#Atrial Septic Defect
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In Q3 of 2020, 31% of US users access the Tumblr app daily.
Text
Atrial Septic Defect
A birth defect that causes a hole in the wall between the hearts upper chambers (atria).
0 notes
Audio
Listen/purchase: SPLIT WITH PHLEGMSEPSIA by ATRIAL SEPTIC DEFECT
0 notes
Text


Joe, Jessica's husband, decided to share what hapend to baby Noble's health... The fight is not over yet... but there are some good news here too...
#Repost @jarielwright
• • • • • •
I haven’t said anything on here about Noble and what he’s been fighting...so I thought I’d share. About 1 month after he was born we found out he had ventricular and atrial septic defects. 3 holes in his heart- 1 very large, 1 medium and 1 small. This was really tough to hear. The first week or 2 of January was Jessie or I staying awake all night holding him to keep him comfortable and relaxed to help regulate his breathing and heart rate. VSDs and ASDs allow too much over oxygenated blood into his lungs and the heart works overtime to try to get it out. Noble began taking 3 liquid meds that addressed the symptoms of rapid heart beat and very fast breathing so his body could try to heal itself. Various heart echos (ultrasounds) Jan-April showed no progress. Noble was down to 5 percentile. He wouldn’t eat much and he wasn’t really gaining weight. It was insanely nerve wracking. We had a 3-4 month gap between heart echos and during this time he slowly started gaining weight. But Doc said it was still about a 25% chance that his holes would close up without open heart surgery. We just had a checkup and heart echo on Tuesday and basically went in with the expectation to talk about the surgery, heal time and all that...well, turns out lil Noble man has just 1 hole left, the large one, and even it has tissue built up around it showing signs that within possibly a year, he could close up. The medium and small holes have sealed up. Noble is about 40 percentile now (in weight). Jesus still works miracles guys...And even when you doubt, He still pulls thru.
7 notes
·
View notes
Text
Juniper Publishers- Open Access Journal of Case Studies
The Warburg Effect - An Onco-hematologic Emergency?
Authored by Poggi Guido
Abstract
Warburg effect is a rare and potentially life-threatening metabolic complication occurring in oncologic patients. The Authors report the case of a 79-year-old man affected by diffuse large B-cell lymphoma presenting with severe lactic acidosis and hypoglycaemia both of which were refractory to conventional management and they critically review the available literature.
Keywords:Warburg effect; Lactic acidosis; Hypoglycaemia; Hematologic malignancies; Cancer cells; Chronic hepatitis C; Nephrology; Bladder tumour
Introduction
The combination of lactatemia and severe untreatable hypoglycaemia is a rare metabolic complication of hematologic malignancies. It occurs more frequently in patients affected by lymphoma, and it is generally associated with an ominous prognosis. It is secondary to an avid consumption of glucose by the cancer cells that even under aerobic conditions switch their glucose metabolism from the oxidative pathway to the glycolytic pathway, leading to increased lactate production. This metabolic shift is known as the “Warburg effect”. Here we will discuss a patient with diffuse large B-cell lymphoma (DLBCL), who presented with hypoglycaemia and lactic acidosis, and we will review similar cases from the relevant literature, which we believe warrant the consideration of the Warburg effect as an onco-hematological emergency.
Case Description
A 79-year-old man was referred to our ward for evaluation of massive hepatomegaly discovered two weeks earlier, when he presented to the emergency department complaining of weight loss, nausea, vomiting and abdominal discomfort. In the emergency department, he was diagnosed with an acute renal injury of prerenal origin, presumptive subacute cholangitis and chronic hepatitis C. He was transferred for evaluation in the nephrology department and received treatment with fluid replacement, resulting in partial improvement of renal function. He was subsequently discharged and referred to us to complete the diagnostic workup. At the time of admission, his therapeutic regimen included edoxaban and flecainide, as well as amlodipine and losartan for arterial hypertension. His medical history was notable for tuberculous spondylodiscitis at age 20, and a cholecystectomy at age 46. In 2017, two years before he was referred to us, he was diagnosed with transitional cell bladder carcinoma that did not infiltrate the muscular layer and was treated with transurethral resection of a bladder tumour (TURBT) followed by intravesical chemotherapy. He was also diagnosed with atrial fibrillation and treated with direct-acting oral anticoagulants (DOAC), and in 2018 he required electric cardioversion. Familial history was notable for the untimely death of his mother at age 35 for a hepatic tumour, and the death of his brother at the age of 66, for multiple myeloma.
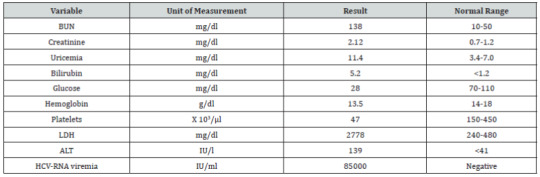
Upon arriving at our ward, the patient was alert and presenting no noticeable neurological alterations. He appeared unfit, complained of profound fatigue, anorexia and abdominal discomfort. He reported to have lost approximately 10kg in the previous two months and denied any episodes of fever or drenching sweats. His temperature was 36.8 °C, the heart rate was 98 beats per minute, the respiration rate was 18 breaths per minute, and the oxygen saturation was at 97% while breathing ambient air. Physical examination revealed massive hepatomegaly, extending on the lower margin to 2cm below the transverse umbilical line, and concomitant splenomegaly with a palpable lower pole 4cm below the costal arch. The ultrasound confirmed massive hepatosplenomegaly; however, the hepatic parenchyma revealed no nodules, but only a focal solitary hypoechoic area of non-nodular appearance. A contrast-enhanced total body CT scan was performed and confirmed the ultrasound findings with liver and splenic homogeneous enlargement and further revealed the involvement of multiple retroperitoneal lymphnodes not found at the US scan. A complete blood count, including a metabolic panel and arterial blood gas analysis, was performed (Table 1-2), revealing significant hypoglycaemia and metabolic acidosis with a high anion gap, consistent with lactic acidosis.
Despite the severe hypoglycaemia, the patient was not complaining of neuroglycopenic symptoms. Endocrinological investigation showed that the adrenal and thyroid functions were normal. Other markers, including insulin, pro-insulin and C-peptide, were all reduced, excluding both endogenous insulin production and exogenous administration as a cause for hypoglycaemia. Biopsies of the bone marrow and liver revealed a massive infiltration of diffuse large B-cell lymphoma (DLBCL), expressing CD 20+, CD 30+ and EBV+ with high proliferative activity (Ki-67 = 90%). Correction of the hypoglycaemia with a continuous IV infusion of a 10% glucose solution and thiamine failed and exacerbated the lactatemia. Therefore, since the patient did not present hypoglycaemic symptoms, the attempt to correct the hypoglycaemia was discontinued. Unfortunately, the rapid progression of thrombocytopenia and the progressive increase in creatinine levels excluded chemotherapy as a therapeutic option. The patient, therefore, received treatment with prednisone (60mg/day) and a weekly regimen of rituximab, which led to a gradual improvement of both the clinical presentation and the blood parameters over the first three administrations of rituximab. However, shortly after that, the clinical picture rapidly worsened, and the patient died.
Discussion
The clinical presentation of Non-Hodgkin’s Lymphoma (NHL) varies depending on the subtype and the involved sites, with symptoms including enlarged palpable lymphadenopathy, B-symptoms (fever, weight loss, night sweats), and symptoms secondary to compression of adjacent structures. In rare cases, the clinical presentation may include metabolic complications [1-3] such as lactic acidosis and hypoglycemia. Lactate is a by-product of glucose metabolism, under anaerobic conditions, when pyruvate is reduced to lactate by lactate dehydrogenase (LDH). In normal conditions, most of the lactic acid is cleared by the liver (80– 90%) and converted to glucose through gluconeogenesis (Cori’s cycle), while the remainder is secreted by the kidneys [4]. Lactate accumulation leads to lactic acidosis when the concentration of lactate in whole blood exceeds 5mmol/L with a pH below 7.35 [3]. Lactic acidosis can result either from hypoperfusion (type A) or from overproduction or decreased clearance of lactate (type B). Type A lactic acidosis can result from clinical settings of hypoxia and inadequate tissue perfusion due to septic or hypovolemic shock. Type B, however, occurs in normal perfusion states and is associated with malignancies, underlying liver or kidney failure, diabetes mellitus, thiamine deficiency, drugs and toxins (e.g., alcohols, metformin, salicylates, reverse transcriptase inhibitors, cyanides) and hereditary enzymatic defects [5,6]. In the case of malignancies, as observed by Otto Warburg many years ago, cancer cells consume glucose and excrete lactate at a significantly higher rate compared to healthy cells, even in normoxic conditions [7]. The increased rate of glycolysis is due to the aberrant expression or over-expression of glycolytic enzymes, as part of the malignant process. One such example is hexokinase II, a rate-limiting enzyme involved in glycolysis, whose activity is regulated by the IGF signalling pathway, which is often defective in malignancies [8,9]. However, even though cancer cells produce increased amounts of lactate, lactic acidosis does not develop until the measure of lactate exceeds the limit of hepatic clearance and overwhelms the renal clearance, which could happen when the underlying disease has developed multiple metastases or diffused infiltration of the liver [10], as it is in the majority of reported cases of leukaemia and lymphoma and in the case we report here.
A literary review of 53 relevant clinical cases published between the years 1985-2019, focused on cases of haematological malignancies associated with lactic acidosis, has shown that as a consequence of the increased glucose consumption by the tumour, 29 (54.7%) of these patients were in a state of persistent hypoglycaemia and in 17 cases (32.1%) there was no report of neurologic deficiencies. This peculiarity is due to an ability of the brain to employ lactate as a primary source of energy, providing the brain with a protective mechanism from systemic hypoglycaemia. However, the mechanism by which this phenomenon occurs remains undetermined [11-13]. Among the 53 reviewed cases, 26 cases reported liver involvement in the development of the pathology, out of which 69.2% of the cases resulted in fatalities. It is relevant to note that the other 30.8% of cases (with reported favourable outcomes) have all engaged in a protocol of chemotherapy. The unusual clinical presentation that we are reporting, characterised by severe, untreatable hypoglycaemia, lactic acidosis, and liver involvement, was only described in 11 malignancy cases, all are cases of lymphoma, and predicts a very poor prognosis (Table 3).
