#lower back pain is usually bilateral but whatever
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr Inc. is funded by 13 investors.
Text
researching the anatomy of the lower back/pelvis/legs/feet to try to figure out what the FUCK is causing my sciatica bc dear GOD am i in agony rn
#it has been!! so bad lately!!#as SOON as i get back from the island im gonna try to see a dr abt it again#its been long enough since my last Traumatic Healthcare Experience that my desperation outweighs my aversion#it feels better when i walk on it but like. fuck. its 5 in the morning and im supposed to be SLEEPING#what am i supposed to do just pace in my room for hours until it goes away??? 😭#i think someone should simply laterally bisect me and throw away my right side#just throw it directly in the trash#literally all my problems are on my right side#tension headaches/migraines? right side#eye focusing issues? right side#earaches? usually right side#fucking. shoulder EVERYTHING? right side#chest pain/weird rib pain? right side#lower back pain is usually bilateral but whatever#sciatica? right side#all the way from my pelvis to my foot#dont even get me started on my right ankle#fuck that thing#foot pain is bilateral too#anyway#yeah#im left handed i dont need a right side just fuckign. get rid of it#godddd i hope my painkillers kick in soon i want to dieeeeee
6 notes
·
View notes
Note
Ok, I’m sorry if you don’t know anything about this but I assume you do cuz you’re an EMT or EMS or whatever fhdkdbdkdbk
So in a story, someone is going to have a seizure, probably not a serious seizure, but I’m curious about them cuz I don’t know a whole lot about them. How long do they last? I know the longer the more deadly they are. What does the victim feel during and after the seizure? Are they awake after? What does it look like? How do you help someone who’s having a seizure? I feel like this is pretty heavy but I wanna be accurate
EMT ;)
And yeah, I know seizure care and stuff! I’ve never had a seizure so I can’t tell you what it feels like, but when patients wake up they don’t usually remember having it - they remember the buildup to it (sometimes you get an “aura,” some kind of physical sensation or sight that’s a warning you’re about to have a seizure), so they might infer what happened if they’ve had a fair amount of seizures before. But they might be alert enough during it, just depends on the seizure too and where in the brain it is. I imagine it’s both extremely terrifying/disorienting and quite painful due to the intense muscle contraction.
You mentioned that they might not have a big seizure, so briefly, different kind of seizures:
Partial - only affects part of the brain, also called a focal seizure. Often the “seizing” is localized as a result, and patients will remain conscious and alert.
Generalized - affects bilaterally, patient will lose consciousness/alertness. Can be an absence seizure or a tonic/clonic, also called a grand mal. Absence seizures look like spacing out, tonic-clonic are the big ones people think of with seizures.
After a generalized seizure, most typically I think with a tonic-clonic one, there’s this period of time called the postictal phase (ictal = seizure, so post, or after, seizure phase) where, essentially, the brain’s trying to do a factory reset after it spazzed out. Confusion, lethargy, lapsing in and out of consciousness is very common. A patient may wake up swinging, scared, confused, disoriented. May pass back out too. May be unconscious for a good while. May even stop breathing for a few seconds. Everyone’s postictal periods are different.
Proper seizure care!! Keep them safe! Help them get into a safe position, such as lowering them to the ground. Get furniture away from them that they could hit by accident. Turn them on their side so they don’t choke on drool and vomit. Time how long they have the seizure, and how many seizures they have, and note if they act normal in the period between seizures (I.e. if they manage to get out of the postictal phase or not before the next seizure). Call for help. Keep them calm as they come out of it. That’s the best you can do.
How long is a normal seizure? It varies. Most averages I’ve heard are less than a minute. I think the last time I timed a seizure it was like… 15 seconds? Thirty? Something like that.
24 notes
·
View notes
Text
You're on watch while the sun slips ever lower, cresting the horizon and igniting it in a watercolor spray of brilliant orange and gold. It's difficult to look at. You're wearing your shades to blunt the severity of the sun's dying rays but your eyes still pulse with pain through your closed lids.
The crunch of approaching footsteps is the only warning you get before your sibling crouches beside you. Like the sun, they too are difficult to look at. Their silhouette, limned in bronze, is turned partially away from you so that you survey them in profile.
"Kobra," says Poison, the word heavy, and then they stop.
Say nothing. If they want to make the untold horrors of your past more real by speaking them into being, you're not about to make it easy for them.
"Do I gotta worry about...about whatever the fuck was goin' on back there?" Credit where it's due: they're abnormally careful about it.
Pause. Look back to the setting sun, because somehow being bilaterally knifed with photons is orders of magnitude less painful than holding your sibling's gaze just now.
"Why were you even in there?" Don't answer their question. Answer it with another question first. Expect Poison to bristle, but they don't.
"Room weren't empty when I found it," says Poison tiredly. "It was him, and some poor bastard he'd just ghosted. Dunno who. Christ, this killjoy - some sunshine in a tiger mask. They'd been torn the fuck apart, Kobra."
