#Respiratory & Anesthesia Monitors
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr has 16.74 million mobile monthly users in the US.
Photo




(via Global Patient Monitoring Devices Market Size, Outlook 2024-2030) Global Patient Monitoring Devices and Accessories market, valued at US$63.4 billion in 2024, is projected to reach US$102.3 billion by 2030, growing at a CAGR of 8.3%. Market growth is driven by the rising prevalence of chronic diseases, technological advancements in AI, IoT, and sensor technology, and the increasing adoption of remote patient monitoring and home healthcare solutions. The demand for wearable health monitors and real-time data-driven care, especially for aging populations, continues to accelerate market expansion.
#patient monitoring#patient monitoring devices#patient monitoring accessories#patient monitoring devices market#patient monitoring market#Blood Glucose Monitors#Cardiac Monitors#Respiratory & Anesthesia Monitors#Blood Glucose Testing
0 notes
Text
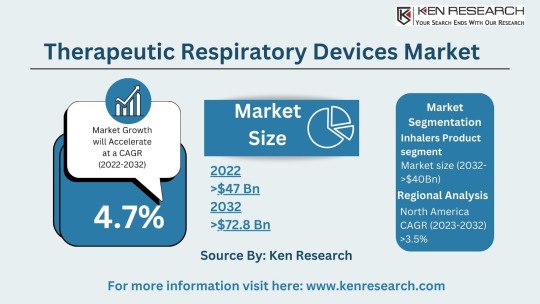
The $64.2 billion Respiratory Market & Its Future Trends, Segmentation and Forecast
The global respiratory market size reached a staggering USD 42.3 billion in 2023. This impressive figure highlights the significant need for respiratory devices and treatments to address a wide range of respiratory conditions. The market is projected to grow at a Compound Annual Growth Rate (CAGR) of approximately 7.4%, reaching an estimated USD 64.2 billion by 2030. This growth can be attributed to several factors:
Rising Prevalence of Chronic Respiratory Diseases: Conditions like asthma, chronic obstructive pulmonary disease (COPD), and sleep apnea are on the rise due to factors like air pollution, smoking, and an aging population.
Increased Life Expectancy: With an aging population, the demand for respiratory support devices for chronic conditions is expected to rise.
Technological Advancements: The development of innovative respiratory devices, such as portable nebulizers and advanced ventilators, offers improved treatment options.
Growing Focus on Homecare: The increasing emphasis on home-based care for respiratory patients fuels the demand for user-friendly respiratory devices.
Respiratory Market Segmentation: Catering to Diverse Needs
The respiratory market segmentation reflects the vast array of products and technologies available to address different respiratory needs:
By Application:
Therapeutic Respiratory Devices Market: This segment includes devices used for treatment, such as nebulizers, metered-dose inhalers (MDIs), and continuous positive airway pressure (CPAP) machines used for sleep apnea. The respiratory inhalers market is a significant sub-segment due to the widespread use of inhalers for asthma and COPD.
Anesthesia & Respiratory Devices: Specialized equipment used in surgical settings to deliver oxygen and maintain proper ventilation during anesthesia. The anesthesia and respiratory devices market caters to the specific needs of hospitals and surgical centers.
Respiratory Gas Analysis: This technology analyzes the composition of respiratory gases to assess lung function and identify potential respiratory issues.
By Device Type:
Respiratory Care Devices: This broad category encompasses various devices used for diagnosis, treatment, and monitoring of respiratory conditions. Examples include nebulizers, inhalers, ventilators, and CPAP (continuous positive airway pressure) machines.
Respiratory Monitoring Devices: These devices track vital signs such as blood oxygen levels and respiratory rate, allowing for continuous monitoring of patients with respiratory difficulties. The respiratory monitoring devices market is experiencing significant growth due to the increasing focus on patient safety and remote monitoring.
Respiratory Measurement Devices: These devices measure lung function and capacity, providing vital diagnostic information for respiratory conditions. The respiratory disease testing market relies heavily on these devices for accurate diagnosis.
Respiratory Protective Equipment (RPE): This equipment protects users from inhaling harmful substances, including masks and respirators. The respiratory protective equipment market is expected to witness growth due to rising concerns about air pollution and pandemics.
Take a look at: Forecasting the Respiratory Market, Size, Segmentation and Future Trends
Top Players in Respiratory Market: Breathing Innovation
Several established medical device manufacturers and specialty respiratory companies dominate the respiratory market:
Some of the top players in the respiratory market include:

Philips Healthcare
ResMed
Medtronic
GE Healthcare
Fisher & Paykel
Emerging Markets: A Rising Demand for Respiratory Solutions
Developing nations with growing populations and increasing healthcare expenditure present a significant opportunity. For instance, the bovine respiratory disease treatment market highlights the growing demand for respiratory solutions in the animal health sector.
Respiratory Market Trends: Shaping the Future of Respiratory Care
Exciting trends are shaping the respiratory market and transforming how we manage respiratory conditions:
Focus on Homecare Solutions: The emphasis on providing effective respiratory care solutions for patients in a home setting is driving innovation in portable and user-friendly devices.
Telemedicine Integration: Telehealth platforms allow remote monitoring and consultations with healthcare professionals, improving respiratory care management.
Connected Devices and Data Analytics: The integration of Internet of Things (IoT) technology allows for real-time data collection and analysis of respiratory parameters, leading to personalized treatment plans.
Emphasis on Early Detection and Prevention: The trend towards early detection and prevention of respiratory diseases through screening programs and lifestyle modifications is gaining momentum.
Challenges and Opportunities: Navigating the Respiratory Landscape
While the respiratory market offers promising opportunities, challenges also exist:
Challenges:
Cost Concerns: The high cost of some respiratory devices, particularly advanced equipment, can be a barrier to access for some patients.
Counterfeit Products: The presence of counterfeit respiratory products poses a safety risk and necessitates stringent quality control measures.
Compliance with Regulations: Navigating evolving regulatory requirements for medical devices can be complex and requires ongoing compliance efforts.
Opportunities:
Focus on Homecare: The trend towards homecare for respiratory patients creates a demand for portable and user-friendly respiratory devices.
Telemedicine Integration: Integrating respiratory monitoring devices with telemedicine platforms allows for remote patient monitoring and improved care coordination.
Emerging Technologies: The potential of new technologies like artificial intelligence and wearable devices can revolutionize respiratory care and diagnosis.
Respiratory Market Future Outlook: A Collaborative Approach
The respiratory market future outlook is promising, with a projected market size of USD 64.2 billion by 2030. And this suggests a market driven by innovation, collaboration, and a focus on improving patient outcomes. Here's what we can expect:
Collaboration between Medical Device Manufacturers and Healthcare Providers: Collaboration between these entities will be crucial for developing and implementing effective respiratory care solutions that address real-world clinical needs.
Increased Focus on Patient Education and Self-Management: Empowering patients with respiratory conditions to manage their health through education and user-friendly technology will be a key focus.
Conclusion:
The respiratory market plays a vital role in supporting lung health and improving the lives of millions suffering from respiratory illnesses. As the market continues to evolve, driven by innovation, collaboration, and a focus on patient-centric care, we can expect a future where managing respiratory conditions becomes more effective, accessible, and empowering for individuals and healthcare professionals alike.You can also read about: Future Forecast and Trends in the $35.58 Billion Respiratory Market
#Respiratory Market#Respiratory Industry#Respiratory Sector#Respiratory Market Size#Respiratory Market Segmentation#Respiratory Care Devices Market#Respiratory Devices Market#Therapeutic Respiratory Devices Market#Respiratory measurement devices market#respiratory gas analysis#anesthesia and respiratory devices market#respiratory disease testing market#bovine respiratory disease treatment market#respiratory inhalers market#respiratory monitoring devices market#respiratory protective equipment market#Top Players in Respiratory Market#Respiratory Market Trends#Respiratory Market Future Outlook
0 notes
Note
On your recent post for Vivisections
Do you have any more advice or maybe a quick scene lay out on how you'd accurately describe and show it? I've not seen many people explain this before I'd love to know more!
Permission to infodump?? awesome :D
Because it's on topic here, there are a few blogs I think need a mention because they have AMAZING medical/torture writing advice (@scripttorture and @justkidneying )
You didn't ask whether the character lives or dies, I don't know which you want so here's info on both scenarios:
Dying:
First off, without anesthesia, the pain alone would likely lead to a thing called Neurogenic Shock, which will in turn cause a BP drop and organ failure among other things. Your character will likely be breathing quickly, appear pale, have a rapid pulse, and be confused if they are still conscious. And yelling in pain of course.
For death due to blood loss: it's hard *not* to hit a major blood vessel if you're flaying someone open neck to groin, and that will also lead to quick death without immediate treatment. Cautery (using electricity to burn an area, stopping bleeding) will work on smaller bleeding but major blood vessels not so much. Symptoms are similar to shock: clammy/pale skin, thready/weak/rapid pulse, loss of consciousness.
Other: you can also risk damaging organs (someone being vivisected probably isn't going to be staying very still, even restrained, and one slip of a scalpel and oops, that's the aorta...) A punctured lung could lead to pneumo/hemothorax (air/blood in the chest cavity (pleural space), where it shouldn't be) causing respiratory distress—and then shock, and without treatment—death. If the heart is damaged, death would be near instant. Other organs like the liver, kidneys, bowels, spleen etc are pretty big bleeders, so see my Blood Loss section.