Presumably, the poor prognoses are due to the aggressive nature of the disease, the fact that these cases are often diagnosed at a rather late stage in the disease progression, and indeed, any part of the clinical presentation may be justifiably suspected as a more prevalent condition. However, it is precisely because of the rarity and peculiarity of this clinical presentation that we believe the consideration and exclusion of a potential hematological emergency should be prioritised in the clinical approach. The Warburg effect, stemming from the alteration of cancer metabolism, seem to be manipulable using dichloroacetate (DCA), which is not yet indicated for the treatment of cancer but is used to treat lactic acidosis and diabetes. Despite the lack of official indication for DCA in this setting, there is an accumulating body of evidence to support its efficacy. DCA is thought to mitigate the Warburg effect by inhibiting pyruvate dehydrogenase kinase, leading to the activation of pyruvate dehydrogenase, and by that process DCA is able to stimulate cellular respiration through oxidative phosphorylation, rather than strict glycolysis, offsetting the relative metabolic advantages that neoplastic tissues hold over their surrounding healthy tissue. Moreover, due to the activation of mitochondrial respiration, DCA can limit the amount of lactate produced by the tumour, changing its chemical environment and inhibiting its cellular proliferation, as well as restoring a degree of apoptotic function through the increase in cytochrome c [52].
However, although DCA represents a promising prospect, it is important to note that the encouragement of mitochondrial activity could have deleterious consequences for the nervous system, as these tissues rely primarily on glycolysis and may lack the cellular functions to sustain the increase in free radicals. Nevertheless, in the context of Warburgism, where the severe systemic hypoglycaemia does not result in neuroglycopenic symptoms, it seems reasonable to hypothesise that the cells of the nervous system have already gone through the necessary remodeling to endure this metabolic shift. However, we are currently unaware of such research.
To know more about Juniper Publishers please click on: https://juniperpublishers.com/manuscript-guidelines.php
For more articles in Open Access Journal of Case Studies please click on: https://juniperpublishers.com/jojcs/index.php
#juniper publishers journals#JuniperPublishers#Cardio-Thoracic Surgery#Hospice and Palliative Medicine#General Surgery Genetics#Dermatology
0 notes
Text
The Doctor Who Thwarted the Charge of the General Medical Council – Part 1
By SAURABH JHA
After Dr. Hadiza Bawa-Garba was convicted for manslaughter for delayed diagnosis of fatal sepsis in Jack Adcock, a six-year-old boy who presented to Leicester Royal Infirmary with diarrhea and vomiting, she was referred to the Medical Practitioners Tribunal (MPT). The General Medical Council (GMC) is the professional regulatory body for physicians. But the MPT determines whether a physician is fit to practice. Though the tribunal is nested within the GMC and therefore within an earshot of its opinions, it is a decision-making body which is theoretically independent of the GMC.
The tribunal met in 2017, 6 years after Jack’s death, to decide whether Dr. Bawa-Garba, after the manslaughter conviction, should be allowed to practice medicine again, whether she should be suspended for a year, or her name be permanently erased (“struck off”) from the medical register. The GMC wanted Dr. Bawa-Garba to be struck off from the medical register because they felt that her care of Jack fell so short of the expected standard, that her return to practice would not only endanger patients but undermine public confidence in the medical profession. The GMC expected the MPT to agree with its uncompromising stance, and the MPT might well have, and probably would have, but for the efforts of Dr. Jonathan Cusack, a consultant neonatologist at Leicester Royal Infirmary (LRI), and a former supervisor and mentor of Dr. Bawa-Garba’s.
Cusack is unassuming even by British standards. You will not find him on social media or taking selfies. A soft-spoken northerner with a steely nerve and an uncompromising deference to facts, Cusack is both old-school and new-school. He has that unassailable integrity which is immeasurable but instantly recognizable. But he’s also savvy – and understands the British medical, regulatory and legal systems inside out. If Dr. Bawa-Garba’s license is reinstated, Cusack’s role would be akin to that of the code breakers in the Second World War. Dr. Bawa-Garba trusts him implicitly. Her legal team can’t function without him.
Cusack was loyally involved in both the rehabilitation of Dr. Bawa-Garba’s clinical confidence after Jack’s death, and her trial. I met him after the first day’s appeal hearing in the pub opposite the Courts of Justice. Originally hesitant to speak to me, being the ostentatious expat Brit that I am, he agreed to an interview on the condition that I not make too much of a song and dance about his contribution. I promised that I wouldn’t. I lied.
Here’s an excerpt of our conversation about the intricacies of the case.
Dr. Jonathan Cusack, a consultant neonatologist at Leicester Royal Infirmary (LRI), and a former supervisor and mentor of Dr. Bawa-Garba’s.
Saurabh Jha (SJ) – Many say you’re the reason the tribunal did not strike Dr. Bawa-Garba off the medical register, and only suspended her for a year.
Jonathan Cusack (JC) – I’m not sure I deserve to be singled out. The facts, by facts I mean Hadiza’s competence as a clinical pediatrician, were irrefutable. I will say that I collected the evidence verifying her clinical competence.
SJ – I can tell by your accent that you were raised in the north. Mind you, I think anything north of Milton Keynes is north.
JC – I’m from the Birmingham, not the North! I went to medical school in Leicester. I did my pediatric training in the Leicester Deanery. I also worked in Australia, in the Northern Territory – Darwin and Alice Springs.
SJ- Can we recap the events of the fateful Friday – February 18th, 2011.
JC – The events have been recorded and dissected but it’s worth recapping. At 10:30 am Jack Adcock, a 6-year-old boy with Down’s, was referred to LRI emergency department with a 12-hour history of diarrhea and vomiting by his GP. He was..
SJ – Sorry to interrupt. What do you mean by “referred to ED by GP”? And what was the GP’s presumptive diagnosis?
JC – As you know from your days in the NHS, a patient can come to the ED on their own or be referred by their GP. The Adcocks took Jack to his GP who instantly recognized that he was ill and referred him to the Children’s Assessment Unit (CAU).
SJ – What was his diagnosis? Did the GP suspect sepsis?
JC – He recognized that Jack was ill. The GP managed Jack well, in so far as he instructed his parents to bring him to the CAU, instantly – which they did. In the CAU he was assessed by an experienced nurse who, instantly realizing he was ill, called Hadiza immediately. Hadiza came over urgently and assessed Jack.
SJ – So the first hour of Jack’s care was exemplary.
JC – There’s not much more Hadiza could have done in her initial assessment. Even the prosecution did not fault her immediate management of Jack. Hadiza did blood gases, basic blood tests, and ordered a chest x-ray for Jack. She prescribed both a fluid bolus and maintenance fluids.
SJ – What was her presumptive diagnosis?
JC – Her diagnosis was shock. Shock can be hypovolemic, cardiogenic or septic. Given Jack’s presentation of diarrhea and vomiting, she believed it was hypovolemic. Given his history of repaired atrial septal defect, cardiogenic shock was also in her differential, and influenced the rate the fluids were administered.
SJ – Did she suspect sepsis?
JC – It wasn’t as high as hypovolemic shock in her differential. I recall you wrote in your piece that the fact she got a chest-ray meant that infection was also in her differential. I agree with that assessment. Also, she obtained a CRP, which was a foresight that she may need to distinguish between bacterial and viral infections. CRP is not a part of the routine blood panel – you have to request it separately.
SJ – What did the first set of blood gases show?
JC –The pH was 7. The lactate was elevated.
SJ – The lactate was 11. Should these numbers have been a clincher for sepsis?
JC – You mean septic shock. I think they should certainly have raised the index of suspicion. But they are not pathognomonic for septic shock. I’ve seen kids with hypovolemic shock with ph’s of 6.9.
SJ – There seems to be a general meme in the public space that Jack’s blood was “full of acid” and that somehow indicated septicemia.
JC – The ph in and of itself isn’t specific for septic shock but is indicative of shock in general. A case can be made that an elevated lactate is suggestive of sepsis, but lactate can be elevated in conditions other than sepsis. Also, 2011 was before we knew a whole lot about sepsis and lactates. It was before mass awareness of sepsis. Lactate wasn’t routinely obtained in ill patients, then. In any case, after the fluid bolus, Hadiza reassessed Jack. He had perked up, was playful, and far more resistant when Hadiza repeated blood gases.
SJ – What did the second set of blood gases show?
JC – There was a problem with the machine. It was unable to record the lactate, but it recorded the ph which was 7.24.
SJ – Normal ph is 7.4, so it was moving in the right direction after the fluid bolus. But we don’t know what the repeat lactate was.
JC – No, we don’t know the lactate – which’ll always be an unknown counterfactual. But the normalizing ph confirmed for Hadiza, as it’d have confirmed for any pediatrician, that the working diagnosis of hypovolemic shock from viral gastroenteritis wasn’t unreasonable.
SJ – And depending on the outcome, that is in hindsight, this is either confirmation or confirmation bias – a mark of clinical acumen or a flaw of judgment. Regardless, it’s fair to say that a doctor who is cautious about fluid administration because of patient’s heart disease, rechecks a patient’s status within an hour, gets specialized blood tests such as CRP, isn’t an indifferent doctor, isn’t a slacker, but a highly thoughtful doctor.
JC – Yes, and that’s what makes this case even more painful. Hadiza is diligent and thoughtful. Despite the fact that she did not immediately diagnose sepsis, her management of Jack was thoughtful.
SJ – Many can’t fathom that a doctor can be thoughtful but still be wrong. One criticism was that the chest x-ray, though performed at 12:30 pm, wasn’t reviewed by Dr. Bawa-Garba until 3 pm.
