#2017. 2021. and all the almosts in between and beyond
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
28.6 is the average number of monthly visits per US mobile user.
Text
Brooks River Hierarchy: Recent History and Potential Contenders
Hierarchy among brown bears is not simple, and importantly, it is not linear. We also don't know a ton about it, because it is very hard to study. In fact, the brown bear cams at Brooks River in Katmai National Park may be the best source of insight we have into this topic.
As a result, I cannot speak to the behavior of brown bears at large -- only to what i've observed myself on the live cams. I also am not a scientist, please don't take anything I say here as a hard-and-true fact. I can only speak to what I have observed, and what I have seen other people say they have observed.
The hierarchy at Brooks River is a complex web of connections between individual bears. While there are broad patterns to these connections, it is ultimately a web of individuals; there is no line along which all bears are placed, and there is no guarantee that there be only one bear-in-charge each season. Boars tend to outrank sows, who tend to outrank subadults, who tend to outrank cubs, but that is a wild oversimplification of what is a very complicated and quite interesting system.
As this post is focused on the very top of the hierarchy, from this point on I will almost exclusively talk about the biggest and most aggressive of the boars.
Recent History
The four most dominant boars are 856, 747, 32 Chunk, and 151 Walker. 856 is likely the oldest of the four, with 747 not all that far behind. 32 Chunk is next, and 151 Walker is the youngest of the group. If we had to estimate ages, then as of 2025, I would put 856 at 26ish, 747 at 24ish, 32 Chunk at 20, and 151 Walker at 18.
856 was the boar at the top of the hierarchy at Brooks River for a long time. He ascended to his position in 2011, when he was probably about 12-13 years old, and he kept it through 2023 -- except 2017, when he was injured, and 2021. But now he's getting old, he's slowing down, and he's chilling out. And that meant that in 2024, it was time for a changing of the guard.
Ultimately, 32 chunk came out on top last year -- both 856 and 747 had chilled out in their old age, and 151 Walker has a long history of getting displaced by other bears (especially 128 Grazer), so 32 chunk seized the opportunity. He was very aggressive, especially early in the season -- he ran other bears off the falls entirely before the salmon even arrived, and he sneak-attacked 747 while the old man was taking a nap! When he went on a long courting journey with 101 in early July, there were lots of jokes about how she was keeping the falls peaceful by dragging him off to the middle of nowhere. This isn't to say that 151 walker didn't put up a fight -- he did! But ultimately, it was 32 Chunk who reigned last year.
But now these next few years could be interesting, because 32 Chunk isn't getting any younger, and there's several other boars who might be looking to take the metaphorical crown for themself.
Potential Contenders
This is entirely speculation & is just for fun.
151 Walker

explore.org capture, taken by me, September 17 2024
I mean, obviously. he's huge and 18 and ready to fight -- though last year he did mostly avoid attacking 32 Chunk, focusing instead on other bears. He's been angling for the top boar position for a few years now, though since he's getting older his opportunity window might be pretty small. I think he's the most likely to displace 32 Chunk in the next year or so, but beyond that, I think it gets tougher for him to beat the younger, faster boars. I also think 503 Cubadult could be a serious challenger to him, even as soon as this coming summer.
503 Cubadult

Explore.org capture, taken by me, September 17 2024
This guy is 12 years old, big as hell (seriously, in early summer he looks like a bear on stilts), and only getting bigger. The main question here, I think, will be whether or not he wants to try and be at the top. Not every boar is the level of dominant or aggressive required to hold that position, and so far he hasn't seemed particularly inclined towards fighting. Though, he does seem to Basically Not Care About 32 Chunk At All. But if he does start leaning towards aggression more heavily, I think the crown could be his pretty quick.
164 Bucky

explore.org capture, taken by me, August 22 2024
This young guy still has a lot of growing to do, as he is only 8 years old. But he is already pretty big, and he's also got a huge attitude, especially with the older, bigger boars. (CW: video of serious bear violence) He had a brutal fight with 151 Walker last year where he refused to back down until 856 showed up, and he is constantly encroaching on other bears' space. I think that if 503 Cubadult doesn't become the level of dominant required, then 164 Bucky has a very serious chance of being in charge -- once his body catches up to his attitude, that is!
If anyone else has thoughts about boars at Brooks River that they think could be in charge in the next few years, i'd love to hear them!!
#katmai national park#katmai#brown bears#katmai bears#bears#ursidae#talking abt bears#decided to write this up now since i have my adhd meds again lol#i think 89 backpack is big enough but i dont think he's interested tbh#too nice and playful lol
33 notes
·
View notes
Text
I just saw some takes on “queer coding” that make me want to scream so I am going to post (part of) a paper I’m writing on queer coding in Supernatural that some of my mutuals encouraged me to post when I talked about it a few days ago. Tl;dr is that queer coding is a negative thing done by othering and/or vilifying a character - this is undisputed in academia and if you use the phrase “queer coded” to mean otherwise you are misusing the phrase.
Fandom has a long-lasting tradition of reading queerness into works of fiction – dating back to the original airing of Star Trek in the 1960s. Supernatural’s fandom has been no different. The show has, in fact, influenced the fandom subculture as a whole more than any other individual TV show this century – though to explore this in detail is beyond the scope of this paper.
The popular queer readings by fans largely center around the intensely macho elder brother, Dean Winchester. While the character’s overperformance of masculinity may lend itself to such readings, it is important to note that he is not traditionally queer coded at all. The vast majority of the traditional queer coding which goes on in the show instead applies to the more sensitive younger brother, Sam Winchester. The extent to which fans refuse to engage with this queer coding is what this section of the paper sets out to explain.
I propose that this reluctance stems from the fact that queer coding is negative. Characters are queer coded through Othering – a process by which they are shown to be different from their communities and from the heroes. The use of this in queer coding is well established – “all the analyzed [queer coded] characters somehow fitting the form of an outcast” (Svobodová, 2022) exemplifies queer coded characters as outcasts. There is also the theme of “monsters as the Other, representing queer people” (Mudry, 2022) and that “[queer coded] characters are meant to symbolise everything that is bad. In the process, they also become the Other,” (Veera, 2023). Queerness and monstrosity are linked through the process of queer coding, and this link makes queerness villainous. Historically this has been used to discourage deviant behavior and encourage conformity to the norm.
The way that this Othering is almost always part of the process of setting up a character as a villain is well established by scholarship that has focused on queer coding broadly (“queer-coded characters are almost always villains,” (Kim, 2017), “most of these [queer coded] characters are villains,” (Brown, 2021)). While many queer people have become fans of villains in response to seeing representation in them as the Other, villains or the monstrous do not appeal to everyone, and queer people are no exception.
While this may very well be a matter of preference, preferences do not form in a vacuum and, especially in the context of politically fraught topics such as queerness, are often indicative of deeper political issues. Even those who are Othered may recoil at unpalatable representations of the Other in fiction. In The Big, the Bad, and the Queer: Analysing the Queer-Coded Villain in Selected Disney Films, it is stated that “Seeing villains that behave in particular, perceivably queer ways creates “a psychological association” between ‘queer’ and ‘evil’ in the minds of children.”” This psychological association has been created through decades of queer coded villains in media and applies to present day characters that exhibit traditionally queer coded monstrous traits. The negative perception of queer coded and monstrous characters can apply to queer people as well as straight people.
Sam Winchester is a traditionally queer coded character. His arc over the first four seasons focuses on him having supernatural abilities that work to Other him. In the world of hunters – those who hunt supernatural beings – all supernatural beings are considered to be evil and are indiscriminately killed. Sam is one of these hunters, as are his family – his brother Dean and his father John. The development of his supernatural abilities over these seasons Others him in relation to his community and his family. The narrative positioning of such abilities as evil also work to position him as an anti-hero in a traditional queer coded villain role.
The show focuses on themes of the monstrous in its monster of the week format, broader plot arcs, and in relation to its main characters. This is often done by paralleling Sam with the monster of the week, done with the werewolf Madison in Heart (2.17) and the rugaru Jack in Metamorphosis (4.4). These parallels further work to place Sam in the role of the monstrous, even while working to humanize the monster of the week.
Queer people who have internalized the messages of queer coded characters as “everything that is bad” from other queer coded media are likely to dislike characters that are queer coded and may wish to distance their own queerness from such portrayals.
#supernatural#queer coding#sam winchester#this is just part of the paper and I do have more it is just a) not presentable yet and b) I plan to publish this and idk how I feel about#posting writing that will be affiliated with my irl name on tumblr
93 notes
·
View notes
Text
My Taekook timeline thoughts
Idea from @blue703.
I'mma try this. Let me preface by saying I'm baby Army, coming up to a year. I pick stuff up fast and I have ADHD so I hyperfixate and deep dive but there's definitely stuff I don't know/am still trying to figure out. I ALSO got exposed to a lot of rumour and speculation without much foundation early on so I'm trying to remove that from my thinking.
2013-2014
Tae is instrumental in bringing Jungkook out of himself. They're CLEARLY close. Initial puppy love vibes.
2014-2015
This always feels to me that the attraction is strongest/most obvious on Jungkook's side. I don't think it's one-sided but Jungkook wears his heart in his EYES and Taehyung finds it easier to centre himself, perhaps. 2015-2017
Jungkook is what, 18-20 at this point, Taehyung 20-22? (my maths is appalling. I think that's right) and they seem to have exactly the kind of relationship that two young guys figuring themselves out have ie; DRAMATIC.
Sweet and clingy and lots of eyes and touching. Doesn't seem beyond the realms of possibility that kissing/whatever might have occurred. They're young and besotted. But it also seems to be a time of some pretty intense down moments like whatever the heck happened around Tokyo.
If you think about the Inkigayo video where JK seems a little bit stroppy with Tae for not being there sooner - well, devolve his emotional maturity by 6 or 7 years. I know people say JK doesn't like when he's not getting attention and it's supported by some clips, I feel. Like the slight drama with Bogum. I can imagine this combined with scary queer feelings combined with *SPECULATION INCOMING* being seperated on camera*, against their natural instinct to be close, would create a pressure cooker of Feels which would only ever come out in drama.
Also: Stigma is released in this time, Namjoon says Tae has his own story about it. I have wondered if Stigma might have been related to HYYH but I don't think the storyline bled into the songs, did they? Please correct me if I'm wrong there.
*side note: Dispatch threat to reveal a same sex couple then Dispatch suddenly getting BTS exclusives is an intriguing theory but I think even if it's nonsense or about a different group, I imagine it would create nervous ripples throughout various agencies? Maybe seperating Taekook was precaution? I don't know. Just a thought.
2018
It's well known JK and Tae were having some of their worst times during 2018 and disbandment talks. What intrigues me is that Jin says JK isolated himself and didn't talk to the members.
But Yoongi sends Tae and JK the supportive text message and Tae says he and JK read the messages together and cried. JK is isolated and not talking to other members but he's with Tae at this point? Interesting.
(I don't know if anyone else gets this but there seems to be a kind of implied "Well except V" in a lot of these stories. JK in his 2023 Sirius interview "I didn't really get a chance to see the members this year." and yet he's with Tae on a number of confirmed occasions and maybe other unconfirmed? Almost like Tae is aside from the collective members when it comes to JK.)
I feel like intentions might have been set here and some kind of commitment made, though I'm not sure it's a "together" commitment. Just an undetermined milestone of things getting much heavier than they were. An admission, a mutual understanding, a commitment to stop the drama... I don't know.
2019-2021
Golden Disk Awards 2020. Grammys 2020. Atomix. That's all. :)
Oh I suppose we have BTS: ITS1 filmed in 2020 and as we all know, Tae and JK have been awkward for a while and the only way Jungkook wants to be near Tae is if Jimin tricks him into going. 🙄
They just seem real sweet and close these years. No particular dramas between the two of them are cropping up for me, correct me if I'm wrong. JK has his tattooist nonsense which just feels like a silly storm in a dumb teacup. Still being seperated and forced to pretend they barely like each other in lives but that's just Bighit Streisand Effecting themselves. 😇
If not 2018 then something in here feels like it might have been the actual commitment.
2022 onwards
Demonstrable time spent together. Confirmed private time where JK hangs out with Tae's friends. Unconfirmed time too. WHATEVER WAS IN THE WATER FOR DREAM PREMIERE. Obviously Jennie weirdness in late '22, early '23 but that feels so much like a press stunt that I just J-Hope side eye it.
I once looked up if there was any telltale signs of fanservice when I was newborn army and so confused. A lot of the response was just "if it looks gay, it's fanservice." LOL but one person replied, paraphrased, "Disregard stages, photoshoots, some of the promotional lives, anything under direct agency management. Consider whether they actually interact privately where nobody is." and I feel like that kind of sums up Taekook since 2022 when BTS are on hiatus and they're still in each other's orbit.
2023
If they're not a couple, they're in love and don't know it. That's a joke. Don't come for me.
Lets see what 2024 onwards brings!
27 notes
·
View notes
Text
The number of women dying during pregnancy or soon after childbirth has reached its highest level in almost 20 years, according to new data. Experts have described the figures as “very worrying”.
How many women are dying?
Between 2020 and 2022, 293 women in the UK died during pregnancy or within 42 days of the end of their pregnancy. With 21 deaths classified as coincidental, 272 in 2,028,543 pregnancies resulted in a maternal death rate of 13.41 per 100,000.
This is a steep rise from the 8.79 deaths per 100,000 pregnancies in 2017 to 2019, the most recent three-year period with complete data. The death rate has increased to levels not seen since 2003 to 2005.
Where have the figures come from?
The data comes from MBRRACE-UK, which conducts surveillance and investigates the causes of maternal deaths, stillbirths and infant deaths as part of the national Maternal, Newborn and Infant Clinical Outcome Review Programme (MNI-CORP).
MNI-CORP aims to improve patient outcomes and is funded by NHS England, the Welsh government, the health and social care division of the Scottish government, the Northern Ireland Department of Health, and the states of Jersey, Guernsey, and the Isle of Man.
Why are so many women dying during or just after childbirth?
The main cause of death was thrombosis and thromboembolism, or blood clots in the veins.
The second most common cause was Covid-19. But even when deaths due to Covid were excluded, the maternal death rate for 2020 to 2022 – 11.54 per 100,000 pregnancies – remained higher than the rate for 2017 to 2019.
Heart disease and deaths related to poor mental health were also common, according to a review of the data by the Guardian.
Why is the mortality rate increasing?
The researchers behind the data project, led by Oxford Population Health’s national perinatal epidemiology unit at the University of Oxford, highlight several issues.
They say maternity systems in the UK are under pressure but also point to pre-pregnancy health and the need to tackle conditions such as obesity, as well as critical actions to work towards more inclusive and personalised care during pregnancy.
Is there any good news?
Not really. The maternal death rate among black women decreased slightly compared with 2019 to 2021, but they remain three times more likely to die compared with white women. Asian women are twice as likely to die during pregnancy or soon after compared with white women.
Are there other factors aside from health?
Absolutely. Women living in the most deprived areas of the UK have a maternal death rate more than twice that of women living in the least deprived areas.
Persisting ethnic and socioeconomic inequalities show the UK must think beyond maternity care to address the “underlying structures” that impact health before, during and after pregnancy, such as housing, education and access to healthy environments, said Dr Nicola Vousden, co-chair of the women’s health specialist interest group for the Faculty of Public Health.
Are deaths during pregnancy only increasing in the UK?
No. Maternal death rates are rising in many countries, yet this alarming trend has not been seriously addressed by governments and healthcare systems worldwide.
Rates have doubled in the US over the last two decades, with deaths highest among black mothers, a study in Journal of the American Medical Association found. Indigenous women had the greatest increase.
It is difficult to compare precise death rates between countries because the data is not uniform. But other countries seeing substantial rises in rates include Venezuela, Cyprus, Greece, Mauritius, Puerto Rico, Belize, and the Dominican Republic.
What can be done to reverse the trend?
Urgent action is needed to bolster the quality of maternal healthcare, ensure it is accessible to all, and repair the damage inflicted by the pandemic on women’s healthcare services more generally.
Clea Harmer, the chief executive of bereavement charity Sands, said improving maternity safety also needs to be at the top of the UK’s agenda.
The government said it was committed to ensuring all women received safe and compassionate care from maternity services, regardless of their ethnicity, location or economic status.
Anneliese Dodds, the shadow women and equalities secretary, said Labour would seek to reverse the “deeply concerning” maternal mortality figures by training thousands more midwives and health visitors and incentivising continuity of care for women during pregnancy.
NHS England said it had made “significant improvements” to maternity services but acknowledged “further action” was needed. It has introduced maternal medical networks and specialist centres to improve the identification of potentially fatal medical conditions in pregnancy.
10 notes
·
View notes
Text
Covers from the Vault # 1
I wanted to post some album covers I had made for the project for unreleased, unfinished or even un-started ones. All of these date to prior to 2020. Tbh if memory serves nothing here is newer than 2018.

