#omicron india cases
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In 2020, Tumblr had 29.4 million users in the US.
Text
कोरोना केस 2025: भारत में फिर बढ़ा संक्रमण, कई राज्य हाई अलर्ट पर #News
0 notes
Text
Old News (Published Nov, 2022)
Also preserved on our archive
Pro-Tip: All covid-19 strains are capable of immune escape from both vaccination and acquired immunity from infection! Mask up to prevent the spread of covid and further mutation toward immune escape!
By Alice Park
New lab data suggest that vaccines and prior infections may not offer enough protection against several new COVID-19 variants cropping up in the U.S. and around the world.
Dr. David Ho, director of Columbia University’s Aaron Diamond AIDS Research Center (ADARC), and his team reported the results from a set of studies at an ADARC symposium. They showed how well some of the latest variants—BQ.1, BQ.1.1, XBB, and XBB.1, which were all derived from Omicron—are evading both vaccine-derived and infection-derived immunity.
These new variants all have mutations in the region that binds to cells and infects them, which means that they’re highly transmissible, as prior Omicron variants were. BQ.1 is growing steadily in France, according to the public database of SARS-CoV-2 variants GISAID. By mid-November, European health officials expect the variant to account for 50% of cases in Europe, and to become the dominant strain in that region by early 2023. XBB is growing quickly in Singapore and India. Both variants have spawned new strains that have each picked up an additional mutation to create BQ.1.1 and XBB.1. As of early November, BQ.1 and BQ.1.1, combined, now make up about 35% of new cases in the U.S.
Other studies have found similar drops in antibody protection against BQ.1 among vaccinated people. But Ho’s group conducted what is likely the most comprehensive look to date at BQ.1, BQ.1.1, XBB, and XBB.1, and how existing immunity—from the original mRNA vaccines, the new Omicron boosters, and natural infections—stands up to them. Scientists took blood sera from 88 people in five groups (below) and exposed it to the four variants in the lab. Here’s what they found:
Fully vaccinated and once-boosted people (three total shots of the original mRNA vaccines) had 37- and 55-fold lower neutralization against BQ.1 and BQ.1.1, respectively, than they did against the original SARS-CoV-2 virus, and about 70-fold lower neutralization against XBB and XBB.1. Fully vaccinated and twice-boosted people (four total shots of the original mRNA vaccines) had 43- and 81-fold lower neutralization against BQ.1 and BQ.1.1, respectively, than they did against the original virus, and 145- and 155-fold lower neutralization against XBB and XBB.1, respectively. Fully vaccinated and twice-boosted people (three shots of the original vaccine plus one Omicron booster) had 24- and 41-fold lower neutralization against BQ.1 and BQ.1.1, respectively, than they did against the original virus, and 66- and 85-fold lower neutralization against XBB and XBB.1, respectively. Fully vaccinated people who had received the original booster and who had been infected with BA.2 had 20- and 29-fold lower neutralization against BQ.1 and BQ.1.1, respectively, than they did against the original virus, and 103- and 135-fold lower neutralization against XBB and XBB.1, respectively. Fully vaccinated people who had received the original booster and who had been infected with BA.4 or BA.5 had 13- and 31-fold lower neutralization against BQ.1 and BQ.1.1, respectively, than they did against the original virus, and 86- and 96-fold lower neutralization against XBB and XBB.1, respectively.
The results show that people who had been infected with BA.2, BA.4, or BA.5 generally experienced the smallest drop in neutralizing antibody levels against against BQ.1 and BQ.1.1. But people who had three doses of the original vaccine and one Omicron booster produced only slightly better neutralizing antibody protection against XBB and XBB.1 than those who received three doses of the original vaccine. Public-health experts say that while vaccines may wane in efficacy against newer variants, they continue to protect people from severe COVID-19. There is early evidence that vaccine-induced immunity may also produce a broader range of virus-fighting antibodies over time.
