#and like. ive engaged in some RISKY behavior
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr Inc. is funded by 13 investors.
Text
Ok, it's no surprise that I deeply enjoy Much Ado About Nothing as a play (and there are some truly delightful film and filmed staged productions), and there's a lot of talk about the scene between Beatrice and Benedick after Hero and Claudio's aborted wedding (Act IV, scene i).
What I don't see a lot of though, is how Benedick literally accidentally talks Beatrice into asking him to kill Claudio.
Yeah, Beatrice didn't walk into that scene ready to ask BENEDICK to make this right. Let's walk through the lesser-quoted lines from this scene.
We all know the iconic, "Lady Beatrice, have you wept all this while," but then we get this little exchange:
Benedick. Surely I do believe your fair cousin is wronged. Beatrice. Ah, how much might the man deserve of me that would right her! Benedick. Is there any way to show such friendship? Beatrice. A very even way, but no such friend. Benedick. May a man do it? Beatrice. It is a man's office, but not yours.
Benedick asking if a man may do "it" is a blatant offer to try to fix things, but it's pretty damn clear at this point in the text that he has big-ass heart eyes and hasn't thought this offer through, because the way to right Hero is to either get Claudio to recant--which he's not going to do because that is going to make him look like an absolute dingus and it will embarrass Don Pedro--or else to kill him in a duel. To ask a man to kill his best friend--even if that best friend is a complete and utter chungus--is cruel. It is one thing to call a friend out for being a dick to Hero, but to ask for Benedick's to be the hand that kills Claudio is a whole other level that Beatrice is going out of her way to excuse him from.
She is explicitly--and correctly, frankly, given the chains of command and power dynamics involved--excusing Benedick from being responsible for Claudio's behavior and correction. And while yes, part of dismantling the patriarchy is men holding each other accountable, murder is not accountability, it's the beginning of a goddamn blood feud. So Beatrice is over here very subtly going "You have clearly not thought this offer through, and I'm not going to ask you to kill your best friend." It is not his office.
And rather than hearing what Beatrice is saying, Benedick goes and MAKES IT HIS OFFICE by declaring his love for Beatrice. Which like...aside from this being not the moment, it just makes it even clearer that Benedick is not actually listening to Beatrice here. His focus is on her, but Beatrice is razor-focused on Hero and the fact that Claudio just more or less ended Hero's life. But here's the other thing.
I subscribe to the "Beatrice and Benedick had a prior relationship before the play and it ended badly" theory, because I think it explains a lot about their dynamics. But that also makes this scene a little bit risky and pointed. Because yeah, while Beatrice warns him not to swear he loves her and then eat his words, if they have a history, then her "Kill Claudio" is not just a request. It's a test.
He already didn't choose her once, presumably for way lower-stakes reasons. So to ask him to choose her, to be on her side, with all of what that means, is a test of a possible new relationship. And it's one Benedict comes perilously close to failing, because of course he's not going to kill his best friend and brother-in-arms.
And just like that, Beatrice is out, because Benedick "dare easier be friends with [her] than fight with [her] enemy." His choice is not her, and she will not be anyone's second choice. Especially given that choosing Claudio means that Benedick is engaging in the infuriating mental gymnastics where Hero can have been done badly wrong, but Claudio somehow isn't Hero and Beatrice's enemy.
This is not a complicated situation; Claudio was absolutely in the wrong, caused harm, and needs to be called on the goddamn carpet for it, and Benedick is over here trying to "both sides" it. I'd have been out too, and then he has the nerve to insist that he and Beatrice be friends before she's allowed to leave the stage! I adore that she then full-on goes off on him, and every single time Benedick tries to get a word in edgewise, Beatrice comes up with another argument and just cuts his ass off. There is no "letting him explain," there is no "I'm just playing devil's advocate," there is no "trust me, I know Claudio." There is only the facts of what happened, and Beatrice hammering them directly into Benedick's head. Lots of productions cut out the attempted interruptions by Benedick in favor of letting Beatrice run with a monologue, but if you look at the text, he tries FOUR SEPARATE TIMES to interrupt her.
But Beatrice just steamrolls on, and the thing is, it works.
Beatrice hits and refutes key arguments that we can just imagine Benedick bringing up. The bullshit logic of him being in a romantic relationship with Beatrice while supporting Claudio's actions. The undeniable public slander of Hero. The bullshit that is slut-shaming and measuring a woman's worth by her virginity. The divide between an "ideal" manhood and the reality of men's behavior. The nonsense that is how easily men are valorized for slandering women. Every point brought up and thrown in Benedick's face until he is left with only one final question; the only possible question that could matter at the end of this scene:
Benedick. Think you in your soul the Count Claudio hath wronged Hero?
And Beatrice is very, very sure. Which ultimately is enough for Benedick to choose her, and agree that yeah, Claudio needs to be called out and corrected, and he is now on board with taking that responsibility.
It is kind of wild to me that this scene begins with Beatrice trying to protect Benedick from the reality of the situation, and insisting that if he wants to be in love with her, if he wants to be in her life again, then this time he has to choose her for all that that means. And as Beatrice makes clear, what that means is a disruption--if brief--of the patriarchy and the status quo. Being with Beatrice means that Benedick has to stop being the prince's jester and stand against toxic masculinity and harmful patriarchy in a real, concrete way.
It's Shakespeare, so that doesn't stick beyond the happy ending, but it is here, and Beatrice really said "if you want to be with me, you have to stand with and for me and the women around me" when it was clear Benedick wasn't taking no for an answer.
35 notes
·
View notes
Text
ok living up to pinned post w some true confessions/dark secrets… so basically after i tried to kms in 2021 fall and went to the hospital i entered a really intense slut era and like started impulsively spending money and stuff too and i didnt have a job so i was like oh omg having a sugar daddy would work out really well for me and also i wanted to do things that would be like damaging or whatever idk why i did it rly. but anyway i engaged in some sugar baby behaviors. and then that winter break i went home from school and met up w some of my friends who ive known since i was a kid. now i have to give a little bit of context here cuz its important. so i have these 3 friends, one of whom ive known since i was 3 years old (N) and the other two since i was like 7 (S and J). and we all live in a very tight knit neighborhood/cultural community where mostly everyone knows everyone. and so my 3 friends parents know my parents. i guess you can see where this is going… but anyway i told them i had a sugar daddy or like it came up in conversation idk. and that was that. then literally the following AUGUSTTTT my mom comes to me and is like oh so some people in the neighborhood have been saying that you’ve been engaging in risky behaviors with older men and that youve been meeting them in hotels. so obviously i denied it very emphatically and tried to pry out who tf she heard that from and honestly i was like what like who could have even spread that and she said J’s mom told her and was lowkey rly cagey about it bc she didnt want to “break her daughter’s trust” and had asked other aunties about the situation like wtfff… and then i remembered i had mentioned to them over winter break so she must have fucking told her mommmm. i decided to assume best intent and chose to believe she was worried abt me and thats why she told her mom so i messaged her like hi did u tell ur mom abt this and i appreciate ur concern but i would have appreciated it if maybe u came to me directly and checked on me it would have been better and u lowkey hurt my feelings cuz now im stressed and anxious and don’t know whos saying what abt me etc etc. and then…
she fucking LIEDDDDD she said she didnt say anything to her mom AND that her mom didnt say anything to my mom!?? which i know is fucking bullshitttt 😭 like it makes 0 sense like if no one said anything is my mom just pulling shit out of the air and if she was how would she land straight on the money like that it just doesnt add up. so i was like um ok ?? uh have a good day. and decided to let it go and i lowkey don’t speak to her anymore and i told N and S that im not speaking to her but they can hang out w her if they want. and i forgot abt it.
but now i just moved back home after finishing school and its lowkey been eating away at me. it hurts me that she was my friend for 13 years and its all up in flames and i never got any closure or an apology or even her to admit or acknowledge the situation?? it hurts me to be at home worried abt what people are saying or thinking about me. i know i shouldnt care but what other people think of me bothers me. im not ashamed of myself and my choices but i don’t want other people to think less of me. i don’t want to reach out to her bc what if she doesn’t care at all about the situation ??? i don’t want to be like this has been eating at me forever and it really hurt me and her to be like what r u talking about i don’t think about you at all. she also just got into med school and im happy for her for real like glad shes doing well its just like. she hurt my feelings really bad :(
anyway if you read this far… what should i do 🥲 is the only path forward trying to let go… tbh i think i just need someone to validate my feelings like am i right to be hurt or is it all my fault and should i beg for forgiveness 😭 like my friend N got coffee w her a couple weeks ago and brought it up to me twice what does that even meannnn
13 notes
·
View notes
Note
tw general mentions of mental health
so i have this friend. let's call them emily. i've known emily for two years now, and they've grown to be one of my closest friends. mostly because we both really struggle with mental health stuff and at that point in my life no one else knew about those struggles. we helped each other through a lot of really crappy stuff and times. the difference is, in those two years, i've gone to, and am still in therapy, and have learned coping skills, have a support system etc etc etc ive tried convincing emily (on numerous occasions) to do the same, but they consistently refuse to do so, and they still pretty much only have me. there's also a ton of other stuff, but i could write a ten page essay about that. pretty much, our friendship, even though it's great feels kind of one-sided where im reaching out and they take weeks or months to respond (if they do at all) and dont really talk to me when we see each other in person and it's just getting really draining emotionally. so a few days ago, i finally make the decision to, well, not cut them off but pretty much tell them i'd had enough and im going to take a break for a while. they responded and pretty much just went straight to the self-deprecation (pretty much im sorry im so worthless and can't even maintain a friendship). and while im just so relieved that i've cut them off, more or less, to some degree, im just so worried since im all they have and if im gone who knows what will happen. so what should i do?
sorry for the long message
hum, that’s a tricky one.
First things first, I’d shove a WHOLE lotta resources on mental health in their messages. I know it may seem like your annoying them, but if it’s that bad they deserve to know there’s helplines and chats and groups that they can turn to. (I suggest vet them before you send them)
Secondly, sometimes it’s hard for people to realize they are allowed to reach out for help. Even if they only think it’s minor or it will take valuable space for others that “ are worst than them” But they have every right to reach out for help, their allowed to go to people with minor issues or major issues. And if you can somehow get that through their head you’ll probably see some improvement.
thirdly, I don’t think they can access traditional in person therapy as it seems. You can never know why, personally for me it’s a whole BIG awful talk about my mental health that I never want to tell my family. And it might be a similar situation with your friend, so unorthodox ways to get that same therapy experience might benefit them alot.
fourthly, you can’t help everyone. Sometimes it’s on them to figure out how to cope and understand how to get better, and even though you love them and care deeply it’s hard to get them to understand that. If you’re worried your friend might be engaging in risky behaviors (S/H, alcoholism, drugs, suicidal behavior, taking too many risks for no apparent reason.)
I suggest trying to talk to them about harm reduction.
fifthly, you being emotionally drained and exhausted by being their therapist friend is totally valid. your friend saying self deprecating things is just a symptom of a bigger problem they have, it's not your fault or anything you need a break from them. if they were in the same situation they would do the same thing, it's hard to manage both your mental health and your friends. I don't blame you for being exhausted, the reason I do this stuff is because I'm exhausted by my own problems and this is a healthy and constructive way to help both you and me. your helping your friend out of love, but also obligation.
I think a good plan to do is.
give your friend a pep talk and show them tons of alternate ways to access therapy that is not in person.
give them helpline information and tell the "I've known you for so long, I'd never try to hurt you. I just want you to know there's options if life gets hard and I'm not around
tell them about harm reduction, and CURB any and all negative connotations about addiction and self harm. if they are suffering the best thing you can do is be accepting and show them ways to safely and also reduce the harm of the addictions/self harm.
tell them if they are being abused. in anyway period, they can trust you to not victim blame or something without knowing the full story. we don't know what's happening with them, but we have to be kind and caring if that's the reason for her mental health. tell them "it was never your fault, you didn't know." or "you were just a kid, it was never you that was the problem but how you were treated. it's okay to be upset or angry, or grieve the life you should have had. that's normal. trust me I'm here for you."
also if the whole abuse thing is a yes, give them tons of abuse helplines. you and I don't know how to go forward with that knowledge but the helplines know how to.
support them and tell them truely why you feel drained (if you Hadn't already.) and tell them you actually care alot about them and this is not an attack or that your mad at them or anything. your overwhelmed too, and you both should feel not overwhelmed. (VERY IMPORTANT, YOU HAVE TO SAY YOUR NOT ANGRY OR ANYTHING. mentally ill people tend to think the worst if you don't say it. be kind and caring, and they should not feel so bad.)
if that doesn't work, I think you yourself should call a helpline and ask about strategies to help your friend. they should know a lot more than both you and me.
thank you for sending an ask in, this has been interesting!
I hope you can figure out a way to help your friend.
if worst comes to worse, I suggest you give your friend character.ai's psychologist's link to your friend. it's better than nothing, and it's surprisingly helped me too. so it might help your friend open up.
here's the link LINK
I hope I was able to provide a push in the right direction, remember this is the BAD advice blog. not everything will work, sometimes we both have to fail a bit to figure out the best way to help people.
#-belle/pop#the bad advice blog#send me anons#mental ill health#mental illness#mental health#answered asks#answered questions#anon#anon ask#asks#anonymous#anonymous asks
3 notes
·
View notes
Text
@random-thought-depository
"AIDS denialists keep dying of AIDS" - If this is so it actually seems noteworthy to me that this happens/non-obvious to me that it would! The behaviors you need to do to avoid being at high risk of AIDS are behaviors lots of people do for reasons besides trying to avoid getting AIDS! Is a lot of AIDS denialism motivated reasoning for wanting to have lots of sex with lots of partners without bothering with condoms or other anti-STI measures so people who aren't attracted to that lifestyle and/or just aren't sexually successful enough to actually live it are less likely to become AIDS denialists?
my thoroughly non-expert-impression is that western aids denialism consists mainly of two camps: conspiracy-brained folks many of whom were looking for ways to score Daring Heterodox Thinker points, and hiv patients in denial looking for alt-medicine cures, with the former (and outright grifters) encouraging some of the latter. the settling of remaining scientific questions around hiv in the 90s and then the development of highly effective retroviral drugs has quelled a lot of the former group, at least in the west; the latter are self-limiting, as they keep dying (and now with the development of therapies like PrEP, fewer people are getting hiv to begin with).
"people who are at risk of catching hiv and want an excuse not to change their behaviors" seem overall to have always been a marginal group, not representative of most prominent western aids denalists. if you're willing to engage in high-risk behavior like sharing iv drug needles, you're sort of by default the sort of person who doesn't need an excuse to engage in that behavior, beyond the low likelihood any given sexual encounter will lead to contracting HIV. mostly what you need is an excuse not to engage in risky behaviors, which is why stuff like needle exchanges are a good idea, since they minimize the friction involved in switching to lower-risk behaviors, and that helps a lot at the margins.
(a lot of the prominent western hiv-positive aids denialists seem to have been women, which perhaps fits with women being generally more open to alternative medicine in general)
AIDS denialism is kind of an interesting example of crackpot bullshit in that it's sort of self-censoring, in that AIDS denialists keep dying of AIDS. makes it a lot harder to keep going as a concern than the flat earthers or creationists.
#annual new hiv infections and aids-related deaths have been declining worldwide since the mid-2000s#at least until this year#i find it hard to tell how much of pepfar is actually up and running right now#obviously i can comment even less on the dynamics of aids denialism in regions like south africa
52 notes
·
View notes
Text
What is a relationship to be continued
You may ask yourself why this is Important yet it is very important! We will discuss Why they are important to your well being and what type of person you are in a relationship? I think if you take the time to read this post in its entirety and intense complexity you will have a better understanding of where you are in life and what more you can become by understanding the perplexity of every relation to man or relationship because trust me THIS BABY is going to get TOUGH.
Lets start of with the first question what is a relationship
the way in which two or more people, groups, countries, etc., talk to, behave toward, and deal with each other. : a romantic or sexual friendship between two people. : the way in which two or more people or things are connected.
Please go ahead and read one more time because that may or may not be the closest thing of a relationship to that you have a mutual relation and understanding of but its way, way more complex just keep reading.
Each relationship we have encountered has been determined by how we were raised Im going to refer to some quick psycho-social information coming from a study introduced during world war 2 by British psychoanalyst john bowbly, whose lonely childhood gave him a lifelong interest in the power of parenthood.
In the 1970s a test was conducted by Bowlby’s student Mary Ainsworth. She performed the strange situation test where children that's age ranged from 12-18 months were put in a toy-filled room with their mother and given a chance to play. A stranger enters and interacts with the parent and child,then mom exited the room-- leaving behind a confused and alarmed little kid. A few minutes later mom returned and comforted her toddler. Needless to say being separated from the person who feeds, protects, and tends to you is frighting for any toddler, but the test showed definite categories of reaction to that fear.
Why is this important ?
Early Attachment.
As seen above you can see that a study was conducted concerning attachment styles. It's important because it is with this information that you find out what type of relationships You are going to be compatible with. Some types absolutely do not collide but if you think this is all about “how do i form a relationship” well keep reading because its not possible for everyone.
1 Secure, when it is evident to have a secure attachment style when the parenting style was: Warm, attentive,relatively consistent, and quick to respond based on that approach the child's Baseline Emotional Status (BES) would have been happy, confident, and curious which would have subconsciously continues into adulthood with the Child’s expectation of life being: My need will be met
2. Anxious -Ambivalent/resistant, it is evident to have an anxious attachment style when the parenting style was: Inconsistent: sometimes responsive and sometimes not. The Child's BES would have been Insecure, anxious, and intensely emotional which in return would have subconsciously continued into adulthood with the child's expectation of life being: “IF i act in the right ways, I might earn love and my needs may be met”
3. Avioident- ,it is evident to have a avoidant attachment style when the parenting style was: Distant and Cold, or harsh and critical. The child's BES would have been Emotionally shut down which in return would have subconsciously continued into adulthood with the child's expectation of life being: “I can't trust anyone to meet my needs. I must meet my own needs.
Im sure your getting the idea of why this is now important
Lets looks at three statements
1 I find it relatively easy to get close to others and am comfortable depending on them. I don't often worry about being abandoned or about someone getting too close to me.
2. I find that others are reluctant to get as close as I would like. I often worry that my partner doesn't really love me or doesn't want to stay with me. I want to get very close to my partner, and this sometimes scares people away.
3 i am somewhat uncomfortable being close to others: i find it difficult to trust them completely, difficult to allow myself to depend on them. I am nervous when anyone gets too close, and often, love partners want me to be more intimate than i feel comfortable being
In 1987 psychologist cindy hazan and philip shaver reported the results of the statements above they called it the ‘love quiz’
56% of adults respondents had identified themselves as secure, 19% as anxious and 25% as avoidant
The perfect combination
Secure people tend to have the most secure relationships, and a relationship needs only ONE secure partner to get that stability. With a partner who is happy to give reassurance and isn't threatened by the idea of being needed, an anxious person can relax, and is often loyal and loving. With someone who doesn't take it personally when their partner wants time alone,avoidant people can worry less about being tied down- however, most of the compromises in the relationship will likely be made by the secure partner. The real problem comes when two insecure types get together. If relationships often get messy for you, learning to recognize attachment styles and understanding how they clash can give you a path through the conflict
But then again Here comes perhaps the most perlex question i can ask? What happens in adult hood when you experience the pain and turama of a heartbreak?
What particularly does that do to each individual and how do they cope?
Do some people perhaps just shut down! Absolutely not! One subconsciously gains the ability to cope with their losses how? Lets start with:
Sexual compulsion – Relationship with sex, attachment and sexual orientation
I know your wondering What the Fuck where did this just turn to but trust me, or dont but you may or may not want to hear this or perhaps your brain craves the knowledge to understand and you ask yourself why your life is working in the way it is; remembemer its all in you!
I believe the first coping skill for some may be Hypersexuallity which I will refer to later.
2. I believe a conduct Disorder DSM-IV-TR 314.9 Is primary consistent with feelings of Emotional shock from a previous ‘heartbreaking’ or traumatic event.
I will explain. I'm going to refer to the diagnostic features of conduct disorder which manifest itself as a repetitive and persistent pattern in which the basic rights of others or major age-appropriate societal norms or rules are violated. These behaviours fall into four main groupings” Criteria A1-A7 aggressive conduct that causes or threatens physical harm to other people or animals .
Or see criteria A8-A9 nonaggressive conduct that causes property loss or damage Or see A9 - A13, DECEITFULNESS OR THEFT
It is definite that promiscuous behavior is dangerous therefore someone engaging in Criteria a1-a7 w/o aggression and associated with parts or in hole with A8-9
Furthermore the prevalence of conduct disorder appears to have increased over the last decades and may be higher in urban than in rural settings.
Course.
Individuals with conduct disorder are at risk for later mood disorders, anxiety disorders, somatoform disorders, and substance related disorders.
Sexual addiction, also known as hypersexual disorder, is associated with serious psychosocial problems for many people.
Sexual addiction, which is also known as hypersexual disorder, has been associated with serious psychosocial problems for many people although it has not been recognized as a disorder that merits inclusion in the DSM (Quadland, 1985) – see Karila et al. (2014) for review. Originally, Carnes (1983)published a book titled Out of the shadows: Understanding sexual addiction, which has raised interest in the area and facilitated a discussion on the best way to define and diagnose the disorder. Despite different views about pathological characteristics of sexual addiction there is an agreement that this is a progressive relapsing condition which does not merely refer to a pathological diagnosis of sexual lifestyle that is socially deviant (Edger, 2010).
Sexual addiction involves compulsive behaviors such as constantly seeking new sexual partners, having frequent sexual encounters, engaging in compulsive masturbation and frequently using pornography. Despite efforts to reduce or stop excessive sexual behaviors individuals find it difficult to stop and they engage in risky sexual activities, pay for sexual services and resist behavioral changes to avert HIV risk (Carnes, 1991; Coleman-Kennedy & Pendley, 2002; Coleman, Raymond & McBean, 2003; Kalichman & Rompa, 1995). Sexual compulsivity has been associated with the number of unprotected vaginal sex acts with female sexual workers, lower self-efficacy for condom use, greater use of illicit drugs, and more financial need (Semple et al., 2010).
Cognitive and emotional symptoms include obsessive thoughts of sex, feelings of guilt about excessive sexual behavior, the desire to escape from or suppress unpleasant emotions, loneliness, boredom, low self-esteem, shame, secrecy regarding sexual behaviors, rationalization about the continuation of sexual behaviors, indifference toward a regular sexual partner, a preference for anonymous sex, a tendency to disconnect intimacy from sex, and an absence of control in many aspects of life (Carnes, 2000, 2001; Carnes & Schneider, 2000; Coleman et al., 2003; Coleman-Kennedy & Pendley, 2002). Finally, some studies find that sexual addiction is associated with or in response to dysphoric affects (Black, Kehrberg, Flumerfelt & Schlosser, 1997; Raymond, Coleman & Miner, 2003; Reid, 2007; Reid, Carpenter, Spackman & Willes, 2008; Reid & Carpenter, 2009) or stressful life events (Miner et al., 2007).
Attachment theory (Bowlby, 1979, 1982) argued that early attachment experiences affect personal and social life, professional relationships, dealing with stress, mental and physical health and cognitive development. According to recent developments in attachment theory, those who developed a safe attachment style which is not anxious or avoidant during infancy can form healthy relationships in adolescence and adulthood and handle life problems (Uytun, Oztop, Esel & Mdusunen, 2013). Individuals with secure attachment are expected to have low chances of becoming addicted to sex since they regulate and limit their sexual activity more than those with insecure attachment (Zapf, Greiner & Carroll, 2008). Furthermore, individuals who are addicted to sex are looking for sexual activity without the need for emotional relationships and they are more likely to be characterized by avoidant or anxious attachment (Gentzler & Kerns, 2004).
Gay men are diverse with respect to the sexual behaviors they both desire and enact (Moskowitz & Roloff, 2010; Sanderson, 1994). Moreover, gay men differ from other groups in their sexual behavior. Research shows that, on average, gay men have more partners, engage in more risky sexual behavior, and are more likely to seek sexual sensation than other groups, such as heterosexual men, women and lesbians (Bailey, Gaulin, Agyei & Gladue, 1994; Ekstrand, Stall, Paul, Osmond & Coates, 1999; Thompson, Yager & Martin, 1993). But among homosexual men there is variability in the propensity to engage in compulsive unprotected sex. Meyer and Dean (1995) have reported that about 6% of their 149 young New York City gay men (aged 18–24 years) engaged in very high risk behavior, defined as unprotected receptive anal intercourse with multiple partners. It appears that very high risk takers are qualitatively different from other risk takers: they reported more mental health problems, including more drug use and higher levels of internalized homophobia and AIDS-related traumatic stress response. Furthermore, there are moderators of sexual behavior among gay men such as being in monogamous relationships. Also sexual health and sexual health behaviors for example sexually transmitted diseases (STDs) were most influential over the enactment of sexual behavior or desires (Moskowitz & Roloff, 2010).
Few studies investigated sexual compulsivity among heterosexual and homosexual men. Furthermore, to the best of our knowledge, the relationships between compulsive sexual behavior and attachment and sexual preference or orientation have not been investigated before. We have therefore investigated sexual compulsivity and attachment style among populations of heterosexual and homosexual men and women. We hypothesized that secure attachment would be associated with lower rates of sex compulsion. Secondly, that homosexual men and women would show higher levels of sexual compulsivity than heterosexual men and women. Thirdly, we hypothesized that attachment style might mediate between sexual orientation and sexual compulsion.
2 notes
·
View notes
Text
Lupine Publishers | Counseling Case Report: Smoking Cigarette
Lupine Publishers | Scholarly Journal Of Psychology And Behavioral Sciences