JC – By the time the chest x-ray was done, and it was done after the second set of blood gases were analyzed, she was, understandably, more certain about her diagnosis of hypovolemic shock because the ph had improved and Jack was perking up. But also bear in mind she was being beeped incessantly, as she was covering more than just the CAU, more than what is safe for a single registrar to cover. She was running around the hospital.
SJ – I can actually picture that. Running up and down flights of stairs to various wards in various parts of the hospital, dashing to the nearest phone to answer her beep, accumulating scraps of paper. It’s easy to forget that chest x-ray that you ordered but you don’t know when it was done, because you’re not told that it was done, let alone that it had an abnormality. For contrast – at my institution, when pneumonia is suspected by the emergency department, a radiologist is supposed to report the chest radiograph in 30 minutes, and call the physician if there is pneumonia.
JC – It was a busy day. Her juniors were new to pediatrics. In the meantime, she had to perform a lumbar puncture (LP) on a patient with suspected meningitis because no one in her team knew how to. You don’t want to be distracted whilst performing an LP in a child.
SJ – And you can imagine that there’s a parallel universe where she spent the entire time in the CAU with Jack, and the kid with suspected meningitis died from meningitis because no one could perform an LP. What of the IT systems being down? What effect did that have?
JC – A lot. One of the juniors on her team spent most of the time calling pathology for results for their patients. Jack wasn’t the only patient she was looking after.
SJ – That’s quite an opportunity cost. So, instead of seeing patients and doing a H&P, the junior doctor was phoning the labs – what a waste. This, of course, meant that Dr. Bawa-Garba had to pick up the slack, and do the work of her juniors.
JC – There was another consequence. When Hadiza phoned pathology for Jack’s results, a frustrated individual, frustrated at being phoned for results all day, recited all of Jack’s results, including creatinine. Normally, what happens is that the results populate in the patient’s records and the abnormal results are highlighted. Jack’s creatinine was mildly elevated. She was told the creatinine, non-judgmentally – i.e. she was not told that it was elevated. When you’re reliant on a system which flags abnormal results it’s easy to miss a mild abnormality when it’s not flagged.
SJ – She returns to Jack at 3 pm. This is her third assessment of Jack, within 5 hours, so she clearly had not forgotten about Jack. Now she looks at the chest x-ray. Did that show barn door pneumonia?
JC – Like a lobar consolidation? No, the abnormalities were subtler, fluffier, and obscured the right heart border. You could make the case that they represented either viral bronchiolitis or bacterial pneumonia.
SJ – Another layer of subtlety added to the complexity of this case. So now she prescribes antibiotics, which were administered an hour later. What was Jack like then?
JC – He had perked up substantially. He was laughing and being playful. Whatever was going on inside his circulation unbeknownst to everyone, externally he no longer appeared ill. Here’s an indication that everyone believed that Jack was on the mend – Jack’s father returned home in the evening. He wouldn’t have done that if Jack hadn’t perked up.
SJ – It’s around 4 pm that she meets Dr. O’Riordan, her consultant, during handover. She tells him about Jack and shows him the blood gases. Neither did she ask O’Riordan to assess Jack nor did O’Riordan offer to assess Jack after seeing his original biochemical profile. It’s fair to say that O’Riordan agreed with her management.
JC – I’ll expand on O’Riordan’s role a bit later because his role in this case is significant. It’s important, also, to understand what was happening on the nursing side. The pediatric nurses are excellent at LRI. As happens far too often in the NHS, acute services are often short of nursing staff. Jack was being looked after by an agency nurse – who wasn’t a pediatric nurse.
SJ – So, some of Jack’s care fell short, as a result.
JC – Some crucial elements of his care fell short. His vital signs weren’t being recorded with the diligence they deserved. There was no record of his fluid input-output. For example, his nappies had not been weighed. The weight of nappies is an indicator of fluid loss.
SJ – This seems like a systems issue rather than Dr. Bawa-Garba’s responsibility. A pediatric registrar can’t possibly be expected to watch over every single element of care of every single patient – this is humanly impossible and inhumane to demand. The system works when every member of the team does what they’re supposed to be doing – i.e. does their job.
JC – Unfortunately, Hadiza was blamed for not spotting the failings of the nursing staff. She reassessed Jack, at 6 pm. She did not look at his observation chart – perhaps because she felt she did not need to. Jack was playful, like a 6 year old should be, and seemed to be heading in the right direction. She didn’t feel the need for consultant review because Jack seemed to be getting better.
SJ – By 6 pm – i.e. 8 hours in the hospital, what was going on inside Jack’s circulation, hemodynamically speaking?
JC – We know from the autopsy that Jack died from Steptococcus A septicemia. We don’t know his vital signs around 7 pm, or his ph. But, that he was mentally alert and playful, meant that his circulatory system may have been in compensation mode, meaning that his homeostatic mechanisms – the ones which constrict the arteries and maintain the blood pressure, may have been in overdrive mode, and may have been at the end of their tethers, and may have only just been successfully maintaining his blood pressure.
SJ – Jack, internally, was waging a war against Streptococcus. Then there was a decisive turning point.
JC – Yes, then what happened was that Jack was transferred to the ward. After the transfer he received his maintenance dose of enalapril. An hour later he went into cardiac arrest. The cause of Jack’s death was Group A Streptococcus. However, many doctors are concerned that what delivered Jack the fatal blow was the enalapril. To recap, enalapril is an angiotensin converting enzyme inhibitor. It dilates the arteries. It undid the compensatory overdrive of Jack’s circulatory system, the overdrive which was so important in maintaining his blood pressure.
SJ – Who administered the enalapril?
JC – This is complicated. Hadiza stopped the enalapril. She deliberately did not prescribe it on the drug chart. LRI has a policy that family members can give maintenance drugs to patients without them being written on the drug chart. Hadiza was not aware of this policy. Jack’s mother asked the nurse to give the enalapril. The nurse asked one of the junior doctors, who said it was fine for Jack’s mother to give the enalapril.
SJ – Was it Dr. Bawa-Garba who approved the enalapril?
JC – It was not clear who it was – it was one of the junior doctors – not Hadiza. He later said he couldn’t remember whether he said it was okay, or not, for Jack’s mother to give the enalapril.
SJ – Do you believe him?
JC – Well, it’s certainly plausible. Doctors give a lot of verbal orders – they can’t possibly remember each and every one of them.
SJ – But it wasn’t the fault of Jack’s mother.
JC – Only a mean-spirited person will blame Jack’s mother for giving Jack the enalapril. It wasn’t her fault. She did what she thought was the right thing to do, and checked that this was OK with healthcare staff.
SJ – And it wasn’t Dr. Bawa-Garba’s fault either.
JC – No. It’s unfair to expect her to anticipate every contingency. She was new to the CAU – she was unaware of its policies. How could she have known that she should tell Jack’s mother not to administer enalapril when the usual practice in hospitals is for drugs to be administered by nurses not parents?
SJ – So, it was the fault of neither Dr. Bawa-Garba nor Jack’s mother, nor the house officer who, allegedly, sanctioned the administration of enalapril. Whose fault was it then? It must have been someone’s fault.
JC – The system. No individual owns the blame here.
SJ – Dr. Bawa-Garba called of the cardiac arrest, briefly, mistaking Jack for another patient. This didn’t look good on her during her trial. Was this because she was fatigued?
JC – Hadiza had been on her feet for thirteen hours by the time Jack went into cardiac arrest. Anyone would have been tired at that point. But the issue wasn’t just tiredness. Earlier in the day a pediatric oncologist told her over the phone that a child with brain tumor was “not for resuscitation.” The child was going to be moved to a palliative care facility. Hadiza scribbled the ward and bed the child was in, and committed that information to memory.
SJ – But that still does not explain why she mixed up Jack with that child.
JC – Wait, I haven’t finished. The child with the incurable brain tumor was sent to a palliative care facility – i.e. was discharged from hospital. Hadiza was not told about his discharge. She still believed the child was in the hospital. Jack was sent to his bed – i.e. same ward, same bed, as the child who was not for resuscitation.
SJ – There’s a cruel irony here – despite Dr. Bawa-Garba being at her wits end, she still had the wherewithal to recall the child who was not for resuscitation. She got his location magnificently right, but was still terribly wrong.
And what an incredible bad luck for everyone involved. What an unfortunate storm of events for Jack and Dr. Bawa-Garba. Even the best sailors can’t stop a boat from capsizing in the severest of storms. To blame the sailor and ignore the storm is no justice.
JC – I agree. Hadiza did not kill Jack. He was killed by Group A Streptococcus. An overstrained system failed to save him from a very dangerous organism.
About the Author:
Saurabh Jha is a radiologist and contributing editor to THCB. He was once a junior doctor in the NHS. He can be reached on Twitter @RogueRad
The Doctor Who Thwarted the Charge of the General Medical Council – Part 1 published first on https://wittooth.tumblr.com/
0 notes
Text
[Bandcamp] ATRIAL SEPTIC DEFECT - SPLIT WITH PHLEGMSEPSIA https://t.co/t7vnYbF3zM http://pic.twitter.com/KBPBQuauoR
— #death metal in BC (@dmtag_bot) April 10, 2017
0 notes
Text
[Goregrind|Bandcamp] ATRIAL SEPTIC DEFECT - SPLIT WITH PHLEGMSEPSIA https://t.co/OimIq0Uh1K http://pic.twitter.com/75vZ3sda5q
— Grindcore Music (@grindcore_bot) April 9, 2017
0 notes
Video
youtube
0 notes
Text
The Doctor Who Thwarted the Charge of the General Medical Council – Part 1
By SAURABH JHA
After Dr. Hadiza Bawa-Garba was convicted for manslaughter for delayed diagnosis of fatal sepsis in Jack Adcock, a six-year-old boy who presented to Leicester Royal Infirmary with diarrhea and vomiting, she was referred to the Medical Practitioners Tribunal (MPT). The General Medical Council (GMC) is the professional regulatory body for physicians. But the MPT determines whether a physician is fit to practice. Though the tribunal is nested within the GMC and therefore within an earshot of its opinions, it is a decision-making body which is theoretically independent of the GMC.
