#USPH
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The Tumblr app for Google Glass was released on May 16, 2013.
Text
Nyo!AmePhil Fluff HCs
Maria sings to Amelia ALL the time. Amelia finds her voice to be the most beautiful and calming thing ever. Maria sings when brushing Ame's hair, when they're in the car together, and even hums soft melodies when she does small things like tie her shoes. Amelia loves this about her.
HARANA!! Phili definitely went outside Ame's doorstep, guitar in hand and serenaded her (im a creep, im a weirdo)
Since Phili is shorter than Amelia, there's a lot of headpats and resting her chin on Phili's head (even if she has to tiptoe to do that last one)
Amelia cannot handle spice while Maria can dump a cup of tabasco on food and feel nothing (exaggeration). This spice tolerance gap leads to very interesting and goofy moments where Ame's face starts burning after eating Maria's sisig, Bicol Express, or any food that's a little spicy
Amelia has a loud laugh that most people will think is annoying, but Maria seems to be the only one who can tolerate it
They both listen to musicals together (i have OdyPen but its Nyo!AmePhil brainrot)
I HC that Amelia does boxing as a hobby and Maria is always there to watch matches, though she gets really worried about Amelia being in pain after sparring. She's very gentle with nursing Ame after she gets hurt.
I also HC that Maria plays volleyball and gets smacked in the face every now and then. Unlike Maria, Amelia freaks the hell out and causes a scene when she's felt the slightest bit of pain (AAAAA WHAT DID YOU DO TO MY BBG type shit lol)
Amelia can doodle and Maria can write. They want to make smol picture books together :3
There's not exactly a "better one" when it comes to video games. Amelia is great at Valorant, Apex Legends, CS;GO while Maria is better at Leauge of Legends, Overwatch, Fortnite. They're kinda balanced in skill at fighting games so the winner normally depends on the circumstance when they play
#nyoamephil#amephil#usph#hetalia#hetalia nyoamephil#hetalia amephil#hetalia usph#nyo america#nyo philippines#hetalia OC#OC
8 notes
·
View notes
Text

Celine Farach by © Justin USPH
2 notes
·
View notes
Text

Mary Lee Mills by Betsy Graves Reyneau 1952
Capt. Mary Lee Mills (1912 – 2010) USPHS, MSN, MPH, RN, CNM, began her career in public health as a nurse-midwife. In 1946, Mills joined the United States Public Health Service, where she completed tours of duty in Liberia, Lebanon, and South Vietnam. She helped to establish the first nursing school in Lebanon. She was awarded Lebanon's National Order of the Cedar in response to her efforts.
#mary lee mills#betsy graves reyneau#black history month#oil on canvas#black women#woc beauty#portrait
737 notes
·
View notes
Note
I encountered a drug called "Dextromethorphan" when looking up things that react with grapefruits for a fic. I found out it's been banned in Sweden since the 90s, so I couldn't use it for this specific story, but if you've got any interesting history I'd be happy so know!
Are you ready for this? Like. Ask yourself. Are you really ready for this?
In 1954, a researcher with the US Public Health Service received $282,215 (1954 dollars) from the US Navy, ostensibly to find a non-addictive alternative to an opiate drug called codeine (used for pain and and as a cough suppressant).
So the researcher found a bunch of people who had substance abuse disorder and tested 800 substances on them, trying to find ones that couldn't cause physical or psychological dependence, even on people who were prone to that sort of thing.
(Now, you might be asking if this experiment was ethical. The USPHS was concurrently doing the infamous Tuskegee Syphilis Study, so while I couldn't find any concrete answer, imma guess no.)
Out of these 800 tested substances, we use 3 today: propoxyphene (used as a painkiller), diphenoxylate (used as a diarrhea medication), and dextromethophan (a cough suppressant (and, as of 2022, part of a fast-acting antidepressant)).
Importantly, it was later noted that all of these are addictive substances and today most of them require a prescription. Though depending on where you are in the world, you might just have to be over 21 and show an ID.
You might think this sounds like a pretty standard story.
You would be wrong.
Because while the US Navy was the one handing the money to the USPHS, the US Navy had come by it via the Central Intelligence Agency.
Yes. The good ol' CIA.
So what stake did the CIA have in a non-addictive codeine replacement? Nothing, it turns out. That's just what they'd told the US Navy. What they really wanted was an incapacitant- a drug that causes incapacitation like unconsciousness or continuous hallucinations- without killing. Incapacitants are also useful for discrediting prominent political figures by making them look like they have severe mental health concerns, which was another reason the CIA wanted them.
This was part of a project called MKPILOT.
And wouldn't you like to know which of the three listed above they liked the most? Dextromethorphan. Because at high doses it causes severe- and incapacitating- hallucinations (this is also why it is banned in Sweden).
The problem with it is that it requires really, really high doses (about 3 grams, which would have to be packaged in some other substrate)- this would make it difficult to slip into a drink or food.
(It should be noted that around the same time, the US Army was doing research into a much more usable incapacitant called 3-Quinuclidinyl Benzilate which required as little as 150mg of the substance to be useful- it was featured in a MacGyver episode and I did a nice little review of it here. While I have no sources that say the CIA was directly involved in funding this, based on their extensive funding of similar DoD projects at the time, they probably did.)
