#Gynecological cancers
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In 2020, 27% of US Tumblr users had an annual household income of over $100,000.
Text
Gynecological cancers encompass a range of malignancies affecting the female reproductive system, including cancers of the cervix, ovaries, uterus, vulva, and vagina. These cancers can have a profound impact on a woman’s health and quality of life. However, with early detection and proactive prevention strategies, the chances of successful treatment and management can significantly improve. Dr. Shweta Mendiratta stands out as the Best Gynaecologist in Faridabad, offering comprehensive services for women in gynecological health.
#Best Gynecologist in Faridabad#Gynaecological Cancer Doctor in Faridabad#Gynecologic cancer Treatment in Faridabad#Gynecological Cancers#best gynaecologist in faridabad
0 notes
Text
Dispelling myths and empowering knowledge! Join Dr. Viral Patel as he debunks common misconceptions surrounding gynecological cancers in our latest video. Let's separate fact from fiction and empower women with the truth. Stay informed, stay empowered. Watch now to learn the facts and protect your health.
youtube
0 notes
Text
Understanding Gynecological Cancer: Detecting, Treating, and Healing

When it comes to women’s health, gynecological cancers stand as a significant concern. Gynecological cancer refers to cancers that specifically affect the female reproductive system. These cancers can occur in various parts of the female reproductive organs, including the cervix, ovaries, uterus, vagina, and vulva. It's crucial for every woman to be aware of the symptoms and treatment options available.
#Cancer#gynecological cancers#gynecological cancers Doctor#gynecological cancers treatment#Cancer treatment
0 notes
Text
Hereditary breast ovarian cancer syndrome: One case, multiple lessons by Ikram Burney in International Journal of Clinical Images and Medical Reviews
Abstract
Ovarian cancer is one the most common gynecological cancers, and epithelial ovarian cancer is the commonest sub-type. Between 10 and 15% of all epithelial ovarian cancers occur secondary to a mutation in BRCA1 or BRCA2 gene, and may be associated with breast cancer, known as hereditary breast ovarian cancer syndrome (HBOCS). We report a case of HBOCS, highlight the importance of family history and treatment history and discuss the recent developments in surgery and systemic treatment for patients in relation to the presentation of this case.
Introduction
Ovarian cancer is one the most common gynecological cancers (Bray 2018). Epithelial ovarian cancer is the commonest sub-type (Kurman 2014). Between 10 and 15% of all ovarian cancers occur secondary to a mutation in a cancer susceptibility gene (Zhang 2011). Mutations in BRCA1 and BRCA2 gene are the commonest cause of hereditary ovarian cancer (Mikki 1994; Claus 1996). These mutations also predispose the individuals to other cancers. Patients with epithelial ovarian cancer may also develop breast cancer (Easton 1993; Easton 1997). We report one such case here, and discuss the recent advances in the medical and surgical management of hereditary breast ovarian cancer syndrome (HBOCS).
Case
A 57 year-old lady presented with abnormal vaginal bleeding and abdominal distention. She was diagnosed to have high grade ovarian cancer, underwent total abdominal hysterectomy, bilateral salpingo-oophorectomy and omentectomy, and was found to have stage IIIC serous papillary type of high grade ovarian cancer. The patient was treated with 6 cycles of Carboplatin and Paclitaxel to complete serological and radiological remission, however, she tolerated the chemotherapy with frequent episodes of febrile neutropenia. Three years later, the disease relapsed and the patient was treated with 6 cycles of Liposomal Doxorubicin to state of complete serological remission. One year later, the disease relapsed yet again, and this time, she received Carboplatin as a single agent. The disease entered serological remission after 3 cycles, however, the patient could not continue treatment because of repeated febrile neutropenia and thrombocytopenia
One year later, the disease relapsed a 3rd time. CT scan showed disease only at one site (figure 1a) and the patient was treated with Carboplatin at a reduced dose, once again to a state of complete serological and radiological remission (figure 1b). A surveillance mammogram was reported as BIRADS II and the bone mineral density revealed osteopenia. One year later, the disease relapsed a 4th time, again in a solitary site, and the patient was counseled about treatment with chemotherapy followed by a secondary cyto-reductive surgery, to which the patient agreed. The patient received 6 cycles of chemotherapy at reduced doses, followed by surgery. There was no residual disease and the patient remained in complete remission for more than one year and 3 months.
