#COVID-19 Contact-Tracing
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was the first site to host the blog for President Barack Obama in 2011.
Text
the hse's advice on covid self-isolation is such dogshit. 'you can come out of isolation after 5 days but don't interact with anyone high risk for 10 days' cool how do i know the person sitting next to me on the bus isn't high risk. the person in line behind me getting groceries, the person i make small talk with in the pharmacy queue. literally eugenics-adjacent advice
#before any cretin responds with the 'high risk people shouldn't be going out anyway' oohhh okay so you think high risk people should cocoon#in their rooms for 4+ YEARS so the rest of us get to live normal lives instead of idk enforcing comprehensive contact tracing paid time off#and proper isolation. not to mention the fact that high risk ppl don't just get to peace out from the regiments of capitalism most disabled#people still have to work because guess what? rent groceries utilities LIVING costs money and is often doubly or more expensive for disable#people. goddddd this makes me so mad. anyway#covid#.txt#covid 19
55 notes
·
View notes
Text
23 notes
·
View notes
Text
Revealing the Potential of COVID-19 Contact Tracking Solutions
#LoRa#IoT#Technology#lansitec#Contact Tracing Badge#Covid 19 Contact Tracing Solutions#Contact Tracing Solutions#LoRaWAN#Tracing#Asset Management
2 notes
·
View notes
Text
December 30, 2024
Arijit Chakravarty: “Learn to live with it,” for other diseases doesn’t mean the same thing as we have applied to COVID. When we say we must learn to live with leprosy, we don’t mean let’s make sure everybody has leprosy. When we say we must learn to live with malaria, we don’t mean let’s make sure everyone gets malaria as often as possible, let’s keep mosquitoes lurking in our tanks outside our house. No one says you must learn to live with tuberculosis. Let’s let it spread as much as possible and see how that goes. No, we suppress those diseases every step along the way. We suppress dengue. We suppress tuberculosis. This whole idea that learning to live with the disease means permitting and encouraging its rampant spread and rapid evolution is just so many levels of stupidity that I don’t have a word for it.
Benjamin Mateus: I’d like to know your thoughts on Trump and RFK Jr., his choice for secretary of health? RFK Jr. has been at the head of vaccine disinformation and anti-public health policies. They are calling for ending any cooperation with the World Health Organization. These will have immense consequences for public health globally. These are political questions, but often I hear scientists do not want to engage in political questions and feel uncomfortable about it. Can we avoid the political implications?
AC: Look, it’s not that I don’t want to get political. It’s that if I was going to get political, I don’t know who to hold up as an example. There’s not a government in the world that has handled this correctly. There’s not a party in this world that’s handled it correctly. It’s all different flavors of stupid. Pick your poison. The Democrats went out of their way to normalize mass infection. They went out of their way to lie about the vaccines and say, “If you’re vaccinated, the pandemic was over.” That was completely unnecessary. It was completely at odds with science. Then you have Trump in the first Trump administration saying, “Why don’t you drink some bleach?” It would be a comedy if the consequences weren’t so grave. Frankly, wherever you go it’s like this. You look at Canada’s Bonnie Henry (Canadian epidemiologist and physician) in British Columbia. On day one she insisted that the kids wouldn’t get infected. Then she went and published a paper, put her own name on it, bragging about how herd immunity has been achieved because 90 percent of Canadian kids have been infected. In the UK you had the hearings on the public health response by the UK government. They noted that the government failed to act quickly. There was no clear policy approach, and they even abandoned contact tracing in mid-March of 2020. They even said that masks don’t help stop the spread and the virus wasn’t airborne. It’s a disgrace. Politicians worldwide have decided that they can brazen out their way through this. And the reason for this is they’ve been advised by a certain set of scientists, a relatively small number of scientists, who have essentially sold out. There are tens of thousands of papers, if not hundreds of thousands of papers, on the risks of COVID. You could literally find thousands of scientists who would be willing to go up in front of the House of Representatives and testify that getting COVID repeatedly is bad for you. Where are those scientists? Nobody’s listening to them. They’re listening to the scientists who whisper in their ears and say that everything will be okay. Ryan Gregory and I wrote a Substack blog post a while back called Calm Mongering where we talk about this—that people have weaponized the logic of science in the service of propaganda by saying, “that’s just a hypothesis.” As soon as you bring up a risk, these “experts” shut down the conversation about the risk by saying we’re not sure that’ll happen. But in fact, that’s an inversion of the precautionary principle. And it’s a lot of the tactics that were used by the merchants of doubt during the tobacco era. The merchants of doubt were a subset of a very small number of corrupt, well-connected and well-funded scientists who went out of their way to make public statements that were at odds with the body of literature that was coming out on lung cancer and tobacco. And we are seeing the exact same thing again. Big tobacco sponsored a bunch of corrupt scientists to create a counter-narrative to reality. This time around, who’s playing the role of big tobacco? It’s the politicians and governments. But the exact same thing is playing out. That nexus between this group of corrupt scientists and politicians who are actively funding their work is a global phenomenon. Unfortunately, I hate to say this, but it’s going to take reality breaking through to solve this. They’ve been very effective at convincing people that this is not a problem you need to worry about.
123 notes
·
View notes
Text
The next pandemic is inevitable. Australia isn’t ready - Published Sept 23, 2024
(Before you Americans yell at me, It's already the 23rd in Australia. This is very late-breaking)
I thought this was a really good breakdown of the current situation given the government-approved covid denial we live in. Long, but worth a read.
By Kate Aubusson and Mary Ward
Top infectious disease and public health veterans at the nerve centre of the state’s war against COVID-19 are sounding the alarm.
NSW is less prepared today to fend off a deadly pandemic despite the lessons of COVID-19, say top infectious disease and public health veterans at the nerve centre of the state’s war against the virus.
And we won’t have another hundred years to wait.
NSW’s gold standard Test-Trace-Isolate-Quarantine and vaccination strategies will be useless if a distrusting population rejects directives, refuses to give up its freedoms again, and the goodwill of shell-shocked public health workers dries up.
A panel of experts convened by The Sydney Morning Herald called for a pandemic combat agency akin to the armed forces or fire brigades to commit to greater transparency or risk being caught off guard by the next virulent pathogen and misinformation with the potential to spread faster than any virus.
“It’s inevitable,” says Professor Eddie Holmes of the next pandemic. A world-leading authority on the emergence of infectious diseases at the University of Sydney, Holmes predicts: “We’ll have less than 100 years [before the next pandemic].
“We’re seeing a lot of new coronaviruses that are spilling over into animals that humans are interacting with,” said Holmes, the first person to publish the coronavirus genome sequence for the world to see.
“People are exposed all the time, and each time we are rolling the dice.”
The independent review of NSW Health’s response to COVID-19 opened with the same warning: “No health system or community will have the luxury of 100 years of downtime.”
Pandemic preparedness needs to be a “permanent priority”, wrote the report’s author, Robyn Kruk, a former NSW Health secretary, “rather than following the path of those that have adopted a ‘panic and forget strategy,’ allowing system preparedness to wane”.
Why we don’t have 100 years to wait for the next pandemic The World Health Organisation has declared seven public health emergencies of international concern since 2014, including the current mpox outbreak.
Climate change is turbocharging the factors that coalesce to create the perfect breeding ground for a pandemic-causing virus, including population increases, bigger cities, and better-connected global markets and migration.
“Animals will be forced into more constrained environments, and humans that rely on those environments will be again constrained in the same environments. There will be more wet markets, more live animal trade that will just increase exposure,” Holmes said.
“It was clear that we weren’t ready [for COVID],” said Jennie Musto, who, after seven years working for the World Health Organisation overseas, became NSW Health’s operations manager for the Public Health Emergency Operations Centre, the team responsible for NSW’s COVID-19 contact tracing and containment.
“Everyone had preparedness plans gathering dust on a shelf, but no one was actually ready to respond, and so everyone was on the back foot,” Musto said. “Perhaps none of us really thought this was going to happen. We were waiting 500 years.”
Who would willingly become the next doomed whistleblower? Eddie Holmes, known for his repeated assertion that SARS-CoV-2 did not come from a lab, is deeply concerned that when the next pandemic-causing virus emerges, chances are it will be covered up.
“My worry is that if the virus appeared in a small population, say, somewhere in Southeast Asia, the people involved wouldn’t blow the whistle now, given the fact that you would get blamed,” he said.
Li Wenliang, the Wuhan doctor who tried to raise the alarm about a virulent new virus, was reportedly reprimanded by police for spreading rumours and later died of COVID-19.
