#occupational therapy in substance abuse
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
US Tumblr user growth rate is estimated to slow down to 4.1%.
Text
REFLECTIONS ON MY COMMUNITY BLOCK: A 4TH YEAR OCCUPATIONAL THERAPY STUDENT PERSPECTIVE
As I write what I believe is my last blog of the year, possibly and hopefully the last blog I will ever write as a student, I reflect on my journey in my community block. For the past 5 weeks, I have had the pleasure and the privilege to serve the Cator Manor Community and the people at the Denis Hurley Center. I have to say, I am filled with gratitude to have been exposed to such a community. Not only has it helped shape me as a student, but it has also helped teach me invaluable lessons that I believe will be useful to me as a future health practitioner.
Serving the Cator Manor community, an under-resourced community with most of the people falling in the lower socio-economic status, I encountered and worked with people with various health challenges including, but not limited to hand injuries, strokes, people in need of wheelchairs, and children with ASD. While working in this community, I came to realize that contrary to my preconceived assumptions about community practice, even though the people come from the same community and share similar cultural backgrounds, each of them has their own story. By understanding that, I believe I was then able to fulfill our roles of promoting health and well-being (AOTA,2020), and ensuring people can participate in occupations meaningful to them. Through collaboration with other healthcare practitioners in the clinic, which included, but was not limited to, having joint sessions with physiotherapists, we did our part in fulfilling the aim of holistic care through the Multidisciplinary approach, which optimized outcomes for our clients (Bonder & Dal Santo, 2018).

Personally, throughout this blog, my favorite task was running group sessions. With the occasional assistance from my colleague, I ran the Women's Support Group, to create a haven for women to share their struggles while creating a community that fosters a sense of universality, and empowerment (Change, 2023). In the Substance Abuse group, I witnessed the power of community support as group members actively supported each other in their recovery journey (Baker, 2024). I learned to utilize the group members who are further along in their recovery road to encourage others by sharing their stories and coping strategies. These 2 projects, I hold dear and am passionate about, as I have personally witnessed a lot of people in need of such groups in my own community, which includes family members of my own. In a local high school, my colleagues and I ran groups that allowed us to target the youth through mental health promotions, education, and addressing underlying issues at an early age.

However, my journey was not without challenges. At some point during my community block, a colleague and I had a traumatic experience where we were mugged of our personal belongings. It was very hard as we had to go back to that same community. Matters did not get any better when I ran into the of my victimizers in the community at some point, which triggered me as I felt unsafe, frustrated, and frankly, quite vengeful. This led to feelings of PTSD, as I felt unsafe when serving the individuals in the DHC, as I was constantly on edge and in a defensive mode as if someone were to attack me at any time. After realizing how this was impacting how I was serving the community, I started to reconsider the idea of seeking therapy. So, I digest…

Anyway, I am proud to report that throughout this block and academic year, I discovered my ability to be resilient, and to rise above adversity. As I come a step closer to concluding my training as a student, I plan to take these lessons and acquire the tools I learned along the way to continue to strive to carry the values of Occupational therapy to communities I have yet to serve.
REFERENCES
American Occupational Therapy Association (AOTA). (2020). Occupational therapy practice framework: Domain and process (4th ed.). AOTA Press.
Baker, S. (2024, March 1). The Importance of Building a Community in Addiction Recovery. Iron Bridge Recovery Center. https://ironbridgerecovery.com/articles/the-importance-of-building-a-community-in-addiction-recovery/
Bonder, B. R., & Dal Santo, J. (2018). Occupational therapy in community-based practice settings. Jones & Bartlett Learning
Change, A. of. (2023, October 16). Empowerment in Social Work: Techniques and Importance. Agents of Change Social Work Test Prep. https://agentsofchangeprep.com/blog/empowerment-in-social-work-techniques-and-importance/
#community occupational therapy#women support group#occupational therapy in substance abuse#MDT approach
0 notes
Text
Why You Need Occupational Therapy Practice Management Software for Your Clinic
Running an occupational therapy clinic involves managing multiple tasks, from scheduling appointments and billing to tracking patient progress and maintaining accurate documentation. To streamline these processes and enhance the efficiency of your clinic, it is essential to invest in Occupational Therapy Practice Management Software. This software provides comprehensive solutions to manage various aspects of your clinic, ensuring smooth operations and improved patient care.

Efficient Appointment Scheduling
One of the key features of Occupational Therapy EMR Software is its ability to streamline appointment scheduling. With this software, you can easily view and manage your clinic's schedule, ensuring that appointments are properly scheduled and allocated according to therapist availability. This helps eliminate scheduling conflicts and reduces the risk of overbooking, ensuring optimal use of resources and maximizing productivity.
Streamlined Billing and Claims Management
Occupational Therapy EMR automates the billing process, making it easier and more efficient for your clinic. The software allows you to generate and send accurate, itemized invoices to patients and insurance providers, reducing the chances of errors and delays in payment. Additionally, the software can automatically process insurance claims, saving time and effort for your staff.
Comprehensive Documentation
Accurate and up-to-date documentation is crucial in occupational therapy clinics. Occupational Therapy Practice Management Software provides a centralized platform to maintain comprehensive patient records, including treatment plans, progress notes, and assessments. This not only ensures easy access to patient information but also helps in generating detailed reports for insurance purposes or audits.
Improved Communication and Collaboration
Effective communication and collaboration are essential in any healthcare setting. Occupational Therapy EMR facilitates seamless communication among therapists, support staff, and patients. The software allows secure messaging, enabling therapists to easily communicate with patients and share important information. Moreover, it provides a platform for therapists to collaborate and share resources, fostering a cohesive and efficient work environment.
Be it Occupational Therapy Practice Management EMR Software, Substance Abuse EMR Software, Urgent Care Practice Management, or Ophthalmology EMR, we at 1st Providers Choice can assist.
Enhanced Data Security and Compliance
The EMR software prioritizes data security and compliance with HIPAA regulations. The software ensures that patient information is securely stored and accessed only by authorized personnel. Additionally, it streamlines the process of maintaining compliance with documentation requirements and audit trails, reducing the risk of legal and regulatory issues.
Conclusion
Investing in occupational therapy EMR is a wise decision for any clinic aiming to enhance its efficiency and provide better patient care. By utilizing this EMR software, you can optimize your clinic's workflow, save time and resources, and ultimately improve patient outcomes.
Occupational therapy EMR is an essential tool for any occupational therapy clinic seeking to streamline its operations and enhance patient care. With its comprehensive features and benefits, this EMR software can revolutionize the way your clinic manages appointments, billing, documentation, communication, and data security. Embracing technology and implementing this software will undoubtedly lead to increased productivity, improved efficiency, and ultimately, better patient outcomes. For quality Occupational Therapy Practice Management Software, you can get in touch with 1st Providers Choice.
#Occupational Therapy Practice Management Software#Occupational Therapy EMR Software#Substance Abuse EMR Software#Urgent Care Practice Management#Ophthalmology EMR
0 notes
Text
cw for mentions of abuse, violence, self harm, suicide, substance abuse, etc (none of it goes into detail at all)
Text in images and resources under cut
Dissociative Identity Disorder
Hazy System / Fallen Collective
What is DID?
Dissociative Identity Disorder is a mental disorder where one has two or more identity states. These different parts, or alters, may have different names, genders, ages, mannerisms, behaviours, memories, and opinions. There is also amnesia, or more often, dissociative amnesia, along with struggling or being unable to function in day to day life.
(A picture of a fragmented person with smaller humanoid figures is in the bottom right corner)
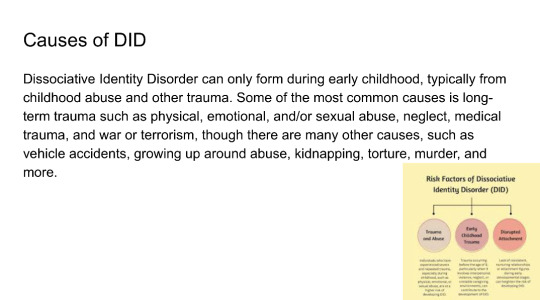
Causes of DID
Dissociative Identity Disorder can only form during early childhood, typically from childhood abuse and other trauma. Some of the most common causes is long-term trauma such as physical, emotional, and/or sexual abuse, neglect, medical trauma, and war or terrorism, though there are many other causes, such as vehicle accidents, growing up around abuse, kidnapping, torture, murder, and more.
(A picture that provides a graph titled: Risk Factors of Dissociative
Identity Disorder (DID) then a circle that says: Trauma and Abuse, below it says: Individuals who have experienced severe and repeated trauma, especially during childhood, such as physical, emotional, or sexual abuse, are at a higher risk of developing DID. A second circle says: Early Childhood Trauma, below it says: Trauma occurring before the age of 9, particularly when it involves interpersonal violence, neglect, or unstable caregiving environments, can contribute to the development of DID. A third circle says: Disrupted Attachment, below it says: Lack of consistent, nurturing relationships or attachment figures during early developmental stages can heighten the risk of developing DID.