But you wanted to know about how grapefruit interacts with dextromethorphan:
A substance in grapefruit (along with seville oranges, limes, pomelos, and possibly pomegranates) blocks the pathway by which many drugs are metabolized in the liver. This causes the levels of drug in the body to be much higher than expected. In the case of dextromethorphan in particular, it can mean that the drug stays in the body a lot longer- up to 24 hours instead of the usual 3-4 hours. It can also make side effects and toxic effects significantly worse, leading to hallucinations and sedation, even at low doses normally used for coughing.
220 notes
·
View notes
Text
Hamilton tour will first premiere tonight at the Philippines!
So here is an art to celebrate it AHSBAHSBAJA

If we premiere a play about the American Revolution here. Should we do a play about the Philippine Revolution + USPH war and premiere it on the US? 👀
#yknow for representation about us filipinos and our history~#“But here lies love is an all filipino play? isnt that the best representation you could ask for?” No ~ <3#hetalia#hws philippines#hetalia world stars#hetalia philippines#aph philippines#hetalia axis powers#hetalia america#hws america#aph america#amephil
151 notes
·
View notes
Text
A "study" was conducted 1932-1972 where the CDC/USPHS lied to and allowed nearly 400 black men to die of syphilis who were completely treatable
24 notes
·
View notes
Text
The Yellow Berets, also known as Public Health Service trainees, were a group of physicians who participated in the National Institutes of Health (NIH) Associate Training Program during the Vietnam War era. They were often derogatorily referred to as "Yellow Berets" by supporters of the war who viewed them as avoiding military service. However, this term eventually became a badge of honor among the participants, many of whom formed a network of influential scientists and medical leaders that continue to dominate the public health enterprise, particularly at NIH. While most of these are now retiring out of the USPHS, they have fostered a culture and mentored others that continue to enforce that culture and support the informal networks, alliances and power relationships that dominate the USPHS and the overall US medical research enterprise.
Physicians who served in the U.S. Public Health Service (USPHS) during the Vietnam War primarily worked at the NIH or other federal health institutions, including the CDC and FDA. For example, during the Vietnam War, physicians could serve their draft requirement by joining the USPHS, which allowed them to work at places like the CDC. Their common experience, background, and cultural biases fostered natural affiliations that eventually developed into a loose network of influence that came to dominate both the NIH and the USPHS. Dr. Anthony Fauci is one example of a successful “Yellow Beret”.
9 notes
·
View notes
Text
20 Questions For Writers
Was tagged by @kuraiarcoiris and decided why not. :V
1. How many works do you have on AO3?
35. I have more on other sites, but since I've made my AO3 account, that's how many I've posted there.
.
2. What’s your total AO3 word count?
656,547. Give or take a couple thousand.
.
3. What fandoms do you write for?
Currently? Dream SMP. But I also have an Inscryption WIP and a couple Kpop WIPs that I really should get back to one of these days. orz But I've written for all sorts of fandoms over the years.
.
4. What are your top five fics by kudos?
5) Its Suffering Was Real [Inscryption]
This is the one that came as the biggest shock to me when I went and looked at my kudos count in preparation for this write-up. Like, really? People like the fic where I torture the sassy robot trapped in the body of a stoat for 7k words that much??
4) A Shoulder to Lean On [Avatar: The Last Airbender]
WHERE did all these people come from, I have like 6 comments on this thing (not counting my replies)??? I mean, I'm flattered, but ??!!?!
3) Accepting Amelioration [Voltron: Legendary Defender]
I mean, it's a Voltron fic posted back when the fandom was in full swing, it doesn't really surprise me the kudos counter is considerable, though I am still surprised it got that much traction considering the fic is gen and not shippy. Am still proud I made the first daemon AU in the entire fandom, though, if this is my claim to fame, then I'm ok with that. :p
2) Temporary Shelter [Astro / VIXX]
I seriously have no freaking clue how this little self indulgent Kpop crossover fic became so popular, I really don't. I mean, Kpop crossovers are niche at the best of times, and these two groups aren't exactly the most popular Kpop fandoms on AO3 if you know what I mean. It basically started as "wouldn't it be fun if my two favorite Kpop groups were secretly friends all this time? How would I have that happen, tho?" and then snowballed from there. I, uh. I'm glad so many other people like it, ig? 0_0
1) Paved with Pawprints [My Hero Academia]
Of course it's the MHA pet AU fic. Of course. OF COURSE-
.
5. Do you respond to comments? Why or why not?
Absolutely. It's only fair I reply if someone takes the time to read on my work and actually give me feedback about it, wouldn't you say? Plus, like most authors, I enjoy talking about my own work, so sue me. >:p
.
6. What’s the fic you wrote with the angstiest ending?
I don't usually do angsty endings; I prefer happy or at least bittersweet ones. I guess by default, it has to be the fic where I slowly killed off America and China from Axis Powers Hetalia for 13k words, while the rest of the cast had already been dead for centuries at that point. So yes, the entire cast of that series was dead by the end of that fic. :))) IN MY DEFENSE, ok, I was actually trying to give them a bittersweet ending by reuniting them with all of their old friends and family by finally letting them rest after so long alone, but it still turned out really sad. TT TT It's basically my only fic where I can't go back and reread it more than once every couple of years, because I still end up a sobbing mess by the end.