The global blame game, culminating in a deep distrust of China and accusations that the virus was grown in a Wuhan lab, is why Holmes believes “we’re in no better place than we were before COVID started, if not worse”.
“I work with a lot of people in China trying to keep the lines of communication open, and they’re scared, I think, or nervous about saying things that are perceived to counter national interest.”
From a vaccine perspective, our defences look strong. There have been monumental advancements in vaccine development globally, driven by mRNA technology. In Sydney this month, construction began on an RNA vaccine research and manufacturing facility.
“But the way I see it is that nothing has been done in terms of animal surveillance of outbreaks or data sharing. The [global] politics has got much, much worse,” Holmes said.
Combat force Conjoint Associate Professor Craig Dalton, a leading public health physician and clinical epidemiologist, called for a dramatic expansion of the public health workforce and the establishment of a pandemic combat force that would routinely run real-time pandemic simulations during “peacetime”.
“No one is upset with fire brigades spending most of the time not fighting fires. They train. A lot. And that’s probably how we need to move,” he said.
“We need exercise training units so that every major player in pandemic response is involved in a real-time, three to four-day pandemic response every three to five years at national, state and local [levels].”
The federal Department of Health and Aged Care recently ran a health emergency exercise focused on governance arrangements involving chief health officers and senior health emergency management officials, a spokeswoman for Health Minister Mark Butler said. The outcomes of this exercise will be tested later this year.
Dalton said desktop simulations and high-level exercises involving a handful of chiefs didn’t cut it, considering the thousands of people working across regions and states. He instead suggested an intensive training program run in the Hunter New England region before the 2009 H1N1 pandemic provided a good model.
“We were ringing people, actors were getting injections, just like a real pandemic,” said Dalton, who once ordered a burrito in a last-ditch effort to contact a restaurant exposed to COVID-19.
Our heroes have had it The expert panel was emphatic that our pandemic response cannot once again rely on the goodwill of the public health and healthcare workforce.
According to the Kruk review, what began as an emergency response ultimately morphed from a sprint into an ultra marathon and “an admirable (yet unsustainable) ‘whatever it takes’ mindset”.
They were hailed as heroes, but the toll of COVID-19 on healthcare workers was brutal. Workloads were untenable, the risk of transmission was constant, and the risk of violence and aggression (for simply wearing their scrubs on public transport in some cases) was terrifying.
“We got through this pandemic through a lot of people working ridiculous hours,” Dalton said.
“You talk to a lot of people who did that and say they could not do it again.”
Tellingly, several expert personnel who worked at the front lines or in the control centre of NSW’s pandemic defences were invited to join the Herald’s forum but declined. Revisiting this period of intense public scrutiny, culminating in online attacks and physical threats, was just too painful.
So long, solidarity Arguably, the biggest threat to our pandemic defences will be the absence of our greatest strength during COVID: the population’s solidarity and willingness to follow public health orders even when it meant forfeiting fundamental freedoms.
The public largely complied with statewide public health orders, including the stay-at-home directive that became the 107-day Delta lockdown, and other severe restrictions prevented many from being at the bedside of their dying loved ones, visiting relatives in aged care homes and attending funerals.
“My worry is that next time around when those sorts of rules come out, people may say, ‘Well, don’t worry about it.’ They relax it in the future. Why don’t we just not stick to the rules?” said Professor Nicholas Wood, associate director of clinical research and services at the National Centre for Immunisation Research and Surveillance.
“I’m not sure we quite understand whether people [will be] happy with those rules again,” he said.
Dalton was more strident.
“I tend to agree with Michael Osterholm … an eminent US epidemiologist [who] recently said the US is probably less prepared for a pandemic now than it was in 2019, mostly because the learnings by health departments in the COVID pandemic may not make a material difference if faced with a community that distrusts its public health agencies,” he said.
“If H1N1 or something else were to spill over in the next couple of years, things like masks, social distancing and lockdowns would not be acceptable. Vaccination would be rejected by a huge part of the population, and politicians might be shy about putting mandates in.”
As for the total shutdown of major industries, people will struggle to accept it unless the next pandemic poses a greater threat than COVID, said UNSW applied mathematician Professor James Wood.
The risk of the virus to individuals and their families will be weighed against the negative effects of restrictions, which are much better understood today, said Wood, whose modelling of the impact of cases and vaccination rates was used by NSW Health.
“Something like school closure would be a much tougher argument with a similar pathogen,” he said.
A previous panel of education experts convened by the Herald to interrogate pandemic decision-making in that sector was highly critical of the decision to close schools for months during NSW’s Delta lockdown.
Greg Dore, professor of infectious diseases and epidemiology at the Kirby Institute, said the public’s reluctance to adhere to restrictions again may, in part, be appropriate.
“Some of the restrictions on people leaving the country were a bit feudal and too punitive,” he said. “Other restrictions were plain stupid, [for instance] limitations on time exercising outside.”
Meanwhile, the delays to publicly recognise the benefits of face masks and the threat of airborne transmission “ate away at trust”, Dalton said.
“We shouldn’t make those mistakes again,” he said.
Transparent transgressions Uncertainty is not something politicians are adept at communicating, but uncertainty is the only constant during a pandemic of a novel virus.
Vaccines that offered potent protection against early iterations of the COVID virus were less effective against Omicron variants.
“[The public], unfortunately, got hit by a rapid sequence of changes of what was ‘true’ in the pandemic,” James Wood said.
Political distrust can be deadly if governments give the public reason to suspect they are obfuscating.
The expert panel urged NSW’s political leaders to be far more transparent about the public health advice they were given before unilaterally enforcing restrictions.
There was a clear line between public health advice and political decision-making in Victoria. The Victorian chief health officer’s written advice was routinely published online.
In NSW, that line was blurred as Chief Health Officer Kerry Chant stood beside political leaders, most notably former premier Gladys Berejiklian, at the daily press conferences.
Public health experts said that they looked for subtle cues to determine the distinction between the expert advice and the political messaging during press conferences, paying attention to body language, who spoke when and who stayed silent.
“It is fine for public health personnel to have a different view to politicians. They have different jobs. What is not OK is to have politicians saying they are acting on public health advice [when they are not],” he said.
The ‘whys’ behind the decisions being made were missing from the daily press conferences, which created “a vacuum for misinformation”, said social scientist and public health expert Professor Julie Leask at the University of Sydney.
“The communication about what you need to do came out, and it was pretty good … but the ‘why we’re doing this’ and ‘what trade-offs we’ve considered’ and ‘what dilemmas we’ve faced in making this decision’; that was not shared,” Leask said.
The infodemic In the absence of transparency, misinformation and disinformation fill the vacuum.
“We had an ‘infodemic’ during the pandemic,” said Dr Jocelyne Basseal, who worked on the COVID-19 response for WHO in the Western Pacific and leads strategic development at the Sydney Infectious Diseases Institute, University of Sydney.
“The public has been so confused. Where do we go for trusted information [when] everyone can now write absolutely anything, whether on Twitter [now called X] or [elsewhere] on the web?” Basseal said.
A systematic review conducted by WHO found misinformation on social media accounted for up to 51 per cent of posts about vaccines, 29 per cent of posts about COVID-19 and 60 per cent of posts about pandemics.
Basseal’s teenage children recently asked whether they were going into lockdown after TikTok videos about the mpox outbreak.
“There is a lot of work to be done now, in ‘peacetime’ … to get ahead of misinformation,” Basseal said, including fortifying relationships with community groups and teaching scientists – trusted and credible sources of information – how to work with media.
In addition to the Kruk review’s six recommendations to improve its pandemic preparedness, NSW Health undertook a second inquiry into its public health response to COVID-19, which made 104 recommendations.
NSW Health Minister Ryan Park said: “We are working hard to ensure the findings and recommendations from those reports are being implemented as quickly as possible.”
The expert panellists spoke in their capacity as academics and not on behalf of NSW Health or WHO.
The ‘As One System’ review into NSW Health’s COVID-19 response made six recommendations 1. Make governance and decision-making structures clearer, inclusive, and more widely understood 2. Strengthen co-ordination, communication, engagement, and collaboration 3. Enhance the speed, transparency, accuracy, and practicality of data and information sharing 4. Prioritise the needs of vulnerable people and communities most at risk, impacted and in need from day one 5. Put communities at the centre of emergency governance, planning, preparedness, and response 6. Recognise, develop and sustain workforce health, wellbeing, capability and agility.
#mask up#covid#covid 19#pandemic#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator
154 notes
·
View notes
Text
Dear readers: Please welcome this sponsored educational piece from Above Phone. This company is at the forefront of the fight against constant surveillance, empowering individuals to “take back our tech” and reclaim control over their digital lives.
