#bc all the agencies & organisations & departments & corporations that are “on the job” are only on the job of securing their own pay checks
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The total number of visits Tumblr.com received during January 2021 is 327 million.
Text
I just had to share this email I got so all y'all can appreciate the absolute state of welfare services in Australia with me:
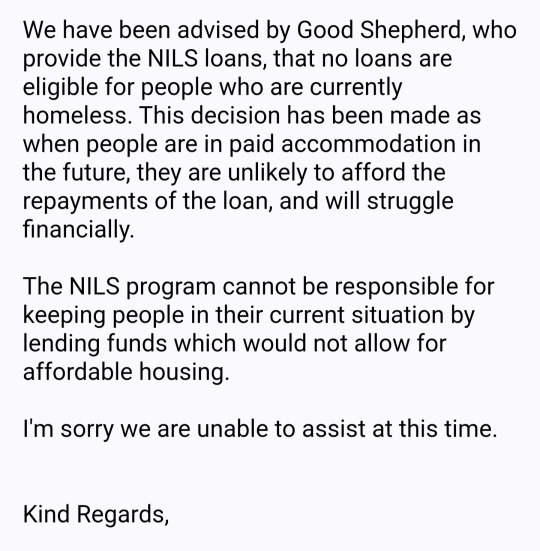
The NILs Loan Scheme is a government funded, no interest loan scheme for people on low incomes, but this leaves me wondering exactly who tf can qualify for their loans. Because it seems like if you have any symptoms of poverty it's a no.
I applied because I need the clutch replaced in my van, which I live in. It's lucky that I actually CAN afford the cost myself (due to living in a van & not participating in Australia's increasingly ridiculous housing market). I thankfully can afford such an expense these days & was just looking for a responsible financial buffer, just in case. But if this had happened to me a few years ago when I first became homeless and was far less financially stable, then my next living situation wouldn't be "affordable housing" it would be a fucking tent.
Anyway, the backwards ass state of a GOVERNMENT FUNDED welfare scheme refusing to assist those who need welfare the most because they don't want to encourage homelessness or whatever the dumb fuck? Just really rustled my jimmies tbh. Just screams "yet another govt welfare scheme that's actually just about handing out money to fake charities & not helping the poor". Good Shephard just got on the "do not donate to these grifters" list along with the Salvos😒
#I got a root canal & a heap of skin cancer to pay for on top of this clutch replacement right#& I got it#but there's going to be $100 left in my bank account with this all said & done#& I could use ZIP or AfterPay or whatever if need be#but I figured a no-interest no-fee no-nothing loan would be the gold standard of responsible financial decision-making#& lol turns out the eligibility requirements for a NILs loan are HIGHER than a Buy Now Pay Later (w exorbitant fees) type of loan#how tf can you call that a loan scheme for people on low incomes?#when you gotta be at least middle class to qualify?#the fucking state of Australian welfare agencies istg#& I ain't even shocked atp because this is the response I've always gotten from welfare agencies#they always have some (often very stupid) excuse as to why they can't do what they say they do#I hear so often “oh there's plenty of support for the poor & homeless they just choose to be that way”#but this is the support just fyi#this is why poverty & homelessness still exist in Australia#bc all the agencies & organisations & departments & corporations that are “on the job” are only on the job of securing their own pay checks#with as little expenditure on the poor as they can get away with#auspol#poverty
9 notes
·
View notes
Text
Sickened By Billing Abuses, Readers And Tweeters Stand Up For Patients’ Rights
Letters to the Editor is a periodic feature. We welcome all comments and will publish a selection. We edit for length and clarity and require full names.
Private Equity Predators?
First of all, let me thank you for writing about such an important issue (“Investors’ Deep-Pocket Push To Defend Surprise Medical Bills,” Sept. 11). I am going to tell you about my personal pain regarding surprising medical billing.
They can call themselves Doctor Patient Unity group or any other fancy name, but the reality is that they are all predators. I say this because I am the victim of these doctors groups. I work as a linguist with the U.S. Army and have top-secret clearance. I could lose my clearance if any of my bills go to a collections agency.