.
7. What’s the fic you wrote with the happiest ending?
Well, I guess that's what you define "happiest" as. The most cathartic? The one with the least amount of trauma and extreme bodily injury incurred by the characters? 🤔 I guess by the latter definition, it would Kaleidoscopic Perceptions, a very fluffy USPH college AU that I actually enjoyed writing a lot despite me not usually enjoying romance or college AUs.
.
8. Do you get hate on your fic?
No, thankfully. I've gotten a couple kinda weird comments, and of course the obligatory "It's been X months since you updated were you aware?????" comments, but no outright negativity.
.
9. Do you write smut?
LMAO. Absolutely not.
.
10. Do you write crossovers?
Yes! I really love crossovers. I have a few common fallbacks that fit with a lot of fandoms (daemon AUs, Firefly AUs, etc.), but I also enjoy fandom-specific crossovers when I can figure out how to pull them off.
.
11. Have you ever had a fic stolen?
No idea. I hope not!
.
12. Have you ever had a fic translated?
Just once for this Gravity Falls fic.
.
13. Have you ever co-written a fic?
Yes. It had a few ups and downs, but it was overall a really positive experience, and I think it turned out really well!
.
14. What‘s your all-time favorite ship?
idk that I have an ALL TIME favorite ship, especially since I hardly ever ship anything, but Frobin is pretty choice, I gotta say.
.
15. What’s the WIP you want to finish but doubt you ever will?
Er, none of them, hopefully? I hope that I eventually get to finish all my WIPs at some point, even if it might take me awhile. >.>; But I suppose if I had to pick ONE to abandon, I'd probably pick Written In, my D&D Inscryption crossover AU. I like the IDEA for it, but writing it out is like pulling teeth, and after the first installment where the party gets together, I don't really have a lot of ideas on where to take the plot. :/ Like I have the general overarching idea but no plot structure or anything but small disconnected story beats.
.
16. What’s your writing strengths?
I like to think I do a pretty good job with descriptions while not bogging the story down too much with too much detail?
.
17. What’s your writing weaknesses?
Uuuuuuuuuuhhhhhh, staying motivated ig. ¯\_(ツ)_/¯ if you're asking my weakness about mechanics, though, uh... exposition, I guess? Dialogue in general, sometimes.
.
18. Thoughts on writing dialogue in another language for a fic?
If there is actual information included in the other language, then you better provide a translation. If it's just for flavor, though, have at it.
-
19. First fandom you wrote for?
TMNT, specifically the 2003 show. It's never been posted anywhere on the internet and never will. :)
-
20. Favorite fic you’ve ever written?
Becoming Real, a Kpop fanfic based on VIXX's Voodoo Doll MV. However, it can easily stand on its own as its own original work. I consider it the most accessible story I've ever written, and it also was just very easy for me to write. Writing is often like pulling teeth for me, but not this story.
Tagging: @breezy-cheezy, @quicktothebatjalopy, @hiding-in-the-vault, @variablememory, @bleue-flora, @theriu
7 notes
·
View notes
Note
oooh, in the last ask you mentioned seasia... i think if done right, amepiri/usph could have some hot yaoiyuri action going on esp knowing their historical background... i KNOW YOU SAID IF AME DIDN'T EXIST ASHDSJGF but i needed to ramble abt my weird amepiri kink and the potential they have... feel free to ignore this ask ღゝ◡╹)ノ♡
ah i kind of think i wouldn't've? 😅🙏... when it comes to seasia colonizer ships im like. i don't even know i probably wouldn't touch the other ships. when it comes to like nethindo it's that i'm mostly seeing other indonesians draw it. 🙆♂️ even then i wouldn't even say nethindo is like the ship i like for neshi. if you're filipino that's your prerogative i just doubt i would've touched that
#ask#also i'm unlikely to be historical hetalia drawing so#if this had been the case i would've not been making anime gooner art#would i have drawn anime gooner art of motherland instead. its a divisive question
4 notes
·
View notes
Note
💌 or 🏆 for the hetalia asks game!
get-to-know-you-better hetalia ask game! version 2.0
💌 - what are your "essential" ships? (in your version of the hetalia universe, these characters have to be a romantic pair - and them not being one feels weird/wrong)
AusHun are always ex-spouses who have unresolved feelings for one another; Velvet Pair are always ex-spouses who are better divorced and still have romantic feelings for one another. FrUk is always on-and-off that everyone just assumes they're shagging at this point. Beyond that, everything is honestly fair game; I tend to treat my ships as scenarios with some I just happen to prefer more than others. Even USPH which has consumed my brain is just a scenario I prefer, although I guess it's prevalence in my headspace might make it count as a default ship? (But even then I think of MexPhil or RusAme or SKUSPH sometimes...)