Bæ / Bœ is a record cover that was made in 2013. All I got for this is the cover. I kinda wanna make the album now after re discovering the cover.

VTN is the only one that was made post 2018. This was made more recently and was fun to make A slick way of dodging the self titled album title.

ļÇȨ was just a cover. I don't think it made it to a release date or even anything beyond the cover concept. The cover was made between 2013 and 2015. It was As much as I like the cover, I don't think I'd release it now. I already made my ice release with The AVC Companion Extended Play. Plus certain people in certain positions, I feel, have taken a word for icey cold and cubes in the winter and turned it's association to negativity. I'm taking in a round about way to say the politicians have made me not want to make this record.

The Asian Lobotomy 3 planned for a 2017 release date. A 3 hour long voice only sound collage that I still have a lot of the recordings for. This later evolved into another cover and became a slotted TAL.09. The closest thing I've released to a fair comparison is the final trackbon the recent Noise Music. release which featured soke recording that were later planned to be used for this record.

Vegan was planned for multiple release dates. I can't tell you when I first thought of it or even when I first made this cover. The most recent date was 2020 but I knew the idea came before that. The record has had a track recorded for it before it was scrapped. The most recent slotted date for release I have listed is April 17th, 2021. I still wanna make this, I just don't really have a clear direction outside of this was going to be Meat the Vegetarian but then ReHeating the Vegetarian was like a re-introduction to the first record with other people playing on it. IDK. The title comes from my desire to never truly release a self titled record from the project.

Torpedo, Johnny planned for a 2015 release date. It was to be album #22 with Castonette's are attacking the Prez and Left by The Drain II preceding and following respectively. It was to be a sequel to the original album.

♭♯♮ ฿₢₣ �� ₧ ♭♯♮ was planned for 2019. The title and sound was inspired by GSYBE!. There was a single place holder track recorded but nothing more. This was to be the 39th release from the project.

Erweiterte Penis EP was planned for a 2013 release. Nothing was recorded for it. Sadly nothing was recorded for it

The Asian Lobo2my was planned for a 2015 release. Eventually pushed back to a February 13th, 2016 release date. Obviously it was never made. This would be a 3 hour track with multiple long sections much like the original. See the 1st was almost completely silence. With a few things thrown in here and there. If I were to release this, I could do the single 3 hour track but this would broken up into a sound collage. The tricky part would be keeping it interesting.

댄 & The Vegetarian was planned for a December 2015 release date. The album never had anything recorded for it. The collaboration singles were to be released yearly until I figured out the rock sound I wanted for this album.

Minimalistic Harmonics was planned for an April 11th, 2015 release date. This was to be, and will still be, a more serious venture into minimalism and modern classical music.

Finally, The First Official Live Album! was planned for a August 20th, 2016 release date. I recorded two backing tracks to play over for this. I was gonna record infront of an audience with multiple computers and had the mixing all set up in my head. Sadly it never came to be buy I'd love to do it still.

