#embryological
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has 4 main sources of revenue.
Text

now accepting guesses as to what this embryo becomes when it matures
#evo-devo is a hell of a drug#zoology#animals#embryology#nature#evolution#can't post a source without giving it away so… sorry.#but the first author on the paper is named Gross#which is just#*chef's kiss*
7K notes
·
View notes
Text
attending!james bringing med student!reg coffee each time he's been at the books for hours. he just wordlessly puts it down, slips his arms around regulus' waist and kisses the tension out of his jaw. hums along while regulus rants about germ layers, embryology, the whole unintuitive mess of it. has to stifle his smile in the back of reg's neck because, yeah he's been there too.
#this is just me projecting my frustration ab cv embryology.. someone sedate me#wishing i had a hot attending gf to bring me coffee mid study session#jegulus#james potter#regulus black
419 notes
·
View notes
Text
My friend is 9 weeks pregnant! Her embryo is 7 weeks gestation. We call them Frijole and in this video they roll over, suck their thumb and wiggle their toes. You can also see their heart thumping!
530 notes
·
View notes
Text
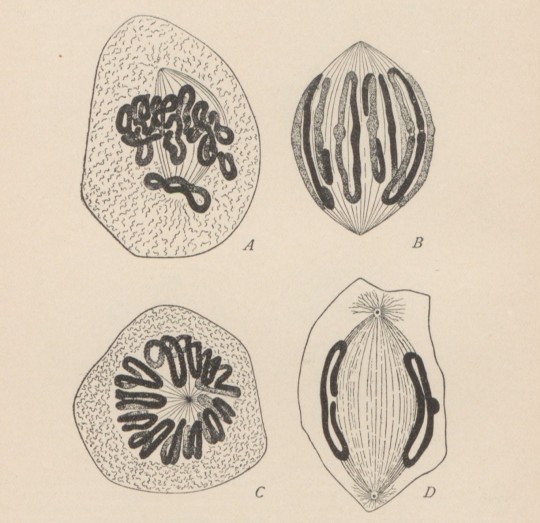
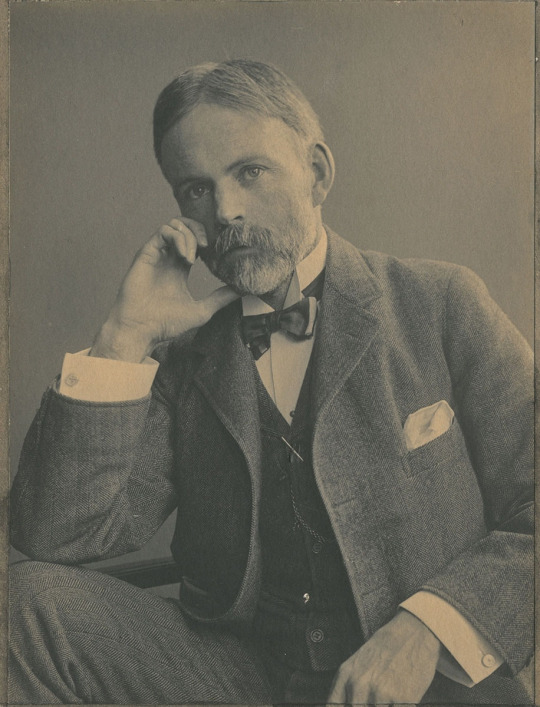
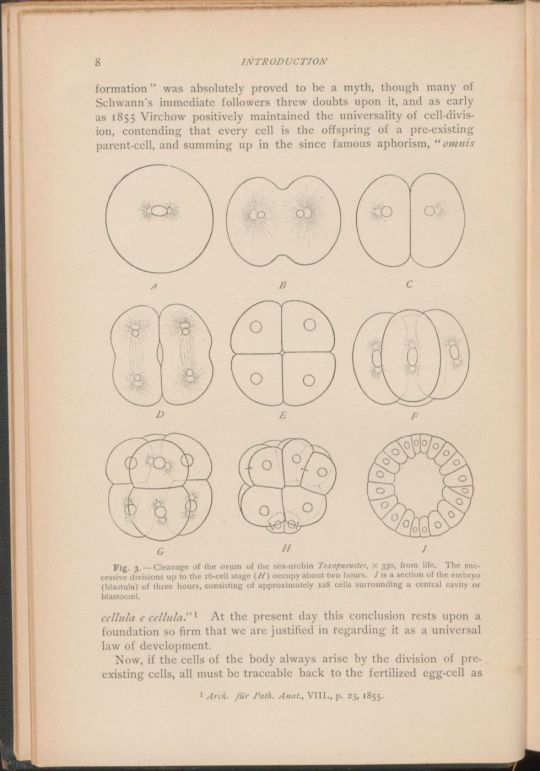