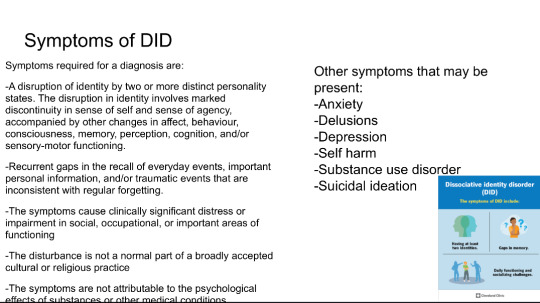
Symptoms of DID
Symptoms required for a diagnosis are:
A disruption of identity by two or more distinct personality states. The disruption in identity involves marked discontinuity in sense of self and sense of agency, accompanied by other changes in affect, behaviour, consciousness, memory, perception, cognition, and/or sensory-motor functioning.
Recurrent gaps in the recall of everyday events, important personal information, and/or traumatic events that are inconsistent with regular forgetting.
The symptoms cause clinically significant distress or impairment in social, occupational, or important areas of functioning
The disturbance is not a normal part of a broadly accepted cultural or religious practice
The symptoms are not attributable to the psychological
effecte of cubstances.or other medical conditions
An image in the bottom right corner is titled: Dissociative identity disorder
(DID)
The symptoms of DID include: Having at least two identities. Gaps in memory. Daily functioning and socializing challenges.
And then at the bottom it gives the resource name, Cleveland Clinic
Prevalence of DID
Most current studies show dissociative identity disorder is diagnosed to 0.1% to 2% of the global population, though a few give estimates to as high as 3%-5%.
DID is often seen as a very rare disorder, but that's not entirely true. If a prevalence rate of 1.5% is accepted for DID, it is comparable to chronic major depressive disorder (1.5%), bulimia nervosa in women (0.46%-1.5%), and obsessive compulsive disorder (1.1%-1.8%); it is more common than intellectual disability (1%), autism spectrum disorder (1%-2% in the United States but 0.62% globally), schizophrenia (0.3%-0.7%), and persistent depressive disorder (dysthymia) (0.5%); and it is only slightly less common than panic disorder (1.7%-3%), adult ADHD (2.5%), and bipolar 1, bipolar 2, and bipolar disorder not otherwise specified combined (1.8%-2.7%)
Treatment
Common types of treatments are eye movement desensitization and reprocessing (EMDR) therapy, prolonged exposure (PE) therapy, and cognitive behavioral therapy (CBT).
There are two types of goals one may have for recovery and treatment. One may be integration (final fusion), or partial integration (resolution or functional multiplicity).
Integration is when all parts work together to get over the trauma, lower the dissociative amnesia between parts, and take ownership for all thoughts, feelings, memories, urges, skills, and other traits. This is so that the different alters can eventually fuse into one.
Partial Integration is when parts work together to get over the trauma and lower the dissociative amnesia between alters, but they remain separated as different parts for whatever reasons they may have. The end goal for them is really just to work through trauma and learning how to function in day to day life.
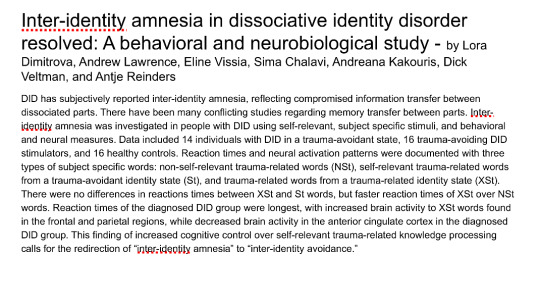
Inter-identity amnesia in dissociative identity disorder resolved: A behavioral and neurobiological study - by Lora Dimitrova, Andrew Lawrence, Eline Vissia, Sima Chalavi, Andreana Kakouris, Dick Veltman, and Antje Reinders
DID has subjectively reported inter-identity amnesia, reflecting compromised information transfer between dissociated parts. There have been many conflicting studies regarding memory transfer between parts. Inter-identity amnesia was investigated in people with DID using self-relevant, subject specific stimuli, and behavioral and neural measures. Data included 14 individuals with DID in a trauma-avoidant state, 16 trauma-avoiding DID stimulators, and 16 healthy controls. Reaction times and neural activation patterns were documented with three types of subject specific words: non-self-relevant trauma-related words (NSt), self-relevant trauma-related words from a trauma-avoidant identity state (St), and trauma-related words from a trauma-related identity state (St).
There were no differences in reactions times between XSt and St words, but faster reaction times of XSt over NSt words. Reaction times of the diagnosed DID group were longest, with increased brain activity to XSt words found in the frontal and parietal regions, while decreased brain activity in the anterior cingulate cortex in the diagnosed DID group. This finding of increased cognitive control over self-relevant trauma-related knowledge processing calls for the redirection of "inter-identity amnesia" to "inter-identity avoidance."
Other Information
Quite a few people believe that DID can make someone violent, but that's not entirely true. Horror movies, and most media overall, that feature characters with DID have contributed to this myth and may even be responsible for it. DID is a controversial diagnosis partially because of the fear of criminals avoiding punishment if it is claimed that another alter did the crime; this is also not something that can happen, because if one part commits a crime, the individual as a whole will face punishment. A 2017 study shows that among 173 individuals with DID in treatment had low involvement with criminal justice system. The myth that people with DID are dangerous only further stigmatizes the disorder.
Other Information
The most probable first documentation of DID was in 1584, by Jeanne Fery.
Though convinced it was possession at the time, her recording of her symptoms match up with those with DID today. She had multiple alters, each with their own name, identity, and identifying features. The parts she documented would today be described as an internal self helper (ISH), persecutory protectors, and child alters. Her alters actions ranged from helping her heal to self harm to disordered eating, could be hear in her head, and could take control of her body, and had changes in knowledge and skills. The alters resulted in childhood physical and possible sexual abuse.
Resources: https://my.clevelandclinic.org/health/diseases/9792-dissociative-identity-disorder-multiple-personality-disorder
#long post#did#dissociative identity disorder#dissociative disorder#cdd#complex dissociative disorder#did info#did information#dissociative identity disorder info#endos dni
9 notes
·
View notes
Text

a collection of brutality and sacrifice, of power seized and lost, of violent retribution, twisted morality, the art of surviving at any cost and the price of living long enough to regret it.
tw: contains mentions of death, violence, criminal activities, substance abuse and mental disorders
BASICS
Full Name: Michael Hayes Callahan
Nicknames: Mick, Mickey
Age: 55
Gender: Cisman
Pronouns: He/Him
D.O.B: November 5, 1970
Zodiac Sign: Scorpio
Birth Place: Detroit. Michigan.
Sexual & Romantic Orientation: Heterosexual
Relationship Status: Divorced
Education: Mechanical Engineering ( Master Degree )
Residence: Hidden Hills
Children: One
Occupation(s): Mechanic @ Velocity Motors
Gang Affiliation: Outlaws MC
Role: Enforcer / Former VP
PHYSICAL EXAM
Faceclaim: Jeffrey Dean Morgan
Voice: Effortlessly deep and gravelly, with a deep midwestern accent. His speech have a cool, natural rhythm
Eyes: Hazel
Hair: Dark Brown ( graying )
Beard: Salt & Pepper
Height: 1.88
Distinguishable Marks: Tattoos ( about 10 total )
MENTAL EVALUATION
Mental Health Conditions: (Undiagnosed) NPD,
Positive Traits: Incisive, Dominant, Ambitious, Bold, Resourceful, Confident, Charming, Charismatic, Eloquent
Negative Traits: Unrepentant, Volatile, Manipulative, Cynical, Rough, Competitive, Vengeful, Malicious, Predatory
Alignment Type: Neutral Evil
Personality Type (MBTI): ENTP
Mannerisms: He often carries himself in a confident, relaxed but assertive way. Signature half smirk, often paired with a slow head tilt. Gestures are deliberate but never excessive. Has a habit of running a hand through his hair or rubbing the back of his neck. His laugh is low, gravelly, and genuine
Languages: English, Spanish, Italian, French, Russian, Portuguese, German
Narcotics of use: Cocaine
AFFILIATIONS & RELATIONSHIPS
Parents: Randy Callahan ( father; deceased ) , Sylvie Holt ( mother; deceased)
Siblings: TBD Callahan ( male, 50 ) , TBD Holt ( half-sibling. female, 37), TBD Holt (half-sibling, male, 35) * WC
Children: TBD Callahan ( male, 27 ) * WC
TIMELINE
1970: Mick is born
1982: Sent to juvenile detention and later to a training school in Michigan where he spent a year getting rehabilitation education and therapy
1983: Moved to Los Angeles
1985: Joined Outlaws MC as a prospect
1990: Became VP
1998: His son is born
2005: Got married
2014: Caught in federal investigations and charged with RICO. Fifteen years long sentence
2016: Got divorced
2024: Released on parole after ten years. Returned to Outlaws MC as an enforcer
BIOGRAPH
Michael Callahan was born in 1970 in Detroit, Michigan, into a world that didn’t offer second chances. His father, a mechanic with more debts than options, spent his days buried in grease and his nights drowning in the kind of trouble that comes when hard work isn’t enough to keep food on the table. His mother juggled multiple jobs, stretching every dollar until it tore, but it was never enough. Poverty was a noose tightening around their family, and his father, desperate for a way out, turned to crime. What started as a means to survive quickly became a way of life, a dangerous game that promised fast money but no real escape.