Thė Öútśįdër: Thē Çhrōñíčles Õf à Mæń Ïñ Łîmbö Øf Łóbòtømÿ Åñd Äsïâń was planned for a 2016 release date. This was to be the conclusion to the series and I've debated coming back and making it better. I feel some of the ideas were later perfected or realized on Exotic Impressions.
0 notes
Text
Permeation
Agnieszka Brzeżańska, Judith Hamann
@ MOS, Gorzów Sep 13—Oct 20, 2024 sound performance by Judith Hamann: Oct 19, 2024 at 6 pm
Permeation juxtaposes the recent paintings and sculptures of Agnieszka Brzeżańska with the sound installation and drawings by Judith Hamann. The joint exhibition of two interdisciplinary artists, who use a variety of methods and approaches in their work, subjecting the surrounding world to sensitive observation and listening, creates a space for experience and joint contemplation of the immediate future.
Agnieszka Brzeżańska uses a variety of media, focusing on the relationship between living beings and other entities inhabiting the Earth. In what appear to be abstract images, her search is for the representation of that which remains beyond the boundaries of anthropocentric reality. Biomorphic shapes represent extraterrestrial bodies, lost, non-existent or imagined entities. Brzeżanska works with a precise, formal shorthand, which can be seen in compositions built from almost a single line—delicately swirling, forming regular circles like ripples on the water, or spreading out in many directions.
Disorderly thoughts/forms, phantoms smiling mysteriously, or perhaps representations of nature, which, according to Agnieszka Brzeżańska, is in principle favourable to all beings? The artist’s ceramic sculptures from recent years seem to capture her interests and fascinations in both form and meaning. The collection of candelabra-like objects with organic shapes (Metaphor of Everything, 2017) is presented as an installation and serves as a symbolic element in the exhibition. Set on mirrors and equipped with candles that are lit during the visit, the figure- like plants enhance the polysensory dimension of the exhibition, while inviting a more intimate contact with the art.
The intangible element that fills the exhibition space is sound, present in the form of Judith Hamann’s audiospheric installation. The composition, based on field recordings, is only a small part of Hamann’s wider research-performative practice, which is rooted in experiments with the instrument and the non-human voice. Hamann refers to the many audible and perceptible properties of sound as a living medium that not only accompanies humans but is above all an intrinsic part of nature. In addition to the auditory form, the exhibition presents an excerpt from the series Paper Membranes (2020/24), for which Judith Hamann uses the technique of frottage, treated as a performative action akin to field recording. She imagines landscapes, interior and exterior spaces as ‘recordings’ made up of the surface of a wall, the trunk of a tree or the texture of a stone. These become part of a single trace, a recording of an impossible-potential landscape.
Agnieszka Brzeżańska (born in Gdańsk) studied at the Academy of Fine Arts in Gdańsk and Warsaw in Prof. Stefan Gierowski’s Painting Studio, and at the Tokyo University of Fine Arts and Music. Her work includes paintings, drawings, photography, film, ceramics and other media. Brzeżanska draws on various registers of knowledge, from physics and philosophy to systems of cognition marginalised by modern science, such as alchemy, parapsychology, esotericism, indigenous knowledge or matriarchal traditions. Since 2016, she has been organising Flow/Przepływ, an artist residency on the Vistula River, together with Ewa Cieplewska. She has presented her works in many solo exhibitions, most recently including ‘Incantations and Ancestors’, Willa Polonia Gallery in Busko-Zdrój (2023), ‘Ancestors’, BWA Warszawa (2023), ‘So Remember The Liquid Ground’, eastcontemporary in Milan (2021), ‘World National Park’, Królikarnia, The Xawery Dunikowski Museum of Sculpture — a division of the National Museum in Warsaw (2019), Gdansk City Gallery (2018). She took part in the 10th Berlin Biennale for Contemporary Art (2018). She collaborates with the BWA Warszawa gallery in Warsaw and the Nanzuka gallery in Tokyo. She lives and works in Warsaw.
Judith Hamann (born in Naarm/Melbourne, Australia) is a composer, performer and sound art maker. They are described as an “extraordinary Australian cellist” (the Guardian) who “destroys the fiction of the musician who lives and works outside conventional parameters and puts in its place a series of compositions that are fundamentally humane” (WIRE). Hamann’s work encompasses performance, improvisation, electro-acoustic composition, field recording, electronics, site specific generative work, and micro-tonal systems in a deeply considered process based, or even ‘nomadic’ approach to creative practice. Hamann explores acts of shaking and humming as formal and intimate encounters; explores ‘collapse’ as a generative, imagined surface; and considers the ‘demystification’ of bodies, both human and non-human, in the context of instrumental practice and the pedagogy of colonial heritage. They have performed at festivals such as Tectonics (Glasgow, Athens, etc.), UnSound (NYC), Sonic Acts (Amsterdam), Maerzmusik (Berlin), CTM (Berlin), Biennale Musica — The International Festival of Contemporary Music (Venice), Tokyo Experimental Festival (Tokyo), and AURAL (Mexico). Hamann enjoys thinking and working with other artists which includes Marja Ahti, Joshua Bonnetta, Pascale Criton, Charles Curtis, Sarah Hennies, Yvette Janine Jackson, and Anike Joyce Sadiq. Their music was released on labels including Blank Forms, Black Truffle, Another Timbre, and Longform Editions. They hold a Doctor of Musical Arts from UC San Diego. Judith Hamann lives and works in Berlin.
Text by Romuald Demidenko Contemporary Art Library
0 notes
Text
youtube
Why Some North Korean Defectors Want to Go Back Nearly 34,000 North Koreans have defected to South Korea since figures were first collected in 1998. While the number of new arrivals dropped to a trickle in recent years due to strict Covid controls in North Korea and China, they are almost certain to start rising again now that border constraints are easing. For many, the journey is arduous. Since the border between the two Koreas is one of the most militarized in the world, almost all defectors first flee to China until they can gather enough money to reach a third country, such as Thailand. Then they can apply for asylum in South Korea, which grants them citizenship after a security screening. Their resettlement should in theory be easier because they’re moving to a country with a common language, culture and traditions. But North Korea’s decades of isolation and lack of uncensored information has caused a wide rift with South Korea. Once North Koreans arrive, South Korea offers an initial settlement funding of 9 million won ($6,900), vocational training and subsidies for employers for hiring defectors. Many live near each other in blocks of inexpensive apartments, oftentimes the so-called 25-square-meter “rental apartments” provided by the government. When the support runs out, they must provide for themselves — often leading to grim outcomes. The unemployment rate for defectors is about twice the national average. Many older defectors retain a northern Korean accent, making them stand out each time they speak. Others bear scars such as psychological trauma or physical problems such as lung damage from digging for coal in unsafe mines with no protective equipment. Nearly 90% of defectors in Seoul said they’ve had trouble settling into their new homes after a decade, according to a 2022 study from the Seoul Institute. North Korean defectors between 2017 and 2021 experienced suicidal impulses more than double the rate of South Korea population, which is already among the highest in the world, according to a survey from the Seoul Institute. In some cases, leaving could prove fatal for family members who don’t flee. Lee, who defected to South Korea in 2017, and only gave her surname due to safety concerns, could only afford to bring one of her sons with her. When the North Korean authorities found out about her defection, they beat her oldest son to death. “I am so lonely,” Lee said. “I want to go back and die there — South Korea is as suffocating as the North.” -------- Like this video? Subscribe: http://www.youtube.com/Bloomberg?sub_confirmation=1 Become a Quicktake Member for exclusive perks: http://www.youtube.com/bloomberg/join Bloomberg Originals offers bold takes for curious minds on today’s biggest topics. Hosted by experts covering stories you haven’t seen and viewpoints you haven’t heard, you’ll discover cinematic, data-led shows that investigate the intersection of business and culture. Exploring every angle of climate change, technology, finance, sports and beyond, Bloomberg Originals is business as you’ve never seen it. Subscribe for business news, but not as you've known it: exclusive interviews, fascinating profiles, data-driven analysis, and the latest in tech innovation from around the world. Visit our partner channel Bloomberg Quicktake for global news and insight in an instant. via YouTube https://www.youtube.com/watch?v=PmmKNGMI9F8
0 notes
Text
Julien Baker
Julien Baker is an American singer-songwriter, guitarist, and producer whose music sits at the intersection of devotion and doubt, pain and grace, and whose body of work has come to define a new, unflinching emotional clarity in modern indie rock. Born in 1995 and raised in suburban Memphis, Tennessee, Baker began writing and performing in her teens, coming out of the DIY punk and hardcore scenes that shaped both her aesthetic and her ethics—minimalism, rawness, and sincerity above all.
Her 2015 debut album, Sprained Ankle, recorded on a shoestring budget while she was still in college, introduced a voice so stark and emotionally exposed it felt almost confrontational. Sparse arrangements—often just voice and reverb-heavy guitar—left space for lyrics that dealt with addiction, mental illness, faith, queerness, and self-doubtwith devastating precision. Baker’s songwriting didn’t aim to resolve suffering, but to sit inside of it, without flinching, offering no easy redemptions. What made Sprained Ankle extraordinary wasn’t its melancholy, but its clarity and restraint—pain rendered in high resolution.
With 2017’s Turn Out the Lights, Baker expanded her sonic palette, layering strings, piano, and vocal harmonies while preserving her lyrical intimacy. The themes remained spiritual and existential, often returning to the tensions between belief and despair, redemption and relapse. A self-described Christian who is also openly queer, Baker navigates these dual identities not to reconcile them, but to articulate the contradictions. Her work rejects easy binaries—between sacred and profane, strong and weak, broken and whole.
In 2021, Little Oblivions marked a significant shift: a full-band sound, self-produced, with drums, synths, and distortion pushing her music into more volatile and dynamic terrain. The album didn’t abandon vulnerability, but it complicated it, presenting a narrator not just suffering but lashing out, numbing herself, losing control. The honesty became heavier, messier, more adult. The result was a record that felt both confessional and confrontational—a confrontation not just with the world, but with the self.
Beyond her solo work, Baker is a founding member of boygenius, alongside Phoebe Bridgers and Lucy Dacus. The supergroup—initially formed as a one-off collaboration—has become a defining force in modern alternative music, not just for the synergy of its members but for the way it embodies a new model of artistic community: one rooted in mutual support, emotional transparency, and radical sincerity. Their full-length debut in 2023 further amplified Baker’s reach, blending her voice into something collective without diluting her singularity.
Julien Baker’s cultural significance lies in her ability to write the internal world with devastating lucidity. In an era saturated with performance and self-branding, her work remains startlingly unfiltered, unmarketed, and emotionally complex. She is not merely a sad songwriter; she is a documentarian of the soul at its most fractured and searching. Her presence in the indie scene has helped expand the boundaries of what queer, Christian, Southern, and female-identifying artists can sound and look like, breaking silent taboos with quiet force.
Whether performing in hushed sanctuaries or before festival crowds, Baker creates a space where contradictions can exist without resolution—a place where self-destruction and self-awareness, guilt and grace, can be held in the same hand. Her music isn’t about healing so much as bearing witness to what hurts, and in doing so, offering a kind of hope that feels earned rather than assumed.
Sprained Ankle (2015)
Turn Out the Lights (2017)
Little Oblivions (2021)
0 notes
Text
Now that I’m a couple weeks back from my huge overseas trip, I’m very much back into my Old GMMTV Challenge Project (which, admittedly, has expanded WELL beyond the original three classic BLs that @absolutebl recommended to watch way back, when many of us were talking about old BL frameworks and tropes earlier this year!). Here’s an update:
1) The end of Love Sick Season 2 is incredibly near, and while, yes, there are many problematic factors to this show -- I think the show’s SHEER LENGTH allowed it to do a LOT with the characters and script that I’m frankly surprised by. It’s delved into allyship, into sexual exploration and revelation (on all the ends of the spectrum), into all the interesting shades of acceptance and casual homophobia among a group of teenage men, and now I see at the end of the show that we’ll (hopefully) get an exploration into acceptance of queer relationships by families, which is always my jam.
I’ll save most of this for my post-watch analytical write-up, but I think for at least this show, to explore EVERYTHING the script got into -- the show needed this length. The writing wasn’t crisp and concise enough to really dig into things à la this wonderful era of GMMTV writing that we’re in NOW. But, I AM surprised by how far this script has gone without being ENTIRELY, 100% problematic. It’s a really good and fascinating watch, and I’m glad I dug into it for the history.
2) Next up will be Make It Right and Make It Right 2, which I originally thought would be my vehicle for learning more about the early high school pulps and getting familiar with pre-GMMTV Ohm Pawat. But I’ve also now been convinced by the wonderful @bengiyo to delve specifically into the works of the prolific New Siwaj, to learn about his focus on the queer male experience, and how he either successfully (or unsuccessfully) (or both, simultaneously) gets his messages across. I haven’t been watching his current works (Between Us, ABAAB), but surprisingly -- he’s a screenwriter on Double Savage, which for now seems very het. But now I wouldn’t be surprised if, à la 10 Years Ticket, we get a queer storyline in the show at some point.
3) Speaking of Double Savage (which I am seriously enjoying -- I already highly recommend it), I’m watching Perth Tanapon for the first time (I didn’t watch Never Let Me Go, and I’m not sure that I will, yet, unless finishing out Double Savage makes me get into a Perth rabbithole). But anyway, I know that Dangerous Romance with PerthChimon is on its way, so I figured -- if Perth is paired with Ohm as brothers in DS -- that I should know about early PerthSaint, as Perth and Ohm had almost the same exact trajectory into GMMTV from their very youthful years in BL.
With that, and considering the new New Siwaj focus: I’m going to add Love By Chance to the list. (But I’m NOT adding the second season.) And it’ll be my first MAME show, and likely something that I feel like I SHOULD watch before watching TharnType later this year.
4) So here’s my newly jujjed list, and I’m fixing some errors for chronology here as well from past lists. I think with what I’ve watched so far -- Bad Buddy, ATOTS, The Eclipse, KinnPorsche, and Moonlight Chicken -- that I’ve already filled holes in this chronology, but I think this list gets me straight on the history I need to know.
If anyone has suggestions on watch order or other essential/necessary/historic/significant shows to watch, I am ALWAYS OPEN to feedback!
1) Make It Right (2016) 2) Make It Right 2 (2017) 3) Love By Chance (2018) 4) Kiss Me Again: PeteKao cuts (2018) 5) He’s Coming To Me (2019) 6) Dark Blue Kiss (2019) 7) TharnType (2019) 8) Theory of Love (2019) 9) Until We Meet Again (2019-2020) 10) 2gether (2020) 11) Still 2gether (2020) 12) ITSAY (2020) 13) I Promised You the Moon (2021) 14) Not Me (2021-2022) 15) My School President (2022-2023)
I can’t wait to finish Love Sick this week and get my write-up going, aaahhh!
#turtles catches up with thai bls#turtles catches up with the essential BLs#turtles catches up with old gmmtv#the old gmmtv challenge#OGMMTVC#love sick#make it right#love by chance#new siwaj
18 notes
·
View notes
Text
I highly recommend subscribing to the Economist btw. But they will let you have access to a few free articles a month anyway, and there are a couple more on trans issues in this edition. https://www.economist.com/briefing/2023/04/05/the-evidence-to-support-medicalised-gender-transitions-in-adolescents-is-worryingly-weak
PRISHA MOSLEY was 17 when she was first given testosterone in a clinic in North Carolina, after she had declared to her parents that she was a boy. She had struggled through her teen years with anorexia and depression after a sexual assault. Luka Hein had both breasts removed as a 16-year-old in Nebraska. Chloe Cole, in California, was a year younger when she had her double mastectomy. She had been on testosterone and puberty-blocking drugs since 13, also after a sexual assault.
All three girls were experiencing “gender dysphoria”, a feeling of intense discomfort with their own sexed bodies. Once a rare diagnosis, it has exploded over the past decade. In England and Wales the number of teenagers seeking treatment at the Gender Identity Development Service (GIDS), the main clinic treating dysphoria, has risen 17-fold since 2011-12 (see chart 1). An analysis by Reuters, a news agency, based on data from Komodo, a health-technology firm, estimated that more than 42,000 American children and teenagers were diagnosed in 2021—three times the count in 2017. Other rich countries, from Australia to Sweden, have also experienced rapid increases.
As the caseload has grown, so has a method of treatment, pioneered in the Netherlands, now known as “gender-affirming care”. It involves acknowledging patients’ feelings about a mismatch between their body and their sense of self and, after a psychological assessment, offering some of them a combination of puberty-blocking drugs, opposite-sex hormones and sometimes surgery to try to ease their discomfort. Komodo’s data suggest around 5,000 teenagers were prescribed puberty-blockers or cross-sex hormones in America in 2021, double the number in 2017.
Dysphoria furoria
The treatment is controversial. In many countries, but in America most of all, it has become yet another front in the culture wars. Many on the left caricature critics of gender-affirming care as callously disregarding extreme distress and even suicides among adolescents with gender dysphoria in their determination to “erase” trans people. Zealots on the right, meanwhile, accuse doctors of being so hell-bent on promoting gender transitions that they “groom” vulnerable teenagers—a term usually applied to paedophiles. In October supporters and critics of gender-affirming care held rival, rowdy protests outside a meeting of the American Academy of Paediatrics. Several American states, such as Florida and Utah, have passed laws banning gender-affirming care in children. Joe Biden, America’s president, has described such laws as “close to sinful”.
Almost all America’s medical authorities support gender-affirming care. But those in Britain, Finland, France, Norway and Sweden, while supporting talking therapy as a first step, have misgivings about the pharmacological and surgical elements of the treatment. A Finnish review, published in 2020, concluded that gender reassignment in children is “experimental” and that treatment should seldom proceed beyond talking therapy. Swedish authorities found that the risks of physical interventions “currently outweigh the possible benefits” and should only be offered in “exceptional cases”. In Britain a review led by Hilary Cass, a paediatrician, found that gender-affirming care had developed without “some of the normal quality controls that are typically applied when new or innovative treatments are introduced”. In 2022 France’s National Academy of Medicine advised doctors to proceed with drugs and surgery only with “great medical caution” and “the greatest reserve”.
There is no question that many children and parents are desperate to get help with gender dysphoria. Some consider the physical elements of gender-affirming care to have been life-saving treatments. But the fact that some patients are harmed is not in doubt either. Ms Mosley, Ms Hein and Ms Cole are all “detransitioners”: they have changed their minds and no longer wish to be seen as male. All three bitterly regret the irreversible effects of their treatment and are angry at doctors who, they say, rushed them into it. Ms Cole considers herself to have been “butchered by institutions we all thought we could trust”.
The transitioning of teenagers has its roots in a treatment protocol developed in the Netherlands in the 1980s and 1990s. It is built on three pillars: puberty-blockers (formally known as GnRH antagonists), cross-sex hormones and surgery. The goal was to alter the patient’s body to more closely match their sense of cross-sex identity, and thereby relieve their mental anguish. A pair of papers published in 2011 and 2014 by Annelou de Vries, one of the Dutch protocol’s pioneers, reported on the experiences of some of the first patients. They concluded that symptoms of depression decreased among patients taking puberty-blockers, and that gender dysphoria “resolved” and psychological functioning “steadily improved” after cross-sex hormones and surgery.
Transition ignition
Puberty-blockers do what their name suggests. The idea is that suspending unwanted sexual development can give patients time to think about their dysphoria, and whether or not they wish to pursue more drastic interventions. The same family of drugs is used to treat “central precocious puberty”, in which puberty begins very early. Some countries also use them to chemically castrate sex offenders. As with many other medicines used in children, the use of puberty-blockers in gender medicine is “off-label”, meaning that they do not have regulatory approval for that purpose.
Patients who decide to proceed with their transition are then prescribed cross-sex hormones. Males will see the development of breasts and alterations to how fat is stored on the body. Giving testosterone to females boosts muscle growth and causes irreversible changes such as deepening the voice, altering the bone structure of the face and the growth of facial hair.
Under the original Dutch protocol, surgery was permitted only after a patient turned 18, although as the cases of Ms Cole and Ms Hein show, in some places mastectomies occur at a younger age. Male patients can have artificial breasts implanted. More elaborate procedures, in which females have a simulated penis built from a tube of skin harvested from the forearm or the thigh, or males have an artificial vagina made in a “penile inversion”, are performed extremely rarely on minors.
In 2020 the National Institute for Health and Care Excellence (NICE), a British body which reviews the scientific underpinnings of medical treatments, looked at the case for puberty-blockers and cross-sex hormones. The academic evidence it found was weak, discouraging and in some cases contradictory. The studies suggest puberty-blockers had little impact on patients. Cross-sex hormones may improve mental health, but the certainty of that finding was low, and NICE warned of the unknown risks of lasting side-effects.
For both classes of drug, NICE assessed the quality of the papers it analysed as “very low”, its poorest rating. Some studies reported results but made no effort to analyse them for statistical significance. Cross-sex hormones are a lifelong treatment, yet follow-up was short, ranging from one to six years. Most studies followed only a single set of patients, who were given the drugs, instead of comparing them with another set who were not. Without such a “control group”, researchers cannot tell whether anything that happened to the patients in the studies was down to the drugs, to other treatments the patients might be receiving (such as counselling or antidepressants), or to some other, unrelated third factor.
The upshot is that it is hard to know whether any of the supposed effects reported in the studies, whether positive or negative, are actually real. Reviews in Finland and Sweden came to similar conclusions. As the Swedish one put it, “The scientific base is not sufficient to assess…puberty-inhibiting or gender-opposite hormone treatment” in children.
Two American professional bodies, the Endocrine Society (es) and the World Professional Association for Transgender Health (wpath) have also reviewed the science underpinning adolescent transitions. But ES’s review did not set out to look at whether gender-affirming care helped resolve gender dysphoria or improve mental health by any measure. It focused instead on side-effects, for which it found only weak evidence. This omission, says Gordon Guyatt of McMaster University, makes the review “fundamentally flawed”. WPATH, for its part, did look at the psychological effects of blockers and hormones. It found scant, low-quality evidence. Despite these findings, both groups continue to recommend physical treatments for gender dysphoria, and insist that their reviews and the resulting guidelines are sound.
One justification for puberty-blockers is that they “buy time” for children to decide whether to proceed with cross-sex hormones or not. But the data available so far from clinics suggest that almost all decide to go ahead. A Dutch paper published in October concluded that 98% of adolescents prescribed blockers decide to proceed to cross-sex hormones. Similarly high numbers have been reported elsewhere.
The reassuring interpretation is that blockers are being prescribed very precisely, given only to those whose dysphoria is deep-rooted and unlikely to ease. The troubling one is that puberty-blockers lock at least some children in to further treatment. “Time to Think”, a new book about gids by a British journalist, Hannah Barnes, cites British medical workers concerned by the latter possibility. They say patients received blockers after cursory and shallow examinations.
The Dutch researchers weigh both explanations. “It is likely that most people starting [puberty-blockers] experience sustained gender dysphoria,” they write. But, “One cannot exclude the possibility that starting [puberty-blockers] in itself makes adolescents more likely to continue medical transition.”
Perhaps the biggest question is how many of those given drugs and surgery eventually change their minds and “detransition”, having reconciled themselves with their biological sex. Those who do often face fresh anguish as they come to terms with permanent and visible alterations to their bodies.
Once again, good data are scarce. One problem is that those who abandon a transition are likely to stop talking to their doctors, and so disappear from the figures. The estimates that do exist vary by an order of magnitude or more. Some studies have reported detransition rates as low as 1%. But three papers published in 2021 and 2022, which looked at patients in Britain and in America’s armed forces, found that between 7% and 30% of them stopped treatment within a few years.
The original Dutch studies published in 2011 and 2014 were longitudinal—that is, they followed the same group of patients throughout their treatment. Yet three recent critiques published in the Journal of Sex & Marital Therapy nonetheless find fault with the studies’ data.
One of the new studies’ concerns is the small size of the original samples. The 2011 paper looked at 70 patients. But the outcome of treatment was only known for between 32 and 55 of them (the exact number depends on the specific measure). And even then, the final assessment of outcomes occurred around 18 months after surgery—a very short timeframe for a treatment whose effects will last a lifetime. (The first patient, “FG”, was followed for longer. In 2011, when in his mid-30s, researchers reported his feelings of “shame about his genital appearance” and of “inadequacy in sexual matters”. A decade later though, things had improved, and FG had a steady girlfriend.)
The critiques also suggest that the finding that gender dysphoria improved with treatment may have been an artefact of how the participants were assessed. Before treatment, female patients were asked to agree or disagree with such statements as, “Every time someone treats me like a girl I feel hurt.” This established their desire to be seen as male. After blockers, hormones and surgery the same individuals were asked questions on a scale originally developed for those born male. It offered statements such as, “Every time someone treats me like a boy I feel hurt.” Naturally, patients who preferred to be seen as male disagreed. In effect, the yardstick was changed in a way that might be seen as making positive outcomes more likely.
Finally, the original studies seem to have inadvertently cherry-picked patients for whom the treatment was most effective. The researchers started with 111 adolescents, but excluded those whose treatment with puberty-blockers did not progress well. Of the remaining 70, others were omitted from the final findings because they did not return questionnaires, or explicitly refused to do so, or dropped out of care or, in one case, died of complications from genital surgery. The data may therefore exclude precisely those patients who were harmed by or dissatisfied with their treatment.
In a rebuttal published in the same journal, Dr de Vries insists that the original papers found a significant improvement in gender dysphoria, the condition the protocol was designed to treat. She concedes that the switching of assessment scales is “not ideal” but says this does not imply the studies’ results were “’falsely’ measured”. In response to worries about the relatively short follow-up, she noted that a study reporting longer-term outcomes is due “in the upcoming years”.
Newer longitudinal studies have been published since, but they have drawbacks, too. One published in January in the New England Journal of Medicine by Diane Chen of Northwestern University and colleagues looked at teenagers after two years of cross-sex hormone treatment. Although participants did typically report improvements in their mental health, they were small—generally single-digit increases on a scale that runs from 0 to 100. The study lacked a control group. Two of the 315 patients committed suicide.
What is more, whatever the merits of the Dutch team’s original research, the patients passing through modern clinics are strikingly different from those assessed in their papers. Twenty years ago the majority of patients were pre-pubescent boys; in recent years teenage girls have come to dominate (see chart 2). The findings of older research may not apply to today’s patients.
The Dutch team’s approach was deliberately conservative. Patients had to have suffered from gender dysphoria since before puberty. Many of today’s patients say they began to suffer from dysphoria as teenagers. The Dutch protocol excludes those with mental-health problems from receiving treatment. But 70% or more of the young people seeking treatment suffer from mental-health problems, according to three recent papers looking at patients in America, Australia and Finland.
Despite the protocol’s caution, says Will Malone of the Society for Evidence-Based Gender Medicine, an international group of concerned clinicians, the reality is often the reverse, especially in America, with mental-health issues becoming a reason to proceed with transitions, rather than to stop them. “We are now told that if we don’t address young people’s mental-health problems caused by dysphoria with transition, they will kill themselves.”
Gender agenda
The original Dutch protocol emphasises the need for careful screening and assessments, as do official guidelines in most countries. But whatever the guidance, there are persistent allegations that it is not being followed in practice. “I had one 15-minute appointment before I was given testosterone,” says Ms Mosley. Many American patients contacted by The Economist reported similarly brief examinations.
The possibility that many teenagers presenting as trans could instead be gay has long been discussed. The Dutch study of 2011 found that 97% of the participants were attracted either to their own sex or to both sexes. In 2019 a group of doctors who resigned from GIDS told the Times, a British newspaper, of their worries about homophobia in some patients and parents. They worried that, by turning children into simulacra of the opposite sex, the clinic was, in effect, providing a new type of “conversion therapy” for gay children.
Both within America and without, whatever the loudmouths may claim, the vast majority of practitioners are simply trying to ease the genuine suffering of adolescents afflicted by gender dysphoria. But in America in particular the charged atmosphere has made it very difficult to separate the science from the politics.
European medical systems have not concluded that it is always wrong for an adolescent to transition. They are not trying to erase distressed patients. They have simply determined that more research and data are needed before physical treatments for gender dysphoria can become routine. Further research could, conceivably, lead to guidelines similar to those already in use by American medical bodies. But that is another way of saying that it is impossible to justify the current recommendations about gender-affirming care based on the existing data.
Anyone have a full version of this they can send me?
404 notes
·
View notes
Text