At this stage the CA-125 was seen to rise again serially, and mammogram showed a 2.2 cm speculated lesion in the left breast. A fine needle aspiration was highly suggestive of breast cancer, and a core biopsy revealed an infiltrating ductal carcinoma, grade II, estrogen and progesterone receptor positive, but negative for HER-2/neu protein (ER positive; PR positive; HER-2/neu negative). The proliferation fraction measured by Ki-67 was 40%. The morphologic and immunohistochemical patterns were consistent with a diagnosis of a primary in the breast (Table 1). Staging CT scan revealed a metastatic lesion in liver and bilateral pulmonary metastases. An attempt at guided biopsy from the pulmonary lesion was unsuccessful and led to pneumothorax. The patient refused further attempt at biopsy and agreed to be treated with Letrozole, considering that the pattern of metastases was more likely secondary to breast cancer rather than the ovarian cancer. Ten months later, the CT scan showed a marked regression in the size of pulmonary lesions, but a stable liver lesion (Figure 2).
Table 1: Immunohistochemical staining patterns of breast and ovarian cancer. WT-1 (wilm’s Tumor 1); PAX 8 (Paired box gene 8); CA 125 (Cancer antigen 125); ER/PgR (Estrogen receptor / Progesterone receptor); CK 7 (Cytokeratin 7); GCDFP-15 (Gross cystic disease fluid protein-15); TP 53 (Tumor protein 53)
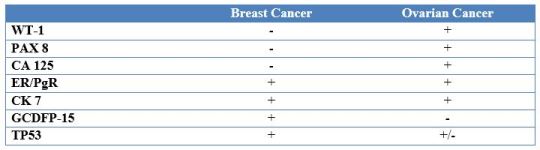
Figure 1: CT scan at the time of the 3rd relapse (Figure 1A) shows a 35 mm x 28 mm mass in the region of omentum, which disappeared completely after 6 cycles of carboplatin AUC 4 (Figure 1B).
Considering that the patient had HBOCS, the patient was referred to the cancer geneticist. A detailed history revealed that her mother had dies of a malignancy of unknown primary site, her sister died at the age of 40 years, of a malignancy with ascites, but the primary site was not known to the patient or the family. The patient underwent counseling followed by assessment with a germline mutational analysis for breast and ovarian cancer panel, which revealed a pathogenic mutation in BRCA2 gene (c.4243G>T), and a variant of unknown significance in the NBN gene (c.425A>G). The BRCA2 mutation was consistent with a diagnosis of HBOCS. One year later, the CA 125 was seen to rise again serially, while the metastatic lesions in the lung and liver were under good remission. The patient was commenced on treatment with Olaparib, and the CA 125 dropped from 324 to 26 in one year (figure 3). The patient continued to receive Letrozole. Twelve years after the diagnosis of ovarian cancer, and while still on treatment for breast and ovarian cancer, the patient passed away of an unrelated cause. During the course of the treatment, patient’s three daughters agreed for mutational analysis; two tested positive for mutation on the BRCA2 gene, and one of those two was screen-detected to have a breast cancer.
Figure 3: Serum CA 125 levels (IU/L) plotted over time. The patient was commenced on treatment with olaparib in Nov 2015. The levels dropped to within the normal limits (<36IU/L) in March 2016 (within 4 months of the treatment).
Discussion
We report the case of a woman diagnosed to have HBOCS, who lived 12 years after the diagnosis of high grade ovarian cancer, received multiple lines of intra-venous chemotherapy, albeit with difficulty, underwent a secondary cyto-reductive surgery, and in the last 4 years of her illness was treated for the two cancers with an oral aromatase inhibitor and a PARP inhibitor. Both breast and ovarian cancers responded to the treatment with the two oral agents. We would like to highlight several aspects of management for the general readership of this journal.