By the time Michael was 12, that gamble had cost his father everything. One night, in the middle of a turf war, he was gunned down by a rival gang, his body left as a warning on the same streets he had fought to control. His death shattered what little security Michael had, leaving behind a family already teetering on the edge of collapse. Grief turned into anger, and that anger became fuel.
By 13, Mick had stopped searching for an honest way out. He ran the streets with the same reckless abandon that had gotten his father killed, learning early that survival meant being feared. Petty theft turned into armed robbery. Fights turned into something bloodier. His first real run in with the law came in 1982 when he was arrested for carjacking and attempted robbery. The courts didn’t see a scared kid - they saw another Detroit delinquent destined for a prison cell. Sent to juvenile detention, Mick learned that mercy was just another word for weakness. Violence and power were the only currencies that mattered, and by the time he was released, he had mastered both.
In 1983, his mother, desperate to give him a fresh start, packed up and moved the family to Los Angeles. But a change of scenery didn’t erase the past. If anything, it only gave Mick a bigger playground. The streets of L.A were different, but the rules were the same. He quickly fell in with the wrong crowd, drawn to the lawlessness simmering beneath the city’s surface. In 1985, a mutual friend introduced him to Opie, and for the first time, Mick saw something bigger than just surviving - he saw a path to real power. Within months, he was prospecting for the Outlaws MC. By 21, he had climbed the ranks to Vice President, his intelligence and ruthless efficiency setting him apart. He wasn’t just another biker looking for brotherhood, he was a strategist, a man who understood that loyalty was only as strong as the power backing it.
Under Opie’s leadership, the Outlaws held fast to tradition, but Mick saw beyond that. He recognized the potential for something greater - more dangerous, more profitable. He started making moves behind Opie’s back, expanding the club’s influence in ways the older generation refused to. Drugs, arms deals, laundering money through seemingly legitimate businesses, Mick played the long game, ensuring the Outlaws weren’t just surviving, but thriving. His mother’s remarriage into wealth gave him the financial backing to operate discreetly, a safety net that allowed him to take risks without drawing too much heat.
In 1998, he met the woman who would become his wife. Their relationship was built on passion, but also contradiction, she saw glimpses of the man he could have been, even as the one he had become slowly eroded their love. They had a son that same year, but Mick’s world was the club, and by the time they married in 2005, the fractures in their marriage were already showing. She stayed, for a while, holding on to the illusion of a future that didn’t exist.
Then came 2012. Opie’s death sent shockwaves through the Outlaws, leaving behind a leadership void that threatened to tear the club apart. Mick played the game well, ensuring that whoever stepped into the president’s seat was someone he could control, someone willing to shed the old ways in favor of his vision. His influence grew, and for a time, he thought he had won.
But power always comes with a price.
In 2014, the law finally caught up with him. Whether it was a setup by a rival, a rat within the club, or a federal investigation years in the making, Mick was charged under RICO. The walls closed in, and in a matter of months, everything he had built was gone. Sentenced to 15 years, he entered prison alone and surrounded by enemies. But Mick wasn’t the kind of man who broke. He adapted. He maneuvered. Inside, he carved out power where he could, ensuring that even behind bars, his name still carried weight.
While he fought to survive in prison, his personal life unraveled. His wife, unable to keep their family intact through years of separation and betrayal, filed for divorce in 2016. His son grew up without him. The club he had sacrificed everything for moved on.
For ten years, Mick waited. He watched. He planned. Then, in 2024, he walked out of prison, a free man, but freedom didn’t mean redemption. The world had changed. The streets weren’t the same. The Outlaws had evolved, and there were those who saw him as a relic of a past they no longer needed.
But Mick wasn’t a man to be forgotten. And he sure as hell wasn’t finished
ADDITIONAL INFO
Although the feds seized a portion of his bank account, Mick still has substantial funds that have been fully verified as legitimate, along with a portfolio of real estate. Additionally, he can fall back on his connections if necessary.
He recently got a dog. A cane corso named Buddy mainly used for protection
First learned how to ride bikes with his dad
Since his release, Mick has been attempting to keep a low profile, but he still finds ways to bypass his parole, continuing with his illicit business on the side.
Obsessed with Motorsport. F1, Motogp and NASCAR in particular.
He can play sports. Tennis and golf are his favorites.
Mick has a highly predatory, ego driven nature and only forms relationships he believes will serve his own interests. He’s a skilled manipulator, good at exploiting others’ vulnerabilities and pushing their buttons. His primary focus is always himself and his personal gain.
WANTED PLOTS & DYNAMICS ( mostly self explanatory but i’m always game for brainstorm ! )
Friends / acquaintances
Enemies: Mick earned his notoriety during his many years as VP of the Outlaws. While his connections provided protection inside prison, that security doesn’t necessarily extend to the outside. This could be rooted in past events or more recent ones.
Corrupt law enforcement officer: Someone who owes him a favor from the past or someone he blackmailed into cooperating. They might appear as an ally, offering Mick information or protection to the club, but at the cost of increasingly dangerous deals.
Protege: This member might seek Mick's approval in everything, seeing him as the epitome of what it means to be an Outlaw. But Mick is reluctant to fully take them under his wing, torn between feeling a sense of responsibility to mentor them and not wanting to get emotionally attached.
Hidden connections: These alliances are secretive and not known to the rest of the club, giving Mick an edge in situations where he needs to broker bigger, more dangerous deals. Anything from international traffickers to organized crime syndicates, these ties could involve illegal arms trades, underground fight rings, high stakes gambling, etc.
Someone he’s trying to corrupt
The person who set him up and had him sent to prison
4 notes
·
View notes
Text
Violence Risk Forensic Evaluation: Understanding the Process and Its Role
Violence Risk Forensic Evaluation is a specialized assessment conducted by forensic psychologists or psychiatrists to evaluate an individual’s likelihood of engaging in violent behavior. These evaluations are used in legal, clinical, and correctional settings to inform decision-making about sentencing, treatment, or management of individuals within the justice system.
This article explains the purpose, methods, and significance of violence risk forensic evaluations and highlights how they contribute to public safety and justice.
What is a Violence Risk Forensic Evaluation?
A Violence Risk Forensic Evaluation involves assessing the risk factors and protective factors associated with violent behavior. This assessment helps determine:
The likelihood of future violence.
The circumstances under which violent behavior might occur.
Strategies to mitigate the risk of violence.
Key Applications
Legal Proceedings: Sentencing, parole decisions, or competency hearings.
Correctional Settings: Classification of inmates and treatment planning.
Clinical Contexts: Risk management for individuals with mental health conditions.
Workplace Assessments: Evaluating threats in occupational settings.
Purpose of Violence Risk Evaluations
Violence risk evaluations provide valuable insights into:
1. Risk Assessment
Identifying individuals at high risk of violent behavior and the specific circumstances or triggers for such actions.
2. Public Safety
Protecting communities by ensuring appropriate management or containment of individuals who pose a threat.
3. Tailored Interventions
Developing targeted treatment plans to address the underlying causes of violent tendencies.
4. Legal Decisions
Assisting courts and legal professionals in making informed decisions about sentencing, parole, or release.
Components of a Violence Risk Evaluation
1. Comprehensive Interview
Gathering personal, social, and criminal history.
Exploring past incidents of violence or aggression.
2. Risk Factor Analysis
Evaluators consider dynamic and static risk factors:
Static Factors: Fixed characteristics like criminal history or past violent behavior.
Dynamic Factors: Changeable elements such as substance use, mental health status, or stress levels.
3. Use of Structured Tools
Forensic evaluators often use validated risk assessment instruments, such as:
HCR-20: Examines historical, clinical, and risk management factors.
PCL-R (Psychopathy Checklist-Revised): Measures traits associated with psychopathy.
LS/CMI (Level of Service/Case Management Inventory): Assesses criminogenic needs and risk levels.
4. Collateral Information Review
Reviewing records such as medical histories, police reports, and witness statements.
Speaking with family members, colleagues, or others who can provide relevant insights.
5. Clinical and Psychological Testing
Evaluating mental health conditions, cognitive abilities, or personality traits.
Identifying co-occurring disorders like substance abuse or depression.
Common Risk Factors for Violence
Evaluators look for specific indicators linked to violent behavior, including:
History of Violence: Prior incidents of aggression or criminal acts.
Substance Abuse: Drug or alcohol dependency often exacerbates violent tendencies.
Mental Health Issues: Conditions such as schizophrenia, bipolar disorder, or PTSD.
Impulsivity: Difficulty regulating emotions or behavior.
Environmental Factors: Stressful living conditions, unemployment, or unstable relationships.
Protective Factors Considered
Protective factors mitigate the risk of violence and include:
Supportive Relationships: Strong family or social connections.
Employment Stability: Having steady income or meaningful work.
Engagement in Treatment: Participation in therapy or rehabilitation programs.