Abstract
This paper is a counseling case report of 15 sessions on a client who has been diagnosed with smoking cigarette from Kelem Worq Preparatory School. CO6 was an 18 -year-old grade 12th social stream student in Keleme Worq Preparatory School. CO6 was the second of the four children in his family. Assessment tools included a detailed interview and behavioral records. CO6 has been smoking cigarette since grade eight. At the time of counseling CO6 smoked five per day. CO6 drunk 4-6 glasses of beer occasionally, has done this for several years. Other than these drugs no other drug use reported. Many factors identified during the assessment were considered critical in accounting for the cause and persistence of CO6’s cigarette smoking [1,2]. Cognitive behavioral counseling was the theoretical framework that informed the case formulation. The counselor used self-reports of the client as outcome measures. SQ3R study method, the five Ds and cognitive behavioral therapy technique were applied to solve the client’s major problems of academic, smoking and alcohol drinking problems, respectively. Progress was evident by improved class attendance, more sustained focus on her academic studies, and continued improvement in sleep. The client has minimized his cigarette smoking and stopped his alcohol drinking.
Introduction
This paper is a counseling case report on a client who has been diagnosed with smoking cigarette from Kelem Worq Preparatory School. The assessment part has included the necessary identifying information with appropriate changes to shield the client’s real identity [3]. As part of the treatment plan the presenting problems will be identified and matched to the criteria set forth in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition text revision (DSM-IV-TR) multi-axial diagnosis( its new version is also available, DSM-V).
Nicotine or Tobacco Use Disorders
Tobacco Use Disorder according to Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), diagnosis assigned to individuals who are dependent on the drug nicotine due to use of tobacco products. Tobacco contains the psychoactive drug nicotine, which is a central nervous system stimulant. The immediate effects of nicotine administration are tachycardia, hypertension, increased respiration, hyperglycemia, enhanced memory storage, improved concentration, and appetite suppression. Nicotine can be taken through several routes, including inhalation (smoking cigarettes, cigars, or pipes), chewing tobacco and snuff [4-8]. Nicotine produces dependence and withdrawal symptoms upon cessation of use, the onset of which occurs about one hour after the last dose. Withdrawal symptoms include irritability, annoyance, anxiety, and cravings for nicotine. Substance abuse disorders have high comorbidity with tobacco use disorder. People in early recovery from other drugs or alcohol tend to smoke heavily or chew tobacco. Features of tobacco products that enhance their addictive potential include the rewarding properties of nicotine, the behavioral reinforcement of the hand- to -to mouth habit, lack of social support to cease smoking, the ease of access of tobacco products, and the cultural acceptance of tobacco products. Another factor which enhances nicotine’s addictive qualities is bioengineering by tobacco companies, which add ammonia to nicotine to facilitate absorption and bioavailability (Figure 1). The Diagnostic and Statistical Manual of Mental Disorders indicates that risk factors for Tobacco Use Disorder include low-income levels, low level of Education, and diagnosis of the following disorders: conduct disorder, depressive disorder, anxiety disorders, personality disorders, psychotic disorders, and other substance use disorders. There is also a genetic component to Tobacco Use Disorder (American Psychiatric Association, 2013).
Case Description
CO6, code name of the client, was an 18-year-old grade 12th social stream student in Keleme Worq Preparatory School. He was the second child among the four children. His father was 55 years old and lives outside Addis Ababa due to his workplace, but he visits his family in every weekend day. C06 had smooth communication with his father. His mother was housewife and learned up to grade 12. C06’s mother was a smart for him, and she communicates friendly. His oldest sister in the family was 22 years old, and she was indulgent, reluctant to take great care of others. The rest younger sister and brother are 14 and 8 years old, respectively, and both of them have good communications with him. C06 described his parents’ parenting style as democratic. C06’s birth and childhood time were normal. He grew up in a close and loving family and recalls a happy childhood, and uneventful adolescence. As he reported that his parents were supportive and sensitive to his needs and encouraged his to be independent and responsible. CO6 describes himself as a “good boy” who excelled socially and involved in many extracurricular activities. But he described himself as not good boy in academic performance as he was socially. He had a healthy self-esteem growing up and never engaged in risky behaviors or got into trouble other than smoking cigarette and drinking alcohol. CO6’s peer relationships during childhood and adolescence were good and he remains close with several high school friends and he was remembered by his jocks. CO6 had also developed good peer relationships with neighborhood children and enjoyed with them sometimes. CO6 dated during elementary school and had a few casual relationships while he was high school students. Still he has not serious romantic relationship with anyone. CO6 struggled to get out of bed in the morning, sometimes missing his morning classes. He stays up until 8:00 or 10:00 pm for eating and watching TV but he did not have much involvement during super time. And he had good self-esteem towards himself and had not suicidal ideation and never attempted suicide. Until this professional contact CO6 had not seen by any other professionals for a serious physical or mental problem.
Clinical Assessment
I would like to inform you that I have had 15 sessions in person with this client. The clinical assessment included a clinical interview and behavioral observation. CO6 has been smoking cigarette since grade eight. At the time of counseling the client smoked five per day. He started smoking again after awaking the first cigarette smoked was within the first 30 minutes. CO6 drunk 4-6 glasses of beer occasionally, has done this for several years. He didn’t see alcohol drinking as a problem. CO6 always smokes while drinking alcohol and CO6 used coffee sometimes. Other than these drugs no other drug use reported. When CO6 became depressed he wants to smoke. In addition to his depression, head ace, watching his friends while they smoked or handed cigarette, drinking alcohols and sometimes his low performance in academic were the most triggering factors for his desire to smoke. CO6 had no past successes with behavior change: Quit smoking twice when he was grade nine for 2 months but relapsed. He, at the time of counseling, wanted to quit smoking to prevent the medical and social consequences of smoking. Even if CO6 was ready to quit at this time, CO6 was worried about his ability to succeed in his quitting. His limited time for self-care, peer pressures, his low selfconfidences to quitting, absences of social supports from his schools and families and his alcohol consumptions were his potential barriers to quitting. However, his strong motivation, strong health reasons, one previous quit attempt with some duration (2 months), his high self–esteem towards himself and, friends who want to quit with him were the assets of the client.
Diagnostic Formulation
Based on the assessment findings in the initial interviews, the following diagnosis was formulated. Axis I: Substance abuse (cigarette smoking and alcohol drinking). Axis II: No Axis III: No Axis IV: Problems related to the social environment (inadequate social support), and Educational Problems (academic problems and inadequate school environment) Axis V: Moderate functioning
Case Conceptualization
Several factors identified during the assessment were considered critical in accounting for the etiology and persistence of CO6’s cigarette smoking. Cognitive behavioral model was the theoretical framework that informed the case formulation. The emphasis placed on developing a case formulation leads to treatment goal-setting and planning. CO6 was an eighteen-year-old boy who came from a medium class family. His chief complaint when he met the counselor was that he smoked cigarette accompanied by symptoms such as withdrawal and tolerance symptoms. CO6 said that he can’t concentrate in attending classes every day, which was why CO6 said he left school to smoke cigarette after break time. As the clinical interview revealed that the client had not exposed his smoking for his parents. CO6’s most serious problem was his cigarette smoking. From a behavioral perspective, these impulse control difficulties may have developed because of faulty learning experiences, including pressures from his close friends in school and neighboring, his modeling of his significant others’ behavior and lack of guidance from parents. For CO6’s problem behaviors, precipitating factors included alcohol drinking, holding of cigarette by his friends and watching of theses friends while smoking , going to toilet with friends at break time and his thought of ‘’I am poor in education”. Client’s perpetuating factors included his poor quit attempts, no support at school, withdrawal symptoms associated with cigarette smoking and his low self-confidence in succeeding in quitting cigarette smoking. CO6’S strengths include his sociable behaviors with school and neighboring friends. CO6 has a strong desire to quit smoking as CO6 believed that health and social consequences of cigarette smoking was inevitable. The counselor selected cognitive behavioral therapy for this client to solve his problems of cigarette smoking and its associated symptoms. It has been shown that cognitive-behavioral therapy, combined with a smoking cessation medication (such as the nicotine patch, nicotine gum, for example), is quite effective for smokers who are motivated to quit. Cognitive-behavioral counseling is an evidenced-based psychological treatment that focuses on identifying and changing maladaptive thoughts, emotions, and behaviors that trigger, worsen, and/or maintain a range of problems (such as depression, anxiety, addiction, etc.). Because changing your smoking-related behaviors-and restructuring your thoughts related to smoking urges- is essential to quitting, cognitivebehavioral counseling can effectively be applied to smoking cessation. An intensive cognitive-behavioral therapy program is typically composed of three phases: preparation, quitting, and maintenance (or relapse prevention).
Treatment Plan and Course of Treatment
Based on the case formulation, CO6 and the counselor collaborated in the development of the following prioritized list of problems and treatment goals. The order and relative importance placed on these goals was largely determined by the client, although there was input from the counselor in directing treatment efforts to goals that would have the most impact on CO6’s cigarette smoking and its associated symptoms, and had the greatest likelihood of success. The treatment plan followed the problem format, a format that presents the target problems with its major goal and objectives and intervention methods in structured form.
Problem-1: low academic performance a) As evidenced by: low results grade to grade. b) As evidenced by: poor class attendance. c) As evidenced by: lack of study skills. d) As evidenced by: absent from schools. e) As evidenced by: late in the morning to go to school.
Goal-1: to improve academic performance Objectives and Interventions.
Objective-1: teaching study skills
Interventions: The SQ3R study method was employed to target co6’s poor study skills and to improve his academic performance.
Objective -2: Increase class attendances
Interventions: To improve class attendance, a behavioral contingency was developed to ensure CO6’s woke up by 7:00 am so he could attend all his scheduled classes for that day. In addition, CO6 would shower, eat a light breakfast, and walk to school. If he completed this schedule 3/5 days, CO6 would reward himself by going pool houses for the weekend or to the movies with classmate.
Objective -3: work on sleep difficulty
Intervention: Poor class attendance and an inability to study were major contributors to poor academic performance. It was decided to target CO6’s sleep difficulties that were a major cause of missing classes and daily fatigue that made it difficult to study. Maladaptive sleep-related behaviors were identified, and corrective homework assigned. The client and the counselor set up a sleep log and agreed to keep the sleep log, maintain regular sleep hours, eliminate daytime naps, to make sure the bedroom has oxygen, and restrict bedroom activities to sleep.
Problem 2: Cigarette Smoking a) As evidenced by: smoked for five years. b) As evidenced by: nicotine dependence withdrawal. c) As evidenced by: fugue out of school for smoking. d) As evidenced by: slum physical appearances.
Goal-2: Cigarette Smoking Cessation Objectives and Interventions.
Objective 1: To confront with the urge to smoke
Intervention
To achieve this objective the client and counselor applied the five Ds
a) Delay, even for a short while. b) Drink water. c) Deep breathing. d) Do something different and, e) Discuss the craving with another person.
Objective 2: Teaching different behavioral tips to quit smoking cigarette
Intervention tips
a) Write out a list of reasons to quit and display it prominently e.g. on wall. b) Get rid of all tobacco products, ashtrays, lighters, matches, etc. from all areas which you inhabit. c) Clean all clothes in order to remove cigarette smell. d) Enlist the support of non-smoking friends, relatives, and workmates. e) Change the environmental cues, e.g. the telephone often causes a reflex action to smoke, move the telephone to another place to change the cue. f) Keep hands busy e.g. knitting, gardening, drawing, origami. g) Sit in non-smoking areas. h) Positive self-talk. i) Try to avoid stressful situations in the immediate period after stopping. j) Set aside the money normally spent on cigarettes to buy something as a reward do not drink alcoholic beverages because these are associated with relapse. k) Avoid, even temporarily, social situations normally associated with smoking. practice saying, “No thank you, I don’t smoke. l) Ask other smokers not to give cigarettes, offer to buy cigarettes or smoke in the patient’s presence. m) Think positive and remember your reasons for quitting in the first place. n) View quitting as a day-at-a-time process rather than an immediate lifelong commitment.
Problem 3: alcohol drinking
Goal 3: To stop drinking alcohol: The psychologist also offered cognitive behavioral therapy techniques for his alcohol abuse and some behavioral tips.
Progresses
The counselor used self-reports as outcome measures. The therapist reviewed co6’s sleep log and daily activity record to evaluate the success of these interventions at modifying sleep behavior and class attendance. Progress was evident by improved class attendance and a more consistent bedtime routine. CO6 reported better class attendance; more sustained focus on her academic studies, and continued improvement in sleep. The client has minimized his cigarette smoking and stopped his alcohol drinking. The treatment is still under supervision.
Strengths and Weakness
Use of the core conditions of (empathy, genuine and unconditional positive regard) as relationship building throughout the whole counseling processes helped me to express my values, reactions, and feelings as they became appropriate to what was happening in the therapy sessions. It helped me to create a trusting working relationship with my client. The process helped the counselor to understand the value of supervision. The supervision helped the counselor to identify themes that had not been obvious to the counselor. It helped the counselor articulate the counselor role as a counselor. Supervision helped the counselor to identify areas where the counselor was not challenging my client enough and to be conscious of any manipulative signs by client and how to handle them. Supervision also helped the counselor to identify strengths in empathizing, listening, summarizing, and paraphrasing. Sometimes client would tend to talk very little and at such times the counselor would tend talk more and to give advice to my client may consider as weakness.
https://lupinepublishers.com/psychology-behavioral-science-journal/pdf/SJPBS.MS.ID.000188.pdf
https://lupinepublishers.com/psychology-behavioral-science-journal/fulltext/counseling-case-report-smoking-cigarette.ID.000188.php
For more Lupine Publishers Open Access Journals Please visit our website: https://lupinepublishersgroup.com/
For more Psychology And Behavioral Sciences Please Click Here: https://lupinepublishers.com/psychology-behavioral-science-journal/ To Know more Open Access Publishers Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers Follow on Twitter : https://twitter.com/lupine_online
#Lupinepublishers#Lupine publishers#lupine publishers indexing Journals#Lupine Publishers Group#sociology#cognition
0 notes
Text
Two Hundred And Four Reasons
Spartan-117 & Spartan-087
[Preface] // [Part 1] // [Part 2] // [Part 3] // [Part 4] // [Part 5] // [Part 6] // [Part 7]
With this past month marking the 4-year anniversary of this blog, I was somewhat at a loss as to what to do to commemorate the occasion...until I remembered there was one more thing I could post as an addendum to my essay series chronicling the development of John-117 and Kelly-087′s relationship throughout Halo canon. There were a few additional pieces of media featuring SPARTAN-II Blue Team that were released in the wake of 2015′s ‘Halo 5: Guardians’ that I think are worth taking a quick look at in regards to how they carry on the tradition of highlighting the bond between a certain Blue-One and Blue-Two.