Edmund Beecher Wilson
Edmund Beecher Wilson, an American zoologist and pioneer cell biologist, died Mar. 3, 1939, at the age of 82.
learn more
#Edmund Beecher Wilson#cell biology#embryology#histsci#histSTM#19th century#20th century#history of science#Ashworth#Scientist of the Day
39 notes
·
View notes
Text

"Development of body form in pig embryo." Comparative embryology of the vertebrates. 1953.
Internet Archive
156 notes
·
View notes
Text
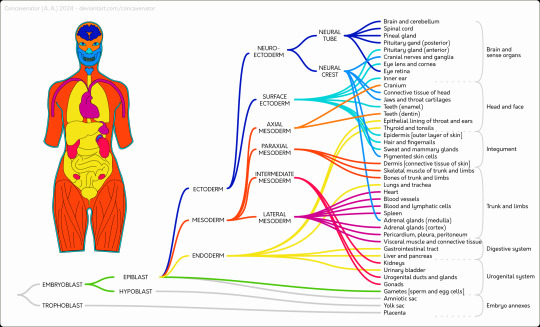
Embryophylogeny
(original picture here)
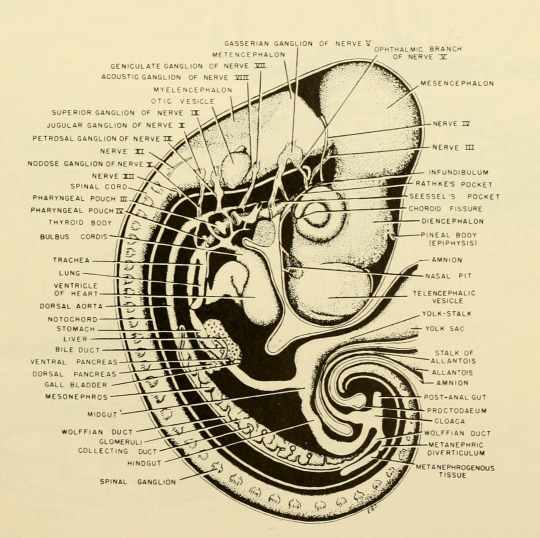
A map showing the derivation of various structures and tissues of the human body from the parts of the early embryo.
Human figure partly traced from this Wiki Commons image (public domain). Main source is TW Sadler, Langman's medical embryology (12th ed.), 2012.
89 notes
·
View notes
Text
This came across my dash via the #lgbt tag yesterday. I don't want to engage with the OP because that would get me into fights on radfem tumblr and I don't have the energy for that. But the post itself I think is worth answering, just because it's so neatly and exactly wrong.
(Not that my answer is going to spread very far, because I have 37 non-bot followers, of whom I think roughly 35.5 are just here for the nude photos. But anyway.)
Even if I agree just for argument's sake that the existence of intersex people proves that some people can have "nonbinary" sexes, or "third" sexes, and that "sex is a spectrum," how does that have any relevance to people who are not intersex? Like okay, let's "agree" for the moment that intersex people are something other than male or female. How does that make YOU, as a person who is not intersex, something other than male or female? Saying that intersex people's existence somehow makes sex "complicated" for you specifically is like saying that the issue of whether or not you can hear is "complicated" because some other people who are not you suffer from hearing loss or deafness. Like sorry but for 99% of the human population it is not "more complicated" than born with perfectly normal male genitalia = male and born with perfectly normal female genitalia = female, and chances are you fall into that 99%. Sex is not a social construct or a nebulous enigma of a concept. It is not debatable and made up in the manner that gender is. You cannot philosophize about whether there are two sexes any more than you can philosophize about whether humans have two kidneys. Someone having a missing or malformed kidney or accessory kidneys does not change the fact that humans as a species have two kidneys. Humans are gonochoric just like nearly all other animal species on Earth.
Let's start with the arithmetic. If 99% people are of binary sex, that leaves 1% of people who aren't. There are approximately 8 billion humans on Earth. 1% of 8 billion is 80 million -- about sixteen times the population of my entire country. Even just the number of intersex Americans is something like two-thirds the population of my country. This is not a negligible number of people.
There's a deeper error here, one that goes to the root not just of this misunderstanding but of many. Biology is always complicated, at every scale and at every level of explanation. It's messy, it's fuzzy, and it's always bottom-up, never top-down. Everything biological is the way it is because it grew that way. Biology never does the same thing twice.
Why does it seem like it does? Because, of all the ways you can arrange the parts of a living body, only an astonishingly tiny fraction of them actually make a living body. Any genetic mutation that nudges an organism outside of that fraction dies out and doesn't get passed on. Embryonic development is a gruelling tight-rope walk over a vast pit of non-existence.
Now for most of the body's systems, evolution has only had to produce one arrangement that works and survives. There's not an alternative plumbing plan where the oesophagus goes to the lungs and the trachea to the stomach. But for the reproductive system, evolution has to allow for two arrangements that work and survive, and it has to grow them both from the same starter kit.
What it does, therefore, is grow a body plan that works with a continuum of possible arrangements that includes both of those two. Various other points on the continuum may or may not be capable of producing viable gametes, but they're all survivable.
What biology doesn't do -- what biology never ever does -- is run new products on a conveyor belt stamping them into shape with cookie-cutters. The only things made that way are artificial constructs.
#science#biology#sex determination#evolution#embryology#lgbt#intersex#transgender#nonbinary#essentialism#biological essentialism#essentialism is not biological#biology is not friendly to transphobes
173 notes
·
View notes
Text