The median survival of patients diagnosed to have high grade ovarian cancer, stage IIIC is dismal at around 3-4 years (Peres 2019). This patient lived for 12 years. Complete response to chemotherapy on five occasions, and a poor tolerance to chemotherapy, even at an age of 57-65 years indicate the tumor is exquisitely sensitive, especially to platinum containing chemotherapy. Platinum derivatives (Cisplatin, Carboplatin and Oxaliplatin) are alkylating agents, which act by disrupting the DNA repair pathways. Usually, PARP (Poly (ADP-ribose) polymerase) enzyme is required for base excision repair (BER). If the enzyme were inhibited, DNA repair would be affected. Also, if one allele is inactivated on the BRCA 1 or 2 gene, such as, because of mutations or methylation, DNA repair will be grossly affected, leading to a process called ‘synthetic lethality’ (Konstantinopoulos 2010; Helleday 2011). In the last few years, three such compounds (Olaparib, Niraparib and Rucaparib) have been developed, tested, and have become the standard of care for patients with either germline BRCA mutations, or even in patients who may have homologous reconstitution deficiency (Ledermann 2014, Mirza 2016; Pujade-Lauraine 2017; Coleman 2017). The first-in-class compound was Olaparib, approved by the FDA in 2014 for use as a single agent in patients who had germline BRCA mutations and had failed three lines of chemotherapy (Ledermann 2012). Our patient was treated and responded to the treatment.
BRCA 1 mutation is more common than mutation in BRCA 2 gene, and it is important to distinguish between the two. Although, response to platinum chemotherapy or PARP inhibitors is the same (Konstantinopoulos 2010), there are phenotypic differences, especially for breast cancer, and the susceptibility to develop other cancers, required for counseling the family members. Patients with BRCA 1 mutation are associated with triple-negative breast cancer (ER negative; PR negative; HER-2/neu negative) in more than 75% of the cases, whereas, patients with BRCA 2 mutations are associated with hormone-receptor positive breast cancer in more than two thirds of the cases (Hartmann 2016). Our patient had BRCA 2 mutation and hormone-receptor positive breast cancer, which was treated with aromatase inhibitor for more than 4 years. Although the life-time risk of developing breast cancer is same (65-70%) in the patients and the first-degree relatives, the life-time risk of ovarian cancer is 40-45% in case of BRCA 1 mutation carrier and 10-15% in case of BRCA 2 mutation career (Antoniou 2003; Hartmann 2016). Our patient had three daughters and they were counseled. Two tested positive for the same mutation. Because of their relatively young age, and the minimal increased risk of ovarian cancer in BRCA 2 mutation carriers, till the age of 45 years, they were advised to consider delaying BSO.
The role of secondary cyto-reductive surgery in ovarian cancer has been contemplated and debated over the last several years. Three major phase III trials have been reported in the past 2 years (Please see table 2). The GOG-0213 trial was the first trial to have been reported (Coleman 2019). The primary end point was overall survival (OS); 485 patients were randomized to receive standard of care chemotherapy with or without secondary cyto-reductive surgery. The patients were selected if the treatment free interval from the last dose of platinum containing chemotherapy was more than 6 months. Although, there was a non-significant prolongation in the progression-free survival (PFS) (18.9 vs 16.2 month; HR 0.82), there was no difference in OS. Actually, the OS was inferior in the group which received secondary cyto-reductive surgery (50.6 vs 64.7 months; HR 1.29). However, a sub-set of patients who achieved R0 resection had a better PFS and OS, compared to those who could not have a R0 resection. The DESKTOP III trial randomized 407 patients to receive standard of care chemotherapy with or without secondary cyto-reductive surgery (du Bois 2017). There was a clinically and statistically significant prolongation in the PFS (19.6 vs 14 months; HR 0.66). Also, the primary end-point was met (du Bois et al 2020). The was a significant 7.6 months prolongation in OS (53.6 vs 46 months; 0.75 (0.58-0.96; P = 0.02). In addition to the criteria of treatment free interval of more than 6 months, the investigators also used the AGO criteria. The AGO criteria was developed after the DESKTOP I trial, and women with no gross residual disease after primary surgery, ECOG performance status of <1, and no ascites on CT scan at recurrence were classified as AGO score positive (Harter 2006). Subsequently, the DESKTOP II trial suggested that patients with a good performance status, absence of ascites at the time for secondary cyto-reductive surgery, more than 12 months of platinum-free interval, isolated site of recurrence, and the possibility of complete resection of disease were likely to benefit from the secondary cyto-reductive surgery (Harter 2011). The 3rd trial (SOC-1 trial) randomly assigned 356 patients with recurrent ovarian cancer in first relapse to either chemotherapy, or cyto-reductive surgery and chemotherapy (Zhang R 2020). There was a clinically meaningful (5.5 months), and statistically significant prolongation in the PFS (17.4 vs 11.9 months; HR 0.58) for the combination of cyto-reductive surgery and chemotherapy arm. The eligibility criterion was different from the first two studies. The SOC1 investigators selected patients if the platinum-free interval was at least 6 months, and an integrative model score was <4.7. However, at the time of management of our patient, results of the randomized trials were not available. We based our decision on the available data from DESKTOP I and II trials. The patient fit both the AGO score positive and the subsequent criterion developed after DESKTOP II trial. Our patient lived more than 5 years after the cyto-reductive surgery without a subsequent recurrence in the abdominal cavity.