Sepsis: If they don't die immediately, sepsis is a big risk, as even in sterile environments you can't completely prevent it. Sepsis is when an infection reaches the bloodstream and is very serious. I imagine whoever is vivisecting the character probably wouldn't care too much about using sterile technique, so you can bet on an infection happening. This can set in within hours or days. Symptoms include high fever, pain, confusion/delirium, sweaty/clammy skin, low blood pressure.
Now, if you want them to live?
Surviving:
If the vivisectionist wants their patient/victim to survive, they'd need a lot of materials. Like any major surgery you'd need blood products, fluids, antibiotics, ligatures, and a way to keep the pain (somewhat) under control. Alcohol has been used in the past for similar procedures, but you could also just opt for a dose of opioids.
Antibiotics are necessary, opening someone up like that is a MAJOR risk (see "Sepsis").
I imagine they'd also somewhat monitor the character's vitals. They'd also probably have a few assistants to help with similar smaller tasks like that—stopping bleeding or handing tools, etc.
Closing the wound: Stitching someone up from such an event would be a lot of work, as you have to close many skin layers (muscle, fat, and the surface skin) and bandage it.
If you don't want to stitch them up immediately, a wound vac (negative pressure wound therapy) would be a good option. Doctors use these in cases of things like compartment syndrome. It is used when you cannot close someone back up right away.
Bandages and proper wound care are also important, you'd need to change the bandages every few hours for the first few days as deep wounds tend to produce a lot of fluids (called "exudate.") Sometimes doctors place drains to help drain away this fluid faster.
All in all, Healing from this would take months, not to mention the psychological trauma from all of this.
The scene:
Writing these scenes is honestly so variable so here's a few thoughts of mine:
You could describe the environment: (cliche, but cold metal table? Harsh lighting? Straps? A table with sharp scary-looking objects on it? How about the scent of disinfectant (or its absence).
The initial sensation would be the biggest to focus on: does the vivisectionist take their time? (pressure before pain?) shock as nerves fire as they are severed (lightning sensation shooting upwards), and the body’s instinctive flinch or freeze. Initially screaming, swearing? Sweating, rapid breathing, muscle spasms, or even vomiting as the body tries to cope?
Smells: Metallic tang of a large amount of blood (I personally HATE this smell, it's like having a penny in your mouth, or if you've ever used a metal scrubber to clean a pan, it smells kind of like that.), burning flesh (if they use cauterization) etc
If the character is partially sedated for it, keep in mind they will still react to pain, albeit sluggishly.
I hope this helps!
#whump#whump writing#whump scenario#whumpblr#whump community#medical whump#whump torture#medically accurate torture#tw torture#whumping#whumpee#physical whump#whump ideas#whump prompt#sick whump#whumplr
82 notes
·
View notes
Note
I don’t know if the prompts can be asking for more in stories you’ve already started, but I would love to see more of the Hero of Shadow and Wild Link interacting, or more on Abel’s heart attack in the HC AU, or more interactions with Zelda and Link after they had to get married (Golden Mercy? The Imprisoning War? Not sure what that one’s called). … Or basically anything involving hurt/comfort or Hyrule, honestly. 😂
I love your writing so much, thank you for sharing it with us! < 3
Hyrule snapped his fingers in front of his friend. “Wild!”
Wild blinked, flinching and taking a step back. “S-sorry—”
“You good? Was that another—I thought the meds—”
“No,” Wild shook his head. “I—it was—sorry, I just—he—”
Wild continued to stammer, at a loss for words. What was he supposed to say? He hadn't spaced out, he'd honed in, his mind had snapped with clarity, screaming at him and wanting nothing more than to run towards the stretcher.
That man—he was—
And he was having a—
"I-I just... need to sit down for a bit," Wild finally said, walking out of the ED.
Wild had yet to fully explain everything that had happened in his past. Everyone knew he had gaps in his memory, that he'd sustained a head injury, that it made him have absence seizures, but the cause of it... the people he'd left behind because of the aftermath...
How could Wild possibly ever explain? He'd failed in his mission, and it had gotten his entire team killed. He could never face anyone from his past, let alone his—
Castle Town had promised a new life, a new beginning, especially as memories had tried to piece themselves back together and make him want to run and hide all the more. If he told everyone... then there was no more running from it.
Wild buried his face in his hands, resting on an empty stretcher in the basement. His mind screamed with anxiety as his past caught up to the present, and his heart screamed with worry over his father.
This was a nightmare.
XXX
Fable looked over her room one more time. Ambu bag? Check. Suction? Check. Defibrillator? Check. She had her maintenance IV fluid set up, the plasmolyte liter set up, the wires for the cardiac monitoring system ready to go, chest tube suction at the ready, and her little trays had all the syringes, saline flushes, blunt tips, alcohol swabs, caps, lab tubes, and everything else she could think of prepared.
She'd chart stalked the patient while he was in the OR, and she'd already gotten report from the nurse. Forty-year-old male (oh he's young, Fable thought, used to seeing far older patients) presented to the ED via EMS with chest pain and shortness of breath, STEMI confirmed with EKG, and he was sent to the cath lab. There they found multiple severe occlusions and opted for an open heart bypass surgery rather than using stents, and off to the OR he'd gone.
The surgery had gone fairly straightforward from what she could see - he'd been on bypass for about an hour, and the surgery itself had been going on for about four. He'd gotten about 500 of cell saver, 2L crystalloid, and 1 RBC, and he'd only been defibrillated once.
Just as she looked over the chart again, roll call was sent out to the unit, and she gathered her thoughts as she went to the room, awaiting the patient. He arrived a minute or so later, and the room quickly filled with Fable, the charge nurse, the tech, another nurse, the anesthesiologist, the attending surgeon, the fellow surgeon, the respiratory therapist, the ICU attending, and the nurse practitioner.
Everyone slipped into different roles and tasks fairly easily and quickly. Anesthesia handed off to the RT, who attached the ET tube to his ventilator, the tech worked on putting chest tubes to suction and getting outputs, Fable assessed her patient and looked at what drips they were on (2 of epi, 4 of levo, 0.02 of vaso, 1.5 of Dex, 1.2 of insulin), charge took the admission note while the surgeons gave report and Fable listened vaguely, her other nurse was attaching the safe set to the arterial line to collect blood for labs and an ABG, and the ICU providers listened to the report.
Vasoplegia, not too much bleeding but enough to merit product, chest tube output was a little high but not alarming, and he was cold at 35.8. Fable asked her tech to get a bear hugger, and x-ray arrived to check ET placement as the surgeons finished report. Fable stripped the chest tubes alongside the surgical fellow before they all stepped out for x-ray. ABG resulted pH 7.33, pO2 107, CO2 38, bicarb 24, and lactate 3.1. Fable opened the extra plasmolyte fluid bolus up to try and help with the lactate, which was likely indicative that the patient was dry.
The surgery team left, and Fable remained to stabilize the patient. She and her charge nurse worked on detangling the lines while the tech covered him in a warm blanket. His blood pressure was within parameters, with a mean arterial pressure greater than 65, though his systolics were in the 120s, which was right at his upper limit, so she tried weaning the levo a little, going to 3 to see what would happen, before continuing to detangle lines, get a blood sugar for the glucommander that was determining the insulin levels to give him, and obtaining cardiac output indeces. His cardiac index was 2.8, and his systemic vascular resistance indexed for his body weight was around 2600. Good CI, a little higher on the SVRI end. Perhaps she should wean the epi too, assuming his MAP tolerated it.
After about an hour, Fable felt a little less overwhelmed, and she called her charge nurse, who had left the room a good while ago alongside the rest of the team. "Have we heard anything about family?"
"He has a wife and daughter," she replied. "But they're a fair distance from here, out in Hateno. I think last we heard they were making arrangements to get here, but it wouldn't be until tomorrow morning."
Fable glanced at the clock. It was almost shift change, so night shift would have to be the ones to wake the man up, get a neuro assessment, and then hopefully extubate him.
Nodding, she went back to work. She wasn't going to wean sedation until he was warm enough, so all she had to focus on right now was stabilizing him. His labs came back and his hemoglobin was a little low, and his two mediastinal and one pleural chest tubes collectively put out about 280mL of blood. It was still a fairly high amount, mostly evenly distributed (the meds were bleeding more, but neither exceeded 100mL for the hour), but not enough to think there was an active bleed that needed surgical intervention. Not yet, at least.
Overall, he looked pretty decent.
After another hour, one blood product later, Fable finally felt like she was starting to get everything settled. Her patient's temperature was normalizing, but she was twenty minutes from shift change, so she figured it was safer to let him sleep through report and then night shift could try to figure out weaning and bathing. His lactic on his repeat ABG was improving at 2.4, so they were likely addressing all the problems.
When a transporter walked by, IV pumps in hand, she noticed him pause in front of her room. She walked over to him. "Hey. Can I help you?"
The transporter, a young man with long blonde hair tied out of his face, jumped, a little startled. "Uh, hi. Yeah. Sorry. I just..."
"What room are you looking for?" she asked helpfully. "I don't need extra channels."
"Uh, these are for 4301."
"You passed it, it's back that way."
"Right," the man nodded, looking back in the room. "Right."
Fable waited a moment, and then asked, "Can I help you with anything else?"
"Is he doing okay?" the man immediately asked.
Fable smiled. "Yeah, he's looking pretty good, I think."
"Can..." the transporter swallowed, shifting anxiously. "Can I talk to him?"
"He's pretty sedated right now," Fable answered cautiously. "Why do you want to talk to him?"
The transporter sighed in defeat. "I... he's my dad. I... haven't seen him in a long time."
His dad? Her charge nurse had said he had a daughter, not a son. Though... looking between her patient and the transporter in front of her, the family resemblance was striking.