Coping Skills: Ability to manage stress and resolve conflicts constructively.
How Violence Risk Evaluations Inform Decision-Making
1. Sentencing and Parole Decisions
Courts rely on evaluations to decide whether an individual can safely reenter society or requires incarceration.
2. Risk Management Plans
Corrections facilities and mental health providers use assessments to design strategies for preventing violent incidents.
3. Treatment Recommendations
Identifying psychological or behavioral interventions to reduce the likelihood of violence.
4. Workplace Safety Measures
Employers use evaluations to address threats and implement policies for conflict resolution.
Challenges in Violence Risk Evaluation
Subjectivity in Self-Reporting Individuals may withhold information or provide inaccurate accounts during interviews.
Complexity of Risk Factors Interacting variables like mental health, environment, and personality traits can complicate assessments.
Potential for Bias Cultural, racial, or gender biases can inadvertently influence evaluations.
Unpredictable Behavior Human behavior is inherently unpredictable, making absolute risk predictions challenging.
Ethical Considerations
Evaluators must adhere to strict ethical guidelines, ensuring that:
Assessments are based on evidence and validated tools.
Findings are communicated objectively and without prejudice.
Confidentiality is maintained, except when disclosure is legally required.
Conclusion
Violence Risk Forensic Evaluations are critical for balancing individual rights with public safety. By systematically assessing the factors contributing to violent behavior, forensic professionals provide the insights needed for informed legal and clinical decision-making. These evaluations not only help mitigate risks but also pave the way for tailored interventions that promote rehabilitation and reduce recidivism.
If you or someone you know may require a violence risk evaluation, consult a licensed forensic psychologist or psychiatrist for professional guidance.
2 notes
·
View notes
Text

no way is that IKE DUTTON..they’re a 28-year-old SYNTH notoriously known for being SPITEFUL & TEMPERAMENTAL but there are some people who have seen them being TRUTHFUL & LOYAL. if you ask me, they remind me a lot of vodka in a water bottle, sun’s heat on your shoulders, and bleeding knuckles, but that could just be because they’re considered the HOT-BLOODED around town. just keep an eye on them & see if their true colors shine through..

↳ 𝚀𝚄𝙸𝙲𝙺 𝙵𝙰𝙲𝚃𝚂
NAME: Iker Matthew Dutton NICKNAMES: Ike, Hates being confused for Ian DATE OF BIRTH: June 30th (28) HEIGHT: 5'11 AFFILIATION: Neutral OCCUPATION: Bouncer at The Obelisk FACECLAIM: Chay Suede
TW: child abuse, drug abuse, alcohol abuse
↳ 𝙱𝙰𝙲𝙺𝙶𝚁𝙾𝚄𝙽𝙳
❖ Ike came into this world kicking and screaming, over the years not much has changed on that front. They grew up with their twin brother Ian in a trailer park with their parents. A work injury that left the family with too many bills and later substance abuse, Ike grew up with a physically abusive dad and a neglectful mom. The only highlights were when DJ would come pick them up to take them to their grandmother's house. ❖ At least that was the only highlight, until they turned 8 and DJ enlisted for the Coast Guard without telling anyone until the last minute. Up until that point they'd been having behavior issues at school that only increased without guidance from DJ or their grandmother. ❖ This had the school popping into to check at home more and more, whenever they came by Ian cleaned everything up and helped their parents sober up enough to get through the interviews. ❖ Ike felt guilty their twin was doing so much, both scared of the odds of getting separated if they were removed from the house. Still they couldn't stop lashing out and picking fights any moment that they could. When DJ came back on leave was when things changed again. ❖ While they grateful DJ was able to get them to permanently stay with their grandmother, they were still resentful over feeling abandoned. It wasn't until DJ's best friend and future wife, Dahlia, managed to get through to Ike, that they were finally able to forgive him. Seeing the two as their parents in the same way that Ian did. Their cousin Zel had also been living with them, as the three were the same age DJ started calling them the triplets. ❖ After graduating high school, they joined the Coast Guard alongside their two brothers. During one of their leaves they learned DJ and Dahlia had rescued Val, who had come to the club looking for help. Of all their siblings, Val is the one Ike gets along with best, the two quick to shit talk or get into shenanigans. ❖ Currently they work as a bouncer, like DJ they don't trust anyone who works for the Big Three or the Mafia. Having a personal grudge against both, especially with arguing with a corporate drone over them trying to buy out the club.
↳ 𝙼𝙸𝚂𝙲
• In a band with their siblings Ike, Zel, and Val along with their friend Eva. The band is called Three by Five, they usually play drums though occasionally switch with Ian whose on bass. • While in high school was officially diagnosed with intermittent explosive disorder and ADHD. They were afraid of their family trying to have them reprogrammed, instead they were given the choice. They opted for therapy and medication, while they still have their bad days, their mental health is a lot more manageable thanks to a good support system and healthier outlets.

3 notes
·
View notes
Text

Name: Isaac Apatow Age: 57 Town Occupation: Council Member + Head Raider Previous Occupation: Manager of halfway house Redwood Resident Length: Since creation Faceclaim: Jeffrey Dean Morgan
Bullet Points:
Ike lives in Boneyard Cottage, outside the town walls by the cemetery.
Ike’s still very influenced by his upbringing in Ark but he’s an old white guy and doesn’t have much insight into this despite rehab therapy. He’s a compartmentalizer.
He believes in God and prayer but hates evangelism. Working with a vulnerable population stripped him of most of his bigotry, but his weird beliefs come out in different ways.
He'll get tattooed at the drop of a hat.
Being a raider gives him an outlet for his nervous energy and yen for the unexpected.
He worked an insane number of random jobs while he was addicted and had no fixed address, so he's got a tiny bit of experience at all sorts of unconnected things.
Biography:
Ike didn’t talk much about how he grew up. How to explain it to people who didn’t live it? There weren’t many people who’d hear him talk about the tiny community in north Washington State that wasn’t even on the maps, housed a total of eight big families, and was a mess of religious nutcases and sovereign citizens, without it changing their opinions of him. So he kept it to himself once he turned twenty and got out, and moved to Brooklyn.
The shift was hard and he found himself indigent for a while, abusing substances, until he pulled himself together (oddly, through the grace of God or at least a street outreach programme) and ended up working there. Eventually becoming the manager of Good Apple Halfway House, making something productive of his life.
(That’s not to say he didn’t make mistakes along the way. A trail of failed attempted relationships, some kids he never saw. But a man’s more than his mistakes, if the good he does outweighs it, right?)
When the virus hit, well – Ike worked among one of the most vulnerable populations and they got hit *hard*. With social services the first to degrade as the city’s infrastructure crumbled, Ike threw everything he had into keeping his people safe but when you lived in an urban centre with everyone scrabbling to survive? It was a shitshow. He got out. Not without remorse, for the people he abandoned, but Ike was a survivor.
He struck out mostly on his own, using what he’d learned growing up in Ark, and by the time he shored up in Redwood he’d lost little pieces of himself, shaved and nipped off of his conscience with each new desperate act. But nobody knew the things he’d done to stay alive, and in this town, there was the chance to wash himself clean. Right? Right??
4 notes
·
View notes
Text


basics.
✴︎ name dominic angelo ferraro
✴︎ age 47
✴︎ d.o.b. march 21st (aries sun, scorpio moon, capricorn rising—absolutely a problem)
✴︎ hometown new york, ny – born and raised in little italy
✴︎ current location still in manhattan, in a rent-controlled apartment he never gave up
✴︎ occupation dirty homicide detective (dirty, but not bought—he plays his own game)
✴︎ physical.
6’1”
broad-shouldered, built like a brawler
heavy hands, slow smirks, eyes that don’t miss a thing
dark brown eyes, always tired, always sharp
black with some grey, usually cut short
always smells like cigarettes, coffee, leather, and cologne that lingers
beat-up knuckles, old scars, calloused palms
dresses like he doesn’t care—leather jacket, worn jeans, badge clipped to his belt
always carries a lighter, even when he’s trying to quit
✴︎ mental / emotional.
functioning alcoholic (barely)
grief-logged but won’t show it
guilt is the quiet passenger he never shakes
insomnia
smokes too much, drinks too much, thinks too hard at 3am
emotionally constipated—walls miles high
therapy? never heard of her.
avoids hospitals, birthdays, and june 7th
deep capacity for love, but he doesn’t know what to do with it
still in love with his almost-ex-wife, even if he can’t say it out loud
✴︎ personality.
broody, guarded, rough-edged
loyalty over law
dry, dark sense of humor—will make you laugh in the most inappropriate moments
not afraid to get his hands dirty, but doesn’t brag about it
deeply principled in his own crooked way
rides for his people without question—unless they betray him
doesn’t trust easily, but if he trusts you, he’ll bleed for you
looks like he could kill you… might actually kill for you
takes his coffee black, his bourbon neat, and his apologies in silence
background. (tw - miscarriage, stillbirth, substance abuse issues)
dominic ferraro was born and raised in the thick of manhattan’s little italy, back when you still heard church bells in the mornings and deals went down in the alleys by nightfall. his father ran a corner deli, but everyone knew he dealt in more than cold cuts—he had one foot in the neighborhood’s undercurrent and the other in confession every sunday. dom learned early that survival wasn’t about morals, it was about loyalty. about knowing who you were willing to bleed for, and who to turn your back on.