Something about this has gotten under their skin. Perhaps the strangeness of it. Scarecrows are a lot of things, but on the whole they tend to work in the way they've been taught. They're dedicated and efficient and for Korse to have devoted that level of effort to an unnecessarily brutal execution of one killjoy in particular, it...says something. He's not fighting the way scarecrows usually fight. It might have been a personal kill but more you're not sure if it's ego or paranoia that leads you to believe that it could be something else. Him trying to send a message to your crew or perhaps to you specifically. Already he's operating outside the parameters of how scarecrows operate and the thought quietly unravels a bright nodule of terror in your chest.
"So do I?" says Poison, breaching your train of thought. Look askance back at them. They've allowed fraction of weariness to bleed into their posture, perhaps without realizing it. Relaxing, ever fractionally, around their little brother. "Do I gotta worry about this, Kobra?"
Debate the merits of how you want to answer. Because Korse did not set himself on your rearviews until you took the Girl from Better Living's doorstep so, in theory, the easiest and quickest way to shake him would be to pass her off to another crew. To do what Dr. Death originally thought might work, and drop her at Gravel Gertie's orphanage. You've been to Gertie's and you know the defenses of that place and Korse would blow through it easily, rip it up like tangled weeds and set the whole mess on fire. His dracs would slaughter every living soul inside for the simple crime of being there.
You know already that you would not be able to live with the needless and wholly avoidable massacre of defenseless children on your conscience, even if there is a part of you, a part you cannot entirely ignore, that wants to tell Poison yes. Yes. There is something to worry about. There is something digging its way into the grave of your past and it will stop at nothing to get its teeth in you. And they'll understand, won't they, that this means that you won't be able to live with Korse in your shadow and the most efficient way to get rid of him would be to make the Girl someone else's problem. To make Korse someone else's monster.
A part of you wants, badly, to say it. It's the same part of you that, however small, however slight, lives with flicker of something almost like envy germinating in the beds of its teeth because Party Poison loves so loudly and so freely and you have always been their little brother but now they have someone more helpless and more deserving that requires their care. A part of you wants to say yes because you've never had to share their attention like this before, because the Girl is special and important and there is something in not wanting to know where Poison's sense of duty toward her ends and where their role as your big sibling begins.
You're afraid you know the answer to that, if you were to ask. You're afraid that if you were to challenge the resonance of those intersecting points, Poison would answer promptly and without hesitation.
But you're not Korse, are you. You're no scarecrow. You're not so cruel as to force that kind of choice upon someone.
"No," you tell Poison. "You don't gotta worry about any of it."
Poison relaxes. Visibly. Their shoulders slump a little and they breathe out and the fact that they let their relief permeate the space between you speaks to how badly the question had been weighing on them. How badly they, too, must not have wanted to have to make a decision between which they would carry to their grave: the Girl or their little brother.
Swallow back a twinge of guilt.
"You're gonna be okay, Kobra." It's the closest they get to asking you if you will be. Their hand settles briefly on your shoulder, transmits a dose of furious contact adrenaline by the pure weight of it. Their grip tightens, impossibly strong and assured - and then it's gone, leaving a warm ghost of pressure behind. "Yeah?"
"Yeah." You answer immediately, because to hesitate would be to suggest that they're projecting something wishful onto you. And Poison...they're like you, like all killjoys. They don't do wishes. "Yeah. I'm gonna be okay."
Manage a smile, though it feels like it's cracked through, crooked and sore.
Poison ruffles your hair with one hand, grins at you. Twitch a vague echo of that smile back at them, hold it in place until they turn away and head back to the Trans Am.
Hold yourself together, even now that you're alone.
It's your last, best weapon: this shield against that which you refuse to acknowledge.
#danger days#kobra kid#party poison#*mine#*snippet#holy heck this one hurt to write#bit of a long snippet but it didnt feel right to leave parts of it out#their relationship is so fascinating to me....so messed up and codependent and agonizing#kobra is sentimental and envious and he loves quietly#poison is loud and unrepentant and they love so loudly#the number of things they DONT say here weight as much as the things that they DO#the way they front around each other in a different way than how they do around everyone else#in some ways they can be most honest with each other. but in others it's almost harder to be honest at all#when there is something with whom you can usually be fully transparent is it not its own agony when there is something you must withhold?#or perhaps something you feel obligated to withhold for their own good?#the way they allow just a peak more through the blinds than most get; exclusively for each other#and the way that even that is not quite complete. because for it to be complete would risk hurting each other irreversibly#and they wont Do That to each other. they wont lance that boil even if it festers.#party poison and kobra kid are the very platonic ideal of choosing your own quiet suffering if it means the people you love stay happy#and neither of them will complain. and neither of them will breathe a word of it to each other.#and they can on some level see it in each other recognize it in each other#but will still do nothing#because to say anything would open up the possibility for the other to challenge that hypocrisy and then they might truly both combust#god i love them. they destroy me.#oh yes and one more thing - this snippet contains a little shadow of the colossus reference in it uwu#part vi is actually almost done? wild.#can you believe i've written 460k words of dd fic in 2 years
51 notes
·
View notes
Photo