Through All These Years
The first of the two is an animated miniseries (though more akin to a motion-comic) that loosely adapts the content of both the novel ‘The Fall of Reach’ and its comic book counterpart (which I’ve previously discussed). Like the comic before it though, this miniseries includes a few minor details that differ from the original source text in interesting ways.
The second is a short story from the comic anthology ‘Tales From Slipspace’, called “On The Brink”, and features some panels and dialogue that I feel are very relevant to the content I’ve analyzed so far in regards to Kelly-087′s character and her dynamic with John-117.
We’ll start with the ‘Fall of Reach’ miniseries. Most notably, the animation is bookended by a rather touching scene involving Blue Team returning to the glassed surface of the planet Reach (some time in between late-2557 and mid-2558) in order to hold a private memorial for Samuel-034. But I’ll get back to this after looking at the body of the animation’s content.
To preface: it is worth noting that the animation includes Fred-104 and Linda-058 in events at which they are not canonically present - mainly the “ring the bell” exercise as part of John-117′s team, and as participants in the assault on the Unrelenting in 2525. This was done in order to better familiarize a general audience with them as characters and the roles on Blue Team they would eventually come to fill in the years after the Spartan-IIs’ training in actual Halo canon.
Unlike the comic book version of ‘The Fall of Reach’s events, this miniseries does make sure to include the crucial lesson that John-117 learns from Chief Mendez after putting himself first during the trainees’ initial obstacle course exercise.

