#if i can find a pattern it might help the cardiologist when i see her eventually
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr is available in 18 languages.
Text
So yesterday my cuz with POTS mentioned using a fitbit to track her heart rate (easier to keep a log of what causesa spike that way). I used to have one and loved the little thing, but sadly it was lost in the move. Pasta Mama heard and just got me one as 'an early Christmas gift'. And so I slapped it on yesterday.
And what do ya know. Despite basically just resting as the doctor ordered until I can be seen, my heart rate was indeed spiking repeatedly out of nowhere. Sometimes when I stood up to stretch or walk around a little so I didn't get stiff, but also sometimes when I was just sitting or laying down doing nothing. No wonder I'm struggling to sleep.
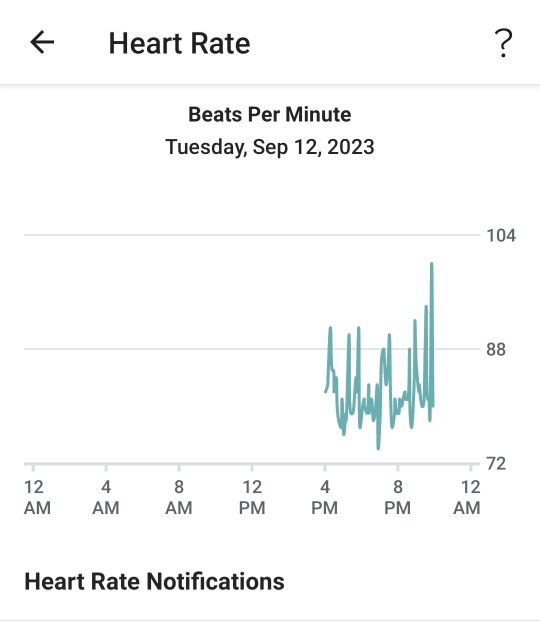
#as best i can tell standing up to walk around is a trigger#but sometimes it does this when I'm basically doing nothing but sit#either way i'm going to try to keep a notes log of spikes and what i'm doing#if i can find a pattern it might help the cardiologist when i see her eventually
26 notes
·
View notes
Note
Hi! Wondering if I can take you up on the offer in that dysautonomia post.
I’ve been feeling randomly more tired than it feels like I should, but I think it’s not general deconditioning? Showers can wipe me out for a few hours and a shower chair is helpful - but I can walk for miles and afaict even a 5 mile hike drained my mental energy before obvious physical exhaustion (noticeably worse executive function and sensory/emotional tolerance but only normal muscle fatigue). Medically, been trying to sort out high hgb/hct that isn’t going down that much with T dose, and also night sweats at least a few times a week, and also I can be lying down to nap with my heart rate over 100 and it only comes down slowly. Can’t freaking tell what’s ptsd triggers, what’s other stress/anxiety, what’s maybe autistic burnout/sensory management taking much more energy than I expect, what’s needing to eat more consistently, what might be sleep issues, what’s effects of hormone levels, or what might be something else. I’m waiting for a sleep study to try to rule out sleep issues. I would really appreciate any pointers if any of this sounds like it might point a particular direction or if other tests might be useful.
Sadly that could be a lot of things, and I definitely think a sleep study is a good way to start. Making sure to manage your food and water intake, fixing your sleep schedule, taking care to be kind to yourself during episodes, those are a good place to start. No, I'm not saying that that will completely fix your problems, but any doctor that knows about POTS that does end up diagnosing you [if you have it] will tell you to do these things anyway. This is why I have been slowly attempting to unfuck my life.
If all of these things don't seem to be helping and the sleep study reveals nothing, the next thing I'd do is buy a cheap blood pressure monitor and see if you can have an actual record of your heart rate and blood pressure before, during, and after these episodes if possible. Something that records the output, or take a photo of the readings so you can show them to your doctor. Personally being a child of diabetics I also recommend buying a cheap glucose test kit to see if your sugar levels are doing anything funky during these times as well. Try to keep a journal of time of day, what you were doing just prior, and the readings you're acquiring to see if someone can point out a pattern.
A really easy way to see if there's a cause for pushing for specific testing is to go from seated to standing at your usual pace. If you are an otherwise healthy person and your heart rate jumps more than 30 bpm there is a pretty good indication that something interesting is happening inside of you that shouldn't be. If you also notice a big spike or drop in your blood pressure when initially standing or after standing still for a long period, that's another clue.
If you unfuck these areas of your life AND are getting concerning readings with little to no improvement on symptoms, it's time to look deeper. Most cardiologists will do a 24hr holtor, an EKG, a tilt table test, and/or a stress test, though the tilt table test is the one that really tends to seal the deal. However with some of your symptoms, I would honestly not be surprised to hear your doctors wanting the sleep study and probably an EEG to rule out things like sleep disorders or epilepsy as there can be some overlap.
It does take the average patient 8 years for a diagnosis- it took me less the first time around because of my family history, but the second time around took more like a year and a half due to comorbidities and I literally almost died. A friend of mine got really jerked around by her doctors for close to 6 months before someone was willing to run a tilt table test and almost instantly diagnosed her the second she fainted during the test. Another friend was told she was being a ridiculous germaphobe while her doctor ordered the test despite having a known dx of something commonly associated with POTS and again she was still diagnosed almost instantly during her tilt table. A third friend keeps getting 'hmm maybe' 'no' 'totally healthyl 'yes?' 'okay well that's weird' when he asks for a tilt table and they refused to give it to him despite picking up arrhythmias during his holtor and EKG- it's been a year and he's still arguing with the doctors to get a tilt table. Unfortunately many doctors simply aren't trained in autonomic disorders or in autoimmune disorders, and POTS is both. It can be very difficult to find someone willing to listen to you.