chordata??
19 notes
·
View notes
Text
In all seriousness though, I love that how, even though Leola has one horn, it has two branches, which just makes me Think Things about elf embryology (if she even developed from an embryo to begin with???)
Like...they probably START with a single horn that's supposed to split and move to the top of the skull as cell division goes along, but that never happened with Leola. Yet the genes for two horns kept going anyway...so we get the single horn with a small branch coming off it, in the middle of her forehead.
Single horns could also be regarded as one of the first signs that a baby might be neurodivergent. (Obviously not EVERY "unique and quirky" elf has had a single horn, but all single horned elves have been "unique and quirky")
#Aaravos how did you make your baby since you clearly selfpregged#The Dragon Prince#The Dragon Prince spoilers#TDP#TDP spoilers#speculative embryology???#Is that a thing???#fantasy autism#tdp leola
53 notes
·
View notes
Text
Ancient times. Perfection. Isolation in the desert.
Atmosphere. Atom. Causality star.
Yes, a child of earth is
conceived.
The embryo of philosophy.
Egg. Perfection. The origin in the nest.
Stamen. Pistil. A single seed.
Yes, a child of earth
grows.
The child of philosophy.
And then
lunar heaven! Mercurian heaven. Venusian heaven.
Solar heaven. Martian heaven. Jovian heaven.
Saturnian heaven. Stellar heaven. Motive heaven.
And then... The endless surface of the torus.
A single organic mechanism.
A single perpetual motion machine.
Ah, it is empty movement.
Just empty movement. Empty...
7 notes
·
View notes
Text
#let them live#abortion#anti abortion#pro life#pro life quote#quote#embryology#science#human development
86 notes
·
View notes
Text

WHY DOES NOBODY TALK ABOUT BAT EMBRYOS THEY LOOK SO COOL
7 notes
·
View notes
Text
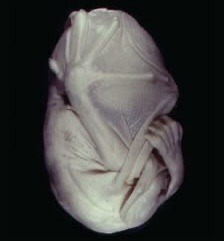
Living human embryo #24, approximately 8 1/2 wks fetal gestational age, removed via hysterotomy during the Davenport Hooker Experiments, which took place between 1932 and 1963. The embryo is prodded by a needle and you can see them react to the touch.
43 notes
·
View notes
Text





Karl Ernst von Baer – Scientist of the Day
Karl Ernst von Baer, an Estonian/Russian biologist and embryologist, was born Feb. 28, 1792, on the family estate in Estonia.
Learn more
#Karl Ernst von Baer#embryology#biology#histsci#histSTM#19th century#history of science#Ashworth#Scientist of the Day
15 notes
·
View notes
Text
Chicken embryo at 20 hours. Comparative embryology of the vertebrates. 1953.
Internet Archive
#textbook illustration#zoology#biology#embryology#chicken#chickens#diagram#science#nemfrog#1953#1950s
160 notes
·
View notes
Text