The tribunal met in 2017, 6 years after Jack’s death, to decide whether Dr. Bawa-Garba, after the manslaughter conviction, should be allowed to practice medicine again, whether she should be suspended for a year, or her name be permanently erased (“struck off”) from the medical register. The GMC wanted Dr. Bawa-Garba to be struck off from the medical register because they felt that her care of Jack fell so short of the expected standard, that her return to practice would not only endanger patients but undermine public confidence in the medical profession. The GMC expected the MPT to agree with its uncompromising stance, and the MPT might well have, and probably would have, but for the efforts of Dr. Jonathan Cusack, a consultant neonatologist at Leicester Royal Infirmary (LRI), and a former supervisor and mentor of Dr. Bawa-Garba’s.
Cusack is unassuming even by British standards. You will not find him on social media or taking selfies. A soft-spoken northerner with a steely nerve and an uncompromising deference to facts, Cusack is both old-school and new-school. He has that unassailable integrity which is immeasurable but instantly recognizable. But he’s also savvy – and understands the British medical, regulatory and legal systems inside out. If Dr. Bawa-Garba’s license is reinstated, Cusack’s role would be akin to that of the code breakers in the Second World War. Dr. Bawa-Garba trusts him implicitly. Her legal team can’t function without him.
Cusack was loyally involved in both the rehabilitation of Dr. Bawa-Garba’s clinical confidence after Jack’s death, and her trial. I met him after the first day’s appeal hearing in the pub opposite the Courts of Justice. Originally hesitant to speak to me, being the ostentatious expat Brit that I am, he agreed to an interview on the condition that I not make too much of a song and dance about his contribution. I promised that I wouldn’t. I lied.
Here’s an excerpt of our conversation about the intricacies of the case.
Dr. Jonathan Cusack, a consultant neonatologist at Leicester Royal Infirmary (LRI), and a former supervisor and mentor of Dr. Bawa-Garba’s.
Saurabh Jha (SJ) – Many say you’re the reason the tribunal did not strike Dr. Bawa-Garba off the medical register, and only suspended her for a year.
Jonathan Cusack (JC) – I’m not sure I deserve to be singled out. The facts, by facts I mean Hadiza’s competence as a clinical pediatrician, were irrefutable. I will say that I collected the evidence verifying her clinical competence.
SJ – I can tell by your accent that you were raised in the north. Mind you, I think anything north of Milton Keynes is north.
JC – I’m from the Birmingham, not the North! I went to medical school in Leicester. I did my pediatric training in the Leicester Deanery. I also worked in Australia, in the Northern Territory – Darwin and Alice Springs.
SJ- Can we recap the events of the fateful Friday – February 18th, 2011.
JC – The events have been recorded and dissected but it’s worth recapping. At 10:30 am Jack Adcock, a 6-year-old boy with Down’s, was referred to LRI emergency department with a 12-hour history of diarrhea and vomiting by his GP. He was..
SJ – Sorry to interrupt. What do you mean by “referred to ED by GP”? And what was the GP’s presumptive diagnosis?
JC – As you know from your days in the NHS, a patient can come to the ED on their own or be referred by their GP. The Adcocks took Jack to his GP who instantly recognized that he was ill and referred him to the Children’s Assessment Unit (CAU).
SJ – What was his diagnosis? Did the GP suspect sepsis?
JC – He recognized that Jack was ill. The GP managed Jack well, in so far as he instructed his parents to bring him to the CAU, instantly – which they did. In the CAU he was assessed by an experienced nurse who, instantly realizing he was ill, called Hadiza immediately. Hadiza came over urgently and assessed Jack.
SJ – So the first hour of Jack’s care was exemplary.
JC – There’s not much more Hadiza could have done in her initial assessment. Even the prosecution did not fault her immediate management of Jack. Hadiza did blood gases, basic blood tests, and ordered a chest x-ray for Jack. She prescribed both a fluid bolus and maintenance fluids.
SJ – What was her presumptive diagnosis?
JC – Her diagnosis was shock. Shock can be hypovolemic, cardiogenic or septic. Given Jack’s presentation of diarrhea and vomiting, she believed it was hypovolemic. Given his history of repaired atrial septal defect, cardiogenic shock was also in her differential, and influenced the rate the fluids were administered.
SJ – Did she suspect sepsis?
JC – It wasn’t as high as hypovolemic shock in her differential. I recall you wrote in your piece that the fact she got a chest-ray meant that infection was also in her differential. I agree with that assessment. Also, she obtained a CRP, which was a foresight that she may need to distinguish between bacterial and viral infections. CRP is not a part of the routine blood panel – you have to request it separately.
SJ – What did the first set of blood gases show?
JC –The pH was 7. The lactate was elevated.
SJ – The lactate was 11. Should these numbers have been a clincher for sepsis?
JC – You mean septic shock. I think they should certainly have raised the index of suspicion. But they are not pathognomonic for septic shock. I’ve seen kids with hypovolemic shock with ph’s of 6.9.
SJ – There seems to be a general meme in the public space that Jack’s blood was “full of acid” and that somehow indicated septicemia.
JC – The ph in and of itself isn’t specific for septic shock but is indicative of shock in general. A case can be made that an elevated lactate is suggestive of sepsis, but lactate can be elevated in conditions other than sepsis. Also, 2011 was before we knew a whole lot about sepsis and lactates. It was before mass awareness of sepsis. Lactate wasn’t routinely obtained in ill patients, then. In any case, after the fluid bolus, Hadiza reassessed Jack. He had perked up, was playful, and far more resistant when Hadiza repeated blood gases.
SJ – What did the second set of blood gases show?
JC – There was a problem with the machine. It was unable to record the lactate, but it recorded the ph which was 7.24.
SJ – Normal ph is 7.4, so it was moving in the right direction after the fluid bolus. But we don’t know what the repeat lactate was.
JC – No, we don’t know the lactate – which’ll always be an unknown counterfactual. But the normalizing ph confirmed for Hadiza, as it’d have confirmed for any pediatrician, that the working diagnosis of hypovolemic shock from viral gastroenteritis wasn’t unreasonable.
SJ – And depending on the outcome, that is in hindsight, this is either confirmation or confirmation bias – a mark of clinical acumen or a flaw of judgment. Regardless, it’s fair to say that a doctor who is cautious about fluid administration because of patient’s heart disease, rechecks a patient’s status within an hour, gets specialized blood tests such as CRP, isn’t an indifferent doctor, isn’t a slacker, but a highly thoughtful doctor.
JC – Yes, and that’s what makes this case even more painful. Hadiza is diligent and thoughtful. Despite the fact that she did not immediately diagnose sepsis, her management of Jack was thoughtful.
SJ – Many can’t fathom that a doctor can be thoughtful but still be wrong. One criticism was that the chest x-ray, though performed at 12:30 pm, wasn’t reviewed by Dr. Bawa-Garba until 3 pm.
JC – By the time the chest x-ray was done, and it was done after the second set of blood gases were analyzed, she was, understandably, more certain about her diagnosis of hypovolemic shock because the ph had improved and Jack was perking up. But also bear in mind she was being beeped incessantly, as she was covering more than just the CAU, more than what is safe for a single registrar to cover. She was running around the hospital.
SJ – I can actually picture that. Running up and down flights of stairs to various wards in various parts of the hospital, dashing to the nearest phone to answer her beep, accumulating scraps of paper. It’s easy to forget that chest x-ray that you ordered but you don’t know when it was done, because you’re not told that it was done, let alone that it had an abnormality. For contrast – at my institution, when pneumonia is suspected by the emergency department, a radiologist is supposed to report the chest radiograph in 30 minutes, and call the physician if there is pneumonia.
JC – It was a busy day. Her juniors were new to pediatrics. In the meantime, she had to perform a lumbar puncture (LP) on a patient with suspected meningitis because no one in her team knew how to. You don’t want to be distracted whilst performing an LP in a child.
SJ – And you can imagine that there’s a parallel universe where she spent the entire time in the CAU with Jack, and the kid with suspected meningitis died from meningitis because no one could perform an LP. What of the IT systems being down? What effect did that have?
JC – A lot. One of the juniors on her team spent most of the time calling pathology for results for their patients. Jack wasn’t the only patient she was looking after.
SJ – That’s quite an opportunity cost. So, instead of seeing patients and doing a H&P, the junior doctor was phoning the labs – what a waste. This, of course, meant that Dr. Bawa-Garba had to pick up the slack, and do the work of her juniors.
JC – There was another consequence. When Hadiza phoned pathology for Jack’s results, a frustrated individual, frustrated at being phoned for results all day, recited all of Jack’s results, including creatinine. Normally, what happens is that the results populate in the patient’s records and the abnormal results are highlighted. Jack’s creatinine was mildly elevated. She was told the creatinine, non-judgmentally – i.e. she was not told that it was elevated. When you’re reliant on a system which flags abnormal results it’s easy to miss a mild abnormality when it’s not flagged.
SJ – She returns to Jack at 3 pm. This is her third assessment of Jack, within 5 hours, so she clearly had not forgotten about Jack. Now she looks at the chest x-ray. Did that show barn door pneumonia?
JC – Like a lobar consolidation? No, the abnormalities were subtler, fluffier, and obscured the right heart border. You could make the case that they represented either viral bronchiolitis or bacterial pneumonia.
SJ – Another layer of subtlety added to the complexity of this case. So now she prescribes antibiotics, which were administered an hour later. What was Jack like then?
JC – He had perked up substantially. He was laughing and being playful. Whatever was going on inside his circulation unbeknownst to everyone, externally he no longer appeared ill. Here’s an indication that everyone believed that Jack was on the mend – Jack’s father returned home in the evening. He wouldn’t have done that if Jack hadn’t perked up.