Well, she hadn't heard of any visitor restrictions for him. "Yeah. You're not on his chart, though - can I get your name?"
The transporter sighed, putting the supplies he'd been carrying on the counter of the nurse's station. "I wouldn't be on it. My family thinks I'm dead. It's complicated."
He—uh... what?
"My name's Link," he answered her nonetheless before entering her patient's room.
Link? Huh. That was...
Wait a second.
"Hey, are you one of my brother's friends?" Fable asked as she followed him into the room.
"Your brother?"
"Link. Likes to call himself Legend to differentiate," she replied with an amused roll of her eyes.
Link gawked at her. "You're Legend's sister? He never even said he had a sister!"
"You two are alike," Fable huffed. "He doesn't particularly want a bunch of people to know he's related to me. But never mind that. Go talk to your dad."
Link stood there a moment, processing the words, before he exhaled shakily and nodded. Fable moved to the computer, working on catching up on charting to give him some privacy but also keep an eye on things. This patient's safety was her responsibility, after all.
Link seemed almost timid to approach the patient, even though he knew he was sedated. He slowly slid his hand into the older man's, shakily and quietly saying, "Hey, Papa. I... I, uh... I-I..."
Fable glanced out of the corner of her eye, seeing the young man getting tearful, and she tried to focus on her work once more.
"I missed you," Link whispered. "I'm s-sorry... about... about everything."
She heard a sniffle, and then the transporter moved quickly out of the room, offering her a brief but quick thanks before disappearing.
Fable turned towards the doorway, and then looked at her patient uncertainly. That was... odd.
Sighing, she walked up to the man, brushing hair out of his face. "Buddy, your family drama sounds almost as crazy as mine."
#you ask skye answers#lovely webhead#don't worry Abel's doing fine lol#Wild on the other hand...#writing#lu in healthcare#lu wild#abel#lu fable
90 notes
·
View notes
Text
Cardiophile Turn On/Off
I got this from @/heartbinary who got it from @/torture-steth-repeat
I wanted to do it myself to not only have some boundaries but also so people can get to know me a tad bit better
💚 = Turn on
💔 = Turn off
🤍 = Neutral/Like it in a non-sexual way
Section 1: Cardiophilia basics
1. My heart being listened to: 💚
2. Listening to others' hearts: 💚
3. Fast heartbeats: 💚
4. Slow heartbeats: 🤍
5. Naturally irregular heartbeats: 💚
6. Deliberately irregular heartbeats: 💚
7. Heart via stethoscope: 💚
8. Heart via EKG: 💚
9. Heart via Doppler: 🤍
10. Heart via ultrasound: 💚
11. Carotid (throat) pulse: 💚
12. Femoral (groin) pulse: 🤍
13. Radial (wrist) pulse: 🤍
14. Chest/belly pulse: 💚🤍
15. Ear stething: 💚
Section 2: Dark Cardiophilia
1. Shocking a healthy heart: 💚
2. Pressure/crushing a healthy heart: 💚
3. Drowning + heart monitoring: 💚
4. Suffocation + heart monitoring: 💚
5. Choking + heart monitoring: 💚
6. Drugs used to affect the heart: 💚
7. Knifeplay + heart monitoring: 💚
8. Needle or injection into the heart: 💚
9. Gunplay (shooting the heart): 💚
10. Being dominated (in a cardiophilia way): 💚
11. Dominating someone else (in a cardiophilia way): 💚
12. Consensual non-consent (CNC) play: 🤍
13. Heart rips: 💔
14. Fucked into cardiac arrest: 💚
15. Heart being fucked: 🤍
16. Heart being licked or bitten: 🤍
17. Heart being eaten: 🤍
18. Hands squeezing the heart directly: 💚
19. 'Unhappy endings' (RIP) for dark cardiophilia: 💔
Section 3: Medfet/Resus
1. Blood pressure readings: 💔
2. Medical equipment: 🤍
3. Medical exam roleplay: 🤍
4. Resuscitation via CPR: 🤍
5. Resuscitation via defibrillator: 🤍
6. Resuscitation via AED: 🤍
7. Cardiac arrest: 💚
8. Respiratory arrest: 🤍
9. Sex and resus combined: 💔
10. 'Unhappy endings' (RIP) for resus: 💔
11. Anesthesia: 💔
12. Breathing masks: 🤍
Section 4: Graphic
1. Open heart surgery footage: 💚
2. Real animal hearts: 💔
3. Real human hearts outside the body: 💚
4. Real human hearts in autopsies: 🤍
Section 5: Adjacent Kinks
1. Gyno medical exams: 💔
2. Pregnancy/breeding: 🤍
3. Belly sounds: 💔
4. Cardiophilia + furry: 💚
5. Vampires: 🤍
6. Necrophliia: 💔
Section 6: 😏
1. Reading someone's bio before engaging with them: 💚
2. Asking about boundaries: 💚
3. Respecting those boundaries: 💚
4. Good spelling: 🤍
#i hope i did this right lmao#cardiophilia#cardiophile#roxie speaks#heartbeat kink#heartbeat#dark cardiophilia
47 notes
·
View notes
Text
Cardiophile Turn On/Off
I saw this going around, I think the original is from @/torture-steth-repeat ! I thought it was a good way to sum up my interests😊
OKAY SO the original said turn on/turn off! But because some of my fixations are both sexual and not sexual I've changed it to:
💚 = I like this
💔 = I don't like this
🤍 = I don't mind this
Section 1: Cardiophilia basics
1. My heart being listened to: 💚
2. Listening to others' hearts: 💚
3. Fast heartbeats: 💚
4. Slow heartbeats: 💚
5. Naturally irregular heartbeats: 🤍
6. Deliberately irregular heartbeats: 💔
7. Heart via stethoscope: 💚
8. Heart via EKG: 💚
9. Heart via Doppler: 💚
10. Heart via ultrasound: 💚
11. Carotid (throat) pulse: 💚
12. Femoral (groin) pulse: 💚
13. Radial (wrist) pulse: 💚
14. Chest/belly pulse: 💚
15. Ear stething: 💚
Section 2: Dark Cardiophilia
1. Shocking a healthy heart: 💔
2. Pressure/crushing a healthy heart: 💔
3. Drowning + heart monitoring: 💔
4. Suffocation + heart monitoring: 💔
5. Choking + heart monitoring: 💔
6. Drugs used to affect the heart: 💔
7. Knifeplay + heart monitoring: 🤍
8. Needle or injection into the heart: 💔
9. Gunplay (shooting the heart): 💔
10. Being dominated (in a cardiophilia way): 💚
11. Dominating someone else (in a cardiophilia way): 💚
12. Consensual non-consent (CNC) play: 🤍
13. Heart rips: 💔
14. Fucked into cardiac arrest: 💔
15. Heart being fucked: 💔
16. Heart being licked or bitten: 💔
17. Heart being eaten: 💔
18. Hands squeezing the heart directly: 🤍
19. 'Unhappy endings' (RIP) for dark cardiophilia: 💔
Section 3: Medfet/Resus
1. Blood pressure readings: 🤍
2. Medical equipment: 💚
3. Medical exam roleplay: 💚
4. Resuscitation via CPR: 🤍
5. Resuscitation via defibrillator: 💔
6. Resuscitation via AED: 💔
7. Cardiac arrest: 💔
8. Respiratory arrest: 💔
9. Sex and resus combined: 💔
10. 'Unhappy endings' (RIP) for resus: 💔
11. Anesthesia: 🤍
12. Breathing masks: 🤍
Section 4: Graphic
1. Open heart surgery footage: 🤍
2. Real animal hearts: 🤍
3. Real human hearts outside the body: 🤍
4. Real human hearts in autopsies: 💔
Section 5: Adjacent Kinks
1. Gyno medical exams: 💚
2. Pregnancy/breeding: 💔
3. Belly sounds: 💚
4. Cardiophilia + furry: 🤍
5. Vampires: 💚
6. Necrophliia: 💔
Section 6: 😏
1. Reading someone's bio before engaging with them: 💚
2. Asking about boundaries: 💚
3. Respecting those boundaries: 💚
4. Good spelling: 🤍
11 notes
·
View notes
Text
Cardiophile Turn On/Off
I got this from @torture-steth-repeat
💚 = Turn on
💔 = Turn off
🤍 = Neutral/Like it in a non-sexual way
Section 1: Cardiophilia basics
1. My heart being listened to: 💚
2. Listening to others' hearts: 💚
3. Fast heartbeats: 💚
4. Slow heartbeats: 🤍
5. Naturally irregular heartbeats: 💚
6. Deliberately irregular heartbeats: 💚🤍
7. Heart via stethoscope: 💚
8. Heart via EKG: 💚
9. Heart via Doppler: 💔
10. Heart via ultrasound: 🤍💚
11. Carotid (throat) pulse: 🤍
12. Femoral (groin) pulse: 🤍
13. Radial (wrist) pulse: 🤍
14. Chest/belly pulse: 🤍
15. Ear stething: 💚
Section 2: Dark Cardiophilia
1. Shocking a healthy heart: 💔
2. Pressure/crushing a healthy heart: 💚
3. Drowning + heart monitoring: 💔
4. Suffocation + heart monitoring: 💔
5. Choking + heart monitoring: 💔
6. Drugs used to affect the heart: 💚🤍
7. Knifeplay + heart monitoring: 💔
8. Needle or injection into the heart: 💔
9. Gunplay (shooting the heart): 💔
10. Being dominated (in a cardiophilia way): 💚
11. Dominating someone else (in a cardiophilia way): 💚🤍
12. Consensual non-consent (CNC) play: major turn-on 💔
13. Heart rips: 💔
14. Fucked into cardiac arrest: 💔
15. Heart being fucked: 💔
16. Heart being licked or bitten: 💔
17. Heart being eaten: 💔
18. Hands squeezing the heart directly: 💔
19. 'Unhappy endings' (RIP) for dark cardiophilia: 💔
Section 3: Medfet/Resus
1. Blood pressure readings: 🤍
2. Medical equipment: 🤍💚
3. Medical exam roleplay: 💚
4. Resuscitation via CPR: 💔
5. Resuscitation via defibrillator: 💔
6. Resuscitation via AED: 💔
7. Cardiac arrest: 💔
8. Respiratory arrest: 💔
9. Sex and resus combined: 💔
10. 'Unhappy endings' (RIP) for resus: 💔
11. Anesthesia: 🤍
12. Breathing masks: 🤍
Section 4: Graphic
1. Open heart surgery footage: 🤍
2. Real animal hearts: 💔
3. Real human hearts outside the body: 🤍
4. Real human hearts in autopsies: 💔
Section 5: Adjacent Kinks
1. Gyno medical exams: 💔
2. Pregnancy/breeding: 💔
3. Belly sounds: 💔
4. Cardiophilia + furry: 🤍💚
5. Vampires: 🤍💚
6. Necrophliia: 💔
Section 6: 😏
1. Reading someone's bio before engaging with them: 💚
2. Asking about boundaries: 💚
3. Respecting those boundaries: 💚
4. Good spelling: 💚
#cardiophile#cardiophilia#heartbeat#heartbeat kink#fast heartbeat#pounding heart#irregular heartbeat
26 notes
·
View notes
Text
⋆ ˚。⋆୨୧˚⋆ ˚。⋆ About Me Cardiophilia ⋆ ˚。⋆୨୧˚⋆ ˚。⋆
(Saw this on few other blogs when clicking around. It looks like, torture-seth-repeat , created this! All credit goes to them, check out their blog for it)
𐙚 Cardiophilia Basics 𐙚
My heart being listened to: Yes, please!