“As we embrace our new normal, MassNotify is a voluntary, free tool to provide additional peace of mind to residents as they return to doing the things they love.”
—MA Governor Charlie Baker
In the summer of 2021, Massachusetts residents saw a notification on their phones prompting them to update a COVID-19 contact tracing application. Only one problem - they had never installed one. How did the app get on their phone without them knowing and without their consent?
15 notes
·
View notes
Text
therealwakeel
blackaliensxyz•Original audio
Liked by
gregorysims24 and 125 others
therealwakeelwas a trial run They create FEAR too control people. It was all an experiment. The wicked elite won't stop until they can control all A lot of you folded and took that "jump shot" KNOW WHO YOUR ENEMY IS!15h
therealwakeel1. COVID-19 was the test of social responsibility-A huge number of unimaginable restrictions for public health were adopted by billions of citizens across the world. There were numerous examples globally of maintaining social distancing, wearing masks, mass vaccinations and acceptance of contact-tracing applications for public health, which demonstrated the core of individual social responsibility15h1 likeReply
maccymazAnd people still won’t wake up to what’s happening In their faces and could tattoo it on their forehead and still would t believe us4h3 likesReply
13 notes
·
View notes
Text

They wanted to know how many people would comply with a complete re-ordering of their lives based on no science at all, just random orders, some of which bordered on absurdity.
I have long said that Covid 19 was launched by design by a small number of people in the globalist predator class for one reason and one reason only — as a beta test for the coming technocratic new world order.
Now, we’ve got the World Economic Forum coming out and all but admitting that was exactly why the Covid-19 “pandemic” had to happen.
The WEF gleefully posted the following snippet to the “My Carbon” page of its website where they make a pitch for so-called smart cities, which is just another term for 15-minute cities.
The first of three “developments” that the WEF says must be in place before the world can evolve into its utopian vision of “smart and sustainable cities,” is compliance with restrictions on our freedom. It writes:
1. COVID-19 was the test of social responsibility – A huge number of unimaginable restrictions for public health were adopted by billions of citizens across the world. There were numerous examples globally of maintaining social distancing, wearing masks, mass vaccinations and acceptance of contact-tracing applications for public health, which demonstrated the core of individual social responsibility.
They were testing us. That’s what Covid was all about. They wanted to see how many of us would give up our individual freedom and individual sovereignty by complying with a “new normal” that consisted of restrictions bordering on the absurd.
Why, for instance was it “safe” to shop at Lowe’s or Home Depot but unsafe to shop at a small business or attend church? Why was it OK to go to strip clubs in Michigan but you couldn’t buy seeds for a garden?
What the WEF is implying with its above statement is that in order to be “sustainable,” people and societies will need to be compliant with a new more authoritarian global order. Don’t ask questions. Don’t resort to logic. Just obey.
Would we be obedient in the face of idiotic new laws and regulations, like wearing face diapers to stop what was said to be an aerosolized virus, and standing six feet apart in public, and submitting to a never-before-used, unlicensed mRNA gene-based injection?
They said it was good for you, so roll up your sleeve. Don’t ask questions. If you did, you could lose your job and be treated as a societal outcast. Many people lost friends or even close family members to this monstrous “test” of our willingness to unquestioningly do what we’re told.
Nearly five years later, arguably the most powerful nonprofit public-private partnership in the world, the WEF, admits it was all a test of our wills and celebrates the fact that most of us failed the test (or passed with flying colors depending how you look at it).
They wanted to find out how many of us would prove our servitude to the lawless, fascistic beast system by complying with “unimaginable restrictions,” many of which were created out of thin air with absolutely no scientific evidence to back them up as contributing anything to public health.
The U.S. government’s top health bureaucrat, Dr. Anthony Fauci, admitted recently that there was no science behind his decision to require Americans to socially distance six feet apart.
youtube
The beta test known as Covid-19 proved once again the validity of the The Milgram Experiment. This experiment was conducted in 1961-1962 by Yale University professor Stanley Milgram.
It showed that the overwhelming majority of Americans would obey a law or command that they knew was wrong if the order were to come from an official authority figure. An alarming 65 percent of Americans would reluctantly violate their own conscience and obey the order even if they knew it would result in the death of an innocent person.
Trending: Here’s the Real Reason Why Hunter Biden Shocked the Courtroom and Pleaded Guilty in Federal Tax Evasion Case
From Wikipedia:
Beginning on August 7, 1961, a series of social psychology experiments were conducted by Yale University psychologist Stanley Milgram, who intended to measure the willingness of study participants to obey an authority figure who instructed them to perform acts conflicting with their personal conscience. Participants were led to believe that they were assisting an unrelated experiment, in which they had to administer electric shocks to a “learner.” These fake electric shocks gradually increased to levels that would have been fatal had they been real.
The experiments found, unexpectedly, that a very high proportion of subjects would fully obey the instructions, with every participant going up to 300 volts, and 65% going up to the full 450 volts. Milgram first described his research in a 1963 article in the Journal of Abnormal and Social Psychology[1].
The Bad News is that we passed the test with flying colors.
11 notes
·
View notes
Text
🧬 How Long Is the COVID-19 Incubation Period?
The COVID-19 incubation period—the time between getting infected and showing symptoms—has shaped almost every aspect of our pandemic response. From quarantine durations to testing strategies, this invisible countdown plays a huge role in public health.
Let’s break it down 👇
📌 What’s the average incubation period?
Studies show that most people who catch SARS-CoV-2 develop symptoms between 3 to 14 days after exposure, with the median around 5 days.
This is why 14-day quarantines were the norm early in the pandemic—it covers almost everyone who might get sick.
But it’s not that simple.
🧫 What influences this timeline?
Several external and internal factors can affect how long it takes symptoms to appear:
Viral variants: Delta vs. Omicron? Omicron tends to show up faster (2–4 days).
Vaccination: Immune systems may respond quicker in vaccinated people, possibly shortening symptom onset.
Age & health: Older or immunocompromised individuals might show symptoms later—or not in typical ways.
Exposure level: High viral load (like close, prolonged contact) can speed things up.
So no, it’s not always five days. Context matters.
🔁 Why does the incubation period matter?
Because people can spread COVID-19 even before symptoms start. That means:
Testing too early can give false negatives
Pre-symptomatic transmission is a real thing
Contact tracing needs to account for 2–3 days before symptom onset
It’s not just about when you feel sick—it’s about when you’re contagious.
🚨 The problem with misinformation
There’s been confusion online—especially early in the pandemic—around what incubation really means:
Some confused it with the infectious period
Others spread stories of “20+ day incubations” without evidence
Misunderstandings led to distrust in health guidelines
As the virus evolves, so must our understanding. Each variant may come with a slightly different clock.
🧠 TL;DR
Most people show symptoms 3–14 days after catching COVID-19
The median is 5 days, but new variants like Omicron can be quicker
Factors like vaccination, age, and exposure matter
Knowing the incubation period helps shape testing, quarantine, and tracing policies
Stay updated—data changes as the virus changes
🔍 Sources
Lauer et al., Annals of Internal Medicine, 2020
CDC COVID-19 Guidelines (cdc.gov)
WHO COVID-19 Dashboard
McAloon et al., BMJ Open, 2020
#covid19#epidemiology#publichealth#scienceblog#healthinfo#pandemic#science#omicron#vaccineswork#pubmed
3 notes
·
View notes
Text
Le Forum économique mondial (WEF) a admis que la pandémie de COVID-19 était un test de l'obéissance du public à accepter son Nouvel Ordre Mondial il a publié l'admission suivante sur la page "Mon carbone" de son site web où ils font un pitch pour les villes intelligentes de 15 minutes Thegatewaypundit.com rapporte : Le premier des trois "développements" qui, selon le WEF, doivent être en place avant que le monde puisse évoluer vers sa vision utopique des "villes intelligentes et durables", est le respect des restrictions à notre liberté. Il écrit :
1. COVID-19 a été le test de la responsabilité sociale - Un grand nombre de restrictions inimaginables pour la santé publique ont été adoptées par des milliards de citoyens à travers le monde. Il existe de nombreux exemples à l'échelle mondiale de maintien de la distanciation sociale, de port du masque, de vaccinations de masse et d'acceptation des demandes de recherche des contacts pour la santé publique, qui ont démontré le cœur de la responsabilité sociale individuelle.