Oh man. Just beware that I have some embarrassingly strong opinions on medical notes. I was (and still am) one obsessive motherfucker when it concerns patients under my care... probably, at times, at the expense of my mental health. So...
We’ll start with your general hospital H&P
As a medical student, however your attending wanted your note written was always the correct answer. That applies to a lesser degree during residency. You’ll generally figure out the people who have strong opinions because, without fail, they will tell you. In those situations, again, the correct answer is whatever your attending says is correct is correct.
The biggest tip I can give is to develop a mental template for everything. I wrote every H&P during residency in a very specific format. It had a couple of advantages: (1) I never left something important out, and (2) it sped up my ability to churn out H&Ps. Now that template had slight variations depending on which service I was on because, as you probably already have realized, different things are important to different subspecialties. In the beginning, it may be near impossible to put together a mental template just because you’re still learning to differentiate the signal from the noise. Everyone is. I will say that my notes now, as an April first year fellow, are much better and more succinct than my notes were as a July first year fellow. That is perfectly ok to adapt things as you learn more and more. So my basic template for a hospital admission was this:
------------------------------------------
HISTORY OF PRESENT ILLNESS
------------------------------------------
A minimalistic one-liner that should tell you, in broad strokes, what you need to know to start formulating a differential diagnosis.
Mr. Smith is a 58 YOM with PMHx significant for [only RELEVANT co-morbidities] who presented by ambulance to the ED for shortness of breath of three days duration.
Next, this is where you break out your mnemonic of choice to describe the patient’s chief complaint. Was onset acute vs slowly progressive? What was his baseline respiratory status and how does it compare to now? Is it continuous or does it only happen when he’s moving? Does he have any pertinent associated symptoms? What makes his sob better or worse? Has this happened to him before? Pertinent negatives to rule out other possible causes of the patient’s chief complaints.
Patient reports his shortness of breath started two days ago and has slowly worsened. At baseline, he is able to ambulate without limitation but is now having difficultly walking more than from room-to-room in his home. While he initially only had symptoms with exertion, he now has symptoms at rest. Sitting in an upright position improves his shortness of breath and lying flat worsens his symptoms. He endorses worsening orthopnea, PND, and lower extremity edema. No fevers, chills, localized symptoms of infection, or sick contacts. No associated cough. No chest pain or anginal equivalents. No personal or family history of blood clots. Reports he was hospitalized two years ago for similar symptoms that required IV diuretics.
Next, I went into the objectives obtained in the ED. What were the patient’s vitals on presentation? What pertinent abnormalities were noted on labs? Imaging? If there were any consults, what was recommended? What treatment was provided in the ED?
In the ED, patient was afebrile, normotensive, but tachycardic to the 120s and initially satting 85% on room air. He was placed on 4L supplemental O2 with improvement. Labs were significant for acute on chronic elevated creatinine, a minimally elevated troponin, and severely elevated BNP. EKG showed sinus tachycardia. CXR showed bilateral pulmonary edema. Cardiology was consulted in the ED and felt his elevated troponin was due to demand ischemia rather than true ACS. Patient received 80 mg IV lasix and was admitted to the gen med service for further care.
------------------------------------------
ASSESSMENT
------------------------------------------
Now a few lines that succinctly presents the case, from beginning to planned end. My goal was always to present a quick overview of the patient’s treatment course.
Mr. Smith is a 58 YOM with NSTEMI s/p DES to the LAD and HFrEF 2/2 ischemic cardiomyopathy who presented to the ED with shortness of breath with a new oxygen requirement and was found to have a HFrEF exacerbation. Treatment course was complicated by a brief transfer to the step-down unit for BIPAP support following admission. He has since been treated with aggressive IV diuresis with improved respiratory status and was transferred back to the floor. He is now maintaining appropriate oxygen saturations on room air. Plan for discharge in 2-3 days following conversion to PO lasix.
------------------------------------------
PLAN
------------------------------------------
These are pretty straightforward. I usually presented off of this part of my note and included things that helped me keep track of my patient’s pertinent history and recent results. For this guy, that would mean knowing this guy’s last EF by echo and when his PCI was performed.
#Acute hypoxic respiratory failure 2/2 HFrEF exacerbation.
-Presented to ED with shortness of breath and new O2 requirement
-Hx of NSTEMI s/p DES to the LAD in Oct 2018
-Baseline EKG with sinus tachycardia. No change compared to prior.
-Last echo in Jan 2019 with EF = 30%; echo 4/8/20 showed EF 15% and WMA of the left apex
-Dry weight 70 kg; patient currently above dry weight at 78 kg
PLAN
-Lasix 40 mg IV; goal net negative 1L
-Follow-up on BID BMP; replete lytes as needed
-Arrange outpatient visit with heart failure clinic
If anyone is interested, especially the new ‘terns or med studs, I can do some additional posts on note writing tips. Outpatient notes are also definitely a completely different ballgame and thus approach.
#medblr#pgy-dinosaur#COVID19-Fest 2020#medical school#internal medicine#residency#internal medicine is the BEST medicine
61 notes
·
View notes
Text
Hide’s likelihood of ever Kissing anyone again and more
A follow up of sorts to my Hide Damage assessment 01 post
Warning :
This will have Hidekane undertones, mostly because I have art for it, it makes for a great example and we know who did it.
Medical jargon ahoy (I make sure to explain it and source a lot of it)
Links for medical samples may be graphic