SJ – It’s around 4 pm that she meets Dr. O’Riordan, her consultant, during handover. She tells him about Jack and shows him the blood gases. Neither did she ask O’Riordan to assess Jack nor did O’Riordan offer to assess Jack after seeing his original biochemical profile. It’s fair to say that O’Riordan agreed with her management.
JC – I’ll expand on O’Riordan’s role a bit later because his role in this case is significant. It’s important, also, to understand what was happening on the nursing side. The pediatric nurses are excellent at LRI. As happens far too often in the NHS, acute services are often short of nursing staff. Jack was being looked after by an agency nurse – who wasn’t a pediatric nurse.
SJ – So, some of Jack’s care fell short, as a result.
JC – Some crucial elements of his care fell short. His vital signs weren’t being recorded with the diligence they deserved. There was no record of his fluid input-output. For example, his nappies had not been weighed. The weight of nappies is an indicator of fluid loss.
SJ – This seems like a systems issue rather than Dr. Bawa-Garba’s responsibility. A pediatric registrar can’t possibly be expected to watch over every single element of care of every single patient – this is humanly impossible and inhumane to demand. The system works when every member of the team does what they’re supposed to be doing – i.e. does their job.
JC – Unfortunately, Hadiza was blamed for not spotting the failings of the nursing staff. She reassessed Jack, at 6 pm. She did not look at his observation chart – perhaps because she felt she did not need to. Jack was playful, like a 6 year old should be, and seemed to be heading in the right direction. She didn’t feel the need for consultant review because Jack seemed to be getting better.
SJ – By 6 pm – i.e. 8 hours in the hospital, what was going on inside Jack’s circulation, hemodynamically speaking?
JC – We know from the autopsy that Jack died from Steptococcus A septicemia. We don’t know his vital signs around 7 pm, or his ph. But, that he was mentally alert and playful, meant that his circulatory system may have been in compensation mode, meaning that his homeostatic mechanisms – the ones which constrict the arteries and maintain the blood pressure, may have been in overdrive mode, and may have been at the end of their tethers, and may have only just been successfully maintaining his blood pressure.
SJ – Jack, internally, was waging a war against Streptococcus. Then there was a decisive turning point.
JC – Yes, then what happened was that Jack was transferred to the ward. After the transfer he received his maintenance dose of enalapril. An hour later he went into cardiac arrest. The cause of Jack’s death was Group A Streptococcus. However, many doctors are concerned that what delivered Jack the fatal blow was the enalapril. To recap, enalapril is an angiotensin converting enzyme inhibitor. It dilates the arteries. It undid the compensatory overdrive of Jack’s circulatory system, the overdrive which was so important in maintaining his blood pressure.
SJ – Who administered the enalapril?
JC – This is complicated. Hadiza stopped the enalapril. She deliberately did not prescribe it on the drug chart. LRI has a policy that family members can give maintenance drugs to patients without them being written on the drug chart. Hadiza was not aware of this policy. Jack’s mother asked the nurse to give the enalapril. The nurse asked one of the junior doctors, who said it was fine for Jack’s mother to give the enalapril.
SJ – Was it Dr. Bawa-Garba who approved the enalapril?
JC – It was not clear who it was – it was one of the junior doctors – not Hadiza. He later said he couldn’t remember whether he said it was okay, or not, for Jack’s mother to give the enalapril.
SJ – Do you believe him?
JC – Well, it’s certainly plausible. Doctors give a lot of verbal orders – they can’t possibly remember each and every one of them.
SJ – But it wasn’t the fault of Jack’s mother.
JC – Only a mean-spirited person will blame Jack’s mother for giving Jack the enalapril. It wasn’t her fault. She did what she thought was the right thing to do, and checked that this was OK with healthcare staff.
SJ – And it wasn’t Dr. Bawa-Garba’s fault either.
JC – No. It’s unfair to expect her to anticipate every contingency. She was new to the CAU – she was unaware of its policies. How could she have known that she should tell Jack’s mother not to administer enalapril when the usual practice in hospitals is for drugs to be administered by nurses not parents?
SJ – So, it was the fault of neither Dr. Bawa-Garba nor Jack’s mother, nor the house officer who, allegedly, sanctioned the administration of enalapril. Whose fault was it then? It must have been someone’s fault.
JC – The system. No individual owns the blame here.
SJ – Dr. Bawa-Garba called of the cardiac arrest, briefly, mistaking Jack for another patient. This didn’t look good on her during her trial. Was this because she was fatigued?
JC – Hadiza had been on her feet for thirteen hours by the time Jack went into cardiac arrest. Anyone would have been tired at that point. But the issue wasn’t just tiredness. Earlier in the day a pediatric oncologist told her over the phone that a child with brain tumor was “not for resuscitation.” The child was going to be moved to a palliative care facility. Hadiza scribbled the ward and bed the child was in, and committed that information to memory.
SJ – But that still does not explain why she mixed up Jack with that child.
JC – Wait, I haven’t finished. The child with the incurable brain tumor was sent to a palliative care facility – i.e. was discharged from hospital. Hadiza was not told about his discharge. She still believed the child was in the hospital. Jack was sent to his bed – i.e. same ward, same bed, as the child who was not for resuscitation.
SJ – There’s a cruel irony here – despite Dr. Bawa-Garba being at her wits end, she still had the wherewithal to recall the child who was not for resuscitation. She got his location magnificently right, but was still terribly wrong.
And what an incredible bad luck for everyone involved. What an unfortunate storm of events for Jack and Dr. Bawa-Garba. Even the best sailors can’t stop a boat from capsizing in the severest of storms. To blame the sailor and ignore the storm is no justice.
JC – I agree. Hadiza did not kill Jack. He was killed by Group A Streptococcus. An overstrained system failed to save him from a very dangerous organism.
About the Author:
Saurabh Jha is a radiologist and contributing editor to THCB. He was once a junior doctor in the NHS. He can be reached on Twitter @RogueRad
The Doctor Who Thwarted the Charge of the General Medical Council – Part 1 published first on https://wittooth.tumblr.com/
0 notes
Text
The Doctor Who Thwarted the Charge of the General Medical Council – Part 1
By SAURABH JHA
After Dr. Hadiza Bawa-Garba was convicted for manslaughter for delayed diagnosis of fatal sepsis in Jack Adcock, a six-year-old boy who presented to Leicester Royal Infirmary with diarrhea and vomiting, she was referred to the Medical Practitioners Tribunal (MPT). The General Medical Council (GMC) is the professional regulatory body for physicians. But the MPT determines whether a physician is fit to practice. Though the tribunal is nested within the GMC and therefore within an earshot of its opinions, it is a decision-making body which is theoretically independent of the GMC.
The tribunal met in 2017, 6 years after Jack’s death, to decide whether Dr. Bawa-Garba, after the manslaughter conviction, should be allowed to practice medicine again, whether she should be suspended for a year, or her name be permanently erased (“struck off”) from the medical register. The GMC wanted Dr. Bawa-Garba to be struck off from the medical register because they felt that her care of Jack fell so short of the expected standard, that her return to practice would not only endanger patients but undermine public confidence in the medical profession. The GMC expected the MPT to agree with its uncompromising stance, and the MPT might well have, and probably would have, but for the efforts of Dr. Jonathan Cusack, a consultant neonatologist at Leicester Royal Infirmary (LRI), and a former supervisor and mentor of Dr. Bawa-Garba’s.
Cusack is unassuming even by British standards. You will not find him on social media or taking selfies. A soft-spoken northerner with a steely nerve and an uncompromising deference to facts, Cusack is both old-school and new-school. He has that unassailable integrity which is immeasurable but instantly recognizable. But he’s also savvy – and understands the British medical, regulatory and legal systems inside out. If Dr. Bawa-Garba’s license is reinstated, Cusack’s role would be akin to that of the code breakers in the Second World War. Dr. Bawa-Garba trusts him implicitly. Her legal team can’t function without him.
Cusack was loyally involved in both the rehabilitation of Dr. Bawa-Garba’s clinical confidence after Jack’s death, and her trial. I met him after the first day’s appeal hearing in the pub opposite the Courts of Justice. Originally hesitant to speak to me, being the ostentatious expat Brit that I am, he agreed to an interview on the condition that I not make too much of a song and dance about his contribution. I promised that I wouldn’t. I lied.
Here’s an excerpt of our conversation about the intricacies of the case.
Saurabh Jha (SJ) – Many say you’re the reason the tribunal did not strike Dr. Bawa-Garba off the medical register, and only suspended her for a year.
Jonathan Cusack (JC) – I’m not sure I deserve to be singled out. The facts, by facts I mean Hadiza’s competence as a clinical pediatrician, were irrefutable. I will say that I collected the evidence verifying her clinical competence.
SJ – I can tell by your accent that you were raised in the north. Mind you, I think anything north of Milton Keynes is north.
JC – I’m from the Birmingham, not the North! I went to medical school in Leicester. I did my pediatric training in the Leicester Deanery. I also worked in Australia, in the Northern Territory – Darwin and Alice Springs.
SJ- Can we recap the events of the fateful Friday – February 18th, 2011.
JC ��� The events have been recorded and dissected but it’s worth recapping. At 10:30 am Jack Adcock, a 6-year-old boy with Down’s, was referred to LRI emergency department with a 12-hour history of diarrhea and vomiting by his GP. He was..
SJ – Sorry to interrupt. What do you mean by “referred to ED by GP”? And what was the GP’s presumptive diagnosis?
JC – As you know from your days in the NHS, a patient can come to the ED on their own or be referred by their GP. The Adcocks took Jack to his GP who instantly recognized that he was ill and referred him to the Children’s Assessment Unit (CAU).
SJ – What was his diagnosis? Did the GP suspect sepsis?
JC – He recognized that Jack was ill. The GP managed Jack well, in so far as he instructed his parents to bring him to the CAU, instantly – which they did. In the CAU he was assessed by an experienced nurse who, instantly realizing he was ill, called Hadiza immediately. Hadiza came over urgently and assessed Jack.