Read More: BQ.1, BQ.1.1, BF.7, and XBB: Why New COVID-19 Variants Have Such Confusing Names
Still, these results are a reminder that vaccines and drug treatments need to evolve with the virus. “These new variants are extremely good at evading our antibodies and are very likely to compromise the efficacy of our vaccines,” says Ho. They may also dodge the available antibody-based treatments for COVID-19, he says. The National Institutes of Health’s COVID-19 Treatment Guidelines currently only include one monoclonal antibody therapy, bebtelovimab, because the virus has evaded all of the previously authorized antibody treatments. But in an October update, NIH scientists acknowledged that the “subvariants BQ.1 and BQ.1.1 are likely to be resistant to bebtelovimab.” The drug is therefore only recommended if people either can’t take the antiviral drugs Paxlovid or remdesivir, or if these medications aren’t available. The virus can evade these treatments as well, but they remain the first line of defense against severe SARS-CoV-2.
The good news is that in places where these variants are spreading, they do not seem to be linked to more severe COVID-19 disease—measured by hospitalizations and deaths—than other Omicron iterations. Still, public-health experts say a spike in infections could still strain health resources, especially as other respiratory infections, including influenza and RSV, also gain momentum. The combination of several circulating infectious diseases could mean more illness overall, and, in turn, more people who might experience severe disease and require intensive medical care.
The rise of BQ.1, BQ.1.1, XBB, and XBB.1 points to the fact that when it comes to immunity, the virus may always be one step ahead, especially with respect to vaccines. “I would start to make these vaccines, and start to test them in animals,” says Ho. Even if those efforts began now, it’s possible they may still lag behind the virus and the new mutations it continues to gain. That’s why researchers are working on developing vaccines that would be more universally applicable to a range of different coronaviruses, which could shorten the amount of time it takes to build up a vaccinated population’s immunity.
#mask up#covid#pandemic#wear a mask#public health#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#covid pandemic#covidー19#covid conscious#covid is airborne#covid isn't over#covid19
19 notes
·
View notes
Text
Zero, Negative, and Infinite Numbers in Antiquity
With the advent of accounting, numbers became more important to people of the Bronze Age and into the Iron Age. Numbers grew into a thing of philosophy as much as they were of accounting and geometry. Number systems were developed, based on systems of 10, 20, or even 60, depending on the culture, but numbers having a value based on where in the number they appear, such as the value of 4 being different in 4356, 43, and 354, was something that came along later. This is something we take for granted now, but wasn't developed until the Hindu people of India. The biggest development that allowed for a positional system of numbers is 0.
Zero shows up in some ways before the Hindu-Arabic numeral system was formalized. The Ancient Egyptians used a symbol called 'nfr' to symbolize when the amount received by pharaoh was equal to what was distributed, but they did not use a positional system when writing other numbers. The Babylonians also didn't use a positional number system, though they might use three hooks, or later two slants, as punctuation marks between between numbers like we use zero now, but they were never used alone or at the end of a number, showing that the concept wasn't fully developed yet.
By Miranche - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=55976282
The ancient Greeks seemed to be philosophically opposed to zero while also needing to use it for their astronomy. They used lower case omicron (ό) initially in place of the punctuation marks that the Babylonians used. The quantity of zero led to the philosophical question 'how can not being be?', on which the paradoxes of Zeno of Elea rest (one of which being 'that which is locomotion must arrive at the half-way stage before it arrives at the goal').
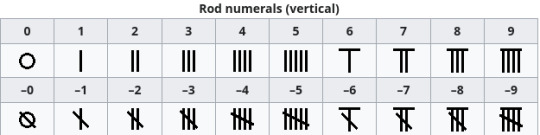
The ancient Chinese used a counting rod system that allowed positive and negative numbers depending on how exactly the numbers were written, but treated zero itself as a vacant place, lending the system a type of positional set up, but without having a zero or null concept. At some point prior to CE 1274, the symbol 〇 as the placeholder and was probably borrowed from the Indian people.