Ils nous testaient. C'est ce qu'était le Covid. Ils voulaient voir combien d'entre nous abandonneraient notre liberté individuelle et notre souveraineté individuelle en se conformant à une "nouvelle normalité" qui consistait en des restrictions à la limite de l'absurde. Pourquoi, par exemple, était-il "sûr" de faire ses achats chez Lowe's ou Home Depot, mais dangereux de faire ses courses dans une petite entreprise ou d'aller à l'église ? Pourquoi était-il acceptable d'aller dans des clubs de strip-tease dans le Michigan mais vous ne pouviez pas acheter de graines pour un jardin ? Ce que le WEF implique avec sa déclaration ci-dessus, c'est que pour être "durables", les personnes et les sociétés devront se conformer à un nouvel ordre mondial plus autoritaire. Ne pose pas de questions. Ne recourez pas à la logique. Il suffit d'obéir. Serions-nous obéissants face à de nouvelles lois et réglementations idiotes, comme porter des couches pour arrêter ce qui était considéré comme un virus en aérosol, et se tenir à 3 mètres l'un de l'autre en public, et se soumettre à une injection non autorisée d'ARNm jamais utilisée auparavant ?

WEF has admitted that the COVID-19 pandemic is a test of the public’s obedience to its New World Order, posting the following admission on the “My Carbon” page of its website where it makes a 15-minute pitch for smart cities. Thegatewaypundit.com reports: The first of three “developments” that the WEF says must be in place before the world can move toward its utopian vision of “smart, sustainable cities,” is compliance with restrictions on our freedom. It writes: 1. COVID-19 has been the test of social responsibility - A large number of unimaginable public health restrictions have been adopted by billions of citizens around the world. There are many examples worldwide of maintaining social distancing, wearing masks, mass vaccinations, and accepting contact tracing requests for public health, which have demonstrated the heart of individual social responsibility. They were testing us. That’s what Covid was. They wanted to see how many of us would give up our individual freedom and individual sovereignty by conforming to a “new normal” that consisted of restrictions that bordered on the absurd. Why, for example, was it “safe” to shop at Lowe’s or Home Depot, but dangerous to shop at a small business or go to church? Why was it okay to go to strip clubs in Michigan but you couldn’t buy seeds for a garden? What the WEF is implying with their statement above is that in order to be “sustainable,” people and societies will have to conform to a new, more authoritarian world order. Don’t ask questions. Don’t resort to logic. Just obey. Would we be obedient to idiotic new laws and regulations, like wearing diapers to stop what was considered an aerosolized virus, and staying 10 feet apart in public, and submitting to an unauthorized mRNA injection never before used?
6 notes
·
View notes
Text
I've caught covid for the first time, after somehow managing to avoid it for almost 4 years, and it thoroughly sucks. I'm far from the only one at the moment (I'm writing this on 8 december 2023) - testing fascilities are all done away with in the Netherlands so the view of the current situation I have is very limited, but I do know that numbers like virus load in our sewers and people in hospital with covid are rapidly going up right now once again.
I'm having a lot of thoughts about it all now, and even though they are far from coherent, I still would like to share them.
In the Netherlands, so far there's been a staggering lack of reflection on anything to do with corona. We have no official moment of rememberance, no monument, no time and place for collective grief. Research into long covid is severely underfunded. There's also been an astounding lack of evaluation into our pandamic response. I've only seen one report so far, and it had a limited scope, pretty much the only conclusion was that the goverment's strategy was 'too fixated on intensive care capacity'. If another new illness will emerge, which of course is only a matter of time, I believe we will make all the same mistakes again.
In summary, I just feel sad and kind of hopeless by it all. The lack of care for the lives of eldery and otherwise vulnerable people, and just for public health in general, displayed during the past years, and all for the sake of corporate interest and personal freedom, is staggering. It all started quite promising, back in March 2020, once it dawned on our government that COVID-19 was a serious illness and that immediate action was required. I myself had basically no knowledge on pandemics yet and the lockdown blew my mind. We were taking action to save lives. I remember feeling hopeful.
But pretty much from the moment we emerged from the first lockdown, our government has each time waited with taking measures until the last possible moment. In comparison to the rest of the world, response was not the worst (at least no outright corona denial or 'drink bleach' here), but it was not good either. The Dutch government basically went 'this is fine' meme until hospitals overflowed (long term health care facilites were barely even considered) and then they panicked, putting lockdowns into place again while those are only really meant as an emergency measure when all else fails. Coherent, preventive measures like testing, masks, clear information, ventilation, contact tracing and isolation were never properly put into place.
And now we've lost tens of thousands of lives prematurely, hospital patients with covid still vastly outnumber those with influenca even in bad years, many still report pandemic-related mental health issues, and an estimated 90.000 people in the Netherlands currently have long covid, including a good friend of me.
I feel like all were in a traumatic event that isn't even over yet, and we're barely even talking about the impact, and the next one will inevitably come and likely just be as bad. It's just a lot.
#corona#pandemic#covid#personal#rambling thoughts#feels good to get this off my chest#covid19#I'll be fine I hope#netherlands#europe#dutch things
9 notes
·
View notes
Text
This interview was conducted with a public health employee of the Hawaii State Department of Health (HIDOH), as part of the WSWS Global Workers’ Inquest into the COVID-19 Pandemic. The worker chose to use the pseudonym Robert to protect their identity.
Evan Blake (EB): Thank you for participating in the Global Workers’ Inquest into the COVID-19 Pandemic, it’s a pleasure to interview you. Can you describe your background and training in public health before the pandemic?
Robert (R): My training in public health began more than 25 years ago, initially centered on women’s reproductive health. I earned a degree in Public Health. My focus soon broadened from just women’s health to everyone’s due to the ongoing HIV/AIDS crisis.
Throughout my career, I collaborated with various organizations, including academic institutions and community health centers, to develop programs targeting most of the populations in the Bay Area. These initiatives encompassed health education, addiction support, and promoting healthy relationships, as well as offering HIV/AIDS and HCV [hepatitis C]testing, counseling, contact tracing, case management and patient navigation services. When I moved to Hawaii, I continued doing health education and working with those experiencing developmental disabilities, aging and chronic illnesses.
EB: What were your initial experiences when the pandemic began in early 2020? How would you characterize the initial pandemic response of DOH [Department of Health] and state officials more generally in Hawaii?
R: I noticed in December 2019, when there was talk of unusual illness in China’s news and social media. Seeing how it was being handled there made me concerned. There seemed to be more effort in hiding it than in handling it.
I waited for our government to mention it, especially on a more local level. I really thought that since, historically, the Hawaiian Kingdom has had effective quarantine and mitigation practices, that the current leadership would follow suit. My thinking was that we don’t have rabies in Hawaii, so obviously we know how to keep viruses out.
By February, I started contacting the DOH to hire me to help out any way possible. This looked like something that could easily be squashed if they rounded up all the HIV experts and put them to work. In early March, I put my disabled clients on quarantine. I bought a bunch of fabric and a serger and my family and I made hundreds of masks. Airborne transmission has always been known.
On March 4, 2020, Hawaii’s Democratic Governor David Ige declared a state of emergency in response to COVID-19, granting the state greater flexibility in responding to the crisis. This is officially when the problems with disappearing COVID funds began. On March 26, Ige issued a stay-at-home order, closing nonessential businesses and implementing strict travel restrictions.
I participated in the statewide Lt. Governor’s COVID town halls. Stay-at-home orders in March and May helped keep the numbers low. I waited for the health department to do something and cranked out masks. Schools had gone online at this point. It went pretty well for us. My kid’s school was really proactive about making sure the kids had access to what or who they needed, including computers.
My partner was labeled an essential worker because he was in construction. His boss took full advantage of this allowance and I wrote several of our state’s representatives who seemed actively concerned about COVID, about what to do in this situation.
By the end of May 2020, Dr. Mark Mugiishi, the chief executive of HMSA, brokered a deal with the UH Manoa nursing school to provide students to be trained as contact tracers. They were supposed to have seven different cohorts, but they stopped at three or four. Most of the trainees were never hired to do any work in the DOH and a majority of the graduates got letters stating thanks, but no thanks. The DOH only ever brought on a couple hundred contact tracers. That was after they got in trouble for not having enough and refusing help.
All the tracers and investigators started out being hired by agencies other than the DOH. This meant that we had no rights, but we had the same responsibilities as any other employee would have. We didn’t get hazard pay, union, or PTO, couldn’t participate in any of the benefits or mental health support and other programs they regularly provided and encouraged all employees to participate in. Most of us worked from 7 a.m. to late in the evening most nights. Most tracers and investigators were not from the locally COVID-trained cohorts.
