#2000a alternative
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The Tumblr office adopted Tommy, an 11-year-old Pomeranian.
Text

#2000s nostalgia#2000s aesthetic#2000s blog#2000s internet#2000s web#2000s fashion#2000s style#2000s girl#striped socks#2000a alternative#alternative fashion#alt fashion#alt girl#alt aesthetic#punk aesthetic#punk girl#2000s punk#pop punk#punk fashion#punk style#myspace#myspace era#myspacecore#myspace aesthetic#myspace graphics
52 notes
·
View notes
Text
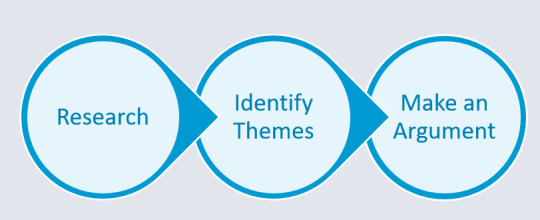
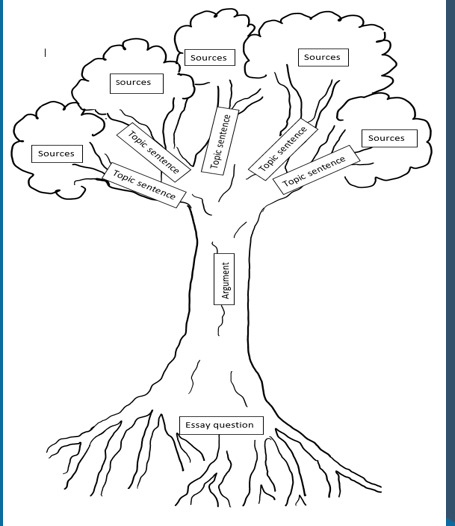
Research Map for argument
•The solipsistic voice – opinionated and is not backed up with literature
•Unaverred voice - provides a ‘patchwork’ of summaries and the student does not provide their own stance
•Unattributed voice – use other people’s ideas as if they were their own
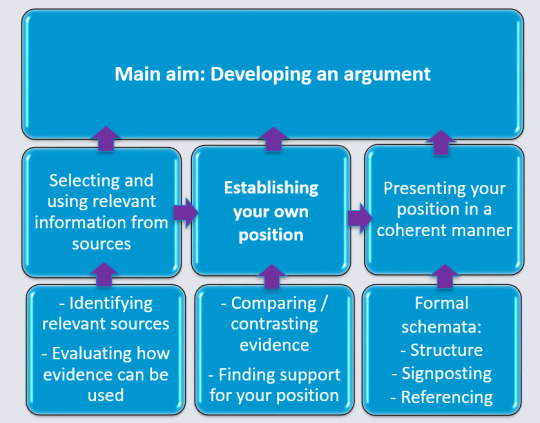
In summary, building a strong academic argument involves:
Wide-ranging research on the subject.
Identifying and considering different perspectives.
Using alternative views to structure your essay or argument.
Engaging with existing literature and addressing what others say.
Participating in the scholarly conversation by first examining the ideas of others.
Carefully analyzing the abstract, introduction, and conclusion of relevant sources to understand the author's position and argument.

When reading various texts, look for patterns and recurring themes in the writing and arguments. You can ask questions such as:
What are the primary arguments on the topic?
Is there consensus or disagreement on the subject or specific aspects of it?
Are there prevalent or trendy arguments?
What are the key strengths and weaknesses of the major arguments you come across?
Do you agree or disagree with the arguments presented?
An argument involves a claim and supporting reasons to convince others of its validity, as per Hanscomb (2016). Distinguish between fact and opinion, incorporate your perspective, and focus on a specific aspect of the question for precision. This forms the basis for your essay's introduction and conclusion. Go with mostly paraphrase (gives the understanding that you get it) Quote where necessary maximum 10% Dont plagiarise. What you say back it up with proof Referencing.
(n.d.) = no date
(Anon) = No author
(et al.) = and other authors. Used when referring to a source with more than three authors in the main body of the essay, e.g. (Smith et al., 2000)
(cf.) = compare (main body of the essay, only)
When referring to more than one work by a given author and the sources share the same year of publication:
(Smith, 2000a)
(Smith, 2000b)
‘… = ellipsis (used at the beginning of the quotation or the end)
[…] = used to signify that you have omitted part of the quotation, or have added your own words
Go to CiteThemRight
Descriptive writing: Says what happened; reports on findings; explains a theory or idea; gives information; lists details; notes methods used; provides a chronology or timeline of key events; outlines the main points of the key studies.