"After John James Audubon (American Woodsman)" 2021.
Vintage posters, Franklinia alatamaha seeds, cotton, antique frame, plywood, plexi, glue, hardware, vintage lumber, iron oxide stain, light-reactive sound device, 1950s sound recordings of Vermivora bachmanii, vintage darning egg, vintage needle and spools, Sturnus vulgaris skull, wool socks knitted by Bobby Wilcox, original wallpaper digitally designed using copyright free historic images, printed by SpoonFlower Inc, self-published zine.
I was invited by Goucher College Curator and Director of Exhibitions Alex Ebstein to create this installation for the "Rediscovering Goucher's Lost Museum" exhibition in fall 2021. Documentation photos generously made by Vivian Marie Doering @vivianmariephoto on Instagram.
Artist Statement:
“On the whole, the task of turning Audubon���s original images into marketable engravings proved to be an extremely labor-intensive process that relied, almost immediately, on the work of dozens of artisans, often working directly under Audubon’s ever-critical eye. But the work process went well beyond the engraver’s shop. Unseen and unheralded others likewise made a critical contribution to the project: the papermakers who produced the huge, high-quality sheets Audubon required; the copper smelters who turned raw ore into clean ingots; the miners who extracted the ore from the earth in the first place; and so forth, back through all the prior steps of production. In that sense, The Birds of America was not just an extensive work of art, not just an example of the sole genius of the lone, struggling artist. It was, rather, an ambitious business venture that relied on a complex labor process and an extensive supply chain, an enterprise in which the artist became not just the designer of the work, but the administrative manager of dozens of people, many of whom could be called artists in their own right, and a marketer to prospective customers, many of whom he had to track down wherever he could find them, on both sides of a very wide ocean.”
--Gregory Nobles, John James Audubon: The Nature of the American Woodsman, 2017. p103
Beyond the ‘supply chain’ of compensated workers existed a backdrop of the truly Unseen and Unheralded – the enslaved Black people whose supportive labor was violently coerced; and the work of Maria Martin, an ‘artist in [her] own right’ whose labor was given, and taken, freely due to her faith and her standing as an unmarried, white woman in the Antebellum South. Utilizing the exquisite Martin-Audubon collaborative painting, "Bachman's Warbler", as a jumping-off point, this installation is a visual exploration of the cultural and structural scaffolding that made such erasure possible during that era, as well as two examples of natural history showcased by the painting that have been lost and found - the now extinct Bachman's Warbler (Vermivora bachmanii) for which this painting and a few short sound recordings are our best documentation of the species' existence, and Franklin Tree (Franklinia alatamaha) a species native to the southeastern US that narrowly avoided utter extinction thanks to the collectors John and William Bartram, and that now exists in scattered cultivation across the country.
This project is not meant as a wholesale ‘cancel’ of John James Audubon or early American naturalists – whose work, at times disturbingly tainted by prevailing beliefs and customs, nevertheless paved the way for the scientific fields of biology and ecology today. This installation is, rather, an acknowledgment of the conflicted entanglements between history, nature, people, race, gender, ideology, belief, imagery, and power.
Collections are essentially a grandiose form of appropriation, recontextualizing objects for myriad purposes. This installation plays with two traditions: collections and appropriation, by appropriating and recontextualizing Audubon’s work, as well as other historical illustrations from various collections, and using metaphor and allegory as tools to tell the story. It would not have been made possible without the help, labor, and/or support of many unseen and unheralded, including the anonymous archivists at the Internet Archive, New York Public Library Digital Collections, and Cornell’s Macaulay Library, collectors on Ebay, Etsy, Facebook Marketplace, and Bazaar in Hamden, the production team at Spoonflower, and most especially Alex Ebstein, Bobby Wilcox, Seth Adelsberger, Denise Wilcox, Patti Murphy, Wyatt Hersey, Jenny Rieke and Oona McKay.
4 notes
·
View notes
Text
Share the Care: Breaking the Gender Bias
Care work, whether paid or unpaid, is essential for all societies to function properly and is mostly seen as a woman’s responsibility. However, despite the impact of care work on our lives, it continues to be undervalued. This article hopes to shed light on the importance of sharing the care at home and beyond.
Unpaid Domestic and Care Work

Photo by J. Aliling for the ILO
“Care work is central to human and social wellbeing. It includes looking after children, the elderly, and those with physical and mental illnesses and disabilities, as well as daily domestic work like cooking, cleaning, washing, mending, and fetching water and firewood.” – Oxfam International
Sharing responsibilities in the home can bring us one step closer to stopping all forms of gender inequality. Various societal norms have reinforced the gender division of labor wherein women and girls are expected to do most of the domestic and care work at home, while men assume the role of being the primary breadwinners of the family. These gender norms have limited the opportunities that give women and girls a better quality of life as they spend more time taking care of responsibilities at home. This situation is even worse for women and girls who live in marginalized areas, where resources are much more limited.
According to the International Labour Organization, “...women perform 76.2 per cent of total hours of unpaid care work, more than three times as much as men” (2018). These statistics have increased drastically due to the COVID-19 pandemic, due to the government mandates and work-at-home setups. However, despite women and men spending more time at home, the former still do most of the domestic and care work. According to the 2021 National Household Care Survey, women have spent 13 hours a day on domestic and care work, while men have only spent 8 hours daily.
Valuing Domestic and Care Work
youtube
“To really value this work, it's important to appreciate its significance for any society or economy.” – UN Women expert, Shahra Razavi (2017)
In the video above, UN Women expert Shahra Razavi says that the value of unpaid care work done in Switzerland would rival the country's banking and insurance industries. Similarly, UN Women reported in 2016 that unpaid domestic and care work almost amounts to 10 to 39% of a country’s Gross Domestic Product (GDP). Despite these numbers pointing to a high economic value of unpaid domestic and care work, this invisible labor continues to be ignored. Notably, the value of care work should not be limited to its possible economic value.
Care work by women has been the backbone of many well-functioning societies and economies. However, care work continues to be undervalued and seen as solely a woman's job. In ending the gender norms that perpetuate such harmful stereotypes, we can begin at home by equally dividing household chores between our sons and daughters. Aside from teaching our sons the importance of care work, men also need to “...challenge traditional thinking and recognize their equal share of care and domestic work responsibilities at home” (Cabaces, 2021).
Sharing the Care Beyond the Home
“Care should not be considered only as a burden and this central activity for well-being should be redistributed between men and women, as well as between the family and the State: States’ failures to provide, regulate and fund domestic and care formal services increase the burden for communities, families and especially women.” – Gaëlle Ferrant, Luca Maria Pesando, and Keiko Nowacka (2014)
Beyond sharing the care at home, legislation and policies are also a must to further support the care economy. These institutional changes can range from maternity and paternity leaves and flexible working arrangements to better childcare and family services. These examples can help ensure a work-life balance for both parents.

Photo by Direct Media on Stock Snap
From teaching our sons to help at home to enacting laws to lessen the burden of care work on women and girls, we can turn a house into a home when we share the care.
References
Cabaces, R. (2021, July 1). When fathers care. ABS-CBN News. https://news.abs-cbn.com/blogs/opinions/07/01/21/domestic-work-oxfam-equality-home
Canadian Labour Congress. (2022, March 7). IWD 2022: Gender equality depends on a healthy care economy. https://canadianlabour.ca/iwd-2022-gender-equality-depends-on-a-healthy-care-economy/
Donner, F. (2020, February 12). The Household Work Men and Women Do, and Why. The New York Times. https://www.nytimes.com/2020/02/12/us/the-household-work-men-and-women-do-and-why.html
Ferrant, G., Pesando, L., & Nowacka, K. (2014, December). Unpaid Care Work: The missing link in the analysis of gender gaps in labour outcomes. OECD. https://www.oecd.org/dev/development-gender/Unpaid_care_work.pdf
International Labour Office, Addati, L., Cattaneo, U., Esquivel, V., & Valarino, I. (2018). Care work and care jobs for the future of decent work.
Miller, C. (2018, August 8). A ‘Generationally Perpetuated’ Pattern: Daughters Do More Chores. The New York Times. https://www.nytimes.com/2018/08/08/upshot/chores-girls-research-social-science.html
Oxfam International. (n.d.). Not all gaps are created equal: the true value of care work. https://www.oxfam.org/en/not-all-gaps-are-created-equal-true-value-care-work
Rodriguez, L. (2021, September 13). Unpaid Care Work: Everything You Need to Know. Global Citizen. https://www.globalcitizen.org/en/content/womens-unpaid-care-work-everything-to-know/
UN Women. (2017, March 3). What is the real value of unpaid work? [Video]. Youtube. https://youtu.be/fcqt0QzgUFU
UN Women. (2019, May 15). Gender equality starts at home: Seven tips for raising feminist kids. Medium. https://medium.com/we-the-peoples/gender-equality-starts-at-home-seven-tips-for-raising-feminist-kids-75e1bf00b863
UN Women. (n.d.). Redistribute unpaid work. https://www.unwomen.org/en/news/in-focus/csw61/redistribute-unpaid-work
3 notes
·
View notes
Text
Every Game I Played in 2021, Ranked
It’s time to say goodbye to 2021 in the only way I know how: ranking the games I played this year. Let’s hop to it.
2015 | 2016 | 2017 | 2018 | 2019 | 2020

14. Deedlit in Wonder Labyrinth – 2021 – Steam – ★★★
Deedlit in Wonder Labyrinth set in the Lodoss War franchise. The “story” as it stands is kind of just an excuse to recycle various dead Lodoss characters into a series of boss fights in what ends up being a pretty linear Metroidvania. The story is really not what you should be here for— if you’re not familiar with Lodoss it’s pretty much nonsense, and as someone who is: still not great.
What works really well here are the controls and element system. You have the ability to swap between two active elements: fire and wind. Whichever is active, you deal that kind of elemental damage, and are absorb that element to refill your mana. You also have various other abilities as a result: wind in particular allows Deedlit to float, which is very useful, and being able to stand in lava is, while not as helpful, definitely a thing.
Of course, enemies have their own weaknesses and resistances (even beyond these, which activated magic can play into), so you’re forced to be constantly swapping between elements (including back and forth during boss fights) to move through the world and attack. Which, all-in-all, feels pretty good. There’s also an interesting puzzle system built around bow-and-arrow hitting targets and cutting ropes.
Sprite work is good, animation is fantastic, music is a bit… basic. Environments look nice but are also devoid of any variety whatsoever.
Beyond the basic-ness of it, the main reason I have this relatively low rated here is that the combat is just suuuuper just “there”. There’s nothing really to it, and it’s pretty trivial. Bosses vary from being very easy to annoying, in part because they’re VERY BAD at telegraphing the moves you’re supposed to be dodging. And you really need to dodge: a core system of the game is building up damage with particular elements so you can refill life since you can’t take many hits, the game has a very harsh fighting-game style stun system, and the knockback is almost comically mean. It’s the kind of stuff that I’d expect they’d have polished with more time and playtesting but… so it goes.
It’s very short, and the variety isn’t huge, but it’s fun enough for a few hours. Honestly, it kind of feels almost like a first pass— I’d be interested in seeing the team behind this working on something with more budget (and with more people) to make a true Metroidvania out of it. Put these people with the Bloodstained team and you’d get a really interesting game out of it.

Ori and the Blind Forest – 2019 – Steam – ★★★★
Ori is a very pretty Metroidvania game with some glaring flaws that bring down the experience. The combat is brainless, you just press an auto-attack button that does all the work for you. There’s an obsession with long, very orchestrated chase sequences that are meant to be “cinematic” but are ultimately just frustrating when you don’t know what they are expecting you to do at a given moment.
But when the mobility abilities are firing, the interconnected flow of combat-and-movement is fantastic. And the game really is very pretty. The writing is decent, though its attempts at emotional moments feel a little forced and obvious. Still, it’s good. It doesn’t compare to its sequel, but…

Metroid Prime 3: Corruption – 2007 – Wii – ★★★★
So, I’ve been slowly— very slowly, given I played through Metroid Prime 2 all the way back in 2015 — getting through the rest of the Prime series. I’ve played Prime 1 a bunch, but for whatever reason I just never got to the others. Well, here we are.
This is by far the weakest of the Metroid Prime series. They tried to make it more of a linear action game, which just… doesn’t work. There’s still exploration, but the kind of spatial reasoning and memorization of areas for backtracking just isn’t here. You barely even have reasons to go back to past areas, and when you do the giant space brain outright tells you what planets to go to instead. Weak.
The addition of the hypermode mechanic just… isn’t good. Like, the base idea of “spend life to increase damage” is perfectly fine, neat mechanical idea. Corruption letting you get more out of your hypermode for the health you spend is cute but poorly explained as well. The issue is that so many enemies require the use of hypermode against them that it kind of invalidates the other combat options?
I like the Prime series’ mobility. I like to charge a beam while dodging around fire to hit something. Shooting missiles that lock. Both of those are immeasurably worse options in this game, if they’re options at all.
Many bosses NEED you to be in hypermode to damage them, which can be tricky if you’re low on health (and thus require you to farm health off them v e r y s l o w l y). Actually, in general: the boss designs in this game are very weird in their difficulty. Things get much better in the latter half, but some fights are just absolutely miserable. Rundas and the first Leviathan Guardian in particular are just so tedious. Ridley, Ganaydra, and the final encounter were all genuinely fun, but man, some of the others.
Some quick thoughts:
The scans not containing much lore on monsters etc. sucks. I miss my science team scans.
Changing up the enemies for particular rooms at certain points in the story is cute, but replacing everything with Phazoids, the most annoying enemy, after you beat an area is miserable. What the fuck?
Playing this game now is hilarious, because there’s a lot of mechanical stuff built in tied to the Friend Voucher system. Backtracking to do a weird environmental puzzle where the only reward was a Friend Voucher… kind of broke me a bit.
The X-Ray visor + Nova Beam combat stuff is hilarious. Props to them on that. Sniping a Metroid Hatcher after the frustration of fighting it previously is very satisfying.
Speaking of funny: the admiral flying down like Patton to say GOOD JOB SAMUS, HERE’S SOME GUYS TO NOT GET KILLED and then fly back to his ship slayed me.
I think I hate motion controls now
Anyway, Prime 1 >>> Prime 2 >>>>> Prime 3

13. Super Mario 3D World + Bowser’s Fury – 2021 – Switch – ★★★★
Mario Odyssey was billed as kind of an “open world Mario 64”, but that really wasn’t the case. The game was inventive, and the way it built its levels was certainly different, but the sheer volume of collectables in Odyssey kind of weakened it overall; it was very much a quantity over quality.
Bowser’s Fury is really, really an “open world Mario 64”, in that you’re basically moving between Mario 64 levels in an open world, each with a set of self-contained goals. This is complicated by the presence of a kaiju Bowser occasionally wrecking shit, sometimes helping out on accident but often getting in the way.
The Bowser’s Fury aspect of Bowser’s Fury is, in my opinion, its weakest aspect. Yeah, there probably needed to be some environmental interactions to make the game work, but interrupting precision platforming with unavoidable horseshit is super not cool, and the number of shines that require his presence and the overall brevity of the game basically forced them to make him spawn really, really often towards the end, which is obnoxious.
But even so, I had a real blast with it. Bowser’s Fury is short, but it’s a good proof-of-concept of a direction they could go with Mario moving forward. I’d much prefer them built out a free-flowing open world Mario along these lines than sticking to the Odyssey model, but we’ll see.
Also, 3D World: that’s still a very good Mario game. Kind of wasn’t feeling it coming back to it, but then I ended up running through the whole thing again anyway. Good stuff.