A majority of the COVID hires weren’t brought in until much later in 2020 or in 2021. More were needed and available and instead of hiring tracers or case management, a call center was contracted to bottleneck the high volume of calls and cases.
State officials are notoriously reactive to any problem, emergency-related or not. The officials in charge of HIDOH when the pandemic was officially recognized were ill-fitted for their positions. Their responses were lackluster at best, with Sarah Park (state epidemiologist, COVID response leader) coming in to the UH Manoa COVID trainings to tell us that contact tracing was ineffective, as well as other disease mitigation techniques that we were being trained on, like routine screening.
When the contact tracing program started at the DOH, the National Guard was tasked with training us and facilitating most of the COVID mitigation efforts. This was after they had only received one day of training themselves. I met not one of them who had any health background whatsoever.
It’s been a performative disaster from the very start. Our DOH and state leadership were instrumental in encouraging the spread of COVID-19. State officials were slow to respond and, when they did, it was never an appropriate response. Hawaii usually sees at least 30,000 visitors per day from all over the world. They did everything in their power to keep that going.
EB: You mentioned that DOH employees were split up into different groups, including groups working with prisoners, homeless people, sports personnel, the wealthy, etc. Can you describe this in more detail and the class divide in the pandemic response in Hawaii?
R: DOH employees as a whole are siloed and do not collaborate or even have the slightest clue what the others are doing ever. It was difficult trying to get resources or info from within when trying to access data or connect people with other services. It was deeply embarrassing to me sometimes how incompetent everyone was.
For the pandemic efforts, the entire venture was militarized and we were beholden to chain of command operations as civilians. We were not allowed to speak to our higher-ups. Many were discouraged from speaking to anyone.
The contact tracing and case investigation were separated into several different focus groups headed by epidemiologists. These epidemiologists already had a disease focus and their loads were not lightened. They were added to. Most of them are not in fact actual trained epidemiologists. They have fallen into the position often through nepotistic means and meet bare minimum educational requirements. They had a lot of weird toxic drama that affected program function overall.
For example, if your team’s epidemiologist didn’t get along with a different team’s epidemiologist and you needed a file or lab result or info about an individual in their category, they may delay the info or just never give it to you. It was the worst addition to an already extreme high-stress situation.
The main group management often fell to the inexperienced National Guard, who were under the epidemiologists. Each group’s numbers fluctuated and usually had about 7–15 people, half National Guard, half civilian. The focuses were separated into schools, food service, military, healthcare and LT facilities, travel/VIP, Pacific Islander, severe/death, correctional facilities and homeless.
We had to wait for the daily cases to be handed to the epidemiologists. They would post new cases as they were processed into the system usually via an external call center, who received the cases mostly via the department’s only fax machine.
HIDOH hired an external call center to handle what was called first contact calls. This was actually one of the biggest obstructions to actual contact tracing or any real handling of infected patients in a timely manner.
First contact call center got the first reporting of the case. The report would come in via fax (another massive problem). That person’s name and number would be taken down and someone from the call center or the National Guard would call and ask screening questions about their health and symptoms, often with not much health training. They had three days for the individual to answer before they stopped calling and threw it out.
By the time investigators or tracers got the case, it was often 5–10 days old. We never did real contact tracing in the department. Real contact tracing would involve calling the case immediately to help them trace and notify anyone who may have been exposed. It would also involve timely and actual distribution of resources, including testing, food and money. This is not what happened.
I saw hundreds of people who were overqualified for resources denied or provided the offered resources too late. Some tracers did what could be considered “guerrilla tracing” because they had their contact info passed around for those who needed help and couldn’t get through to the health department when they needed to, or they just needed resources or their results.
A majority of people who were infected did not receive a call from the DOH or any help. They also didn’t receive guidance on quarantine or health at all. Internally, there was never training or updating on variants, pathology or how to ask sensitive questions and talk to the general public. There was a lot of secrecy and internal guidance that wasn’t health-oriented or generally useful. It was often self-congratulatory and bloviated.
This all increased the class divide as those in the service industry couldn’t afford to heal or get better and many lost and are losing their jobs. Those who were able to sealed themselves away. Admin stayed in their offices and told no one to enter, and there was an increase in work-from-home jobs for those with privilege or education, like myself.
EB: Hawaii has the highest per capita number of active US military personnel of any US state and is the state’s largest income producer, yet tourism is often claimed to be the state’s dominant industry. What were the roles of the military and the tourism industry in relation to the pandemic?
R: The military has largely handled their own COVID cases, navigation, and often not sharing when they have clusters that directly impact civilians.
The tourism industry has a finger in everything. They have been extremely instrumental in helping COVID spread. Tourism interests are largely against the people of Hawaii, who are more often harmed than helped by their existence. Tourism and business degrees are what steers most of the boards of every institution in this state. You will find significantly more business degrees than Kanaka (Hawaiian person) representing leadership in the islands. Tourism is why most of those whose birthright is the islands are homeless or not in the islands.
Both industries had large roles in facilitating spread. They pushed to keep everything open and often refused to cooperate with the HIDOH in COVID mitigation efforts.
EB: How have the federal pandemic funds approved under Trump and Biden been dispersed within Hawaii? Can you describe any corruption or negligence that you’ve seen in this regard?
R: I can pretty much only describe corruption and negligence regarding the usage of funds. The HIDOH let over 30 million dollars’ worth of badly needed COVID tests go to waste and then spent over $60,000 to destroy them. The schools never saw much of the Elementary and Secondary School Emergency Relief (ESSER) funds put to use in the schools for mitigation efforts. Countless non-profits denied resources to the community. A robot dog was purchased to test homeless people for COVID, over $1 million were spent on Thanksgiving turkeys in Maui. Oahu’s police department got a bunch of new toys.
The HIDOH never upgraded their information transmission capabilities. They depended on two fax machines for the entirety of the COVID efforts, meaning that all data and case info was transmitted through these machines, slowing down any work or real efforts.
The machines ran over the weekend and whoever was on the following Monday had literal piles of data to enter into the system for reported cases, hospital data, etc. The whole venture has been performative negligence. The funding was better and more resources were distributed while Trump was president. Biden is an absolute disgrace, considering he campaigned on getting rid of COVID.
Most of the funds that could have been used to improve the community and help mitigate COVID were used irresponsibly and have been absorbed by the state. Governor Ige went out of his way to pass legislation that approved shady usage of funds and halt transparency. Governor Green is even worse. The COVID response was just a preview for how Green is handling the Lahaina fires.
EB: Schools reopened with less and less mitigation measures each year, causing repeated waves of mass viral transmission. Can you describe this process and the public health measures you advocated for them to implement? What was the response of various officials to your efforts? How are you seeing the impacts on children, including with Long COVID?
R: The 2020 school response was much better than the following years. Students were provided Chromebooks and instruction from their teachers. It wasn’t implemented in a way that made it easy for many instructors and families, but it was the safest option that was provided.
The following year, the district (the state has only 1) offered something completely different.
In-person instruction or a program for those staying home, that required the parent or caregiver to spend 4–6 hours per day implementing. With no live teachers or real support offered from the school or Department of Education (DOE). The schools who offered it didn’t even know what it was or how it functioned. They just referred parents to the program’s website or phone number if they needed any assistance.
Often parents who required more support or Special Education (SPED) services for their children were ignored, punished, had CPS called on them, or were harassed by some school’s staff and admin.
In many of the poorest areas, where much of our service industry workforce resides, the schools didn’t even offer an alternative to in-person classes. I’m in one of these areas and I removed my child from her school after they refused to provide any support or programming besides that awful program they were offering which forced the parent to provide instruction without support. I already had a job. They called CPS on me. They would send staff to my door every week to sign unnecessary paperwork. They did this for two years. Officials didn’t care. The School’s Superintendent and the super for my area was never even available and never returned calls. I called weekly. I was working on so many cases connected to our schools the whole time, it was no question about removing my kid.
None of the public schools had their air systems improved or HEPA filters added. Some were using hand sanitizer on children’s desks in between classes when they were supposed to sanitize them properly. There wasn’t any solid guidance provided to the schools. Every time I got through to a school nurse or principal about a case, they begged for info on what to do and how to handle mitigations with all the sickness.
Sickness in children and school staff wasn’t being reported accurately because contact tracers were instructed not to connect cases in the classroom with each other. This kept the cluster report low. Many teachers were punished for mentioning their own infections and they were not allowed to notify students’ parents either. This devastated our community, since it has one of the highest counts of multigenerational households in the nation.