🏆 - sell us on a character! maybe it's someone who you think deserves more love - tell us why they should be liked!!
there's a lot of untapped potential with exploring HWS Singapore! A boy whose ambition was born out of circumstance, driven to a place from the consistent disappointments and betrayals from the figures around him that brought him to the conclusion he must change himself to survive, and change himself he did in a single generation that he still hasn't processed what he's had to trade off in expense to secure his stability and success. A pragmatist by circumstance! Has a lot of identity issues because of the strict definitions he's structured himself around and how those don't always neatly fall into lived realities! Food is his ultimate expression! I'm rambling at this point but gestures!! he's been a brainrot I've had for a while and this doesn't even scratch the surface of that brainrot but gestues!!!!
6 notes
·
View notes
Text
Nyo!AmePhil Headcanons
Hi so Philippines' personality is mostly based off my OC (notes found here) and for the sake of simplicity I'll refer to them as Ame and Phili
I went over their history dynamics over in my PH rant so let me summarize by saying that Ame and Phili were childhood friends who wrote to each other while they were still colonies
Ame promised Phili that one day they will both be free together
Now we skip to when Ame made this whole elaborate lie to cover up the whole Treaty of Paris thing and made it look like she single handedly freed Phili herself
Of course Phili was glad that her best friend kept her promise! Now she can be independent and happy
Obviously that didn't happened because Ame stabbed Phili in the back and the imperialism thing happened
Phili being pissed at the lie and betrayal tried to fight her way out of it but failed. Even though Ame said the rule was temporary it still pissed her off.
I like to think that Phili burned all the letters between them (NOT A HAMILTON REFERENCE) as a sign of her trust in Ame disappearing.
She'd snub Ame's advances and attempts to "win her back"
And then Japan invaded in WWII and Ame promised that "She shall return" to Phili
And Phili put up a good fight but was no match for Japan. She hated not being strong enough and secretly dreamt of Ame fulfilling her promise to free her.
Eventually Ame did come back and shooed away the Japanese forces.
I like to think that this is where Phili first caught feelings for Ame but just repressed it
Anyways Ame asked if Phili wanted to still be a colony of hers or be free and Phili (tired of not being independent) chose freedom. Even if it meant she and Ame won't be that close anymore.
So here's where I headcanon that they kiss each other goodbye LMAO and Phili hopes that Ame will keep in touch
Ame did in fact NOT keep in touch
Ame was so busy with the cold war and race to space stuff that it seemed like she neglected Phili and that upset Phili again
So she buried whatever romantic feelings she had for Ame, and moved on with her life
But Ame never forgot about Phili. She lived rent free in her mind. But the sad thing is that she was too caught up with her being a growing nation that she wasn't able to be as close as she wanted to be.
The first time they saw each other was in ASEAN's first world meeting and Phili still held a grudge while repressing her feelings
Ame tried to catch up and get her crush friend to talk to her again but she was given the cold shoulder
So yeah happy ending? We'll see where this goes, I'll just and make content for them eventually but I adore the idea of them not being in good terms and learning to fall in love with each other again slowly
EDIT: I FORGOT that my angst headcanon is that since philippines is normally liked by her peers and america is disliked for being (yk america), there's this sort of envy that clashes with the on/off crush thing that makes this yuri complicated~
#amephil#usph#hetalia amephil#nyoamephil#actually my tag for this stuff will be nyoamephil#hetalia oc#nyo america#nyo philippines#aph usph#aph amephil
2 notes
·
View notes
Text
Home and Community-Based Waiver Services Program in Alaska Needs Statement. According to Goins and Spencer (2005), the provision of services to specific populations, particularly those groups who face barriers to equity in healthcare, has always been an important focus of public health. The public health perspective outlines a societal approach to protecting and promoting health, which emphasizes prevention, macro-level interventions, and the reshaping of public policy. A primary difference between public health and the more biomedical model is that the government often subsidizes care providers in public health, with a focus on preventing, rather than curing, disease (Goins & Spencer, 2005). Older American Indians and Alaska Natives (AI/ANS) life expectancy has increased dramatically since the early 1970s. This increase, from 63.5 years in 1972 to 73.2 years in 1994, is largely attributed to the efforts of the Indian Health Service (IHS) to eliminate infectious disease and meet the acute-care needs of AI/ANS (Goins & Spencer, 2005). Despite these improvements, much remains to be done to bring the healthcare standards of these peoples up to the national standard. In this regard, Padgett (1999) emphasizes that, "Problems with health and mental health that face older American Indians and Alaska Natives are widespread and likely to intensify if current trends continue. Several publications have detailed their excess morbidity and mortality and in comparison with whites and other ethnic minorities" (p. 139). The IHS reports that The Alaska Area Indian Health Service (IHS) works in conjunction with Alaska Native Tribes and Tribal Organizations (T/TO) to provide comprehensive health services to 139,107 Alaska Natives (Eskimos, Aleuts, and Indians). Approximately 99% of the Alaska Area budget is managed by T/TOs pursuant to the Indian Self-Determination and Education Assistance Act, P.L. 93-638, as amended. The Alaska Area negotiates and administers 14 Title I contracts and one Title V compact with 25 separate tribal funding agreements. The latter has resulted in the Alaska Tribal Health Compact, which sets forth terms and conditions for tribal management of a comprehensive system of health care that covers all 228 federally recognized tribes in Alaska. IHS-funded, tribally-managed hospitals are located in