The processes that can turn an aggregate of cells into a complex organism. ADH: cell adhesion. APO: apoptosis, or selective cell death. ASM: asymmetrical morphogenesis. DAD: differential cell adhesion, sorting cells by type. ECM: secretion of extracellular material. LAT: lateral inhibition, a switch that can turn a cell into two different states. MIT: mitogenesis, or localized cell division. MOR: diffusion of a morphogenic signal. OSC: timed osclllation between different states. POL: polarization, or differential properties at different ends of a cell. TUR: Turing reaction-diffusion pattern. (pic: Newman & Bhat)
It's all well and good to say that DNA contains the instructions to produce an organism, but all DNA can do is induce the secretion of chemicals. There are no printed instructions or little foremen supervising the growth of an embryo. So how does secreting chemicals in a clump of identical cells end up producing something as complex as an animal?
Here's some tricks.

Differential adhesion. The cells of all animals have surface proteins called cadherins that bind each other into solid tissues. If all cells were uniformly covered in cadherins, they would form homogeneous spherical lumps; but if some cells are covered more or less sparsely than the others, then they will spontaneously sort by cadherin density, forming clumps and layers much like the spontaneous sorting of water and oil. If some surfaces are not adhesive at all, those will find themselves surrounding cavities. (pic: Gilbert & Barresi)
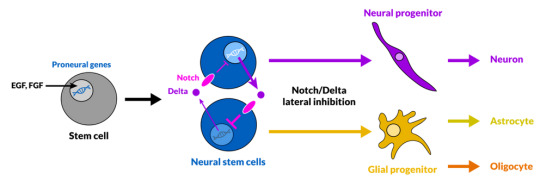
Lateral inhibition. The Notch protein forms a trans-membrane complex; when the external portion receives a signal from the environment, the internal portion breaks off and enters the cell nucleus to activate the expression of otherwise repressed genes. Thus, the Notch system works as a switch between two different states of a cell depending on whether or not it receives a particular signal. This is called "lateral inhibition" because it makes neighbor cells, such as neurons and glia in the brain, develop into complementary forms repressing each other's unnecessary genes. (pic: Audrey Effenberger, Wiki)
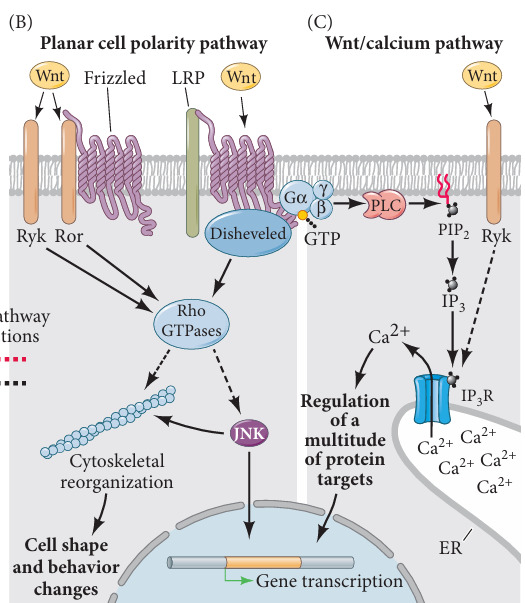
Cell polarization. "Wnt" is the name of a family of secreted signal proteins that have a multitude of functions. Among this is establishing cell polarity: through a cascade of signals, it can cause the cell's cytoskeleton -- its internal scaffolding -- to rearrange itself into an asymmetrical shape (... I think. This part of the process isn't fully clear to me), which leads to further differentiation. If the polarity involves different types or densities of adhesion proteins, then differential adhesion will sort polarized cells into distinct layers or hollow sacs and tubes -- hence, organs and body cavities. Cell polarization also leads to the establishment of the head-tail and back-belly body axes. (pic: Gilbert & Barresi)


Morphogenic gradients. When a cell or group of cells start secreting a diffusing chemical, this will naturally form a gradient with its concentration fading away with distance. This can direct differential development of cells over the organism body. Even if the chemical gradient is smooth, the morphological one doesn't need to be: cells can have different thresholds that will cause them to take one or another form. So there will be different discrete types of cells, each developing at a fixed range of distances from the source of the gradient. For example, in vertebrates, the protein Shh in the notochord induces the formation of motor neurons in the ventral side of the neural tube, which is closest. (pic: Gilbert & Barresi)