I had appendix surgery on Nov. 6, 2018, at the Davis Medical Center in Layton, Utah. The surgeon had told me that my surgery would take only 10 to 15 minutes. After two hours of surgery, I was released from the hospital and sent home. My insurer, CIGNA, paid all the Davis hospital bills and I paid my portion of the bills. Then in March 2019, I received two separate doctor’s bills totaling about $48,000. My insurance was not paying the doctor’s bills because they were out-of-network. The doctor’s office kept sending me letters to pay $48,000 from my pocket; if I did not pay, I was told, my bills would be sent to collections.
Finally, I received a letter from the collections agency saying that if I did not pay $26,770, it would send the information to the credit agencies. Can the Doctor Patient Unity group tell me what I should do? Should I lose my clearance and my job because I cannot afford to pay $26,770? Should I borrow money from the bank and then pay high interest to the bank for the rest of my life?
— Aziz Rehman, Kaysville, Utah
This is a very misleading article. Many independent physicians speaking out want IDR to solve the problem of outliers and take patients #OutOfTheMiddle. Insurance-backed lobbyists are using this issue as a #TrojanHorse to enrich corporate shareholders at expense of physicians.
— Amy Mecozzi Cho, MD MBA (@amychomd) September 12, 2019
On Twitter, Dr. Amy Mecozzi Cho of Minneapolis diagnosed holes in the article. For example, she told KHN, “the contracted rates for insurance are misleading since our bad debt for patients with high-deductible insurance is greater than 60% of their deductible, but insurance companies won’t bill them because they know this. And so our effective rates for commercial insurance are actually much lower than contracted. The medical loss ratio and the CBO estimates are not capturing these costs to patients and physicians.”
Religious Malpractice
My sister, a hospital chaplain (of Roman Catholic faith), informs me that it’s considered chaplain malpractice to try to force a patient to cope with suffering in the exact way others think they should (“Firing Doctor, Christian Hospital Sets Off National Challenge To Aid-In-Dying Laws,” Aug. 30). It would follow, then, that a hospital’s requiring staff to “help” patients “appreciate the Christian understanding of redemptive suffering” is a paternalistic dismissal of patient integrity and a form of malpractice. The medical relationship is between the patient and the doctor, not the patient and the Vatican.
— Gloria Kohut, Grand Rapids, Mich.
Many hospitals in India are controlled by religious organisations (Hindu, Jain, Christian, Muslim) Are they also as intolerant to differences in one's approach to what is ethical in medical practice as the Christian hospital in this case? https://t.co/Nzy6JN348B
— Amar Jesani (@amarjesani) September 8, 2019
— Amar Jesani, Mumbai, India
It’s unfathomable that students with disabilities can’t get the aid they need to attend college and live in the community! Bravo to this Stanford freshman for fighting for services. It’s past time for readily available help for students! #DisabilityRightshttps://t.co/EuVnUzEX8b
— Areva Martin, Esq. (@ArevaMartin) September 2, 2019
— Areva Martin, Los Angeles
Squeezing The Most Out Of Student Aid
I saw Jenny Gold’s excellent article in the Los Angeles Times about a disabled student’s need for assistance as she starts school at Stanford (“Spotlight: A Young Woman, A Wheelchair And The Fight To Take Her Place At Stanford,” Sept. 4). I wanted you to be aware that the Department of Rehabilitation in California pays for additional expenses for students to train them for future employment. This includes laptops, supplies, transportation expenses, necessary expenses. They might also pay for expenses for care above and beyond the approval of the state Department of Health Care Services.
All students face the issue of how to support themselves while in college. Stanford’s lovely gift of education for all who are accepted is often not used due to the high expenses of that area. Many students are unable to afford college, even with a full scholarship.
Those who have paid their way with student loans and are now employed in high service areas, such as medicine, psychiatry, social services and teaching, are strapped with lifetime payments. Our best and our brightest who serve our communities are in debt to the point where their income barely pays their lifetime of student loans. Sylvia Colt-Lacayo’s situation may have more expenses, but the debt of $2,000 a month is not unique for a full-time university student.
— Teresa L. Pardini, LMFT, Creativity in Counseling, Nipomo, Calif.