“You don’t win unless your team wins.”
Much like in the novelization though, Kelly in particular takes a stand against John’s selfish behavior before he proves he is willing to make amends for his mistake and commit to being a team player.


After the young members of Blue Team reconcile, we are then shown the Spartan-IIs’ wilderness training exercise that takes place two years later. And, in a new addition to this part of the story, we see Sam make a pit-stop to carve the symbol of an eagle and a lightning bolt (which would later become Blue Team’s insignia) into a tree in commemoration of the group’s friendship as John and Kelly look on and consider their next move. As described in ‘The Fall of Reach’, Kelly is noticeably taller than John as a child, which is a small detail I appreciate being included in the animation.

From here things follow the comic adaption pretty closely through the augmentation procedures and the Spartans’ first official mission to Eridanus Secundus to capture insurrectionist Colonel Robert Watts. A few nice asides are made throughout the entire animation where the members of Blue Team casually converse like normal teenagers (making jokes, encouraging one another, offering advice, invitations to do activities, etc.) when not directly engaged in mission-relevant dialogue. So it is good to see this kind of additional humanization of the S-IIs based off of what has long been established about them in Eric Nylund’s books.


Finally the last section of the miniseries is narrated by Kelly-087 herself in flashback (with Michelle Lukes reprising her role from ‘Halo 5: Guardians’), which covers the Spartan-IIs receiving their first sets of MJOLNIR Armor and Sam’s death at the hands of the revealed alien Covenant.
Without quoting every line she says, I will simply say this portion of the animation is well worth watching just for Kelly’s commentary. After Blue Team is outfitted with their suits of Mk. IV armor on Chi Ceti, we come to the Spartans’ infiltration of the Covenant ship Unrelenting. In a small departure from the novel and the comic book, Kelly is actually pulled aboard the vessel by John just as she is about to fly off into space - and though I doubt it was intentional, I find it is an interesting reverse-parallel to what we see in the ‘Halo Legends’ animated short “The Package” all the same.

From here events proceed in general accordance with canon, with Sam’s armor eventually breached by a plasma bolt after being shot while pushing John out of the line of fire. Once Blue Team makes it to the ship’s reactor, they hold off a few waves of Covenant while reading the bomb they brought with them to destroy it. John and Kelly work in tandem as Blue-One and Blue-Two; and in an amusing exchange of roles at one point, we see Kelly take charge of the situation and sprint across the bridge to shut the doors leading to the reactor room while ordering John to complete the work on the nuke.


“I’ll seal the door. John, finish arming that warhead!”
“I remember thinking that no matter how dark the future, we could face it as a team.”
However, as we all know, things reach a breaking point when Sam admits that he has to stay behind on the ship due to the irreparable damage to his armor. This part of Nylund’s book always struck me right in the heart, and the scene here is no exception. This moment is then bolstered by Kelly’s reflection on how this first loss in battle deeply affected not only her and John, but all of Blue Team.

“I know Spartans don't cry...but for once, I was glad for the helmet.”
“We thought training, augmentation, armor made us untouchable, invulnerable, immortal. Blue Team. But we were wrong - we were children. This was the only thing John was ever afraid of: losing one of us. And we knew we weren’t finishing this fight, we were just getting started.”
The animation then ends with the Spartan-IIs visiting the same place Sam originally “carved their mark into the world”. They take a moment to remember their fallen friend and reflect on the meaning of his heroic sacrifice, as the Chief sincerely asks his remaining comrades if they will continue to have faith in him to lead them through whatever lies ahead.


“Last time we were here, I asked Sam to trust me to take us home, to follow me. Will you trust me now? Will you follow me?”
...which plays perfectly into the next section of this write-up.
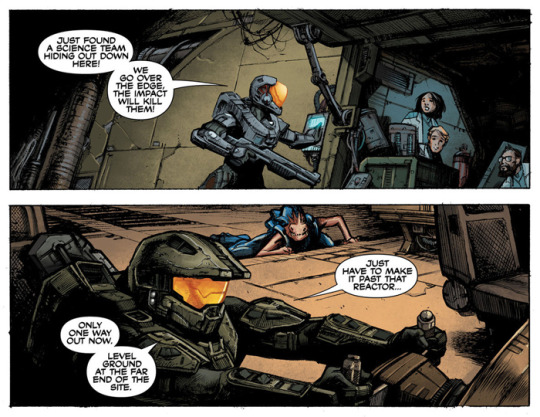
"On the Brink” is a short comic featuring Blue Team that was relased as part of the ‘Tales From Slipspace’ anthology book in the fall of last year. It takes place in 2558 and is a fairly self-contained story about one of the Spartans’ many exploits after their reunion in 2557. Specifically, they are looking to stop a Mammoth that has been hijacked by some splinter-Covenant from running into a UNSC nuclear reactor. Once again the events are overlayed with a narration by Kelly-087.
The 12-page comic can be viewed in its entirety here. And while it is brief and rather straightforward in terms of the story’s content, there are a few panels that I would like to take a closer look at. Most prominently, this section where Kelly muses on the steadfastness of the Chief’s leadership.

I love How Kelly notes that even though she’s dog-tired and in the middle of a violent firefight, hearing the voice of her best friend is all it takes to renew her focus, confidence, and determination to complete the mission - in a way nothing else can. For his part, John continues to rely Kelly to back him up and talks to her throughout the operation even as her discovery of some civilian scientists aboard the Mammoth forces him to make a risky evasive maneuver in order to save them. And honestly I don’t know what could speak more for the strength of the bond that these two characters have and the kind of trust they have in each other.
After the massive vehicle finally comes to a complete stop, the reactor remains intact and some extensive property damage to the surrounding area is the only fallout of the Covenant attack on the UNSC base. This does not appease the site’s foreman however, and he confronts Blue Team. John keeps his cool while Fred reacts angrily in turn to the man’s disrespect and thankless attitude. Kelly looks on, and can’t help but wonder when John will finally grow weary of the tumultuous and unsure environment the Spartan-IIs have found themselves mired in in the wake of the Human-Covenant War.
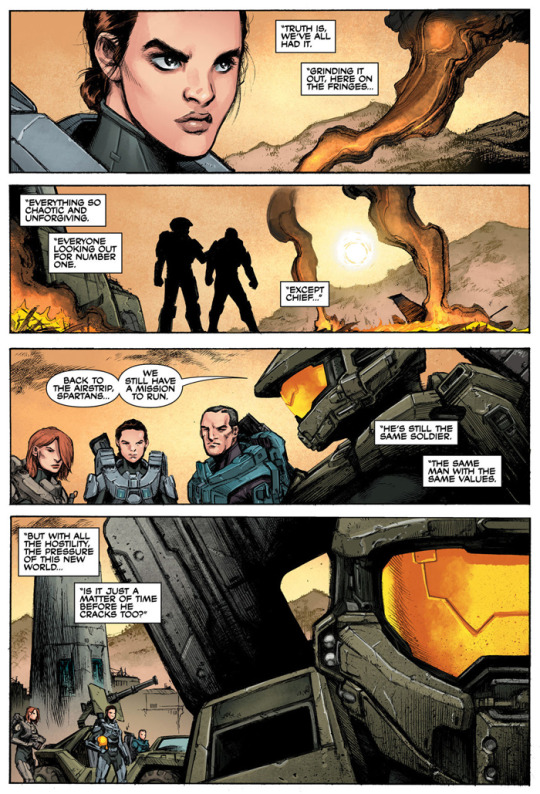
The end of this story presents us with quite the conundrum from Kelly’s point of view. Because while she will always support John and believe wholeheartedly in his ability to triumph over adversity, her final thoughts reveal that she does indeed recognize that for all the ways he’s remained stalwart he still has limits too. Just like the rest of them. Which once again works to emphasize how human these characters still are.
These pieces of media continue to paint the same picture of these characters that we have gotten for the last 15+ years: two people who have grown together over a lifetime of experiencing all manner of hardships and yet they maintain a healthy mutual relationship based in respect and honest care. How this may come into play later in the series after the events of ‘Halo 5: Guardians’ remains to be seen, but for now it is good to at least have a few more moments to add to John-117 and Kelly-087′s catalog of positive representation.
#Halo#Master Chief#John 117#Kelly 087#S2BlueTeam#Two Hundred And Four Reasons#opinion post#...about a month and a half late - but I got it done!
72 notes
·
View notes
Text
Picking up from where we left off...
John and Mycroft helped Mary fake her death. Sherlock wasn’t in on the plan.
John got hooked up to TD 12 to make him forget about the fake death--that’s why he was acting like Mary was truly dead in The Lying Detective.
Before John’s memory was erased though, he wrote a note to Sherlock and asked Molly to deliver it.

Whether by accident or design, something about John’s note gave away the fake death to Sherlock.
Sherlock Holmes needed his memory to be erased now, too.
Mary and Mycroft knew Sherlock wouldn’t be likely to agree to a memory wipe on his own, so they set their own plan in motion.


Mary left a video message for Sherlock encouraging him to engage in risky behavior in a bid to reconcile with John.
Mycroft and Mary then sought out Wiggins. The whole fake death plan was going down because they were trying to go up against bad guys known as the Scowrers (or that’s their name is in canon, they may well end up with a different one here). Wiggins used to be a Scowrer, and Mary knew it. So they were able to either convince or blackmail Wiggins into helping them out.
When Sherlock predictably went back on drugs as a way to mess himself up to the point of John not being able to resist helping, Wiggins was there to provide.
Remember Sherlock’s own words from His Last Vow, though: “Wiggins is an excellent chemist.”
See the “coffee” he’s pointing at? That’s an IV bag full of some brownish fluid.

Sherlock flashed to the same stuff briefly while he was throwing “Faith’s” gun into the Thames, because that moment reminded him of what he knew about the fake death. What the TD 12 had made him forget.
Wiggins mixed up some kind of drug cocktail with TD 12. Sherlock (knowingly) gets high and (unknowingly) gets his memory erased simultaneously, thinking it was his own idea the whole time.
(Another option for this is that the effects of TD 12 had proved too weak for Sherlock’s unusual mind, and Sherlock was instead upgraded to the stronger TD 13. In which case, that’s what the post-it on Mycroft’s fridge was referring to. But I’m going to keep calling it TD 12 until someone in the show acknowledges the existence of another version.)

The connection between the drugs and TD 12 was also foreshadowed when John checked Sherlock for signs he’d been using again by pulling up Sherlock’s right sleeve.

Sound familiar?