If you do all of these things and land on 🤷♂️, a lot of times it's things like fibro or MS, and the knowledge gained from these tests will help find a diagnosis of whatever-it-is affecting you.
6 notes
·
View notes
Text
Its not personal
The last two weeks have been incredibly stressful. I haven’t felt this pressured since, lets see, 2018. No one told me this job was ever going to be easy, but at least leave me the right to crib about it. I don’t usually though. You might ask “Well, isn’t that what this blog is all about?” No. This blog is an outlet in my journey towards self realization, so don’t be a douche about it. This post is a tale of personal trial and tribulation and how this has had a profound impact on how I treat my patients. Needless to point out, like every other blog post, this is fairly long, so brace yourself.
I had just come back from an evening shift and was catching up on season 2 of The West Wing, nothing different from the usual post shift nights. It was around 1 am when my neighbor knocked on my door. His father who lived 3 hours away from the city was taken to a nearby hospital with complaints of severe retrosternal chest pain. The doctors there diagnosed it as a cardiac event and did not have the facilities to handle the patient. My visibly worried and flustered neighbor, who is other wise one of the most calmest people I know, had come to me for counsel. I spoke to the doctors over the phone and their diagnosis was clear - ST depressions in the ECG and typical nature of the pain - this was likely an NSTEMI or Unstable Angina. I asked for a cardiac enzyme panel and an immediate transfer to my hospital in Hyderabad. The cardiac enzymes came negative in the time they were arranging for the ambulance, So most likely an unstable angina. I asked my neighbor to relax and bring him to Hyderabad immediately. This should be pretty straight forward to handle. We both left to my hospital in anticipation of his arrival. I spoke to the managers on duty before hand so we could get the financial conversations out of the way early. This was around 3 AM in the morning and I was in the ER following up lab and radiology reports of the patients I admitted the previous night as I awaited their arrival and my neighbor waited at the hospital entrance. The ER door slammed open with a trolley being wheeled in in a rush and a patient lying in a pool of vomit, semi conscious, and then right behind the trolley, I saw my neighbor running in breathless, looking for me. Shit. This patient was my neighbor’s father. Something had gone very very wrong.
We moved him to Priority 1, me and two other ER docs took charge. The patient was now coming around and writhing in chest pain radiating to his back. He was incredibly restless, bouncing up and down the trolley to a point where we had to physically restrain him just to get the ECG. Pain score easily at 9/10. Non medically speaking - imagine being awake watching a bear maul your guts. The cardiologist was right by side, ecg now showed a qRBBB pattern - this is bad, very bad. I was holding the patients hand trying to calm him down as pain meds were being pushed in in rapid succession, and then it happened. I was talking to him, calming him down, and in that moment, he stopped talking, his eyes rolled up, he protruded his tongue, clenched his jaw, squeezed my hand in a death choke, started seizing and crashed. My colleagues crash intubated him and as I looked away in despair, my eyes met with my neighbors.
I was at a loss of words to explain the turn of events over the last five minutes. Most likely vasovagal, but this was unanticipated. I felt responsible and I felt helpless. A 70 year old in cardiogenic shock on mechanical ventilator and likely aspiration - I knew the odds. I knew I was staring down a barrel of potential complications most likely ending in death, but little did I know there was far worse in store. For now though, I tried to explain to my neighbor that we’re doing whatever we possibly can, that we’re taking him to the cath lab and I’m going to be there by his fathers side through all this. One look at his father lying motionless on the bed with an Endotracheal tube down this throat, he held my hand and broke down crying.
We rushed him to the cathlab, angio showed double vessel disease with stenosis but it didn’t explain the pain. This was not an infarct and the flow to myocardium was still intact. It had to be something else. We took the cue of the severe tearing type of pain radiating to the back he complained of on presentation and took him to CT aortogram to rule out a dissection, also because there was some disagreement over how his distal pulses were. It was negative for dissection but I noted a mildly bulky pancreas and asked for a serum amylase and lipase to cover that base. It was 6 am by now and there was nothing more to be done than wait and hope the vasopressors held on to dear life. I walked out of the Cardiac ICU, mustered all my courage and told the family that this is looking bad. We’re doing our best, but with no concrete diagnosis, I had little to offer. The neighbor drove me and his family back home. His sister and his completely unaware mother sat in the back seat worried and . The silence on the way back home was defeaning.
I hadn’t felt a depressive episode like this, not in the last 8 years. I tried to sleep it off, but that was futile. I was responsible. It was my decision to treat him at my hospital and he was my responsibility. Despite doing everything we possibly could, I was going to lose him. The very thought that I would have to face my neighbor everyday, and be seen in his eyes as the guy who couldn’t save his father, broke me. I came home at around 6 30 am and got a call from my HOD at 8 am that there’s an acute shortage in the ER and they needed me to come in to work and help out. If this were my older self, I would have been there in a jiffy, but on this morning, I could not get myself out of bed. I felt despair, I felt pain and I felt hopeless. I did not want to disappoint my HOD and I also wanted to know how my patient was doing, so I pushed myself and got to work to one of the most messed up shifts I’ve done in a while. May be it was just my depression, but it was a one hell of a busy republic day morning. Why oh why do people save their illnesses just for the holidays?! My patient was still on the ventilator, high inotropic support, an unreasonable no. of ectopics on the ecg and pretty bad lungs, but negative amylase and lipase. I still had no hope to offer and everything seemed so futile. I don’t even recall how the next few days passed. I barely ate, barely slept and I still put up a face at work, try and be the most pleasant doctor you could find in the ER.