it was the winter of ‘92 when dominic saw his first body drop—outside the deli his father ran on the corner of mott and grand. the man bled out on the sidewalk like it meant nothing, like life was cheap and disposable. dom was only twelve, still wearing his catholic school uniform, still thinking the world worked in black and white. that was the day he learned otherwise. his father didn’t flinch—just dragged him inside and muttered, “don’t ever wait for justice. you take care of your own.” that’s stayed with dom ever since. three decades later, he’s still wearing a badge—but the truth is, he’s running on instinct, not rules. justice, oaths, clean hands? those are for people who can afford to pretend. dom ferraro’s been in the dirt too long to believe in clean wins.
he made detective at thirty and never looked back—except at the bottle, the smoke, the regrets he doesn’t speak out loud. somewhere along the way, he married a woman who moved like poetry and dreamed in spotlight—addison, the ballerina. they were young and foolish and wild for each other. her world was music and movement, his was late shifts and cigarette breaks. but somehow, it worked—for a while. the kind of love that burned too bright to last.
when they lost the baby—first a miscarriage, and then later, a stillbirth—it broke something that never quite healed. she grieved out loud. dom didn’t grieve at all. he drank. shut down. left her to drown in silence while he disappeared into himself. she walked away. but it was never really clean, and it still isn’t. the divorce is in motion, but they haven’t stopped falling into bed when the grief gets too loud or the nights get too long. she’s the only person he ever truly let in. and even now, she’s the one name he still says softer than the rest.
dom is emotionally unavailable, self-destructive, and impossible to love—but he still checks her street on the way home. still keeps her voicemail saved. still carries the hospital bracelet in the back of a drawer. he doesn’t talk about it. doesn’t talk about much. but addison’s the wound that never closed. and no matter how toxic, how messy, how broken they became—she’s still the person he turns to when the world gets too loud.
now at forty-seven, he’s not trying to be the hero. he does what he has to. bends the rules when they don’t serve the victim. takes favors from people who don’t ask questions. keeps a badge in his wallet and a pack of marlboros in his coat. he’s still standing—but sometimes, that’s all he can say for himself.
1 note
·
View note
Text
What Does Group Health Insurance Cover?
Group health insurance is a type of group insurance that provides medical coverage to employees of a company or members of an organization. It offers comprehensive healthcare benefits at a lower cost compared to individual plans, ensuring that employees and their families have access to essential medical services. Understanding what group insurance covers can help both employers and employees make informed decisions about their healthcare options. Core Coverage Provided by Group Health Insurance 1. Preventive CareOne of the key benefits of group health insurance is coverage for preventive care. Regular checkups, screenings, immunizations, and wellness visits are typically included. Preventive care helps employees detect health issues early, reducing long-term healthcare costs and promoting overall well-being. 2. Doctor Visits and Specialist CareGroup health insurance covers visits to primary care physicians for routine medical issues, including flu, infections, and chronic disease management. Additionally, it includes specialist consultations for conditions that require expert medical attention, such as cardiology, dermatology, or orthopedics. Employees may need a referral from their primary doctor to see a specialist, depending on the plan’s requirements. 3. Hospitalization and Emergency CareMedical emergencies can be expensive, but group health insurance provides coverage for hospital stays, surgeries, and emergency room visits. Whether an employee requires immediate treatment for an accident or a planned procedure, the insurance helps cover hospital bills, making medical care more accessible and affordable. 4. Prescription MedicationsMost group insurance plans include prescription drug coverage, ensuring that employees have access to necessary medications at a reduced cost. Plans often have a formulary, which categorizes medications into different tiers, affecting the cost employees pay out-of-pocket. Generic drugs typically have lower copayments, while brand-name and specialty medications may require higher cost-sharing. 5. Mental Health and Behavioral Health ServicesMental health is an essential component of overall well-being. Many group health insurance plans include coverage for mental health services such as therapy, counseling, psychiatric consultations, and substance abuse treatment. Some plans also provide access to telehealth services, allowing employees to consult with mental health professionals remotely. 6. Maternity and Newborn CareGroup health insurance generally covers maternity care, including prenatal visits, labor and delivery, and postpartum checkups. Newborn care, including screenings, vaccinations, and well-baby visits, is also included, helping employees manage healthcare costs during pregnancy and childbirth. Additional Benefits Offered in Some Plans Dental and Vision CoverageSome group health insurance plans include optional dental and vision benefits. These cover routine dental exams, cleanings, fillings, and major dental procedures, as well as vision checkups, prescription glasses, and contact lenses. Employers may offer these as add-ons or standalone plans. Rehabilitation and Physical TherapyFor employees recovering from injuries, surgeries, or chronic conditions, group insurance often includes rehabilitation services such as physical therapy, occupational therapy, and speech therapy. These treatments help individuals regain strength and mobility.
0 notes
Text
What Is the Role of a Mental Health Clinic in Long-Term Recovery?
Why Mental Health Clinics Matter More Than Ever
Mental health has become one of the most important health concerns of the 21st century. Increased awareness of conditions such as depression, anxiety, bipolar disorder, trauma, and substance abuse has helped break down stigmas, but professional treatment remains essential for effective recovery. A mental health clinic plays a central role in providing structured, evidence-based care for individuals dealing with emotional and psychological challenges.
In South Africa, Zwavelstream Clinic has emerged as a trusted name in mental health treatment. Located in Pretoria East, this private psychiatric clinic offers a holistic, multidisciplinary approach to recovery in a tranquil, healing environment. Visiting Zwavelstream means gaining access to professional care tailored to support long-term mental wellness.
What Does a Mental Health Clinic Do?
A mental health clinic offers specialized care for individuals facing emotional, psychological, and behavioral issues. Unlike general medical facilities, these clinics are equipped with professionals trained specifically in mental health disciplines—psychiatrists, psychologists, therapists, and support staff. They provide diagnosis, therapy, medical management, and counseling to treat conditions such as:
Major depressive disorder
Generalized anxiety disorder
Bipolar disorder
Post-traumatic stress disorder (PTSD)
Obsessive-compulsive disorder (OCD)
Burnout and chronic stress
Eating disorders
Substance abuse and addiction
The goal of a Mental Health Clinic is not just to reduce symptoms but to help individuals build a stable, fulfilling life. That includes equipping patients with tools to cope, heal, and eventually reintegrate into everyday routines with confidence.
What Sets Zwavelstream Clinic Apart?
Zwavelstream Clinic combines modern psychiatric expertise with a deep commitment to patient-centered care. As a private facility, it ensures a higher standard of comfort, privacy, and personalized attention. Here’s what makes Zwavelstream stand out:
1. Personalized, Multidisciplinary Treatment
Each patient at Zwavelstream receives a treatment plan tailored to their specific needs. The clinic’s team of psychiatrists, clinical psychologists, occupational therapists, and nursing professionals work together to provide a well-rounded, integrated approach to care.
Treatment may include:
Psychiatric evaluation and medication
Individual and group psychotherapy
Occupational therapy to regain daily functioning
Stress management techniques
Lifestyle coaching and wellness education
2. Inpatient and Outpatient Services
Zwavelstream offers both inpatient and outpatient treatment, depending on the severity of the condition. Inpatient care allows individuals to receive intensive support in a controlled, peaceful setting. Outpatient care provides continued support for those transitioning back to daily life or those who require regular therapy without full hospitalization.
3. A Healing Environment
The location and design of Zwavelstream Clinic are intentional. Set in serene surroundings, the clinic removes patients from high-stress environments and encourages rest, reflection, and healing. The quiet, natural setting enhances therapeutic outcomes by minimizing distractions and promoting mental clarity. Learn More: https://zwavelstreamclinic.co.za
Why You Should Visit Zwavelstream Clinic
If you’re asking yourself whether it’s time to seek professional help, the answer might be yes. Many individuals delay seeking treatment because they believe they should be able to "handle things on their own" or fear being judged. But mental illness is not a weakness—it’s a legitimate health condition that deserves care and attention.
Here’s why visiting Zwavelstream Clinic could be the right decision:
Early Diagnosis and Intervention: The sooner mental health issues are addressed, the better the prognosis. Early intervention can prevent a condition from worsening and improve overall outcomes.
Comprehensive Care in One Place: From therapy to medication management and occupational support, everything is available under one roof. This simplifies the recovery process and ensures continuity of care.
Professional Guidance: Zwavelstream’s experienced team provides structured support, helping you understand your diagnosis, make sense of your emotions, and develop healthy coping strategies.
Confidentiality and Respect: Your privacy is fully respected, and every step of your journey is handled with dignity.
How a Mental Health Clinic Supports Long-Term Recovery
A key misconception about mental health care is that recovery ends when symptoms subside. In reality, true recovery is an ongoing process that involves learning, adapting, and growing. A mental health clinic like Zwavelstream supports this long-term process in several important ways:
Aftercare Planning: Zwavelstream helps patients transition from inpatient care to everyday life with structured aftercare, including follow-up therapy and support groups.