Yakuza: Like a Dragon – 2020 – Steam – ★★★★
I’ve largely enjoyed the Yakuza franchise from afar. But the move to a dedicated goofy RPG system seemed weird enough that I had to check it out first hand.
The RPG system is a good first try. It functions, but it does not really shine. There’s just not a lot of systematic depth to the progression. See, it uses a job system with unlockable abilities, ala Final Fantasy 5, that progresses independent of your level. Different jobs have different skills and specializations, as well as different weapon specializations.
Problem is, there’s actually not much depth to job switching. Very few abilities are actually usable by other jobs once unlocked, and most abilities are very flat in both their usage and damage. While there are a few damage types, there’s typically only one unlockable attack type of a given elemental type available to a character, so you basically just grind to get those abilities so you have a full elemental coverage, before swapping them back to whatever class is the highest DPS for them / has the highest ability variation.
There’s just not much decision making in “do I attack with Big Punch A or Big Punch B”, really; you just mash whatever attack does the most damage and isn’t resisted by the target. The fact that stat modifiers for opponents are typically kind of useless given weaker enemies die too quickly for them to matter, and bosses almost always resist them anyways.
The way summons work is pretty interesting, in that they actually use money and are available based on environmental conditions, and time last used. Them also being connected to side story progression is very good; it allows them to really build dumb emotional connections as to why Kasuga is summoning a swarm of crawfish to fight someone etc.
Story wise… it’s a Yakuza game. It’s a well-executed one of those, but ultimately, it’s just one of those. If you like the crime melodrama of Yakuza, you’ll have it here. Kasuga as a protagonist is a good replacement to Kiryu in that he’s much more… emotive and involved, but it is very funny to me that the series is obsessed with putting washed up 40+ year olds in the protagonist seat, to the point where even their new junior protagonist has to be one too.
12. Subnautica: Below Zero – 2021 – Steam – ★★★★
The last time I played Subnautica was when the original back in 2018. I rather enjoyed it at the time, and I’ve grown fonder of it since. The core formula of Subnautica— a sort of underwater survival Metroidvania, where the progress “locks” are both a tech tree and spatial knowledge— just rang quite true for me, and the way it approached an open, unfolding narrative was great.
Subnautica: Below Zero is an expandalone sequel for the original Subnautica, and it’s… well, it’s not quite as good. But: it’s still Subnautica. I do not like it nearly as much as I did the original, but I still enjoyed my time with it. I do not think there is any reason to check it out if you haven’t already played and enjoyed the base game though.
Let’s touch on some positives first before I start getting into all my nits: It runs and looks considerably better. Them making the narrative much more personal— with you as an actual named, voice-acted character looking to see what happened to her sister— is a good turn. It’s an interesting expansion to the story of base Subnautica, though I’m not entirely sure if the story it’s telling is particularly revelatory in the same way. And, again: the core gameplay loop is still the same as Subnautica, which is a fun loop overall.
Alright, let’s pick those nits:
Below Zero takes a big focus on on-land (well, on ice a lot of the time) movement and exploration, and it just doesn’t work very well. The physics system can’t quite handle animal movement on land very well, particularly when it’s aggressive, and the movement is just slowww. Heat as the oxygen of the land— while being a funny statement— just isn’t that interesting. The loss of vertical movement there is really limiting, too.
My main issue with Below Zero is its layout and progression. The game is much smaller by landmass, and as a result it has compensated by reducing vehicle movement speed, made biomes much more labyrinthine and compressed, and just made the overall flow of the exploration not as good. OG Subnautica had a kind of natural sequence to the map and the technologies you followed— born both on how it slowly gave you waypoints, the way sight-line landmarks were used to lead you in particular directions, and the way it slowly gave you access to particular mobility / depth enhancement technologies and their required resources.
Below Zero being squished makes all this instead kind of weird: you’re less gated, but there’s so many areas that don’t actually matter, and you end up getting some technology / access to certain resources in what seems like a very odd order sometimes. Subnautica just felt more deliberate in how you tended to stumble your way through the game; not so here.
This lack of structural guidance also kind of bears out in the story, weirdly. There’s two major narrative threads, one of which kind of just ends fairly abruptly (and, on my part, kind of accidentally), and then the “main” plot also sort of wraps up melodramatically, in that it… wasn’t that hard to do? Compared to the main ending challenges of base Subnautica— including the extremely fraught but fun journey to the bottom of the map that really felt like an expedition— the jaunt to what ended up being the end of Below Zero was… pretty basic and easy?
Some of this admittedly could be born of not remembering annoyances with the base game which would elevate Beyond Zero by their correction, but… overall, I think this is fun enough, but not as fun.

11. Shin Megami Tensei 3: Nocturne HD Remaster – 2021 – Steam – ★★★★
This was actually my first time playing through Nocturne, and boy: that sure is a 20-year-old game huh! Like, the core SMT systems are still good and enjoyable, and the tone is still great, but there’s just aspects of the experience that haven’t aged well. A lot of expectation for you to either just know stuff or have a guide, and not a lot of respect for your time.
That being said: The turn press combat introduced here is still great, and adds a lot of fun to the sort of push-and-pull of critical hits and weakness exploitation. It’s fun!
This Remaster adds voice acting— which I found pretty good— cleans up the graphics, removing randomization from skill inheritance (oh thank god), and pulls in all of the variants of the Maniax dungeon stuff. Annoyingly, I had multiple softlocks in the Labyrinth of Amala around the Maniax cutscenes, which ate hours of my time. Which: cool, great, thanks.
Still need to check out SMTV despite owning it. Just need to build up the headspace energy for it.

10. Castlevania: Advance Collection – 2021 – Steam – ★★★★
This collection is complicated. I am on the record as loving the portable Castlevanias— and I do— and I all onboard for them getting a new release so that I can play them on, say, the Switch or something. Of course, they’re all super emulatable, and have been for two decades now, but that’s kind of the nature of game rereleases I suppose. This package includes all three of the GBA Castlevanias, as well as the SNES release of Dracula X. It adds some minor additional art stuff, some audio with better compression (well, in a few cases), and also some actually pretty useful on-screen pop ups tied to bestiary item / soul collections.
As far as deals go, it’s a decent one, but again, kind of pointless. I’ve played all the games in this collection before, so let’s just briefly run them down:
1. Circle of the Moon
This game has aged terribly. It feels stiff, empty, and super basic. The whole card combination system for special moves is really neat actually, but the drop rates for cards is terrible, to the point that you can go a lot of the game not getting new ones. It’s a tolerable experience, but not an enjoyable one.
2. Harmony of Dissonance
This game is pretty good still! Like, the Castle design is kind of complex to the point of being genuinely confusing at times— I have gotten genuinely lost in this game before multiple times, kind of an uncommon experience really— but that’s part of the fun. This game truly captured the idea of “let’s do Symphony of the Night but on the GBA”, and did so pretty well. It’s not the best portable Castlevania by any means, but it’s pretty good.
3. Aria of Sorrow
Now we’re talking. Aria of Sorrow is very good. It’s easily the best GBA Castlevania, and in the running for one of the best Castlevanias period. I don’t know what to say about it at this point. The collection aspect is good, the abilities are fun, the game moves and just feels good in a way Circle and Harmony both kind of struggled with. It’s just a fun game to play. As a Metroidvania it’s not especially open or hard in the sense of getting lost in it (beyond chasing the abilities necessary for the “true ending”) but there’s certainly more narrow ones out there.
4. Dracula X
… Why are you here? You’re not a portable game. You’re not even the best version of the game that represent. Legitimately, why are you in this collection? Y’all couldn’t be bothered to just give us a good ass Rondo of Blood port instead? Whatever.

9. Mass Effect: Legendary Edition – 2021 – Steam – ★★★★
Hoo boy. So, Legendary Edition is a packaged rerelease / slight remastering of the Mass Effect trilogy. Way back when, I rather enjoyed the first two games, and avoided the third in-light of the drama around its original release. This rerelease was my excuse to revisit it all at once, and finally give that third game a try.
Mass Effect 1 definitely feels like an older game. There are aspects of its design that you can tell stem from it being a relatively smaller game made by a relatively smaller team— there’s a lot of asset reuse (particularly on side missions), and they hadn’t quite locked down what exactly people liked about the franchise (namely, the side characters and party members). But the world building and narrative design really did shine here. The way it presents a complete blank slate science fiction setting that’s both expansive and detailed is great. It’s a great start for the series and setting.
Mass Effect 2 is the jump into “triple A” polish and design. Combat feels better, there’s a lot more bespoke assets, and the team and your interaction with them is put at the forefront. It’s definitely the best game in the series, the most interesting and complex. Going back now, there’s still some aspects I found a bit annoying. The way it handles certain narrative points of return— basically punishing you for advancing the story in certain places not knowing that things can turn out badly for characters as a result— is stupid. Certain plot hooks are dropped outright in ME3.
My feelings about Mass Effect 3 are complicated. Obviously, I’m coming to this with all the various DLC and fixes layered on, though I was well aware of the various flaws and foibles of the game going in (spoilers aren’t the end of the world for me— I care a lot more about plot execution than plot surprises). Mass Effect 3 almost feels like it was made by two different writing staffs. The character writing is still good. The way they gave the party a real send-off with the Citadel DLC was great, and the way the general game pushed more party-member-to-party-member interaction was good. But boy, the central plot just doesn’t work well, and the resolution is tepid– even after them going back to clean it up. You can tell they put it together under a schedule gun.
I get what they’re going for with the big focus on the war in ME3, and a lot of that works well enough. The whole gathering of disparate assets and factions is neat, and the general plot being about gathering allies on the national scale etc is fine. But the actual missions, and what you’re up against is very flat, straight forward, without nuance. For a series that often had very complex narratives with interesting choices— if not necessarily that consequential when tied to those choices— everything here is hyper-focused to basically how much do you oppose genocide really. A lot of the “gray areas” from previous games are hyperfocused into black-and-white, and indoctrination becomes a catchall solution to the plot’s woes.
I wonder what the hell they’re going to do with the ostensible Mass Effect sequel we have coming. Dragon Age: Inquisition showed that BioWare can in fact make a game like this still, even if Andromeda was a big ol’ flop, but I’m not sure how one does a direct sequel now. I guess you could pull a Deus Ex and do the “combine all three endings” thing, which… would be fine, I guess.

8. Halo: Infinite – 2021 – Steam – ★★★★
It has been ages since I last played a Halo. I only play first-person shooters on PC generally, and I do so only very sporadic at that (see: the past few years rankings). But, with Halo: Infinite being F2P, I figured hey, why not dip my way back in? I had a fun time with Halo 1 on PC back in the day.
And turns out, Halo: Infinite is a good time. There’s a lot of good mechanical evolutions, fun match styles, and good weapons. The flow of kills feels pretty good. Folks complain a bunch about the “progression”, and I acknowledge that their complaints are justified, but as someone who is here to just have a good time and not necessarily chase the number dragon… ehhhh it’s fine. It doesn’t impact me really.
I ended up shelling out for the campaign, and it is pretty neat. The gameplay loop is fun, particularly with the mobility added by the grapplehook. But boy that narrative is weird as shit. I’d love to hear what the hell happened production wise that led them here, because it is genuinely bizarre structurally. How late did they pivot to… this?

7. Stellaris: Nemesis – 2021 – Steam – ★★★★
It’s been a hot minute since I touched Stellaris; last time I reviewed some expansions on here, I dwelled a lot on the issues Stellaris has; a lot of those still are here. AI is dumb as shit and doesn’t play by the same rules, there’s occasionally back-breaking bugs, and the level of micro becomes absurd at times, especially in certain “builds”. War is such a goddamn hassle.
On the plus side: there’s actually been a ton of improvements since I last dipped in. The AI is genuinely better; it’s not exactly good, but it is much less pants-on-head frustrating. The additions to Stellaris via Nemesis are also neat; the whole becoming-the-Crisis gives another option for end-game for people getting bored with the game state, as-is forming the galactic imperium. The changes made to first contact and the addition of intel is good, if a bit micro heavy and inconsequential a lot of the time.
They’ve also generally just added a ton of new small events across the game. Their addition of a team whose entire job is to polish up old expansions and add small content like this is a godsend for improving the experience. I hope they continue to add more weird Origins; the divergence of experience tied to them is really good.

6. Animal Crossing: Happy Home Paradise – 2021 – Switch – ★★★★
This is quite an improvement on base Animal Crossing! It doesn’t exactly reduce the long-term tedium or anything, but it certainly gives more incentive to consistently come back. I guess this is technically a review of both the 2.0 update and that DLC.
The addition of Gyroids, out-of-season islands, the ability to visit Harv’s Island to deal with roaming stores consistently (particularly Redd, who will rotate art in as you buy), various item additions, and of course Brewster is all pretty great. Lot of fun details (as one would expect). The game as a whole feels a lot more rounded with it.
Happy Home Paradise is just a fun little excuse to make cute houses. If you aren’t “playing along” you could easily metagame it to try to speed run your way through, which… that doesn’t seem especially fun. But if you’re just having a good time customizing and taking your time, it’s a real hoot.
It is kind of weird to me that they’ve gone out of their way to say that this is the last major (free?) update to the game, given how huge AC is. AC seems ripe for them providing ongoing, almost Sims-esc support. People are very hot on AC, it’d be a waste to not, y’know, capitalize on it. Ah well.

Ori and the Will of the Wisps – 2020 – Steam – ★★★★★
OK, now we’re talking. Ori and the Will of the Wisps pretty much addresses every single issue I had with Ori and the Blind Forest.
The combat is much improved, since now it’s an actual honest-to-god combat system with manual attacking. It’s very satisfying; as someone who disliked how flat Hollow Knight’s combat system was, this is a good example of a very similar game with a similar combat still that built the system out for strong in-combat feedback.
They also doubled down on the combat-mobility mechanics, encouraging more active use of the various movement abilities that can be interlinked with combat. Them having many of the unlockable ability-modifiers be based on a limited slot system further encourages you to specialize, though some are too essential to not be “mandatory”.
Story is much better this time. It still has a lot of the similar narrative “tricks”, but they’re performed much more elegantly here. It’s also enhanced by having a lot of smaller sub-narratives and stories.
I suppose I’d be remiss not to mention how gorgeous this game is. It’s legitimately one of the prettiest damn games to date; the amount of environmental and background animation is at work is incredible. You’d think a move from 2D to 3D models would reduce the hand-crafted artistic quality, but it’s very much enhanced the experience instead.
They still kept in the obnoxious chase sequences for some reason, but they at least made them less fail-state-y and more forgiving.

5. Deathloop – 2021 – Steam – ★★★★★
Y’know, it’s weird; the interactive sim genre— as it were— hasn’t changed much in the last, what, twenty plus years? Sure, different games grant you different ability sets and what not, and the set dressing varies, but the core experiences are pretty similar. “Use ability to navigate environment in a first-person shooter, depending how you specialize you can approach this from different angles.” Different titles approach their RPG-itude differently, but overall, the general intent is that two different people’s “runs” of the same game would result in them picking different approaches through the environment based on their specialization.
Deathloop is a neat attempt at innovating on that, in that in that it is deliberately focused on the replay aspect— specialization occurs on a fairly limited level, and “runs” are more often about applying learned information and knowledge of an environment over and over again. I don’t think it does a perfect job— there’s not a lot of reason to swap “builds” between going loud or quiet, and the lack of specialization typically means you just take the optimal path each time— but it’s at least doing something different. It does encourage you to learn the environments and incorporate that into your memory between each loop, even if it doesn’t give you a ton of incentives to vary things up beyond “hey why not.”
The big complicating factor is the introduction of a Dark Souls-style PVP invader, which is quite fun from both sides of the equation. I’ve had a blast invading folks as Juliana and blasting away, and her being in a level does encourage you to take different approaches, but… not necessarily that different. A lot of folks seem to just camp out until she leaves, which is boring.
Weirdly, I’d say that this game’s strongest point is actually its writing? The targets you are killing aren’t necessarily that well-developed, but Colt, the player character, is fantastic. Incredibly funny and well-acted. The ending is kind of ehhhh fine, but Colt himself and the narrative largely around him is great.

4. The Outer Wilds: Echoes of the Eye – 2021 – Steam – ★★★★★
I was of mixed emotions about Outer Wilds getting DLC. I am on the record as having really, really liked that game. But it was so self-contained and well-made that, well, what could a DLC really add to the game? Wouldn’t it just bloat it, or just be the game in miniature?
Echoes of the Eye is kind of just that, yea. It’s a self-contained little journey that is wrapped in the burrito that is the rest of Outer Wilds. But it is also, like Outer Wilds, pretty dang good, so hey.
I’m not sure there’s much to say about this that isn’t a ditto from the Outer Wilds in terms of what I liked about it. There are aspects of it that I don’t care much for in terms of the overall flow, and how little it takes advantage of mechanics established elsewhere in the game (it is, again, pretty much self-contained, and that includes mechanically), but that honestly borders on quibbles compared to the enjoyment I got out of it.
It’s a nice little addition to Outer Wilds that, overall, does add some more context to the events you are uncovering elsewhere in the base game. It also adds a nice little to bonus to the ending of the base game, so hey.