On the third day, he started improving rapidly. No more vasopressor support, no more ectopics, resolving TLC. On day 4, he was extubated and I finally breathed a sigh of relief. I finally slept peacefully. I finally smiled at home and spoke up to my worried sick mother. I haven’t seen her this helpless before. She knew I only had the best intentions, she liked to believe that I did nothing wrong at all, that I was their best hope. Can’t blame her. Mothers are like that. Unconditional love, unshakable confidence in you and blind faith. She could not do or say anything that would make me feel better. She knew how much I cared about this, how much I’ve put myself into this, but for now, she was helpless. That all changed like I said. The patient was off the ventilator and on his way to a full recovery.
He came home today. After two full weeks in the Cardiac ICU, he came home today. I paid him a visit and he himself pulled up a chair to offer me a seat. Today is a good day. I smiled with all my heart and a sense of satisfaction I haven’t felt in ages. I cannot take credit for all the hardwork put in by some of the finest cardiologists, intensivists, emergency physicians and nurses to bring him back. I am proud that I can look up to these people at times of despair and I am lucky. As for his loving wife and caring son, I can only feel happy and thankful. I did give him a thorough dressing down for popping NSAIDs like tic tacs and trusting his local pharmacist more than his doctor, but that’s just most Indians.
The purpose of this post is not to talk about a very odd presentation or a difficult case management lesson. The purpose of this post is to talk about physician wellness. The toll that the responsibility of someones life in your hands takes on your mental state of being is indiscernible to someone who has never faced it before. I spent the last two hours on this particular sentence trying to come up with a way to explain it and I’ve failed. Writers block? No. It is a sense of duty and privilege we can never fathom fully.
This is a tale of a very personal emergency. I went the extra mile with this patient. This made me ask myself if I’m not doing to this every patient. Is it humanly possible to feel this deeply about all of my sick patients and live a normal life without going absolutely mad?. It’s like having 40 to 60 of your family members fall incredibly sick in a span of 6 hours and all come to you for treatment. That’s my ER’s average foot fall in a day. I will most definitely die an early death , not that i’m not going to now. It is tough, what we do. It breaks us and yet, we keep going. It takes a different kind of crazy to go back to all this, everyday, every patient. It is my hope through this blog that my people realize that these heroes don’t wear capes or don’t have billboards. They’re fighting a system rigged against humanity in general and doing their part as best they can. Cut them some slack, because they’re walking a thin line - to feel, yet not to feel.
6 notes
·
View notes
Note
Dr Who but each incarnation is swapped with one of their companions.
omg?? I love it??

The First Doctor:
She’s not completely unfriendly, exactly, she just doesn’t have time for humans being idiots. In the right circumstances, she can actually be very warm. She loves history, which is lucky because her granddaughter Susan does too (they tell people Susan is her daughter, but even then it’s a bit of a stretch, human ages are weird). Of course, then two of Susan’s teachers follow her home one night, and next thing the Doctor knows she has a crotchety old history teacher and a handsome young science teacher on her spaceship with no way to get rid of them that isn’t morally questionable.
Whoops?
The humans help her lose some of her haughtiness. She leaves Susan in the 22nd century to become her own woman.
Along the way and against her better judgement, she falls hopelessly for Ian Chesterton. He wants to stay with her forever, but she knows it would never work, and encourages him to go with John Foreman in the Dalek Time Machine to get back to his own time.
Later, in other lives, she checks in on him occasionally.

The Second Doctor:
The baby face is a problem. It takes a good twenty minutes on a lot of occasions to get anyone to take her seriously. On the bright side, a lot of Polly’s clothes fit her now.
She finds a best friend in Scotsman Jamie McCrimmon, whose rather naive approach to futuristic technology is extremely refreshing, as is his unique insightfulness.
After Ben and Polly leave them, they rescue Victoria, who Jamie is utterly taken with. Victoria is unsure about living a life so unsupervised by someone older and won’t listen to the Doctor’s insistence that she is in fact perfectly qualified to look after them all.
She and Victoria spend a good many nights aboard the TARDIS talking about women’s history and the things to come for women in the future and how women act on other planets. Victoria is fascinated, occasionally horrified, and often quietly thrilled at the things she learns.
It’s a shame to see her go, but all she ever wanted was a family and security, and the Doctor can’t provide that.
They meet an eccentric man on a space station, with funny trousers and an obsession with the recorder. The Doctor and Jamie like him instantly, and invite him on board only to learn that the man had been considering stowing away if not invited.
The Time Lords take her friends away from her. She is forced to regenerate and exiled to Earth, as punishment for her interference.

The Third Doctor:
Shrewd, passionately devoted to science, and not one to take kindly to interruptions or anyone trying to talk down to or even disagree with her, it’s a wonder the Doctor even gets hired by UNIT at all. But then again, beggars can’t be choosers.
On the bright side, this fellow John Smith from Cambridge seems to be the one person around with an actual brain and not just a penchant for attacking first and thinking later.
They’re friends instantly. Or, they are once she makes it perfectly clear that she is the cleverer of the two. The look on his face when he realises is a memory she’ll treasure forever.
He eventually leaves to go back to his own research, upon realising she doesn’t need him.
It’s a shame and she misses him, but then Jo Grant comes into her life. Despite an awful first impression, the two women are soon fiercely devoted to each other. Jo keeps going on about women having to stick together amongst all the army boys, and while the Doctor could usually not care less about gender politics, if it means Jo hangs around her more, then so be it.
The Master turns up. It’s exhausting and exasperating and oh so much fun.
Meanwhile, the Doctor’s told herself to not let herself fall for humans, after how much Ian hurt. But with Jo, it’s impossible not to. (Not that she hasn’t noticed the Brigadier’s lingering stares, or failed to appreciate him in his uniform. But he’s far too professional to ever do anything, and too trigger happy besides.)