Listening to others' hearts: Yes
Fast heartbeats: Yes
Slow heartbeats: Yes
Naturally irregular heartbeats: Yes
Deliberately irregular heartbeats: Yes
Heart via stethoscope: Yes, please!
Heart via EKG: Yes
Heart via Doppler: Yes, please!
Heart via ultrasound: Yes, please!
Carotid (throat) pulse: Yes, please!
Femoral (groin) pulse: Yes
Radial (wrist) pulse: Yes
𐙚 Dark Cardiophilia 𐙚
Shocking a healthy heart*: Sometimes
Pressure/crushing a healthy heart: Yes
Drowning + heart monitoring: Yes
Suffocation + heart monitoring: Yes
Choking + heart monitoring: Yes, please!
Drugs used to affect the heart: Yes
Knifeplay + heart monitoring: Yes, please!
Needle or injection into the heart: Yes
Gunplay (shooting the heart)*: Yes
Being dominated (in a cardiophilia way): Yes, please!
Dominating someone else (in a cardiophilia way): No way!
Consensual non-consent (CNC) play: Yes, please!
Heart rips*: Sometimes
Fucked into cardiac arrest*: Yes, please!
Heart being fucked*: Yes
Heart being licked or bitten*: Yes
Heart being eaten*: Sometimes
Hands squeezing the heart directly*: Yes, please!
'Unhappy endings' (RIP) for dark cardiophilia*: Sometimes
𐙚 Medfet/Resus𐙚
Blood pressure readings: Yes
Medical equipment: Yes, please!
Medical exam roleplay: Yes, please!
Resuscitation via CPR*: Sometimes
Resuscitation via defibrillator*: Sometimes
Resuscitation via AED*: Sometimes
Respiratory arrest*: Yes
Sex and resus combined: Sometimes
'Unhappy endings' (RIP) for resus*: Sometimes
Anesthesia*: Sometimes
Breathing masks: Yes, please!
𐙚 Graphic𐙚
Open heart surgery footage: Yes
Real animal hearts: No Way!
Real human hearts outside the body: Yes
Real human hearts in autopsies: Yes
𐙚 Adjacent Kinks𐙚
Gyno medical exams: Sometimes
Pregnancy/breeding: Yes, please!
Belly sounds: Yes
Cardiophilia + furry: No way!
Vampires*: Sometimes
Necrophliia*: No way!
* fantasy/RP only
31 notes
·
View notes
Text
About Me
Welcome to my blog!
18+ / MINORS DNI
I'm Luna, 24, queer, demigirl, healthcare worker.
YES: light cardiophilia, medfet, gyno, d/s, dd/lg, md/lg, cnc, enemas, breeding, impregnation, breath play, virgin, anal, restraint, voyeurism, sounding, tentacles, oviposition, depth play, lactation, belly bulge, fisting, somno, pet play, mild intoxication (weed, mild sedatives/anxiolytics), knotting, omo (holding only, no wetting), humiliation, light needle play, praise, and sensory deprivation.
NO: resus, dark cardiophilia, necro, furry, scat, anaesthesia, surgery, knife play, degradation, dumbification.
I don't share pictures of myself so don't ask and I don't want to see pictures of you without preamble, either. I don't share my heartbeat unless I choose to, either, so don't ask. If I want to listen to your heartbeat, I'll ask. I don't role play or engage in virtual exams unless I feel like it and I don't do so with complete strangers that I've never talked to before. Just because I'm a kink blog doesn't mean I'm here to fulfill your fantasies or be treated like an object. I'm lots of fun and love to chat but I don't put up with rude or gross behavior. Show a little respect and we'll get along just fine. ♥
Click through the read more for my preferences and feel free to send an ask or DM if you have questions or want to say hello!
XoXo
credit goes to @torture-steth-repeat for this template
Cardiophilia Basics
1. My heart being listened to: yes
2. Listening to others' hearts: sometimes
3. Fast heartbeats: sometimes
4. Slow heartbeats: yes
5. Naturally irregular heartbeats: yes
6. Deliberately irregular heartbeats: hard no
7. Heart via stethoscope: yes
8. Heart via EKG: yes
9. Heart via doppler: yes
10. Heart via ultrasound: yes
11. Carotid (throat) pulse: yes
12. Femoral (groin) pulse: yes
13. Radial (wrist) pulse: yes
Dark Cardiophilia
1. Shocking a healthy heart: hard no
2. Pressure/crushing a healthy heart: hard no
3. Drowning + heart monitoring: only in fiction
4. Suffocation + heart monitoring: only in fiction
5. Choking + heart monitoring: only in fiction
6. Drugs used to affect the heart: hard no
7. Knifeplay + heart monitoring: hard no
8. Needle or injection into the heart: hard no
9. Gunplay (shooting the heart)*: hard no
10. Being dominated (in a cardiophilia way): yes
11. Dominating someone else (in a cardiophilia way): sometimes
12. Consensual non-consent (CNC) play: yes
13. Heart rips*: hard no
14. Fucked into cardiac arrest*: hard no
15. Heart being fucked*: hard no
16. Heart being licked or bitten*: hard no
17. Heart being eaten*: hard no
18. Hands squeezing the heart directly*: hard no
19. 'Unhappy endings' (RIP) for dark cardiophilia*: hard no
Medfet/Resus
1. Blood pressure readings: yes
2. Medical equipment: yes
3. Medical exam roleplay: yes
4. Resuscitation via CPR*: hard no
5. Resuscitation via defibrillator*: hard no
6. Resuscitation via AED*: hard no
7. Cardiac arrest*: hard no
8. Respiratory arrest*: hard no
9. Sex and resus combined: hard no
10. 'Unhappy endings' (RIP) for resus*: hard no
11. Anesthesia*: hard no
12. Breathing masks: hard no
Graphic
1. Open heart surgery footage: hard no
2. Real animal hearts: hard no
3. Real human hearts outside the body: hard no
4. Real human hearts in autopsies: hard no
Adjacent Kinks
1. Gyno medical exams: yes
2. Pregnancy/breeding: yes
3. Belly sounds: no
4. Cardiophilia + furry: no
5. Vampires*: sometimes
6. Necrophliia*: hard no
45 notes
·
View notes
Text
Bedside Monitors Explained: Functions, Advantages, and Cost Considerations

How do Bedside Monitor Work?
Bedside monitors are essential medical devices designed to continuously track a patient's vital signs in real time. They work by using various sensors and electrodes to capture critical physiological data such as heart rate, blood pressure, oxygen saturation (SpO₂), respiratory rate, and sometimes temperature and other parameters, depending on the model.
The monitor is equipped with multiple sensors or probes that are attached to the patient’s body. Once connected, these sensors continuously send data to the bedside monitor. The device processes the data through algorithms to provide accurate, real-time readings.
The monitor displays the data on a screen, often with individual panels for each parameter. The display is typically bright and easy to read, allowing quick assessment. Monitors are usually set up with alarms to alert caregivers if a reading falls outside of a safe range.
Modern bedside monitors can store data over time for trend analysis and are often connected to a central monitoring system.
Bedside monitors play a critical role in patient care by offering accurate, continuous observation, especially in intensive care, emergency departments, and during surgeries.
What are they used to bedside monitor?
Bedside monitors are used to continuously observe and measure a patient's vital signs, providing essential information for healthcare providers to make informed decisions. Here are some common applications scene for bedside monitors:
Intensive Care Units (ICU): Bedside monitors are crucial in ICUs. They track key metrics such as heart rate, respiratory rate, blood pressure, and oxygen saturation, alerting staff to any changes that may need immediate attention.