SJ – So the first hour of Jack’s care was exemplary.
JC – There’s not much more Hadiza could have done in her initial assessment. Even the prosecution did not fault her immediate management of Jack. Hadiza did blood gases, basic blood tests, and ordered a chest x-ray for Jack. She prescribed both a fluid bolus and maintenance fluids.
SJ – What was her presumptive diagnosis?
JC – Her diagnosis was shock. Shock can be hypovolemic, cardiogenic or septic. Given Jack’s presentation of diarrhea and vomiting, she believed it was hypovolemic. Given his history of repaired atrial septal defect, cardiogenic shock was also in her differential, and influenced the rate the fluids were administered.
SJ – Did she suspect sepsis?
JC – It wasn’t as high as hypovolemic shock in her differential. I recall you wrote in your piece that the fact she got a chest-ray meant that infection was also in her differential. I agree with that assessment. Also, she obtained a CRP, which was a foresight that she may need to distinguish between bacterial and viral infections. CRP is not a part of the routine blood panel – you have to request it separately.
SJ – What did the first set of blood gases show?
JC –The pH was 7. The lactate was elevated.
SJ – The lactate was 11. Should these numbers have been a clincher for sepsis?
JC – You mean septic shock. I think they should certainly have raised the index of suspicion. But they are not pathognomonic for septic shock. I’ve seen kids with hypovolemic shock with ph’s of 6.9.
SJ – There seems to be a general meme in the public space that Jack’s blood was “full of acid” and that somehow indicated septicemia.
JC – The ph in and of itself isn’t specific for septic shock but is indicative of shock in general. A case can be made that an elevated lactate is suggestive of sepsis, but lactate can be elevated in conditions other than sepsis. Also, 2011 was before we knew a whole lot about sepsis and lactates. It was before mass awareness of sepsis. Lactate wasn’t routinely obtained in ill patients, then. In any case, after the fluid bolus, Hadiza reassessed Jack. He had perked up, was playful, and far more resistant when Hadiza repeated blood gases.
SJ – What did the second set of blood gases show?
JC – There was a problem with the machine. It was unable to record the lactate, but it recorded the ph which was 7.24.
SJ – Normal ph is 7.4, so it was moving in the right direction after the fluid bolus. But we don’t know what the repeat lactate was.
JC – No, we don’t know the lactate – which’ll always be an unknown counterfactual. But the normalizing ph confirmed for Hadiza, as it’d have confirmed for any pediatrician, that the working diagnosis of hypovolemic shock from viral gastroenteritis wasn’t unreasonable.
SJ – And depending on the outcome, that is in hindsight, this is either confirmation or confirmation bias – a mark of clinical acumen or a flaw of judgment. Regardless, it’s fair to say that a doctor who is cautious about fluid administration because of patient’s heart disease, rechecks a patient’s status within an hour, gets specialized blood tests such as CRP, isn’t an indifferent doctor, isn’t a slacker, but a highly thoughtful doctor.
JC – Yes, and that’s what makes this case even more painful. Hadiza is diligent and thoughtful. Despite the fact that she did not immediately diagnose sepsis, her management of Jack was thoughtful.
SJ – Many can’t fathom that a doctor can be thoughtful but still be wrong. One criticism was that the chest x-ray, though performed at 12:30 pm, wasn’t reviewed by Dr. Bawa-Garba until 3 pm.
JC – By the time the chest x-ray was done, and it was done after the second set of blood gases were analyzed, she was, understandably, more certain about her diagnosis of hypovolemic shock because the ph had improved and Jack was perking up. But also bear in mind she was being beeped incessantly, as she was covering more than just the CAU, more than what is safe for a single registrar to cover. She was running around the hospital.
SJ – I can actually picture that. Running up and down flights of stairs to various wards in various parts of the hospital, dashing to the nearest phone to answer her beep, accumulating scraps of paper. It’s easy to forget that chest x-ray that you ordered but you don’t know when it was done, because you’re not told that it was done, let alone that it had an abnormality. For contrast – at my institution, when pneumonia is suspected by the emergency department, a radiologist is supposed to report the chest radiograph in 30 minutes, and call the physician if there is pneumonia.
JC – It was a busy day. Her juniors were new to pediatrics. In the meantime, she had to perform a lumbar puncture (LP) on a patient with suspected meningitis because no one in her team knew how to. You don’t want to be distracted whilst performing an LP in a child.
SJ – And you can imagine that there’s a parallel universe where she spent the entire time in the CAU with Jack, and the kid with suspected meningitis died from meningitis because no one could perform an LP. What of the IT systems being down? What effect did that have?
JC – A lot. One of the juniors on her team spent most of the time calling pathology for results for their patients. Jack wasn’t the only patient she was looking after.
SJ – That’s quite an opportunity cost. So, instead of seeing patients and doing a H&P, the junior doctor was phoning the labs – what a waste. This, of course, meant that Dr. Bawa-Garba had to pick up the slack, and do the work of her juniors.
JC – There was another consequence. When Hadiza phoned pathology for Jack’s results, a frustrated individual, frustrated at being phoned for results all day, recited all of Jack’s results, including creatinine. Normally, what happens is that the results populate in the patient’s records and the abnormal results are highlighted. Jack’s creatinine was mildly elevated. She was told the creatinine, non-judgmentally – i.e. she was not told that it was elevated. When you’re reliant on a system which flags abnormal results it’s easy to miss a mild abnormality when it’s not flagged.
SJ – She returns to Jack at 3 pm. This is her third assessment of Jack, within 5 hours, so she clearly had not forgotten about Jack. Now she looks at the chest x-ray. Did that show barn door pneumonia?
JC – Like a lobar consolidation? No, the abnormalities were subtler, fluffier, and obscured the right heart border. You could make the case that they represented either viral bronchiolitis or bacterial pneumonia.
SJ – Another layer of subtlety added to the complexity of this case. So now she prescribes antibiotics, which were administered an hour later. What was Jack like then?
JC – He had perked up substantially. He was laughing and being playful. Whatever was going on inside his circulation unbeknownst to everyone, externally he no longer appeared ill. Here’s an indication that everyone believed that Jack was on the mend – Jack’s father returned home in the evening. He wouldn’t have done that if Jack hadn’t perked up.
SJ – It’s around 4 pm that she meets Dr. O’Riordan, her consultant, during handover. She tells him about Jack and shows him the blood gases. Neither did she ask O’Riordan to assess Jack nor did O’Riordan offer to assess Jack after seeing his original biochemical profile. It’s fair to say that O’Riordan agreed with her management.
JC – I’ll expand on O’Riordan’s role a bit later because his role in this case is significant. It’s important, also, to understand what was happening on the nursing side. The pediatric nurses are excellent at LRI. As happens far too often in the NHS, acute services are often short of nursing staff. Jack was being looked after by an agency nurse – who wasn’t a pediatric nurse.
SJ – So, some of Jack’s care fell short, as a result.
JC – Some crucial elements of his care fell short. His vital signs weren’t being recorded with the diligence they deserved. There was no record of his fluid input-output. For example, his nappies had not been weighed. The weight of nappies is an indicator of fluid loss.
SJ – This seems like a systems issue rather than Dr. Bawa-Garba’s responsibility. A pediatric registrar can’t possibly be expected to watch over every single element of care of every single patient – this is humanly impossible and inhumane to demand. The system works when every member of the team does what they’re supposed to be doing – i.e. does their job.
JC – Unfortunately, Hadiza was blamed for not spotting the failings of the nursing staff. She reassessed Jack, at 6 pm. She did not look at his observation chart – perhaps because she felt she did not need to. Jack was playful, like a 6 year old should be, and seemed to be heading in the right direction. She didn’t feel the need for consultant review because Jack seemed to be getting better.
SJ – By 6 pm – i.e. 8 hours in the hospital, what was going on inside Jack’s circulation, hemodynamically speaking?
JC – We know from the autopsy that Jack died from Steptococcus A septicemia. We don’t know his vital signs around 7 pm, or his ph. But, that he was mentally alert and playful, meant that his circulatory system may have been in compensation mode, meaning that his homeostatic mechanisms – the ones which constrict the arteries and maintain the blood pressure, may have been in overdrive mode, and may have been at the end of their tethers, and may have only just been successfully maintaining his blood pressure.
SJ – Jack, internally, was waging a war against Streptococcus. Then there was a decisive turning point.
JC – Yes, then what happened was that Jack was transferred to the ward. After the transfer he received his maintenance dose of enalapril. An hour later he went into cardiac arrest. The cause of Jack’s death was Group A Streptococcus. However, many doctors are concerned that what delivered Jack the fatal blow was the enalapril. To recap, enalapril is an angiotensin converting enzyme inhibitor. It dilates the arteries. It undid the compensatory overdrive of Jack’s circulatory system, the overdrive which was so important in maintaining his blood pressure.
SJ – Who administered the enalapril?
JC – This is complicated. Hadiza stopped the enalapril. She deliberately did not prescribe it on the drug chart. LRI has a policy that family members can give maintenance drugs to patients without them being written on the drug chart. Hadiza was not aware of this policy. Jack’s mother asked the nurse to give the enalapril. The nurse asked one of the junior doctors, who said it was fine for Jack’s mother to give the enalapril.
SJ – Was it Dr. Bawa-Garba who approved the enalapril?
JC – It was not clear who it was – it was one of the junior doctors – not Hadiza. He later said he couldn’t remember whether he said it was okay, or not, for Jack’s mother to give the enalapril.
SJ – Do you believe him?
JC – Well, it’s certainly plausible. Doctors give a lot of verbal orders – they can’t possibly remember each and every one of them.
SJ – But it wasn’t the fault of Jack’s mother.
JC – Only a mean-spirited person will blame Jack’s mother for giving Jack the enalapril. It wasn’t her fault. She did what she thought was the right thing to do, and checked that this was OK with healthcare staff.