Jo is like sunshine and she’s always there and smiling and pressing herself against the Doctor out of fear or shock, until one day they’re in the supply closet of a spaceship and they’re kissing furiously instead of listening out for their pursuers.
It’s wonderful, being with Jo. Until Clive Jones comes along, and the Doctor has to tell her to forget about her and marry the nice young man who can grow old with her and give her the life she wants.
She drinks more champagne than she is proud of that night.
Luckily, along comes Sarah Jane Smith, who is exactly the kind of human that the Doctor automatically adores. Inquisitive, sharp, and a vocal feminist. What a woman.
Of course, then giant alien spiders happen, and it’s time for a change.

The Fourth Doctor:
Or… not. Apparently, she’s doomed to be young, attractive, humanoid, and pale skinned throughout all her lives. There are worse fates, but she wouldn’t mind a little variety, frankly. And being so small is getting infuriating.
Harry takes a long while to take her seriously, but once he does, he is steadfastly loyal. Sarah Jane takes the regeneration in stride for the most part.
And after them, Leela, who is so strange and savage but so utterly charming in her honesty. They share a few kisses, but nothing more.
Then comes Romana. A young Time Lord who looks older than her, is far taller than is sensible, and has an even more absurd grin. She can’t stand him, with his bragging about his grades and thinking he knows everything.
She soon teaches him that experience wins every time.
Of course, then he spots some pretty princess on Tara, and next thing she knows, the moment the whole Key To Time mess is sorted, Romana is now a less taller, less ridiculous, utterly beautiful Time Lady in her first regeneration.
She tries to argue against what she can only consider body theft, or at least copying, but it is a relief to not have to crane her neck up to speak to her companion.
Romana becomes a most dear friend. She’s missed being around someone like her, someone who understands. It makes it all the worse when she leaves, leaving the Doctor with only Adric and his incessant questions.

The Fifth Doctor:
There’s something about this body, a regality, that commands a little more respect than the ones before it, despite it following the pattern of her others.
Adric’s questions exasperate her, while Tegan’s demands to be taken home are met with gentle requests for patience and promises of Heathrow airport, and this Traken prince she’s picked up is thankfully one of the most polite people she’s ever had in the TARDIS. Decent brain on him, too.
Tegan’s smile sometimes makes her stomach do backflips. The Doctor ignores it. She’s learned her lesson. It’s almost a relief to see Tegan reach her breaking point and leave, except it isn’t, because for a long while it feels like a part of her is missing.
Turlough is a curiosity, but a nice one who makes for surprisingly good company in the absence of the others.
Perpugilliam Brown is a surprise. The Doctor remembers why she has tried to avoid America where possible in her travels. Americans are loud. But in the case of Peri, it involves shouting at the Master, and as such, the Doctor decides that Perpugilliam Brown can stay as long as she likes.
Between the two of them and soon Erimem, uncrowned Pharaoh of Egypt, they make quite the team.

The Sixth Doctor:
It’s about time! Finally, a more weathered model. Peri is surprised to say the least, and seems a little disappointed to lose out on her best friend who had until now looked a very similar age to her, but soon realises very little has changed.
And now she lets the Doctor take care of her a bit better. Thank goodness for that! The maternal instincts in this body are absurdly strong, she has no idea what she would do if she couldn’t express them.
Now, the borderline narcissistic but quietly lovable history professor she accidentally picks up some time after losing Peri is a trickier matter. Still, at least he shares her love for chocolate cake.

The Seventh Doctor:
Bright, bubbly, and able to get most people to like her within ten seconds. Now this is a regeneration she likes. Plus, her most impressive set of lungs yet. Handy, for calling companions who like to wander off.
She tries to not encourage Ace’s use of explosives, but it’s difficult when she sees how genuinely happy they make the girl. She’s getting soft in her old age, she knows.
Still, at least her brain makes up for it. She can out-think a computer, easily. The universe is her chessboard and she’ll do whatever the hell she pleases with it.

The Eighth Doctor:
She’s a jolly thing. Always keen for adventure, ready to shout at anyone who deserves it, and just wants to have a good time, really.
After a rather rocky start involving amnesia and kissing the cardiologist who had caused her regeneration in the first place, the Doctor is just minding her own business when she accidentally messes with history.
It seems that saving this stowaway on the R101 might not have been the best idea after all. But he’s so charming and sweet and genuine, sharing her utter passion for life, that by the time she realises her mistake, she’s not willing to part with him.
That goes… about as well as one might expect.

The Ninth Doctor:
It’s funny, being a weathered old war veteran with a guilty conscience, and simultaneously looking like someone who could be on the front of a magazine.
Life is hard, after the time war, but she meets a man with big ears and blue eyes and things get better. A lot better. It feels good to smile again.
The addition of Captain Jack Harkness is an interesting one, but she’s always said the more the merrier. Their other companion is not quite as happy about this development, but before long they’re the best of friends.

The Tenth Doctor:
She’s gentler now, somehow. Oh, she has her anger and her snark, and boy does this body have a set of lungs on her. But she’s so much softer, underneath.
Losing her friends from her last body takes its toll. She at least manages to avoid comparing Martha to them that came before her. Martha is wonderful, always completing even the most impossible tasks that the Doctor puts to her. They part on good terms, after the Master’s ravaging of the Earth. (The Master had not been so impressed with this version of her. He had trouble seeing the strength within, seeing that she was more than the duality of compassion and shouting.) Martha needs to look after her family, and that’s probably for the best.
And then there’s the skinny idiot in the suit. He actually talks faster than she does, which is absurd, but she wonders if that’s simply because of his questionable family. Perhaps not letting them get a word in is how he survives.