Analytical Writing: Applies ideas to a different setting; evaluates strengths and weaknesses; draws conclusions; determines the validity of different parts of a study; identifies significance; advances ideas/hypotheses; justifies selection of different options.
0 notes
Text
Peter's lips twisted to one side when the other man spoke about how Ben always had the best stories. "Yeah, he did," he mused. He could still remember being twelve years old and equally entranced and horrified at his uncle's harrowing tale of having saved a junior electrician's life.
"Alan, he just onboarded with us three months ago but he's got ten years' experience, so he knows what he's doing… but today could've been his last. He wasn't wearing gloves, got hung up touching a main buss on a 2000a service because his elbow happened to glance it, and the bucket had a short from the knife to the can. Mark saw as it was happening, but Richie was closer and he just ran straight at him, full speed, to knock him off, hard hat down like he was Ray Lewis. Then Mark, Richie, and I all alternated CPR on him for almost a full hour before life flight got to us. He's hanging on, but…"
Peter shook himself out of the memory to refocus his gaze on his alternate, just in time to see his rueful chuckling over the speed of the local cops. It drew a wry smile on the darker-haired Parker. "Yeah, these guys are good. And maybe not my biggest fans, sorry to say, but there's a reason…"
The sudden note about food gave him pause, and suddenly he felt that certain protective streak within rising up. Whether it was a little kid, an old woman, or a fellow Spider-Man, he wasn't about to leave someone out in the cold and hungry if he had the power to change it.
"My place is about five blocks from here," he said. "I've got a shower and a… well, more like a loveseat than a full couch, but it's at least padded and none of the springs have burst through the cushions yet. Dangers of secondhand and all that." He tilted his head, looking the other Parker up and down a little more critically. "You might be a size or so off from me, but I'm sure I've got some fresh clothes you can use. And I can hook you up with a couple slices from Sal's, but let's get you cleaned up so the cops don't keep chasing you around like a bum. C'mon."
He began walking, glancing towards his counterpart as he moved to make sure he fell into step beside him. "What about the under-threads? Need an update? I've got a couple spares. Occupational hazard."
"Damn, I was kinda hoping your Ben was still alive. Mine always told the best stories. Though I didn't know it at the time." It wasn't hard for Peter to admit how much he missed his Uncle Ben. Being so far away from home only made him miss Aunt May and Mary Jane all that much more.
"I don't need a beast-mode, multiverse-hacking Peter Parker. Just one who believes me and maybe has a couch I crash on while I figure this out. The cops in Central Park put me through the wringer last night. They are surprisingly fast in this universe." A playful little chuckle with a hand rubbing over the back of his neck.
"Honestly the donut joke probably didn't help - " His voice cut off and eyes grew wide. "Food. I wasn't exactly carrying money on me before I got dumped here. What I wouldn't give for a hot meal. And a shower! I don't mean to be begging here...but I'm begging. I'm cold, hungry, and dirty. I can't figure out what I need to do what I need to do to get home on an empty stomach and running from the Central Park police."
#alwaysxinxtrouble#peter parker 1610#muse: peter parker#{ peters gotta stick together! }#{ easy enough when they already come sticky... }
6 notes
·
View notes
Text
Repaired Electrical Equipment Can Be Safe, Reliable and Sustainable

Just about every product in the world has two main requests one for new product, and a alternate request for used occasionally appertained to as fat, repaired, rebuilt or remanufactured product. buses, computers, jewelry, and electronics are just a many exemplifications of thriving diligence that trade in used goods. The marketable and artificial electrical force requests are no exception. Electrical outfit, like motorcars and artificial ministry, are designed to last decades. still, like other durable goods, electrical outfit can be dangerous to the inexperienced whether it's new or habituated product. The convergence of these two data means that product safety not just vacuity is critical to a healthy electrical business. In 1908, the National Association of Electrical Distributors was formed to" establish the electrical distributor as an essential force in the electrical assiduity and frugality," followed by the National Electrical Manufacturer's Association( NEMA) in 1926. These venerable associations ultimately expanded to include educational programs and norms to help ameliorate the operations and safety of the electrical force chain with a focus on new product from electrical Original Equipment Manufacturers( OEMs). During the coming 50 times, two other associations surfaced to help service the used and installed base of electrical outfit. The Electrical Apparatus Service Association( EASA) concentrated on rewinding norms for electric motors, while the InterNational Electrical Testing Association( NETA) offered guidance, education, and instrument for field- testing electrical outfit. But it was not until 1996 that a group of independent electrical distributors joined forces to promote the revamping of artificial electrical product. The Professional