Taken together, the three randomized trials comparing chemotherapy with or without cyto-reductive surgery suggest that there may be a benefit for surgery in carefully selected patients who can undergo potentially complete (RO) resection in women who have recurrent platinum-sensitive ovarian cancer. Although, results of randomized trials should not be compared, however, it would be useful to note that the magnitude of benefit seen in the DESKTOP III trial (HR 0.75), is similar to the recently reported SOLO2 study. The later study compared the OS in patients with platinum-sensitive ovarian cancer, but who also had a BRCA mutation, and who were treated with the PARP inhibitor, olaparib and had a median OS of 51.7 months compared to 38.8 months in the placebo arm with a HR of 0.74 (Poveda 2020). Although, olparaib is the standard of care for maintenance treatment in patients with BRCA mutated platinum-sensitive ovarian cancer, the cost of drug and the overall cost of management remains very high. Cyto-reductive surgery in carefully selected patients, with a potential to achieve R0 resection may be an alternative, especially for patients with BRCA negative platinum sensitive ovarian cancer in first relapse.
In conclusion, we report the case of a patient with HBOCS, and highlight the recent developments in the systemic and surgical management of patients with ovarian cancer.
Table 2
SCS: Secondary cyto-reductive surgery; CT: Chemotherapy; OS: Overall survival; HR: Hazard ratio; PFS: Progression-free survival
Conflict of Address
Ikram Burney:
Principal Investigator for the hospital site for Astra-Zeneca sponsored PREDICT study Served on the advisory board for Astra Zeneca Other authors declare no conflict of interest
Author’s contribution:
Dr Juhaina Al Hinai – Data curation; Writing – original draft.
Dr Moza Al Kalbani – Surgical Oncology management, Methodology; Writing – review & editing.
Dr Marwa Al Riyami – Pathology reporting, methodology; Writing – review & editing.
Dr Abeer Al Sayegh – Clinical Genetics management, methodology; Writing – review & editing.
Dr Ikram A Bunrey - Conceptualization; Formal analysis; Supervision; Writing – original draft; Writing – review & editing.
Informed Consent:
All data are anonymised, and patient identification is not possible.
For more details: https://ijcimr.org/editorial-board/
#Ovarian cancer#gynecological cancers#HBOCS#Epithelial#abnormal vaginal#bleeding and abdominal#Liposomal#Doxorubicin#chemotherapy#Immunohistochemical#pulmonary#Olaparib#Ikram Burney#ijcimr
0 notes
Text
Following the news that Kate Middleton has in fact been diagnosed with cancer, I’d like the take the time to offer some information on cancer in afab people and some charities to support.
Cancer is a very personal and scary thing to face, and according to Cancer Research UK, every two minutes in the uk someone is diagnosed with cancer. Over 182000 women in the uk are diagnosed every year.
Almost half of all cancer cases are diagnosed at stages 3 & 4, and screening rates for breast and cervical cancers have fallen in the last few years in England and Scotland.
According to The Eve Appeal, around 60 afab people are diagnosed with gynecological cancers alone every day in the uk, and 21 of them will not be able to receive appropriate treatment in time.
People around the world are woefully uneducated about cancer as a whole, but the stigma and lack of proper knowledge given to the public and young afab people about our own bodies means that we often go under diagnosed, or are too afraid or ashamed to see a doctor until it’s too late.