Either way, they get along like a house on fire. Losing him, wiping his memory and seeing him stare right through her and smile that stupid smile, is almost enough to break her.
No more companions, she swears.
The Eleventh Doctor:
It’s all about fun, now. Impressing the little boy whose garden she crashes in and then impressing him when he’s grown up and has waited 14 years for her. (To hell with her rule about no more companions. Her old self was full of dumb ideas anyway.)
Oh yes, she likes Rory Williams a lot. And his best friend John isn’t bad either. Mind you, that nose…
She has her spaceship, and her boys, and life is good. Well, there’s River Song to worry about, but she can never be sure if the archaeologist is more interested in her or John. Just one more mystery, it seems.
Losing Rory, and then John, is hard. But she knows that they’re happy, and that’s enough.

The Twelfth Doctor:
Short, bossy, a control freak, and a slight obsession with tartan. Also, her English teacher companion is secretly a rock star wannabe, disguised as a reclusive Scottish nerd.
What’s a girl to do?
(Apparently, find out that her best enemy is alive, and now also female. And Scottish like her companion. The first kiss had been… shocking to say the least. The ones after, against her better judgement, decidedly less so.)
She cares about her companion more than she will ever say, and when faced with losing him, takes things too far. Further than anyone should ever take anything. And when it is all said and done… she can’t remember his face, or his voice, or how he sounded when he mocked how large her eyes were.
River is there to comfort her, though, in those 24 years on Darillium.
And then Bill. Brilliant Bill. Oh yes, they make quite the team. And Nardole helps sometimes too.
Send me an AU and I’ll expand on it!
#Anonymous#doctor who#doctor who au#dw au#female doctor#female doctor au#companions#this took SO LONG#and isn't quite in the same format as a normal AU expansion but that's cool#this got pretty gay lmao#i can't help it ok this fandom is so good for femslash and this au especially#au ask meme#i didn't do war cos lack of companion#maybe he has one in the audios but idk#this was fun if tiring#CAN WE PLEASE HAVE A FEMALE DOCTOR LIKE SERIOUSLY
3K notes
·
View notes
Text
Could the Apple Watch Save Your Life?
I come from a family of a-fibbers (and I’m not talking about their charming tendency to enhance their stories with a wee bit of fiction). My father, two uncles and a sibling have all been diagnosed with atrial fibrillation (AFib.) While the exact incidence of familial AFib isn’t known, studies have shown that up to 30% of people with AFib may have a relative with the heart condition, according to the Mayo Clinic.
Needless to say, I was intrigued, so I decided to try out the Apple Watch ECG app and irregular heart rhythm notification feature, which together help identify potential incidents of AFib. (The ECG app is part of a free update to watchOS 5.3 Series 4, and the irregular rhythm notification feature works on Series 1 and higher.)
Before I reveal my results, here’s a quick primer on what AFib is according to the Heart & Stroke Foundation of Canada. It’s described as an irregular heart rhythm, or arrhythmia, that is caused by electrical signal disturbances in the upper chambers of the heart, or atria. When the signals are regular, the blood is pushed from the atria into the lower chambers (the ventricles), where it is pumped to the rest of the body. If you have AFib, the upper and lower chambers don’t beat in sync, which means they aren’t pumping efficiently.
AFib, which can be treated with medication, affects approximately 200,000 Canadians. If untreated, it can increase your chances of having a stroke or experiencing heart failure. The risks increase with age, or if you have health issues like diabetes or high blood pressure or other heart-related conditions.
With AFib, some people notice that their heart is beating very quickly (sometimes more than 150 beats per minute)—even though they’re not doing anything physical. Others might feel like it’s skipping a beat, while some may have no symptoms, which is why this ECG app and irregular rhythm notification feature might be a real lifesaver.
.embed-container { position: relative; padding-bottom: 56.25%; height: 0; overflow: hidden; max-width: 100%; } .embed-container iframe, .embed-container object, .embed-container embed { position: absolute; top: 0; left: 0; width: 100%; height: 100%; }
Here’s how they work:
Irregular rhythm notification:
In addition to the high heart rate and low heart rate notifications, your Apple Watch can now alert you when your heart is beating irregularly and suggest that you see your doctor if you haven’t already been diagnosed with AFib. You’ll receive this notification if an irregular rhythm has been detected on five rhythm checks taken over a minimum of 65 minutes. Unlike the ECG app, which only works on Series 4 because it has electrodes built into the back crystal and Digital Crown, this notification works on Series 1 or later. How accurate is it? According to data collected from the Apple Heart Study, almost 80% of the participants who wore the watch, as well as a clinical ECG patch, received the notification and showed AFib on their ECG patch. Of note, 98% who received the notification showed other arrhythmias on their ECG patch.
ECG app:
This app, which had to be approved by Health Canada because it is considered a medical device, allows you to take an electrocardiogram (ECG) right from your wrist. It’s really simple to do. Launch the ECG app on your Apple Watch Series 4 and hold your finger on the Digital Crown. After 30 seconds, you’ll receive a notice that your reading is sinus rhythm (which means it’s normal and has nothing to do with your sinuses), AFib or inconclusive. At this point, you can also add in symptoms like rapid, pounding or fluttering heartbeat, skipped heartbeat, fatigue, shortness of breath, chest tightness or pain, fainting, dizziness, other or none. The reading, and any symptoms you added, will be sent to your Health app on your iPhone, and you can email a PDF of the reading to your doctor.
