#but for reference I use emergency steroids like once every OTHER year
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In 2020, 27% of US Tumblr users had an annual household income of over $100,000.
Text
Got exposed to one of my top-tier asthma triggers at work yesterday and had a miserable night's sleep, even with my rescue inhaler and my routine inhaled steroid.
So guess who got to start her emergency steroids today, which were swapped for no obvious reason from Medrol (6 days, moderate side effects) to prednisone (12 days, I am going to eat my fucking dining room chairs if I'm not careful)?
I DO feel better now that it's been 12ish hours since my first dose but AUGH.
#if you're new here my asthma is considered “moderate” and I've never had anything like a true capital-e Emergency#nor gone to the ER for asthma nor had a nebulizer treatment ever#I didn't sleep well and I was not comfortable but it's better now#but for reference I use emergency steroids like once every OTHER year#stop b think of the children
7 notes
·
View notes
Text
Wooden Blocks
Chapter 1: the first well child check
Pairing: Minato x Sakura
Rating G
TW: mentions of character death
Summary: Minato never imagined he would be raising little Naruto on his own. Kushina had found the perfect pediatrician for Naruto. She didn't realize she would be finding the perfect person for Minato as well.
For the lovely @whisperedsilvers. Blame the MultiSaku discord for this
Posted on AO3 as well
Minato sat in the waiting room. Naruto bouncing on his lap. Since his son was born nothing was like how Minato pictured it. Kushina was supposed to be by his side. Naruto was supposed to be born healthy, not premature. Minato thought back to that night.
Kushina had woken with severe abdominal pain and bleeding. She was 31 weeks along with their son. Minato had never jumped out of bed so fast. He didn’t care about all the laws he broke getting Kushina to the emergency department. It was all a whirlwind after that. She was immediately rushed to the OR for an emergency c-section. Placental abruption. He had never heard of it before, but he will never forget what took his wife away from him. She lost too much blood and didn’t get to see their son take his first breath.
Little Naruto had a rough course in the neonatal intensive care unit, NICU. He was there for over 2 months. Minato remembers the breathing tube tapped to his face after he was born. His lungs were underdeveloped. Due to the emergency situation Kushina wasn’t able to get the course of steroids before he was born. Steroids that would have helped his lungs. However, every day Naruto got stronger and stronger. It was like Kushina was helping him, giving him her strength. They were discharged with a large farewell from the staff.
Now Minato sat in the pediatrician's waiting room waiting for Naruto’s first appointment. Thankfully Naruto was able to be weaned off his oxygen before they went home. Minato found himself not sleeping at night, concerned if anything would happen to Naruto. Minato wanted to be ready. He started to doze off for a second as he was sitting up. It wouldn’t hurt if he shut his eyes for a few seconds.
Minato didn’t know how long his eyes were closed, but nearly jumped out of his seat when he heard a shrill voice.
“Uzamaki Naruto.” Naruto started to cry. Minato quickly went to soothe his son as he gathered their things. He was so focused on his son, he didn’t notice all the eyes on him from the women in the office.
“Shh Shh. It will be alright little one. Come on don’t cry.” Minato kept his voice as soft and calm as possible. He made his way to the door with the nurse. Soon they were rushed back to get Naruto’s weight, length, and head circumference. The almost calmed Naruto started crying tenfold compared to earlier. The cold wooden board and scale must have been torture for the naked baby.
After the measuring, Minato swaddled Naruto in his blanket, decorated in bowels of ramen. He would dress him once they got to the room. The exam room was brightly colored with child geared toys decorating the walls. Naruto will love playing with those when he gets older. A sting shot through Minato’s heart, just one more thing he will do alone.
“Dr. Haruno will be with you shortly. Please just leave him only in his diaper for the exam.” And just like that Minato was alone with Naruto again. He could do this. Minato just stared down at his son, his face looked so much like Kushina. Kushina had found this office a week before Naruto was born.
“Oh Minato, you will not believe the pediatrician I found. She has been out of training for 2 years. Do you know she trained under Dr. Tsunade Senju! All of the moms at the mommy to be class raved about her! We will need to schedule an appointment to meet with her closer to the due date. Oh I just can’t wait.”
This office had Kushina’s seal of approval and that was good enough for Minato. As he waited he took time to fill out more of the developmental forms. Naruto had finally calmed down and was starting to sleep cradled against his chest.
“Hello. I’m Dr. Haruno. This little guy must be Naruto and you must be his father, Mr. Uzamaki. “ Her voice was sing song, that was the first thing he noticed. When he looked up he was flabbergasted at the young Doctor. Her cascading cotton candy locks fell to her mid back. She had sparking emerald eyes that looked full of kindness. He thought about how she looked and how children must be in awe of her. She extended her hand out for him to shake. He took note of her smooth hands.
“Yes this is Naruto. I’m Minato Namikaze, Nartuo’s father.” Her grip was strong. Minato wanted Naruto to carry part of Kushina with him for life, so he gave Naruto her surname.
“Oh sorry about that Mr. Namikaze. Let’s start with any questions or concerns for little Naruto since leaving the NICU.” He was pulled out of his daydreaming with her question.
“He doesn’t sleep through the night yet and coughs when he is laying down.” Naruto was zonked out. Unlike the nurse’s voice Dr. Haruno’s didn’t seem to hurt his ears.
“Let’s see little Naruto is 3 months old, so we wouldn’t expect him to sleep through the night until 6 months of age. However every child is different so he may do it sooner or even when he is older.” Dr. Haruno smiled as she looked at Naruto.
“Now this coughing does it happen every time he is laying down?” Minato shifted in his seat to look at her better when they talked. The jostling around caused Naruto to wake up and start crying. Before he could do anything Dr. Haruno spoke.
“You have your hands full. Let me take him for a little.” Minato could only watch as Naruto was taken from his arms. This was the first time someone other than Minato had held Naruto outside of the NICU. Anxiety filled Minato’s veins. Naruto quickly quieted down with the coos from Dr. Haruno. Minato didn’t think it was fair she could calm his son so quickly.
“It is mainly at night. The NICU talked about keeping him upright after feeding and burping him frequently to help with reflux.” Minato made sure to follow all the advice he had gotten before leaving the hospital. He kept a notebook in his work bag and referred to it multiple times a day.
“Does he spit up excessively or seemed bothered by it?” Dr. Haruno didn’t even bother to look at Minato.
“He spits up a little, nothing excessive. He never seems bothered by it.” Naruto cold guzzle formula like a champ.
“That’s good. I was reading that he was placed on flovent for his chronic lung disease of prematurity. How often is he getting it?”
“I give it to him once a day in the morning. He was on it twice a day, but I was told he could be weaned down since he was doing so well.” Minato wanted to reach into his bag and look at the paperwork. He was now worried he was doing something wrong.
“How many puffs does he get in the morning?”
“Two. I give it to him every morning with the spacer we left the NICU with.”
“Perfect. How about you try giving him one puff twice a day. That way he will get the same dose, but having part of it at night should help with any inflammation in his lungs. Splitting the dose will help give him a more consistent level of medicine in his lungs. Has he had any fevers, runny nose, congestion?”
“No.”
“Will he be going to daycare or staying home?” Dr. Haruno had started to walk over to the exam table. She delicately placed Naruto on the table, after she laid out his blanket.
“He will be starting daycare next week when I have to go back to work.” After his wife’s death he was able to take some time off to be with Naruto. He was able to go back part time when Naruto was still in the NICU, but he took a couple of weeks off after he was discharged. He wanted time to settle Naruto in before starting back up at work and putting Naruto in daycare.
Minato watched as Dr. Haruno checked Naruto over. Naruto looked memorized by the doctor.
“Just to go over some general cares. Most children in their first year of life can have 10-13 viral illnesses, making it seem like they are sick all the time. Naruto should still go to daycare, but he may have a tendency to catch a cold easily. If that comes up and you have any concerns bring him in or call into the office. We don’t have to do any vaccines today, but he will need his second round at 4 months of age. I recommend having him come in at that time for another check up. Let me give you our card with the office hours and contact numbers. We do have doctors on call at night if any questions or concerns arise. It would either be me or one of the other 3 pediatricians who work in the office.” Minato took the card and placed it in his bag. He made sure to take a picture of it to save on his phone as well.
“Well I must say you have a beautiful baby boy. I look forward to seeing him in a month. Please let us know if anything comes up in the meantime.” Dr. Haruno wrapped Naruto back up in his blanket, her swaddle was so perfect he was jealous.
“Thank you Dr. Haruno. We will be seeing you again in a month.” Her smile made him melt before she bid them goodby and left.
Minato sat in the exam room for a moment. He could do this. At least they had an emergency contact number for the nights. He hoped he didn’t need to use it to much.
________________
Sakura stepped out of the exam room and sighed. She felt sorry for little Naruto and his father. She had heard from Hinata about their story. Hinata was one of the neonatologists who took care of Naruto in the NICU. She wanted to reprimand the nurses for their giggles about how attractive Mr. Namikaze was.
Sakura moved from exam room to exam room. She got coughed on by 3 patients, almost punched in the face by a 3 year old, and a teenager cursing at her. She was ready for the day to be over. Checking her watch she realized she would have to go home soon to get ready for her date. Ino had decided to set her up with a blind date, which Sakura begrudgingly agreed to. She checked her in-basket one more time before heading out.
_______________
Sakura sat nervously at the front of the restaurant. Her date was 20 minutes late. What if they stood her up? She knew this was a bad idea.
“Sakura?” A deep baritone voice brought her out of her thoughts. She looked up to see one of the most gorgeous men in her life.
“Yes. You must be Kakashi.” Kakashi gave her a dazzling smile.
“Sorry I’m late. I got held up at the office.” He was the second most gorgeous man she had seen today. Kakashi offered his hand as she stood up, which she easily took.
“No problem. What do you do?” Sakura couldn’t help but ask. Ino had told her almost nothing about this blind date. The only fact Ino found important was that Kakashi was tall and handsome.
“I am an architect. My boss wanted to go over one of the new accounts this afternoon. He has been off for family matters.” They easily fell into a conversation.
As their date winded down to a close, Sakura's phone went off.
“Sorry I have to take this. I am on call this week.” Sakura felt bad as she went outside. Kakashi gave her an understanding nod.
“Mr. Namikaze is everything alright?” Sakura could tell it was going to be a long first year of Naruto’s life.
18 notes
·
View notes
Note
Hiii, If you feel comfortable of course, I'd like to know how was your pregnancies. Where they calm? Complicated? How did you dealt with them? Did you always wanted children? Just your overall experience 😊🤗
HI!!! Oh this is a fun question, I’ll be happy to answer! This is gonna get long so I’ll put it under a cut!
So starting info: I have two children, Sis is seven and Bubba is five. I have always wanted children, ever since I was five years old and got my first actual babydoll. It’s in my blood, I’m phenomenal with children, and my body was designed for it, shaped for it even. My mother always called it “those child-rearin’ hips”. 😂
Now the background of meeting the hubs in case you haven’t read: we met in 2011, got engaged in 2011, got married in 2012, got pregnant in 2012. We weren’t playin’, y’all. 😬 So anywho, my pregnancy with Sis was fairly smooth sailing up until the end; my morning sickness with her was minor, it lasted from 5 weeks to 13 weeks but I only threw up maybe three times? The rest was just occasional bouts of minor nausea, and I had no other complaints besides my wisdom teeth finally erupting.
Around 34 weeks she tried to come out early; I was having minor twinges that didn’t really hurt, they just didn’t feel right, so to the hospital I went. Sure enough, I was having contractions that they struggled to stop. I was kept overnight for observation once they got the contractions to stop (it’s basically a shot they give you and they had to administer it thrice), given steroids to help baby’s lungs develop, and then sent home on mild pelvic rest for three weeks, aka sit down all the time unless you have to use the bathroom and NO sex.