Emergency Departments (ED): In emergency settings, bedside monitors are used to assess patients quickly and monitor their stability. They provide real-time data, helping emergency physicians make fast, informed decisions during critical moments.
Operating Rooms (OR): During surgeries, bedside monitors track a patient’s vital signs to ensure they remain stable under anesthesia.
Post-Operative Recovery: After surgery, patients are often monitored until they stabilize.
General Wards and Step-Down Units: Bedside monitors help track vital signs as patients wake from anesthesia and recover, ensuring they respond well and identifying any potential complications.
These monitors allow medical staff to intervene quickly and improve patient outcomes across various medical environments.
What are bedside patient monitors expensive?
Bedside monitors are highly beneficial in healthcare settings due to their ability to provide real-time, continuous monitoring of a patient’s vital signs. Here are some key benefits:
Enhanced Patient Safety: Bedside monitors often include alarms to alert medical staff if any parameter goes beyond a safe range.
Improved Efficiency for Medical Staff: Continuous monitoring reduces the need for frequent manual checks by nurses or doctors, freeing up their time for other patient care tasks.
Better Data for Informed Decision-Making: Bedside monitors collect data over time, allowing healthcare providers to analyze trends and make more informed treatment decisions.
Enhanced Recovery and Post-Operative Care: Any post-operative complications can be detected and addressed promptly, improving recovery outcomes.
Are bedside patient monitor expensive?
The cost of bedside patient monitors can vary widely depending on the monitor’s features, complexity, and brand. Here are some factors that influence bedside patient monitors' price: Features and Functionality, Display Quality and Size, Technology and Connectivity, Durability and Portability
Basic bedside monitors can range from a few hundred to a few thousand dollars. While the upfront cost of bedside monitors can be high, they are considered a valuable investment because they help prevent complications, improve patient outcomes, and enhance workflow efficiency. Many healthcare providers consider the long-term benefits and cost savings in patient care when deciding on the investment.
Know More>>https://www.daweimed.com/Patient-Monitoring.html
5 notes
·
View notes
Text
Jägermeister
Chapter Nineteen: Rivalry
“That was not Newt Oji-chan.”
“Of course it wasn't,” said Hermann. His voice was rough, but not from being choked. Newton had barely started to squeeze before he was restrained by medical staff. “He didn't speak.”
They were on the flight back to the Hong Kong Shatterdome, Newton sedated and restrained to a gurney only a meter away.
By the time they reached the Shatterdome, the Four Seasons Hangzhou had forwarded the results of Newton’s MRI. All those top-dollar doctors, and all they were able to discern conclusively was that the swelling in his brain had become so severe that it was pressing up against his skull.
Newton was placed in a medically-induced coma until the encephalitis could regress. The doctors administered anesthesia, monitoring his brain activity via EEG until it reached the target level. The anesthetic suppressed his respiratory drive, so he also had to be intubated.
They all took shifts watching over him, even though he had a dedicated medic with him at all times. Marshal Hansen himself took the first shift, after ordering them all to take naps, or at least showers. Hermann took the second shift after doing neither. Tendo supplied the coffee.
A day passed, and the swelling did not go down.
Eddie the medic attempted to distract them all with photographs of his gravid gecko in her nesting box. He had decorated it with a miniature banner that read, “It’s a gecko!”
Another day passed, and the swelling did not go down.
Dr. Lightcap came out of retirement to consult, and while Hermann had once been accused of going ‘full fangirl’ by Newton when they heard her speak at a conference in 2021, he now found himself unjustly frustrated with her for not having any answers either.
Another day passed, and the swelling did not go down.
Dr. Lightcap recommended a controlled drift.
It was theoretically possible to establish a neural link despite the anesthesia, though it had never been attempted before. Many medically-induced coma patients reported vivid dreams, interpreting their surroundings through a surreal filter. Some believed they were taking part in the conversations carried on over their head. Others experienced the application of ice packs as nightmares about going down with the Titanic.
At first, Hermann was vehemently opposed to Dr. Lightcap’s recommended treatment. It seemed too much like what had been done to Newton in captivity, but he knew that was not entirely accurate. They would not be forcing Newton to drift with a kaiju. They would be forcing him to drift with Hermann.
It was with some trepidation that Hermann donned the squid cap and listened to Dr. Lightcap count down from three.
The hive mind felt almost omnipresent. Everything shone with the heat shimmer of an orange sun, dark at the center, like the theoretical ‘dark star’ of Newtonian mechanics. Everything echoed with their clicking, like a million ticking War Clocks. Everything hissed.
Newton’s presence in his own mind was little more than a whisper, but Hermann followed that whisper as though it was played by Pied Piper.
He saw more of Newton’s memories. Getting all As. Getting a few Bs on purpose to fit in better. Getting nearly waterboarded, by several boys significantly his senior, in an MIT toilet stall, if the graffiti on the door was anything to go by. Hermann hadn’t even known ‘swirlies’ existed in real life, let alone at a private institute of higher learning, even if it was American.
Then he saw a rabbit.
Hermann did not see a Random Access Brain Impulse Trigger.
He saw Bugs Bunny.
“What’s up, Doc?” asked Bugs, a carrot sticking out of his mouth like it was a stogie.
“I beg your pardon?” asked Hermann, more out of habit than anything else.
Bugs Bunny suddenly cocked his head to the side, one ear perfectly erect.
Hermann could hear something too, just the barest strains of music rising over all the clicking and hissing. It was Wagner. A piece from Die Walküre.
Bugs Bunny turned and started to follow the music.
So Hermann followed the rabbit.
Bugs ducked into a bulkhead style corridor that twisted, turned, and forked before letting out into a theater. It was a gorgeous auditorium, with a proscenium stage, red velvet curtains, and a grand chandelier. The seats were all empty, but a woman was performing onstage.
Hermann recognized her as Newton’s mother, Monica Schwartz. Her photograph had been easier to come by than Newton’s own when their correspondence first started. She looked too beautiful to be fully real, and Hermann knew that was because Newton remembered her primarily from photographs as well.
Her voice was equally beautiful, but there was a very insistent part of Hermann that hated it with an intense and fiery passion.
Bugs Bunny began applauding loudly even though the piece was nowhere near completion. When Hermann turned to look at him, Bugs shrugged and said, "Well, what did you expect in an opera? A happy ending?"
Then he played dead, performing a teetering twirl on the spot before falling over in full rictus. When Hermann continued to stare at him, Bugs cracked open one eye, and pointed an ear towards the stage. “I think Brünnhilde is up there. Watch out for the flames though. This whole place is burning.”
Even Hermann could follow a cue so overt. He climbed the steps onto the stage, where he was thoroughly ignored by Monica Schwartz. The backstage led to another bulkhead passage, this time with only one egress.
Hermann emerged in a small room. It was sparsely furnished, but heavily decorated. The walls were covered with photographs, documents, and handwritten notes, all connected by red string tied around push pins like some sort of particularly intricate spider’s web.
The photographs were all of Hermann. The documents were his academic papers. The handwritten notes were unmistakably his correspondence with Newton.
Newton was in the middle of it all, standing on both a chair and the tips of his toes to add more string. A row of pushpins was held between his pursed lips and he was humming, more or less along with the Wagner, but at twice its actual tempo.
“Newton!”
He startled, spitting pins and nearly falling off his chair.
“Christ on a cock, Hermann! What are you doing here?”
“I'm here to save you,” said Hermann, like a complete prat.
Newton rolled his eyes, which were not shot with blood the way they were in the real world. Hermann wondered if he even knew how badly he had been hurt.
“That's…. great. The NPCs have developed free will, and I have apparently developed a damsel-in-distress complex. I appreciate the initiative, Ghost Hermann. I really do, but I don't think you can do anything I can do better. I'm supposed to be in charge here, at least if you listen to the Existentialists. Although I don't think either one of us likes them.”
Hermann had tuned out, more or less on instinct, after ‘NPC,’ but he got the gist. Newton thought he was a figment of his imagination. Hermann might have corrected this misapprehension if he wasn’t so distracted by the decor.
“What is this place?”
Newton winced. “Wow, this is just as humiliating as I always imagined, even though neither of us is a real boy. Still, I guess it beats talking to myself. I do a pretty good Hermann, if I don't mind me saying so.”
“So, this is…” Hermann knew there were more important topics of conversation, but it was difficult to focus on anything else when he was looking at a photograph of himself offering Mako-chan his fifth attempt at omurice, complete with a crooked ketchup smile drawn on top to match his own.
Hermann was reasonably certain no such photograph existed in the real world. Newton had attempted to take one, but Hermann had confiscated his phone in protest. Apparently, he had captured it in his memory instead.
Newton referred to his memory as ‘semi-eidetic,’ but Hermann had always argued that ‘selectively-eidetic’ would be more apt.
Apparently, he had selected Hermann.
Repeatedly.
There were photographs of Hermann writing on his chalkboards, drinking Jägermeister, arguing. There was a photograph of the day they met, before it all went wrong. There was another one of the day they drifted, before it all went wrong again.
“This is the Hermann Cave! The real you wouldn't get that, so pretend you don't, for authenticity’s sake.”
Hermann didn't have to pretend.
“I made this room to hide from the Precursors. I mean, sure, technically they know exactly where to find me, but they don't like coming here. It’s not even because of Mom— She’s just the perimeter guard. I mean, don’t get me wrong, they hate opera, but it turns out there's something they hate even more.”
“Oh?”
“Love,” said Newton. “They hate love! They’re not even homophobic. They hate all love equally. See I've got sections for Dad, Uncle Illia, Mako-chan, and the Frog Formerly Known as Prince, may he rest in peace. So sure, Hermann Cave is technically a misnomer, but it’s also hilarious.”