This young woman got 4.25 GPA & a full ride to Stanford despite never drinking ANYTHING at school so she wouldn't have to pee, bc that's what it takes for ♿ kids to excel in an abled world. That she still has to fight for care should infuriate you.https://t.co/B9vH1c1ATK
— Sonja Sharp (@sic_sonja) September 3, 2019
— Sonja Sharp, Los Angeles
A Heroine In The Opioid Fight
Please thank this wonderful, dedicated and tough woman (“Longtime Crusader Against OxyContin Begins To See The Fruits Of Her Struggle,” Sept. 17). That criminal company and every single member of the Sackler family had been well aware of the entire scam for decades, but they kept their mouths shut, turned their heads, denied everything and couldn’t care less since they were stuffing their individual pockets with hundreds of millions of dollars for each member of that large family. Every dollar should be clawed back from each family member. They’re laughing all the way to the Sackler Wing of 20-plus museums around this planet.
— David Padawer, Pittsburgh
As the father of a recovering opioid addict I see Barbara's efforts and passion for accountability is so heroic. The loss of her son is so terrible….
— Dave (@dwpena) September 17, 2019
— Dave Pena, Roseville, Calif.
Senior Hunger And Pangs Of Conscience
I’ve been a medic for over 20 years. I have patients that have to pick between eating or taking their medications. It’s disgraceful. We need to have articles like this written every day (“Starving Seniors: How America Fails To Feed Its Aging,” Sept. 3). Thank you.
— Eric Johnson, Marana, Ariz.
Many hospital stays are for ppl w complications of starvation and malnutrition – confusion/delirium, dangerous electrolyte imbalances in salt, sugar, potassium
We need programs for starving People.
How America Fails To Feed Its Aging https://t.co/gv6Z8HnqZH @khnews
— Tina Chee, MD, MPA (@Tina_Chee_MD) September 3, 2019
— Dr. Tina Chee, New York City
I’m 68, a widower, disabled after two open-heart surgeries, with no family left. The last person to visit me at home was the yearly home health care nurse, back in February.
I am just like the people in your article: old, worn-out and forgotten. After a lifetime of work, I get by on a check that’s half of what a minimum-wage worker flipping burgers might make at $15 an hour. I can barely afford to eat the burgers now. No one, no insurance company, no politician is trying to help seniors out of poverty.
My biggest fear is dying and my little dogs being left alone for weeks or months to die before anyone finds me. Having moved to a rural area after my wife died, people don’t warm up fast to outsiders. It’s awful not to speak to anyone for years — yep, years — outside of cashiers. Just letting you know there are a lot of us out here.
— Rick Wrenn, Mount Carmel, Tenn.
What happens when the system designed to protect millions of seniors facing starvation is broken? The Older Americans Act is one critical piece holding many local Meals on Wheels programs together. We need you to ask… https://t.co/eicvq9gRln
— Chapa Arts & Photog. (@Berrysicles) September 12, 2019
— Maria De Jesus Chapa, Houston
Double Checking Fact-Check Facts
As the chairman of Physicians for Fair Coverage (PFC), I have joined doctors around the country in working to protect patients from surprise medical bills. I am writing now to set the record straight on the implications of various federal policies under debate in Congress. Not only did KHN’s recent article (“Doctors Argue Plans To Remedy Surprise Medical Bills Will ‘Shred’ The Safety Net,” Aug. 7) overlook research from the American Journal of Managed Care, the Centers for Disease Control and Prevention, and the Congressional Budget Office, it created a myopic interpretation of our argument in order to label it as “false,” which resulted in an inaccurate conclusion with respect to a complex issue that deserves a thorough, data-driven and factual examination.
According to the CBO, a benchmarking approach would cut payments to in-network physicians by as much as 20%. This translates into tens of billions of dollars shifted away from in-network physicians who are not sending surprise bills over the next decade. Emergency physicians treat all patients regardless of their insurance status. As a result, 70% of their patients are uninsured, seniors or poor families and children. Therefore, there is no practical difference between reducing commercial insurance payments and reducing Medicaid or Medicare rates. KHN’s own previous case study found that contributing factors to hospital closures include “high uninsured rates and a payer mix dominated by Medicare and Medicaid.” So, a benchmarking policy would create even larger disparities in quality and access to care over time for vulnerable populations.