3. Super Robot Wars 30 – 2021 – Steam – ★★★★★
It’s unbelievable that this happened. An official release of a main-line, non-OG SRW title in the West, on Steam. Absolutely unbelievable. And yet, here it is.
After a few years away— presumably from a mix of pandemic and just a general need to rework the systems after years of pretty same-y titles— SRW30 is actually fairly different mechanically. It removes the route system in favor of dynamic mission selection, allowing for more dynamic plot events where dialog shifts based on who you’ve recruited and the order of missions. The changes aren’t large, but they are interesting, and it does let them just pack tons of missions into the game. The game is big, even as Super Robot Wars titles go.
The cast list is also pretty different, if weird. I’m glad SSSS.Gridman has made an appearance, and the way it brings CCA/Zeta Gundam in this time around is certainly different. No real objections there, even if the Victory Gundam inclusion seems kind of funny overall.
I do have considerable issues with SRW30. The big one is the same issue I’ve brought up every time I talk about a SRW in these write-ups: the game is too goddamn easy. Like, yes, a lot of that is born from being familiar with the mechanics, and thus being able to take advantage of them. But the game also loves going out of its way making it very unchallenging to just absolutely break the systems. It’s not that there aren’t any stakes or challenge at all during missions, it’s just that any amount of understanding of the systems makes it not a challenge.
These games keep adding more and more ways for you to put yourself ahead of the curve. Upgrade your units? Upgrade their skills? Use spirits? Use power parts? Upgrade the AOS system? Use attacks in an optimal fashion? Use a small team? Perform any one of these, and even at the highest difficulty the game won’t be hard. Engage with multiple of them— or, God forbid, optimize based on your understanding of those systems— and the game become INCREDIBLY easy. It’s the thing where there’s whole systems that just don’t really come up because you never have to engage with them anymore. Enemies basically never use spirits except when triggered by cutscenes, tile-effects almost never come up— many stages don’t even use them— and the fact that the morale system can be broken in like 20 different ways makes the idea of Morale Downs completely pointless.
Some of this also comes down to mission structure; there’s not many missions that are just “ok, we’re forcing you to use some odd ball units, good luck”, or “we’re constraining how many units you have; you’ll have to play it smart”. You almost always just have to outlast the timer for 2 turns before reinforcements arrive, and the loss of a dedicated route system has introduced the unfortunate effect that you are never forced to “scrounge” lesser-played units. Who the hell is going to be sticking Tomache on the field when you have 80 more interesting protagonists that you can field at a given time?
That all being said: this is still a good time, just not necessarily the most intellectually stimulating time. Seeing the weird mash-ups and plays on lore is fun, and the systems are, at their heart, pretty relaxing. I want it to be better because I enjoy it. SRW30 came out at the right time, and it’s a deeply satisfying experience to me— I just wish it was more stimulating.

2. Metroid Dread – 2021 – Switch – ★★★★★
After nearly two decades of waiting, we’ve finally gotten a proper new 2D Metroid. And even better… it’s good.
There was a lot of reason to be skeptical, honestly. Other M was Metroid at its lowest, with Sakamoto going as far away as possible from what people like about Metroid in terms of both mechanics and narrative. None of the good Metroidvania exploration, and the plot was just awful.
I understand that most people don’t come to Metroid for ““the lore”” but it is something I genuinely enjoy and am somewhat invested in. In part because it’s so vague and weird and stupid (SCIENCE TEAM RULES), but also because Samus is genuinely cool. She’s a bounty hunter who was injected with birdman DNA by her bird dads after a space dragon ate her parents, and she proceeds to repeatedly cause planets to explode over the course of her job. She later gets Metroid DNA injected in her body, making her a bird-human-metroid hybrid. She twice got evil space gooed but she got better.
Starting with Fusion, Sakamoto started losing the thread of what people liked about Samus— the idea of this stoic space amazon, facing down monsters and repeatedly manifesting as different civilizations’ prophesized space messiah as part of just doing The Mission. Instead, she got internal monologues, she got bossed around. It sucked. But the criticism of all this seems to have finally got through— a lesson that carried through Samus Returns, and culminated finally in this.
Samus is so fucking cool in this game. She speaks exactly one line of dialog in the entire game, and it fucking rules. The silent characterization conveyed through the muted language of “eyes seen through power armor, and also a gun” works so much better than a constant monologue about ~THE BABY~.
The plot is also good. It’s a good follow up to story set up in previous titles (hey, maybe the Chozo weren’t all that great!!), and it really does put a bow on several plotlines while setting some stuff up for the future. The environmental storytelling could be somewhat better— I’d love a slightly more Prime-like touch— but overall, it works.
Speaking of environments: damn this game is pretty. Just really good animations and background, looks nice even on the Switch. The music works for it but is unremarkable. The gameplay feel is super smooth and good. Samus controls like a dream.
I’m somewhat torn about certain aspects of the gameplay, though. It’s a great game even with these qualms, but still: boy huh they really encourage linearity and discourage some kinds of backtracking. Like, the game isn’t quite Fusion level where you have Adam saying GO HERE TO GET THIS SAMUS HOW DARE YOU DIVERGE, but that’s mostly because it’s trying to be subtle about it instead. “Ooops you got this ability and we one-way doored you into this area so you can’t go back yet weird huh” “Huh you got this ability and there’s a teleporter nearby that immediately pops you to where we’d want you to backtrack to get your next ability weird huh.” “Oh, you got the thing over there now? Cool, we’re going to block off exploring around this area also and force you to go along this arbitrary path.”
None of this is bad perse, but it isn’t exactly as free form as some Metroids have been in the past. There are certainly some opportunities for sequence breaking in the game (much of it intended by the staff), but I think it could have done with a freer hand. The item collection aspects were fun, and they do tone it down as you get deeper, but still.
The boss designs are… fine. I think some of them hit too hard, or are somewhat overdesigned in that they do too many damn unique things. Whereas in the past you usually had enough life to tank a boss long enough for you to figure out what to do, bosses will kill you here in like 4 hits, pretty much no matter what, forcing you to learn patterns for dodging much more like a Souls-like. Which is fine I guess, particularly given the checkpointing before boss doors, but I found some fights generally just kind of long and annoying. I’m sure mileage will vary there, as both me and Red had pretty different picks of what bosses we liked and hated.
The EMMI encounters seem controversial but overall, I really liked them as a change of pace. You generally have enough mobility to get around them and avoid needing to “stealth”, and the checkpoints before reach EMMI area makes failure not too bad. They did become a little rote after a while, but so it goes.
But yeah, overall: pretty happy with the game. It’s probably my 4th or 5th favorite Metroid? Which, pretty good place to be.

1. Guilty Gear Strive – 2021 – Steam – ★★★★★
Totsugeki.
#metroid#metroid dread#guilty gear strive#super robot wars 30#outer wilds#ori#animal crossing#halo infinite
7 notes
·
View notes
Text
aimless musings on subgenre, citypop, and internet subcultures
theres something very interesting about watching citypop become very mainstream in korea and watching that feed back into both western listeners’ opinions and also into the sometimes-cynical efforts of a variety of kpop producers
a lot of people in the youtube/kpop sphere talk about the growth of citypop as if it were a spontaneous wave that appeared out of nowhere with mariya takeuchi’s plastic love getting picked up by the youtube algorithm in like 2018 or whatever, but thats a very like online-ignorant view of the interaction between vintage japanese music and worldwide online EDM production. citypop has been used in future funk and vaporwave for almost a decade by now, and, as a result, a number of citypop songs took off on social media here and there before plastic love’s acceleration— dress down by kaworu akimoto is one of the big examples off the top of my head, but there’s likely many many more.
youtube
“Plastic Love” by Mariya Takeuchi (1984). if you haven’t heard this yet, you’d better listen to it now. The video that first went viral was uploaded in 2017
youtube
“Selfish High Heels” by Yung Bae, Macross 82-99, and Harrison (2014) is a popular Future Funk remixes of Dress Down by Kaoru Akimoto (1986)
people who haven’t been very aesthetically literate online over the years— musically or visually, since those things are tied in subcultures— treat things like they come from nowhere. there are ongoing subcultural conversations that lead to certain aesthetic choices, and when someone tries to cash in on a trend without understanding what the trend is, that leads people to call bullshit. calling bullshit is not meanspirited, in my opinion, because it very much is like somebody who can’t speak a language getting up in front of everybody and saying “hey, i’m fluent!” and then speaking some vaguely that-language-sounding nonsense. of course people who genuinely speak that language will be outraged instinctively. it feels like being mocked.
that’s why the difference between music producers picking up on a trend cynically and music producers picking up on a trend with earnest interest in that trend’s origins feels different, even if the producers are similarly distant from the original subculture that produced that trend.
youtube
“Lady” by Yubin (2018) committed hard to the 80s JP citypop aesthetic, musically and visually, down to the sets, all fairly early in the major resurgence.
i’m sure that anyone with a passing familiarity with citypop and kpop can ascertain that not all kpop producers know what citypop is and what makes it citypop. all they know is that it is on-trend and they have to make it. not all kpop listeners know what citypop is and what makes it citypop. all they know is their idol said citypop as a buzzword in their little prepared statement. all this results in some interesting moments for me as a Music Fan, Online.
here is where i get to the thing that spurred this post: loona “did a citypop” for their japanese comeback. it doesnt sound like citypop.
youtube
“Hula Hoop (Citypop Version)” by Loona (2021). It has very odd percussion rhythms and mixing for citypop, no real attempt at a citypop verse, and strangely sparse gestures towards citypop in the form of a few seconds of bass and some synthesized orchestral embellishments that were taken from the original mix …all in spite of a very disco-inspired melody that should have worked perfectly for citypop
this is not a very big deal, and im not mad about it or anything. when a kpop act i like gets saddled with an unfortunate B-Side track i dont tend to take it very hard. however, it did raise a little bit of musical discourse in the loona fandom— in the form of remixes.
youtube
“hula hoop if it was actually a citypop song” by loonahatetwinks and Olivia Soul on youtube. this one has an original instrumental that is spot-on for contemporary k-citypop
My most favorite one of these remixes is a futurefunk remix by ZSunder, one of the very best LOONA fan producers. The fact that ZSunder thought to make a future funk remix at all speaks more to an understanding of the mutually supportive relationship between citypop and EDM genres than most kpop citypop producers or fanmixers seem to care to know about.
youtube
“Hula Hoop (Future Funk Mix)” by ZSunder is futurefunk made and mixed with such love that it has the infectious summery energy of a polished, big-name future funk hit
in the comments of this video, some people seemed to get the citypop-future funk connection and some didnt. many did get it, don’t get me wrong! but also, its not all that surprising for some kpop-focused listeners to not know much about EDM subcultures and the reasons behind various trends among producers, since kpop as an institution tends to take influences from any genre and culture it likes and then decontextualize those influences by just having their names used as buzzwords in the blurbs the idols have to recite when variety show hosts ask them about their latest single. this isn’t a criticism of the genre or the fans really, it’s just a part of the kpop industry that is used to add shine to an endless firehose-like stream of polished pop tracks. there are some issues with using whole genres and subcultures with complex histories as buzzwords, but god help us if we ever want a pop industry to give its influences their dues.
anyway, the intention behind ZSunder’s future funk Hula Hoop remix happened to remind me me of why i love Yukika’s discography so much, especially the Soul Lady album. I’ve seen some reviews online baffled by parts of Soul Lady, because the album in general is an exploration of that relationship between citypop and modern/internet EDM. i’ve seen plenty of Soul Lady reviews especially baffled by pit-a-pet, saying something along the lines of “what’s with the modern-sounding dance track in the middle of a retro album?”, but i think that pit-a-pet is a futurefunk-inspired track, at least in the chorus. considering both that and the Chill Lo-Fi Interludes, it seems like estimate’s team put together Soul Lady for Yukika in a way that shows that they love citypop and understand the online-specific electronic music subcultures that led to citypop’s resurgence.
youtube
“pit-a-pet” by Yukika (2020). the stacatto, bass heavy chorus is futurefunk enough, but the soaring orchestral part in the final chorus seals the deal for my interpretation.
youtube
“All Flights Are Delayed (1 hour version)” by Yukika (2020). Estimate literally released an hour-long youtube mix of one of the Lo-Fi interludes on Soul Lady as part of their promotion, clearly inspired by “Lo-Fi anime beats to chill out to,” which is another example of online producers from around the world using Japanese samples as a focal point of their music
Estimate, in the end, is still a Kpop production company, just the same as BBC, so they have no inherent claim over citypop, but the way that their exploration of subgenres clearly comes from passion and interest on the part of their production staff makes it so that their work with Yukika rings true. on the other hand, i really appreciate Ryan S. Jhun’s work on LOONA’s JP comeback, as well as on Not Friends, but the citypop mix thing was so clearly an afterthought to the point where fans of Loona who like citypop seem mostly just irritated by the cynical-seeming attempt.
heres one last good modern kpop citypop MV that has nods to the internet culture that led to its revival in the form of the videography— vaporwave, future funk, lofi, and other internet genres along those lines tend to have videos consisting of looping anime and vhs clips. future funk in particular is known for this, especially since a lot of future funk music, esp early future funk, is just loops of very short, catchy segments of citypop and disco songs. it’s all about the loops
youtube
“My Type” by Yoon JongShin ft. Miyu Takeuchi (2019). This song is so dedicated to the retro JP citypop sound that it’s almost beyond my personal taste. The singer, Miyu, was a headlining act at a seoul citypop festival and sang this song as part of her act (:
youtube
this video of “Only One” by Conscious Thoughts (2015) has a looped clip as an example for comparison with My Type. it also has a pulsing sidechain compressor working in time with its drum beat in a way that is common for future funk and that i think is a good example for my pit-a-pet yukika comparison to future funk
i guess the takeaway here is that media is more and more online, and the creation and propagation of digital audio and video content has been in the hands of literally almost anybody who wants to do it for the past two decades thanks to garage band and fruityloops and audacity and tiktok and youtube and bandcamp and soundcloud and myspace and newgrounds and p2p file sharing and so on and so forth. and therefore like… as with all things, the consumer class more and more is also the creator class, and therefore every member of an audio-visual subculture will have the ability to discern what is and isnt made with knowledge of the audio-visual language of that subculture
#me using elder millennial phrasing for Loona Did A City Pop to imply how out-of -touch it is kfhajfhs#mine#music#long post#Youtube
19 notes
·
View notes
Text
For Women's History Month 2021, GRAMMY.com is celebrating some of the women artists nominated at the 2021 GRAMMY Awards show. Today, we honor Taylor Swift, who's currently nominated for six GRAMMYs.
When we met Taylor Swift in 2006, it was immediately apparent that her songwriting approach was like ripping a page out of her diary.
"Just a boy in a Chevy truck/ That had a tendency of gettin' stuck/ On backroads at night/ And I was right there beside him all summer long/ And then the time we woke up to find that summer gone," she lamented in the first verse of her debut single, "Tim McGraw(opens in a new tab)." The way the then-16-year-old Swift could turn personal anecdotes into instantly memorable hooks mirrored the prowess of an industry veteran, appealing to more than just the teenage girls that could relate to a short-lived high school romance.
Now, nearly 15 years later, Swift has introduced another layer of intrigue with a foray into indie folk, unveiling a pair of albums, folklore and evermore, last year. Recorded entirely in isolation after the COVID-19 pandemic hit in March 2020, folklore has been widely acclaimed(opens in a new tab) as Swift's best album, touted for its intimate songwriting and cinematic dynamics; evermore has received similarly glowing reviews(opens in a new tab).
folklore was 2020's best-selling album(opens in a new tab) and earned Swift five GRAMMY nominations at the 2021 GRAMMY Awards show, including her fourth Album Of The Year nod. (evermore will be eligible for the 64th GRAMMY Awards in 2022.) As her 10 previous GRAMMY wins suggest, though, this new chapter isn't an abrupt departure for the star—it's a masterful continuation of her evolution as a singer/songwriter.
If there's one thing that Swift has proven throughout her career, it's that she refuses to be put in a box. Her ever-evolving sound took her from country darling to pop phenom to folk's newest raconteur—a transition that, on paper, seems arduous. But for Swift, it was seamless and resulted in perhaps her most defining work yet. And folklore’s radiance relies on three of Swift’s songwriting tools: heartfelt balladeering, autobiographical writing, and character-driven storytelling.
While there was always a crossover element to Swift's pop-leaning country tunes, her transition from country starlet to pop queen began with Red. The album’s lead single, the feisty breakup anthem "We Are Never Ever Getting Back Together(opens in a new tab)," was Swift's first release to reach No. 1 on the Billboard Hot 100 (and, ironically, scoffed "indie records much cooler than mine"). She declared a full pop makeover with 2014's 1989, but the response proved that her bold move was the right one: Along with spawning three more No. 1 hits, the project won Swift her second GRAMMY for Album of the Year.
From there, 2017’s Reputation, a response to media scrutiny, and 2019’s Lover, an often bubbly exploration of all facets of affection, followed. Although they shared similarly grandiose production, Lover featured a handful of poetic ballads, including "The Archer(opens in a new tab)," a self-reflective love song that teased Swift's folk sensibilities through storybook lyrics and ambient textures.
Swift’s ballads are key in understanding the full essence of folklore. They’ve regularly marked standout moments on each of her albums, both thanks to her poignant vulnerability and rich tone. Fearless standout "White Horse" earned Swift two GRAMMYs in 2009; Red's painstaking "All Too Well" was an instant fan favorite; 1989's "This Love" and Reputation's "New Years Day" provided tenderness amid otherwise synth-heavy sounds.
The raw emotion she puts into her downtempo songs comes alive on folklore, introducing a new wave of neo-classical sonics that elevate her fanciful penmanship to an ethereal level. Whether or not Swifties saw a full indie-pop record coming—at least not yet—the shift isn't all that surprising. Folklore’s romanticized lyrics and relatively lo-fi production are arguably what many fans have been patiently waiting on.
Lyrically, the super-personal nature of Swift’s music has always captivated fans and naysayers alike; diehards and critics dissected each of her albums for its real-life subjects and hidden meanings. While she played into those conspiracies at the time—whether she was revealing names in titles like "Hey Stephen(opens in a new tab)" and "Dear John(opens in a new tab)" or scathing the other girl on "Better Than Revenge(opens in a new tab)"—even Swift herself admits that her teenage method had an expiration date.
"There was a point that I got to as a writer who only wrote very diaristic songs that [it] felt unsustainable for my future moving forward," she told Apple Music's(opens in a new tab) Zane Lowe in December of 2020. "It felt like too hot of a microscope ... On my bad days, I would feel like I was loading a cannon of clickbait when that's not what I want for my life."
That realization is what helped make folklore so memorable: Swift stripped away the drama to let her artful storytelling shine. Sure, there are occasional callbacks to personal happenings ("invisible string(opens in a new tab)" references sending her exes baby gifts and "mad woman(opens in a new tab)" alludes to her legal battle with Scott Borchetta and Scooter Braun). Still, she largely shies away from her autobiographical narratives to make way for her imagination.
"I found myself not only writing my own stories, but also writing about or from the perspective of people I've never met, people I've known, or those I wish I hadn't," Swift wrote in a letter to fans(opens in a new tab) on social media the day folklore arrived. "The lines between fantasy and reality blur and the boundaries between truth and fiction become almost indiscernible."
folklore might be her first full project dedicated to creating characters and projecting storylines, but Swift has shown a knack for fantasy from the start. Tracks like "Mary's Song (Oh My My)(opens in a new tab)" on her self-titled debut and "Starlight(opens in a new tab)" on Red saw Swift craft stories for real-life muses ("Mary's Song" was inspired by an old couple who lived next door to Swift in her childhood; "Starlight" was sparked from seeing a picture of Ethel and Bobby Kennedy as teens). Even when songs did pertain to her real life, Swift often had a way of flipping memories into whimsical metaphors, like the clever clap-back to a critic on Speak Now's "Mean(opens in a new tab)" or the rebound relationship in Reputation's "Getaway Car(opens in a new tab)."
To think that we wouldn't have folklore without a pandemic is almost surreal; it's already become such a fundamental piece of Swift’s artistic puzzle. There was no telling what may have come after the glittering "love letter to love itself” that was Lover, but it seems isolation made the singer rethink any plans she may have had.
"I just thought there are no rules anymore because I used to put all these parameters on myself, like, 'How will this song sound in a stadium? How will this song sound on radio?' If you take away all the parameters, what do you make?" she told Paul McCartney in a November (opens in a new tab)Rolling Stone(opens in a new tab) interview(opens in a new tab). "And I guess the answer is folklore."
Even if she hasn’t been making indie music herself, Swift has shown an affinity for the genre over the years through curated digital playlists(opens in a new tab). Those included four songs by The National including "Dark Side of the Gym," which she references on folklore single "betty(opens in a new tab)," and "8 (Circle)" by Bon Iver, Swift's collaborator on folklore's gut-wrenching "exile(opens in a new tab)" as well as evermore’s title track. (“Exile” is one of folklore’s GRAMMY-nominated cuts, up for Best Pop Duo/Group Performance.)
The National’s guitarist Aaron Dessner co-wrote nine and produced 11 of folklore's 16 tracks, soundtracking Swift's imaginative tales with sweeping orchestration and delicate piano. Their partnership started with "cardigan(opens in a new tab)," a melancholy take on teenage love(opens in a new tab) that's up for Best Pop Solo Performance and the coveted Song of the Year. The team-up was a dream come true for Swift, a self-proclaimed National superfan and a career highlight for Dessner, who shared in an Instagram post(opens in a new tab) about folklore that he's "rarely been so inspired by someone." He sees the album as a pivotal moment for both Swift's career and pop music.
"Taylor has opened the door for artists to not feel pressure to have 'the bop,'" Dessner shared with (opens in a new tab)Billboard(opens in a new tab) in September. "To make the record that she made, while running against what is programmed in radio at the highest levels of pop music—she has kind of made an anti-pop record. And to have it be one of the most, if not the most, successful commercial releases of the year that throws the playbook out.
"I hope it gives other artists, especially lesser-known or more independent artists, a chance at the mainstream," he continued. "Maybe radio will realize that music doesn't have to sound as pushed as it has. Nobody was trying to design anything to be a hit. Obviously, Taylor has the privilege of already having a very large and dedicated audience, but I do feel like it's having a resonance beyond that."
Swift's other primary folklore collaborator was Jack Antonoff. He has been her right-hand man since they first paired up on 2013's promotional single "Sweeter Than Fiction(opens in a new tab)" (Swift referred to him as "musical family" in her folklore announcement(opens in a new tab)). Even after years of creating stadium-ready pop smashes, Antonoff said in his own folklore Instagram post(opens in a new tab), "I've never heard Taylor sing better in my life / write better."
As Swift recognizes herself, folklore ushered in a new way of thinking for the superstar that not only brings out her best, but sets a promising precedent for what's to come. "What I felt after we put out folklore was, 'Oh wow, people are into this too, this thing that feels really good for my life and my creativity,'" Swift added in her interview with Lowe. "I saw a lane for my future that was a real breakthrough moment of excitement and happiness."
Her enthusiasm is tangible on both folklore and evermore. Dubbed folklore’s sister record, evermore further expands Swift’s newfound mystical atmosphere. Much to the delight of many Swifties, the follow-up also calls back to her country beginnings on tracks like the HAIM-assisted “no body, no crime(opens in a new tab),” as well as her pop expertise on more uptempo cuts like “long story short(opens in a new tab).”
Together, the albums are a momentous reminder that Swift is a singer/songwriter first. Her wordcraft is some of the most alluring of her generation, and that’s never been lost on her music, regardless of the genre she’s exploring. But now that Swift also feels she's at her best, it’s evident folklore was just the beginning of Taylor Swift in her finest form.
49 notes
·
View notes
Text
30 (Technically 34) Albums We Loved That Happened To Come Out in 2020
So much has already been said and written about this cursed past year, but a few good things came out of it, including the music. Album-wise, like many before it and many to come, it was an embarrassment of riches. But even with so much time on our hands to devour new tunes, it was often old favorites, songs of comfort or familiarity that garnered the heaviest rotation. For many artists, too, it was a year ripe for revisiting or reissues of old material, looking at existing songs with fresh and new perspectives. Simply put, with so much to listen to, new and old, the prospect of ranking a finite number of albums felt not only daunting, but frankly a bit stupid. Maybe we were late to the game, but 2020 taught us that music should and can be appreciated in multiple contexts, not limited to but including when it first came out and when it was heard again and again, even if years later. The records below--listed in alphabetical order--happened to be released in some form in 2020, whether never-before-heard or heard before but in a different format. And the only thing I know is that we’ll be listening to them in 2021 and beyond.