Prompt (anon ask) :
“How would Hide eat? And how do you think his injuries affect his current quality of life? (Pain, keeping saliva in, eating, breathing, all that shit)”
In this essay I will (for real) :
be identifying important facial muscles
show you what Hide’s healthy facial muscles used to look like
tell you the functions of said facial muscles
breakdown Hide’s damages in parts to show how bad the damage is
inform you of his speech
give you an idea of how food consumption works for him
Teeth or no Teeth missing
Inform you as to whether or not he can kiss or be kissed
tell you how a kiss would work for him
tell you If Hide has any sensation on his lower face
whether or not Hide can keep fluids in his mouth
research If Hide can he close his mouth
after his traumatic sewer experience.

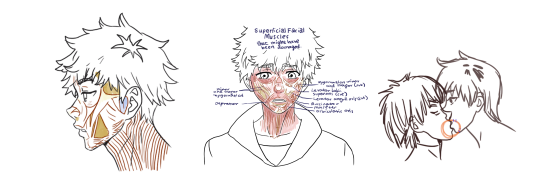
Hide’s facial muscles are fucked.Now that it is confirmed that they are fucked, we can identify what is fucked and how fucked it is, better!
Albeit, I wish we had more shots of uncovered Hide for the sake of better accuracy but, this will do:


We can see that his left side has taken the most damage.
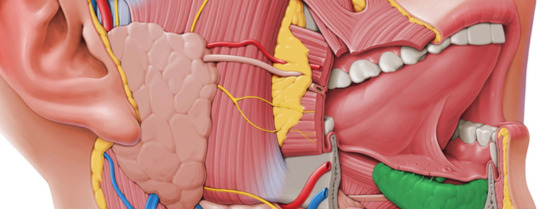
Before we proceed, here is what a healthy facial structure looks like:

from my Damage assessment 01 (transparent!)
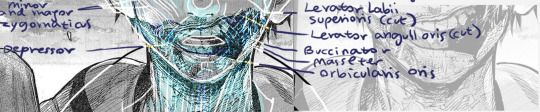
Important Muscles he has had damaged and their function:
Buccinator
The Buccinator’s purpose is to pull back the angle of the mouth, to aid in holding the cheek to the teeth during chewing. This action causes the muscle to keep food pushed back on the occlusal surface of the posterior teeth, as when a person chews. It aids whistling , smiling and more.
Masseter