We thought we were gonna have a thanksgiving baby... NOPE. Little Miss got offended that we didn’t want to meet her yet, so she stayed put until two days before her due date. 🙄 Cue 12 hours of walking to get me to progress enough to where we could go to the hospital. I had wanted a natural delivery but her head was tilted at a slight angle and caused back labor instead of typical labor, and I was in so much pain my body was shaking by four cm dilation. Epidural it is! I slept then, and she was born the next day around 4pm. I pushed for three hours, the epidural wore off, and I had a second degree tear. All worth it to see that tiny bundle I’d waited for my whole life. ❤
My son was a different story. He was conceived when Sis was about 15 months old, and his pregnancy was NOT fun, not in the slightest. I had fewer weeks of morning sickness with him, only from about 8-11 weeks, but they were HELL. I was nauseous all day, every day for three weeks. I hated it. I had heartburn with him from about 22 weeks on so I had to limit my diet and go on additional daily medication, and he rode so low that my sciatica was thrown into over drive.
Now see, he tried to make his appearance EARLY. I first went into labor with him at about 24ish weeks? It was minor, but to this day I cannot tell you the plot of the movie Interstellar, I was too busy counting contractions and freaking out. Fortunately they subsided, and we went on our merry way.
Then came 36 weeks. I went into labor again at the same time that I got the stomach flu. Real deal labor. My husband was in the city at a football game for work, so my Mother-in-Law came over and packed me a hospital bag while I was puking my guts out. The contractions had stopped by the time my hubs got home, so I opted for sleep and would go to the hospital in the morning if they came back.
They came back. This was different than Sis’s labor though, the contractions wrapped all the way around my belly and they felt manageable. I drove myself to the hospital after my Sis-in-Law came over to babysit, and went from being dilated from a 2 to a 4 in the space of an hour. Unfortunately, because he was only 36 weeks, he had what they jokingly refer to as “white boy lung syndrome”, which is simply that Caucasian males’ lungs do not develop as fast as girls or as other races, and so he needed to cook a little longer. Steroids again, halted labor again, pelvic rest AGAIN. Goddamn, the things I did for these babies. 😂
That lasted not quite two weeks and then I went into labor AGAIN on Christmas Eve. Just make it through the family events, child... you can be born tomorrow. Labor stopped again, and you’re about to find out why. We ended up at my 38 week appointment which was a few days after Christmas; I was dilated to a 5, 100% effaced, I was halfway there, dammit. Natural delivery, here I come! NOPE. My doc is feelin’ around and I could see concern on her face and I’m like wtf talk woman, and she says “Huh. I don’t feel his head.”
WUT.
I go in for an immediate ultrasound and sure ‘nuff, my ridiculous child is butt first, hence why labor never continued. 🤦♀️ So that afternoon they attempted an ECV (which I don’t wish upon my worst enemy, that is the most excruciating pain in my life), he wouldn’t flip, and I went into labor AGAIN. My doc made the executive decision to go ahead and pull him before my water broke and he got stuck or further risks occurred, and I agreed.
I was rushed to an emergency C-section which prep for is supposed to take two hours? They did it in one. Surgery itself is supposed to take an average of 45 minutes? They did it in 22. He was born around 9pm the same size as his sister, and had some slight breathing difficulties but by his second APGAR test he was fine.
So yeah, those are my birth stories! Thank you for letting me talk about them, I love my children with all my heart and I’d go through it all again if it meant getting to be their mother. I’d go through pregnancy again too if any of my closest friends needed a surrogate; I really didn’t mind being pregnant. ❤
1 note
·
View note
Text
BC/AD
I want to tell this story. I think it is important to tell, especially in this moment—when collectively we are straining against the changes wrought by a global pandemic.
Maybe I should start by saying that sometimes stories are something you’ve been working on in your life for years. You’ve crafted and cultivated it. Nurtured and pruned it to your liking. But this story was thrust upon me. This story began in an instant and I could do nothing but see it play out, catch up to its lightning speed pace, and hold on for dear life.
This story began on January 13, 2018 at approximately 11:30pm. It began with a sleeping child on a gurney in a hospital emergency room with his worried parents and a hesitant ER doctor.
While holding my sleeping child, I was given the worst news you could imagine: “He has blasts in his blood. When a child has these blasts it points to leukemia or lymphoma. We’ll be admitting your son tonight.” Cancer. Six letters that spell something life changing.
I remember a teacher once describing the difference between B.C. and A.D. when referring to dates in a history book. When I was a child, I used to think about it as “Before Christ” and “After Death” (meaning Christ’s death). I always thought it was such a strange and monumental way to mark time. Now, it doesn’t seem so strange. Our lives are literally divided into B.C., “Before Cancer” and A.D. “After Diagnosis.” But I’m getting ahead of myself.
For all we knew, our son was a healthy and happy almost three year old. He was a younger brother and would soon become a big brother—just two months prior to this night we had discovered we were pregnant with our third child. He liked Paw Patrol and playing soccer and other sports. An old soul from birth, our middle child both impressed and challenged my husband and I with his iron-strong will.
He had gotten a cold shortly before Christmas. But unlike before, he didn’t bounce back to his normal effervescent self. He got pale, was emotional, lost his appetite and after we spent the night of January 12th up every hour with him moaning, my husband decided to take him to the pediatric urgent care. I had to go to work that afternoon. I run a community wide children’s program in Montclair, New Jersey. My husband said he’d take both boys to the urgent care if he still wasn’t better after his afternoon nap. I met them there that evening after the event, in time to hold my son down while they fished around for a vein from which to draw blood. I hate getting blood drawn. When I was a child, I’d had to be held down because my younger brother was sick and they wanted to make sure I was okay. It traumatized me. But more than having my blood drawn, I hated having to be the one holding my child down for this. Little did I know that this would become a routine part of our existence.
While I waited with our middle son for the blood results, the other two hit up Smashburger in the strip mall next door. It was dinner time now and we were anticipating a rush once we left the urgent care to get our kids fed and ready for bed. Instead, the doctor came in and asked if there was someone local who could take care of our older son while we went to the pediatric emergency room. She was very specific: take him to [redacted for privacy]; no, you cannot go home and eat dinner with your children first. And don’t Google anything. I remember how strange that comment was—mostly because I didn’t even know what I would Google. She hadn’t told us anything about the blood results, only that we needed to go immediately to the Pediatric ER and that she’d called ahead.
We called our pastor, and his wife came over to stay with my oldest until my sister could get out to us from Long Island City.
My husband and I spent the 20-minute car ride to the emergency room trying to distract our two year old with his favorite song at the time: I’m Still Standing from the movie SING! An Elton John classic. It instantly became our mantra in the days ahead.
So there we were, the ER doctor just left the room after dropping the cancer bombshell us. I instantly started weeping, as did my husband. It was completely surreal. An orderly came in to wheel us up to the fifth floor of the hospital. We gathered our things. I was on the gurney with our still sleeping boy. It was after midnight now. January 14th. I don’t think I fully processed that leukemia was cancer until I saw the sign “Pediatric Hematology/Oncology” painted over the door we entered on the fifth floor. It was a waking nightmare.
We were 23 days in the hospital after his initial diagnosis. The first few days were a whirl of tests, surgeries and a steady rotation of doctors, nurses, and specialists. There was paperwork to sign: releasing the doctors and hospital of liability if something happened to our child when he was under sedation for a port placement, spinal tap, and chemo infusions. There was a social worker, a nutritionist, and a flurry of texts from family members and friends as we slowly put the word out.
Around day seven we got another bombshell—type 1 diabetes. Yep. We got a “two-fer.” So not only were we learning all we could about acute lymphoblastic leukemia and fielding calls, texts, and emails from family, friends, and friends of friends who knew someone with leukemia, but we were learning how to take blood glucose readings through “finger sticks,” calculate insulin to carbohydrate ratios, and give manual insulin injections to our son. Our son lost 9 pounds—which on a tiny toddler body renders a child gaunt. He started to associate finger sticks and shots with eating, so naturally, he stopped wanting to eat. They had to put an NG tube in—a tube that goes up the nose, down the back of the throat and esophagus directly into the stomach, so that we could give him Pediasure if he didn’t eat. He caught a cold somewhere around week two, which meant isolating him to his hospital room. He rarely smiled, he mostly slept and cried about taking the few oral medications he had to take daily. By the time of discharge, he could barely walk. His muscles had atrophied from being in bed for so long. Our once very active child couldn’t even climb the stairs at home or get up from a sitting position without assistance.
The day after we were discharged we were right back in the outpatient clinic at the hospital wrapping up the first of five cycles of what is called Frontline Treatment. Each cycle, outside of that first month is 60 days. But it isn’t necessarily a straight 60 days through. Continuing treatment is tied to how a child’s blood counts (red and white blood cells, platelets, and immune cells) are doing. If they are too low, they won’t continue treatment. If they are dangerously low, you’ll be spending a full day in the clinic getting a blood or platelet transfusion. Some cycles require weekly visits to clinic, some daily. Some cycles had four day hospital admittances. It was a tsunami of information and so many appointments to keep track of, along with his diabetic appointments and my OB appointments. And when we weren’t at clinic we were at home. Our son could no longer be in his daycare. We had to forego his friends’ birthday parties and play dates. It took our boy 11 months to finish Frontline Treatment.
The isolation felt overpowering at times. The parts of life we had to give up, the ways we had to change our routines to protect his fragile immune system. We were in survival mode and mostly just trying to get through each day. He hit remission in May 2018. But while he had no detectable cancer cells in his blood, it didn’t mean there weren’t any—and we would have to complete three more years of treatment.
Fast forward to March 2020. Our son has been in what is called “long-term maintenance” for a little over two years (meaning 14 months more until we are off of treatment). He’s been thriving: back at school, managing his meds well, his endocrinology team has been very happy with how we’ve managed his diabetes amidst chemotherapy and steroid treatments . . .
We’d been increasingly worried about what we were hearing in the news about a novel virus: COVID-19. We pulled our middle child out of school a couple of days before the state stepped in and mandated stay in place orders. Suddenly, the whole world was navigating a BC/AD moment: Before Coronavirus/After Disease. Everyone’s lives were instantly changed; families were having to adjust their routines for a huge unknown. Gloves and masks and disinfectant: a norm in our lives for two years now, were becoming household staples.
During our son’s frontline treatment we did not have to follow recent practices to the extreme, but since the stay in place orders, so many of our friends and family have been reaching out. “So this is what this was like.” Yes. Yes, this is a lot like what we have navigated since our son was diagnosed with leukemia. It’s hard, right?
It is hard. And the collective grief that we are all processing as a result of losing jobs, daily routines, a sense of control, and even loved ones can be overwhelming at times. But always, always amidst the darkness, there is light. There is joy and gratitude that can be cultivated and expressed. There are acts of selflessness and generosity to be witnessed and to perform. This is the “brutiful” gift of a situation like this. And really, this is an opportunity to pause and take stock of what is essential to our human existence and to a life well lived.
Nobody asked for this. Nobody wants it. But we find ourselves in the midst of it anyway. What we do and how we hold space in this time is what will matter moving forward. It will be part of our story. That is all I can offer you. In these BC/AD moments, there isn’t a simple solution or even a lot of answers. But I do know this, we will make it through. Life moving forward will not be the same. It can’t be. But we will find our new normal. My hope? That the new normal will mean that we seek and cultivate community more. That we realize we have all been helped by others and that we NEED others to make it through this life. That we have more generosity and compassion for one another because we are more aware that we’ve all been through some shit. Selah.
0 notes
Photo