So, how accurate is it? According to clinical trials, when the results of readings from the ECG app were compared with 12-lead ECG readings done by a cardiologist, the ECG app picked up 98.3% of instances of AFib and 99.6% of sinus rhythms. While it might be tempting to be constantly taking ECGs, Apple recommends you take it when you’re feeling symptoms like a rapid or skipped heartbeat. It’s important to know that this app can’t tell you if you’re having a heart attack or stroke. If you feel any chest pain, pressure, tightness or what you think might be a heart attack, call 911.
The verdict:
I was relieved that my ECG readings were all sinus. I did have some inconclusive results, which might be because I was moving around. You need to be seated with your arm resting on a hard surface when you take the reading, and the Apple Watch needs to be snug around your wrist. There are stories online about the app alerting people to potential heart issues, including this story from a c|net reporter who tested the watch and it “detected something strange about her heart rhythm.” Concerns about false positives, or cases where the AFib rhythm isn’t detected, have also been raised by some physicians, but given my family history I still find it comforting to know that any irregular patterns might be detected. And knowing that I can quickly take an ECG if I experience any symptoms is pretty empowering.
The post Could the Apple Watch Save Your Life? appeared first on FASHION Magazine.
Could the Apple Watch Save Your Life? published first on https://borboletabags.tumblr.com/
0 notes
Text
Freed From the iPhone, the Apple Watch Finds a Medical Purpose
“This is an important step in the evolution of wearables,” said Tim Bajarin, president of Creative Strategies, an advisory and research firm. “The Apple Watch can now be on you all the time doing this type of medical monitoring.”
The Apple Watch has dominated competitors in the nascent smart watch market, but it has not taken a place alongside the iPod, iPhone and iPad as the next breakthrough Apple product. Apple does not disclose specific sales numbers for the watch, but the company has said its sales have risen 50 percent compared with a year earlier for three straight quarters. An Apple spokeswoman declined to comment further.
A digital health revolution has been predicted for years, of course, and so far has been more hype than progress. But the hope is that artificial intelligence systems will sift through the vast amounts of data that medical accessories will collect from the Apple Watch and find patterns that can lead to changes in treatment and detection, enabling people to take more control of how they manage their conditions instead of relying solely on doctors.
Vic Gundotra, chief executive of AliveCor, a start-up that makes portable electrocardiograms, said this would put patients on a more equal footing with doctors because they would have more information on their own conditions.
“It’s changing the nature of the relationship between patient and doctor,” he said, adding that doctors will no longer be “high priests.”
Last month, AliveCor introduced a band for the Apple Watch with a built-in electrocardiogram, or EKG, to detect irregular heart activity such as atrial fibrillation, a form of arrhythmia and a potential cause of a stroke. AliveCor uses the watch’s heart rate monitor to alert patients to take an EKG when their pulse quickens or slows unexpectedly.
Photo
Members of the media examining the Apple Watch at a preview in 2014 in Cupertino, Calif. Credit Monica Davey/European Pressphoto Agency
The band, known as the KardiaBand, was the first Apple Watch accessory approved by the Food and Drug Administration. When a thumb is placed on the band’s sensor, EKG readings are taken in 30 seconds and sent wirelessly to the patient’s cardiologist. That helps resolve one of the biggest headaches in detecting atrial fibrillation — catching it during an episode so a cardiologist can properly assess it.
Continue reading the main story
Elena Remus, 36, a digital marketing consultant from Alameda, Calif., has experienced what the KardiaBand can do. She had suffered heart palpitations on and off for the last five years, but there was little her doctors could do because they were never able to catch the incidents in real time.
Shortly after buying a KardiaBand for her Apple Watch a few weeks ago, Ms. Remus felt the onset of palpitations as she was making morning coffee. She looked down at her watch and saw that her normal heart rate of around 75 beats a minute had surged to 205 beats a minute. She started taking an EKG reading on her wrist and was finally able to record the activity, allowing her doctor to diagnose her condition as atrioventricular nodal re-entrant tachycardia — or in nonmedical speak, an abnormally fast heart rhythm — and plan a course of treatment.
“Now, I don’t feel like I’m going to pass out at home alone,” Ms. Remus said.
Apple is also looking for its own medical breakthroughs. Last month, the company announced a joint research study with the Stanford University School of Medicine to see whether the Apple Watch’s heart rate sensors could detect irregular heart activity without an electrocardiogram to notify people who might be experiencing atrial fibrillation.
Apple is also looking at potentially building an electrocardiogram into future models of the Apple Watch, according to a person familiar with the project, who spoke on the condition of anonymity because the details were confidential. It is unclear whether the EKG development, earlier reported by Bloomberg, would be introduced; such a product would most likely require F.D.A. clearance.
Separately, Apple is continuing research on a noninvasive continuous glucose reader, according to two people with knowledge of the project. The technology is still considered to be years away, industry experts said.
The current solution used by many diabetics is also coming to the Apple Watch. Dexcom, a maker of devices measuring blood sugar levels for diabetics, said it was awaiting F.D.A. approval for a continuous glucose monitor to work directly with the Apple Watch. Continuous glucose monitors use small sensors to pierce the skin to track blood sugar levels and relay those readings through a wireless transmitter.
Kevin Sayer, Dexcom’s chief executive, said that patients could opt for a monitor to communicate directly with the watch for convenience, but that the big payoff could come with combining sleep or activity data from the watch with glucose readings from its device to find correlations.
“We’re just beginning to unlock the potential of that data,” Mr. Sayer said.
Health care professionals said there was a risk of too much information. Dr. Khaldoun Tarakji, a cardiac electrophysiologist at Cleveland Clinic, said doctors needed to guide patients about who would benefit from more information and how much data was the right amount.
“We need to think about when too much information becomes just noise,” said Dr. Tarakji, who has worked with AliveCor to test KardiaMobile, a portable electrocardiogram that works with iPhones.