Josh Green, who is now Hawaii’s governor, was the head of the COVID Task Force. His main messaging has only ever been regarding vaccines. He spent a significant amount of time pointing the finger at many of our Pasifika communities in regard to their vaccine hesitancy instead of working with them to mitigate COVID in other ways.
When the 2021–22 school year started, the district was ill-prepared and kids weren’t approved for vaccines yet. The school’s superintendent, Christina Kishimoto, was completely useless at getting any mitigations in the schools at all. She ignored the entire community, including so many teachers and parents who tried to keep or make the schools, or at least education, safe and accessible to all.
Senator Brian Schatz and others who had been previously notified about in-school spread and the actual numbers present instead of the falsely low reported ones, maintained the script that children needed to learn in-person. Even after in-person learning saw children being shoved together in cafeterias all day without proper instruction due to sick staff, those in charge maintained that the children needed to be in schools. This was supposedly for their mental health and education, which had never been prioritized previously.
Hawaii has had a major deficit in adequate and accessible education, as well as mental health care providers and services, for a very long time. Additionally, we don’t have school nurses in each school like many contiguous states offer. Many of our schools share a nurse and may not have an area for children to be sick or wait for someone to get them from school.
In-school cases often fell to vice principals and other staff. By the 2022–23 school year, schools had removed any guidance that was useful. They never upgraded or improved the air systems. Many of our schools have had problems with lack of proper air conditioning for a long time before the pandemic. The pandemic just made it worse.
There was a program created at the start of the 2022–23 school year to make the DOH, DOE and CDCF work together to improve the conditions in the schools. The HIDOE refused to meet or participate in any improvements to their school’s systems, provide resources such as testing, PPE or pandemic guidance.
Our state leadership has met with many COVID experts, DOH employees and medical staff who have told them what is happening in their districts, classrooms, hospitals and the community throughout the official pandemic and even now. They all have given lip-service and often have reacted appropriately in those meetings but nothing ever comes of it.
At first, children were just getting cold-like symptoms like everyone else. Those who had existing health issues usually suffered more. Not many children’s cases were followed past the initial call. Over time, Multisystem Inflammatory Syndrome in Children (MIS-C) became a focus as the children’s symptoms didn’t always go away.
Since Omicron emerged in November 2021, kids have had an increase in seizures and a lot of problems with focus and memory. My child has had several friends die from COVID. Long COVID in kids is terrifying, and the impact is already noticeable. Mine just stated that what everyone needs to know is that it’s harder for kids to learn now. She notices so much brain damage in her peers already. Before she got COVID, it was easier for her to process information. Things take much longer now.
To be honest, I’ve rarely seen an actual full recovery. People move benchmarks and brain damage is extremely hard to self-identify. COVID is long and lasting. Nearly every infection shows damage whether it’s noticed or not. For those who don’t have immediate consequences, it’s playing the long game.
EB: How else are you seeing the ongoing impacts of the pandemic associated with COVID-19 infection, including Long COVID?
R: I noticed very early on that regardless of how mild the cases were, there were often residual issues with the person’s ability to handle and process information. The one symptom that should be tracked more than temperature is cognitive ability—confusion, disorientation, odd and unusual thoughts and behaviors. The ongoing impact of any COVID infection is a significant amount of unchecked and untracked brain damage. It’s very difficult to self-diagnose and most of our medical providers are still unaware of COVID and how it presents.
Getting infected with COVID can reduce the immune system’s ability to function. Each reinfection can reduce immune function even more, inviting opportunistic infections to eventually kill us. This is how HIV functions, but at least there is treatment for that. There’s no treatment for Long COVID and there’s even less treatment or care for those under 12 years old. The impact I see right now is immense. Children and young adults are exhibiting Alzheimer’s and dementia-like symptoms, and there are huge increases of cancer, diabetes and heart problems at the population level.
EB: What have been your experiences advocating for Long COVID patients, and what are some of your greatest concerns with the “mass disabling event” of Long COVID associated with the pandemic? What do doctors know or not know, and what do you think needs to be done to address this?
R: While documenting cases in 2020, some had symptoms that just wouldn’t resolve. A few threatened to commit suicide and were in constant and severe pain. Many of their doctors didn’t believe them. I would contact their doctors and explain what Long COVID was. I would send them studies if they requested and would tell them what labs or referrals to order for their patients.
Many doctors were receptive at first. Some would gaslight the patients, saying that they were experiencing anxiety and not their actual ongoing COVID symptoms. I made an extra effort to contact those ones because they were making the patients worse and confused. I spent hundreds of hours on social media spaces giving talks about COVID, Long COVID and what I was seeing. Other Long COVID sufferers and advocates would join.
None of this data was being collected or distributed by our DOH, regardless of how the variants mutated or the community was being impacted. Any attempts to send information up the chain of command to the top were ignored and sometimes punished.
Over time, the doctors I was working with were getting Long COVID themselves. It led to a significant reduction in care for their patients. Some would brush the issue off because they had it and they were working, which they thought meant they were fine.
Doctors need to have proper information and guidance. Without it, many people are being told COVID isn’t really a problem. They trust their doctors to know about COVID. Their doctors are unknowingly feeding them to the fire. Vaccines are only one layer of a many-layered solution, and at this point vaccines aren’t very effective at preventing infection as the virus continues to rapidly mutate and new variants continue to evolve.
In terms of public health as a whole, the CDC is looked at as the main guidance for all these institutions. They need to be putting out clear messaging about COVID being airborne, the fact that an infection commonly lasts anywhere from 14–20 days, each reinfection can reduce immune function, and COVID is a vascular disaster that can wreck any and all organs of the body. These are things that scientists have known since 2020. There is absolutely no reason Drs. Rochelle Walensky and Anthony Fauci didn’t know the correct protocols for handling this pandemic. They both have HIV backgrounds.
My greatest concern about this mass disabling event is that I live in Hawaii. Disabled people were hidden, ignored and underserved here before the pandemic. It was nearly impossible to find mental and behavioral health services and they were often insufficient at best.
When everyone keeps getting reinfected, they will not be able to function. There’s low availability for services now and it’s already getting pretty noticeable. My friends working in the hospital are reporting incredibly low staff numbers and extreme burnout. We only had nine ambulances in circulation a couple weeks ago due to callouts.
Suicides, mental hospital stays and inability to function are becoming increasingly common and we’re just getting started. Since the pandemic began, there’s been an increase in car and plane accidents, heart attacks, diabetes, cancers, previously rare disorders and sudden deaths. Currently, COVID is listed as the third leading cause for death in the US, but if data were properly collected, COVID would be number one.
I took someone to the doctor for a head wound to be stitched and the doctor didn’t even mention concussion protocol. He said strange things that hadn’t been relevant regarding COVID since 2021. He behaved odd and childlike.
This mass disabling event is largely invisible. Many cannot self-diagnose the brain damage that a significant percentage of infections cause to some degree. It changes moods, thoughts, function, and can make people confused or angry.
My biggest concern is that with mass infection and reinfection, everyone is getting their brains melted. Who will take care of anyone when no one is left healthy and functional? Who will grow our food, participate in society, or even be able to get out of bed after we’ve all had multiple infections? Who will be left?
EB: Those are critical points, and concerns that should be more widely shared. The propaganda of the corporate media and political establishment has had a real impact, and prevented masses of people from understanding the dangers of COVID-19 and Long COVID.
Changing topics somewhat, when we spoke before you said that “Lahaina is an active crime scene, just like the COVID situation here is also an active crime scene.” Can you elaborate more on this and the criminal negligence that you believe caused this catastrophic fire? What other connections do you see between this fire and the COVID-19 pandemic?
R: Just the fact that there’s such a focus from those in charge on reopening and getting back to work tells me everything I need to know. The community just experienced a life-altering trauma and instead of really taking care of them and helping them get situated and time and resources to heal, it’s full-steam ahead. Open up, get back to work, go to school. Don’t worry about how you’re going to pay that mortgage on the burn pile where you used to live.
Just like with the COVID pandemic, the Emergency Management Agency lead didn’t have experience. They didn’t sound any alarm, and clearly weren’t well versed on emergency response protocols, otherwise they would have correctly used the emergency alarm system. Instead, Herman Andaya reasoned with everyone about why he didn’t think they were necessary.
For COVID, Josh Green facilitated thousands of tourists freely and consistently infecting our community with almost no guidance other than to get vaccinated. He gaslit us for years from his whiteboard and scrubs. He got even worse after he got COVID. The brain damage is real.