Surely enough, the pictures on the wall did seem to include several photos of Mako by herself, Jacob and Illia Geiszler, and an African Dwarf Frog.
“They really hate the romantic kind though,” Newton was saying, “and they really, really hate the sappy, song-writing, decades-of-pining kind I've got for you. I’ve been trying to figure out exactly why love is such an anathema for the Precursors. My working hypothesis is that they can’t comprehend sacrifice for something that’s not a part of themselves. Don’t quote me on that though. It might just be like Kryptonite.”
“Oh,” said Hermann. “Oh.”
Before he could say anything else, he was forcibly ejected from the drift. Everything seemed to freeze, like a lagging computer, and then he was back in the Medical Bay of the Hong Kong Shatterdome, surrounded by anxious faces.
“Your heart-rate spiked,” said Tendo. “Like, a lot.”
It took Hermann a moment to catch his breath, and even then, all he could manage to say was, “Yes, I imagine it did.”
...
@lastdaysofwar
3 notes
·
View notes
Text
Turn-Ons & Turn-Offs Cardiophile Edition
Got this list from @torture-steth-repeat
Section 1: Cardiophilia Basics
My heart being listened to: Major Turn-on
Listening to others' hearts: Major Turn-on
Fast heartbeats: Major Turn-on
Slow heartbeats: Turn-on
Naturally irregular heartbeats: Major Turn-on
Deliberately irregular heartbeats: Major Turn-on
Heart via stethoscope: Major Turn-on
Heart via EKG: Major Turn-on
Heart via Doppler: Turn-on
Heart via ultrasound: Major Turn-on
Carotid (throat) pulse: Turn-on
Femoral (groin) pulse: Meh
Radial (wrist) pulse: Meh
Section 2: Dark Cardiophilia
Shocking a healthy heart*: Major Turn-on
Pressure/crushing a healthy heart*: Major Turn-on
Drowning + heart monitoring*: Major Turn-on
Suffocation + heart monitoring*: Major Turn-on
Choking + heart monitoring: Meh
Drugs used to affect the heart*: Major Turn-on
Knifeplay + heart monitoring*: Major Turn-on
Needle or injection into the heart*: Major Turn-on
Gunplay (shooting the heart)*: Turn-on
Being dominated (in a cardiophilia way)*: Major Turn-on particularly by men
Dominating someone else (in a cardiophilia way)*: Major Turn-on particularly on men
Consensual non-consent (CNC) play*: Major turn-on
Heart rips*: Meh
Fucked into cardiac arrest*: Major turn-on
Heart being fucked*: Major turn-on
Heart being licked or bitten*: Turn-on
Heart being eaten*: Turn-off
Hands squeezing the heart directly*: Major Turn-on
'Unhappy endings' (RIP) for dark cardiophilia*: Major Turn-off
Section 3: Medfet/Resus
Blood pressure readings: Meh
Medical equipment: Major Turn-on
Medical exam roleplay: Major Turn-on
Resuscitation via CPR*: Major Turn-on
Resuscitation via defibrillator*: Major Turn-on
Resuscitation via AED*: Turn-on
Cardiac arrest*: Major Turn-on
Respiratory arrest*: Turn-on
Sex and resus combined*: Major Turn-on
'Unhappy endings' (RIP) for resus*: Turn-off
Anesthesia*: Meh
Breathing masks: Meh
Section 4: Graphic
Open heart surgery footage: Turn-on but depends on case by case basis
Real animal hearts: Major Turn-off
Real human hearts outside the body*: Turn-on but depends on scene and case by case basis
Real human hearts in autopsies: Major Turn-off
Section 5: Adjacent Kinks
Gyno medical exams: Turn-off
Pregnancy/breeding: Turn-off
Belly sounds: Meh
Cardiophilia + furry: Turn-on
Vampires*: Turn-on
Necrophilia*: Major Turn-off
Section 6: 😏
Reading someone's bio before engaging with them: Major Turn-on
Asking about boundaries: Major Turn-on
Respecting those boundaries: Major Turn-on
Good spelling: Turn-on *fantasy/RP only
86 notes
·
View notes
Text
Ok Wild Angsters, you wanted a continuation, so here you go :)
Four already knew what he would be walking into. His phone had been blowing up for hours. He’d come in to work early. Whether he was assigned to take care of Wild or not was another matter - Vaati loved to try and take all the admissions, convinced he was the best nurse on the unit. If Four could just keep Vaati out of Wild’s room, he’d consider it a success.
When the charge nurse told him he would be admitting the trauma alert, he knew who he was getting.
Pre-admission jitters always made Four anxious, but this was an entirely other level of fear. He almost wanted to request a different assignment, but it was too late now. What if he couldn’t take caer of him because he was his friend? What if that impair his decision making? What if he just wasn’t skilled enough to handle it? He knew Ezlo wouldn’t give him an assignment he couldn’t handle, wouldn’t be there to support him, but still…
Four went over the supplies in his room once more. Safety checks were fine—they had suction, they had a bag valve mask, the code card was nearby—and he had all the supplies he needed. It was just a waiting game.
Four paced the unit at least three times before he looked at the OR status board again. Wild was still in surgery. He poked in his chart, glancing at injuries, looking at vital signs and anesthesia notes. The last update he saw was that Wild had gotten another unit of blood. Estimated blood loss so far was around 2200mL.
2200mL. That… wasn’t too terrible, Four supposed. He’d… seen worse.
Please don’t get worse.
Four knew for certain that Wild had been mass transfused in the ED. Warriors, his primary nurse when he was there, had told him as much. Between that and the multiple blood products he’d gotten in surgery, as well all the crystalloids he was likely getting as well…
Four took a breath. Then another. He grabbed his phone, texting Warriors. You doing ok?
Wars didn’t reply.
Four wasn’t entirely sure where everyone was at this point. Hyrule had stayed at the hospital, lingering in the emergency department and then the operating room waiting area, but Four hadn’t seen him since he’d clocked in. Warriors and Legend should be getting off shift now, but whether they were going to stay up was another matter. Time was obviously in the OR (Wild’s wreck had been around 10pm, he’d arrived in the ED around 10:45, and he’d been stabilized for surgery and gone to the OR by around midnight - it was 7am now… he wasn’t sure how long this was going to take, but it couldn’t be much longer). Malon should be getting on shift now as well - she had come in last night when everything had gone down, alongside Twilight. Wind had been cautiously left out of the loop until Wild had gone to surgery, simply because nobody had really had much information at the time, so no one wanted to worry the kid until they could figure things out. Everyone had their hands full as it was. But by now, Four knew Wind was either in the OR waiting room, harassing every respiratory therapist he knew, or in the hospital library pacing anxiously. As for Sky, the last Four heard he was bouncing between different people, checking in on everyone.
He clicked through more anesthesia notes, looked at flow sheets for blood products. There wasn’t much to go on, as charting was sparse. What Four did know was that Wild had been obtunded, got mass transfused, had gotten a chest tube, had been intubated, blood was evident in his abdomen, and he had an open femur fracture. He’s been taken to Time’s OR for a ex-lap. Head CT had shown a bleed, and they were monitoring it. That was all the information Legend had told the group when he’d had a moment to spare.
Four’s vocera activated, telling him he had a call from the charge nurse. When he answered, he was told Malon had called and said they’d be finishing up in about thirty minutes and were likely to come up open.
Why was he coming up with his abdomen open? When had they gone from exploratory laparotomy to a full on open abdomen?
Ten minutes later, Malon called back to give report. When Four answered, the first thing he asked was, “How’s he doing? Is he okay? Are you okay?”
“I’m fine,” Malon said, even though she sounded exhausted. “And he’s… hanging in there. I’ve seen worse, I’ll say that. I’ll give you the full rundown, okay?”
Four listened as Malon gave report, feeling his heart settled into his stomach, which was tying itself in knots. Multiple spots of bleeding, possible compartment syndrome in his abdomen, a likely kidney injury due to compression from the bleeding on some major vessels, a small hematoma in his brain… they’d had to call neurosurgery to do an emergency craniotomy out of overt concern of swelling, given that Wild had apparently had previous head trauma, based on what they saw in the OR.
Open abdomen, craniotomy, ICP monitoring, bleeding, one chest tube… this was a disaster. Four swallowed as he wrote, feeling his hand shake a little as his heart raced. He was not qualified enough to be admitting this. He was not.
But the turnaround on his unit was pretty insane, and he was the most experienced nurse on the unit today. At least Ezlo was charge; he knew he’d be well supported.
This was a nightmare. But Four had dealt with nightmares, and he would deal with this. He wasn’t going to screw up taking care of any patient, but especially his friend.
Sighing, he hung up the phone after thanking Malon, pushing worries for her and Time aside, trying to focus on what he would need, who he should grab to help him, and how he should prep his room.
It was time to get to work.
When everyone arrived from the OR, Four made brief eye contact with Time. He couldn’t read much from the man, who was stone faced, aside from the exhaustion evident in the dark circles under his eyes. Four got to work quickly, assessing Wild from head to toe as he looked to see what IV medications he was on. A coworker wrote the note while Ezlo helped detangle his lines (the OR always brought up a mess, after all). Time gave an overview of the surgery, and Four listened along as he checked pupils, as he zeroed the arterial line and the ICP monitor, as he listened to lung and heart sounds, as he checked the chest tube and stripped it with his fingers to ensure patency, as he checked peripheral pulses, as he looked at the abdominal dressing to get a baseline in case there was swelling from bleeding later. One of the techs connected the chest tube to wall suction, and Four looked over his drips. Only having levophed at 2 wasn’t terrible, and he was getting a unit of red blood cells, which was in a transfusion set that was y’d to some lactated ringers fluid. He was on propofol for sedation. Another nurse grabbed a blood gas from his arterial line and sent off labs. His foley he had was temp sensing, and Four quickly ascertained that Wild was cold, so he set up the blanket warmer and covered his friend up.
