore Year-2013/2014
The house I lived in sophomore year was a spacious raised-ranched property. There was a huge living room that connected with the dining room and kitchen along with 2 full bathrooms and an outdoor deck that had stairs leading to the roof where I could marvel at the ocean in the distance (basically the ocean was my backyard). I lived with three other people, Posh and Goldy, who were my frat brothers, and Gucci who is my cousin (who is also my writing partner).
Now, it would be criminal to write a year worth of EVERYTHING that happened in that house. To abuse your innocent eyes with the tens of thousands of words that describe the insanity, nastiness, and overall ridiculousness that took place would be nothing short of eye-rape. So instead I offer you, the reader, the choice to whether or not my stories are worthy to continue on. I will go into as much detail as my memory will allow and share with you what happened that day/night.
Rivy, being myself, and Gucci being my cousin, will switch off narrating for you depending on the story and the people involved. Before each post, we will be sure to note whose authoring said story. For my first post, I will tell a story that isn’t too sickening, but falls into the spectrum of straight up stupidity. I hope this breaking of the literary ice is to your liking. Without further a due…
My cousin is around 5’7 and looks like a morphed version between Adrian Brody and Robert Downey Jr., added with a hint of 1990’s fashion (this took place in 2013/2014). Other than his looks, his skinniness happens to be his most notable feature. In fact, he is so skinny, pointed, and angular it wouldn’t be a surprise to me if a carpenter used him to take exact angled or perfect 90-degree measurements. The story begins in the quiet morning of a random day during the second semester of the school year (a good five months into our occupancy of this house). I am awoken to the sound of my cousin wallowing in pain, as his room is close to mine in the basement.
“Ow! Jesus Christ! My goddamned knee!”
This is a daily, common occurrence due to the fact that my cousin is a drummer and has his set only a few inches outside his bedroom door. Every time in the morning he, in his drowsy state of mind, would always open his door and immediately whack a part of his pointed body on his drum kit. Apparently the winner this morning was his knee.
Judging by the pain in his voice, I could instinctively concur that he really whacked his knee hard. So I giggle quietly to myself before I fall back asleep.
Time goes by and I’m on campus during a break between classes. My cousin’s schedule is similar to mine so around this time we’d meet up at the campus café’ and shoot the shit before my next class. I get there, and to my surprise, he isn’t sitting down at our usual spot typing away on his MacBook. I look around for a few seconds, but to no avail. Now, this is new to me. Throughout the whole year at this point, my cousin hasn’t been absent ONCE from our café breaks. So naturally, I text him. No response. I wait. I wait a little longer. I text him again. Nothing.
It went from “Hey dude, I’m at the Clams Den. (not the real name of the café’) Where the fuck are you?” to “Listen you bastard! I’m sitting down alone like a fucking leper! Stop jerking your crooked, skinny, wart and pimpled covered dick and come here!” Nothing.
So I sit down, alone, and get some work done before my next class. I arrive home early in the evening and notice my cousins Jeep is here. My two other roommates aren’t home yet. “Great.” I thought to myself. “He wasn’t kidnapped and forced to stick matchsticks up his ass while lemons were being squeezed in his eyes.” (That’s another story….) So no need to worry there.
I enter the house and go upstairs to grab a drink from the fridge when I see my buddy Hencho sitting on the couch in the living room smoking the communal bong.
A little backstory on Hencho: Hencho is around 30+ years old at the time. He is a Canadian from Canada who is in the same frat as me. He lived a few streets over and was taking classes to finish up his degree. Hencho resembled Cosmo Kramer in a way. No, not the whacky hair or the way he looked, but a resemblance of his mannerisms. At times he’d barge in the house without knocking, pack the bong bowl to the brim with his weed, and rip the WHOLE thing in one go. He’d hold in the smoke for as long as he could, slowly exhale where no smoke would come out, give us or whoever was there a quick wink, and leave without saying a word. It was pretty funny to say the least.
I plop down next to him and we talk and take rips of the bong. He asks me where Posh and Goldy were; I say I have no idea. We keep smoking and smoking until we get retardedly high. Like Helen Keller high but we obviously can still see, hear, and speak.
Anyway, I get hungry and forgot to go grocery shopping. I wasn’t about to move my lazy ass to get something so I decide to do the appropriate thing and order a pizza. Me, being the selfless and caring roommate/cousin that I am, text Gucci to see if he wanted anything. Ten minutes go by and there’s no response. What the fuck is this kids deal? First he ignores me during break, makes me sit alone at the café’ and now he’s STILL not responding to my texts to see if he wants pizza! PIZZA! It’s not like I’m offering him a gooey slice of coagulated dolphin jizz. It’s fucking delicious PIZZA! This pisses me off.
I ask Hencho if my cousin is even home since his car was outside and he hasn’t come up stairs for the good 30 minutes I’ve been here. He says he saw him walk in, didn’t say hi, and went straight downstairs into his room. “Okay, maybe he’s having a bad day and whatnot. I can deal with it…nah, fuck that.”
In our high and clouded state of mind, we decide we are going to address my cousin for being such a flake today. We both go downstairs to see what this kids problem was. I approach his closed door and knock. No response. I look out the sliding doors and see his car is still in the driveway. I put my fucking ear against door and can hear the TV on. I knock louder. No response. I jerk around with the doorknob and the door is locked. Okay, you dick. I see how it is. Hencho and I take a step back and look around for things to use to fuck with him. All of a sudden I see the big TV stand in the corner of the basement.
I begin to smile larger than an autistic hyena.
I quietly push my cousin’s drum shit as far away from his door as it can go. “Yo Hencho, see that fucking TV stand over there, help me move and prop it on Gucci’s door.” I whispered. We quietly lift the TV stand up and move it over to his door. Now this TV stand is kinda tall and pretty fucking heavy. I’m not a weak guy, and even with two men this was kind of bitch to move. This stand was all solid wood with all the draws filled with shit. It had to be at least 200-250+ lbs total.
We balance the stand until it’s on one leg and leaning on his door. “Great, you don’t wanna come out and be social, you can stay in there all night!” I thought to myself.” My cousin is a string bean so there’s no way he’s opening his door with the stand propped on it. His room is too small to even get a running start and to push it open. We giggle more and more as we position the stand so it’s stable as possible.
All of a sudden…. “What are you fucking retards doing out there?!” my cousin says as he unlocks and opens the door…. BAM! The stand crashes into my cousin’s head right before Hencho and I quickly catch it.
Me being the complete fucking idiot I am forgot that his door opens from the INSIDE, not out. Our plan of him being stuck in his room and not being strong enough to push his door open quickly failed as the complete weight of the balanced TV stand cracked him in the head. Luckily, our reflexes were fast enough to maneuver the stand away from crushing my cousin’s malnourished and fetal-positioned body on the floor.
We say sorry a million times as he is rolling on the ground in pain. As I was profusely apologizing, I was also processing what just happened in my mind and couldn’t help but laugh a little. My cousin gets up, sticks his head in our faces to show that he has a pretty decent cut and is bleeding (nothing serious), grabs his things, and walks out of the house. He backs out of the driveway and screws off.
Hencho and I quickly talk about what just happened. Laughed it off. Went back up stairs and continued to smoke. This story is NOTHING compared to the shit we did that year… This was just a taste ;)
TL;DR: My roommate/cousin was being a flake one day, balanced a tv stand on his bedroom door so he can't get out, tv stand crashes into his head.
0 notes