Eventually, Sherlock went so far off the deep end that Wiggins bolted from 221B.
Mycroft then brought a team of agents into the flat, claiming that he was trying to figure out “what drove Sherlock off the rails.”
The reality was Mycroft already knew exactly what had done it. But he did use the opportunity to feel out whether John had caught on yet.
Mycroft also had his agents “collect evidence,” which was really just an excuse to get the incriminating TD 12 / drug cocktail remains taken away.
Like it never even happened.
#sherlock#sherlock theories#bbc sherlock#sherlock holmes#wiggins#john watson#mary morstan#mycroft holmes#molly hooper#rosamund mary watson#culverton smith#td 12#scowrers#birdy edwards#the six thatchers#the lying detective#series 4#my life would be different if i hadn't noticed how bad mary is at bandaging sprains
399 notes
·
View notes
Text
New Post has been published on Payment-Providers.com
New Post has been published on https://payment-providers.com/primer-on-merchant-accounts-part-2-providers-isos-how-to-choose/
Primer on Merchant Accounts, Part 2: Providers, ISOs, How to Choose
The digital payments industry is notoriously confusing. This post is the final installment of a 2-part series on merchant accounts, which are required for all businesses that accept credit cards. “Part 1” described the purpose of such accounts.
I’ll address in this article merchant account providers and the role of independent sales organizations. I’ll also offer tips for selecting the best provider for your business.
All of this follows my 3-part “Credit Card Processing FAQs” series, in which I explained industry jargon, pricing models, and fees.
Card Brands
Recall from “Part 1” that “acquirer,” “merchant account provider,” “merchant acquirer,” and “acquiring bank” refer to the same thing: a financial institution that has been registered and approved by one or more of the card brands (Visa, Mastercard, Discover, American Express) to accept card payments on behalf of a merchant.
Cards brands govern the business of acquiring. Their role is enormous. Acquirers must comply with the brands’ rules and regulations. Thankfully, the brands compete to register and retain acquirers.
Card brands — American Express, Mastercard, Visa, and Discover — set rules and regulations for providers of merchant accounts.
The card brands charge licensing, application, and membership fees. Other merchant account roles of brands include:
Rules and regulations. The brands create, modify, and publish the rules for the acquiring industry.
Security. The industry depends on protecting sensitive card data and personal information. Many of the rules for acquirers concern security. Among other measures, acquirers, including their partners and subcontractors, must comply with PCI-DSS.
Technology. Card brands have created electronic systems that allow acquirers to receive, route, and secure payment transactions. This includes, for example, services that encrypt and securely store card data. Other services include fraud prevention, transaction routing, data storage, and business intelligence (data and analytics).
Compliance. The brands police their own acquiring networks, with frequent audits to ensure compliance with the rules. Offenders can lose their acquiring licenses, although it’s much more common for the card brand to levy a fine and help the acquirer become compliant. I’ve seen a card brand waive, usually temporarily, one or more of its rules for an acquirer. This typically occurs when an acquirer needs more time to implement a new procedure, such as PCI.
Third Parties
Understanding the merchant account needs of every type of business is a near-impossible task, even for the largest banks, who do not typically have specialized expertise. As a result, acquiring banks rely on third-party providers.
What follows are common third-parties.
Independent sales organization. An ISO is a company that markets acquiring services to merchants on behalf of an acquiring bank. An ISO is similar to an independent insurance agency. The ISO will tailor a range of payment-acceptance services for merchants and will receive a commission — usually a one-time fee or a percentage of the revenue generated — from the acquiring bank and payment processor. ISOs can sell the services of many different acquirers, picking and choosing the best fit for the merchant. Less reputable ISOs sell the services that offer the highest commissions or fees instead of the best option for the merchant. ISOs are typically experts in a particular industry. Some payment processors also operate as ISOs — the processor sells on behalf of an acquiring bank. Some ISOs call themselves acquirers.
Member service provider. MSP is Mastercard’s name for ISO.
Third-party agent. TPA is Visa’s name for ISO.
Value-added reseller. A VAR integrates the technology of third-parties into a single product or offer. An example is integrating payment gateways into point-of-sale equipment. VARs are not acquirers, but they may operate like ISOs or own ISO businesses.
Referral agents. Some acquirers and ISOs offer referral fees to agents, who can be ISOs but are usually unrelated to payment processing, such as accounting firms. Unlike ISOs, referral agents do not have to register with the card brands. Thus referral agents cannot call themselves acquirers or use Visa or Mastercard’s branding. They also cannot perform the functions of an acquirer.
Monitoring ISOs
The card brands have strict rules for ISOs. An ISO must register with each card brand and with each acquirer that it represents. ISOs pay sign-up and annual fees to the card brands, who audit ISOs annually for branding and other compliance rules.
The card brands have strict rules for ISOs.
The card brands hold acquirers responsible for the behavior of ISOs. If an ISO brings a fraudulent merchant into the payment network, the acquirer is responsible. If a merchant signed by an ISO incurs chargebacks, the acquirer refunds the issuer. If an ISO’s merchant accepts payments but does not fulfill orders, the acquirer remediates. Thus acquirers select, underwrite, audit, and monitor their ISOs carefully.
Merchant acquiring can be a risky business for the following reasons.
Chargebacks. A chargeback is a transaction reversal when a cardholder claims that he did not make a purchase. The issuing bank will return the cardholder’s money almost immediately and file a claim against the merchant’s acquirer.
According to the rules, the acquirer must first refund the issuer (which has already refunded the cardholder). Only after the refund occurs can the merchant and its acquirer dispute the process. Regardless, the acquirer will remove the funds from the merchant’s merchant account — no questions asked — plus a hefty chargeback fee. When a merchant is unable to refund chargebacks, the acquirer must cover the charges. In short, acquirers (not merchants) control merchant accounts.
Fund reversals. A fund reversal is a refund (or partial refund) granted to the customer by the merchant. Because the acquiring bank deposits funds in the merchant’s merchant account, often before the expiration of product warranties and guarantees, acquirers are exposed to the risk that a merchant will refuse to refund customers (resulting in chargebacks) or the risk that a merchant will go out of business before refunding its customers. In both cases, the acquirer is responsible for chargebacks if the merchant cannot perform.
Merchant solvency. Merchants that go out of business (i) cannot pay their merchant account fees, (ii) cannot cover chargebacks, and (iii) could fail to return an acquirer’s point-of-sale equipment.
Merchant fraud. Merchants that engage in fraud expose acquirers to (i) chargebacks, as explained above, (ii) fines and other penalties levied by the card brands, and (iii) reputational damage to the acquirer and the brands.
How Acquirers Make Money
The primary source of revenue for acquirers are merchant account fees, fines, and miscellaneous revenue from payment processors and other value-added providers. Acquirers do not receive interchange fees, which is revenue for the issuing banks.
Revenue from merchants includes fees for:
Registration,
Account setup, maintenance, and closure,
Support and service,
Currency conversion,
Chargebacks and chargeback disputes,
Audits,
PCI compliance,
Settlement, also known as batch or daily batch,
Monthly minimums.
Acquiring banks can generate additional revenue by partnering with processors to offer both merchant accounts and payment processing solutions. Some acquirers, usually the largest banks (e.g., Chase, Citi), have internal departments for acquiring, issuing, and processing.
Selecting a Merchant Account Provider
Merchant acquiring is highly competitive. Pricing and contractual terms differ among providers. Consider these tips to find the best provider for your business.
Know the details. Make sure the salesperson is disclosing all of the costs and restrictions, such as (i) all fees and penalties, (ii) the company’s policy for holds and reserves, (iii) when to transfer funds out of the merchant account, (iv) procedures if you’re not satisfied, (v) monthly minimum fees or other hidden fees, and (vi) the length of the contract and the early termination fees.
Understand your processing volume (daily, monthly, yearly) before negotiating. Knowing your transaction volume will help determine whether you need a dedicated merchant account or an aggregate account, such as Stripe, Square, PayPal. The type of account will dictate your payment processing fees as dedicated accounts allow less expensive interchange-plus pricing.
Understand your business’s risk profile. Take steps to reduce chargebacks. Acquirers don’t like risk. If you operate in a high-risk industry, help your acquirer understand how you plan to reduce its exposure. High-risk businesses can expect to pay higher fees or incur larger holds. Ask the acquirer if it can help avoid fraudulent payments.
Ask about discounts from potential acquirers if you use their payment processing services or their partners’ services.
Integration. Confirm that a potential acquirer can integrate with your business’s customer and accounting systems. Inquire as to the difficulty and the cost. Sometimes acquirers will absorb that cost.
Source link
0 notes
Text
Yahoo Hong Kong debuts the list of top pandemic-related keyword searches
Surgical masks top the list of pandemic-prevention supplies Yoga is the choice of physical & mental exercise for Hong Kongers Air Fryers & air purifiers are must-haves for home quarantine HKTVMALL gains big points for investing 200k into a mask factory Webinars takes the throne in key tools to keep learning at home Netflix & TVB streaming shows claim Top 3 in popular Home Entertainment The Dow Jones & Financial Secretary’s 10k cash handout are the working class’ most frequent searches
As the COVID-19 pandemic prevails, technology has become an essential part of life for health-conscious Hong Kongers, whose digital consumption behavior has seen a drastic change whether in searching for pandemic-prevention supplies, daily essentials or online learning tools. Large populations working from home also resulted in immense demand for streaming services and entertainment, opening up commercial opportunities for businesses big or small. Verizon Media has always prioritized COVID-19 prevention by offering a plethora of trusted online content for everyone to enjoy at home. As a media and search company that amplifies what matters to users most with trust and empathy, Verizon Media’s subsidiary brand Yahoo Hong Kong (www.yahoo.com.hk) has partnered with top-notch service providers to serve Hong Kongers’ needs. Yahoo Hong Kong has charted the list of top pandemic-related keyword searches to review the topics and entertainment that Hong Kongers are most concerned about.
Yahoo’s keyword search during COVID-19: Top-10 anti-pandemic supplies 1. Surgical masks 2. mask 3. toilet paper 4. bleach 5. hand sanitizer 6, two boxes, thanks 7. ethanol 8. rice 9. hand sanitizer formula 10. sanitizing cotton
Masks in short supply; overnight queues a common sight COVID-19 strikes panic in all of us. Hong Kongers who had experienced the painful lessons of SARS in 2003 were aware of the importance of wearing masks for health protection. Yet their single-use means consumption and demand are massive, urging citizens to spare no effort to queue overnight just to get a box of masks. Businesses are also sourcing masks from around the world and selling them on social media. As such the comment of "two boxes of masks, thanks" messages flooded the online world, crowning it second place in the list of popular pandemic-prevention supplies.
Toilet paper panic-buy due to rumours of depletion At the beginning of the COVID-19 outbreak, a rumour spread online about toilet paper manufacturers switching to producing masks, igniting a wave of panic-buys in the town. Toilet rolls, boxed tissues, kitchen paper, and even sanitary pads were wiped out. Subsequently, the supermarkets clarified that their supply is sufficient and limited purchases to stop panic buys. As such, “snapping up toilet paper” also became one of the top-10 pandemic-prevention search words.
Yahoo’s keyword search during COVID-19: Top 10 products and people for mental and physical well being
1. Yoga 2. Hiking trails 3. Elva Ni 4. Hiking shoes 5. Nintendo Switch Ring Fit 6. Fitness bike 7. Fitness equipment 8. Country Parks 9. Fitness Centres 10. Hiking Gear
Home exercises and yoga gain popularity Self-protection is important, but so is boosting our immune systems against the virus, thus giving birth to the trend of home exercises. Yoga can regulate the entire body, improve blood circulation, promote endocrine balance and release stress. It is easy to get started and can be easily practiced at home, making it the first choice of workout for Hong Kongers! Viewers can also live-stream a yoga or fitness session with KOLs to achieve results while saving big bucks. Yoga KOLs like Elva Ni, as such, have gained popularity.
Suns out and masks off: country parks and hiking trails become new stomping grounds The city is packed with people and has poor air circulation, making nature the next best thing for Hong Kongers to, literally, get a breather sans mask. Therefore, search words like “hiking trails”, “country parks”, “outlying islands” and “hiking gear” gained much traction. Taking to nature is, of course, a healthy option, but please keep the mask on if the trails are crowded.
Yahoo’s keyword search during COVID-19: Top 10 home appliances 1. Air Fryer 2. Air Purifier 3. Air Cleaner 4. Dehumidifier 5. 5G Mobile Phones 6. Washing Machine 7. PlayStation 5 8. Combination Ovens 9. Bread Maker 10. Ovens
Home-cooked meals go up, as does creativity in the kitchen Eating out is risky so Hong Kongers are inclined to stay home for meals, thus boosting the search for kitchen appliances and tools. Topping the list is the air fryer, which can achieve the same crispy results but with less oil – surely a treat for everyone in the family. Ovens and halogen ovens share the spotlight among couples who’re into making candle-lit dinners or parents wishing to surprise their kids with homemade cakes. After the pandemic, everyone's cooking skills will definitely improve a lot!
Home Appliances go head-to-head with one another & air purifiers claim top 3 Spring humidity is upon us, and dehumidifiers have long been the top-three in years prior; but due to COVID-19, air purifiers became the new winner. Aside from air purifiers for the home, wearable air purifiers are equally popular: this thumb-size device is easy to carry and blocks pollen and PM2.5 pollutants by generation ions. Yet the virus is ubiquitous: aside from air purifiers, we must still beware of personal hygiene, keep our hands clean and wear masks.
Yahoo’s keyword search during COVID-19: Top 10 online shopping platforms 1. HKTVMALL 2. Watsons 3. ParknShop 4. Bonjour 5. Wellcome 6. SaSa 7. Ztore 8. Aeon 9. Carousell 10. Yata
HKTVMALL gains brownie points for investing 200k to make masks In the beginning of month, HKTVMALL announced the establishment of its mask factory and expects to start selling month-end. Its company’s value climbed to 4.6 billion. Prior to the pandemic, HKTVMALL dispatched two teams to source masks around the world and materials for masks production around Southeast Asia. Its USD 200k investment to build a mask factory has sparked heated discussions online. As the leading online retailer, HKTVMALL has been the go-to for searching daily staples, bleach, rice, toilet paper; it even hired more delivery people when orders started piling up. There is no doubt that HKTVMALL is at first place in the most-searched online shopping platform.