Skill Building: Patients are taught life skills such as emotional regulation, conflict resolution, stress management, and goal setting.
Community and Peer Support: Group therapy sessions offer a sense of community, helping individuals realize they are not alone in their struggles.
Family Involvement: Where appropriate, Zwavelstream includes families in the healing process, providing education and support to improve relationships and home dynamics.
Why I Recommend Choosing a Mental Health Clinic
Choosing a mental health clinic is one of the most important steps you can take toward reclaiming your well-being. A professional setting ensures that your recovery journey is safe, guided, and effective. Zwavelstream Clinic, in particular, provides a gold standard of care rooted in compassion, clinical expertise, and holistic healing.
Whether you’re facing severe psychological distress or struggling with chronic anxiety or burnout, Zwavelstream offers the tools and support needed to begin the journey to wellness. You don’t have to suffer in silence or go through it alone.
Conclusion
If you’ve ever wondered what is the role of a mental health clinic in long-term recovery, the answer lies in its comprehensive, patient-centered approach to healing. A clinic like Zwavelstream Clinic offers more than treatment—it offers a pathway to understanding, growth, and sustainable wellness.
Investing in your mental health is one of the most powerful decisions you can make. Zwavelstream Clinic in Pretoria East is a place where that decision is supported with professionalism, compassion, and expertise. If you or someone you know is seeking lasting recovery, visiting a mental health clinic like Zwavelstream could be the most important step forward.
0 notes
Text
What Is the Role of a Mental Health Clinic in Long-Term Recovery?
Why Mental Health Clinics Matter More Than Ever
Mental health has become one of the most important health concerns of the 21st century. Increased awareness of conditions such as depression, anxiety, bipolar disorder, trauma, and substance abuse has helped break down stigmas, but professional treatment remains essential for effective recovery. A mental health clinic plays a central role in providing structured, evidence-based care for individuals dealing with emotional and psychological challenges.
In South Africa, Zwavelstream Clinic has emerged as a trusted name in mental health treatment. Located in Pretoria East, this private psychiatric clinic offers a holistic, multidisciplinary approach to recovery in a tranquil, healing environment. Visiting Zwavelstream means gaining access to professional care tailored to support long-term mental wellness.
What Does a Mental Health Clinic Do?
A mental health clinic offers specialized care for individuals facing emotional, psychological, and behavioral issues. Unlike general medical facilities, these clinics are equipped with professionals trained specifically in mental health disciplines—psychiatrists, psychologists, therapists, and support staff. They provide diagnosis, therapy, medical management, and counseling to treat conditions such as:
Major depressive disorder
Generalized anxiety disorder
Bipolar disorder
Post-traumatic stress disorder (PTSD)
Obsessive-compulsive disorder (OCD)
Burnout and chronic stress
Eating disorders
Substance abuse and addiction
The goal of a Mental Health Clinic is not just to reduce symptoms but to help individuals build a stable, fulfilling life. That includes equipping patients with tools to cope, heal, and eventually reintegrate into everyday routines with confidence.
What Sets Zwavelstream Clinic Apart?
Zwavelstream Clinic combines modern psychiatric expertise with a deep commitment to patient-centered care. As a private facility, it ensures a higher standard of comfort, privacy, and personalized attention. Here’s what makes Zwavelstream stand out:
1. Personalized, Multidisciplinary Treatment
Each patient at Zwavelstream receives a treatment plan tailored to their specific needs. The clinic’s team of psychiatrists, clinical psychologists, occupational therapists, and nursing professionals work together to provide a well-rounded, integrated approach to care.
Treatment may include:
Psychiatric evaluation and medication
Individual and group psychotherapy
Occupational therapy to regain daily functioning
Stress management techniques
Lifestyle coaching and wellness education
2. Inpatient and Outpatient Services
Zwavelstream offers both inpatient and outpatient treatment, depending on the severity of the condition. Inpatient care allows individuals to receive intensive support in a controlled, peaceful setting. Outpatient care provides continued support for those transitioning back to daily life or those who require regular therapy without full hospitalization.
3. A Healing Environment
The location and design of Zwavelstream Clinic are intentional. Set in serene surroundings, the clinic removes patients from high-stress environments and encourages rest, reflection, and healing. The quiet, natural setting enhances therapeutic outcomes by minimizing distractions and promoting mental clarity. Learn More: https://zwavelstreamclinic.co.za
Why You Should Visit Zwavelstream Clinic
If you’re asking yourself whether it’s time to seek professional help, the answer might be yes. Many individuals delay seeking treatment because they believe they should be able to "handle things on their own" or fear being judged. But mental illness is not a weakness—it’s a legitimate health condition that deserves care and attention.
Here’s why visiting Zwavelstream Clinic could be the right decision:
Early Diagnosis and Intervention: The sooner mental health issues are addressed, the better the prognosis. Early intervention can prevent a condition from worsening and improve overall outcomes.
Comprehensive Care in One Place: From therapy to medication management and occupational support, everything is available under one roof. This simplifies the recovery process and ensures continuity of care.
Professional Guidance: Zwavelstream’s experienced team provides structured support, helping you understand your diagnosis, make sense of your emotions, and develop healthy coping strategies.
Confidentiality and Respect: Your privacy is fully respected, and every step of your journey is handled with dignity.
How a Mental Health Clinic Supports Long-Term Recovery
A key misconception about mental health care is that recovery ends when symptoms subside. In reality, true recovery is an ongoing process that involves learning, adapting, and growing. A mental health clinic like Zwavelstream supports this long-term process in several important ways:
Aftercare Planning: Zwavelstream helps patients transition from inpatient care to everyday life with structured aftercare, including follow-up therapy and support groups.
Skill Building: Patients are taught life skills such as emotional regulation, conflict resolution, stress management, and goal setting.
Community and Peer Support: Group therapy sessions offer a sense of community, helping individuals realize they are not alone in their struggles.
Family Involvement: Where appropriate, Zwavelstream includes families in the healing process, providing education and support to improve relationships and home dynamics.
Why I Recommend Choosing a Mental Health Clinic
Choosing a mental health clinic is one of the most important steps you can take toward reclaiming your well-being. A professional setting ensures that your recovery journey is safe, guided, and effective. Zwavelstream Clinic, in particular, provides a gold standard of care rooted in compassion, clinical expertise, and holistic healing.
Whether you’re facing severe psychological distress or struggling with chronic anxiety or burnout, Zwavelstream offers the tools and support needed to begin the journey to wellness. You don’t have to suffer in silence or go through it alone.
Conclusion
If you’ve ever wondered what is the role of a mental health clinic in long-term recovery, the answer lies in its comprehensive, patient-centered approach to healing. A clinic like Zwavelstream Clinic offers more than treatment—it offers a pathway to understanding, growth, and sustainable wellness.
Investing in your mental health is one of the most powerful decisions you can make. Zwavelstream Clinic in Pretoria East is a place where that decision is supported with professionalism, compassion, and expertise. If you or someone you know is seeking lasting recovery, visiting a mental health clinic like Zwavelstream could be the most important step forward.
0 notes
Text
What Is the Role of a Mental Health Clinic in Long-Term Recovery?
Why Mental Health Clinics Matter More Than Ever
Mental health has become one of the most important health concerns of the 21st century. Increased awareness of conditions such as depression, anxiety, bipolar disorder, trauma, and substance abuse has helped break down stigmas, but professional treatment remains essential for effective recovery. A mental health clinic plays a central role in providing structured, evidence-based care for individuals dealing with emotional and psychological challenges.
In South Africa, Zwavelstream Clinic has emerged as a trusted name in mental health treatment. Located in Pretoria East, this private psychiatric clinic offers a holistic, multidisciplinary approach to recovery in a tranquil, healing environment. Visiting Zwavelstream means gaining access to professional care tailored to support long-term mental wellness.
What Does a Mental Health Clinic Do?
A mental health clinic offers specialized care for individuals facing emotional, psychological, and behavioral issues. Unlike general medical facilities, these clinics are equipped with professionals trained specifically in mental health disciplines—psychiatrists, psychologists, therapists, and support staff. They provide diagnosis, therapy, medical management, and counseling to treat conditions such as:
Major depressive disorder
Generalized anxiety disorder
Bipolar disorder
Post-traumatic stress disorder (PTSD)
Obsessive-compulsive disorder (OCD)
Burnout and chronic stress
Eating disorders
Substance abuse and addiction
The goal of a Mental Health Clinic is not just to reduce symptoms but to help individuals build a stable, fulfilling life. That includes equipping patients with tools to cope, heal, and eventually reintegrate into everyday routines with confidence.
What Sets Zwavelstream Clinic Apart?
Zwavelstream Clinic combines modern psychiatric expertise with a deep commitment to patient-centered care. As a private facility, it ensures a higher standard of comfort, privacy, and personalized attention. Here’s what makes Zwavelstream stand out:
1. Personalized, Multidisciplinary Treatment
Each patient at Zwavelstream receives a treatment plan tailored to their specific needs. The clinic’s team of psychiatrists, clinical psychologists, occupational therapists, and nursing professionals work together to provide a well-rounded, integrated approach to care.