His friend. His friend.
Four shook his head. He had to focus.
As Time left the room, he put a hand on Four’s shoulder, making him freeze. The surgeon didn’t speak, just locking eyes with him. Four wasn’t entirely sure if it was for his own benefit or not. But he had no more time to let his emotions make any decisions for him. He nodded to the doctor, who nodded in return, and then the two went their separate ways.
This was going to be a long day.
#Apologies if this sounds too similar to Level One because I haven’t read that fic in over a year and never finished it#So I don’t remember what happened to Wild in it aside from he was also in an MVC and was in rough shape LOL#Writing#lu in healthcare#lu wild#lu four#lu time#lu malon#dang how long is this storyline gonna be lol#I get too caught up in the medical side of it HA#He’ll be fiiiiine#I got all excited talking about admission from the OR stuff lol#It’s so chaotic y’all#There are like eight thousand people in the room and the lines are a hot mess and I HATE when teh lines are a hot mess#But this was also weird because I admit heart patients… and Wild—being a trauma patient—has… so few drips?? Compared to heart patients???#Like… trauma patients aren’t usually on pressors because what they need is blood#Whereas cardiac surgery patients might need blood… or they’re just vasoplegic… or their heart sucks…#Lots of different options lol#Anyway I’m rambling in the tags whoops#Skye time travels through the queue
93 notes
·
View notes
Text
Top 5 Most Needed Equipment in a Hospital
Hospitals are the cornerstone of healthcare, playing a crucial role in saving lives and improving the quality of care. To deliver optimal treatment, hospitals must be equipped with the latest and most essential medical devices. These tools not only enhance diagnostic accuracy but also ensure patient safety and efficient operations. In this article, we’ll explore the top 5 most needed equipment in a hospital, detailing their importance and functionality. If you’re looking to procure high-quality devices, consider exploring options to buy medical supplies online, where convenience meets affordability.
1. Diagnostic Imaging Systems
Diagnostic imaging systems are indispensable in modern medicine, allowing doctors to view and analyze internal structures of the body. Equipment such as X-ray machines, CT scanners, and MRI machines provide critical insights into a patient’s condition.
Why They’re Needed:
Enable early and accurate diagnosis.
Help in planning surgical procedures.
Monitor the effectiveness of ongoing treatments.
Investing in reliable diagnostic imaging systems ensures better patient outcomes and streamlines the treatment process. High-quality imaging devices are widely available through medical supplies online platforms, offering advanced technology at competitive prices.
2. Patient Monitoring Systems
Patient monitoring systems are essential for tracking vital signs such as heart rate, blood pressure, oxygen saturation, and temperature. These systems are particularly crucial in intensive care units (ICUs) and operating rooms.
Key Features:
Continuous monitoring of patient health.
Real-time alerts for any abnormalities.
Integration with hospital information systems for data storage and analysis.
Modern patient monitors are equipped with wireless capabilities, enabling remote monitoring. This feature is invaluable, especially during emergencies or in telemedicine settings.
3. BPL ECG Machine
An electrocardiogram (ECG) machine records the electrical activity of the heart and is essential for diagnosing various cardiac conditions. Among the top-rated ECG machines, the BPL ECG machine stands out for its precision and user-friendly design.
Benefits of BPL ECG Machines:
High accuracy in detecting arrhythmias and heart abnormalities.
Easy-to-use interface for healthcare professionals.
Portability, making it ideal for both hospital and home use.
Cardiac health is a critical aspect of patient care, and a dependable ECG machine ensures timely intervention. Purchasing a BPL ECG machine from trusted sources online guarantees authenticity and quality.
4. Surgical Instruments and Equipment
No hospital can function without a comprehensive range of surgical instruments. From scalpels and forceps to advanced robotic surgical systems, these tools are vital for performing both minor and major surgeries.
Must-Have Surgical Equipment:
Sterilizers to ensure a contamination-free environment.
Laparoscopic tools for minimally invasive procedures.
Advanced anesthesia machines for patient safety during operations.
To maintain high standards of patient care, hospitals must regularly update and replace their surgical instruments. Many healthcare facilities prefer sourcing these items through medical supplies online, ensuring timely delivery and cost-effectiveness.
5. Ventilators and Respiratory Equipment
Ventilators and other respiratory equipment have become indispensable, especially in the wake of the COVID-19 pandemic. These devices provide critical support for patients who struggle to breathe independently.
Importance of Ventilators:
Assist patients with respiratory failure.
Play a crucial role in ICUs and emergency care units.
Provide life-saving support during severe illnesses or post-surgical recovery.
Modern ventilators come with advanced settings to customize airflow and pressure, catering to the unique needs of each patient. Hospitals can explore various models and price ranges by purchasing these devices from medical supplies online platforms.
Why Choose Medical Supplies Online?
The healthcare industry is evolving rapidly, and so is the way hospitals procure equipment. Buying medical supplies online offers several advantages, including:
Wide Range of Options: From basic tools to advanced machinery, online platforms provide a comprehensive selection of medical equipment.
Cost Efficiency: Competitive pricing and frequent discounts make online shopping more affordable.
Convenience: Avoid the hassle of visiting multiple vendors; place orders with just a few clicks.
Authenticity: Reputable platforms ensure that all products meet international quality standards.
2 notes
·
View notes
Text
Aspiration pneumonia due to anesthesia digestive endoscopy under COVID-19: a case report by Xin Wang in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
Background: Digestive endoscopy is an important test for early cancer screening. The most serious complication during the examination was aspiration pneumonia. However, these patients currently do not receive much attention.
Case report: A woman was brought to the Emergency Department because of fever. Chest computed tomography revealed consolidation of the lower left lung, so the patient was diagnosed with aspiration pneumonia after anesthesia digestive endoscopy. we collected Bronchoalveolar lavage (BALF) for testing of metagenomic next generation sequencing (mNGS). The result of mNGS was normal. After 7 days of medical treatment, the pneumonia subsided.
Conclusion: This case reminded us that digestive endoscopy under sedation carried a risk of aspiration pneumonia in even healthy patients. When COVID-19 prevalent, we should make a definitive diagnosis of patients with fever as soon as possible and improve etiological tests to prevent delays.
Keywords: Aspiration pneumonia, Digestive endoscopy, Case report
Introduction
Digestive endoscopy is an important test for early cancer screening. As the test is uncomfortable so more and more people choose general anesthesia. The most serious complication during the examination was aspiration pneumonia due to reflux and aspiration.
However, these patients do not currently attract much attention, especially from anesthesiologists. Here, we report a healthy nurse who had undergone digestive endoscopy, aspiration pneumonia developed during induction of general anesthesia under COVID-19.
Case Report
A woman was brought to the Emergency Department of the Center Hospital of Jinan because of fever. She got aspirated and developed severe shortness and chest pain. History of anesthesia digestive endoscopy 1 day ago, accompanied by vomiting. Her past medical history was unremarkable, she denied cigarette smoking, and has no history of allergy, anaphylaxis or bronchial asthma. Upon arrival at the hospital, she was connected to the monitor and put on humidified oxygen. On examination, she was severely distressed, blood pressure of 120/60mmHg, pulse rate of 108 beats per minute, oxygen saturation of 95% at room air, and respiratory rate of 26 breaths per minute, temperature of 39 degrees. On physical examination, wet rales were heard in the lower left lung. Blood gas analysis showed pH 7.45, partial pressure of carbon- dioxide 36.00 mmHg and partial pressure of oxygen 71.00 mmHg with 2 L/min oxygen via nasal cannula. The peripheral white blood cell count (9940/μL) and C-reactive protein level (78.5mg/h) were slightly high. The results of blood coagulation function test, biochemistry tests, myocardial enzymes, urinalysis and stool analysis were normal. Chest computed tomography revealed consolidation of the lower left lung.
Under COVID-19, in order to rule out the atypical pathogen infection and assist the patient in expulsion of inhaled substances, we performed tracheoscopy. Flexible bronchoscope showed injured and edematous surfaces of the large airways. Bronchoalveolar lavage was performed from the posterior segmental bronchus of the upper lower of her left lung. A cell count of the bronchoalveolar lavage fluid (BALF) revealed57.5% macrophages, 28.0% neutrophils, 11.0% lymphocytes, and 3.5% eosinophils. The total BALF cell count was 4.2 × 106/mL. No bacteria or fungus was isolated from cultures of BALF. we collected BALF for testing of metagenomic next generation sequencing (mNGS). The result of mNGS was normal.
During hospitalization, the patient received piperacillin/ tazobactam to prevent bacterial pneumonia,hormonal anti-inflammatory and bronchodilators to improve the bronchospasm or wheezing.
After 7 days of medical treatment, the pneumonia subsided, blood, sputum cultures revealed negative findings. and she was discharged in a stable condition. The Fig. 2 was the chest CT of review.
Discussion
The possibility of aspiration pneumonia was considered based on the rapid onset of the patient, the absence of previous upper respiratory infection and chest CT findings. The patient's clinical manifestations, chest CT and hematological examination results further confirmed the hypothesis. The patient's symptoms improved after early treatment with oxygen therapy, anti-infection and hormone anti-inflammatory therapy, which was also consistent with previous research results (1).