Anchorage, Barrow, Bethel, Dillingham, Kotzebue, Nome and Sitka. There are 37 tribal health centers, 166 tribal community health aide clinics and five residential substance abuse treatment centers. The Alaska Native Medical Center in Anchorage is the state-wide referral center and gatekeeper for specialty care. Other health promotion/disease prevention programs that are state-wide in scope are operated by the Alaska Native Tribal Health Consortium (ANTHC), which is managed by representatives of all Alaska tribes. There are 37 residual positions in the Alaska Area IHS, which perform inherently federal functions that cannot be contracted to T/TOs. The Alaska Area supports USPHS Commissioned Corps officers and civil service employees to T/TOs to aide them in the provision of health services. Additionally, to address the critical shortage of medical providers in remote facilities, the Alaska Area IHS awards federal personal services contracts for itinerant and emergency providers to work in tribal facilities. During FY 2010, providers hired through Area Office PSCs numbered 44 dentists, 27 physicians, 3 nurses, 20 pharmacists, 3 optometrists and 4 nurse practitioners. Other federal agencies such as the Arctic Investigations Laboratory of the Centers for Disease Control (CDC), work closely with the Alaska Area IHS and the tribes to improve the health status of Alaska Natives. The Indian Health Service still holds title to six tribally operated hospitals and three tribally operated health centers in Alaska, and is responsible for their maintenance (Alaska Area Indian Health Service, 2011). Although the life expectancy of AI/ANS has improved, it is still below the national average. Certain demographic characteristics make older AI/ANS particularly vulnerable to experiencing health disparities, compared to the general population. Poverty and low educational levels are common among AI/ANS; 27% of AI/ANS ages 65 to 74 live below the poverty level, compared to 10% of the general population and 8% of Caucasians, and one-third of AI/AN elders age 75 years or older live in poverty, compared to 17% for the general population and 15% for Caucasians. Some 8.9% of AI/ANS have a bachelor's degree or higher, compared to 20.3% of the general population and 21.5% of Caucasians. Taken together, poverty and low educational levels are strongly associated with poor health and an increased likelihood of chronic and disabling conditions (Goins & Spencer, 2005). As they have for other ethnic groups, the most notable population health problems experienced by AI/ANS have shifted from infectious diseases to chronic diseases. Two of the most prevalent chronic diseases among older adults in this group are diabetes and arthritis. AI/AN elders experience some of the highest rates of diabetes in the world. In general, diabetes is four to eight times more common among AI/ANS than among the overall U.S. population. The prevalence of arthritis is also greater among AI/ANS than among non-AI/ANS, a difference most likely genetic in origin. Furthermore, the age of disease onset may be earlier. For example, half of one reservation population with rheumatoid arthritis was diagnosed with the disease before age 35, much earlier than is commonly found among non-AI/ANS. Mounting evidence suggests that such chronic and disabling diseases among AI/ANS are increasing and represent substantial healthcare costs (Goins & Spencer, 2005). One of the strongest determinants of use of long-term care, either institutionalized or non-institutionalized, is health and functional status. Estimates suggest that AI/AN elders experience some of the highest physical disability rates of any U.S. ethnic group. While African-Americans are more likely than Caucasians to experience the disadvantages of shorter life and longer periods of health impairment, for AI/ANS, the levels of impairment and length of inactive life are the highest among all ethnic groups, with approximately 50% to 60% of the later years spent with disabilities (Goins & Spencer, 2005). Thus it is not surprising that long-term-care provision is especially important in Indian Country, because of the socioeconomic disadvantages to which AI/ANS are subject and the growing rates of chronic disease and physical disability that they experience, as described above. While one of the core functions of public health is to ensure that all populations have access to appropriate care, a number of issues present particular problems in delivery of services-especially provision of long-term care. Distinctive factors related to culture, AI/ANS political status, and related implications for health policy appear to compound the problems of low socioeconomic status and poor health for AI/ANS (Goins & Spencer, 2005). Federally recognized tribes have a unique political status that has influenced provision of public health services that is based on the sovereignty of federally recognized tribal governments, the treaty-making process under which the U.S. assumed certain responsibilities to tribal governments, and the resulting federal-Indian relationship. A breakdown of the native peoples of Alaska is provided in Table __ below. Table Breakdown of Native Peoples of Alaska Native People Description/Status Eskimos More than half of all Alaska Natives are Eskimo. The two main Eskimo groups, Inupiat and Yupik, differ in their language and geography. The former live in the north and northwest parts of Alaska and speak Inupiaq; the latter live in southwest Alaska and speak Yupik. Few Eskimos can still speak their traditional Inupiaq or Yupik language as well as English. Along the northern coast of Alaska, Eskimos are hunters of the bowhead and beluga whales, walrus and seal. In northwest Alaska, Eskimos live along the rivers that flow into the area of Kotzebue Sound. Here, they rely less on sea mammals and more upon land animals and river fishing. Most southern Eskimos live along the rivers flowing into the Bering Sea and along the Bering Sea Coast from Norton Sound to the Bristol Bay region. Aleuts Most Aleuts originally lived in coastal villages from Kodiak to the farthest Aleutian Island of Attu. They spoke three distinct dialects, which were remotely related to the Eskimo language. When the Russians came to the Aleutian Islands in the 1740s, Aleuts inhabited almost every island in the chain. Now, only a few islands have permanent Aleut villages. Severe and