I’ll be listing some informational pages to help people learn about the signs of breast and gynecological cancers that I believe every young person with an afab reproductive system needs to know. On the pages from The Eve Appeal and Breast Cancer UK there is also information for transgender and intersex people.
All of these sites have information on how to identify possible markers of cancer, information on how to get tested, and on how to donate to their charities. I highly suggest everyone regardless of gender identity have a look through to potentially help yourself or a loved one.
-Roe
62 notes
·
View notes
Text
huh, cool
#r#HPV vaccine#gardasil#female health#gynecology#i am aware of the class action lawsuit but at least it seems like it works for cancer risk reduction#radfems do interact
65 notes
·
View notes
Text
It’s over.
It’s finally over.
I’m free.
Had my final appointment at the cancer clinic today. It was a pelvic exam and colposcopy to make sure that I was all healed up inside after the hysterectomy and that there were no traces of any abnormalities. I’d been anxious about the appointment for WEEKS.
It wasn’t my surgeon who saw me, it was one of her associates, but she was so kind and understanding and empathetic that I felt good about it going into the procedure. The procedure itself was super un-fun given how one of the symptoms of menopause is vaginal dryness/atrophy. All the lube in the world didn’t make that speculum go in any easier and it hurt like hell, but once it was in place it was fine.
After a thorough look and feel and a LOT of anxiety on my part, the doctor pronounced me fully healed and fit to return to all activities. She said that there is no need for them to see me again, that this is it, but that if I have any concerns come up or any questions in the future or issues related to any pelvic health, to give them a call back and they’d take me back on without question.
That said, though, I never need another pelvic exam. I never need another pap test. I never need to deal with all of the menstrual bullshit again. I can bid cancer goodbye and good riddance.
It’s actually, finally over.
#cancer tag#tw cancer#tw endometrial cancer#tw gynecologic cancer#tw medical procedure#tw colposcopy#tw pelvic exam#I'm going to be crying about this for a few days#until it really sinks in#I am O V E R W H E L M E D#not in a bad way#but not quite in a good way yet either?#I'm not quite sure what I feel right now#other than the urge to take a hot shower and get the excess lube off lmao#FUCK this has been a JOURNEY
23 notes
·
View notes
Text
(Inspired by this post, but separate to avoid derailing.)
I’m going to get more personal here than I would really like to, but I know a lot of other people have had awful gynecologist experiences, and I hope sharing both the negative and positive experiences could help.
I have had three Pap smears. The first two were traumatic, not in a hyperbolic way but in an “I cried about them to my therapist when trying to face the idea of having to get another one and she specifically called it medical trauma” kind of way.
For me, they were extremely painful, and I was told “no it isn’t,” both by the doctors in the moment and by everything I was able to look up about Pap smears afterwards. Counterintuitively, I was also told that if it was painful, it was because I was doing something wrong. The only people I saw saying Pap smears hurt were other women who had had terrible gynecologist appointments and who were also planning on never going back.
After my first experience, I did what you are supposed to and warned my next doctor that my last experience was painful. Some warning signs that I should have left and found a different doctor include that she acted inconvenienced by that idea, and then was actively annoyed by my admission that I’d never had penis-in-vagina sex, because that would presumably have made it easier to insert the speculum. I went through with the procedure with her anyway, and she somehow couldn’t reach my cervix at first and guilted me for it while actively rooting around in my vagina. I felt like I had to go through with it once it had started, but I kind of wish I had exercised my rights and called it quits. Which is something you can absolutely do. If you’re uncomfortable with the way your doctor is talking to you, or if you think something is going wrong and your doctor is ignoring your needs, you can call off the whole thing and go somewhere else.
Aside from the physical pain and misplaced blame, in both of my bad experiences I was explicitly told that part of the problem was that I wasn’t having “real sex” (referring, of course, to penis-in-vagina sex). If anyone ever asks, I will confidently tell them that the most homophobic experiences I’ve had have been in the gynecologist’s office.
After years of being nagged by my primary care doctor and multiple therapy appointments, I researched my options and was able to find a specifically LGBTQ+ aligned clinic. In my research, I also found that, while gynecologists seem to understand and discuss the need for trauma-informed practice, it is hard to find gynecologists who describe themselves as trauma informed.