Others agree that commercial payments play a critical role in supporting the care of America’s most vulnerable patients, including: American Academy of Orthopaedic Surgeons, American College of Emergency Physicians, American College of Radiology, America’s Essential Hospitals, American Hospital Association, American Medical Association, Association of American Medical Colleges, Catholic Health Association of the United States, Children’s Hospital Association and Federation of American Hospitals.
Instead of speaking with health care experts to better understand how reimbursement dynamics and patient access are inextricably linked in today’s economy, this article relied exclusively on the opinions of two biased research fellows who advocate for the very policy that our ad opposes and whose statements are misleading at best. The assessment also disregards a quote from the California Medical Association describing a lack of available anesthesiologists under California’s benchmarking approach.
PFC’s mission is to protect patients from surprise medical bills. That is why, this year alone, we helped drive constructive compromises that produced new laws in Texas, Colorado, Nevada and Washington. Similarly, at the federal level, we support legislation that uses a proven independent dispute resolution model to protect patients without disrupting responsible, in-network practices. To further protect patients, it’s important that Congress does not create an even larger public health issue with respect to the safety net while fixing the real issue of surprise bills.
— Dr. Sherif Zaafran, Washington, D.C.
When I traveled around the state last fall, Kansans made it clear that Medicaid expansion is a high priority. I'm going to do everything in my power to ensure this will be the year we will finally expand Medicaid in Kansas. #RebuildingKansashttps://t.co/gg7BXeopMp
— Laura Kelly (@LauraKellyKS) September 6, 2019
— Gov. Laura Kelly, Topeka, Kan.
Infected With Advocacy
Your story about Medicaid expansion fails to attempt any serious description of the reasons for opposition to this expansion (“How Political Maneuvering Derailed A Red State’s Path To Medicaid Expansion,” Sept. 6). The reader is left with the clear impression that opponents are ill-informed, parsimonious, uncaring of others (especially the poor) or all of the above. There is no suggestion that such opposing might be in good faith. You really can do better than this. You insult the intelligence of your readers when you fail to deliver the whole story in a fair and evenhanded manner so they can decide for themselves. There is enough “us vs. them” in current media. Don’t drag it into health care. If you want to take positions on important health care issues, please create an editorial page; don’t infect your “news” with those positions. And no, I’m not a Republican. I’m an independent tired of constant advocacy in the media disguised as news. Thank you.
— Geoff Hargreaves-Heald, Lincoln, Mass.
Two (not shocking, maybe disappointing) takeaways: – Citizen intent matters little if a few state actors know how to work the system. – Nothing works better than high medical bills for getting middle class voters to empathize with Medicaid recipients.https://t.co/JxHaho26pU
— Juhyung Sun (@JuhyungSun) September 6, 2019
— Juhyung Sun, Tucson, Ariz.
Why Prescribed Weight Loss Is Ill-Advised
What the author of the article dismissing the opinion of the dietitian who claimed stigma and yo-yo dieting cause more harm than obesity itself failed to mention is that, for many people, how weight might contribute to the development of physical illnesses is immaterial (Obesity Stigma And Yo-Yo Dieting, Not BMI, Are Behind Chronic Health Conditions, Dietitian Claims, Sept. 17). The prescription to lose weight, in and of itself, is damaging. Most dieters regain 100% or more of weight lost within five years. Additionally, people who are told to lose weight and subsequently diet are at significantly increased risk for body dissatisfaction, bingeing, disordered eating and eating disorders.
Health is not just physical health. Descartes invented mind-body dualism in a thought experiment in the 1600s. It is an idea that permeates modern culture and medicine to this day. However, we are not separate from our minds. Our mental health is not separate from our “true” health.
Obesity may or may not cause illness. If the process of losing weight creates more illness in the form of shame and eating disorders as well as health care avoidance, then continuing to blindly recommend it is irresponsible. The recommendation to diet should be made with an informed consent process. “Being overweight may put you at risk of developing X, Y and Z. I am recommending caloric restriction to remedy that. Caloric restriction is known to be ineffective in the long term, and puts you at risk of developing an eating disorder or of weighing more than you do now. The alternative to caloric restriction is to thoughtfully examine obstacles to your access of whole, nutritious foods, whether they be financial, psychological or otherwise.