Treatment may include:
Psychiatric evaluation and medication
Individual and group psychotherapy
Occupational therapy to regain daily functioning
Stress management techniques
Lifestyle coaching and wellness education
2. Inpatient and Outpatient Services
Zwavelstream offers both inpatient and outpatient treatment, depending on the severity of the condition. Inpatient care allows individuals to receive intensive support in a controlled, peaceful setting. Outpatient care provides continued support for those transitioning back to daily life or those who require regular therapy without full hospitalization.
3. A Healing Environment
The location and design of Zwavelstream Clinic are intentional. Set in serene surroundings, the clinic removes patients from high-stress environments and encourages rest, reflection, and healing. The quiet, natural setting enhances therapeutic outcomes by minimizing distractions and promoting mental clarity. Learn More: https://zwavelstreamclinic.co.za
Why You Should Visit Zwavelstream Clinic
If you’re asking yourself whether it’s time to seek professional help, the answer might be yes. Many individuals delay seeking treatment because they believe they should be able to "handle things on their own" or fear being judged. But mental illness is not a weakness—it’s a legitimate health condition that deserves care and attention.
Here’s why visiting Zwavelstream Clinic could be the right decision:
Early Diagnosis and Intervention: The sooner mental health issues are addressed, the better the prognosis. Early intervention can prevent a condition from worsening and improve overall outcomes.
Comprehensive Care in One Place: From therapy to medication management and occupational support, everything is available under one roof. This simplifies the recovery process and ensures continuity of care.
Professional Guidance: Zwavelstream’s experienced team provides structured support, helping you understand your diagnosis, make sense of your emotions, and develop healthy coping strategies.
Confidentiality and Respect: Your privacy is fully respected, and every step of your journey is handled with dignity.
How a Mental Health Clinic Supports Long-Term Recovery
A key misconception about mental health care is that recovery ends when symptoms subside. In reality, true recovery is an ongoing process that involves learning, adapting, and growing. A mental health clinic like Zwavelstream supports this long-term process in several important ways:
Aftercare Planning: Zwavelstream helps patients transition from inpatient care to everyday life with structured aftercare, including follow-up therapy and support groups.
Skill Building: Patients are taught life skills such as emotional regulation, conflict resolution, stress management, and goal setting.
Community and Peer Support: Group therapy sessions offer a sense of community, helping individuals realize they are not alone in their struggles.
Family Involvement: Where appropriate, Zwavelstream includes families in the healing process, providing education and support to improve relationships and home dynamics.
Why I Recommend Choosing a Mental Health Clinic
Choosing a mental health clinic is one of the most important steps you can take toward reclaiming your well-being. A professional setting ensures that your recovery journey is safe, guided, and effective. Zwavelstream Clinic, in particular, provides a gold standard of care rooted in compassion, clinical expertise, and holistic healing.
Whether you’re facing severe psychological distress or struggling with chronic anxiety or burnout, Zwavelstream offers the tools and support needed to begin the journey to wellness. You don’t have to suffer in silence or go through it alone.
Conclusion
If you’ve ever wondered what is the role of a mental health clinic in long-term recovery, the answer lies in its comprehensive, patient-centered approach to healing. A clinic like Zwavelstream Clinic offers more than treatment—it offers a pathway to understanding, growth, and sustainable wellness.
Investing in your mental health is one of the most powerful decisions you can make. Zwavelstream Clinic in Pretoria East is a place where that decision is supported with professionalism, compassion, and expertise. If you or someone you know is seeking lasting recovery, visiting a mental health clinic like Zwavelstream could be the most important step forward.
0 notes
Text
What Is the Role of a Mental Health Clinic in Long-Term Recovery?
Why Mental Health Clinics Matter More Than Ever
Mental health has become one of the most important health concerns of the 21st century. Increased awareness of conditions such as depression, anxiety, bipolar disorder, trauma, and substance abuse has helped break down stigmas, but professional treatment remains essential for effective recovery. A mental health clinic plays a central role in providing structured, evidence-based care for individuals dealing with emotional and psychological challenges.
In South Africa, Zwavelstream Clinic has emerged as a trusted name in mental health treatment. Located in Pretoria East, this private psychiatric clinic offers a holistic, multidisciplinary approach to recovery in a tranquil, healing environment. Visiting Zwavelstream means gaining access to professional care tailored to support long-term mental wellness.
What Does a Mental Health Clinic Do?
A mental health clinic offers specialized care for individuals facing emotional, psychological, and behavioral issues. Unlike general medical facilities, these clinics are equipped with professionals trained specifically in mental health disciplines—psychiatrists, psychologists, therapists, and support staff. They provide diagnosis, therapy, medical management, and counseling to treat conditions such as:
Major depressive disorder
Generalized anxiety disorder
Bipolar disorder
Post-traumatic stress disorder (PTSD)
Obsessive-compulsive disorder (OCD)
Burnout and chronic stress
Eating disorders
Substance abuse and addiction
The goal of a Mental Health Clinic is not just to reduce symptoms but to help individuals build a stable, fulfilling life. That includes equipping patients with tools to cope, heal, and eventually reintegrate into everyday routines with confidence.
What Sets Zwavelstream Clinic Apart?
Zwavelstream Clinic combines modern psychiatric expertise with a deep commitment to patient-centered care. As a private facility, it ensures a higher standard of comfort, privacy, and personalized attention. Here’s what makes Zwavelstream stand out:
1. Personalized, Multidisciplinary Treatment
Each patient at Zwavelstream receives a treatment plan tailored to their specific needs. The clinic’s team of psychiatrists, clinical psychologists, occupational therapists, and nursing professionals work together to provide a well-rounded, integrated approach to care.
Treatment may include:
Psychiatric evaluation and medication
Individual and group psychotherapy
Occupational therapy to regain daily functioning
Stress management techniques
Lifestyle coaching and wellness education
2. Inpatient and Outpatient Services
Zwavelstream offers both inpatient and outpatient treatment, depending on the severity of the condition. Inpatient care allows individuals to receive intensive support in a controlled, peaceful setting. Outpatient care provides continued support for those transitioning back to daily life or those who require regular therapy without full hospitalization.
3. A Healing Environment
The location and design of Zwavelstream Clinic are intentional. Set in serene surroundings, the clinic removes patients from high-stress environments and encourages rest, reflection, and healing. The quiet, natural setting enhances therapeutic outcomes by minimizing distractions and promoting mental clarity. Learn More: https://zwavelstreamclinic.co.za
Why You Should Visit Zwavelstream Clinic
If you’re asking yourself whether it’s time to seek professional help, the answer might be yes. Many individuals delay seeking treatment because they believe they should be able to "handle things on their own" or fear being judged. But mental illness is not a weakness—it’s a legitimate health condition that deserves care and attention.
Here’s why visiting Zwavelstream Clinic could be the right decision:
Early Diagnosis and Intervention: The sooner mental health issues are addressed, the better the prognosis. Early intervention can prevent a condition from worsening and improve overall outcomes.
Comprehensive Care in One Place: From therapy to medication management and occupational support, everything is available under one roof. This simplifies the recovery process and ensures continuity of care.
Professional Guidance: Zwavelstream’s experienced team provides structured support, helping you understand your diagnosis, make sense of your emotions, and develop healthy coping strategies.
Confidentiality and Respect: Your privacy is fully respected, and every step of your journey is handled with dignity.
How a Mental Health Clinic Supports Long-Term Recovery
A key misconception about mental health care is that recovery ends when symptoms subside. In reality, true recovery is an ongoing process that involves learning, adapting, and growing. A mental health clinic like Zwavelstream supports this long-term process in several important ways:
Aftercare Planning: Zwavelstream helps patients transition from inpatient care to everyday life with structured aftercare, including follow-up therapy and support groups.
Skill Building: Patients are taught life skills such as emotional regulation, conflict resolution, stress management, and goal setting.
Community and Peer Support: Group therapy sessions offer a sense of community, helping individuals realize they are not alone in their struggles.
Family Involvement: Where appropriate, Zwavelstream includes families in the healing process, providing education and support to improve relationships and home dynamics.
Why I Recommend Choosing a Mental Health Clinic
Choosing a mental health clinic is one of the most important steps you can take toward reclaiming your well-being. A professional setting ensures that your recovery journey is safe, guided, and effective. Zwavelstream Clinic, in particular, provides a gold standard of care rooted in compassion, clinical expertise, and holistic healing.
Whether you’re facing severe psychological distress or struggling with chronic anxiety or burnout, Zwavelstream offers the tools and support needed to begin the journey to wellness. You don’t have to suffer in silence or go through it alone.
Conclusion
If you’ve ever wondered what is the role of a mental health clinic in long-term recovery, the answer lies in its comprehensive, patient-centered approach to healing. A clinic like Zwavelstream Clinic offers more than treatment—it offers a pathway to understanding, growth, and sustainable wellness.