At my third Pap smear, I explained my past experiences to the doctor. After listening, the doctor gave me a list of options that could suit a variety of comfort levels. These included a traditional Pap smear, the doctor trying to swab my cervix without using a speculum, and me self administering the test in private, also without a speculum. I chose the last one, and she gave me a swab and detailed instructions on what to do. The only risk to this approach was the possibility that I might not get a usable sample. In that case, I would have to come back to the office to try again. I was able to get a usable sample on the first try, and it was so quick and easy that I’m honestly baffled that this isn’t how Pap smears are usually administered.
Some green flags at this appointment included that I was given space to explain my past experiences, I was not criticized or judged for those experiences, and the conversation about what I needed happened before any move toward the exam table. In fact, that doctor never even touched me. I was also given clear explanations of my options, and the doctor explicitly included the option of leaving the office without getting a Pap smear at all.
Pap smears do not have to be painful or traumatic, and I’m angry that I had to have the first two experiences before the third. I understand that there is probably a reason the traditional method is preferred, but I strongly believe that by actually presenting patients with options and treating us with respect, getting a Pap smear can become a significantly less awful experience. And if patients don’t feel dehumanized and abused for experiencing pain during an objectively unpleasant procedure, they might actually get the tests done.
I have been one of the women who considered just never getting any more Pap smears, in spite of the risks, and I’m glad I had an experience that changed my mind. I hope others who have had negative experiences, or even who are worried about it, are given the choices I was and are able to advocate for themselves and be heard and respected.
#Pap smear#cervical cancer#medical trauma#snackerdooodle actually makes a post#Homophobia cw a bit too#Medical cw#Gynecology
11 notes
·
View notes
Note
I don't know if this is your department but what would happen if a complete hysterectomy was medically necessary (cancer) in the middle of puberty?
Hi Anon,
This is technically not my department - a patient undergoing this would be under the care of a gynecologic oncologist, and a fertility specialist will also probably be a part of the team.
That said, I can discuss the physiology of what would happen:
Uterine cancer in an adolescent is exceedingly rare, and a total hysterectomy would be a treatment only of last resort. The result of a hysterectomy is that the person would become unable to become pregnant.
If the uterus is taken but the ovaries are spared, the person would still go through puberty as normal, developing female secondary sex characteristics, but they would just never menstruate. They would still ovulate, and could theoretically produce a biological child using in vitro fertilization (when eggs are retrieved surgically and fertilized outside the body) and a surrogate to carry the pregnancy.
If both ovaries also had to be removed in addition to the uterus (exceedingly, very very, super rare), the young person would become permanently sterile (no more eggs), and need to receive estrogen hormone replacement therapy to ensure proper growth and health. Estrogen isn't just responsible for the menstrual cycle or for feminizing features - it's also important for bone and cardiovascular health.
For those who are wondering how rare this is:
The annual incidence (how many people per year get a thing) of gynecologic cancers in adolescents (age <18) is 6.7 per MILLION. Of those, 87.5% are of the ovary and only 2.5% are of the uterus. So, out of a MILLION adolescent AFABs, 5.6 people will get ovarian cancer, and 0.2 will get uterine cancer.
That's 2 out of 10 MILLION!
The good news is the survival rates for these cancers is very high!
(Source: Wohlmuth, C., & Wohlmuth-Wieser, I. (2021). Gynecologic Malignancies in Children and Adolescents: How Common is the Uncommon?. Journal of clinical medicine, 10(4), 722. https://doi.org/10.3390/jcm10040722)
---
If this is your situation, Anon, I am very sorry to hear about it. I wish you good health and excellent care!
8 notes
·
View notes
Text
Cervical cancer
Cervical cancer is a type of cancer that develops in the cervix, which is the lower part of the uterus that connects to the vagina. It is the fourth most common cancer in women worldwide and can affect women of all ages. However, it is most often diagnosed in women between 35 and years of age.
Causes of cervical cancer:
The main cause of cervical cancer is infection with human papillomavirus (HPV), a sexually transmitted virus. There are more than 100 different types of HPV, and some types can cause cervical cancer. Other factors that can increase the risk of cervical cancer include smoking, a weakened immune system, a family history of cervical cancer, and multiple sexual partners.