Autechre - SIGN & PLUS (Warp)
The legendary British electronic music duo surprise released SIGN a mere month and a half after its announcement and then PLUS 12 days later. The former was a beatific collection of soundscapes that belied the band’s usual harsh noise, while PLUS embraced that noise right back, drawing you in with the clattering chaotic burbles of opener “DekDre Scap B” and lurching forward. -Jordan Mainzer
Against All Logic - 2017-2019 (Other People)
The perennially chill ambient house artist Nicolas Jaar had a busy 2020, as usual, releasing two albums under his name, Cenizas and Telas. But it was 2017-2019, the follow-up to the debut album from his Against All Logic moniker, that came first and throughout the year helped to illustrate Jaar’s penchant for combining inspired samples with club beats and tape hiss. Take the way the lovelorn vocals of “Fantasy” or soulful coos of “If Loving You Is Wrong” war skittering, scratchy percussion and cool arpeggios, respectively: Jaar is coming into his own as a masterful producer almost a decade after he released his first full-length. Oh, and bonus points for including none other than Lydia Lunch on a banger so blunt it would make Death Grips blush. - JM

Bartees Strange - Live Forever (Memory Music)
Like many, my introduction to Bartees Strange was through Say Goodbye to Pretty Boy, his EP of The National covers. Creativity and shifting perspectives shine through each song’s reimaging, like flipping the coarse, almost manic “Mr. November” into something softer, more meditative. It felt like a mere peek into what was to come on Live Forever. Bartees Strange is a world-builder. Each track on his debut unfolds and welcomes you to a wildly engaging tableau, a fully constructed vision. “Jealousy” opens with soft vocals and birdsong. “In a Cab” is the slick soundtrack to racing through a cityscape in the rain, seeing the blurred lights of the high-rises above as you pass by. “Kelly Rowland” warps wistful pop song feelings. “Flagey God” takes you into a dark, pulsing club while only a few songs later, “Fallen For You” wraps you in echoed vocals and romantic, raw acoustic guitar.
It’s an accomplishment to craft an album of individual songs that stand strongly on their own but still feel cohesive. 2020 wasn’t all bad. It gave us Live Forever, a declaration of an artist’s arrival. - Lauren Lederman

Charli XCX - how i’m feeling now (Atlantic)
Back in the spring, many of us wondered who would put out something great in 2020’s quarantine. It was hard to imagine that the intensity of a global pandemic would really allow for artists to embrace creativity. That thought carries the same eye-roll inducing feeling of “We’ll get some great punk music out of a Trump presidency,” but of course, Charli XCX delivered. Through live workshops with fans and longstanding collaborators, she delivered songs to dance alone to in your bubble. Charli embraces the unknown of the moment but clutches onto what’s familiar. Under the glitch-pop veneer of the album, she digs into the anxieties of not just this moment of time but of the bigger questions we all confront: trajectories of relationships with friends, romantic partners, ourselves. Album standouts “forever” and “i finally understand” embrace that feeling of both looking for control and accepting the lack of it. Charli is a master at balancing this. - LL

Christine and the Queens - La Vita Nuova (Because Music)
Named after a Latin text by Dante Alighieri about missing a woman who has died, Chris’ La Vita Nuova is not about mourning a death but instead about loneliness and isolation, post-relationship or otherwise. It doesn’t bang quite like her previous two albums, but it hits harder than ever.
Read our full review here.

Dogleg - Melee (Triple Crown)
Released on March 13th, right as the COVID-19 pandemic hit, Melee was supposed to be supported by three cancelled tours–SXSW, an opening slot for Microwave, and an opening slot for Joyce Manor–and an appearance at this year’s cancelled Pitchfork Music Festival. Listening to the songs on the record, you can only imagine how they translate: the jerky momentum of “Bueno”, build-up of “Prom Hell”, gang vocals of “Fox”, clear-vocal anthem of “Wrist”, and odd groove of “Ender”.
Read “Buckle Up, Motherfucker”, our interview with Dogleg.
Dua Lipa - Future Nostalgia & Dua Lipa/The Blessed Madonna: Club Future Nostalgia (Warner)
Where Dua Lipa’s much-anticipated second album Future Nostalgia succeeded was in its disco anthems and retro, club-ready beats, so who better to bring out the best of the record than The Blessed Madonna? The turntablist masterfully curates a mix of heavy hitters of the charts and the underground that not only offers an essential complement to Future Nostalgia but transcends it. Sending the tracks out to various producers and singers for features and then adding her own samples on top, she invites you to peel back the layers, enter a YouTube rabbit hole of sample searching as much as bopping along.
Read our full review here.

Emma Ruth Rundle & Thou - May Our Chambers Be Full (Sacred Bones)
Roadburn Festival has long been on my bucket list, and since the pandemic showed me how much live music can be taken away in a flash, when it’s safe again to travel and go to a festival, I may just pull the trigger and go--especially considering it’s the springboard for such fruitful and inspired collaborations as the one between Louisville singer-songwriter Emma Ruth Rundle and Baton Rouge sludge dwellers Thou. Rundle embraces the heavier opportunities on the follow-up to her incredible 2018 record On Dark Horses with the ever-flexible Thou backing her up vocally and instrumentally. Slow-burning opener “Killing Floor” offers a familiar introduction to fans of both--sort of what a Rundle/Thou song would sound like--before grunge chugger “Monolith” introduces huge, catchy riffs and “Out of Existence” a True Widow-esque dirge, newfound inspirations for both artists bringing the best out of each other. - JM
Fiona Apple - Fetch the Bolt Cutters (Epic)
What makes Fetch the Bolt Cutters stand out among Apple’s catalog and music in general is the clarity with which Apple seethes at those who have wronged her, whether ex-boyfriends or patriarchal oppressors, and looks to her relationships with other women for peace of mind.
Read our full review here.
HAIM - Women in Music Pt. III (Columbia)
For HAIM, the title Women in Music Pt. III is suggestive that, more than their previous two records, their third centers around the experiences of being an all-female band in a historically white cis male-dominated scene, at least one that wouldn’t call catchy riffs written by a man “simple” or call attention to the faces a man makes while playing. What it doesn’t let on to is how deeply personal the record is, how, by unabashedly embracing genres and styles of music that they love, HAIM have made far and away their best album. Co-produced by the usual suspects, Danielle Haim, Ariel Rechtshaid, and ex-Vampire Weekender Rostam Batmanglij, it’s instrumentally and aesthetically dynamic and diverse, consistently earnest without devolving into cheese.
Read our full review here.
Irreversible Entanglements - Who Sent You? (International Anthem)
I’ve been captivated by Irreversible Entanglements ever since I first saw them at Pitchfork Music Festival 2018. The radical poetry of Camae Ayewa (aka Moor Mother) is the perfect front for a ramshackle mix of Luke Stewart’s spidery bass, Tcheser Holmes’ weighty drums, and a horn section that concocts tones that range from hopeful to desperate. At their best, Who Sent You? is a shining example of celebratory Afrofuturism and metaphysics that makes the urgency of Ayewa’s more concrete and political words all the more necessary. “No Más”, composed by Panamanian-born trumpeter Aquiles Navarro, is a declaration against imperialist oppression, while the stunning title track flips the switch like a Kara Walker painting, as Ayewa’s the one interrogating the police officer terrorizing her community. “Who sent you?” she repeats, never spiraling, grabbing a hold of the power and never letting go. - JM

Jeff Parker - Suite for Max Brown (International Anthem/Nonesuch)
It’s Jeff Parker’s mom’s turn. After 2016′s The New Breed ended up being a tribute to the guitarist’s father, who passed away during the making of it, Parker decided to pay tribute to Maxine while she was still alive. Suite for Max Brown (Brown is his mother’s maiden name; Max is what people call her) is a genre-bending collection of tracks inspired by Parker’s DJing, juxtapositions of sequenced beats with improvisation that certainly sound like the brainchild of one individual. Indeed, Parker plays the majority of the instruments on it and engineered most of it at home or during his 2018 Headlands Center residency in Sausalito, CA; though all of the players and the vocalist (Jeff’s daughter Ruby Parker) on The New Breed show up, plus a couple trumpeters (piccolo player Rob Mazurek and Nate Walcott of Bright Eyes) and cellist Katinka Kleijn, Suite for Max Brown is a distinctly Jeff Parker record.
Read our preview of Jeff Parker & The New Breed’s set at Dorian’s last year.
Jeff Rosenstock - NO DREAM (Polyvinyl)
Jeff Rosenstock throws us right into the spinning, manic energy of NO DREAM, his latest release from a seemingly endless well of music that never lacks urgency. It’s a reminder that though it’s been a strange year, the issues Rosenstock tackles here aren’t new. There’s no interest in making you feel comfortable here. On the album’s title track, Rosenstock sings, lulling you into a false sense of security, “They were separating families carelessly / Under the guise of protecting you and me.” But reality sets in, and the hazy guitars spin out as he spits, “It’s not a dream!” and, “Fuck violence!”
My image of Jeff Rosenstock in the year 2020 is masked up with “Black Lives Matter” scrawled across the fabric of his mask in Sharpie, performing album highlight “Scram!” on Late Night with Seth Meyers as high energy as ever. It felt like watching someone send out a beacon, both a distress signal and a call to arms. - LL
Jessie Ware - What’s Your Pleasure? (PMR/Friends Keep Secrets/Interscope)
I am not someone who goes to clubs. I don’t “go out dancing,” preferring to let loose in the privacy of my own home or a trusted friend’s house party. But Jessie Ware’s What’s Your Pleasure? makes me think I could embrace a night out like that, once the world opens up again, of course. The album is filled with syncopated disco beats that feel fresh and classic all at once. The abundant horns and strings on “Step Into My Life” are decadent, like light bouncing off sequins in a dark room. Ware’s voice is slinky and velvety one moment, windswept like her album cover the next. It’s songs like “Save a Kiss” that embrace both, allowing her to show off her range. - LL