unpredictable weather conditions in the Aleutian Islands make transportation both expensive and time-consuming. The region is dependent on the fishing industry, which is variable from year to year. Interior Indians The Athabascans inhabit a large area of Central and Southcentral Alaska. They may have been the first wave of Natives to cross the land bridge over 15,000 years ago. Although their language is distinct, they may be linguistically related to the Navajo and Apaches of the Southwest U.S. There are eight Athabascan groups in Alaska. Characteristics of all eight groups include similar language, customs and beliefs. Source: Indian Health Service Alaska Area Services (2011) The Indian Health Service is a federal agency in the U.S. Department of Health and Human Services that provides free healthcare to tribally enrolled AI/ANS, more than 1.6 million individuals, principally through the operation of sixty-one health centers and thirty-six hospitals (Goins & Spencer, 2005). It should be noted, though, that the provision of these healthcare services is constrained by the vast geographic distances that are involved in Alaska. The majority of communities in Alaska are separated by vast distances and the distance from many communities to the nearest medical facility is equivalent to the distance from New York to Chicago (Indian Health Service Alaska Area Services, 2011). A study funded by AOA examined issues affecting access to home- and community-based long-term-care services among AI/ANS. Study results indicated that home healthcare was one of the most frequently needed services among AI/ANS. Further, 88% of the services sometimes, rarely, or never met the need, and 36% of services were rarely to never available (Jervis, Jackson & Manson, 2002). Only twelve tribally operated nursing homes exist in the U.S., and these rely predominantly on funding from Medicaid and tribal subsidies. Many tribes would like to have nursing homes but are blocked by state certificate-of-need requirements, Medicaid licensing requirements, and lack of commercial financing. The lack of alternate medical resources, whether private insurance or public programs, may limit for AI/ANS access to specialty medical care and long-term care not included as part of IHS benefits. This situation makes older AI/ANS particularly likely to experience disruption in continuity of care. Tribes have started to express a growing interest in providing options for home -- and community-based long-term care to keep ciders in their homes as long is possible. Some important services funded through Title 6 of the Older Americans Act include congregate and home-delivered meals, information and referral, home assistance services, and the relatively new Family Caregiver Support program (Goins & Spencer, 2005). 2. The goals and objective of the change effort There are three main goals for this policy initiative as follows: 1. The main goal is to increase accessibility for individuals who will need these services. This will help reduce institutionalization of this group and enable them to remain in their own home. 2. Create an environment where individuals who receive services will have their rights protected and not have services denied unjustifiably. 3. Quality of these services should be maintained or increased when possible. In support of the three overarching goals above stated, the policy initiative will also be guided by the following objectives: 1. Educate the "community" to increase participation in this program. Most eligible people don't even know that programs like these exist. 2. Work with area hospitals to ensure that individuals being discharged are recommended for waiver services which will enable them to return to their own homes or communities. 3. State of Alaska will ensure that enhance services are available to qualified individuals in the most effective manner. 4. Ensure that the state has an efficient system for those who don't qualify can appeal their cases. 5. Address the shortage of staff at the state level to ensure that people needing HCBWS are located and assessed quickly. 3. Overall policy strategy. The unique political relationship between the federal government and AI/AN tribes adds another layer that must be considered in determining how to best serve this population (Goins & Spencer, 2005). Therefore, the overall policy strategy that will be used to achieve the above-stated goals and objectives are as follows: 1. Since there could be a waiting period for recipients to get screened for HCBWS, early application should be encouraged. 2. Grants should be readily available as a stopgap measure for those on the waiting lists. 3. As noted above, Alaskan communities are far and wide. Agencies located in remote areas should also meet the same certification requirements as those in big cities. With no one to take care of their elderly parents, the cost to society in hospital care begins to strain the system. Therefore, one viable approach will be to have HCBWS services in place to help reduce costs in the long run as described further below. 4. Alternative proposals for the change effort, and the criteria used to select an alternative. Usually there will be many criteria to follow when selecting a proposal. This will depend greatly on the "complexity" of the proposal. In the case of the HCBWS proposal, I will use the value-based criteria. This is an important criteria according the class text, "they provide a normative basis for comparing options," in this case the options will be the fairness of leaving the elderly and disabled to be institutionalized or having them back in their homes where they may be more comfortable in among their neighbors while cost of care is reduced at the same time. Therefore, the policy issue addressed in this project concerns the role of home and community-based waiver services (HCBWS) and the role played by in-home support services in the lives of frail elderly individuals in Alaska. Formulation 1. Rationale for the proposal. Identify additional data to be compiled to back up proposal. At present, a broad array of evidence-based practices exist to care for the elderly in their communities, but there remains a lack of application of these practices to the population of interest to this study. For example, according to Padgett (1999), "Our recognition and understanding of health and mental health problems of older Indians have been slow to mature in spite of evidence of extensive need. Programs to identify and intervene among the elderly in the general population have been found to be effective. Yet, few of these have found their way to Indian and Native communities" (p. 140). 