SJ – And it wasn’t Dr. Bawa-Garba’s fault either.
JC – No. It’s unfair to expect her to anticipate every contingency. She was new to the CAU – she was unaware of its policies. How could she have known that she should tell Jack’s mother not to administer enalapril when the usual practice in hospitals is for drugs to be administered by nurses not parents?
SJ – So, it was the fault of neither Dr. Bawa-Garba nor Jack’s mother, nor the house officer who, allegedly, sanctioned the administration of enalapril. Whose fault was it then? It must have been someone’s fault.
JC – The system. No individual owns the blame here.
SJ – Dr. Bawa-Garba called of the cardiac arrest, briefly, mistaking Jack for another patient. This didn’t look good on her during her trial. Was this because she was fatigued?
JC – Hadiza had been on her feet for thirteen hours by the time Jack went into cardiac arrest. Anyone would have been tired at that point. But the issue wasn’t just tiredness. Earlier in the day a pediatric oncologist told her over the phone that a child with brain tumor was “not for resuscitation.” The child was going to be moved to a palliative care facility. Hadiza scribbled the ward and bed the child was in, and committed that information to memory.
SJ – But that still does not explain why she mixed up Jack with that child.
JC – Wait, I haven’t finished. The child with the incurable brain tumor was sent to a palliative care facility – i.e. was discharged from hospital. Hadiza was not told about his discharge. She still believed the child was in the hospital. Jack was sent to his bed – i.e. same ward, same bed, as the child who was not for resuscitation.
SJ – There’s a cruel irony here – despite Dr. Bawa-Garba being at her wits end, she still had the wherewithal to recall the child who was not for resuscitation. She got his location magnificently right, but was still terribly wrong.
And what an incredible bad luck for everyone involved. What an unfortunate storm of events for Jack and Dr. Bawa-Garba. Even the best sailors can’t stop a boat from capsizing in the severest of storms. To blame the sailor and ignore the storm is no justice.
JC – I agree. Hadiza did not kill Jack. He was killed by Group A Streptococcus. An overstrained system failed to save him from a very dangerous organism.
About the Author:
Saurabh Jha is a radiologist and contributing editor to THCB. He was once a junior doctor in the NHS. He can be reached @RogueRad
The Doctor Who Thwarted the Charge of the General Medical Council – Part 1 published first on https://wittooth.tumblr.com/
0 notes
Text
The Doctor Who Thwarted the Charge of the General Medical Council – Part 1
By SAURABH JHA
After Dr. Hadiza Bawa-Garba was convicted for manslaughter for delayed diagnosis of fatal sepsis in Jack Adcock, a six-year-old boy who presented to Leicester Royal Infirmary with diarrhea and vomiting, she was referred to the Medical Practitioners Tribunal (MPT). The General Medical Council (GMC) is the professional regulatory body for physicians. But the MPT determines whether a physician is fit to practice. Though the tribunal is nested within the GMC and therefore within an earshot of its opinions, it is a decision-making body which is theoretically independent of the GMC.
The tribunal met in 2017, 6 years after Jack’s death, to decide whether Dr. Bawa-Garba, after the manslaughter conviction, should be allowed to practice medicine again, whether she should be suspended for a year, or her name be permanently erased (“struck off”) from the medical register. The GMC wanted Dr. Bawa-Garba to be struck off from the medical register because they felt that her care of Jack fell so short of the expected standard, that her return to practice would not only endanger patients but undermine public confidence in the medical profession. The GMC expected the MPT to agree with its uncompromising stance, and the MPT might well have, and probably would have, but for the efforts of Dr. Jonathan Cusack, a consultant neonatologist at Leicester Royal Infirmary (LRI), and a former supervisor and mentor of Dr. Bawa-Garba’s.
Cusack is unassuming even by British standards. You will not find him on social media or taking selfies. A soft-spoken northerner with a steely nerve and an uncompromising deference to facts, Cusack is both old-school and new-school. He has that unassailable integrity which is immeasurable but instantly recognizable. But he’s also savvy – and understands the British medical, regulatory and legal systems inside out. If Dr. Bawa-Garba’s license is reinstated, Cusack’s role would be akin to that of the code breakers in the Second World War. Dr. Bawa-Garba trusts him implicitly. Her legal team can’t function without him.
Cusack was loyally involved in both the rehabilitation of Dr. Bawa-Garba’s clinical confidence after Jack’s death, and her trial. I met him after the first day’s appeal hearing in the pub opposite the Courts of Justice. Originally hesitant to speak to me, being the ostentatious expat Brit that I am, he agreed to an interview on the condition that I not make too much of a song and dance about his contribution. I promised that I wouldn’t. I lied.
Here’s an excerpt of our conversation about the intricacies of the case.
Saurabh Jha (SJ) – Many say you’re the reason the tribunal did not strike Dr. Bawa-Garba off the medical register, and only suspended her for a year.
Jonathan Cusack (JC) – I’m not sure I deserve to be singled out. The facts, by facts I mean Hadiza’s competence as a clinical pediatrician, were irrefutable. I will say that I collected the evidence verifying her clinical competence.
SJ – I can tell by your accent that you were raised in the north. Mind you, I think anything north of Milton Keynes is north.
JC – I’m from the Birmingham, not the North! I went to medical school in Leicester. I did my pediatric training in the Leicester Deanery. I also worked in Australia, in the Northern Territory – Darwin and Alice Springs.
SJ- Can we recap the events of the fateful Friday – February 18th, 2011.
JC – The events have been recorded and dissected but it’s worth recapping. At 10:30 am Jack Adcock, a 6-year-old boy with Down’s, was referred to LRI emergency department with a 12-hour history of diarrhea and vomiting by his GP. He was..
SJ – Sorry to interrupt. What do you mean by “referred to ED by GP”? And what was the GP’s presumptive diagnosis?
JC – As you know from your days in the NHS, a patient can come to the ED on their own or be referred by their GP. The Adcocks took Jack to his GP who instantly recognized that he was ill and referred him to the Children’s Assessment Unit (CAU).
SJ – What was his diagnosis? Did the GP suspect sepsis?
JC – He recognized that Jack was ill. The GP managed Jack well, in so far as he instructed his parents to bring him to the CAU, instantly – which they did. In the CAU he was assessed by an experienced nurse who, instantly realizing he was ill, called Hadiza immediately. Hadiza came over urgently and assessed Jack.
SJ – So the first hour of Jack’s care was exemplary.
JC – There’s not much more Hadiza could have done in her initial assessment. Even the prosecution did not fault her immediate management of Jack. Hadiza did blood gases, basic blood tests, and ordered a chest x-ray for Jack. She prescribed both a fluid bolus and maintenance fluids.
SJ – What was her presumptive diagnosis?
JC – Her diagnosis was shock. Shock can be hypovolemic, cardiogenic or septic. Given Jack’s presentation of diarrhea and vomiting, she believed it was hypovolemic. Given his history of repaired atrial septal defect, cardiogenic shock was also in her differential, and influenced the rate the fluids were administered.
SJ – Did she suspect sepsis?
JC – It wasn’t as high as hypovolemic shock in her differential. I recall you wrote in your piece that the fact she got a chest-ray meant that infection was also in her differential. I agree with that assessment. Also, she obtained a CRP, which was a foresight that she may need to distinguish between bacterial and viral infections. CRP is not a part of the routine blood panel – you have to request it separately.
SJ – What did the first set of blood gases show?
JC –The pH was 7. The lactate was elevated.
SJ – The lactate was 11. Should these numbers have been a clincher for sepsis?
JC – You mean septic shock. I think they should certainly have raised the index of suspicion. But they are not pathognomonic for septic shock. I’ve seen kids with hypovolemic shock with ph’s of 6.9.
SJ – There seems to be a general meme in the public space that Jack’s blood was “full of acid” and that somehow indicated septicemia.
JC – The ph in and of itself isn’t specific for septic shock but is indicative of shock in general. A case can be made that an elevated lactate is suggestive of sepsis, but lactate can be elevated in conditions other than sepsis. Also, 2011 was before we knew a whole lot about sepsis and lactates. It was before mass awareness of sepsis. Lactate wasn’t routinely obtained in ill patients, then. In any case, after the fluid bolus, Hadiza reassessed Jack. He had perked up, was playful, and far more resistant when Hadiza repeated blood gases.
SJ – What did the second set of blood gases show?
JC – There was a problem with the machine. It was unable to record the lactate, but it recorded the ph which was 7.24.
SJ – Normal ph is 7.4, so it was moving in the right direction after the fluid bolus. But we don’t know what the repeat lactate was.
JC – No, we don’t know the lactate – which’ll always be an unknown counterfactual. But the normalizing ph confirmed for Hadiza, as it’d have confirmed for any pediatrician, that the working diagnosis of hypovolemic shock from viral gastroenteritis wasn’t unreasonable.
SJ – And depending on the outcome, that is in hindsight, this is either confirmation or confirmation bias – a mark of clinical acumen or a flaw of judgment. Regardless, it’s fair to say that a doctor who is cautious about fluid administration because of patient’s heart disease, rechecks a patient’s status within an hour, gets specialized blood tests such as CRP, isn’t an indifferent doctor, isn’t a slacker, but a highly thoughtful doctor.
JC – Yes, and that’s what makes this case even more painful. Hadiza is diligent and thoughtful. Despite the fact that she did not immediately diagnose sepsis, her management of Jack was thoughtful.
SJ – Many can’t fathom that a doctor can be thoughtful but still be wrong. One criticism was that the chest x-ray, though performed at 12:30 pm, wasn’t reviewed by Dr. Bawa-Garba until 3 pm.
JC – By the time the chest x-ray was done, and it was done after the second set of blood gases were analyzed, she was, understandably, more certain about her diagnosis of hypovolemic shock because the ph had improved and Jack was perking up. But also bear in mind she was being beeped incessantly, as she was covering more than just the CAU, more than what is safe for a single registrar to cover. She was running around the hospital.