Neutrogena Light Therapy Acne Mask Reviews Light therapy is an accepted form of treatment that is preferred by most dermatologists. . As more people try to find natural ways to deal with their acne, light therapy is an excellent way to complement their treatment since it is safe to use. For many years, you could only find devices to treat acne through light therapy only with dermatologist due to their size, bulk and price. Today, technology has made things simpler with more inventions of in-house light therapy treatment gadgets that go for half the price. One of the most prominent and favorite for many dermatologists is Neutrogena Light Therapy. It does not emit any harmful rays to the skin. It is FDA approved meeting all the safety standards. Neutrogena is a skin care brand that manufactures and produces beauty and skin care products in more than 70 countries. It is the number one recommended OTC brand by dermatologists in America. Here are the three most crucial light therapy acne treatment devices the brand provides. See also: [su_note note_color="#e8f8b7"] Best Foundation for Acne Skin For Complete Coverage Best Foot Massager Reviews Best Moisturizer for Acne Prone Skin [/su_note] Top 3 Neutrogena Light Therapy Neutrogena Light Therapy Acne Treatment Face Mask [amazon box="B01HOHBW6M" grid="1"] The Neutrogena Acne Treatment Face Mask is the best entry-level light therapy device if you do not want to spend too much. Dermatologists from all over the world recommend the use of the mask. It is made up of a clinically proven technology used mainly by dermatologists to clear acne from the face and allow the skin to re-heal. It is 100 percent free from chemicals and does not emit any UV rays. The mask uses both blue and red LED lights to target facial acne. The device contains 21 small LED light bulbs where 12 emit a blue ray while 9 emit a red ray. The blue light deals with the bacteria while the red light helps acts on acne inflammation. It comes pre-equipped with 30 treatment session all which should take 10 minutes each. You should only take one treatment per day. It has a wire that attaches to the battery. To use it, you need to switch the on and off button. There is a counter that helps you to keep track of the number of treatments are left. The mask automatically switches itself off after you finish a session. The Neutrogena Light Therapy Acne Treatment Face Mask has been clinically proven to have visible results within one week of use with the results continually improving over time. Ninety-eight percent of all users that use the mask are seen to show fewer breakouts. Once the 30 treatment sessions are over, you need to purchase a new Activator. Neutrogena Acne Clearing Light Therapy Acne Treatment Face Mask Activator [amazon box="B01LETUP1E" grid="1"] The Neutrogena Face Mask Activator is made to work only on the Neutrogena Light Therapy Face Mask. The activator powers a 10-minute treatment session using the dermatologist proven in-office acne technology. It –works by delivering a consistent dose of each light treatment. Since the light is for medicinal purposes, you need to control the amount that gets to your face for it to e functional. You need to use the activator for thirty days before acquiring another one. You will find free batteries inside the activator packaging. Neutrogena Light Therapy Acne Spot Treatment [amazon box="B0719SV6VB" grid="1"] If you are suffering from sporadic spots, you need to consider purchasing the Neutrogena Light Therapy Acne Spot Treatment rather than the facial mask. It is a pen-like device that produces both red and blue light which you need to focus on the specific area of treatment for two minutes three times every day to speed up the healing process. The red and blue light does not flake or burn the skin. Its unique design allows the light to surround a pimple that is targeted in the treatment effectively. The blue light penetrates beneath the skin surface to deal with the bacteria that is causing the acne while the red light goes deep into the skin to soothe and reduce the inflammation. The device does not eliminate all types of acne. However, if you want to get rid of a deep acne cyst, you need to first receive an injection of dilute steroids by your dermatologist before performing a spot treatment. It is easy to use and good for on-the-go treatment. It is FDA cleared and does not emit any UV light. The device is powered by one triple A battery. You can tell if it has low power when you see it beeps and flashes three times. It is easy to replace the cells by using a Philips head screwdriver. The device works on all skin types without leaving any mess or residue behind. Treating Acne through Phototherapy If you are dealing with stubborn acne that does not budge even after using other treatments, you should consider using light to deal with the problem. Acne forms on the skin when oils, dirt and dead sin get trapped into the skin pores. When the pores clog, bacteria on the skin leads to the pores swelling into bumps called acne. Initially, dermatologists were using UV light to clear the acne. However, UV light is dangerous to use since it may lead to cancerous growth. Therefore, doctors now use lights with specific wavelengths to kill bacteria in the skin and get rid of the toxic substances that are clogging the skin pores. The light in use for therapy is red and blue light and works only on mild to moderate acne. You need to consult your dermatologist before using BLUE LIGHT THERAPY FOR ACNE. He or she may advise on stopping to use some of your skin care products to achieve the best results. You may even receive a particular medication called photosensitizers to help your skin become more alert to the light. Both blue light and red light can treat the raised red spots on the skin surface but cannot do anything for whiteheads or blackheads. The red light reduces the reaction by your body’s immune system by reducing the pain, redness and swelling that of each zit. On the other hand, the blue light targets the bacteria that causes the acne commonly referred to as Propionibacterium acnes. The bacteria has a compound called porphyrins that when in contact with the blue light releases free oxygen radicals that lead to the death of the bacterium. Several studies have been performed to determine the effects of lht therapy on the skin. Neutrogena conducted on if such studies where 98 percent of all people that used the light device depicted fewer breakouts after 12 weeks of continuous use. The journal of cosmetic and Laser Therapy also indicated that 81 percent of all the human trials conducted by Neutrogena had fewer zits after 12 weeks while the Laser in Surgery and Medicine show a 78 percent improvement in users with acne after eight weeks of treatment. Frequently Asked Questions How often should I use the Neutrogena mask and what do I do if I miss a treatment? To attain the best results, you should use the mask for 10-minute sessions every day. You do not need to keep count of the time as the device switches itself off after the time is over. If you happen to miss any session, you should try and use the mask as soon as possible. However, you should not use it more than once I one day. Is there a need to purchase a new activator after 30 sessions? The purpose of the activator is to control the amount of light that the mask delivers ensuring that the energy is steady with time. For it to function effectively, the activator is programmed for use for only 30 sessions. Since it is a medical device, you need to ensure that the light supply is exact. Therefore, after the 30 treatments are over, you need to dispose of it and acquire a new one. Conclusion For decades, light therapy technology has been used by dermatologists in their offices. With the onset of modern technology, things have taken rather a better turn with the emergence of portable, easy to use and light therapy devices for use at home. Even so, not many devices have received the FDA approval for use by acne suffering consumers. The Neutrogena light therapy mask is indeed the BEST BLUE LIGHT THERAPY in the market since it is the cheapest of all with approval but provides the highest care you would receive from a dermatologist. The treatment covers your face as you sit back and relax. Since the device does not emit any harmful rays, it should have any side effects upon use. However, in the event of any discoloration or discomfort that lasts for more than one day, you should discontinue using the device immediately. It is essential to always consult the dermatologist before using any light therapy on your skin. Bài viết đã xuất hiện lần đầu tiên tại https://www.cosmeticnews.com/neutrogena-light-therapy-acne-mask-review/?feed_id=118&_unique_id=5e27e25acb792 #cosmeticnews #janebrody #haircare #makeup #skincare #skinconcern #beautydevices
0 notes
Text
The dangers of polypharmacy: Do you really need all of those medications?
You generally take more medications as you get older. The doctor prescribes a statin to lower cholesterol, a steroid spray for allergies, a proton pump inhibitor for reflux, and a painkiller for the knee that’s still sore after that running injury a few years back. But too many medications, sometimes referred to as polypharmacy, can become a problem—the more medicines you take, the greater the chances one medication will have a negative interaction with another and cause a serious adverse effect.
At some point, you and your doctor may need to ask a fundamental question: Do you need all of these medications?
“It’s always a little bit of detective work to figure out where the medications came from—who prescribed them and when,” says Gregory Ouellet, MD, MHS, a geriatrician at Yale Medicine’s Dorothy Adler Geriatric Assessment Center.
Adverse drug events, or unexpected medical problems that occur during treatment with a drug or other therapy, cause 1.3 million emergency department (ED) visits in the United States each year and about 350,000 hospitalizations, according to the Centers for Disease Control and Prevention (CDC).
These medical events are most common among older people—those over 65 are nearly seven times more likely than younger people to be admitted to the hospital after an ED visit, and most of the time that visit is due to a negative drug interaction. “It only takes one unnecessary medication or a negative drug combination to cause a serious problem,” says Karen Jubanyik, MD, an emergency medicine specialist.
In many cases, you may not need all the medications you’re taking, says Marcia Mecca, MD, a Yale geriatrician who directs a “de-prescribing” program at the Veterans Affairs (VA) Connecticut Healthcare System in West Haven called IMPROVE (Initiative to Minimize Pharmaceutical Risk in Older Veterans Polypharmacy Clinic). The clinic’s sole purpose is to eliminate unnecessary medications and help avoid emergency room visits for patients who are 65 or older, have multiple chronic conditions, and take 10 or more medicines a day.
“We look at people’s medication lists carefully—especially if they have a new concern, are having trouble with their memory, or are at risk for falling,” Dr. Mecca says. It’s a process that involves listening to the patient and learning about what they want and expect from a given medication, she says.
Is polypharmacy a communication issue?
One phenomenon Dr. Ouellet has seen is what’s called the prescribing cascade. “Basically, a patient was started on one medication, had side effects from that, and then was given another medication to deal with the side effects of the first,” he says. “Soon the patient has multiple medicines interacting and causing symptoms.”
Another scenario Dr. Jubanyik sees is a patient taking two types of the same treatment—for instance, a primary care doctor may have prescribed a diuretic, and then a cardiologist—who didn’t know about the first prescription—prescribes another one.
Yet another issue involves a misunderstanding of instructions. “I worked with a patient who had been taking an allergy medication year-round for decades only to learn it was for allergy season only,” says Dr. Mecca.
Many medication problems aren’t diagnosed until patients end up in the ED, where they are surprised when a doctor recommends they eliminate one, says Dr. Jubanyik.
A long-standing problem
When Dr. Jubankyik suspects a new patient in the ED is experiencing an adverse drug reaction, she works with pharmacists to investigate, often searching the patient’s electronic medical record (EMR), which she says is an invaluable tool. Before EMRs were in place, clinicians had to rely on their patients for information about current prescriptions. Or if they were lucky enough to get a paper chart for a patient, providers often had to analyze poor handwriting, buried deep in the chart, to come up with a medication list. It was often difficult to tell which medications a patient was still supposed to be taking and which medications had been discontinued.
Even with EMRs, physicians still run into problems when patients see multiple providers who each prescribe a number of medications. One medical specialist may be hesitant to interfere with a prescription made by a doctor in a different specialty, Dr. Jubanyik says. “It’s hard to tell a patient to stop taking a medication prescribed by another provider. We wouldn’t want to undermine the therapeutic alliance between the other clinician and the patient. There is a possibility that there are legitimate reasons for the medication to be prescribed,” she adds. “The explosion of specialists and hyper-specialists has made it more likely that patients will see multiple prescribing providers. Best practice dictates that they all talk frequently about each patient’s medication regimen, but realistically that does not happen.”
She recommends using pharmacist colleagues to oversee and monitor multi-provider prescribing to best advocate for the patients.
Drugs that are common culprits
There is no “one-size-fits-all” approach to eliminating medications, says Dr. Mecca. “Each patient is unique, and the approach for one patient is different than for another,” she says. Guidelines are a starting place. One resource doctors turn to is the American Geriatrics Society Beers Criteria, which is updated every few years (last updated in 2019). Beers includes multiple tables of medications with recommendations on drugs to avoid or use with caution in older patients, and known drug–disease and drug–drug interactions.
“There is a host of drugs that can cause problems,” says Dr. Jubanyik. For older people, many of the ED visits that lead to hospitalizations are because of a handful of common drugs, such as blood thinners; opioid analgesics, which have contributed to deaths from overdoses; and medications that require routine monitoring with blood tests, according to the CDC.
What’s more, some medications and combinations of medications can affect a person’s ability to think and concentrate, and cause confusion, memory loss, and delusions—symptoms that can be mistaken for dementia or Alzheimer’s disease. For older people, sedative, hypnotic drugs such as zolpidem, diazepam, and alprazolam “can really cloud their picture and make the memory worse,” Dr. Jubanyik says. “Some drugs that calm down a younger patient can have a paradoxical reaction in older patients, causing them to grow agitated and confused, and putting them at higher risk for dizziness and falls.”
Why drugs are so complicated for older people
Drugs affect the aging body differently and having this information can help people make better choices about the drugs they take. For instance, physical changes that come with aging can cause the kidneys to take longer to clear medications, which can essentially mean they’re experiencing the effects of a higher dose, says Dr. Mecca. What’s more, the liver and kidneys are the major organ systems that metabolize and clear out the byproducts of medication, and a 90-year-old’s organs are not going to function the same as a 30-year-old’s, Dr. Jubanyik says, noting that medication that doesn’t leave a person’s system can accumulate and become toxic.
Another important piece of information relates to a drug’s long-term benefit. “Many medications for chronic diseases are focused on reducing the risk of a bad outcome in the future. In studies, we see that there is often a lag time—from months to years—from starting a medication to seeing an actual reduction in the risk of a bad outcome,” adds Dr. Ouellet. “If the typical time to see a benefit is longer than a patient’s life expectancy, we may be subjecting them to adverse effects with little chance of benefit.”
Opioid medications can raise difficult questions as well, says Dr. Jubanyik, who has seen cases where patients at the end of life were prescribed opioids for pain with the assumption that they would not need to worry about addiction. But then, because of a new treatment, a patient lived longer than expected and continued to take the opioids, she says. “Family members are surprised when their grandmother becomes dependent, but there is nothing special about an 80-year-old’s brain that protects it from becoming dependent on a medication,” she says.
Underlying all of these issues is that there isn’t always good data around how a particular drug will affect an older person—clinical trials to prove safety and effectiveness usually focus on younger patients, Dr. Jubanyik says. That means a doctor prescribing a medication to an older person doesn’t always have a clear roadmap of what to expect. “Drug companies, looking at a drug that will be used mostly in 50- or 60-year-olds, don’t tend to include many 90-year-olds, who might have multiple chronic diseases, in their clinical trials. They are not going to study it in people who are on several other medications, either,” she says. “But, once that drug is approved, you learn a lot more. In thousands and thousands of older people, you start to see side effects that weren’t anticipated.”
Patients need to know what they’re taking
For these reasons, bring your pill bottles (with the original labels that include details like proper dosage) to doctor appointments and pharmacy trips, says Dr. Ouellet. Toss in over-the-counter medicines and vitamin supplements and be prepared to talk about foods or beverages that contain ingredients like caffeine.
If you are seeing multiple specialists, doctors encourage you to review medications regularly with all of them.
Yale Medicine doctors suggest asking the following questions:
Should I continue to take a drug that doesn’t seem to be helping me?
Should the dosage be adjusted?
Am I following the instructions correctly?
Could a new symptom be related to a drug?
Do the benefits outweigh the risks for a particular drug?
Could one medication help with two conditions?
If taking medicine feels complicated, buy a pill box
Even after doctors help patients eliminate medications, the daily pill regimen can be overwhelming, says Carolyn Fredericks, MD, a neurologist. She sees this become especially problematic among those with cognitive issues or dementia and says some patients will need a family member or a hired caregiver to help. Dr. Fredericks also recommends asking the pharmacy to provide medications in a blister pack so pills can be punched out each day, leaving a record of how many were taken. Another solution is to set up reminders on a mobile phone.
Or you can go low-tech. “A pill organizer box helps,” Dr. Fredericks says. Pillboxes range from simple and inexpensive ones to tech-savvy ones that make a sound when it’s time to take a pill; some of the tech-heavy ones can cost hundreds of dollars. “Even a basic one is better than nothing,” says Dr. Fredericks, adding that for some people it’s the best choice. “All the bells and whistles are great, but you want to make sure it’s something you can set up that you don’t have to be constantly rethinking. If the person is 90, they may not be technical or understand Bluetooth.”
In the end, doctors suggest trying the method of keeping track of medications that works best for you. “Missing a dose or two can lead to significant problems,” Dr. Fredericks says. “Medication only helps if it’s taken properly.”
source https://scienceblog.com/518306/the-dangers-of-polypharmacy-do-you-really-need-all-of-those-medications/
0 notes
Text
Temporary Hearing Loss Causes
Now and again listening to loss is only temporary. However, that does not imply you may not nonetheless be concerned while you first word this surprising trade for your listening to. Fortunately, among the motives why this listening to loss takes place are due to conditions that can be speedy remedied.