Is one of the muscles of mastication.The action of the muscle during bilateral contraction of the entire muscle is to elevate the mandible, raising the lower jaw. Elevation of the mandible occurs during the closing of the jaws.
Depressor

The depressor anguli oris (triangularis) is a facial muscle associated with frowning. It originates from the mandible and inserts into the angle of the mouth.The depressor anguli oris is a muscle of facial expression. The muscle depresses the corner of the mouth which is associated with frowning.
Zygomaticus minor aka the "zygomatic head" of the levator labii superioris muscle.

The zygomaticus minor is a muscle of facial expression.
It draws the upper lip backward, upward, and outward and is used in smiling.
Zygomaticus +major
It is a muscle of facial expression which draws the angle of the mouth superiorly and posteriorly to allow one to smile
It raises the corners of the mouth when a person smiles. Usually a single unit, Dimples are caused by variations in form.
Source other than wiki
So then, let’s see how busted he is :
Left side 1/3

Left side important muscles affected
Minor and major zygomaticus : are almost nonexistent.
Lerator anguill oris : seems to be fine as it should be higher up
Buccinator : ripped away for the most part and is likely a very weak muscle.
Masseter : is within the darkened area, I will assume that it is still usable considering he can speak.
Oribicularis oris : Pieces of it left so we’re good there
Depressor : busted.
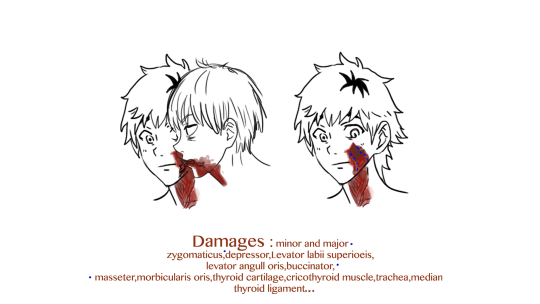
from my Damage assessment 01 (transparent!)
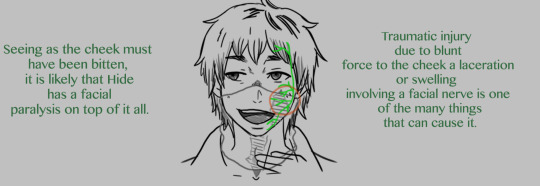
Right Side 2/3

To the right, damages are mostly Flesh wounds.

A flesh wound is an injury that pierces the skin and does not injure bones or vital organs.The damage is for the most part skin deep, muscles were exposed at some point but it probably did not affect them much, except for his Depressor, his Depressor is once again fucked.
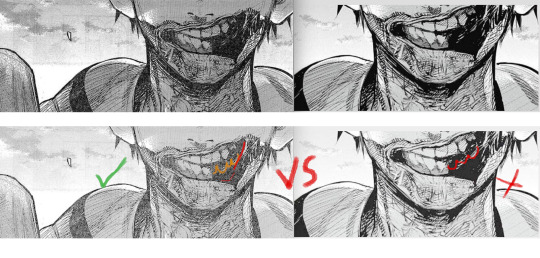
Middle 3/3

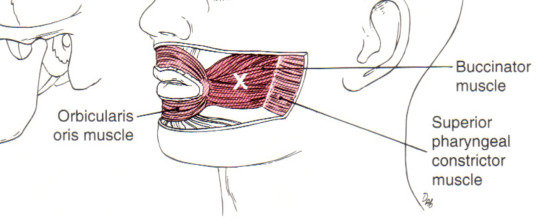
Hide’s lip muscles. Overall, his buccinator on both sides is pretty much gone, his incisivus superior and inferior are for the most part intact (minus the left side), his naso-labialis is safe.