SJ – I can actually picture that. Running up and down flights of stairs to various wards in various parts of the hospital, dashing to the nearest phone to answer her beep, accumulating scraps of paper. It’s easy to forget that chest x-ray that you ordered but you don’t know when it was done, because you’re not told that it was done, let alone that it had an abnormality. For contrast – at my institution, when pneumonia is suspected by the emergency department, a radiologist is supposed to report the chest radiograph in 30 minutes, and call the physician if there is pneumonia.
JC – It was a busy day. Her juniors were new to pediatrics. In the meantime, she had to perform a lumbar puncture (LP) on a patient with suspected meningitis because no one in her team knew how to. You don’t want to be distracted whilst performing an LP in a child.
SJ – And you can imagine that there’s a parallel universe where she spent the entire time in the CAU with Jack, and the kid with suspected meningitis died from meningitis because no one could perform an LP. What of the IT systems being down? What effect did that have?
JC – A lot. One of the juniors on her team spent most of the time calling pathology for results for their patients. Jack wasn’t the only patient she was looking after.
SJ – That’s quite an opportunity cost. So, instead of seeing patients and doing a H&P, the junior doctor was phoning the labs – what a waste. This, of course, meant that Dr. Bawa-Garba had to pick up the slack, and do the work of her juniors.
JC – There was another consequence. When Hadiza phoned pathology for Jack’s results, a frustrated individual, frustrated at being phoned for results all day, recited all of Jack’s results, including creatinine. Normally, what happens is that the results populate in the patient’s records and the abnormal results are highlighted. Jack’s creatinine was mildly elevated. She was told the creatinine, non-judgmentally – i.e. she was not told that it was elevated. When you’re reliant on a system which flags abnormal results it’s easy to miss a mild abnormality when it’s not flagged.
SJ – She returns to Jack at 3 pm. This is her third assessment of Jack, within 5 hours, so she clearly had not forgotten about Jack. Now she looks at the chest x-ray. Did that show barn door pneumonia?
JC – Like a lobar consolidation? No, the abnormalities were subtler, fluffier, and obscured the right heart border. You could make the case that they represented either viral bronchiolitis or bacterial pneumonia.
SJ – Another layer of subtlety added to the complexity of this case. So now she prescribes antibiotics, which were administered an hour later. What was Jack like then?
JC – He had perked up substantially. He was laughing and being playful. Whatever was going on inside his circulation unbeknownst to everyone, externally he no longer appeared ill. Here’s an indication that everyone believed that Jack was on the mend – Jack’s father returned home in the evening. He wouldn’t have done that if Jack hadn’t perked up.
SJ – It’s around 4 pm that she meets Dr. O’Riordan, her consultant, during handover. She tells him about Jack and shows him the blood gases. Neither did she ask O’Riordan to assess Jack nor did O’Riordan offer to assess Jack after seeing his original biochemical profile. It’s fair to say that O’Riordan agreed with her management.
JC – I’ll expand on O’Riordan’s role a bit later because his role in this case is significant. It’s important, also, to understand what was happening on the nursing side. The pediatric nurses are excellent at LRI. As happens far too often in the NHS, acute services are often short of nursing staff. Jack was being looked after by an agency nurse – who wasn’t a pediatric nurse.
SJ – So, some of Jack’s care fell short, as a result.
JC – Some crucial elements of his care fell short. His vital signs weren’t being recorded with the diligence they deserved. There was no record of his fluid input-output. For example, his nappies had not been weighed. The weight of nappies is an indicator of fluid loss.
SJ – This seems like a systems issue rather than Dr. Bawa-Garba’s responsibility. A pediatric registrar can’t possibly be expected to watch over every single element of care of every single patient – this is humanly impossible and inhumane to demand. The system works when every member of the team does what they’re supposed to be doing – i.e. does their job.
JC – Unfortunately, Hadiza was blamed for not spotting the failings of the nursing staff. She reassessed Jack, at 6 pm. She did not look at his observation chart – perhaps because she felt she did not need to. Jack was playful, like a 6 year old should be, and seemed to be heading in the right direction. She didn’t feel the need for consultant review because Jack seemed to be getting better.
SJ – By 6 pm – i.e. 8 hours in the hospital, what was going on inside Jack’s circulation, hemodynamically speaking?
JC – We know from the autopsy that Jack died from Steptococcus A septicemia. We don’t know his vital signs around 7 pm, or his ph. But, that he was mentally alert and playful, meant that his circulatory system may have been in compensation mode, meaning that his homeostatic mechanisms – the ones which constrict the arteries and maintain the blood pressure, may have been in overdrive mode, and may have been at the end of their tethers, and may have only just been successfully maintaining his blood pressure.
SJ – Jack, internally, was waging a war against Streptococcus. Then there was a decisive turning point.
JC – Yes, then what happened was that Jack was transferred to the ward. After the transfer he received his maintenance dose of enalapril. An hour later he went into cardiac arrest. The cause of Jack’s death was Group A Streptococcus. However, many doctors are concerned that what delivered Jack the fatal blow was the enalapril. To recap, enalapril is an angiotensin converting enzyme inhibitor. It dilates the arteries. It undid the compensatory overdrive of Jack’s circulatory system, the overdrive which was so important in maintaining his blood pressure.
SJ – Who administered the enalapril?
JC – This is complicated. Hadiza stopped the enalapril. She deliberately did not prescribe it on the drug chart. LRI has a policy that family members can give maintenance drugs to patients without them being written on the drug chart. Hadiza was not aware of this policy. Jack’s mother asked the nurse to give the enalapril. The nurse asked one of the junior doctors, who said it was fine for Jack’s mother to give the enalapril.
SJ – Was it Dr. Bawa-Garba who approved the enalapril?
JC – It was not clear who it was – it was one of the junior doctors – not Hadiza. He later said he couldn’t remember whether he said it was okay, or not, for Jack’s mother to give the enalapril.
SJ – Do you believe him?
JC – Well, it’s certainly plausible. Doctors give a lot of verbal orders – they can’t possibly remember each and every one of them.
SJ – But it wasn’t the fault of Jack’s mother.
JC – Only a mean-spirited person will blame Jack’s mother for giving Jack the enalapril. It wasn’t her fault. She did what she thought was the right thing to do, and checked that this was OK with healthcare staff.
SJ – And it wasn’t Dr. Bawa-Garba’s fault either.
JC – No. It’s unfair to expect her to anticipate every contingency. She was new to the CAU – she was unaware of its policies. How could she have known that she should tell Jack’s mother not to administer enalapril when the usual practice in hospitals is for drugs to be administered by nurses not parents?
SJ – So, it was the fault of neither Dr. Bawa-Garba nor Jack’s mother, nor the house officer who, allegedly, sanctioned the administration of enalapril. Whose fault was it then? It must have been someone’s fault.
JC – The system. No individual owns the blame here.
SJ – Dr. Bawa-Garba called of the cardiac arrest, briefly, mistaking Jack for another patient. This didn’t look good on her during her trial. Was this because she was fatigued?
JC – Hadiza had been on her feet for thirteen hours by the time Jack went into cardiac arrest. Anyone would have been tired at that point. But the issue wasn’t just tiredness. Earlier in the day a pediatric oncologist told her over the phone that a child with brain tumor was “not for resuscitation.” The child was going to be moved to a palliative care facility. Hadiza scribbled the ward and bed the child was in, and committed that information to memory.
SJ – But that still does not explain why she mixed up Jack with that child.
JC – Wait, I haven’t finished. The child with the incurable brain tumor was sent to a palliative care facility – i.e. was discharged from hospital. Hadiza was not told about his discharge. She still believed the child was in the hospital. Jack was sent to his bed – i.e. same ward, same bed, as the child who was not for resuscitation.
SJ – There’s a cruel irony here – despite Dr. Bawa-Garba being at her wits end, she still had the wherewithal to recall the child who was not for resuscitation. She got his location magnificently right, but was still terribly wrong.
And what an incredible bad luck for everyone involved. What an unfortunate storm of events for Jack and Dr. Bawa-Garba. Even the best sailors can’t stop a boat from capsizing in the severest of storms. To blame the sailor and ignore the storm is no justice.
JC – I agree. Hadiza did not kill Jack. He was killed by Group A Streptococcus. An overstrained system failed to save him from a very dangerous organism.
About the Author:
Saurabh Jha is a radiologist and contributing editor to THCB. He was once a junior doctor in the NHS. He can be reached @RogueRad
The Doctor Who Thwarted the Charge of the General Medical Council – Part 1 published first on https://wittooth.tumblr.com/
0 notes
Text
[Grindcore|Bandcamp] ATRIAL SEPTIC DEFECT - SPLIT WITH PHLEGMSEPSIA https://t.co/dyakIxsHXk http://pic.twitter.com/pSDFiDNfX1
— Grindcore Music (@grindcore_bot) April 9, 2017
0 notes
Text
[Goregrind|Bandcamp] Phlegmsepsia - split w Atrial Septic Defect https://t.co/CnkEjrjkVj http://pic.twitter.com/AJbeW9TRlL
— Grindcore Music (@grindcore_bot) April 9, 2017
0 notes
Text
[Goregrind|Bandcamp] ATRIAL SEPTIC DEFECT - HEAVILY MASTICATED https://t.co/tKiQllQKCP http://pic.twitter.com/T3ewMrBvD9
— Grindcore Music (@grindcore_bot) February 25, 2017
0 notes
Text
[Grindcore|Bandcamp] ATRIAL SEPTIC DEFECT - HEAVILY MASTICATED https://t.co/sRwW6l7NKx http://pic.twitter.com/tQTD5RufsH
— Grindcore Music (@grindcore_bot) February 25, 2017
0 notes
Text
[Bandcamp] ATRIAL SEPTIC DEFECT - HEAVILY MASTICATED https://t.co/w1VhDDKxYF http://pic.twitter.com/khd8YSaxhK
— #death metal in BC (@dmtag_bot) February 25, 2017
0 notes