By National Geographic - National Geographic [1]. Non creative image of a 2D artifact from the 3-4th century CE., Public Domain, https://commons.wikimedia.org/w/index.php?curid=73315832
In India, a black dot was used as a symbol for zero, which gradually became hollow. It was fully recognized as a number as far back as CE 224, though Pingala, a Sanskrit scholar who lived around the 2nd or 3rd century BCE, created a type of notation similar to Morse code with long and short sylables and included a zero, using the word Śūnyatā शून्यता to represent zero. The word is generally translated as 'insubstance' or 'nothingness'.
Negative numbers are a part of accounting, so they existed from the beginning of the idea of counting. The only known group of peoples to have specific notation for them, though, are the ancient Chinese with their counting rod system.
By Nevit Dilmen - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=4182698
In ancient cultures, infinity wasn't a number, but an idea to be explored through philosophy. The earliest record we have of this discussion is Anaximander, who lived from about 610-546 BCE, who called it apeiron ἄπειρον, which is translated as 'unlimited, boundless, indefinite'. He considered this to be the basis of reality. Anaxagoras, who lived from about 500-428 BCE, believed that the universe had the capacity to be infinitely divided (leading to the idea of atoms). Aristotle (384-322 BCE) rejected the idea that infinity was a real thing and could only be an idea. Aristotle's ideas were not widely disputed until the Enlightenment.
By I, Tó campos1, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=2304574
Early Indian thinking on infinity was written into the Jain upanga Agamas जैन साहित्य around 400 BCE. There it is held that numbers can be divided into three groups: enumerable (lowest, intermediate, highest), innumerable (nearly innumerable, truly innumerable, innumerably innumerable), and infinite (nearly infinite, truly infinite, infinitely infinite). They were the first group to recognize that not all infinites are the same, which corresponds with the modern mathematical thinking. Infinite length, infinite area, and infinite volume are all infinites, but not the same infinite.
#numbers#ancient egypt#hindu numbers#infinity#negative numbers#zero#mathematics#math history#maths history
2 notes
·
View notes
Photo

India has reported a sudden rise in COVID cases, starting from late May. Authorities said the number of active cases of the disease has surpassed 5,000.India is the latest of a number of countries to report an uptick in COVID cases this year as, more than five years after the virus was declared a global pandemic, waves of new strains continue to emerge. Here is what we know about the new variant of COVID and where it has spread: How many COVID cases are there in India? As of Thursday this week, there are 5,364 active cases in India, according to India’s Ministry of Health and Family Welfare. Since January 1, more than 4,700 people have recovered from COVID in India, while 55 people have died from the virus. Which variants are causing new cases and where? The main coronavirus variant causing a new spread of the disease is known as NB.1.8.1. Cases caused by this variant have been reported in the United Kingdom, the United States, Australia, Thailand, China and Hong Kong, among other countries. It is now the dominant variant in China and Hong Kong. A second variant, LF.7, is also responsible for some of the cases in India. The UK Health Security Agency (UKHSA) said it had recorded 13 cases of the NB.1.8.1 variant in England, with “small numbers” detected across the UK. By late April, NB.1.8.1 comprised about 10.7 percent of submitted sequences globally, according to the World Health Organization (WHO). This rose from just 2.5 percent one month before. What do we know about the NB.1.8.1 variant? The Omicron variant NB.1.8.1 was first detected in January this year. Advertisement It is a “recombinant” variant, which means it has arisen from the genetic mixing of two or more existing variants. On May 23, 2025, the WHO declared the NB.1.8.1 strain a “variant under monitoring” (VUM). According to a 2023 definition by the WHO, a VUM is a variant which has undergone genetic changes that scientists believe could potentially affect the behaviour of the virus; early data suggests that this variant can grow faster or spread more easily than others, but this has not yet been confirmed. The evidence of the variant’s impact on health, immunity or transmission is still unclear. Why are there so many new cases? While the NB.1.8.1 strain is still being researched, the evidence so far suggests that the strain may spread more easily, virologist Lara Herrero wrote for The Conversation on May 28. Researchers using lab-based models have found that of several variants tested, the new strain had the strongest ability to bind to human cell receptors. This suggests that the strain may “infect cells more efficiently than earlier strains”, Herrero wrote. “It is more transmissible,” Subhash Verma, a professor of microbiology and immunology at the University of Nevada, Reno School of Medicine, told CBS News. What are the symptoms? Common symptoms of the NB.1.8.1 strain include a sore throat, cough, muscle aches, fever and nasal congestion. It can also cause gastrointestinal symptoms such as nausea and diarrhoea. Are COVID vaccines effective against the new strain? Vaccines remain a powerful defence against COVID infections, severe sickness, hospitalisation and death, clinicians say. However, virologist Herrero wrote that besides spreading more easily, NB.1.8.1 may “partially sidestep” immunity gained from the vaccines or prior infection. For now, health authorities say current COVID jabs are expected to be effective against this coronavirus variant and protect people from severe illness. Should we be concerned? Health experts worldwide say there is no evidence that the new strain of the coronavirus is more severe or deadly than any previous strain. However, it does appear to spread more easily. Since COVID spreads through airborne particles and droplets, the spread of the virus can be prevented by getting tested if symptoms show, wearing a mask and social distancing, clinicians have advised.