What reasons brief listening to loss
Temporary hearing loss
Ear infections can cause temporary
listening to a decline in children and adults. For employees who paintings in a high noise place of job or for folks that experience noisy pursuits, protecting the ears must be of extreme significance. Even brief quantities of time spent in these styles of environments can cause transient listening to lose.
If noise exposure is rare, hearing can also recover. But, persistent exposure to noise that is loud enough to purpose ringing in the ears can eventually result in permanent noise-brought on hearing loss (NIHL). Excessive noise can arise in places you can now not count on, so be always organized with a pair of inexpensive foam earplugs.
The identical holds true for those folks who pay attention to their headphones too loudly or regularly attend intense live shows. Ringing inside the ears often referred to as tinnitus usually consequences from high noise exposure. Turn down the volume or wear defensive ear system to lessen the hazard of developing permanent listening to lose.
Accumulation of earwax

Even though production of earwax is a normal method of the frame defensive the ear canal, there are instances while the wax becomes impacted or stuck in the ear canal. This blockage can cause surprising lack of listening to in a single or both ears, hindering the capability of sound waves to tour thru the ear canal to the eardrum.
When the eardrum is unable to function properly, hearing can be negatively affected. The most straightforward manner to repair regular listening to while a wax impaction is a gift is to visit a healthcare issuer who can without problems flush or eliminate the wax from the ear canal. For many human beings, the system is brief and pretty painless.
Center ear infections
youtube
While the vicinity at the back of the eardrum is invaded employing bacteria-stuffed fluid, then the disease is very in all likelihood to expand. Because the center ear contains a passageway to the return of the throat, ear infections can increase from an unpleasant cold or virus. Those infections are common in children and could affect their capability to pay attention quickly.
An infection inside the middle ear can reason a construct-up of fluids when the body is attempting to combat the disease. These fluids can put pressure on the systems of the ear which might be used in hearing amplifier, such as the middle ear bones. In some cases, these fluids motive so much pressure that the eardrum can rupture and leak blood and pus-like fluids from the ear. A ruptured eardrum may be painful. However, it can often restore itself once the infection has cleared.
The remedy for ear infections is generally a route of antibiotics. If you are prescribed antibiotics for an ear infection, do not prevent taking them merely due to the fact you feel higher. Keep taking medicine until it's miles gone to ensure you've got worn out the contamination completely.
What's temporary hearing loss deafness?
Surprising sensorineural listening to loss (SSHL), typically called extraordinary deafness, occurs as an unexplained, fast loss of hearing—commonly in a single ear—both right now or over several days. It must be taken into consideration a scientific emergency.
Everyone who experiences SSHL needs to go to a physician right away. Now and then, people with SSHL remove seeing a physician because they think their listening to loss is because of hypersensitive reactions, sinus contamination, earwax plugging the ear canal, or other standard conditions. But, delaying SHHL diagnosis and treatment may also decrease the effectiveness of treatment.
9 out of ten human beings with SSHL lose hearing in handiest one ear. SSHL is identified by accomplishing a hearing check. If they take a look at suggests a lack of at least 30 decibels (decibels are a degree of sound) in 3 connected frequencies (frequency is a degree of the pitch—high to low), the hearing loss is recognized as SSHL. As an example, a hearing loss of 30 decibels would make conversational speech sound extra like a whisper.
Many humans are aware that they have SSHL once they wake up in the morning. Others first are aware of it while they are trying to apply the deafened ear, inclusive of when they use a telephone. Nonetheless, others word a noisy, alarming "pop" directly earlier than their hearing disappears. Human beings with temporary hearing loss causes frequently come to be dizzy, have ringing in their ears (tinnitus), or each.

Approximately half of the human beings with SSHL will recover a few or all of their listening to spontaneously, generally inside one to two weeks from onset. 80-five percent of folks that acquire remedy from an otolaryngologist (a physician, occasionally called an ENT, who makes a specialty of sicknesses of the ears, nose, throat, and neck) will recover a number of their hearing.
Experts estimate that SSHL strikes one individual consistent with five,000 every 12 months, typically adults in their 40s and 50s. The real wide variety of recent instances of SSHL every yr might be a whole lot better because the condition often is going undiagnosed. Many human beings recover fast and by no means seek clinical help.
What reasons temporary hearing loss deafness?
Most uncomplicated 10 to fifteen percent of the people diagnosed with SSHL have an identifiable reason. The maximum, not great ideas are:
Infectious illnesses
How is temporary nano hearing aid review deafness identified?

To diagnose SSHL, a physician will use listening to check referred to as natural tone audiometry. This test helps her or him to determine if the listening to loss is caused by sound not achieving the internal ear (due to an obstruction together with fluid or ear wax) or by a sensorineural deficit (because the listener isn’t processing the sound that reaches it). Pure tone audiometry can also display the range of listening to what's been lost.
If you are diagnosed with temporary hearing loss deafness, your health practitioner will possibly order different assessments to attempt to determine an underlying motive on your SSHL. These checks might also encompass blood assessments, imaging (generally magnetic resonance imaging, or MRI), and balance assessments.
How is temporary hearing loss deafness treated?