Laura Marling - Song for Our Daughter (Partisan)
With sparse production, mostly from her but with additions from Ethan Johns and Dom Monks, Marling foregoes the comparative maximalism of the Blake Mills-produced Semper Femina, her last proper full-length, and 2018′s LUMP collaboration. The songs aren’t simple, but they’re succinct, and every element, from Marling’s finger-picked guitars, the occasional slide guitar, and that unmistakably calm voice, sometimes alone and sometimes layered, fits. It’s her most universal set of songs yet, centering around the times when we’re apart from one another but reflecting on when we were together and when we might be together again, with no guarantees.
Read the rest of our review here.
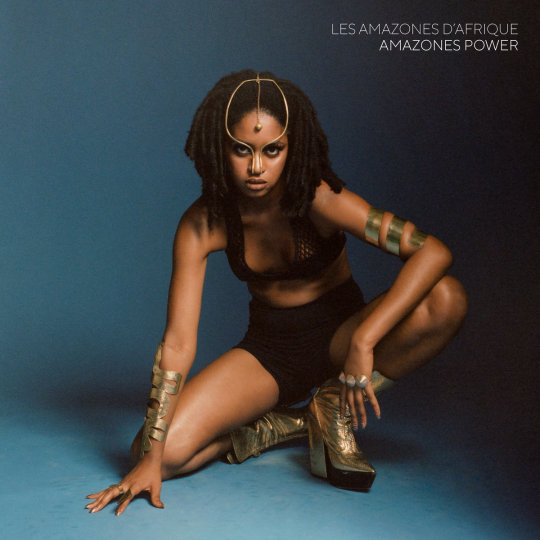
Les Amazones d’Afrique - Amazones Power (Real World Records)
The groovy pan-African collective expands upon their debut Republique Amazone and then some with Amazones Power, a tour-de-force statement of female empowerment in the face of oppression against women throughout the African diaspora. Indeed, the album is more than just songs boldly decrying FGM, though those demands ring heavily. Instead, the group goes further, delving into gender power structures in marriage on “Queens” and selectively finding strength in tradition on “Dreams”. And this time, they include men to stand alongside with them. “Together we must stand / Together we must end this,” sings Guinean musician/dancer/artist Niariu on opener “Heavy” in solidarity with features Douranne (Boy) Fall and Magueye Diouk (Jon Grace) of Paris band Nyoko Bokbae. But perhaps it’s her kiss-off on “Smile” that hits hardest: “I shut up for no one.” - JM

Lianne La Havas - Lianne La Havas (Nonesuch)
The British singer-songwriter’s much anticipated follow-up to 2015′s Blood was better than I could have ever imagined. A song cycle about life cycles--of nature, of lives, of a relationship--inspired by an actual breakup, Lianne La Havas is a contemporary neo soul masterpiece. Overview opener “Bittersweet” is an instant earworm, La Havas’ coo-turned-belt filling the space between classic and increasingly emotive slabs of piano and guitar. Funky, lovestruck strut “Read My Mind” is the soundtrack for the unbridled confidence of finding new love. Yes, the doubts begin to sow on the fingerpicked melancholy of “Green Papaya” and “Can’t Fight”, and where the album goes from a simple narrative perspective may be predictable: They break up, they don’t get back together, La Havas enjoys her independence. But the depth of the arrangements and assuredness of La Havas’ singing is a product of an artist starting to really show us what she can do. And how many people can pull off a Radiohead cover like that? - JM
Lomelda - Hannah (Double Double Whammy)
What does it mean to title an album after yourself? Lomelda’s latest album is centered around discovering more about yourself while not always having the answers. Despite the lyrical content, the album is self-assured. Hannah Read’s voice feels as steady as ever as it navigates these twisting questions, like the way the world can shift after a kiss. She finds power in softness and reflection throughout the album, like when she explores the mantra-like words of “Wonder” or through a reminder to do no harm in “Hannah Sun”. In a year that allowed for perhaps more reflection than usual, Hannah makes space for the questions that arise out of figuring yourself out, of making sense of the messiness of it all, wrapped in warm guitar, balanced vocals, and steady drums. - LL
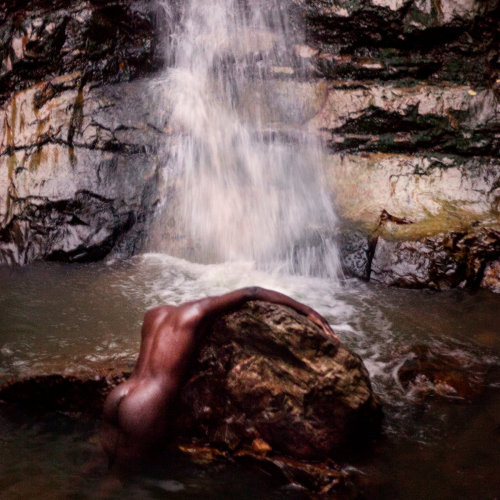
Moses Sumney - Grae (Jagjaguwar)
“Am I vital / If my heart is idle? / Am I doomed?” Moses Sumney famously sang on his stunning 2017 debut Aromanticism, an album that saw him developing his acceptance of being alone. grae, his two-part 2nd full-length, and his first since officially moving from L.A. to the Appalachian Mountains of Asheville, North Carolina, doubles down on themes of heartbreak, but instead of being sure in his seclusion, he embraces the unknown. The album teeters between interludes of platitudes about isolation and ruminations on failed human connection, and maximally arranged clutches of uncertainty. “When my mind’s clouded and filled with doubt / That’s when I feel the most alive,” Sumney coos over horns and piano on slinky soul song “Cut Me”; it’s an effective mantra for the album.
Read the rest of our review here.
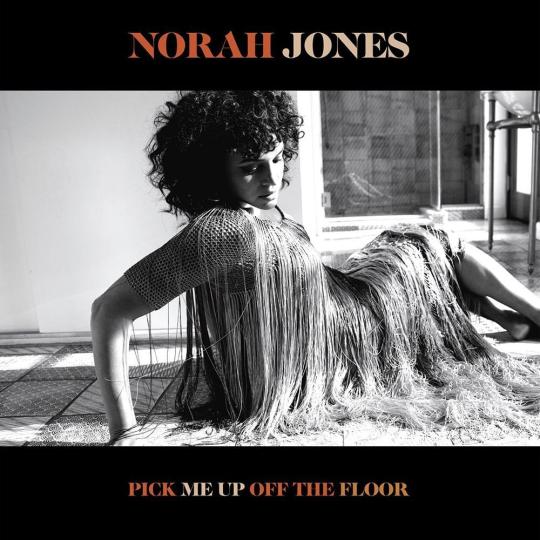
Norah Jones - Pick Me Up Off The Floor (Blue Note)
At the time we previewed Norah Jones’ 7th studio album, she had only released a few tracks from it. Turns out the rest was just as powerful. From the blues stomp of “Flame Twin” to the rolling piano stylings of “Hurts to Be Alone”, Pick Me Up Off The Floor is an album full of jazzy orchestrations and soul and gospel-indebted arrangements, Jones’ silky, yearning voice tying together the simple, yet lush and deep instrumentation. And that other Tweedy feature, that closes the album? It’s a heartbreaking portrait of loneliness, one of many on a record that still manages to celebrate being alive all the while. - JM

Phoebe Bridgers - Punisher (Dead Oceans)
Phoebe Bridgers is a master of details. Her lyrics shine when they get specific. They range from the mundane to morbid: A superfan’s ghost-like wandering under a drugstore’s fluorescent lights, a skinhead likely buried under a blooming garden, reckoning with the you in “Moon Song”’s lines, “You are sick, and you’re married / And you might be dying.” Bridgers has always been able to set a scene meticulously, and Punisher arrived with 11 songs that expanded that skill, both lyrically and musically, with her dark humor intact and a fuller sound that includes her boygenuis collaborators’ harmonies. - LL
PJ Harvey - To Bring You My Love: The Demos & Dry - The Demos (Island)
Yes, revisiting Dry’s demos as a separate entity is still worthwhile. Harvey’s powerhouse vocal performance carries the acoustic strummed “Oh My Lover”, while the comparatively minimal arrangement of “Victory” highlights bluesy riffing, call-and-response harmonies, and layered guitar and vocals. The singles, the slinky and sharp “Dress” and propulsive anthem “Sheela-Na-Gig”, hold up to their ultimate studio versions, too. But it’s the To Bring You My Love material that provides novelty because it’s never been released and more so because it encompasses the greatest aesthetic contrast from the album. From the warbling hues and guitar lines of the title track to the tremolo haze of “Teclo” to the crisp snares of “Working With The Man”, the demos show a continuity and level of cohesiveness with the diversity of Dry and Rid of Me not shown on the studio version of Harvey’s more accessible commercial breakout. (Predictably, the album’s most well-known song, “Down by the Water”, is the closest to its eventual version.) “Long Snake Moan” is simultaneously more spacious and more noisy, its garage blues a total contrast to the lurking “I Think I’m A Mother” and swaying shanty “Send His Love To Me”. And “The Dancer” fully embraces its flamenco influences, hand claps and all.
Porridge Radio - Every Bad (Secretly Canadian)
Is there a better opening line than “I’m bored to death, let’s argue”? That kind of duality is found across all of Every Bad as it grapples with the frustrations and anxiety of trying to figure it all out, whatever that might mean for you. “Maybe I was born confused, but I’m not,” vocalist Dana Margolin repeats throughout the opening track, roping in listeners with the dizzying feeling of trying to make sense of yourself. The band’s guitar and synth sound coupled with Margolin’s howl makes for a dance party filled with dread, rendering Margolin’s already strong, repetitive lyrics even more spiraling. And yet, by the time we get to “Lilacs”, a glimmer of something else shines through as the music gets more manic and Margolin’s voice begins to soar: “I don’t want to get bitter / I want us to get better / I want us to be kinder / To ourselves and to each other.” - LL
Sault - Untitled (Rise) & Untitled (Black Is) (Forever Living Originals)
Yes, Black Is still pulls plenty of devastating punches. “Eternal Life”, a segue from the gospel boost of “US”, juxtaposes a deliberate drum beat with zooming synths, both ascending like a chorus of angels, as they sing, “I see sadness in your eye / ‘Cause I know you don’t wanna die,” presenting the oppression of Black life at the hands of white supremacy in inarguable terms. Ultimately, though, it’s the anthemic nature of the songs, resistant of platitudes, that shines through. “Nobody cared / This generation cares,” says Laurette Josiah on “This Generation”. Whether she’s talking about young people in general or the latest generation of young Black leaders, the sentiment is reflected on songs like “Black”, wherein over dynamic, sinewy instrumentation, the singers alternate between encouragement, support, and love of the self and others.
Read our full review here.

Shamir - Shamir (self-released)
Shamir’s voice is a bright beacon in a sea of conventional singers. Shamir captures the effervescence of pop music and weaves it together with elements of country, alt rock, and diary confessional lyrics all supported by the emotion and range of his vocals. There’s something for everyone across the album’s 11 shimmering tracks. Lead single and opener “On My Own” feels like a declaration of self and self-sufficiency, an anthem of a breakup song. The almost pop-punk bounce of “Pretty When I’m Sad”, paired perfectly with lines like the angst-ridden, “Let’s fuck around inside each other’s heads,” feels impossible to not bop along to. The twang of “Other Side” would put a country crooner to shame. That’s the power of Shamir. His voice has the ability to smoothly convey joy, resilience, and humor. He uses elements of several genres, not just the dance-pop of his debut, to build a unique album that gives listeners so much to sift through and, of course, dance to. - LL

Songhoy Blues - Optimisme (Fat Possum)
If Songhoy Blues’ second album Resistance lacked “the grit of its predecessor,” it’s clear from the hard rock stomp of the opening track of Malian band’s third album Optimisme that they rediscovered their mojo. More importantly, they couple this maximal brashness with tributes to those who make their world a better place: fighters for freedom, women, the young. It’s perhaps the first Songhoy Blues record to truly combine the celebratory nature of their desert blues with a balanced mixture of idealism and vigor. - JM

Spanish Love Songs - Brave Faces Everyone (Pure Noise)
How can you find hope in hopelessness, or optimism when every news story points to cruelty? Is it naïve to keep searching for light in the dark? I don’t think so, and I don’t think Spanish Love Songs does, either. I’d like to think we both believe that’s not naivety, but power. It’s the embers you need to really ignite a flame. After all, this is the band with a song titled “Optimism (As a Radical Life Choice)”. It’s a band whose crunching guitars and earnestness insist that despite death and depression and addiction, the instinct to survive shines brightly above all. That relentless hope resurfaces across Brave Faces Everyone’s 10 tracks even as it works through the bleakness of everyday life. - LL

Tashi Dorji - Stateless (Drag City)
The magnum opus from the Asheville-based picker is a group of evocatively titled, disorderly songs about the desolate hellscape of America for outsiders and immigrants. Enigmatic in its nature, not exactly narrative, Stateless combines Dorji’s urgent strumming with moody motifs, captured beautifully in a studio setting for maximum emotional wallop. - JM

Touche Amore - Lament (Epitaph)
Is this what an almost uplifting Touche Amore album sounds like? It’s cathartic in a newer way for the band, especially after the beautifully rendered grief of Stage Four. Lament loses none of the band’s aggression or urgency. “Come Heroine” thrusts listeners into that urgency and introduces a moment of warmth, Jeremy Bolm’s vocals still rasping and insistent: “You brought me in / You took to me / And reversed the atrophy.” The bounciness of “Reminders” may seem close to optimism, but a sharper look at the lyrics uncovers more than blindly looking to the things that bring joy. “I’ll Be Your Host” is reflective, a few years removed from Touche Amore’s previous album and the immediacy of loss, self-aware and growing, but still raw. The album closer, “A Forecast”, takes a turn, a lone voice and piano acting as a confessional before giving way to thrashing guitars and the realization that growth and reckoning with trauma doesn’t mean minimizing it. It means learning to keep moving forward and to stop for help when you may need it. - LL

Waxahatchee - Saint Cloud (Merge)
The best album yet from Katie Crutchfield is inspired by positive personal change (getting sober, dealing with codependency issues, her blossoming love with singer-songwriter Kevin Morby) and reflections on family and friends. Named after the suburb of Orlando where her father’s from, Saint Cloud is a genre-hopping collection of stories and feelings that doesn’t necessarily follow any semblance of narrative. On opener “Oxbow” and country-tinged ditty “Can’t Do Much”, Crutchfield’s increasingly aware of the need to pick your side and your battles, whether in the relationship between two people or between the allure of the bottle and the next-day hangover. Some of the best songs on the album see her finding commonalities with others as a means towards self-love. Gentle strummer “The Eye” refers to her natural creative relationships with Morby and her sister Allison. “War” she wrote for herself and best friend, who is also sober, the title a metaphor for one’s fight to remain substance-free. “Witches” is an ode to her best friends, including Allison and Snail Mail’s Lindsey Jordan, all equally frustrated by the toxic nature of the music industry and the world at large, ultimately lifting each other up because they simply have each other.
Read our full review here.
#autechre#against all logic#bartees strange#charli xcx#christine and the queens#dogleg#dua lipa#emma ruth rundle & thou#fiona apple#haim#irreversible entanglements#jeff parker#jeff rosenstock#jessie ware#laura marling#les amazones d'afrique#lianne la havas#lomelda#moses sumney#norah jones#phoebe bridgers#pj harvey#porridge radio#sault#shamir#songhoy blues#spanish love songs#tashi dorji#touche amore#waxahatchee
66 notes
·
View notes