0 notes
Text

JN.1, a fast-moving sub-variant of Omicron, is currently circulating across India. While it is highly contagious, most reported cases have shown only mild symptoms. Let’s stay alert and informed—not fearful.
0 notes
Text
Dr explains: Why booster shots are crucial even with mild Covid-19 symptoms prevailing
Dr explains: Why booster shots are crucial even with mild Covid-19 symptoms prevailing India is experiencing a mild surge in Covid-19 cases driven by new Omicron subvariants, with mostly mild symptoms. Experts stress the importance of boosters, surveillance and protecting vulnerable groups. Firstpost brings out a doctor’s view on symptoms, vaccine effectiveness, and the country’s preparedness in…
0 notes
Text
COVID-19 Cases Rise In India: Here's What You Need to Know About The Symptoms
Last Updated:June 03, 2025, 17:03 IST Covid cases in India today: Kerala continues to report the highest number of active cases at 1,435, followed by Maharashtra with 506 and West Bengal with 330 The rise in cases is likely due to the spread of the JN.1 variant, a subvariant of Omicron India Covid Cases Today: India is witnessing a fresh surge in COVID-19 cases, with the number of active…
0 notes
Text
COVID-19 Cases Rise In India: Here's What You Need to Know About The Symptoms
Last Updated:June 03, 2025, 17:03 IST Covid cases in India today: Kerala continues to report the highest number of active cases at 1,435, followed by Maharashtra with 506 and West Bengal with 330 The rise in cases is likely due to the spread of the JN.1 variant, a subvariant of Omicron India Covid Cases Today: India is witnessing a fresh surge in COVID-19 cases, with the number of active…
0 notes
Text

🚨 𝐂𝐎𝐕𝐈𝐃 𝐀𝐋𝐄𝐑𝐓: 𝟑,𝟎𝟎𝟎+ 𝐀𝐂𝐓𝐈𝐕𝐄 𝐂𝐀𝐒𝐄𝐒 🚨 Is another lockdown on the way? 😷
India is seeing a sudden rise in COVID-19 cases, with 3,395 active cases and 4 deaths in just the last 24 hours. 🚩 Kerala, Maharashtra, and Delhi are among the most affected states.
🔬 The main reason behind this new wave is the JN.1 subvariant — a version of Omicron. The good news? Most cases are mild. The concern? Elderly people and those with weak immunity are still at risk.
🦠 The symptoms feel just like the flu — so don’t ignore even a slight fever or cough. ✅ Stay alert. Get tested. Wear a mask if needed. Let’s stay safe and protect our loved ones! ❤️ The Health Ministry continues to monitor the situation closely and has advised citizens to maintain basic precautions — mask in crowded areas, ensure proper hygiene, and avoid self-medication. This isn’t a cause for panic, but a call for preparedness. The virus is evolving, and so must our response. Stay safe, stay updated, and protect those around you.💉😷🧼 Follow ProCapitas (the financial services arm of Jobaaj Group) for more.