Why didn’t Maui sound the emergency system that is used for emergencies including wildfires? Why didn’t HIDOH enact their public health police powers to protect the community from COVID? Why do they both consistently report false numbers? Why do they both tell the community about resources that exist, but in reality are not actually available? Why is the community being forced to bear the brunt of the outcome of both disasters alone? Why does our leadership refuse to work with the community to solve either issue?
I know how greedy and careless this government is first-hand. Especially when local people are involved. Both disasters have resulted in very high losses to our Filipino and Pasifika communities.
How are we the only state without a fire marshal? Why is there never anyone held accountable? How do all these incredibly incompetent folks keep getting replaced by more incompetence? Nepotism. It has led to incredible incompetence and I have to assume it’s why there’s no accountability or oversight anywhere or for anything.
EB: Since the beginning of the pandemic, the WSWS has advocated for the full deployment of all available public health measures to eliminate SARS-CoV-2 throughout the world. Multiple countries proved that such a Zero-COVID strategy was possible, and we now know even more about viral transmission.
We have stressed that the fundamental reason this global elimination strategy has not been implemented is due to the division of the world into rival nation-states and the refusal of the capitalist ruling elites to accept any impingement on their ability to exploit workers and generate profits. What are your thoughts on this, and do you agree that we need to fight for a global elimination strategy?
R: The SARS-CoV-2 pandemic has exposed the challenges associated with the division of the world into nation-states, each pursuing its own approach to pandemic management. It’s been an absolute disaster.
When the virus first hit and people began seeing consequences and acting accordingly, I thought we had a chance at stopping the virus. Then the countries with more behaved greedily. They hoarded and wasted resources in the face of the countries who couldn’t get access to resources from the global market.
We are all in this together and no one is getting off this rock alive. Working together is the only way to get rid of this virus and all the others that have been popping up in the past few years.
Unfortunately, such an approach seeks to prioritize the well-being of individuals and communities over economic interests as Cuba has done. They developed their own COVID-19 vaccines. They consistently have the lowest reported COVID cases and deaths globally. Often close to zero. Their vaccines work much better than ours have been.
This reflects true commitment to public health and an ability to leverage existing medical and scientific infrastructure to respond to the pandemic independently.
EB: Thank you for this invaluable interview and contribution to the Global Workers’ Inquest.
R: Thank you.
#covid 19#hawaii#long covid#covid response#covid pandemic#class war#brain damage#Rochelle Walensky#Anthony Fauci
14 notes
·
View notes
Text

antibody - amasosha omzimba
asymptomatic - ongabonisi izimpawu
contact tracing - ukulandela umkhondo wabahlangene nonegciwane
contagious - thelelanayo
coronavirus - igciwane lekhorona
Covid-19 - ikhovidi-19 or i-Covid-19
face mask - imaskhi or isamfonyo
hand sanitizer - isibulali magciwane sezandla
pandemic - ubhubhane
pneumonia - inyumoniya
symptom - uphawu
to vaccinate - goma
vaccine - umuthi wokugoma
virus - igciwane
5 notes
·
View notes
Text
How Increased Surveillance by the China Government during the Global COVID-19 Pandemic Affects Online Communities?

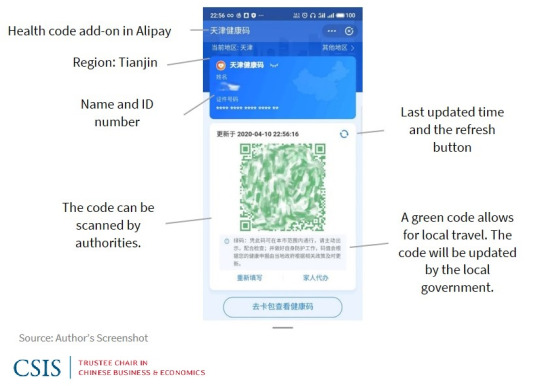
In the wake of the global COVID-19 pandemic, governments worldwide, including China, intensified surveillance measures to curb the virus's spread. In this context, China's implementation of stringent surveillance, notably through Health Code Apps, has raised profound concerns about its impact on online communities. As facial recognition and data collection become intrinsic to daily life, the potential repercussions on digital spaces and the people within them demand careful examination. This discussion delves into the multifaceted consequences of increased surveillance by the Chinese government and its tangible effects on the dynamics of online communities.

Privacy Erosion
In response to the global COVID-19 pandemic, various countries implemented measures to track and control the virus's spread, introducing tools such as contact tracing apps (Ojokoh et al., 2022), temperature checks (Qu & Lv, 2021) and travel restrictions (Burns et al., 2021). Simultaneously, In China, where stringent surveillance measures were already in place, the government leveraged technology to an even greater extent, using facial recognition and health QR codes to monitor citizens' movements. This involved the deployment of a series of applications known as "Health Code Apps," which have raised concerns about privacy erosion, particularly regarding the use of health code applications. Online communities are not immune to this erosion, as the data collected through these apps includes personal information, health status, and location details. This data is then utilized to assign one of three colours, indicating the user's health status (Ramos, 2020). However, Data is funnelled to entities like the provincial Big Data Bureau, Alibaba, and the telecommunications department, expanding the accessibility to user information, ranging from personal details to health status, location, and device specifics. This centralized model amplifies the risks of data aggregation and user re-identification, exemplified by the Beijing Health Bao system's data leak in December 2020. The incident exposed the photographs, ID numbers, and nucleic acid test information of celebrities, highlighting insufficient safeguards in place (Zhang, 2022). Online communities may find their members exposed to privacy breaches, leading to a chilling effect on open communication and expression within these digital spaces.

Potential for Abuse of Power:
The potential for the abuse of power in the context of surveillance, inadequate transparency and compliance measures is a significant concern for online communities as well. This concern is exemplified by recent events in Henan Province, where health code apps were allegedly manipulated to suppress protests related to potential losses in rural banks on the brink of collapse (Zhang, 2022). The legitimacy of these health code apps faced a setback as city officials marked over a thousand individuals as red, restricting their entry into Zhengzhou City and highlighting the vulnerability of such systems to misuse (Zhang, 2022). This incident underscores the potential for health code apps, initially designed for public health purposes, to transform into tools of surveillance, allowing government agencies to exert control under the guise of maintaining public health. The lack of stringent transparency requirements heightens the risk of these technologies being misused for purposes beyond their intended scope, which negatively impacts the freedom of expression within online communities. As governments exploit surveillance tools to monitor and influence online discussions, online communities may face challenges related to censorship and control, further emphasising the interconnected nature of surveillance concerns and their impact on digital spaces.
Technological Dependence:
Embracing extensive surveillance often involves a reliance on advanced technologies. In the case of Health Code Apps, facial recognition technology is integrated into residential area access control systems, permitting entry only to those with a green code (Ramos, 2020), which has implications for online communities. This reliance on advanced technologies may neglect more human-centric approaches to online interaction, potentially excluding or disadvantaging certain members of digital communities. As surveillance technologies become integral to online platforms, the balance between security measures and preserving the inclusivity and diversity of online communities becomes a critical consideration.
Trust Deficit:
The colour-coded system assigned by health code applications has far-reaching consequences for millions of users in their interactions within both physical and online communities. Requiring individuals to display their health codes in public transportation, shopping malls, markets, and other public places may contribute to a trust deficit between citizens and the online platforms they engage with (Jao et al., 2020). Users within online communities may question the motives behind such surveillance measures, especially if their personal information is shared without their knowledge. Rebuilding trust within online communities, once eroded by mandatory health code reliance, poses a considerable challenge, impacting the dynamics of digital social spaces.
In conclusion, the surge in surveillance by the Chinese government amid the global COVID-19 pandemic undeniably leaves a lasting imprint on online communities. The colour-coded system mandated by health code applications not only infiltrates public spaces but also infiltrates the very essence of digital interactions. This imposition triggers a tangible trust deficit within online communities as individuals question the motives behind these surveillance measures. Rebuilding trust within these virtual spaces, essential for vibrant and open communication, becomes a formidable challenge in the aftermath of mandatory health code reliance. The delicate equilibrium between bolstering security measures and safeguarding the inclusivity of online communities emerges as the linchpin for preserving the dynamic and diverse nature of these digital spaces. In essence, the impact of increased surveillance by the Chinese government is intimately intertwined with the well-being and resilience of online communities.
"Considering the implications of increased surveillance by the Chinese government during the global COVID-19 pandemic on online communities, we'd like to hear your perspective. How do you perceive the effects on privacy erosion, potential abuse of power, technological dependence, and the trust deficit within these digital spaces? Share your insights and cast your vote below."