The maximum common treatment for surprising deafness, especially in cases where the cause is unknown, is corticosteroids. Steroids are used to treat many extraordinary issues and generally paintings with the aid of lowering infection, lowering swelling, and helping the frame combat infection. Steroids are usually prescribed in pill form. In recent years, direct injection of steroids at the back of the eardrum into the middle ear (from right here the steroids journey into the inner ear), referred to as intratympanic corticosteroid therapy, has grown in recognition.
In 2011, a clinical trial supported utilizing the NIDCD confirmed that intratympanic steroids were no less valid than oral steroids, however, have been much less comfortable typical for sufferers. They stay an option for those who can’t take oral steroids.
Additional remedies can be wasted if your health practitioner discovers an actual underlying reason for SSHL. For instance, if an infection causes your SSHL, your doctor can also prescribe antibiotics. In case you’re taking pills recognized to be toxic to the ear, your doctor may additionally inform you to forestall or switch to some other drug. When you have an autoimmune situation that causes your immune device to assault the inner ear, you may want to take drugs to suppress your immune system.
What research does the NIDCD help on surprising deafness?
Because so little is understood about the reasons of maximum cases of SSHL, researchers are studying how modifications inside the internal ear, such as disrupted blood flow or inflammation, may additionally contribute to hearing loss. Researchers also are trying out new ways to apply imaging to help diagnose SSHL and doubtlessly hit upon its reasons.
In which am I able to find new statistics approximately SSHL?
The NIDCD continues a directory of agencies that offer facts at the normal and disordered procedures of listening to, balance, taste, smell, voice, speech, and language.
#hearing loss deafness treated#nano hearing aid review#temporary hearing loss causes#Accumulation of earwax
0 notes
Text
Daniel’s Nerve Cancer Story
New Story has been published on https://enzaime.com/daniels-nerve-cancer-story/
Daniel’s Nerve Cancer Story
Daniel was an otherwise healthy toddler until he suddenly started spitting out his food at meals, having recurrent fevers, and experiencing sore knees. He endured months of misdiagnosis before doctors identified advanced neuroblastoma, a rare cancer of the nerve tissue. At Memorial Sloan Kettering, he received an innovative therapy that activated his immune system to fight the cancer.
In June 1989, at the age of two and a half, Daniel, who had always been a good eater, started spitting out his food regularly at meals. A large, apparently healthy child who was at the upper end of the height and weight charts for his age, Daniel had never previously experienced any significant health problems. This sudden change was very troubling to his mother, Karen, who, at the time, had just given birth to Daniel’s brother, Michael. “I spent all of my well-baby visits for Michael inquiring about Daniel,” Karen remembers.
Karen asked the pediatrician to do a chest x-ray, believing that some sort of obstruction must be preventing him from swallowing his food. The pediatrician refused, insisting that he did not want to expose a two-year-old to what he felt was unnecessary radiation.
At the same time, Daniel began to develop recurring fevers not seemingly related to any other symptoms. While both Karen and Daniel’s father, John, found these developments to be worrisome, the pediatrician reassured them that such symptoms were normal childhood occurrences. By September, Daniel’s condition had worsened. He came down with a different cold or flu almost every week, but, still, the pediatrician was not concerned, blaming the continual illnesses on nursery school, which, Karen was quick to point out, Daniel did not attend. “I just thought there was definitely something seriously wrong with him,” she says. “It was my mother’s intuition.”
Tumor Hiding — in Plain Sight
One morning in early October, Daniel woke up crying. Unable to walk or crawl, he told Karen that his knee hurt. Karen took Daniel to the pediatrician immediately, whereupon she was told to go to the emergency room of their local hospital in New Jersey to meet with an orthopedist. After a long, painful day of waiting in the ER, the orthopedist arrived. Despite Karen’s pleading for an x-ray of Daniel’s knee, the orthopedist, believing that a virus located in the hip was the cause of Daniel’s pain, ordered x-rays of only the hip. When the x-rays came back, neither the doctor nor the consulting radiologist saw anything of concern in Daniel’s hip. (Later, when Daniel was finally correctly diagnosed with neuroblastoma, doctors at Memorial Sloan Kettering reviewed these initial x-rays and identified the presence of a large tumor in Daniel’s spine — a tumor that had been missed by the previous doctors, who had been looking only at the hip portion of the x-rays.)
Because Daniel’s fevers had never dissipated, the pediatrician ordered a series of blood tests, the results of which all appeared normal. The pain, fever, and absence of a diagnosis continued through November, even after the pediatrician referred them to a pediatric specialist for a second opinion. Throughout this period, Daniel’s doctors, suspecting arthritis, considered sending him to a rheumatologist in Manhattan, but since none of the blood tests confirmed its presence, the referral was never made. Instead the pediatrician advised Karen to treat Daniel’s pain with Tylenol and told her that she could rest assured that whatever was going on with Daniel it was minor, since all the tests ruled out anything serious.
Prayers and Supplements
By Thanksgiving, Karen and John were at the end of their ropes. “I didn’t feel very thankful,” Karen says. She felt helpless as Daniel’s fever and intense pain persisted. Karen adds, “I just prayed, ’Lord, I know I should be thankful, but please show us the cause of Daniel’s suffering!’” With few options remaining, in early December Karen and John took Daniel for a painfully uncomfortable two-hour car ride to a highly recommended naturopathic doctor. The naturopath prescribed $400-worth of vitamins and supplements without even examining Daniel. “I felt so sorry,” Karen recalls, “that we caused Daniel to endure so much extra pain on this long trip, in our desperation to find an answer to Daniel’s suffering.”
It was a really big help knowing that these are caring human beings helping you.
John ErdDaniel’s Father
Reflecting on those early weeks of December, Karen and John say they noticed that Daniel’s pain had moved from one knee to the other knee, then from the knees to his hip. He also started to complain of a “tummy ache.” When Karen asked him to point to where it hurt, he pointed to his back. It turned out that “tummy ache” was Daniel’s catchall phrase for “pain.”
Finally, a Doctor Who Listens
It was around this time that Karen made a conscious decision to place everything in God’s hands. When the stress over Daniel’s condition began to get the most of her, Karen concentrated on reassuring Bible verses like Proverbs 3:5-6: “Trust in the Lord with all your heart and lean not on your own understanding; in all your ways acknowledge Him, and He shall direct your paths.” “Various scripture passages reminded me that it is God who is in control,” Karen says. “After much prayer and reflection, I thought perhaps a rheumatologist has seen something like this.” In mid-December, she insisted that the pediatrician provide her with names of rheumatologists, since Daniel’s severe knee and hip pain resembled the symptoms of arthritis. As she pondered the names of the doctors and hospitals given to her, Karen prayed that God would make it extremely obvious to her where to bring Daniel.
When Karen called to schedule an appointment with Dr. Thomas Lehman, a pediatric rheumatologist at the Hospital for Special Surgery in Manhattan, the doctor himself answered the phone. The receptionist was strangely absent from her desk, Dr. Lehman explained, so while he and Karen waited for the receptionist to return, Dr. Lehman proceeded to inquire about Daniel’s symptoms. “He listened for almost 30 minutes,” Karen remembers with appreciative amazement. A further sign to Karen that her prayers were being answered, Dr. Lehman just happened to have an opening at eight o’clock the following morning. Karen could not help but think that perhaps Dr. Lehman would be the one to finally diagnose Daniel’s mysterious illness.
It was nearing Christmas when Karen and John took Daniel to the appointment with Dr. Lehman. They remember his excitement at driving across the “Christmas bridge”— the George Washington Bridge, which connects northeastern New Jersey to upper Manhattan. Almost immediately, Dr. Lehman proved to be different from Daniel’s previous doctors. “He was wonderful!” Karen gushes. “None of the other doctors had wanted to hear the full chronology of Daniel’s illness, but Dr. Lehman wanted to know everything since he was in utero.” Karen is quick to mention, too, that as a physician Dr. Lehman recognized the utter importance of listening carefully to the mother, who knows her child best.
After absorbing the details of and asking questions about every iota of Daniel’s condition, Dr. Lehman said that Daniel was exhibiting many of the symptoms of some rarer types of juvenile rheumatoid arthritis (JRA). While waiting for the results of the blood tests, Dr. Lehman prescribed Daniel the non-steroidal anti-inflammatory drug naproxen used to treat a rare form of JRA.
At Last, a Diagnosis — “Daniel Has Cancer”
Daniel appeared to improve over Christmas, but on the evening of New Year’s Day he complained that his chest hurt. When Karen and John lifted his shirt to see what was wrong, they were horrified to find that his chest was swollen like a barrel. They notified Dr. Lehman, who insisted that they bring Daniel in first thing the following morning. “And we got a phone call from his office before 7 am to make sure we were coming,” Karen notes. “At that point,” John remembers, “we knew it was bad, but we still never thought cancer.”
Karen spent the day and night with Daniel at the hospital, as he received blood tests and the chest x-rays that Karen had requested of Daniel’s previous doctors six months before. Early the next morning, waking next to Daniel in his crib, Karen overheard someone in the hallway mention “the big C.” Suddenly, a voice in her head said, “Daniel has cancer.” Shortly after, Dr. Lehman walked in the room and told Karen that Daniel most likely had cancer, possibly neuroblastoma, but that it was treatable.
“After I calmed down a bit, I said I needed to call my husband, although I could barely utter the words through my tears,” Karen says. “It was such a huge shock, but it was also a great relief to finally have a diagnosis,” she adds. “The next thing Dr. Lehman told me was that he had already contacted the best neuroblastoma oncologist in the world, Nai-Kong Cheung from Memorial Sloan Kettering Cancer Center. Little did I know that he literally was the best doctor in the world!”
Dr. Cheung arrived later that afternoon having already studied Daniel’s blood samples and the chest x-rays, which showed a large mass in his chest. After more tests and scans, he told Karen and John that Daniel had advanced stage IV neuroblastoma, which is a relatively rare cancer of the nerve network that carries messages from the brain throughout the body. Dr. Cheung recommended that Daniel be transferred to Memorial Sloan Kettering to begin treatment at once. “We very quickly knew, after speaking to a number of people, that Memorial was the best place in the world to treat this,” comments John.
New Treatment Provides New Hope
When they arrived at Memorial Hospital, the Erds were informed that a new treatment protocol called immunotherapy had recently been approved for patients with neuroblastoma. This was welcome news because, at the time, no child with stage IV neuroblastoma had been completely cured with the standard therapy. Immunotherapy uses the patient’s own immune system, through the injection of what is known as a monoclonal antibody, to help fight the cancer. The monoclonal antibody attaches to a marker on the surface of neuroblastoma cells, which becomes a target for the patient’s immune system to attack and kill the tumor. Daniel, at three years old, would be one of the very first patients in the world to receive this innovative protocol.
But first he would have to undergo standard chemotherapy to reduce the size of the tumor, which had invaded his knee and hip bones, a number of his ribs, as well as his spinal canal. It had taken so long to make the correct diagnosis that the tumor now blocked his spinal fluid from circulating and was crowding his organs, including his lungs, to such an extent that one of his lungs collapsed during the initial surgery to install the chemotherapy port in his chest.
The doctors informed the Erds that the entire treatment process would take eight months. To ease Karen and John’s commute, Karen’s parents quickly volunteered to take in the couple along with Daniel’s eight-month-old brother, Michael, for what turned out to be almost an entire year. “Words cannot express how thankful we are for the prayers and support of our families and so many others throughout our ordeal,” says Karen.
The Power of Childhood Resilience
Daniel was vomiting on and off throughout the night of his first chemotherapy treatment, which also happened to be his third birthday. But by the next morning, when Karen comforted him, saying, “You poor baby, you were so sick last night,” he remembered nothing. He was more interested in going to the hospital playroom, which he had seen the day before. “That’s the one positive thing about having cancer at that young age,” Karen explains. “The younger kids do better because all they know is today,” adds John.
Dr. Cheung was amazed at Daniel’s almost immediate positive response to the chemotherapy. When he came to see Daniel the following Monday, he found the three-year-old happily running around the playroom, seemingly free of pain. Unfortunately, the entire process was not as easy, with Daniel experiencing various infections, including a very serious case of septic shock. Throughout it all, Karen and John asked many questions, a practice that Dr. Cheung encouraged. “He told us, ’Doctors don’t know everything. In many cases, we try something and if that works, then we continue down that path,’” John recalls. “He was the most humble, selfless, caring doctor I have ever met,” Karen adds.
Everybody in the neuroblastoma team is thrilled to know that Daniel is coping well, and that he learned the art of healing in nursing school, which will allow him to give back to those less fortunate.
Nai-Kong V. CheungNeuroblastoma Program Head
And it wasn’t just Dr. Cheung. Once the chemotherapy had shrunk the tumor enough to allow the bulk of the remaining portion to be surgically removed, Michael P. La Quaglia, a pediatric surgeon specializing in treating children with neuroblastoma, performed Daniel’s delicate surgery in August. “When we initially met Dr. La Quaglia, after listening to our story he said, ’I can’t imagine what you are going through.’ He was so personable and caring right from the start. It was a really big help knowing that these are caring human beings helping you,” John says.
Success — Daniel as a Happy Young Adult
Between the chemotherapy, the monoclonal antibody immunotherapy, and the surgery — which together accounted for the 350 days Daniel spent in the hospital during that fourth year of his young life — the tumor eventually disappeared. “Daniel’s positive attitude and compliant nature were so helpful throughout the entire ordeal,” Karen remembers. There were a number of post-treatment-related health concerns, including some developmental delays, but Daniel went on to be a smart and happy child, adolescent, teenager, and, now, young adult.
Inspired by all the remarkable healthcare workers he has met during his treatment, Daniel has decided he wants to give something back and is currently studying to receive his degree in nursing. He is also an avid and talented artist, and has been actively involved in hockey, paintball, and snowboarding with his brother, Michael, and friends. Looking back on the long, twisting road that has led them as a family to the present, the Erds, fortified by their faith in God, take nothing for granted and are able to appreciate the great gift of life that is presented to them each and every day.
The Erd family dedicates this story of courage and resilience to Daniel’s loving grandparents — Henry and Lida Erd, and Anton and Kay Thomasen.
#chest X-ray#child with stage IV neuroblastoma#children with neuroblastoma#large tumor#orthopedist#Cancer
0 notes
Text
Greetings fellow travelers,
I hope that wherever you’re reading this from, you are safe.
I haven’t been safe in awhile.
Yes, I have a roof over my head. (A new, expensive one at that; first year home-ownership can be stressful).
Yes, I have food and water. (Well, sometimes there’s food – usually the fridge is empty-ish and even when it’s not, I’m not really into eating it.) This fact alone makes me safer than millions and millions of people.
I am – generally speaking – not in danger.
Except last week. Last week, I was in a lot of danger. And it wasn’t the first time.
It comes as no surprise to anyone following my story that as a “Professional Patient” I spend most of my days balancing doctors appointments and symptom-tracking and medications. To be honest (and you should always be honest, right Justin?), I’ve been doing a truly shitty job managing my illnesses. It starts simply enough – one bad day. That bad day leads to two, and by then I’ve decided nothing I could do matters and I let go of the controls. Sounds healthy, right?
So a couple of weeks ago, as I was juggling my annual OBGYN visit, IUD discussions, a urology referral, a visit to UNC to discuss my constant nausea and further testing, a mammogram, vision testing for new glasses and contacts (and WAY more money than we have), my therapy visits and then 3 or 4 “normal” appointments, I kind of lost my mind.
The thing is, it wasn’t even beyond the scope of normal; that’s a pretty average week in my life. Where things started to go sideways was in the creeping, slinking, insidious feeling that an MS relapse – or something worse – was coming on. I’ve described this enough times that I feel we are all comfortable with what this looks like, so I’ll just summarize by saying that at this point in the story I was no longer in control of my motions, thoughts, words or feelings.
When Thommy and I went on our annual wedding anniversary trip in early October, we spent most of our time playing the previously referred to “ER or nah??” game. I didn’t want to go to an ER out of state (we were in Tennessee) so we just assumed the worst was yet to come and tried to enjoy what we could of the Smokey Mountains. BUT, because my brain wasn’t working properly, I forgot to pack both my cane AND my handicap placard, so we weren’t able to do much sightseeing or exploring. In fact, we barely left the condo. Since we’ve been married for 9 years, and together for 13, we don’t need a lot of special attractions to enjoy a trip; just being in each others’ presence is special enough.