0 notes
Text
coronavirus-in-india-covid-new-cases-deaths-omicron-variants
डराने लगा COVID! ऐक्टिव केस 4 हजार के करीब, हर 6 घंटे में औसत�� 1 मौत!

कोरोना एक बार फिर डराने लगा है. इसके मामले लगातार बढ़ते जा रहे हैं. इसके साथ ही कोविड से होने वाली मौतों की संख्या भी अब चिंता बढ़ाने लगी है. स्वास्थ्य मंत्रालय के मुताबिक, देश में कोविड के ऐक्टिव केसेस की संख्या 4 हजार के करीब पहुंच गई है.
स्वास्थ्य मंत्रालय की ओर से जारी किए गए आंकड़ों के मुताबिक, देशभर में अब कोविड के ऐक्टिव केसेस की संख्या 3,961 पहुंच गई है. पिछले 24 घंटों में कोविड के नए मामलों की संख्या 203 बढ़ गई है. इसके साथ ही 24 घंटे में 4 मौतें भी हुई हैं. इस हिसाब से देखा जाए तो कोविड से हर 6 घंटे में औसतन एक मौत हुई है.
सबसे ज्यादा 1,435 ऐक्टिव केस केरल में हैं. 24 घंटे में केरल में कोविड के 35 नए मरीज सामने आए हैं. इसी दौरान 1 मरीज की मौत भी हुई है. इस साल 1 जनवरी से 1 जून तक केरल में कोविड से 8 मरीजों की मौत हो चुकी है.
पूरा आर्टिकल पढ़ने के लिए नीचे लिंक पर क्लिक करें👇
डराने लगा COVID! ऐक्टिव केस 4 हजार के करीब, हर 6 घंटे में औसतन 1 मौत!
#covid#coronavirus in india#why covid is not going away#covid is endemic#why covid cases increasing#covid news#corona#coronavirus#कोरोनावायरस#कोविड
0 notes
Text
Active Covid cases in India rise to 3,395
India’s active COVID-19 cases surpass 3,000, with Kerala leading at 1,336. Four deaths reported in 24 hours. ICMR’s Dr Rajiv Behl assures current Omicron subvariants are not severe.
0 notes
Text
Why Biden’s premature COVID ending could help it surge - Published Sept 23, 2022
Two years out from the publication of this article, and we can really see how true these warnings were. Why does the mainstream media and DNC refuse to do anything about forever covid?
This week, President Biden said what millions of Americans have been hoping to hear since the spring of 2020: “The pandemic is over.”
I understand the impulse to close the book and move on. But I am deeply concerned that this declaration is not only premature but also dangerous.
The SARS-CoV-2 virus has shown us, again and again, the danger of hubris. Think of the lethal impact of the omicron virus last winter, just when we were so grateful that the delta wave had ebbed. Think of the deadly surges this summer, just when we were planning our long-delayed vacations. This is a virus that has humbled us too often. We must approach it with humility.
This declaration has many damaging effects: As others have noted, it will now be even harder to persuade Americans to get the new bivalent boosters. It’ll be tougher to persuade Congress to fund essential COVID responses. And it will be nearly impossible for local officials to impose new indoor mask requirements should another surge arrive.
To be sure, Biden did acknowledge in his “60 Minutes” interview that “we still have a problem with COVID” and added that “we’re still doing a lot of work on it.” But he sandwiched that message between two flat declarations that the pandemic is over. Those are the soundbites that have reverberated most loudly, and they are decidedly unhelpful.
Dr. Tom Frieden, former director of the Centers for Disease Control and Prevention, has spoken often about how the U.S. has lurched from a cycle of panic to neglect when it comes to public health. Many of us in the field had hoped that the COVID-19 pandemic would break that cycle — a sliver of silver lining amid all the grief.
We had hoped that policymakers and voters alike would understand how essential it is to upgrade our data infrastructure, stockpile essential medicine and equipment, invest in preventive care for vulnerable populations, restructure our emergency response agencies and support an infusion of public health workers at the local and state levels. Surely, COVID would be the spur needed to finally bump U.S. spending on public health to more than 3 cents on the health care dollar.