A flood of information, albeit potentially useful, may overwhelm doctors instead of assisting them. Initially, KardiaMobile patients sent their doctors an email each time they took an EKG reading. The flood of emails became confusing and raised questions about where the doctor should store that information. In response, AliveCor introduced a software platform for doctors that could populate the readings from patients and help detect early signs of atrial fibrillation.
Continue reading the main story
“A wearable device does not equal a wearable physician,” Dr. Tarakji said. “As a medical community, we have to be intelligent about how to use these new technologies.”
Continue reading the main story
DAISUKE WAKABAYASHI
The post Freed From the iPhone, the Apple Watch Finds a Medical Purpose appeared first on dailygate.
0 notes
Text
Pig and Pepper Part 1
Masterlist
Sam and Dean stood in a garage with their shirt sleeves rolled up staring at the car before them. Some guy had smashed through the windscreen of the car while it was parked where it stood now. It was supposedly the car James Dean had died in and Dean had been tasked with checking to see if it was true. They stared at it uncertainly.
"You want me to do it?" Sam asked.
"No... no, no I've got it." Dean approached the car. "Okay baby I'm not gonna hurt you, so ...don't hurt me." He told it as he slid underneath it on a roller board.
"I wasn't planning to." Came a voice from the other side of the car. Dean jumped banging his head on the bottom of the car. "You Okay under there?" Laceys face appeared underneath the car.
"Yes, geez Lace." She smiled at him and stood back up. Dean took a rubbing of the number on the engine and rolled back out from under the car. Lacey was standing next to Sam now. She was wearing a blue and black striped jumper that hung off one of her shoulders with a short black skirt, black patterned tights and stiletto boots. Dean glanced at her appreciatively as he got to his feet. He handed the number to Sam.
"Find out who owned it. Not just the last owner, you gotta take it all the way back to 1955."
"That's a lot of research."
"Well I guess I just made your afternoon." Dean said as they exited the garage.
"What's going on?" Lacey asked.
"Killer car." Lacey raised an eyebrow. "How was the spa thing?"
"Bath house. It was OK once I got through to them that I wasn't taking all of my clothes off." Dean chuckled.
"If I'd have known it was that kind of place I might have come with you." Lacey gave him a shove knocking the wind out of him a little.
"I did get my nails done too." She proffered her hands, the nails covered in glitter and bows.
"Yikes." Dean said raising both his eyebrows.
"You want me to shove you again?" Lacey asked playfully.
"No ma'am. Dean replied. Lacey laughed and linked arms with him as they headed back to the Impala.
A while later they were sat in their motel room, Sam doing research on his laptop, Lacey had kicked her boots off and had her feet up on one of the beds watching a movie. Dean opened a bottle of beer and sat down next to her.
"What we watching?"
"A Good Woman." Lacey said, her eyes transfixed on the screen.
"Right." Sam said from across the room. " I've managed to trace all of the cars previous owners."
"Any of 'em die bloody?"
"Nope, in fact the cars first owner was a cardiologist in Philadelphia, drove it till he died in 1972."
"So you're saying?"
"That Porsche is not, nor has it ever been James Dean's car. It's a fake little bastard."
"Well then what was it that killed the guy?"
"Good question."
The following morning Sam was awoken by his phone going off. He blearily reached for it and flipped it open.
"Hello?" As he sat up he glanced across the room. Lacey was curled up next to Dean, the TV still playing whatever channel it had been left on the previous night. "There's been another killing?" Sam asked focusing back on the phone call. "OK we'll be right there." Sam climbed out of bed. "Dean, Lacey." he shook Laceys shoulder and she woke up with a start.
"What's going on?"
"There's been another murder." Sam told her as Dean stirred from the other side of the bed.
"I'll get ready." Lacey replied as she jumped out of bed and went to the bathroom.
"Huh?" Dean asked shaking the cobwebs away.
"Just get ready dude." Sam said shaking his head. He began pulling clothes out of his bag. When he was sure they couldn't be overheard he turned back to Dean.
"Do you know what you're doing?" He asked. Dean stared at him as if he was stark raving bonkers.
"Getting dressed." He said slowly as if he was talking to a child.
"No I mean about Lacey."
"Oh." Dean shrugged. "There's no need to get a bug up your butt. She just ends up falling asleep with me watching movies. It's a pretty regular thing. Think she just likes the company." Sam studied him for a moment.
"And that's it?" Dean raised his eyebrows and grinned at him.
"For now."
"Dean." Sam warned. "I don't think…" Dean waved him off.
"I'm not stupid Sam. She's not your average girl I get that." Sam was about to reply when the bathroom door opened and Lacey stepped out. She was wearing jeans and black boots with a grey and pink baseball shirt. Her wet hair was pulled into a plait to one side of her head and a black hat was shoved over the top. Dean avoided the rest of the conversation by darting into the bathroom behind her and shutting the door. Lacey looked at Sam.
"What's his rush?" Sam shrugged his shoulders and went back to getting ready.
Half an hour later they were stood outside an office building surrounded by cops. Dean approached one of the officers in charge.
"Heard you got another weird one."
"Uh well it's a … little strange on the surface, I admit but uh, you know once you look at the facts…"
"William Hill died from a gunshot wound to the head. No gun, no gun powder, no bullet." Sam butted in.
"Nope nothing strange about that." Dean said giving the cop a look.
"Well there's gotta be a reasonable explanation. There always is."
"Well what's your reasonable explanation?" Dean asked. The Cop leant in and whispered.
"Professional killer."
"Come again?" Sam asked.
"Well CIA, NSA one o' them trained assassins, like in Michael Clayton." They stared at him.
"Right." Dean dragged the word out.
"You're welcome to look around but those guys don't leave finger prints."