Symptoms of cervical cancer:
Cervical cancer does not necessarily cause symptoms in its early stages. As the cancer progresses, symptoms may include abnormal vaginal bleeding, pelvic pain or discomfort, pain during intercourse, and unusual vaginal discharge. It is important to note that these symptoms can be caused by other diseases, so it is important to consult a doctor to get a proper diagnosis.
Prevention and early detection of cervical cancer:
The most effective way to prevent cervical cancer is the HPV vaccine. The HPV vaccine protects against the types of HPV that cause most cases of cervical cancer, as well as against other types of HPV that can cause other types of cancer. The vaccine is recommended for males and females between 9 and 26 years of age.
Regular cervical cancer screening is also important for early detection. A Pap test is a test that checks for abnormal cells on the cervix. It is recommended that women start regular Pap tests from the age of 21. In addition, the new HPV test can also detect the presence of the virus that causes cervical cancer. Women should discuss with their healthcare provider which exams are right for them.
Treatment of cervical cancer:
Treatment of cervical cancer depends on the stage of the cancer and other factors such as the woman's age and general health. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
In summary, cervical cancer is a common female cancer that can be prevented by vaccination and detected early by regular screening. Women should consult with their health care provider to determine appropriate screening and vaccination. If cervical cancer is diagnosed, early treatment can lead to a better outcome.
For more information Visit: www.oncorelief.in
#Cervical cancer#Women's health#Cancer prevention#Cancer screening#HPV vaccine#Pap test#HPV test#Cancer treatment#Early detection#Health education#Gynecologic oncology#Oncology nursing#Reproductive health#Sexually transmitted infections#Public health#Medical research#Health advocacy#Patient support#Survivorship
4 notes
·
View notes
Text
Specialty Surgical Oncology Hospital and Research Centre
Description- Specialty Surgical Oncology is exactly as the name suggests, it is one of the top cancer hospitals with a leading group of specialist cancer surgeons with vast experience in highly focused areas of cancer surgery, who have joined together to provide the best of their collective expertise to patients battling this difficult disease.
Address- Silver Point, 6th Floor, Lal Bahadur Shastri Rd, Kasturi Park, Maneklal Estate, Ghatkopar West, Mumbai, Maharashtra, 400086.
Phone/Mobile Number- 8268880185 Website URL-https://specialtysurgicaloncology.com/

#Breast Cancer#Gynecological Cancer Treatment#Head and Neck Tumor / Cancer Surgery#Breast Cancer Treatment#Lung Cancer Treatment#Ewing's Sarcoma Treatment#Giant Cell tumour Treatment#Cancer Screening (Preventive)
2 notes
·
View notes
Text
#Gynecological Cancer Surgeon in delhi#Uterine Cancer Specialist in Delhi#Dr. Kanika Batra Modi#Gynecological Cancer Surgeon
0 notes
Text
i’ve discovered my niche redbubble sticker/shirt art category: funny and/or cute cancer designs. made one on my phone last night, just a quick little practice design bc it’s been so long since i’ve used photopea

#i’m sorry it leans into gender roles#also thinking about making versions where the ribbon is the colors for other gynecological cancers too#cancer post#if you want this on a sticker or shirt etc message me for the link
0 notes
Text
Gynecological Cancer Treatment in Indore | Dr. Megha Agrawal

If you’re facing gynecological cancer, specialized treatment options offer effective solutions for better outcomes. Gynecological cancer treatment includes surgery, chemotherapy, and radiation, tailored to each patient’s needs. For advanced gynecological cancer treatment in Indore, several reputable clinics provide comprehensive care plans, helping patients fight cancer with expert support and modern therapies.