By declaring the pandemic over when we are still very much in the thick of the fight, President Biden is undercutting that message.
Let’s look at where we are right now. The U.S. is still reporting close to 60,000 cases and 400 deaths each day. Millions are struggling with long COVID; by some estimates, this often debilitating condition is keeping 4 million adults out of work. Those at work may have less flexibility: Major companies are ending work-from-home policies and Starbucks announced this week that it will no longer give employees paid time off to isolate or get vaccinated. Biden’s remarks will only accelerate that trend.
Meanwhile, only 67 percent of Americans are vaccinated and only half of them have been boosted. While many of the remaining have some immunity from infection, the death toll makes clear that large swaths of the population remain highly vulnerable. And of course, new variants continue to emerge; right now, all eyes are on BA.2.75.2, a mutation of the omicron variant that is notably better at evading antibodies acquired from vaccination or prior infection and is spreading rapidly in India.
Declaring the pandemic over at this stage is tantamount to accepting all this misery as background noise.
And if we accept the status quo as background noise — rather than the urgent and immediate threat it represents — it’s nearly impossible to make the case that we need to do more as a society to protect the vulnerable, respond to surges, or prepare for future crises.
The Biden administration has made significant strides on COVID. It made tests, vaccines and treatments widely available across the country, which improved outcomes and saved lives. The vast majority of Americans feel we’re in a better place than at this time last year and many have returned, at least in large part, to normal activities.
It is an appropriate moment for our leaders to turn the page away from our wartime footing and begin a sober discussion about the next steps: the risks that remain, the importance of responding quickly to local surges, the value of supporting the Global South in building their own vaccine infrastructure — and the critical need to rebuild the battered and woefully outdated public health infrastructure in the U.S.
It is not the moment to declare victory.
John M. Barry, author of “The Great Influenza: The Story of the Deadliest Pandemic in History” has a stark warning from history. He writes that the world had largely moved on from the 1918 influenza pandemic when a fourth wave struck in 1920. By then, the U.S. had plenty of natural immunity from prior infection. Still, the virus spread ruthlessly. Public officials failed to respond. They, like the public, wanted the pandemic to be over — so the virus rolled on unchecked. In some cities, the death toll in 1920 exceeded the toll of the huge second wave.
We should not make the same mistake now. With humility as our watchword, we can move to the next chapter without closing the book. That is the way forward.
Michelle A. Williams is dean of the faculty of the Harvard T.H. Chan School of Public Health.
#covid#mask up#pandemic#covid 19#wear a mask#coronavirus#sars cov 2#public health#still coviding#wear a respirator#us politics#joe biden#democratic party
16 notes
·
View notes
Text
What's behind the recent rise in Covid 19 cases?
The recent rise in COVID-19 cases in India and other parts of the world is emergence of new omicron subvariant, notably NB.1.8.1 and NF.7. These variant are more transmissible, leading to increased infections, especially in densely populated areas. Emergece of new variants: The NB.1.8.1 variant first identified in travellers from countries like china, japan and spain, has become dominant in…
0 notes
Text
COVID-19 Cases Rising Again in 2025: What You Need to Know

Introduction
After a few quiet years, COVID-19 is once again making headlines in 2025. Many people thought the virus was gone for good, but recent data shows a steady rise in new cases across several countries, including India. While the current variants may not be as deadly as those in the past, it's still important to stay alert and take precautions.
This blog will help you understand why COVID-19 cases are increasing again, what symptoms to look for, how to protect yourself, and why vaccination is still important. Let’s break it down in simple terms.
Why Are COVID-19 Cases Rising Again in 2025?
Health experts say that the recent rise in COVID-19 cases is due to several reasons:
1. New Variants Emerging
The virus is constantly changing. In 2025, a new Omicron sub-variant has been spreading faster than older versions. These new variants may not cause severe illness but are highly contagious, meaning more people are getting infected quickly.