Asymmetrical morphogenesis. But then how do we end up with asymmetrical morphogenesis, for example our heart growing more on the left than on the right side? Morphogens don't have to spread only by themselves: in vertebrates, the morphogenic protein Nodal is systematically pushed to the left by beating cilia. Malformations in cilia can result into situs inversus, the development of organs in a position that mirrors the usual one. In addition (see "reaction-diffusion" below), Nodal induces the secretion of the protein Lefty2 which in turn inhibits Nodal and spreads faster, resulting into a side of the body where Nodal cannot accumulate. (pic: Green & Sharpe)
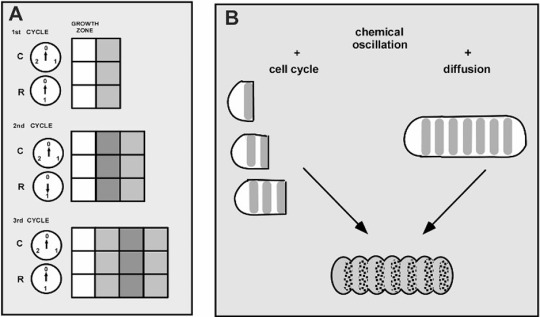
Chemical oscillation. If gene-activating factors inhibit their own synthesis, then they will come and go in regular waves, growing when they are few and decaying when they are many. This gives cells their own internal clock, which for example allows a cell to replicate at regular intervals. In multicellular organisms, the oscillation occurs in space as well as in time, as growth signals are released in waves. So they determine the formation of regular segments: for example, our vertebrae. (pic: Müller et al.)
Extracellular matrix secretion. While cells in epithelial tissues (like the outer layers of skin, or the lining of body cavities) stick closely to each other, those in connective tissues (like the inner pulp of skin, cartilage, or fat) are sunken in a matrix of various composition, but which usually contains elastic fibers of collagen. When a cell develops into a fibroblast, it starts secreting around itself the component of extracellular matrix with various mechanical properties, affecting the shape and structure of the body (especially when the cell is polarized). Even bone is simply a connective tissue whose matrix in rich in calcium phosphate mineral.

Turing patterns (reaction-diffusion). A chemical produced by a cell activates both itself and its own inhibitor. Activation is powerful but short-ranged; inhibition is weaker but spreads farther. Once a cell has produced the chemical past a critical threshold, its keeps reinforcing its own production, but also inhibits its neighbor from doing the same. At a greater distance, however, another cell or group of cells could also start the synthesis on their own. Depending on the range and power of activation and inhibition, this produces all sorts of patterns of activation: spots, stripes, waves, grids, rings. (pic: Green & Sharpe; Metz &al)
Apoptosis. Cells that receive a certain signal die, and their matter is recycled. If the signal of death is distributed according to Turing patterns, then living tissue can be cut and molded in very precise ways. For example, cells in the developing limb-bud of a vertebrate die in waves leaving behind parallel cylinders: the beginning of fingers.
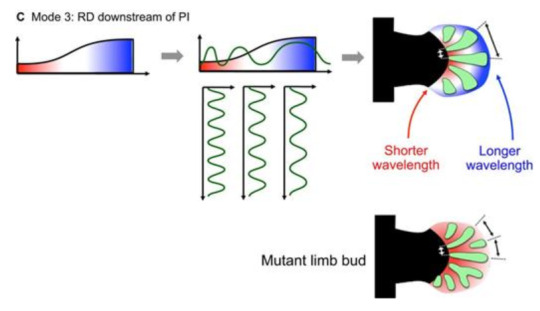
Multiple mechanisms coming together to make vertebrate limbs: a morphogenic gradient distinguishes base and tip of a forming limb; reaction-diffusion creates a Turing pattern (diverging waves) that determines where finger bones will develop; and finally apoptosis cuts away the intermediate tissue. (pic: Green & Sharpe)
SOURCES
Gilbert & Barresi (2016), Developmental Biology Green & Sharpe (2015), Positional information and reaction-diffusion: two big ideas in developmental biology combine Newman & Bhat (2009), Dynamical patterning modules: a "pattern language" for development and evolution of multicellular form
20 notes
·
View notes