#cervical cancer treatment in indore#endometrial cancer treatment in indore#endometriosis clinic in indore#endometriosis treatment in indore#gynae cancer doctor in indore#gynaec cancer surgery in indore#gynaec laparoscopic surgery in indore#gynaecological oncology in indore#gynecological cancer surgeon in indore#gynecological cancer treatment in indore#gynecological oncologist in indore#high risk pregnancy doctor in indore#high risk pregnancy in indore#obstetrics and gynecology in indore#ovarian cancer treatment in indore#best doctor for normal delivery in indore#ovarian cyst doctor in in indore#best gynec for pcod in indore#5 * gynec in indore#best gynec for urine infection in indore#best gynec for white discharge in indore#gynecologist in shalby hospital indore#best gynec for laproscopic hysterectomy#pcos treatment in indore#best doctor for fibroid treatment#best doctor for fibroid surgery#laproscopic fibroid treatment in indore#laproscopic ovarian cyst treatment in indore#best gynecologist for cesarian delivery in indore#best gynecologist for laproscopic operation in indore
0 notes
Text
Comprehensive Gynecological Care in Baner: Dr. Balaji Nalwad Reddy for Ectopic Pregnancy
Women’s health requires specialized care, particularly when dealing with complex conditions like ectopic pregnancy, fibroids, or endometriosis. In Baner, Dr. Balaji Nalwad Reddy is recognized as a leading expert in treating ectopic pregnancies and a range of gynecological conditions. His dedication to women’s health and advanced expertise make him a top choice for women seeking compassionate, expert care.
Understanding the Risks of Ectopic Pregnancy
Ectopic pregnancy is a medical emergency that occurs when a fertilized egg implants outside the uterus, often in a fallopian tube. If untreated, it can lead to serious complications, including rupture and internal bleeding. Common symptoms include severe abdominal pain, irregular bleeding, and dizziness. Dr. Balaji Nalwad Reddy is highly experienced in managing ectopic pregnancies and offers minimally invasive treatments like laparoscopy to ensure quick and safe recovery.
Expert Treatment for Common Gynecological Conditions
Dr. Balaji Nalwad Reddy provides specialized care for a variety of conditions beyond ectopic pregnancy, including:
Endometriosis: This condition can cause chronic pain and affect fertility. Dr. Reddy uses laparoscopy to effectively manage endometriosis, relieving pain and improving quality of life.
Fibroids: Uterine fibroids can cause discomfort, heavy bleeding, and other issues. Dr. Reddy’s minimally invasive techniques, such as hysteroscopy and laparoscopy, make fibroid treatment safer and reduce recovery time.
Ovarian Cysts: Cysts in the ovaries can lead to pain or complications if left untreated. Dr. Reddy’s experience with laparoscopic techniques allows for safe removal, ensuring minimal scarring and faster recovery.
Advanced Surgical Techniques: Laparoscopy and Hysteroscopy
Dr. Balaji Nalwad Reddy’s expertise in laparoscopy and hysteroscopy makes him an ideal choice for women who prefer minimally invasive treatments:
Laparoscopy: A keyhole surgery technique, laparoscopy allows Dr. Reddy to diagnose and treat issues like ectopic pregnancies, endometriosis, and ovarian cysts without large incisions, leading to quicker recovery.
Hysteroscopy: This procedure is used to examine and treat conditions within the uterus, such as fibroids. By inserting a small camera through the cervix, Dr. Reddy can diagnose and treat uterine issues in a safe, non-invasive way.
These advanced techniques help patients experience less pain and faster recovery, allowing them to resume their normal lives more quickly.
Compassionate and Patient-Centered Care
Dr. Balaji Nalwad Reddy’s patient-centered approach is what truly sets him apart. His ability to listen, explain, and guide each patient through her treatment journey fosters a sense of trust and comfort. Women in Baner and nearby areas can rely on Dr. Reddy for personalized care and support throughout their treatment.
If you are facing an ectopic pregnancy or any other gynecological condition, Dr. Balaji Nalwad Reddy’s clinic in Baner offers top-quality care that combines expertise with compassion.
#gynecological#polycystic ovarian syndrome#premature ovarian failure#chronic fatigue#endometriosis treatment#ovarian#ovarianstimulation#endometriosis#fibroid surgery#ovarian cyst#gynecological health#gynecologicalcare#gynecological services#gynecological problems#ovarian cancer
0 notes
Text
Gynecological Cancer Surgery in Delhi: What You Should Know?
#gynecological cancer surgery in Delhi#best gynecological cancer surgery in Delhi#top gynecological cancer surgery in Delhi#gynecological cancer surgery in Delhi near me
0 notes