At the Tennessee Welcome Center
So let’s catch up: we got home, the symptoms got way worse, and on Friday, October 27th, I went again to see my primary care doctor. He took an X-Ray of my neck first to see if that could explain some of the symptoms. Luckily, it did a little – I now have 3 herniated discs and something wrong with the curvature of my spine – and had we not had more pressing issues he said we would be discussing physical therapy, cortisone shots and possibly surgery – but since I couldn’t feel my leg or finish a complete sentence, we had bigger problems.
He sent me over to the hospital as a direct admit. He assured me they would give me sedatives before the MRI of my brain, thoracic and cervical spine (a 2 hour procedure), but the hospital was experiencing a severe shortage of IV Valium so they gave me Ativan instead, and it did nothing, except possibly make me MORE agitated. Over the course of my stay they tried 7 IVs. 2 blew. One nurse cried and I did everything I could to convince her it was me, not her.
It is now Sunday, November 5th and it hurts just to type this. But what I want to say is important; I was diagnosed as having another MS flare.
After 3 MS medications THIS YEAR ALONE.
After the hell of Ocrevus JUST TWO MONTHS AGO.
The reason MS patients put up with all the bullshit is to STAY OUT of relapses. I tortured myself all year just to end up here anyway. And that’s JUST the MS – never mind everything else in my body hatching plans against me.
So. They prescribe 3 days of IV steroids (WHY, GOD, WHY?), fluids and pain management. Fine. I’m pissed but I can do this. What’s 3 more days in the hospital? I am safe.
Except.
Except…
I can’t do it. I am not safe.
A psychiatrist comes to talk to me on the day of discharge. “Are you safe at home?”
(Mental checklist: roof, food, check.)
“Yes.”
“OK,” she says, “do you have thoughts of hurting yourself or others?”
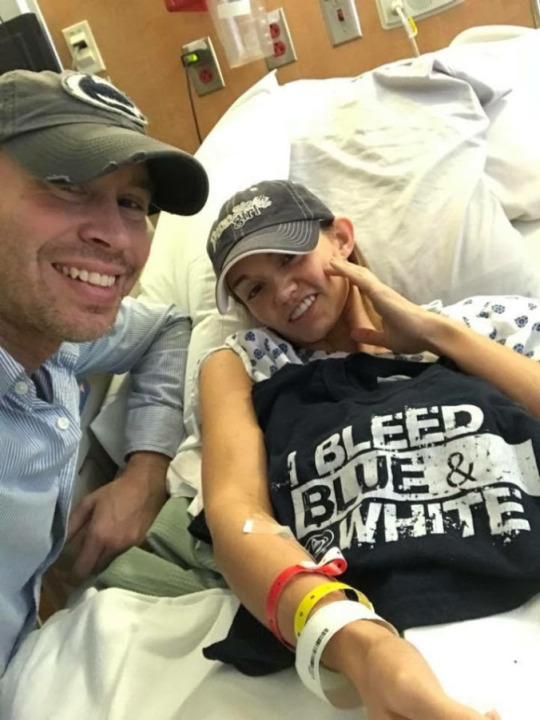
Let’s do the easy one first. Do I want to hurt others? Like this guy – this guy here who SLEPT IN A CHAIR FOR 3 DAYS AND BARELY LEFT MY SIDE AND DECKED OUT OUR ROOM IN PENN STATE STUFF FOR THE GAME DESPITE THE FACT THAT I KEEP YELLING AT HIM AND CRY INCOHERENTLY?? No. No, I do not want to hurt him.
(Well, I didn’t. But now that I’m at home, in pain, miserable and riding steroid rage, ummmm…..)
But do I want to hurt myself?
Yes. I want to find a way to trump the pain I’m in every day, I want to be the one doing the hurting, actively, so I’m no longer passively being injured, I want it to be quiet, I want it to stop, I want it to end. Please. Make it all stop.
“Would you allow yourself to be voluntarily committed to our behavior health unit?”
What’s left to hide from? What’s left to be scared of? I’ve seen the worst, I’ve felt the worst, I’ve been in the dark for a long time.
What it feels like she’s asking is, “Do you want to save what’s left of you?”
“Yes.”
And that’s where another story starts and ends. The only other time I’ve been hospitalized for mental health issues since Renfrew, and this time it was only 3 days because on the chaotic and teary night of admission I signed my 72 hour release form. (They really should make you wait until morning to do that, but what do I know…)
So basically I asked to leave before I had even fully been processed.
But that’s OK because 3 days in a psych unit is a powerful time. Every single person you meet changes you forever. And I want to do justice to that story so we’ll save it for another day.
But what I want you to know now is that on Monday, November 6th, I will start a 6 week intensive partial hospitalization; that means from 9am to 1pm I’ll be in intensive therapy, both group and individual and I’ll meet each week with a psychiatric nurse to continue to adjust my medications and with a psychiatrist to keep this journey moving. In addition, I can still see my normal therapist once a week, who I’ve been seeing for two years, and who has been remarkable.
There are three other things I want you to know, and they are so important to me, that I’m asking you to really hear the words in your head – and I’m asking you to remember.
1.) I would be dead right now if it wasn’t for Thommy, my mom, a handful of the best friends I actually don’t deserve, and a tribe of “Rhea Team” warriors who pray for me and send me their positive energy and their love and their notes and their gifts and who keep showing up despite the tedious repetition of my illnesses and shortcomings. I know that I am blessed. I do not take it for granted. Please keep reminding me of the good things – please keep your words of love and light coming; it’s my way out of the darkness.
2.) You need to vote better. Sorry if that’s whiplash but it’s true. You and me both. I am getting the most amazing, thorough and continued treatment because of insurance. There was a time I didn’t have that. And there were people I met in the hospital who were released before they were stable because of insurance. Cuts to mental health services, Medicare, Medicaid, etc, literally, literally, literally KILL PEOPLE. I might be one of them. Vote in every election you can for leaders who will protect those services. I can’t believe this country works that way but here we are.
3.) Mental health stigma needs to end. And it can start with you. Stop using the word “crazy” a dozen times a day when it’s not necessary. That’s the easy one – challenge yourself today and see what happens. Don’t use diagnoses as adjectives. OCD, bipolar, schizophrenia, manic/mania, depressed, anorexic/bulimic, PTSD, cutting/cutters/self-harmers … all those things are real life. They can be nightmares that people may never wake up from. Some of us will get help and regulate it but we ALL need to stop carrying around the shame of it. It is not a punchline to your shitty joke. If someone trusts you enough to share their story with you: listen without judgement. You don’t have to fix them. You don’t have to feel their pain to help them through it. You can hold space with love and respect and allow them to process their emotions freely. Not everyone is ready to accept help – it is not your job to lecture them. Memorize the number to the suicide hotline (1-800-273-8255) so that you can provide a resource to someone is crisis. (Obviously, if it’s an emergency, call 911). But from experience, I can say that I’ve lost track of how many times I’ve had a meltdown on the phone with someone while I told them I couldn’t make it one more day – and the act of simply being heard has kept me here one more day.
One more day.
That’s what’s left.
Or, like we talked about in the hospital, one more minute. It’s 7:31am right now. Can I make it until 7:32am? What can bridge those 60 seconds? Breathing? Medication? A phone call?
I know I said I needed you to know 3 things, but I lied, there’s one more:
I am not ashamed. As someone with complex mental illnesses AND complex physical illnesses, stuffing that all inside and hiding it from the world is what usually gets me into the darkest recesses of my mind and keeps me buried. As someone with mental illness, I *DO* feel guilty, all the time, for hundreds of things, real and imaginary; but, what I don’t feel guilty about, is sharing this with you. There is a level of self-loathing I experience that I didn’t even have words for until I was on the psych unit, but my head will not hang one inch lower after posting this and sharing it. I hope if you read this and you want to talk, you reach out. I hope if you read this, and you are so inclined, you share it with your circle because there might be someone who needs to read it and know help is out there and they don’t have to feel alone or ashamed.
I’m redefining myself with the pieces of what’s left; and with each new illness and test and hospitalization and med change, etc., I do feel like I lose some of the person I wanted to be. Or at least the person I thought I was. But there is so much power in realizing you can create someone new. And know this: if you’ve had to do this (I mean, REALLY, do this): you are a fucking superhero. Suit up. Here’s your cape…
xoxo
Rhea
What’s Left. Greetings fellow travelers, I hope that wherever you're reading this from, you are safe. I haven't been safe in awhile.
0 notes
Text
Liberal Jimmy Kimmel is making a joke of health care
Jimmy Kimmel may be a funny man, but he doesn’t understand Obamacare, according to a U.S. senator who the late-night TV host slammed this week as dishonest in describing a Republican alternative to the health care law.
Sen. Bill Cassidy, R-La., one of the chief authors of legislation to partially repeal Obamacare, sought to make himself clear Thursday morning on a friendlier show.
“Jimmy doesn’t understand, not because he’s a talk show host—[but] because we’ve never spoken,” Cassidy said on “Fox and Friends” of Kimmel’s contention that Senate Republicans’ bill would abandon Americans with pre-existing medical conditions.
“He’s only heard from those on the left who are doing their best to preserve Obamacare,” Cassidy said of Kimmel and his appraisal of the bill. “He’s not heard from me, because we’ve not spoken.”
youtube
Cassidy, a physician, apparently meant they haven’t talked about the details of his bill. The legislation, drafted with three fellow Republican senators—Lindsey Graham of South Carolina, Dean Heller of Nevada, and Ron Johnson of Wisconsin—would repeal Obamacare’s mandates requiring individuals to obtain health insurance and larger employers to offer it.
Other conservatives came to Cassidy’s defense on the particulars of the so-called Graham-Cassidy legislation.
In his own interview with “Fox and Friends” Thursday morning, Mike Needham, chief executive officer of Heritage Action for America, the lobbying affiliate of The Heritage Foundation, said Kimmel’s estimation of the Graham-Cassidy bill was incorrect.
“What Section 106 of the bill says is that every single state has to make sure that there continues to be affordable access for people with pre-existing conditions,” Needham said, adding:
The entire thing is kind of what is wrong with the way we talk about policy in this country. I am sure Jimmy Kimmel is a nice guy, I am sure he is very well intentioned, but he is both wrong on what this bill does, and he doesn’t understand. There’s a whole bunch of conservative ideas as to how we can take care of people with pre-existing conditions.
youtube
President Donald Trump, who had announced he would sign the Graham-Cassidy bill, tweeted Wednesday night:
Senator (Doctor) Bill Cassidy is a class act who really cares about people and their Health(care), he doesn’t lie-just wants to help people!
— Donald J. Trump (@realDonaldTrump) September 21, 2017
I would not sign Graham-Cassidy if it did not include coverage of pre-existing conditions. It does! A great Bill. Repeal & Replace.
— Donald J. Trump (@realDonaldTrump) September 20, 2017
Graham, co-sponsor of the bill, also came to Cassidy’s aid in the pop culture battle:
Claims that #GrahamCassidy-Heller-Johnson doesn’t cover pre-existing conditions — #FakeNews on steroids! https://t.co/pRHcaG2KNz
— Lindsey Graham (@LindseyGrahamSC) September 21, 2017
Conservative commentator Ben Shapiro, whose daughter received care at Children’s Hospital Los Angeles for a heart condition similar to that of Kimmel’s son, said the entertainer isn’t an authority on health insurance just because his son had a major medical issue.
In a piece published Wednesday in The Daily Wire, Shapiro wrote:
It’s absurd on a logical level: having a child with a heart condition doesn’t make you an expert on health care anymore than it makes you an expert on heart surgery. I should know—as I’ve said before, and only in response to Kimmel’s invocation of his own son, my daughter received open heart surgery at a year-and-a-half old at CHLA, at the hands of the same magnificent doctor Kimmel used.
So by this logic, my opinion should be treated with precisely the same kind of moral weight Kimmel’s is. But I don’t think that the fact that my daughter had her heart fixed at CHLA is what grants me credibility to talk about health care.
Joe Walsh, a former Republican congressman from Illinois, said Kimmel’s comments show he is out of touch with mainstream America.
Oh look, little @jimmykimmel doesn’t like to be criticized.
Just turn him off like we turn off the rest of these Hollywood twits.
— Joe Walsh (@WalshFreedom) September 21, 2017
According to Cassidy’s website, the Graham-Cassidy bill would give states the freedom to waive Obamacare regulations, protect patients with pre-existing conditions, and provide block grants to states by “equalizing the treatment between Medicaid expansion and non-expansion states through an equitable block-grant distribution.”
A former Republican senator and presidential candidate, Rick Santorum of Pennsylvania, also helped draft the Graham-Cassidy bill, which is expected to go to a Senate vote next week, Politico reported.
“This guy, Bill Cassidy, he just lied right to my face,” Kimmel said on Tuesday night’s show, referring to Cassidy’s appearance nearly four months ago, adding:
For lots of people, the bill will result in higher premiums, and as far as lifetime caps go, the states can decide on that, too—which means there will be lifetime caps in many states … Not only did Bill Cassidy fail the Jimmy Kimmel test, but he failed the Bill Cassidy test, too.
The comedian and host of ABC’s “Jimmy Kimmel Live!” was referring to a comment Cassidy made on the show in late May. “We’ve got to have insurance that passes the Jimmy Kimmel test,” the Louisiana Republican said then.
Also on Tuesday night’s show, Kimmel said the Graham-Cassidy bill actually is contrary to the “Kimmel test,” which, he said, is: “No family should be denied medical care, emergency or otherwise, because they can’t afford it.”
Kimmel previously announced on air in May that his son, Billy, was diagnosed with a heart condition and underwent successful surgery. He said Tuesday night that under the “current plan,” meaning Obamacare, his son’s medical treatment would be covered.
“Our current plan protects Americans from these [insurance] caps and prevents insurance providers from jacking up the rates for people who have pre-existing conditions of all types, and Sen. Cassidy said his plan would do that too,” Kimmel said.
Then, on Wednesday night’s show, Kimmel slammed Cassidy and the Senate bill again, saying:
Oh, I get it. I don’t understand because I’m a talk show host. Then help me out, which part don’t I understand? Is it the part where you cut $243 billion from federal health care assistance? Am I not understanding the part where states would be allowed to let insurance companies price you out of coverage for having pre-existing conditions?
Cassidy also replied on Twitter to criticism distributed by National Public Radio:
The ACA repeal effort has risen once again from the ashes in the form of a bill known as Graham-Cassidy. https://t.co/lDAOEHSmUg
— NPR (@NPR) September 19, 2017
Ed Haislmaier, a senior research fellow in The Heritage Foundation’s Center for Health Policy Studies, told The Daily Signal in an interview Thursday that Kimmel’s comments were misinformed.
“The bill does retain prior law,” Haislmaier said of the Graham-Cassidy legislation, adding:
It doesn’t change prior law on [pre-existing conditions] and … a lot of this was dealt with before Obamacare. …
In terms of the actual Graham-Cassidy bill, they specifically say that they have to cover…they have to explicitly use the money in a way that makes sure that people with pre-existing conditions have access to health care. So it reinforces that.
Report by Rachel del Guidice. Originally published at The Daily Signal.
0 notes
Text
Liberal Jimmy Kimmel is making a joke of health care
Jimmy Kimmel may be a funny man, but he doesn’t understand Obamacare, according to a U.S. senator who the late-night TV host slammed this week as dishonest in describing a Republican alternative to the health care law.
Sen. Bill Cassidy, R-La., one of the chief authors of legislation to partially repeal Obamacare, sought to make himself clear Thursday morning on a friendlier show.
“Jimmy doesn’t understand, not because he’s a talk show host—[but] because we’ve never spoken,” Cassidy said on “Fox and Friends” of Kimmel’s contention that Senate Republicans’ bill would abandon Americans with pre-existing medical conditions.
“He’s only heard from those on the left who are doing their best to preserve Obamacare,” Cassidy said of Kimmel and his appraisal of the bill. “He’s not heard from me, because we’ve not spoken.”
youtube
Cassidy, a physician, apparently meant they haven’t talked about the details of his bill. The legislation, drafted with three fellow Republican senators—Lindsey Graham of South Carolina, Dean Heller of Nevada, and Ron Johnson of Wisconsin—would repeal Obamacare’s mandates requiring individuals to obtain health insurance and larger employers to offer it.
Other conservatives came to Cassidy’s defense on the particulars of the so-called Graham-Cassidy legislation.
In his own interview with “Fox and Friends” Thursday morning, Mike Needham, chief executive officer of Heritage Action for America, the lobbying affiliate of The Heritage Foundation, said Kimmel’s estimation of the Graham-Cassidy bill was incorrect.
“What Section 106 of the bill says is that every single state has to make sure that there continues to be affordable access for people with pre-existing conditions,” Needham said, adding:
The entire thing is kind of what is wrong with the way we talk about policy in this country. I am sure Jimmy Kimmel is a nice guy, I am sure he is very well intentioned, but he is both wrong on what this bill does, and he doesn’t understand. There’s a whole bunch of conservative ideas as to how we can take care of people with pre-existing conditions.
youtube
President Donald Trump, who had announced he would sign the Graham-Cassidy bill, tweeted Wednesday night:
Senator (Doctor) Bill Cassidy is a class act who really cares about people and their Health(care), he doesn’t lie-just wants to help people!
— Donald J. Trump (@realDonaldTrump) September 21, 2017
I would not sign Graham-Cassidy if it did not include coverage of pre-existing conditions. It does! A great Bill. Repeal & Replace.
— Donald J. Trump (@realDonaldTrump) September 20, 2017
Graham, co-sponsor of the bill, also came to Cassidy’s aid in the pop culture battle:
Claims that #GrahamCassidy-Heller-Johnson doesn’t cover pre-existing conditions — #FakeNews on steroids! https://t.co/pRHcaG2KNz
— Lindsey Graham (@LindseyGrahamSC) September 21, 2017
Conservative commentator Ben Shapiro, whose daughter received care at Children’s Hospital Los Angeles for a heart condition similar to that of Kimmel’s son, said the entertainer isn’t an authority on health insurance just because his son had a major medical issue.
In a piece published Wednesday in The Daily Wire, Shapiro wrote:
It’s absurd on a logical level: having a child with a heart condition doesn’t make you an expert on health care anymore than it makes you an expert on heart surgery. I should know—as I’ve said before, and only in response to Kimmel’s invocation of his own son, my daughter received open heart surgery at a year-and-a-half old at CHLA, at the hands of the same magnificent doctor Kimmel used.
So by this logic, my opinion should be treated with precisely the same kind of moral weight Kimmel’s is. But I don’t think that the fact that my daughter had her heart fixed at CHLA is what grants me credibility to talk about health care.
Joe Walsh, a former Republican congressman from Illinois, said Kimmel’s comments show he is out of touch with mainstream America.
Oh look, little @jimmykimmel doesn’t like to be criticized.
Just turn him off like we turn off the rest of these Hollywood twits.
— Joe Walsh (@WalshFreedom) September 21, 2017
According to Cassidy’s website, the Graham-Cassidy bill would give states the freedom to waive Obamacare regulations, protect patients with pre-existing conditions, and provide block grants to states by “equalizing the treatment between Medicaid expansion and non-expansion states through an equitable block-grant distribution.”
A former Republican senator and presidential candidate, Rick Santorum of Pennsylvania, also helped draft the Graham-Cassidy bill, which is expected to go to a Senate vote next week, Politico reported.
“This guy, Bill Cassidy, he just lied right to my face,” Kimmel said on Tuesday night’s show, referring to Cassidy’s appearance nearly four months ago, adding:
For lots of people, the bill will result in higher premiums, and as far as lifetime caps go, the states can decide on that, too—which means there will be lifetime caps in many states … Not only did Bill Cassidy fail the Jimmy Kimmel test, but he failed the Bill Cassidy test, too.
The comedian and host of ABC’s “Jimmy Kimmel Live!” was referring to a comment Cassidy made on the show in late May. “We’ve got to have insurance that passes the Jimmy Kimmel test,” the Louisiana Republican said then.
Also on Tuesday night’s show, Kimmel said the Graham-Cassidy bill actually is contrary to the “Kimmel test,” which, he said, is: “No family should be denied medical care, emergency or otherwise, because they can’t afford it.”
Kimmel previously announced on air in May that his son, Billy, was diagnosed with a heart condition and underwent successful surgery. He said Tuesday night that under the “current plan,” meaning Obamacare, his son’s medical treatment would be covered.
“Our current plan protects Americans from these [insurance] caps and prevents insurance providers from jacking up the rates for people who have pre-existing conditions of all types, and Sen. Cassidy said his plan would do that too,” Kimmel said.
Then, on Wednesday night’s show, Kimmel slammed Cassidy and the Senate bill again, saying:
Oh, I get it. I don’t understand because I’m a talk show host. Then help me out, which part don’t I understand? Is it the part where you cut $243 billion from federal health care assistance? Am I not understanding the part where states would be allowed to let insurance companies price you out of coverage for having pre-existing conditions?
Cassidy also replied on Twitter to criticism distributed by National Public Radio:
The ACA repeal effort has risen once again from the ashes in the form of a bill known as Graham-Cassidy. https://t.co/lDAOEHSmUg
— NPR (@NPR) September 19, 2017
Ed Haislmaier, a senior research fellow in The Heritage Foundation’s Center for Health Policy Studies, told The Daily Signal in an interview Thursday that Kimmel’s comments were misinformed.
“The bill does retain prior law,” Haislmaier said of the Graham-Cassidy legislation, adding:
It doesn’t change prior law on [pre-existing conditions] and … a lot of this was dealt with before Obamacare. …
In terms of the actual Graham-Cassidy bill, they specifically say that they have to cover…they have to explicitly use the money in a way that makes sure that people with pre-existing conditions have access to health care. So it reinforces that.
Report by Rachel del Guidice. Originally published at The Daily Signal.
0 notes
Text
Megadeth Deliver Thrash Filled and Heartfelt Performance in Boston