"Mind if we talk with the witness?" Sam asked.
"Be my guest. She's not making any sense! And she's not making any sense in Spanish either."
"Right." Dean said again and they headed outside to find the witness.
"Consuela Alvarez?" Dean asked as they approached.
"Yes?" The woman asked looking up at them.
"FBI." Dean said and they showed her their badges. "Now uh, you said you saw something in the professors house right? Something in the window?"
"Estaba sacundo la basura Imire por la ventana y vi al hombre que mato al Senor Hill!" Dean looked to Sam.
"Uh Senora Alvarez. Calmese, por favor. Uh diganos lo que vio?"
"Nice." Dean grinned at him.
"Freshman Spanish." Sam shrugged.
"Era Alto. Muy Alto. Y Ilevaba el abrigo negro largo y tenia bigotes!"
"Okay uh, a tall man, very tall. With a long black coat and a… a beard?" He looked at the woman for clarification and she nodded.
"Beard." Sam nodded.
"Y un sombrero." The woman continued.
"Dude was wearing a sombrero?" Dean asked incredulously. Lacey giggled.
"Uh, a hat, not a…" Sam looked at her questioningly.
"no, no, no un sombrero alto."
"A tall hat?"
"Oh like a top hat?"
"Un sombrero alto. Muy alto" The woman said putting her hand above her head.
"What you mean like a stovepipe hat?" Dean asked imitating her gesture.
"Si."
"Oh yeah, like Abraham Lincoln."
"Si. El Presidente Lincoln." They looked at her confused. "Abraham Lincoln kill Mister Hill!"
"Huh."
"So I go home now?" She asked.
"Uh Si Gracias." Sam nodded to her.
"Gracias." Dean added as she got up.
Later they returned to the motel to do some more research as nothing the witness had said had really helped. Sam sat at the table surfing the web for any info while Dean, using a computer borrowed from the police station, re-watched the video of Cal Hawkins death. Lacey sat next to him her arms crossed on the table, her chin resting against them. She winced at the sight of the blood spattered across the windscreen.
"Whoa." Dean paused the video and leant forward peering at the screen.
"What?" Sam asked. Dean scrolled through the freeze frames for a moment before settling on one.
"It's a freeze frame from Jim Grossmans video." Sam and Lacey leant forward too. Dean was suddenly aware of how close Laceys' body was to his. Dean cleared his throat. "Am I crazy or does that look like James Dean?" He asked pointing at a reflection in one of the cars wheels.
"That looks like James Dean." Sam clarified.
"So we got Abraham Lincoln and James Dean? Famous ghosts?" He asked sceptically.
"Maybe."
"Well that's just silly." Dean leant back in his chair.
"No actually there's a ton of lore on famous ghosts. More than the, you know, not famous kinds. I'm actually surprised we haven't run into one before."
"Any Audrey Hepburn sightings?" Lacey asked sounding excited.
"Not that I can remember." Sam replied raising an eyebrow at her.
"Oh." Lacey said her smile falling, she slumped back in her chair.
"Yeah but now we got two of 'em?" Dean continued the conversation. "Two extremely pissed off ghosts?"
"Who are apparently ganking their fans."
"What do you mean?" Dean asked.
"Professor Hill was a civil war nut." Sam said indicating the page he had been reading. "He dug Lincoln."
"And Cal must have been a James Dean freak." Dean added putting the pieces together. "He spent seventeen years of his life tracking down the guys car. So you're saying we've got two super famous, super pissed off ghosts killing their… super fans?"
"That's what it looks like." Sam shrugged his shoulders.
"OK not so sad about Audrey Hepburn now." Lacey said perking up. Dean shook his head.
"Well that is muchos locos." Sam smiled.
"Muy." Both Lacey and Dean cocked their heads comically at the same time. Sam laughed. Not muchos."
"Yeah well the big question is what the hell are they doing here?"
"Yeah. Ghosts usually haunt the places they live. I mean, I get Abraham Lincoln at the White House …"
"And James Dean at a race track, but what the hell are they doing in Canton?" Sam shrugged his shoulders and began typing away on his laptop. Dean left him to it and got up from the table. He pulled a soda out of the fridge and offered one to Lace. She smiled and took it from him, their hands brushing slightly. Dean felt a jolt go through him, like an electric shock. Lacey blushed and turned to sit back down. Not even sure what he was doing Dean reached out and put a hand on her arm to stop her. Ash she turned back to him a look of surprise on her face, Sam exclaimed;
"You gotta be kidding me?"
"What?" Dean asked quickly moving to look over Sams shoulder at the screen.
"You gotta be kidding me." Dean repeated as he read what was on the screen.
@18crazybutcutealsopsycho @aprofoundbondwithdean @thing-you-do-with-that-thing @nichelle-my-belle @notnaturalanahi @impala-dreamer@deathtonormalcy56 @samsgoddess @deansleather @curliesallovertheplace @whywhydoyouwantmetosaymyname @waywardjoy@mrswhozeewhatsis @imadeangirl-butimsamcurious @kayteonline@supernatural-jackles @wevegotworktodo @quiddy-writes@babypieandwhiskey @deantbh @deanwinchesterforpromqueen @chaos-and-the-calm67 @memariana91 @plaidstiel-wormstache @teamfreewill-imagine@chelsea-winchester @fandommaniacx @revwinchester @castieltrash1@supernaturalyobsessed @winchester-writes @deals-with-demons @faith-in-dean @winchestersmolder @bennyyh @clueless-gold@deanwinchesterxreader @melbelle45 @winchester-family-business @4401lnc
#supernatural#supernatural fanfiction#down the rabbit hole#dean winchester#dean x oc#dean winchester x oc#spnfanficpond
0 notes