2. The arena for policy change. The proposed budget for the home and community-based waiver services (HCBWS) program will consist of funding requests that will sustain the program over the next two years. We have included the salary request for various staff members who will be involved with the program in the final narrative provide the explanation for the total cost of the program. The initiative would use the state's fiscal year July 1 through June 30 as its budget year. Some funding will come from the federal government because this program is a partnership between the state and federal government. This program will be seeking funding based on what it would take to administer education provide in-home support; providing training to direct caregivers intercessors who will qualify consumers of this program over the year. It is anticipated that 1000 applicants will enroll in the first year with roughly 10% not deemed qualified to enroll for the program. It is anticipated that of the qualified enrollees 5% might not make it through the year because of the severely of their illness. The narrative for funding and expenses is located at the end of this budget report. 3. An analysis of political feasibility of the policy/program including your approach to garnering support from decision-makers (both for and against) who will be involved in the change effort. With the current healthcare environment undergoing fast changes in policies and laws by the state and federal governments, it is very easy for HCBWS and in-home supports issues for the elderly to fall by the wayside. Successful advocacy on this will require taking this issue to the legislature and insisting that legislative power and political clout to determine which strategies will work most. Some of the strategies will include initiating policy proposals, identifying and understanding the relevant legislative committee chairpersons, as well as developing a comprehensive understanding of these committees and also how to communicate and negotiate with them. Stakeholders will work to develop solutions by providing information and tools to ensure that elderly individuals who need HCBWS as are not overlooked. 4. An analysis of economic feasibility, including the projected costs and the availability of current and future funding. The director of HCBWS ensures that the program is established and remains successful. The director is the head of SDS and is in charge of all seniors and disabilities services and reports directly to the commission of the HHS who reports to the governor. The director can also answer to the legislature, works with all other community-based organizations. Program managers will ensure that the programs are implemented according to state regulations and standards. They will ensure individualized program success through education, adult protection, quality assurance, etc. The program also ensures that assessments are carried out on applicants to determine their eligibility for the program. Administrative assistants and office assistants will ensure that all office supplies, travel request, administrative support are maintained. The total cost to implement my proposal in 2011 is projected to be $6,910,000 and for 2012, the figure will be $9,025,000. Implementation 1. A projection of the effectiveness of the policy. It is anticipated that by 2012 the program would have been well-known in the community hence the increase. 2. A discussion of interactions among policies/programs or possible unintended outcomes. There are some potential cross-cultural constraints to the delivery of the healthcare services envisioned in this policy initiative that may adversely affect the effectiveness of the program. Such cross-cultural differences are well documented in other settings, but even here, there remains a paucity of timely and relevant research concerning the needs of frail elderly AI/ANS today. In this regard, Goins and Spencer emphasize that, "The professional move toward acknowledging and effectively addressing the role of culture in provision of appropriate care or services is referred to as cultural sensitivity or cultural competence. Challenges associated with measuring and assessing cultural competence have been well documented. Still, the role of culture in the public health of AI/ANS necessitates an effort to better understand the effect of cultural differences on service provision" (2005, p. Read the full article
0 notes
Text

U.S. Physical Therapy Reports Strong Financial Results for 2023 as Dividend Payout Ratio Increases $USPH #Dividend #NYSE #StockMarket https://csimarket.com/news/u-s-physical-therapy-reports-strong-financial-results-for-2023-as-dividend-payout-ratio-increases2024-02-28214563?utm_source=dlvr.it&utm_medium=tumblr
0 notes
Text
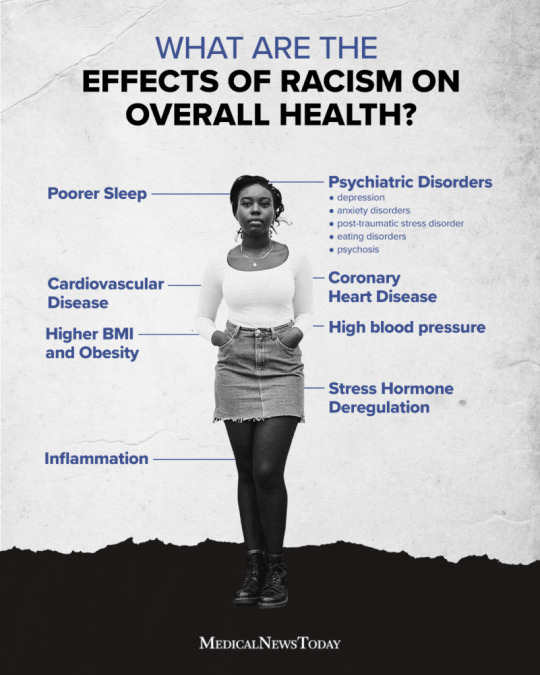
Racism in Healthcare
By Christian Dela Cruz
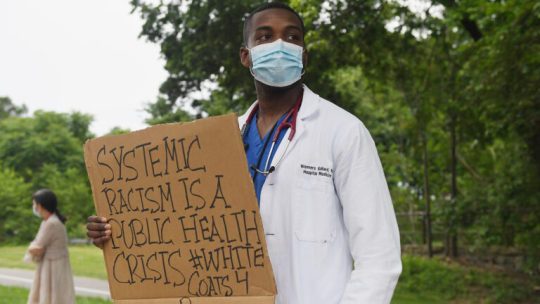
Racism in Healthcare. Throughout America decades and even centuries of racism, bias, and stereotypes has affected the level of care provided to those of color. Disproportionately affecting minority health as compared to their white counterparts. For example the Center for Disease Control states, " The data show that racial and ethnic minority groups, throughout the United States, experience higher rates of illness and death across a wide range of health conditions, including diabetes, hypertension, obesity, asthma, and heart disease, when compared to their White counterparts. Additionally, the life expectancy of non-Hispanic/Black Americans is four years lower than that of White Americans." This highlights how race affects those of color regarding the quality of healthcare in which they receive compared to their white counterparts. Throughout America as a result of systemic racism many minorities view the healthcare system as a scam used to take advantage of the poor. This directly leads to minorities not taking part in annual checkups leading to lower life expectancies as they are diagnosed at later times preventing them from receiving the proper preventative care to limit their exposure to things like diseases or catching cancer early.