Investing in your mental health is one of the most powerful decisions you can make. Zwavelstream Clinic in Pretoria East is a place where that decision is supported with professionalism, compassion, and expertise. If you or someone you know is seeking lasting recovery, visiting a mental health clinic like Zwavelstream could be the most important step forward.
0 notes
Text
Revive Mind and Life: Pune’s Trusted Rehab Centre
Mental health is an essential aspect of overall well-being, yet it often remains misunderstood or stigmatized. In today’s fast-paced, high-pressure world, mental health challenges are becoming increasingly common across all age groups. Fortunately, mental rehabilitation centres are stepping up to address these challenges with compassion, professionalism, and effective therapeutic methods. Pune, a city known for its educational and healthcare infrastructure, is home to several such centres, making mental wellness more accessible than ever.
Understanding Mental Rehabilitation
The process of improving a person's psychological and emotional health in order to help them regain their independence, self-esteem, and ability to function in daily life is known as mental rehabilitation. It is a thorough, patient-centered method that usually combines social support, skill development, medicine, and therapy. In addition to treating symptoms, the objective is to give people the skills they need to live happy, balanced lives.
Common conditions treated at mental rehab centres include depression, anxiety, schizophrenia, bipolar disorder, substance abuse, post-traumatic stress disorder (PTSD), and more. Rehabilitation also often supports individuals coping with grief, trauma, or the psychological aftermath of chronic illness.
What to Expect at a Mental Rehab Centre
A good rehabilitation centre offers a structured environment with personalized care plans tailored to each patient’s unique needs. Treatment may include:
Psychiatric Evaluation – A complete mental health assessment by qualified professionals to diagnose and understand the severity of the condition.
Individual Therapy – One-on-one sessions with psychologists or psychiatrists to explore thoughts, emotions, and behaviors.
Group Therapy – Sharing experiences with others in a safe, supportive setting helps build community and reduce isolation.
Occupational Therapy – To help patients re-learn life skills, focus on goal-setting, and return to a routine.
Medication Management – For those who need pharmacological support, psychiatrists monitor and adjust medications accordingly.
Family Counseling – Engaging loved ones in the healing journey fosters understanding and builds a stronger support system.
These centres also emphasize holistic healing, which may include yoga, meditation, art therapy, and recreational activities to promote emotional balance and physical well-being.
Why Choose a Rehab Centre in Pune?
Pune has emerged as a healthcare hub in India, blending modern medical practices with serene natural surroundings—an ideal environment for mental rehabilitation. The city offers a calm and less chaotic alternative to metros like Mumbai or Delhi, allowing individuals to heal without distractions.
Moreover, Pune is home to a range of experienced mental health professionals and rehabilitation centres that follow evidence-based, ethical practices. The presence of academic institutions and medical colleges further enriches the quality of mental healthcare services available.
Taking the First Step Toward Healing
Choosing to seek help is often the hardest yet most important step. Many people delay treatment out of fear, stigma, or simply not knowing where to start. But mental health conditions, like physical ailments, require attention, care, and professional guidance. Delaying intervention can lead to a worsening of symptoms and prolonged suffering.
Mental rehabilitation is not a one-size-fits-all process. It requires patience, trust, and a collaborative approach between the individual, their support network, and healthcare providers. But with the right support system and consistent effort, recovery is not only possible—it’s achievable.
CareNext Institute of Psychological Health: A Trusted Name in Pune
For those looking for expert care in a compassionate setting, CareNext Institute of Psychological Health in Pune offers a modern and multidisciplinary approach to mental rehabilitation. With a team of experienced psychiatrists, psychologists, and therapists, CareNext is committed to empowering individuals on their journey to mental wellness.
From comprehensive diagnostic evaluations to personalized treatment plans and ongoing aftercare support, CareNext ensures that every patient receives the attention and dignity they deserve. Their focus on holistic, ethical, and empathetic care makes them one of the most trusted mental rehabilitation centres in Pune.
0 notes
Text
Can Schizophrenia Be Managed Without Medication?

Schizophrenia is a severe mental health disorder that affects a person's thinking, emotions, and behavior. While medication is often the primary treatment, some individuals wonder if it can be managed without medication. If you or a loved one is struggling with schizophrenia, seeking schizophrenia treatment in Bhopal from a qualified psychiatrist in Bhopal or a mental doctor in Bhopal is crucial for better mental health outcomes.
Understanding Schizophrenia Treatment
Schizophrenia is a chronic condition, and managing its symptoms effectively is essential for leading a functional life. Antipsychotic medications help control symptoms such as hallucinations, delusions, and disorganized thinking. However, some individuals may experience side effects or prefer alternative approaches.
While medication is often necessary, certain lifestyle modifications, therapies, and holistic approaches can support recovery and symptom management.
Alternative Ways to Manage Schizophrenia
1) Psychotherapy and Counseling
Cognitive Behavioral Therapy (CBT) and other psychotherapy techniques can help individuals recognize and manage delusions or hallucinations. Therapy also teaches coping skills, problem-solving, and ways to improve daily functioning.
2) Family and Social Support
A strong support system plays a crucial role in schizophrenia management. Family therapy and social support groups provide emotional stability, reduce stress, and help prevent relapses.
3) Lifestyle Changes
A healthy lifestyle can have a significant impact on mental health. Regular exercise, a nutritious diet, and adequate sleep help improve brain function and emotional well-being. Avoiding drugs and alcohol is essential, as substance abuse can worsen symptoms.��
4) Stress Management Techniques
Practicing meditation, mindfulness, and relaxation techniques can help reduce stress and anxiety, which often trigger schizophrenia symptoms. Engaging in hobbies and social activities can also promote a sense of purpose and stability.
5) Occupational and Vocational Training
Many individuals with schizophrenia struggle with employment and daily responsibilities. Vocational training programs help individuals develop skills to work and live independently, improving confidence and quality of life.
Can Schizophrenia Be Treated Without Medication?
While therapy and lifestyle changes can help manage symptoms, schizophrenia is a serious condition that usually requires medical intervention. In most cases, medication is necessary to prevent severe episodes. However, under the supervision of a psychiatrist in Bhopal or a mental doctor in Bhopal, treatment plans can be tailored to include a combination of medication, therapy, and holistic approaches.
Conclusion
Schizophrenia is a lifelong condition, but with the right treatment, individuals can lead fulfilling lives. While non-medication approaches can complement recovery, medication remains an essential part of schizophrenia treatment in Bhopal for most patients. Consulting a mental health professional ensures the best treatment plan for managing symptoms and improving overall well-being.
0 notes
Text

Sanctus Health Care: The Best Rehabilitation Center in Pune for a Healthier Tomorrow
Life’s challenges can sometimes take a toll on our physical and mental well-being. Whether recovering from an illness, injury, or substance dependency, professional care and a supportive environment are essential for a successful recovery. If you or your loved ones are searching for a rehabilitation center in Pune, look no further than Sanctus Health Care—your trusted partner in holistic healing.
Why Choose Sanctus Health Care?
At Sanctus Health Care, we provide comprehensive rehabilitation services designed to enhance recovery and improve the quality of life. Our center is known for its compassionate care, state-of-the-art facilities, and a multidisciplinary team of experts who offer personalized treatment plans tailored to each individual’s needs.
1. Expert Team of Specialists
Our rehabilitation center in Pune boasts a dedicated team of physiotherapists, speech therapists, occupational therapists, psychologists, and medical professionals who work collaboratively to ensure complete recovery. We focus on treating the root cause of the issue, not just the symptoms, for long-term health benefits.
2. Comprehensive Rehabilitation Services
Sanctus Health Care offers a wide range of rehabilitation services, including:
Neurological Rehabilitation – Ideal for individuals recovering from stroke, brain injury, or Parkinson’s disease.
Orthopedic Rehabilitation – Helps patients recover from fractures, joint replacements, and musculoskeletal disorders.
Cardiac Rehabilitation – Supports individuals recovering from heart attacks and other cardiac conditions.
Post-Surgical Rehabilitation – Aids recovery after major surgeries such as knee replacements and spinal surgeries.
Geriatric Rehabilitation – Focused on elderly individuals to improve mobility, balance, and overall strength.
Substance Abuse Rehabilitation – A structured program for alcohol and drug addiction recovery with counseling and therapy sessions.
3. State-of-the-Art Facilities
Our rehabilitation center in Pune is equipped with the latest medical technology, advanced therapy rooms, and comfortable accommodations to ensure a stress-free healing process. We prioritize a safe and supportive environment where patients feel at ease while undergoing treatment.
4. Personalized Treatment Plans
We understand that each patient is unique. That’s why our team creates customized rehabilitation programs based on a thorough assessment of medical history, lifestyle, and recovery goals. This ensures faster recovery and better long-term outcomes.
Holistic Approach to Healing
At Sanctus Health Care, we believe in holistic rehabilitation, combining medical treatments with complementary therapies such as yoga, meditation, diet planning, and mental wellness programs. Our goal is not just physical healing but also mental and emotional well-being.
How to Get Started?
If you or your loved one needs a trusted rehabilitation center in Pune, Sanctus Health Care is here to help. We provide one-on-one consultations, guided therapy sessions, and continuous support to ensure a seamless recovery journey.
0 notes