“Compassionately adopting a diet that over time puts more colors on your plate and replaces processed foods with whole foods may in itself lead both to weight loss and decreased risk of chronic medical conditions. Additionally, finding a way to increase your physical activity, such that the activity is associated with joy and self-care, will also be protective against chronic conditions and may contribute to weight loss. However, if at any point weight loss becomes the goal rather than the logical outcome of sustainable changes, then we are back at the dieting step, with all its consequent risks.”
It doesn’t matter whether obesity causes illness. Deliberately losing weight is an ineffective approach to addressing what may or may not be a problem, and additionally causes harm. Let us guide patients toward what they have control over: food choices and increased activity, and let go of the number, not because it doesn’t influence health, but because focusing on it is ineffective and counterproductive.
If a formerly obese person is now skinny but miserable, hungry, obsessive, depressed and food-preoccupied because that’s what we evolved to do in the context of weight loss, why is that better? Any solution has to respect mental and physical health outcomes, or it is not truly a health-based recommendation.
— Dr. Sarah O’Neil, Boston
This article ignores the massive growing body of evidence around #weightstigma, argues against just two pieces @chr1styharrison put forward, then just uses quotes from experts to rebuff this claim and not evidence and the use of an odd metaphor about carrots.
— Kerry (she/her) (@HAEScoach) September 18, 2019
— Kerry Beake, Mandurah, Australia
Summer Camp Rehab — Or Torture?
The article “At This Summer Camp, Struggling With A Disability Is The Point” (Aug. 13) portrays what you describe as “necessary” but what many of us adults with disabilities remember as rehab torture — traumatic memories of painful so-called therapy with questionable or no demonstrable results. Even if the program had results, many of us would have chosen not to experience the pain. It’s old-style rehab of pretending it isn’t torturous and “we know what’s best for you.” This sort of rehab was vehemently rejected by disability activists years ago. It’s too bad adults who experienced this kind of therapy weren’t consulted. I believe few of them would describe this in positive terms. It’s not a new concept: If you work hard, with pain, you can become independent! So if you can manage to dress yourself in four hours and get ready for bed in three hours, you’re independent and met the goals set for you, even though you’re so tired you can’t enjoy the remaining few hours of your day. Most adults with disabilities would set a goal of having a quality of life over being independent. This was a very biased story and should have been more balanced from very different perspectives, especially from those with disabilities.
— RoAnne Chaney, executive director of the Michigan Disability Rights Coalition, East Lansing, Mich.
SUMMER CAMP FOR KIDS WITH DISABILITIES! There should be more camps just like this one! This Nashville camp was started for kids who have disabilities that require physical therapy, and the camp counselors turn the exercises into games! https://t.co/F2uMFpSSLs
— D'Amore Injury Law (@DAmoreInjuryLaw) July 31, 2019
— Tom von Alten, Boise, Idaho
Prescribing A ‘Deep-Dive’ Into Hospital Excesses
I think KHN Editor-in-Chief Elisabeth Rosenthal’s piece on hospital excesses is right on the mark (“Analysis: How Your Beloved Hospital Helps To Drive Up Health Care Costs,” Sept. 5). I was affiliated with a New York City hospital as a voluntary internist and retired four years ago. I wonder if it would be possible to do a “deep dive” analysis of a representative hospital’s charges and expenditures (several New York hospitals come to mind as candidates) by an investigative reporting group. I suspect there is a lot of money being spent that does not enhance patient quality of care (i.e., excessive numbers of administrators getting egregious salaries). I think you’ve discussed the salient reasons these contributing cost factors have not been widely discussed or debated ― but they must be.
I remember a news story about a patient who bought his artificial hip implant in the U.S. wholesale and, to save money, took it with him to Belgium to have it inserted. The hospital looked like a factory, and he was reluctant to go in — but he did, and as it turned out everything went well and he saved a lot of money!
― Dr. Lawson Moyer, New York City
from Updates By Dina https://khn.org/news/september-letters-readers-and-tweeters-patient-rights/
0 notes