Dave Mustaine & Megadeth – House of Blues – Boston, MA – June 25, 2017
Megadeth’s and Metallica’s DNA will forever be intertwined as both bands helped define the thrash and speed metal genre that emerged on both coasts of the United States in the early to mid 1980’s.
There’s also the other obvious connection between Megadeth and Metallica as anyone reading this article is likely more than familiar with the pair’s shared history.
However, it would be short sighted to fixate on the personal history between the two metal titans, as it’s each of these bands’ impact and influence within the world of heavy metal that matters far more.
Hetfield, Ulrich, and Mustaine took the genre of music that Black Sabbath cooked up back in 1970 and added the elements of thrash and speed. In doing so they simultaneously laid down the foundation for aggressive metal to have its place in music for generations to come.
And let’s be honest here, Mustaine likely long ago came to the conclusion that he’ll never be able to completely shake the shadow that Metallica cast over him since his unceremonious ousting from the group and his formation of Megadeth in the aftermath.
Perhaps the Big Four shows a few years back, as well as winning a Grammy after being nominated for the eleventh time this past February for 2016’s Dystopia, finally laid to rest any ill will Mustaine once harbored for his former band.
A peculiar thing though has happened over the course of the last thirty plus years regarding the gap between Metallica and Megadeth in terms of their stature within the metal community amongst the hard line faithful.
There are more than a few old school metal fans that view Metallica as a legacy thrash and speed act that long since abandoned the genre for the riches and global popularity mainstream success have provided them.
Additionally, there could be a valid argument to be made that although Metallica’s first three records could go down as three of the most important albums in heavy metal history, Megadeth’s body of recorded material may very well be superior in overall quality when comparing each bands’ complete discography.

This alteration in the perception of each band could also be attributed in part to the fact that Metallica willfully chose to abandon traditional metal with the release of the self-titled Metallica, otherwise known as the “Black” album, in 1991.
In doing so they opened the door for bands like Megadeth, Slayer and Anthrax to further endear themselves to the hard core thrash audience they were choosing to leave behind.
This condition may be best explained by simply describing how truly divergent the Metallica and Megadeth concert experiences are these days. Although Metallica may play to tens of thousands on any given night, their live shows are at times as much about spectacle and the opportunity to take in a one of a kind visual experience, than they are about the actual music.
Conversely attending a Megadeth concert, such as the show the band recently played to an at capacity House of Blues in Boston, can make one feel as though they’ve been transported back to the thrash heyday of the 1980’s.

Mustaine, long time bandmate and bassist David Ellefson, as well as new comers guitarist Kiko Loureiro and drummer Dirk Verbeuren, delivered a performance in Boston that was not only fiery in every sense of the word, it was also one that came across as deeply sincere and even playful at times.
When Mustaine and company played Megadeth classics such as show opener “Hanger 18”, “Tornado of Souls,” “Peace Sells” and set closer “Holy Wars…. The Punishment Due” the energy inside the venue percolated to an almost voltaic level of intensity.
More than a few circle pits would materialize out of nowhere throughout the course of the evening, while the more sedentary fans would go on to engage in several impromptu sing-a-longs with Mustaine as Megadeth’s post-apocalyptic imagery played behind the band throughout the duration of the performance.

Megadeth’s official mascot Vic Rattlehead even chose to make a few appearances on the night. Rising from out of the shadows initially during Dystopia track “Conquer or Dire” and then again during “Peace Sells.”
The band’s talisman evilly pandered about the stage attempting to engage in mortal combat with band members one moment, while menacingly taunting random fans in the audience the next.
It wouldn’t be a Megadeth show if the irascible Mustaine didn’t engage the crowd in some sort of humorous banter. This time around the front man’s ire would be directed towards a muscle bound head banger that kept interrupting him as he was attempting to tell a story.
At one point the lead singer directly called out the pumped up audience member stating, “I’m waiting for you to shut the fuck up so I can tell a story bro. Go fucking shoot some steroids outside, I don’t care. You don’t have to be quiet, just don’t be a dick.”

Mustaine then went on to spin a yarn about how he and Ellefson had played a show in Northern Ireland a long time ago and that during the concert he apparently at one point had said to the audience before slugging down a Guinness, “Give Ireland back to the Irish, this one is for the cause.”
The “cause” of course being a reference to the ideology of Irish Repulicanism, a topic that most Irish residents don’t take all too lightly today, let alone back in the much more volatile and active IRA days of the 1980’s.
The “cause” is also a deeply personal Irish issue as it cuts across political, religious, and even ancestral lines in Ireland. In other words it’s subject matter that may be best left to those in Ireland to debate, or even toast, versus the lead singer of a thrash metal band from across the pond.
Well apparently Mustaine’s political and semi-quasi religious musings didn’t go over too well as the following morning he was informed by Ellefson that they had to be escorted out of the city in a bullet proof van the night previous because of his ramblings.
According to Mustaine the incident inspired him to pen one of Megadeth’s most revered songs the very next day, “Holy Wars,” which the band would go on to play next and the track that would also serve as the concert’s swan song.

It should be noted that the newer Megadeth material played on the evening, which included songs such as “Fatal Illusion,” Poisonous Shadows” and “Dystopia,” all fit in nicely with the classics.
These more recent tracks seamlessly blended into the overall pacing of the set quite nicely while also giving fans reasons to believe that Megadeth has more than a few resplendent records up their sleeves before they may call it quits someday.
It’s also worth mentioning the rejuvenated vigor in which Megadeth seem to be playing with on this current tour cycle. Perhaps this resurgence can be attributed to somewhat of a return to form in terms of the band’s recorded material.
2016’s Dystopia is a more aphotic and heavier record with the album aligning more sonically with Megadeth staples such as “So Far, So Good…. So What!” and “Rust in Peace.”

Additionally, new band members Louriero and Verbeuren, both of whom were brought into the fold by Mustaine following the unexpected departures of both guitarist Chris Broderick and drummer and Shawn Drover back in 2014, have breathed new life into the band’s live shows.
Louriero is not your typical snarl in place, look evil and play killer riffs type of metal axe slinger. Instead the Brazilian guitarist is a whirling dervish of riff ferocity and hyper activity.
Louriero as it turns out is the perfect foil for the more stoic Mustaine, as his Tasmanian Devil guitar stylings are not only technically jaw dropping, his energy on stage draws the audience that much further into Megadeth’s evil sonic web.
Drummer Dirk Verbeuren, primarily known for his time in Swedish death metal stalwarts Soilwork, is as entertaining as any metal drummer out there touring day and much like every player in Megadeth, the Belgian’s level of musicianship is beyond reproach.
There’s just something about Verbeuren’s play style, mechanics and sound that seem reminiscent of classic Megadeth era drummer Nick Menza. Perhaps this a figment of on an overworked imagination or maybe Verbeuren’s just the right fit for Megadeth on numerous levels, similarly to the way Brooks Wackerman seemed destined to become Avenged Sevenfold’s new drummer.