Watsons sells masks online; mascot “WatsBag” rises to fame When Watsons sold masks at its brick and mortar shops, queues piled up at the door. Yet, high demand means lining up overnight may not always be met with success. Some citizens even started arguments with Watsons staff and fellow mask-seekers. As such, the pharmacy moved the reservation process online: at its peak, the system saw 1.49 million people queuing up. During the wait, mascot WatsBag (a green shopping bag) entertains those in the queue with comical expressions and dialogue that soon became inspiration to derivative work and Whatsapp stickers designed by creative netizens. Soon after, Watsons released WatsBag’s life story and other family members in a series of peripheral products for sale. Some WatsBag’s nicknames have also made it to Yahoo’s top-three searches.
ParknShop shines during Home Quarantine As the plague of COVID-19 drags on, the majority of the public remains indoors, but daily staples and foods still need to be replenished. And for that, Hong Kongers prefer heading to CK Hutchison Holdings’ ParknShop headed by tycoon Li Ka-shing. Many supermarkets’ online platforms are, too, grasping onto this business opportunity as they see overwhelming orders. While we enjoy the convenience of deliveries, we should also be thankful for the people who are braving the pandemic to bring these goods to our doorsteps.
Yahoo’s keyword search during COVID-19: Top 10 learning-at-home tools 1. Zoom 2. eClass 3. iPad 4. Kindle 5. pagamo 6. Phonics 7. eLearning 8. happypama 9. TEDEd 10. Lego Steam
Learning Online is Packed with Fun Though schools are under suspension, learning never stops but has instead shifted to online education. Online conference platforms feature screen-sharing functions so lecturers can share learning materials while teaching, offering a much more engaging experience than rote learning. Conferences are two-ways, and incidents of students accidently leaving on the microphone have caused a raucous. Zoom – a platform more common among students – topped the list of 10 most popular searches in the “learning at home” category.
Learn at home with the help of Technology For parents, school suspensions and executing classes at home are big headaches. Fortunately, a number of schools are using the eClass learning platform to share electronic learning materials. Students need only log into the eClass system to access their assignments so as to learn at their own pace and time at home even under class-suspension. As such, PaGamO, Happy PAMA, and other target-oriented, online self-learning platforms stand out from the crowd and made it to the Top 10 most popular searches in the “learning at home” category.
Yahoo’s keyword search during COVID-19: Top 10 home entertainments 1. Crash Landing on You 2. Joy of Life 3. Forensic Heroes IV 4. Three Lives, Three Worlds, The Pillow Book 5. Itaewon Class 6. The Dripping Sauce 7. Kingdom 8. Someday Or One Day 9. Parasite 10. Running Man
When it comes to binge-watching at home, Korean dramas are the go-to Until a cure is available for COVID-19, medical staff highly recommend the public to stay home, and the best way to kill time? Binge-watching shows. “Crash Landing on You” by Netflix tells of a girl from an upper-class family and her adventures in North Korea after she accidentally paraglided into the country. During her stay, she falls in love with the captain of the North Korean Special Forces in a romantic tale that has mesmerized the young generation, making it the most-searched show. Second and third places are TVB’s primetime shows, “Joy of Life” and “Forensic Heroes IV”. The binge-worthy “Joy of Life”, produced in Mainland China, illustrates a mysterious, good-looking man who makes a legend out of himself. “Forensic Heroes IV”, on the other hand, is the brainchild of esteemed producer Mui Siu-Ching and has reached new heights in viewership of 40-plus points.
Yahoo’s keyword search during COVID-19: Top 10 finance-related keywords 1. Dow Jones Industrial Average 2. Financial Secretary Budget 3. 10k cash handout 4. RMB exchange rate 5. Yen to HKD 6. Anti-epidemic Fund 7. Australian Dollar 8. Hong Kong Dollar Fixed Deposit 9. Community Care Fund 10. Pounds to HKD
US Stock market plummets, worst performance in 30 years No country is free from the wrath of COVID-19. As situations worsen in the United States, businesses and corporations have been forced to come to a halt. Three major stock indexes plummeted, of which the Dow recorded the largest quarterly decline since 1987, hovering at 15293 points, making this the headline search item.
Financial Secretary’s 10K cash handout encourage spending Financial Secretary Paul Chan Mo-Po announced in February the 2020-21 Budget composed of a number of bailout features, of which the 10k cash handout to all Hong Kong permanent citizens aged 18 or above has received the most attention. This scheme is believed to benefit more than 7 million Hong Kongers both living in the city and overseas. In such economic turmoil, the cash handout will surely lessen citizens’ financial pressure and encourage spending. Hong Kongers can apply for the 10K cash hand out scheme in July via online and paper forms and receive the money as early as August.
Co-head of APAC, Verizon Media Mr. Rico Chan says, “As a trusted media partner of Hong Kongers, Yahoo has been walking alongside people of this city for the past 20 years. Under the plague of COVID-19 and daily surges of news and updates on the pandemic, we are on an information overload. Yahoo Hong Kong continues to stand with Hong Kong with a Combating COVID-19 live log and website featuring unbiased, accurate and real-time information. Aside from trusted sources of information, Yahoo Hong Kong also lends a helping hand during these challenging times to source masks and sanitizing supplies from around the world and making them available to our members via the Yahoo App. In lieu of school closure, we also launch an all-new online learning hub (Yahoo Kids Up) that amalgamates reputable self-learning channels to offer students at home premium content and support within the confines of their homes. With faith, Yahoo will stand strong with Hong Kongers to overcome this pandemic.”
0 notes
Text
A Future Without HIV: Are We There Yet?
Jennifer Waugh
The findings of a major eight-year-long HIV study known as the PARTNER2 study have shown that so long as HIV+ partners are being fully treated, there is no chance of passing on HIV to a sexual partner, even with unprotected sex. What does that mean, and where do we stand now that we know this?
Last weekend was huge for HIV research. Literally epic.
The Guardian, CNN and other major news sources reported on the findings of a major eight-year-long HIV study known as the PARTNER2 study. This landmark study followed 1000 male couples where one partner was HIV positive and on antiretroviral (ARV) medication, and one partner was negative for the disease, across fourteen different countries in the United Kingdom.
The study findings showed that when men were adherent to their ARVs (when they took their meds daily and as directed), they became virally suppressed, and had no chance of passing on HIV to their sexual partner, even with unprotected sex. These couples reported engaging in unprotected sex more than 77,000 times collectively without any transmission of the virus.
You heard that right: so long as the HIV+ partners were being fully treated, it was found that there was no chance - zero — of passing on HIV to their sexual partner, even with unprotected sex.
The findings of this study were published in 2018, but the CDC recognized the fact that undetectable viral loads lead to zero HIV transmission in 2017, showing support of the Prevention Access Campaign’s “Undetectable = Untransmittable,” or “U=U." More than eight hundred organizations across one hundred countries have now joined together in support of the U=U campaign. HIV/AIDS has claimed the lives of millions since it was first discovered in 1983, but it seems things may finally be looking up.
This is obviously amazing news. This is also a lot to unpack, though, so let’s talk basics, filling in gaps you might have about HIV or AIDS, treatment, and their history, then let's take a look at the view from here.
What are HIV and AIDS, anyway?
HIV (Human Immunodeficiency Virus) is a disease that attacks the immune system, and which makes anyone who has it more susceptible to other infections that can then cause AIDS (Acquired Immune Deficiency Syndrome). A person living with HIV is considered to have AIDS when their CD4 count — the amount of white blood cells in the body — drops below 200 (the normal range is 500-1,500), and they have been diagnosed with what's called an opportunistic infection. Some of the most common opportunistic infections are recurrent pneumonia, toxoplasmosis, hepatitis B and C, and candidiasis (yeast infections or thrush) - though there are many. Basically, because HIV attacks the immune system, which makes it easier to fall seriously ill by another serious infection, and greatly inhibits the body’s ability to fight back. Good CD4 cells are destroyed, and HIV begins creating new copies of the virus.
One big misconception that still exists, thanks in part to stigma and lack of accurate education, is that HIV = AIDS, or even that HIV always leads to AIDS. That’s not true. With advances in research and treatment options, many people with HIV in developed nations now never experience AIDS.
HIV was initially found in 1981 and first called GRID -- Gay-Related Immunodeficiency -- because it was first seen in gay men. This framing unfortunately perpetuated stigma (negative, oftentimes shameful, perception) that still surrounds both gay men and HIV to this day. HIV isn’t just about gay men. It can be transmitted (passed from one person to another) through bodily fluids including blood, semen, vaginal fluids, and breastmilk. Though the virus passes most easily during anal sex (due to the ease with which anal tissue tears, making the act more “risky” for the receptive, or bottom, partner) HIV does not discriminate based on sexuality, gender, or skin color. Contrary to historical stereotypes, statistics show that globally heterosexual women are who experience the highest rates of HIV infection.
In the 1980s and 1990s when treatments were not yet readily available or affordable, hundreds of thousands of gay men had died from AIDS, largely due to homophobia. In the USA alone, "By 1995, one gay man in nine had been diagnosed with AIDS, one in fifteen had died, and 10% of the 1,600,000 men aged 25-44 who identified as gay had died." Gay men have accounted for more than half (55 percent) of all AIDS deaths since the epidemic’s beginning.
Sensationalized news articles and headlines across the world played a great part in this by demonizing gay men, using terms like “gay plague,” “gay cancer,” and displayed images of tombstones and the Grim Reaper. Heartlessly, HIV and AIDS were viewed by many as a punishment for what they or others considered “amoral behavior,” like sex between men, IV drug use, or sex work. This, combined with existing intense bias against these groups, led to a mass amount of fear, and tremendous silence surrounding the disease. At the height of the AIDS epidemic in the US and beyond, gay men led activist movements criticizing the government’s blind eye and lack of action at such a crucial time, fighting for the Reagan administration to pay attention and to fund research and treatment. It wasn’t until 1986 that President Reagan even mentioned the word AIDS publicly. During this time, HIV was still considered by many to be a death sentence, as affected populations continued to be further marginalized.
Ian Green, Chief Executive of Terrence Higgins Trust, a British charity that provides services relating to sexual health and HIV, was diagnosed with HIV 23 years ago. In a recent interview, Ian, now undetectable, disclosed fears he had when he was diagnosed that many still have today when they test positive for HIV. “The most significant [emotion] at that point in time was how long did I have to live. The other thing that really concerned me for a very long time is am I a risk to other people?” I can only imagine the immense relief that might now be felt by a person living with HIV to learn they are unable to pass it on to anyone else – to not feel as though they are any sort of danger to other people, so contrary to perceptions and experiences of the past.
In the United States, specifically, the population most affected by HIV is still men who have sex with men, accounting for 26,000 new infections each year. Worldwide, though, women represent the majority — 52% — of all adults living with HIV. Though we know anal sex poses the greatest risk of transmission, penis-vaginal intercourse is also a leading cause of transmission worldwide. Similar to the anus, it's easy for the vaginal wall to experience small (usually unnoticeable) tears during intercourse, providing a route for HIV transmission. Vaginal tissue is highly susceptible to any type of infection. Beyond basic physiology, women (including those who don't have vaginas) also remain disproportionately affected by the virus due to vulnerabilities created by social, economic, and cultural status. Gender inequality, as well as intimate partner violence, reinforce harmful power dynamics, both on a personal and systemic scale. In many countries, women face significant barriers to education and healthcare, contributing to a known lack of understanding around pregnancy and HIV.
What about treatment?
HIV treatment medications (ARVs) became available in the late 1980s, starting with the first licensed drug, AZT (of the drug class Nucleoside Analogs), which was initially highly toxic.
Fast forward to the 1990s and a new era of ARVs. Researchers began to realize that one class of drugs was not enough to control CD4 counts, and eventually introduced HAARTs – highly active antiretroviral therapies – made up of combinations of Nucleotide Reverse Transcriptase Inhibitors (NRTIs), Non-nucleoside Reverse Transcriptase Inhibitors (NNRTIs), Protease Inhibitors, Fusion Inhibitors, CCR5 Antagonists, and Integrase Inhibitors. Not only were these treatments (called “cocktails” in early years) numerous - sometimes 20 or more pills a day - but many doctors refused to even treat people living with HIV. Then there’s the fact that even seeing a doctor and paying for these incredibly costly meds meant having health insurance (something many, many people didn’t have), and a plan that would potentially pay thousands upon thousands monthly for treatment.
Through years of advocacy and research, ARVs became more effective in treating the virus, and HIV resource agencies began growing around the world, making it easier for more people to access these medications. Drug trials continued, and researchers found the right combination of these different classes of drugs.
Today, people living with HIV who are connected to treatment can now take as little as one single pill per day as their full treatment. (That one pill contains at least three types of medications, though.) By finding these effective combinations, remaining adherent to one’s ARVs has become much easier than not only remembering to take, but having to swallow, handfuls of pills per day.
This brings us back to the results of the PARTNER2 study and what life looks like for people who receive HIV treatment today.
UNAIDS data from 2018 reported that 21.7 million of the 36.9 million people living with HIV worldwide were receiving treatment in 2017. Their current initiative and goal is 90/90/90: that 90% of people living with HIV will know their status, 90% of those people will be on treatment, and 90% will be virally suppressed. Adherence to treatment is key to suppression of the virus.