Systemic racism in healthcare can lead to unethical medical practices and experiments. One notable example of this is the Tuskegee syphilis study conducted by the US Government in the 1930s. During the experiment, the United States Government selected 600 African Americans from the south for the experiment with promises of medical insurance and better health care than what was available to them. The purpose of the experiment was to study the syphilis and its effects on the human body. As treatment for the disease became available to the public the 600 participants were denied care for their disease as it was viewed at the time as necessary in order to study the effects of syphilis. As a result of this the participants were denied the penicillin necessary to cure them of their ailments. Due to this many of them would pass away along with passing the disease to many of their family members. Following public outcry and class action lawsuit from the survivors and their family members of those who passed away from the experiment the United States government created a fund in order to compensate them from the medical malpractice and participation in the experiment. The government also promised them free medical care. Though this would be ill served as by the time of this promise many of the survivors had passed away as a result of the experiment.
Addressing Racism in Healthcare
Racism in healthcare can be addressed by following simple steps. For example by increasing the diversity of a healthcare facilities employees patients can feel more open to their healthcare providers as they can feel more comfortable communicating their healthcare concerns to someone who looks like them as opposed to a white doctor that they may not feel comfortable sharing their health concerns with. Another step one can take to address racism in health care is by making it more accessible to those in lower income communities. Which are predominately made up of minorities as a result of systemic racism. This disproportionately affects people of color as quality healthcare becomes unavailable to them. By lowering the cost of health care minorities can have more access to hospitals that can increase their life expectancy. These are just a few examples as to how racism can be addressed in healthcare thus bettering the quality of patient care for people of color.
Additional Links For Information regarding Racism in Healthcare
Sources Used
0 notes
Text
Tuskegee Institute, Zelle, Meme History, More: Tuesday ResearchBuzz, November 14, 2023
NEW RESOURCES National Library of Medicine: Digitized Document Collection from USPHS Untreated Syphilis Study at Tuskegee Now Publicly Available Through NLM. “A collection of reproduced documents from the 1932 study by the U.S. Public Health Service (USPHS) on the effects of untreated syphilis in Black men at Tuskegee Institute is now available as a digitized collection through the National…
View On WordPress
0 notes
Text
There are federal employees paid at the local level in public health, though their employment structures vary depending on their roles and the programs they support. This arrangement typically occurs through federal assignments, cooperative agreements, or partnerships with state and local governments.
Key Examples of Federal Employees Working Locally:
Commissioned Corps of the U.S. Public Health Service (USPHS):
Officers are federal employees deployed to local health departments, tribal health organizations, or other public health entities.
They may serve in roles related to disease prevention, emergency response, or program implementation.
CDC Field Staff:
The Centers for Disease Control and Prevention (CDC) places epidemiologists, public health advisors, and other experts in state and local health departments.
These positions are part of programs like the Public Health Associate Program (PHAP) or specialized initiatives like the Epidemic Intelligence Service (EIS).
These individuals remain federal employees, but their work is carried out at the local level.
Health Resources and Services Administration (HRSA):
HRSA funds and deploys personnel to federally qualified health centers (FQHCs) and other local facilities.
While these individuals are often federally funded, they work closely with local public health and community health systems.
Indian Health Service (IHS):
IHS staff, including healthcare providers and public health professionals, work in tribal and urban Indian health facilities.
These employees are federal workers providing localized services.
Federal Emergency Assignments:
During emergencies (e.g., natural disasters, pandemics), federal employees from agencies like the CDC, FEMA, or ASPR (Assistant Secretary for Preparedness and Response) may be temporarily stationed at local health departments or response sites.
They are federally paid but work on local public health challenges.
Veterans Health Administration (VHA):
Some VHA employees collaborate with local public health agencies to address veteran-specific health issues, especially in rural or underserved areas.
0 notes