Chest CT of aspiration pneumonia often shows multifocal consolidation or patchy ground-glass opacity (2). Because the patient was in left decubitus at the time of digestive endoscopy, so gastric contents flowed back into the left side, then large exudate shadows can be seen in the lower lobe of the left lung. We all know, Aspiration of large amounts of gastric acid will result in the induction of a chemical injury to the airways and lung parenchyma. Aspiration is recognized as an independent risk factor for the subsequent development of pneumonia or acute lung injury or acute respiratory distress syndrome (ALI/ARDS). (3)
Our patient developed dyspnea and hypoxemia. In order to prevent further exacerbation of lung injury, we treated with hydrocortisone. The other study suggested that, in bronchi-aspiration, Steroids are not proven to improve outcome or reduce mortality (4). After hormone therapy, the patient's symptoms of dyspnea and hypoxemia were significantly improved. There were any adverse reactions. However, it remains to be discussed whether hormones can be used as a routine treatment for aspiration pneumonia.
Conflict of interest statement
All authors have read and approve the final manuscript.
Author contribution statement
Wang Jing wrote the manuscript, conceived and designed the report; Cui JY collected and prepared the images; Wang X reviewed and confirmed the final version of the manuscript.
Ethics statement
The authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
#Aspiration pneumonia#Digestive endoscopy#Case report#Journal of Clinical Case Reports Medical Images and Health Sciences submissions#jcrmhs#Journal of Clinical Case Reports Medical Images and Health Sciences (JCRMHS)| ISSN: 2832-1286
3 notes
·
View notes
Text
Angela “Angie” Hall, 29 (USA 1991)

Angela Hall was 29 years old and pregnant with her 6th child. She already trying to take care of so many kids and didn’t think she could feed another one. She was desperate and overwhelmed and she didn’t know where to turn to.
Angela needed real help and support. Instead, she was lured into a dangerous second-trimester abortion by an advertisement showing a happy couple arm-in-arm with each other. Ashamed to admit what she was about to do, Angela gave her mother an excuse about going somewhere else and had her friend Annette Wilson drive her to Birmingham for an abortion.
The abortion facility advertised in the picture was owned by abortionist Thomas Tucker, who regularly traveled between Alabama and Mississippi to perform abortions and claimed to be doing over 60% of the abortions in Mississippi. Joy Davis (one of his employees) screened Angela and found out that she was anemic and she had a fever. Because of Angela’s poor condition, Joy called Tucker and told him that Angela should be referred to a hospital.
Tucker didn’t care about Angela’s safety. He told Joy, “You know we need the money. Just do it. Just put the patient through.”
The first time Tucker so much as laid eyes on Angela, she was already under anesthesia. Tucker frequently had staff with no medical credentials administer anesthesia and laminaria dilators to his clients. Even Joy Davis, who had been tasked with examining Angela before the abortion, had no formal medical training. Yet even she could tell that Angela was unhealthy and at risk.
Just as the abortion was finished, Angela took a turn for the worse. She started gasping for air and an alarm on her blood pressure monitor was going off. Tucker told his staff to turn off the alarm because other clients would be able to hear it.
After screaming at his employees and temporarily stabilizing Angela’s blood pressure, Tucker sent Angela to a so-called recovery room. Packing was put in place in an attempt to stop her from bleeding, but Angela was so severely injured that she bled profusely through the packing material.
The bleeding was extremely dangerous. According to Joy, “Blood was running down the table. It was pooling in the floor and running down behind her back.” Joy wanted to call an ambulance, but Tucker didn’t want anyone to know about his second severely injured client that same day. (Before performing an abortion on Angela, he sent another client to the hospital.) He told his scared employee that he was the doctor and if anybody was going to make a decision to call the ambulance, it was going to be him. Angela was left in the sheets and hospital gown that were soaking in her own blood.
Unsurprisingly, Angela kept getting worse. Joy knew that Angela was still bleeding, so she went to Tucker and told him. His callous response was, “What do you want me to do?” Finally, Joy stood up to her boss and told him, “I don't know, but I want you to do something. She's going to lay here and die.” Tucker told her, “Fine. Call the fucking ambulance.” He then left the building and Joy (who had no formal medical training) was left trying to keep Angela alive until the ambulance could get there.
The ambulance took Angela to the hospital, where she was placed in the ICU. She suffered from respiratory failure, clotting, blood loss and sepsis. Hours later, Angela’s friend Annette finally called Angela’s mother (Mrs. Kidd) and told her that Angela was in the ICU. Mrs. Kids arrived to find her daughter covered in tubes and barely even breathing.
Angela died on June 14 just before midnight. Her autopsy found numerous tears and lesions in the pelvic area, which had leaked amniotic fluid into her bloodstream. She had congestive necrosis in her liver and spleen. The doctors concluded that the amniotic fluid embolism caused clotting problems that resulted in the necrosis, septic shock and cardiac arrest.
Alabama authorities subpoenaed Angela's records. To cover up what he had done, Tucker told the traumatized Joy to destroy some records and falsify others. On his orders, she tore up the records, which Tucker then tried to burn in an ashtray, setting off the facility’s smoke alarm. Tucker put out the fire, bagged up the damaged papers and ordered Joy to take the papers to the basement and burn them. Instead, she taped the pieces back together and eventually turned them over to the medical board.
The investigation found seemingly endless malpractice. Tucker had failed to report multiple malpractice lawsuits, most of which involved his abortion clients. He perforated the uteruses of at least 3 other clients, allowed untrained staff to administer anesthesia, insert laminaria and perform abortions, had been known to disregard the state’s waiting period for abortions, falsified records, destroyed incriminating evidence and wrote fake prescriptions in order to sell addictive drugs. He was also responsible for the death of 21-year-old Michelle Jordan, who came to one of Tucker’s facilities to have the birth control implant in her arm removed. (The implant could easily be removed with only local anesthetic, but Tucker unnecessarily had general anesthesia used instead. He may have also had one of his unqualified employees administer anesthesia to Michelle, who died from complications of anesthesia.)
In 1994, Tucker was stripped of his license to practice medicine in Alabama. The attorney general and the state medical board declared him an “immediate danger to his patients.”
Joy Davis was done working for Tucker. She became a very active Pro-Lifer and started working to help vulnerable women avoid sharing Angela’s fate.
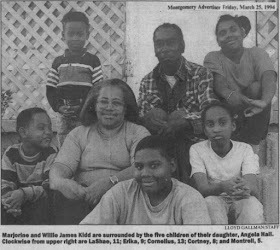
As for Angela’s 5 surviving kids, they were adopted by their grandmother, who did the best she could to raise them all in a 2-bedroom house. The youngest can recognize a picture of his mother, but all he remembers of her is bringing flowers to her grave.
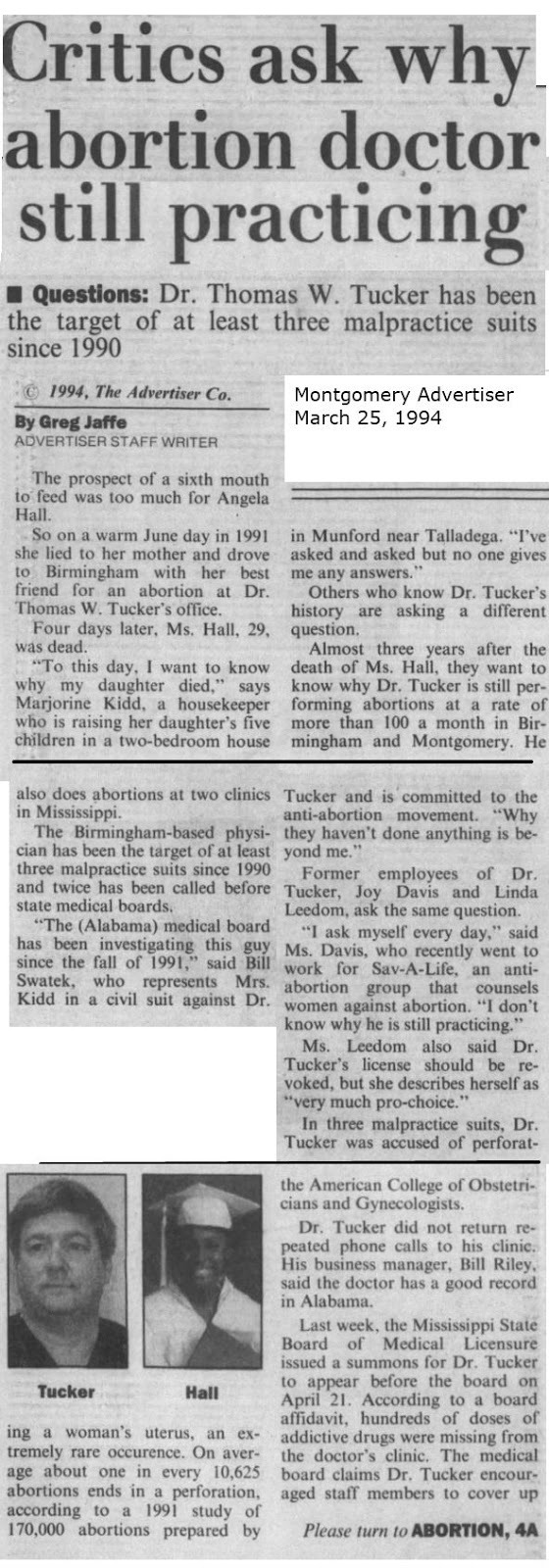

#tw murder#tw abortion#tw ab*rtion#tw blo0d#tw death#pro life#pro choice#abortion#abortion debate#unsafe yet legal#black lives matter#unsafe but legal
42 notes
·
View notes