Current standards of treatment include taking daily medication and having lab work done every six months prior to checking up with a healthcare provider. Today there are many ARV medications, and doctors choose the best regimen for each individual patient. Typically, after a few months of taking medication (and depending on how long they have been living with the disease untreated), people diagnosed with HIV will have such a small amount of copies of HIV in their blood that they are considered “undetectable.” People achieve viral suppression (a controlled, lowered amount of the virus) when the copies of HIV are less than 200 per milliliter (mL) of blood. This doesn’t mean that a person with an undetectable viral load will test negative for HIV, but during routine labs (which check the CD4 – the level of good white blood cells, and the amount of HIV copies in the blood) their amount is so small that it will not show up on that particular test.
It’s important to note that just because a person achieves undetectable status does not mean they can stop taking medication. If a person begins missing more than 3-4 doses of their ARV per month regularly, their viral load can climb to a detectable value, and they may need to switch medications to get that number back under control.
So, what does this news mean for everyone?
Obviously, the fact that HIV treatment has now been proven to prevent transmission when taken properly is incredible news, and is potentially momentous both for people living with HIV and those of us who have worked or are currently working to prevent it. Researchers have been working hard for decades on the science behind HIV and developing and administering effective treatment.
But what about the people who don’t have access to these medications? In developing nations, poor economy contributes to a lack of healthcare, and the availability of medication to fight HIV. UNAIDS estimates that more than $26.2 billion will be required to combat HIV/AIDS in the year 2020. Treatment is expensive.
Stigma plays — as it always has — another huge role in the ability to receive treatment. Even just being tested for HIV is scary because of fear of judgment and discrimination. In terms of HIV, however, ignorance is not bliss. It is crucial to know one’s status so that treatment can be initiated, and more people will not come in contact with the virus. 73 countries worldwide still consider homosexuality to be a prosecutable offense, sometimes punishable by death: these attitudes and policies obviously keep many people from even getting tested. A key proponent to HIV prevention is education and counseling, but for many, the idea still exists that HIV = gay, and it can be dangerous to discuss either.
There are many other barriers that exist that prevent people from receiving HIV treatment. People of color and those who are low-income are incredibly underserved. Many people do not have access to health insurance or appropriate healthcare. ARVs cost upwards of $3,000 per month without insurance. Even with insurance, lack of education often leads to the inability to understand a diagnosis and other parts of health, and makes it difficult for many marginalized people to communicate their needs with a doctor. What about transportation? Just getting to a doctor’s office or pharmacy is often a task on its own, especially in rural areas or healthcare deserts (areas with no clinics or hospitals). Additionally, housing and food security play their own roles in creating barriers to optimal HIV health. Without a safe place to live, many people lack a safe place to store their medications even if they can get them. Most ARVs need to be taken with food to be absorbed properly: not knowing where your next meal will come from adds another layer to the struggle with adherence.
Luckily, there are many HIV resource agencies to assist people with some of these barriers and help to make access to HIV healthcare easier. In the United States, the AIDS Drug Assistance Program (ADAP - though the name varies by state; for example, this resource is called MIDAP in Michigan) provides free HIV healthcare and HIV medications for people enrolled in the program. This organization even covers undocumented citizens. HIV resource agencies often provide testing, education, counseling, and HIV health management services (including social work, and food, housing, and insurance assistance) for people who are lucky enough to have an organization in their area.
There are also other recent HIV advancements to be excited about. Pre-Exposure Prophylaxis (PrEP) was initially approved by the FDA as a preventative medication from MeetPositives SM Feed 4 http://bit.ly/30bb2qr via IFTTT
0 notes
Text
8 Benefits of Voluntary Mental Health Admission
When a mental health condition has deteriorated to the point of a severe psychiatric break, hospitalization is the appropriate level of care. When a loved one is in the midst of a psychiatric event or crisis it is presents difficult choices. Will your loved one voluntarily agree to be admitted to the hospital or is an involuntary admission necessary?
Understanding the options available and the differences between an involuntary and voluntary mental health admission can help smooth the way toward your loved one’s healing.
What Constitutes a Mental Health Crisis?
When living with a mental health disorder each day can present unpredictable developments. While one day the individual is feeling stable and optimistic, the following day might find them contemplating suicide. Mental illness is complex and does not progress in a straight line. Even the most closely monitored disorders can suddenly take an extreme turn for the worse.
Signs that a mental illness has become a psychiatric crisis revolve around impaired functioning and being a danger to oneself or others. When the individual’s symptoms appear to have deteriorated, the following signs would constitute grounds for hospitalization:
Becoming incommunicative, catatonic
Extreme mood swings
Cognitive impairment
Unable to function at even basic daily tasks
Aggressive or violent behaviors
Impulsive risky behaviors that endangers the individual or others
Psychotic symptoms, such as paranoia, hallucinations, or delusions
Neglecting personal hygiene
Not eating or sleeping normally
Threatening suicide
When some of these signs are present it is important to discuss a voluntary mental health admission with the individual.
Different Types of Mental Health Treatment Centers
Covering a wide spectrum of mental health disorders at varying levels of care, mental health programs come in a variety of formats. These include:
Outpatient private practice providers
Outpatient mental health treatment centers or day programs
Residential mental health centers
Dual diagnosis treatment programs
Psychiatric hospitals
The psychiatric hospital provides the highest level of care, with acute stabilization services, 24-hour monitoring, medical care, and intensive psychiatric treatment. These facilities may be a state psychiatric hospital, a private psychiatric hospital, or a general hospital with a designated psychiatric floor.
8 Benefits of Voluntary Mental Health Admission
When approaching a loved one about voluntarily admitting to a mental health center for more focused care you may be met with resistance. This is understandable, as no one likes the idea of needing this level of care for a mental health disorder. But it is helpful to convince them that by entering a program voluntarily there are several benefits, versus involuntary admission. These benefits include:
Self-admitting into a psychiatric hospital or residential mental health program with acute stabilization services is the most efficient option for getting the necessary psychiatric help quickly.
There is reduced stigma attached to a voluntary hospitalization versus an involuntary admission.
It gives the patient a feeling of control over their desire and need for treatment, versus being taken against their will.
It allows the patient to voluntarily leave the facility.
The individual will feel a sense of ownership about their treatment, leading to higher levels of involvement in the treatment interventions and activities.
Patients who enter treatment voluntarily are more inclined to experience improvement than those admitted involuntarily.
Voluntary admissions are often shorter than involuntary admissions, often because the patient is engaged in his or her treatment and more cooperative.
The relationship between the patient and the doctors assigned to them is less adversarial with voluntary admissions.
What to Expect in a Psychiatric Hospitalization
Someone who is admitted into a psychiatric hospital, either voluntarily or involuntarily, will likely require acute stabilization. This involves continual monitoring, medication analysis, adjustment, and prescription of psychotropic drugs, IV fluids, and the initial evaluation and preliminary diagnosis of the admitting psychiatrist. Patient medical history and psychiatric history will be reviewed, as well as current symptoms. Until stabilized the patient will remain in a secured area of the hospital.
Ongoing treatment during the hospital stay will involve an integrated approach using evidence-based therapies, medication, and adjunctive therapies. Holistic therapies may also be included in the treatment program, as these are conducive to stress management and relaxation.
Individual and group therapy sessions will be provided daily. These enable the patient to work through underlying psychological issues that may be contributing to the enhanced psychiatric break. In addition to examining past traumas or other painful events in their life, the patient will also likely have to process feelings of shame or guilt related to their mental condition. Many patients feel as if they are a burden to loved ones and fear abandonment or rejection.
Once the patient has achieved a stabilized status they may request to leave the hospital setting and step down to either a residential or outpatient mental health program. Only patients who are admitted voluntarily can make such requests.
Stepping Down After Psychiatric Hospital Stay
When it is appropriate for the individual to leave the hospital setting and transition to either residential or outpatient care, they will experience more freedom and autonomy. A residential program will likely offer many of the same treatment elements, but may have a more relaxed setting compared to the hospital. A residential stay can be as short as a couple of weeks up to several months, depending on the unique mental health needs of the patient.
Outpatient programs are available once the individual is ready to return either home or to reside in transitional living for a period of time. The outpatient program can be minimal, such as one or two therapy sessions per week, to more intensive such as a day program.
The Treatment Specialist is An Online Resource For Mental Health Information
The Treatment Specialist offers help for individuals or loved ones experiencing psychological distress. Our trained specialists provide free information about the mental health disorder and can guide individuals toward appropriate treatment options for the specific disorder or dual diagnosis. If you need more information about a voluntary mental health admission, please connect with The Treatment Specialist today at (866) 644-7911 for a free confidential assessment.
The post 8 Benefits of Voluntary Mental Health Admission appeared first on The Treatment Specialist.
8 Benefits of Voluntary Mental Health Admission published first on https://familycookwareshop.tumblr.com/
0 notes
Text
Financial Misconduct in Utah Divorce Cases
What is financial misconduct? In Utah, it is a basis upon which an Utah divorce court can make a distributive award.
Consider this:
If a spouse has engaged in financial misconduct, including, but not limited to, the dissipation, destruction, concealment, nondisclosure, or fraudulent disposition of assets, the court may compensate the offended spouse with a distributive award or with a greater award of marital property.
So what does this mean in plain English? It means if you are getting divorced and your spouse is destroying, ruining, hiding, or getting rid of assets in a sneaky way, the court can give you some of their separate property to punish them. When a court does this, it is called a distributive award.
youtube
So what is separate property?
(a) “Separate property” means all real and personal property and any interest in real or personal property that is found by the court to be any of the following:
(i) An inheritance by one spouse by bequest, devise, or descent during the course of the marriage;
(ii) Any real or personal property or interest in real or personal property that was acquired by one spouse prior to the date of the marriage;
(iii) Passive income and appreciation acquired from separate property by one spouse during the marriage;
(iv) Any real or personal property or interest in real or personal property acquired by one spouse after a decree of legal separation issued under section 3105.17 of the Revised Code;
(v) Any real or personal property or interest in real or personal property that is excluded by a valid antenuptial agreement;
youtube
(vi) Compensation to a spouse for the spouse’s personal injury, except for loss of marital earnings and compensation for expenses paid from marital assets;
(vii) Any gift of any real or personal property or of an interest in real or personal property that is made after the date of the marriage and that is proven by clear and convincing evidence to have been given to only one spouse.
So what does this all mean? It means if your spouse has separate property, and they are playing games with the marital property, the court can remedy this by giving you some of their separate property.
Retroactive Arrearage Modification Not Prohibited
The Supreme Court has decided that parties to a support order may modify child support by agreement. In Byrd v. Knuckles the Supreme Court held that nothing prohibits a juvenile court from adjusting an existing arrearage in child support if the parties agree to do so.
In this case, as part of an agreement to consent to a step-parent adoption, the Mother agreed that the Father’s child support arrearage would be reduced by 50%. After the adoption was completed, the Father attempted to have his child support arrearage reduced pursuant to this agreement, and the Court found that it had no authority to reduce this arrearage under the Law. This matter was appealed, and then brought before Supreme Court.
The Supreme Court noted that this decision does not mean that a court MUST accept a parties’ agreement to reduce a prior arrearage, but that a court is not prohibited from doing so pursuant to the Law. As in this case, this issue is particularly relevant where one party is willing to sign away their legal rights in order to be released from future, and possibly past child support obligations.
Free Consultation with a Utah Divorce Lawyer
If you have a question about divorce law or if you need to start or defend against a divorce case in Utah call Ascent Law at (801) 676-5506. We will help you.
Ascent Law LLC8833 S. Redwood Road, Suite CWest Jordan, Utah 84088 United StatesTelephone: (801) 676-5506
Ascent Law LLC
4.9 stars – based on 67 reviews
Recent Posts
Change of Circumstances and Grandparent Custody
Child Sexual Abuse Investigation
Contracts and the Roles They Play in Business
How to get 50 50 Custody
Fundamental Documents in a Divorce Case
How to form an S corporation
From http://www.ascentlawfirm.com/financial-misconduct-in-utah-divorce-cases/
from https://familylawattorneyut.wordpress.com/2018/03/18/financial-misconduct-in-utah-divorce-cases/
0 notes
Text
Harm Reduction for IV Drug Users: Clean Syringe Availability for Addicts Controversy
There is no argument that the best way to prevent the spread of HIV and other bloodborne illnesses is to refrain from engaging in risky behavior. One of the fastest ways that HIV spreads is through illegal IV drug use. The financial and social repercussions of IV drug use (most commonly heroin, cocaine, and diverted forms of pharmaceuticals) are severe enough; add the existence of a chronic, painful, fatal illness and the problem compounds tenfold.
youtube
The Idea is Terrifying