Even long time Megadeth bassist Ellefson, as well as Mustaine himself, seem to both be playing with an amped up, almost youthful enthusiasm on this current tour run. And really how could the pair not be excited right now?
Dystopia was critically well received by the music industry and the fans, the Recording Academy recognized the album via awarding it the Grammy for Best Metal Performance this past year and fans are also still coming out in droves to see Megadeth perform live.
All of this could lead some to conclude that Megadeth may actually be morphing into a more positive, more accessible and dare I say, more affable band. Oh the horror.
Should this sentiment actually hold true it may be wise to never let Mustaine in on the secret. A metal world without an at least sometimes acerbic Mustaine would likely be one none of us would want to live in.
The biggest takeaways from Megadeth’s performance in Boston this past weekend may be rooted in the simplistic. The connections fans made with one another, with the band onstage and ultimately with the music itself are the exact elements that combine to make the heavy metal community’s bonds with one another so concrete and so ever lasting.

And that right there may be the essence of what separates a band like Megadeth from a band like Metallica as both bands approach their 40th year in existence.
Megadeth’s live performances still have this uncanny ability to make those in attendance feel like the angst riddled teenagers that would steal ten dollars from their mom’s purse to buy a cassette copy of Killing Is My Business… And Business is Good from their local Strawberries or Tape World.
The band’s concerts also continue to bond friends, family and strangers in ways that we all seemed to be able to do more effortlessly before mortgages, ISIS and other real world impediments became barriers to our being able to do something as trivial as banging our heads to evil riffs.
I suppose at the end of the day is there any greater gift that music bestows upon the world than providing its inhabitants with the opportunity to make them feel like kids again?
Hats off to Megadeth for reminding everyone in Boston that it’s still okay for adults to crash and bang into one another while singing songs about end times, corporate greed and social anarchy. Long live Megadeth, long live Dave Mustaine and love live the once and future kings of thrash.
[ngg_images source=”galleries” container_ids=”1101″ display_type=”photocrati-nextgen_pro_horizontal_filmstrip” image_crop=”0″ image_pan=”1″ show_playback_controls=”1″ show_captions=”0″ caption_class=”caption_overlay_bottom” caption_height=”70″ aspect_ratio=”1.5″ width=”100″ width_unit=”%” transition=”fade” transition_speed=”1″ slideshow_speed=”5″ border_size=”0″ border_color=”#ffffff” override_thumbnail_settings=”1″ thumbnail_width=”120″ thumbnail_height=”90″ thumbnail_crop=”1″ ngg_triggers_display=”always” order_by=”sortorder” order_direction=”ASC” returns=”included” maximum_entity_count=”500″]
Connect with Megadeth (click icons):





All Writing & Photography: Robert Forte
Instagram: http://www.instagram.com/40_photography/
Facebook: http://www.facebook.com/4zerophotography
Megadeth Deliver Thrash Filled and Heartfelt Performance in Boston was originally published on RockRevolt Mag
#Dave Ellefson#Dave Mustaine#david ellefson#dirk verbeuren#Dystopia#hobboston#holy wars#House of Blues#house of blues boston#Kiko Loureiro#Live Nation#Megadeth#peace sells#rust in peace#umg#universal music#Universal Music Group#Vic Rattlehead
0 notes
Text
Android Circuit: Massive Galaxy S8 Leaks Reveal Everything
New Post has been published on https://universeinform.com/2017/03/24/android-circuit-massive-galaxy-s8-leaks-reveal-everything/
Android Circuit: Massive Galaxy S8 Leaks Reveal Everything
Taking a look again at seven days of information and headlines the world over of Android, this week’s Android Circuit includes all of the info of the Galaxy, more information on the release date, secrets of the Samsung Browser, Nokia avoids the flagship combat, why coloration is the following cell war, the extraordinary OnePlus 3T, a long-term overview of the LG G6, and Google’s new Family Link software program for Android.
Android Circuit is right here to remind you of a few of the many stuff that has befallen around Android within the remaining week (and you could discover the weekly Apple information digest right here).
The entirety You’ll Love Approximately The Galaxy S8
Are you geared up for the huge tick list of thrilling matters in the Galaxy S8? Forbes contributor Gordon Kelly has the listing, he’s checked it twice and Samsung is prepared to visit metropolis with the 2017 flagship, in addition to the overall numbers:
Further, [industry analyst[ Kuo expects a 6:4 shipment cut up in favor of the Galaxy S8 with forty-45 million handsets sold all through 2017. This slightly decreases then the 52M Galaxy S7 units shipped in 2016, but Kuo says That is no cause for Samsung to be disenchanted. Instead, he points out Galaxy S7 shipments were unusually high because of the recalled Galaxy Note 7 which driven capacity Be aware customers back to this handset. the next huge moment inside the cellphone story of 2017 will be the launch and launch of the Galaxy S8 and S8 Plus handsets by Samsung. With a media occasion on March 29, the focal point turns to the timing of the retail release in April. TechRadar has more on the diary control:
Samsung’s teased the Galaxy S8 on video, and now it begins placing up print adverts in elements of Asia, giving us clues as to whilst we might be capable of buying it. One of the posters, spotted by way of leaked @UniverseIce, contains the reference to April 2017, and as the Samsung Galaxy S8 is being introduced on March 29 meaning April is probably whilst it’s going to hit shops.
The poster doesn’t certainly display whatever else new, but it all over again highlights the threshold-to-part display, and with a big ‘S’ inside the center there’s no question that That is an advert for the Samsung Galaxy S8.
The popular know-how now is that pre-orders will start via April 10th, with the first handsets physically released on April twenty-first.
Android Application Development Solutions – Where Did It All Start?
When Apple was first founded via Steve Jobs, Steve Wozniak, and Ronald Wayne in April 1976, to increase and sell private computers, the era changed into astounding, and not anything like anything we had seen earlier than. With digital era so superior, human beings had been convinced that no other competitor could ever evaluate. Then something pretty amazing passed off While Android stepped up to the mark. Android, Inc. turned into founded in October 2003 through Andy Rubin, Wealthy Miner, Nick Sears and Chris White. The aim of Android was to broaden…
Smarter cellular gadgets that are more privy to its owner’s region and Andy Rubin
At this modern-day time, Android’s intentions were to create operating systems for virtual cameras. However Whilst Google obtained Android Inc for $50 million in July 2005, it changed into in question whether or not Google had been planning to enter the cellular phone marketplace, and that they did! Google then developed a platform for mobile devices powered by using the Linux Kernel and has firmly rooted the Android emblem as it’s miles these days. Considering 2008 Android has had numerous updates to streamline improvements in its operating systems, and with its interface capabilities and customer usability, it’s clearly considered to be a force to be reckoned with!
In latest years Android has slowly been changing an increasing number of iPhone consumers into Android customers, because of its elite functionality. Thanks to this, there has been a surprising surge in the wishes and development of Android packages, however, what does it take to make an Android app?
All apps have the ability to increase the functionality of the tool it’s using within a sure technical region, so with regards to Android software improvement solutions, all are written the use of the SDK (Software improvement Kit). The SDK presents an intensive set of improvement tools which incorporates Software program libraries, a debugger, a handset emulator, documentation, a pattern code, and tutorials. Java is used as the principle programming language because it has whole get entry to the Android APIs (application Programming Interface). different improvement tools are generally to be had just like the Local development Kit, the Google App Inventor that’s remarkably visible surroundings for any trainee programmers, and of direction a diffusion of cross-platform frameworks for mobile internet programs.
Of path, if you’re a non-technical person and this sounds particularly overwhelming, then there are quite a number IT corporations inside the virtual global that would assist you to fulfill your imaginative and prescient, and construct your Android App for you at a value. Although the disadvantage of this is that you may need to pay out a touch more to get what you want, on the plus side of things you will be working with a business enterprise that may provide a team of experts, which generally has an extensive heritage in Android software Software improvement. Most services will abide by way of improvement recommendations and rules, which guarantees that your Android application won’t comprise any dodgy surprises. Also, Maximum IT organizations will provide comprehensive utility checking out, protection checks and Also product guide on launch, and in some cases thereafter.
Once your Android app is good to head, you could sell it on Google Play, wherein customers can download it for a small fee or totally free. Google play is the primary app save this is mounted on all Android devices that follow Google’s compatibility necessities.
How to Build Massive Muscle Workout Program
Hello My Buddy,
Do you understand that “the high-quality physiques had been all built by way of tough paintings on the fundamental, heavy responsibility sporting activities?” There are no exceptions to this announcement. Even smooth-gainers like John Grimek and Steve Reeves who could build up muscle very easily could have never reached the Hercules-sized muscle mass they built without a maximum attempt. John Grimek labored up to squats with six hundred pounds, in the back of the neck presses with three hundred pounds, and bench presses with four hundred kilos and this became inside the days before steroids, HGH and unique lifting shirts and leg wraps!
Genetic advantages or not, John Grimek skilled tough and heavy to earn the massive body he obtained that let him emerge as the only an entire life Mr. The united states. And so did every different character with steroid-unfastened natural constructed massive muscle whose muscles are not simply bloated pumped-up tissue. WHAT these primary sporting activities are, and how hard you ought to work on them for extraordinary outcomes, is the “secret components” you must practice to make a reputedly “simple exercising” right into an “outstanding workout” when you perform it!
My Preferred simple exercises for maximum Muscle Boom
1. The Squat – Normal, parallel, heavy respiratory style
2. Stiff-legged lifeless elevate or bent-leg
3. Bench urgent – barbell or heavy dumbbells, Incline or flat bench style
4. Rowing – Bent over, barbell or dumbbells, one or two arm
5. Army Press – Seated or status, barbell or heavy dumbbells
6. Energy cleans barbell or dumbbell
My remark and experimentation have led me to consider that an exercise is productive in building “muscle tissue” if it lets in you to use very heavy weights brings into play the Massive muscle corporations — and creates plenty of over-all frame fatigue.
From this vantage factor, it is clean to look why most of the sporting events observed by way of most weight lifters do not degree as much as the standards required for building most muscle mass. Minnie-mouse sporting activities like Back-to-the-wall-awareness-curls, lateral increases, frontal leg extensions, triceps “kickback”, lunges, cable go-overs and different physical games of the like are a waste of an entire life in case your purpose is to build large muscle tissue.
Shop yourself a lifetime and in all likelihood wasted years of effort. Do no longer hassle with the little sports if your aim is to attain your genetic potential for max muscle length and power.
I at an entire life, get plenty of flak from trainee’s, “muscle gurus” and want-to-be muscle developers when I write articles or deliver a seminar speaking the reality about sensible barbell education for constructing real muscle that lastsThe comments from meat heads, the “commercial-muscle-makers,” the steroid-takers and others don’t hassle me one bit. I let them do their element; my venture is to train the fact to folks who want to the actual solutions to constructing real muscle without all the commercialism and hype.
Welded Wire Mesh – Everything You Need To Know About
Production manner for welded wire mesh
Welded cord mesh has replaced the fashion of concrete fencing to a terrific quantity. This assists with a transparent partition and is found generally used with stadiums and parking space. However with the years, now humans also are using the identical for guarding their homes. In line with the welded wire mesh producer, the Production process includes various machines including the lathe or transformer. These machines employ the electric power to feature and achieve the project.
Cloth used for manufacturing welded twine mesh and their characteristics
Transferring in advance with the Fabric used for production welded cord mesh, the most popular Fabric that is used for the reason is stainless steel alloy. This alloy is fabricated from diverse factors which include nickel, chromium, copper, nitrogen, carbon. Upon undergoing the conversion procedure, These metals show sizable changes in their mechanical and chemical properties. They render tremendous homes like resistance to annoying cracking, anti- corrosive and sturdy. But, alike all matters, it’s too is the situation to wear and tear. Up to a widespread duration says 3-4 years, no weather condition can result in corrosion, But past the equal, corrosion isn’t uncommon. To prevent the identical, it’s miles suggested to offer a coating of nickel or Percent on the same. This enhances their durability for another ten years.
Search the only you want as according to your wishes
Nowadays there is a massive quantity of welded cord mesh producers inside the market offering a wide range to cater your myriad of wishes. Of path, the only supposed for residential fencing can’t be used for fencing your farmland or a commercial complex. These wires range regarding Material used, design and size. Other than the identical, you could additionally get wires as per your given specs to fulfill your preferred needs. The only component you need to do right here is taking the pain to search for a depended on welded cord mesh producer imparting you with this provider.
Right choice for less expensive fencing
Aside from rendering a tidy and smooth surface, welded wire mesh additionally adds a decorative contact to your home. Together with Those, every other enticing function you revel in with Those is that they’re without problems less expensive while in comparison to another fencing forms. So if you are looking ahead for an inexpensive yet durable fencing, not anything may be higher than going beforehand with the same. Take time from your busy schedule and search for the most dependable supplier in this field.To make your Search smooth, the internet is there to your rescue.
0 notes