2. People Letting Their Guard Down
Many people have stopped wearing masks or washing hands regularly. With large gatherings, events, and travel back to normal, the virus has more chances to spread.
3. Vaccination Gaps
Booster shots are essential for continued protection, especially for older adults and people with weak immune systems. However, a large number of people in India haven’t taken the latest COVID-19 booster.
4. Seasonal Changes
Just like the flu, COVID-19 seems to rise with seasonal shifts, especially in colder months when people spend more time indoors.
Common Symptoms in 2025
The symptoms of the latest COVID-19 variant are slightly different from those we saw in the early years of the pandemic. Most people are experiencing:
Sore throat
Dry cough
Fatigue or tiredness
Nasal congestion or runny nose
Headache
Mild fever or chills
Most cases are mild, and people recover at home. However, the elderly or people with chronic conditions like diabetes or heart problems should be more careful.
What To Do If You Feel Sick
If you notice any of the symptoms mentioned above:
Stay home and isolate yourself.
Wear a mask to avoid spreading the virus to others.
Take a COVID-19 test (at home or at a nearby health center).
Monitor your oxygen levels with a pulse oximeter.
Stay hydrated and rest.
Talk to a doctor online or in person if symptoms worsen.
You can book online consultations and COVID tests from trusted platforms like SecondMedic for quick support.
Importance of Vaccination in 2025
Many people wonder: “If I’ve already had COVID or got vaccinated earlier, do I still need a booster?”
The answer is yes.
Here’s why:
Immunity from old vaccines can fade over time.
New variants may escape older protection, but boosters are updated to fight them better.
Getting a booster shot can reduce the risk of severe illness, hospitalization, or death.
People above 60, pregnant women, and those with chronic conditions should get vaccinated or take a booster dose as soon as possible.
How To Protect Yourself and Others
Even though the current wave is not as dangerous as the earlier ones, it's still better to be safe than sorry. Follow these simple steps to reduce your risk:
1. Wear a Mask
Use a good quality mask like N95 when you're in crowded places like markets, public transport, or hospitals.
2. Wash Hands Regularly
Use soap or hand sanitizer, especially after touching public surfaces.
3. Avoid Crowds
If you’re feeling unwell, stay home. Avoid crowded events if possible.
4. Ventilate Rooms
If you're indoors, make sure there is proper airflow.
5. Stay Updated
Check your local health department's guidelines and case updates regularly.
What the Government Is Saying
Health departments in India and globally are keeping a close watch. So far, there are no full lockdowns, but some states have started recommending masks and social distancing in public places.
Airports, hospitals, and some schools have reintroduced temperature checks and COVID screening. The government is also encouraging people to get booster doses and has increased vaccine availability in public and private hospitals.
Online Healthcare Services: A Safer Option
One major lesson we’ve learned from the pandemic is the power of online healthcare. Teleconsultations and medicine delivery have made healthcare safer and more convenient.
Websites like SecondMedic allow you to:
Book COVID tests at home
Consult doctors online
Order COVID safety kits and medicines
Schedule vaccinations
It’s a safe and smart way to avoid hospital visits unless absolutely necessary.
Final Words
We all hoped COVID-19 was behind us, but the recent rise in cases reminds us that the virus is still around. The good news is, we’re better prepared than before. With awareness, vaccination, and some basic precautions, we can stay safe and healthy.
Let’s not ignore the signs or take unnecessary risks. Whether it’s wearing a mask, getting a booster, or staying informed — every step counts.
Conclusion
As COVID-19 cases rise again in 2025, don’t panic — but don’t ignore it either. The virus may not be as deadly, but it’s still affecting lives. Protect yourself and your loved ones by staying informed, taking your booster, and being responsible.
If you’re looking for fast, trusted help — from COVID tests to doctor consultations — visit www.secondmedic.com today. Stay safe and stay informed about “COVID-19 Cases Rising Again in 2025: What You Need to Know.”
0 notes
Text
India Witnesses Rise in COVID-19 Cases Amid Emergence of New Omicron Subvariants NB.1.8.1 and LF.7...
0 notes