It looks like on the top his lips are eaten to the point where his obicularis oris muscle is exposed, though, because it is still present, at least on the right side of his face he can move. But likely cannot stretch enough to cover his mouth completely.
When it comes to the bottom of his lips, lower pars marginals seems to be kind of busted but still present.
Muscles beneath that look unaffected, so he should be theoretically able to move his bottom lip as well (again minus the left side).
Here is an example of a cadaver (not really graphic) with exposed muscles under skin for reference.Hide’s case on the right side is superficial.
Speech
He’s overall ability to speak due to the left side being so mangled, would be sort of like what’s going on in this here video.( funny and non graphic)
And that, is ignoring how it would sound due to the Voice Prosthesis.

We are focusing on what he is able to articulate due to the loss of muscle and not the surgery because for a person to articulate words, the mouth still has to be able to move. Which is why when I drew a bunch of likely faces for Hide before the reveal, I declared that ‘Put me on a skateboard was not the likely design of choice’ .

(for questions on that, refer to damage assessment 01 again)
Hide is likely unable to articulate sounds like :
-pa ,-ba, -mm

since most of his lips are gone. Here is the Video reference of linguist speaking about Parseltongue and how snakes not having lips cannot make those sounds.
Howeverrrr,

in ventriloquism you learn that because you cannot use your lips you can replace sounds like -m -p -q -v -w with other sounds !

D for B, soft Th for F, Nah for M, T for P, Koo for Q, Th for V and Oo for W
And again, hide’s lips and ability to move them is not fully gone, so he can work it pretty well in all likelihood.

What held him back before was the damage to his vocal fold.
Drinking / Eating
As for figuring out whether Hide can eat or drink...

People with surgically cut cheek holes can give as an idea : This video shows Joel Miggler (Warning Body shocker) who willingly surgically cut holes on his cheeks and they are 34 mm each! We can see the kind of color around the area, how accessible and exposed it is and more.
ie. That man is able to eat food in small doses and soups tend to spill.
Also for the heck of it, Hide can go underwater and hold his breath.
A video of a man with cheek holes swimming underwater and letting bubbles go on purpose.
When it comes to teeth, I would like to believe that he has them because otherwise, that is a whole other mess.Here is how I understand the rendering of the reveal art from the manga.In orange is the outline of the teeth.In red is the muscles dipped in darkness that are coming forth.
In conclusion, he can hold his breath, use a straw, is more likely to eat clumsily and makes sure to eat in small pieces.
Kissable or Not?
Here is video of Joel Miggler, again, this time being drawn in through one of his cheek holes for a kiss. I’m sure that when it comes to Hide being appealing, a lot of people can agree that :
When it comes to whether or not he is capable of it...
Kissing is a complex behavior that requires significant muscular coordination involving a total of 34 facial muscles and 112 postural muscles.

The most important muscle involved is the orbicularis oris muscle, which is used to pucker the lips and informally known as the kissing muscle.
Hide as we mentioned before, still has both the bottom and top one for the most part!
The zygomaticus major is another very important muscle of facial expression and in our case, for kissing.And that is because, as we know, it draws the angle of the mouth superiorly and posteriorly to allow one to smile.That muscle on Hide is pretty damaged.
Passionate kissing can involve as many as 23 to34 facial muscles and 112 postural muscles.

When there is a will, there is a way!
Simple kisses use as few as 2 muscles!!!

Kiss art above
Kisses Hide can receive (from Ken??) :
Teeth Kiss (it’s a joke but Aeon Flux did it sooo...) / Hand kissing / Kissing on the nose / Affection Kiss / Greetings kiss / Kiss of tenderness / Passionate kiss

The kind of kissing Hide can do :
Flying kiss / Kissing on the nose / Romantic kiss

Source for kissing info and and names
Last but not least.
Will he feel a kiss? tl;dr? now of all times?? I’m inclined to believe he can.
Hide is pretty badly damaged but, Ishida ignored the likelihood of facial palsy altogether (unless he decides to show that Hide he had the non permanent version of it at some point during recovery) so when it comes to moving whatever he has left and having some sensation on his face? he can.
from my Damage assessment 01

Congrats! You are now Done!

Tune in for more posts like this one!
Also cool to see : Damage assessment 02
Hidekane : Fanart / Fanimation / Fancomics / Theories & Analysis
Like BNHA?! Check out my analysis on Dabi !
#hideyoshi nagachika#hidekane#tokyo ghoul re analysis#tokyo ghoul re theory#hideyoshi nagachika theory
205 notes
·
View notes