For many addicts, just the idea of not using for one day or even a few hours is terrifying – worse than death itself. Those who oppose clean syringe availability have argued that addicts are aware of the consequences, and are only hurting themselves, killing themselves quicker. Opponents have also expressed concerns that accessibility of syringes might increase IV drug use, reasoning that those who were once deterred by fear of disease could be lured into the next level of drug abuse by the safer alternatives.
But what are the real repercussions when an addict contracts HIV? Have new laws allowing addicts to buy syringes over the counter or through exchange programs increased drug use by frequency or population?
Chronic Illnesses
Any IV drug user who contracts HIV, or any other chronic illness via blood such as Hepatitis C, will eventually need medical care. It does not matter if the person is still using or has been sober for ten years, has Medicaid or the best private pay insurance (or none at all) – the expense of this medical care will be astronomical. This expense is absorbed not only by the individual, but the government, insurance companies, and sometimes private charities; in short, by everyone in the community both locally and nationally no matter where you live.
In addition to the financial aspect, the physical and social burden that the disease itself puts on the patient and those around him or her is extreme. Even setting aside the actual physical pain, there is lost work and productivity, other healthy family members are burdened by caretaking, and there may be infected offspring. One serious illness causes a ripple effect not only into the immediate family but co-workers, friends, healthcare workers, and other community members. The duration of the acute stages of illnesses such as AIDS and cirrhosis caused by Hepatitis is also important to consider – patients do not fall ill and die within weeks or months, but years, and often the treatment is as debilitating as the illness itself.
Since many areas began passing laws to increase the accessibility of syringes beyond those with a diabetic prescription, there is no longer a basis for any founded fears of increased drug use. Leniency still varies from state to state in the US, mostly depending on political climate, yet nearly all have loosened restrictions in some form or another.
Making and keeping new, clean syringes available to the IV drug using population may not seem like a step in the right direction, but perhaps we should ask ourselves this: is our true goal not a happier, healthier world? If so, then let’s begin with keeping people as safe as they can be under their present circumstances. We can only fix one thing at a time.
The post Harm Reduction for IV Drug Users: Clean Syringe Availability for Addicts Controversy appeared first on Alcohol and Drug Addiction.
from Alcohol and Drug Addiction http://www.spiashop.com/harm-reduction-iv-drug-users-clean-syringe-availability-addicts-controversy/
0 notes
Text
A GOP Health Care Plan May Ruin Our Best Chance At Ending HIV And AIDS
Before the pharmacist retrieves my prescription, she leans in and whispers: “Just so you know, it’s $1,300.” This happens almost every time, so I already have at the ready my coupon card from the drug’s manufacturer.
Each month, the card provides me with $6,000 in co-pays, or about four months worth of medicine, but now I’ve run out. I’m only on the hook for $80, after which I’ll hit my $7,150 health insurance deductible for the year. Then, until January, each monthly prescription will be free for me. I swipe my credit card.
Between the manufacturer-provided discounts and my private health insurance, I can afford Truvada, which blocks HIV transmission, and, most likely, I’ll be able to continue my regimen even if the Affordable Care Act is repealed. But, that won’t be the case for thousands of other at-risk people who could potentially lose coverage, meaning we may miss the best chance we’ve ever had to end the AIDS epidemic.
“Universally available PrEP and treatment could end the HIV epidemic,” said Dr. Robert Grant, an AIDS clinician and researcher at the University of California, San Francisco. However, the implementation still needs some work.
In 2012, when the Food and Drug Administration approved Truvada for the prevention of HIV, a treatment also called pre-exposure prophylaxis (PrEP), it seemed like a watershed moment. The pill is taken once a day, has comparatively mild side effects, requires only routine blood tests, and is up to 99 percent effective. Public health officials in major U.S. cities, such as New York and San Francisco, embraced Truvada, which is more effective than condoms and also an option for IV drug users, who now account for 10 percent of all new HIV infections.
The major barrier then — and now — is the $1,300-a-month price tag.
Currently, only 125,000 people are on PrEP in the United States, the majority of whom are white men living in cities — a troubling disparity considering that, during the past decade, overall HIV infection rates have fallen by 20 percent but risen, during this same period, by almost a quarter for black and Latino men who have sex with men, populations that are also disproportionately uninsured and on Medicaid. Likewise, because of a combination of stigma and inaccessibility, rural communities are also lagging behind.
Though small in absolute terms, the number of PrEP users has grown more than 13 percent since the end of 2016, thanks in part to new advertising campaigns from the drug’s manufacturer, Gilead.
Moreover, the benefits extend beyond greater protection from HIV. Truvada is “a wonderful gateway drug to primary care,” according to Grant.
When someone comes in for an HIV test, Cody Shafer, the PrEP coordinator for Iowa’s Department of Public Health, directs him to a patient navigator who specializes in ACA enrollment and assists him during the 20-minute wait for results. Shafer says it’s the first time that many of his patients have had insurance, which allows them to access a host of preventive services, such as programs to quit smoking, treat substance abuse and combat diabetes risks.
What’s more, to maintain their PrEP prescriptions, each recipient must get tested for HIV every three months, four times as frequently as other men who have sex with men, according to Grant’s experience as a clinician and data from the Centers for Disease Control and Prevention. This infrequent testing helps explain why 1 in 8 HIV-positive people in the U.S. is unaware of their status.
But, these secondary benefits may soon disappear.
Though it’s unclear how (or if) the ACA will be repealed, the plan passed by the House last week would certainly lead to fewer insured Americans and, by extension, fewer patients able to afford PrEP. Gilead offers that $6,000 co-pay discount to patients with insurance and a full subsidy to those without, but that assistance will be insufficient.
“To qualify for those programs, you need to have a motivated physician who’s willing to fill out the forms. If you don’t have insurance, you won’t have a physician,” Grant said.
And, Gilead also doesn’t cover lab fees, which, for my latest visit, would have cost me $615.81.
The dangerous practice some users engage in
When patients are unable to access Truvada through official channels, they find other means. Shafer told me he’s already seen men in Iowa who drop down to four doses a week to conserve pills, HIV-positive patients who ask for early refills to share or sell, and PrEP users who continue to fill prescriptions even after they’ve stopped engaging in risky behavior.
“They want to have extra on hand to help out friends and partners who lose coverage,” he said.
Considering the drug’s effectiveness and ease of use, it’s understandable that patients will choose to have some protection over none. However, the greatest risk of PrEP is contracting HIV and then taking Truvada, which is also used to treat the disease, and that potentially leading to mutations that make patients resistant to an entire class of antiretrovirals.
To make matters worse, HIV can lie dormant and asymptomatic in the body for years, and at-home tests can miss an infection as far back as a month. Newly infected patients are the most contagious vectors, and without any symptoms to slow them down, they can spread the disease with astonishing quickness. (Some of the first men to die of AIDS reported more than 2,500 lifetime partners.)
A missed opportunity
Republicans’ health care reform proposal comes at a precipitous time for the AIDS epidemic. Current treatments are effective enough that HIV becomes nearly undetectable in the blood, but antiretrovirals don’t come cheaply. The CDC estimates that the lifetime cost of treatment is $379,000, and allowing insurers to discriminate based on pre-existing conditions would, of course, be catastrophic for HIV-positive patients, 30 percent of whom are already uninsured.
Echoing Shafer, Dr. Michael Ohl, an infectious disease specialist at the University of Iowa, says that these patients may sell their Truvada to make ends meet, which will raise their viral load — and their chances of transmission.
By all accounts, I’m fortunate: for being young, healthy and without any pre-existing conditions and for being well-equipped to navigate bureaucracies, able to afford health insurance, and now in a monogamous relationship. If the ACA is repealed, however, others won’t be so lucky, which could jeopardize the last three decades of progress in combating the epidemic.
-- This feed and its contents are the property of The Huffington Post, and use is subject to our terms. It may be used for personal consumption, but may not be distributed on a website.
A GOP Health Care Plan May Ruin Our Best Chance At Ending HIV And AIDS published first on http://ift.tt/2lnpciY
0 notes
Text
A GOP Health Care Plan May Ruin Our Best Chance At Ending HIV And AIDS
Before the pharmacist retrieves my prescription, she leans in and whispers: “Just so you know, it’s $1,300.” This happens almost every time, so I already have at the ready my coupon card from the drug’s manufacturer.
Each month, the card provides me with $6,000 in co-pays, or about four months worth of medicine, but now I’ve run out. I’m only on the hook for $80, after which I’ll hit my $7,150 health insurance deductible for the year. Then, until January, each monthly prescription will be free for me. I swipe my credit card.
Between the manufacturer-provided discounts and my private health insurance, I can afford Truvada, which blocks HIV transmission, and, most likely, I’ll be able to continue my regimen even if the Affordable Care Act is repealed. But, that won’t be the case for thousands of other at-risk people who could potentially lose coverage, meaning we may miss the best chance we’ve ever had to end the AIDS epidemic.
“Universally available PrEP and treatment could end the HIV epidemic,” said Dr. Robert Grant, an AIDS clinician and researcher at the University of California, San Francisco. However, the implementation still needs some work.
In 2012, when the Food and Drug Administration approved Truvada for the prevention of HIV, a treatment also called pre-exposure prophylaxis (PrEP), it seemed like a watershed moment. The pill is taken once a day, has comparatively mild side effects, requires only routine blood tests, and is up to 99 percent effective. Public health officials in major U.S. cities, such as New York and San Francisco, embraced Truvada, which is more effective than condoms and also an option for IV drug users, who now account for 10 percent of all new HIV infections.
The major barrier then — and now — is the $1,300-a-month price tag.
Currently, only 125,000 people are on PrEP in the United States, the majority of whom are white men living in cities — a troubling disparity considering that, during the past decade, overall HIV infection rates have fallen by 20 percent but risen, during this same period, by almost a quarter for black and Latino men who have sex with men, populations that are also disproportionately uninsured and on Medicaid. Likewise, because of a combination of stigma and inaccessibility, rural communities are also lagging behind.
Though small in absolute terms, the number of PrEP users has grown more than 13 percent since the end of 2016, thanks in part to new advertising campaigns from the drug’s manufacturer, Gilead.
Moreover, the benefits extend beyond greater protection from HIV. Truvada is “a wonderful gateway drug to primary care,” according to Grant.
When someone comes in for an HIV test, Cody Shafer, the PrEP coordinator for Iowa’s Department of Public Health, directs him to a patient navigator who specializes in ACA enrollment and assists him during the 20-minute wait for results. Shafer says it’s the first time that many of his patients have had insurance, which allows them to access a host of preventive services, such as programs to quit smoking, treat substance abuse and combat diabetes risks.
What’s more, to maintain their PrEP prescriptions, each recipient must get tested for HIV every three months, four times as frequently as other men who have sex with men, according to Grant’s experience as a clinician and data from the Centers for Disease Control and Prevention. This infrequent testing helps explain why 1 in 8 HIV-positive people in the U.S. is unaware of their status.
But, these secondary benefits may soon disappear.
Though it’s unclear how (or if) the ACA will be repealed, the plan passed by the House last week would certainly lead to fewer insured Americans and, by extension, fewer patients able to afford PrEP. Gilead offers that $6,000 co-pay discount to patients with insurance and a full subsidy to those without, but that assistance will be insufficient.
“To qualify for those programs, you need to have a motivated physician who’s willing to fill out the forms. If you don’t have insurance, you won’t have a physician,” Grant said.
And, Gilead also doesn’t cover lab fees, which, for my latest visit, would have cost me $615.81.
The dangerous practice some users engage in
When patients are unable to access Truvada through official channels, they find other means. Shafer told me he’s already seen men in Iowa who drop down to four doses a week to conserve pills, HIV-positive patients who ask for early refills to share or sell, and PrEP users who continue to fill prescriptions even after they’ve stopped engaging in risky behavior.
“They want to have extra on hand to help out friends and partners who lose coverage,” he said.
Considering the drug’s effectiveness and ease of use, it’s understandable that patients will choose to have some protection over none. However, the greatest risk of PrEP is contracting HIV and then taking Truvada, which is also used to treat the disease, and that potentially leading to mutations that make patients resistant to an entire class of antiretrovirals.
To make matters worse, HIV can lie dormant and asymptomatic in the body for years, and at-home tests can miss an infection as far back as a month. Newly infected patients are the most contagious vectors, and without any symptoms to slow them down, they can spread the disease with astonishing quickness. (Some of the first men to die of AIDS reported more than 2,500 lifetime partners.)
A missed opportunity
Republicans’ health care reform proposal comes at a precipitous time for the AIDS epidemic. Current treatments are effective enough that HIV becomes nearly undetectable in the blood, but antiretrovirals don’t come cheaply. The CDC estimates that the lifetime cost of treatment is $379,000, and allowing insurers to discriminate based on pre-existing conditions would, of course, be catastrophic for HIV-positive patients, 30 percent of whom are already uninsured.
Echoing Shafer, Dr. Michael Ohl, an infectious disease specialist at the University of Iowa, says that these patients may sell their Truvada to make ends meet, which will raise their viral load — and their chances of transmission.
By all accounts, I’m fortunate: for being young, healthy and without any pre-existing conditions and for being well-equipped to navigate bureaucracies, able to afford health insurance, and now in a monogamous relationship. If the ACA is repealed, however, others won’t be so lucky, which could jeopardize the last three decades of progress in combating the epidemic.
-- This feed and its contents are the property of The Huffington Post, and use is subject to our terms. It may be used for personal consumption, but may not be distributed on a website.
from http://ift.tt/2rcPdYM from Blogger http://ift.tt/2rnGQah
0 notes