Reference List
Burns, J., Movsisyan, A., Stratil, J. M., Biallas, R. L., Coenen, M., Emmert-Fees, K., Geffert, K., Hoffmann, S., Horstick, O., Laxy, M., Klinger, C., Kratzer, S., Litwin, T., Norris, S. L., Pfadenhauer, L. M., Von Philipsborn, P., Sell, K., Stadelmaier, J., Verboom, B., . . . Rehfuess, E. (2021). International travel-related control measures to contain the COVID-19 pandemic: a rapid review. The Cochrane Library, 2021(3). https://doi.org/10.1002/14651858.cd013717.pub2
Jao, N., Cohen, D., & Udemans, C. (2020). How China is using QR code apps to contain Covid-19. TechNode. https://technode.com/2020/02/25/how-china-is-using-qr-code-apps-to-contain-covid-19/
Ojokoh, B. A., Aribisala, B. S., Sarumi, O. A., Gabriel, A. J., Omisore, O. M., Taiwo, A. E., Igbe, T., Chukwuocha, U. M., Yusuf, T. A., Afolayan, A., Babalola, O., Adebayo, T., & Afolabi, O. (2022). Contact Tracing Strategies for COVID-19 Prevention and Containment: A scoping review. Big Data and Cognitive Computing, 6(4), 111. https://doi.org/10.3390/bdcc6040111
Qu, J., & Lv, X. (2021). The response measures to the coronavirus disease 2019 outbreak in China. Open Forum Infectious Diseases, 8(2). https://doi.org/10.1093/ofid/ofab014
Ramos, L. F. (2020). Evaluating privacy during the COVID-19 public health emergency. The ACM Digital Library, 176–179. https://doi.org/10.1145/3428502.3428526
Zhang, X. (2022). Decoding China’s COVID-19 health code apps: the legal challenges. Healthcare, 10(8), 1479. https://doi.org/10.3390/healthcare10081479
4 notes
·
View notes
Text
Summer COVID surge shows we may have to return to 2020 pandemic measures - Published Aug 29, 2024
As summer 2024 draws to a close, the U.S. finds itself once again grappling with a surge in COVID-19 infections.
This wave has taken many people by surprise, particularly as the country has largely consigned the pandemic to the past. While public life has pretty much returned to pre-pandemic norms — something almost none of us would have believed in the summer of 2020 — the virus itself has not.
Mutations of the virus continue to occur, and new variants are emerging, posing ongoing challenges to public health and safety. As we look ahead to the remainder of 2024 and into early 2025, we need to take stock of where we are, understand the factors driving this resurgence and better anticipate how the pandemic might evolve.
The recent surge in COVID-19 cases has disrupted summer travel plans, overwhelmed healthcare facilities in certain areas, and left many Americans dealing with the familiar symptoms of fever, cough and fatigue. The summer months, typically associated with lower respiratory virus activity, have instead seen a significant uptick in COVID-19 infections. Several factors contribute to this unexpected surge.
One factor is the high transmissibility of newer variants. The virus has continued to mutate, with certain variants displaying enhanced ability to spread, even among populations with high vaccination rates. While vaccines remain effective at preventing severe disease and death, breakthrough infections are becoming more common, especially as immunity from earlier vaccinations wanes.
Second, the widespread relaxation of public health measures has created an environment conducive to transmission. Mask mandates, social distancing guidelines and restrictions on large gatherings have all but disappeared. This return to normalcy, while massively psychologically and economically beneficial, has provided the virus with ample opportunities to spread.
Finally, the pervasive sense of pandemic fatigue has led to a serious decline in vigilance. Many people, weary of the pandemic’s disruptions to their lives, have become markedly less cautious. This complacency, coupled with the underestimation of the virus’s ability to adapt, has allowed COVID-19 to regain a foothold.
The federal government’s response to the latest surge has been tepid at best. After years of intense focus on COVID-19, there is a palpable desire in Washington to move on. This has resulted in a fragmented approach, with responsibility for managing the current wave largely devolving to state and local governments. While some have reinstated certain precautions, others have continued with business as usual, leading to inconsistent messaging and outcomes.
Moreover, the federal government’s decision to end the public health emergency earlier this year has had unintended consequences. The end of the emergency declaration led to a reduction in federal funding for testing, contact tracing, and vaccination efforts, just as these tools are once again needed. The lack of a coordinated national strategy has hampered efforts to control the surge and has left healthcare providers scrambling to manage increased caseloads with fewer resources.
Looking ahead, the trajectory of the pandemic remains uncertain, but there are several key trends and scenarios to consider.
The virus is likely to continue mutating, with new variants emerging that could potentially evade immunity from previous infections or vaccinations. This means that COVID-19 will remain a moving target, requiring ongoing surveillance and adaptation of public health strategies. The development of updated vaccines and treatments will be critical in staying ahead of the virus, but the speed at which these can be rolled out will determine their effectiveness.
We can and should also expect periodic surges in COVID-19 cases, particularly in the fall and winter months, when respiratory viruses typically thrive. These surges may not reach the levels seen during the height of the pandemic, but they could still cause significant disruption, particularly in areas with low vaccination rates or limited healthcare capacity. Localized outbreaks, driven by specific variants or super-spreader events, will likely become regular features of the landscape.
The healthcare system, already strained from years of dealing with the pandemic, is also going to face additional pressure if the current surge continues into the fall and winter. Hospitals and clinics will need to balance the demands of COVID-19 patients with the resumption of regular medical care that had been postponed during the pandemic’s earlier phases. This balancing act could lead to increased wait times, resource shortages and burnout among healthcare workers.
And we can’t underestimate how public fatigue with COVID-19 precautions will grow, making it more difficult to reimpose restrictions or encourage preventive behaviors. This resistance could be particularly strong in regions that have experienced relatively low case numbers or where political leaders have downplayed the severity of the virus. Overcoming this fatigue will require clear and consistent communication from public health officials, as well as community-level engagement to reinforce the importance of ongoing vigilance.
We are also making a big mistake if we ignore the economic and social implications of continued COVID-19. The virus’s persistence may lead to renewed disruptions in the travel industry, supply chains and workforce participation. Along with this, the psychological toll of a prolonged pandemic, with the associated uncertainty and anxiety, could have lasting effects on mental health and societal cohesion. Policymakers will need to address these challenges proactively, with a focus on resilience and support for affected populations.
So where do we realistically go from here, given that it is clear that COVD-19 is far from over? While much progress has been made in terms of vaccination and treatment, the current surge is a stark reminder that complacency is not an option. The road ahead will require a renewed commitment to public health, both from government leaders and from individuals.
We all need to prepare for not only the possibility of continued disruptions but for another new normal that might be a little closer to 2020 than how we’ve recently been living. That means preparing for future waves and the long-term implications of a world in which COVID-19 remains a persistent, if manageable, threat.
Aron Solomon is the chief strategy officer for Amplify. He has taught entrepreneurship at McGill University and the University of Pennsylvania.
#covid#mask up#covid 19#pandemic#wear a mask#coronavirus#sars cov 2#public health#still coviding#wear a respirator
40 notes
·
View notes
Text
Written By Zowe Smith
The Last American Vagabond
Mar 15, 2025
By Zowe Smith | My Life In The Thrill Kill Medical Cult Substack | Telegram
Part 1 of “Medical Surveillance” revealed how contact tracing evolved into databases called real-time AI ecosystems. The data stored in these ecosystems ranges from medical records to genomic sequences that were largely collected using Covid-19 PCR tests. Health privacy laws were revised to enable an alarming amount of data sharing with public and private intelligence agencies for military operations. Using the Covid-19 scamdemic as a front, the military worked with so-called health authorities to weaponize Covid-19 statistics to target non-compliant or undesirable groups with mRNA vaccines, ventilators, and Remdesivir. In other words, it was a military operation that utilized covertly collected private medical and genetic data to deploy bioweapons. Targets were acquired using AI generated predictive behavior models provided by government intelligence agencies like Palantir. If that sounds disturbing to you, keep reading because that was just a warm-up.
The DELAYED REACTION THAT ENABLED THE ILLUSION OF THE PANDEMIC OF THE UNVACCINATED
As contact tracing phased into the background and the genome-collection method known as PCR testing was normalized, one more important piece of data needed to be collected: vaccination status.
The mockingbird media foreshadowed that vaccination status must be made public information because during a public health emergency everyone has a right to know their risk. Soon everyone would need to have a Covid-19 shot to travel, work, go to school, and participate in society. All this would inevitably lead to a vaccine passport. Yet there was no official way to track who was vaccinated in the healthcare industry.
2 notes
·
View notes