Electrical Apparatus Recyclers League( PEARL) is the only trade association that offers specialized revamping norms for artificial electrical product, a law of ethics, ongoing education, point and technician instrument, and stylish practices. moment, PEARL's commercial class has grown to further than 70 independent electrical resellers with earnings in excess of$ 500 million each time. Why Do We Need habituated Electrical Equipment? Why does a secondary, or" out of channel" request for electrical outfit live? It exists for the same reason that electrical OEMs and noncommercial distributors live- force and demand. Consider a manufacturing factory that has a failed element in a critical electrical service. A new relief element isn't available from the manufacturer and distributors for weeks, months, or worse, not at all. So what's the factory to do? How about the power generating station that distributes electricity through a stretch- but impeccably serviceable- 15kv switchgear erected in 1959. The station needs to upgrade their integral tie swell from 2000A to 3000A to keep up with raising demand. The most cost effective( and practical) way to upgrade the service is to replace the tie swell with one of analogous stretch and design, but with the advanced current standing. Unfortunately, primary force channels stopped grazing this product 30 times agone . What about the new office structure that's falling further and further behind schedule staying for a certain size and type of conduit or conduit fittings, only to discover weeks past the original delivery date that the material is on backorder with no estimated time of delivery? Each of these cases represents need- it- now demand for electrical products-critical demand from the guests' perspectives. Enter the secondary electrical force house. They have acquired and housed hard- to- find electrical product for just these types of situation. still, indeed when the relief element is located, the question remains How safe is the relief? The only way to answer the" safety" question is to validate the element through acceptance testing, and when necessary, doctor the element to meet or exceed the product's original performance specifications, or upgrade the element with newer technologies that exceed the original specification.
0 notes
Text
I have asked my medical professionals in my life what is best for me. And what is best for me is to acknowledge my parts as both parts of me and people.
Here’s a section from the official ISSTD treatment guidelines.

Rewritten below, with bolded emphasis mine:
Many terms have been developed to describe the DID patient's subjective sense of self-states or identities. These include personality, personality state, self-state, disaggregate self-state, alter, alter personality, alternate iden-tity, part, part of the mind, part of the self, dissociative part of the personality, and entity, among others (see Van der Hart & Dorahy, 2009). Because the DSM-IV-TR (American Psychiatric Association, 2000a) uses the term alternate identity, this term is used in the Guidelines for consistency.
Clinicians should attend to the unique, personal language with which DID patients characterize their alternate identities. Patients commonly refer to themselves as having parts, parts inside, aspects, facets, ways of being, voices, multiples, selves, ages of me, people, persons, individuals, spirits, demons, others, and so on. It can be helpful to use the terms that patients use to refer to their identities unless the use of these terms is not in line with therapeutic recommendations and/or, in the clinician's judgment, certain terms would reinforce a belief that the alternate identities are separate people or persons rather than a single human being with subjectively divided self-aspects.
Simply put: clinicians agree that whatever language the individual uses is what is best to use, so long as they can still recognize at the end of the day that they are a single human being with subjective self-aspects. As in, it is not a fact that they are simply divided self-aspects; that is based on opinion.
So long as the individual can recognize system accountability (the idea that all parts of a system are viewed as one person in the wider scheme of things, and thus the system must be accountable of all their actions as one unit), so long as they can recognize they only have one physical body, then fuck it, use whatever language you want.
For our system, thinking of ourselves as strictly and only parts of a whole isn’t enough for healing. If helped us, yes, but what helped most was recognizing we are simply parts while also recognizing our individual personhood. Acknowledging our personhood helped us to lower barriers between ourselves, as we didn’t need to keep as rigid a structure to fulfill our “roles” if we were unique people with unique lives. People don’t exist for their jobs — just like how we exist for more than the survival mechanism we were split for.
And at the end of the day, it’s not up to you to decide the language people use. You are not a psychiatrist yourself. If we stick to a strictly medical view, you have no say over this at all. The ISSTD quite literally dictates it’s up to the individual.
Lastly; if you’re who I think you are, I saw the conversation you’re discussing. The majority of those systems you spoke with have CDDs (complex dissociative disorders). Not just “endogenics” believe this. That’s because it’s literally spelled out in the ISSTD treatment guidelines, so CDD systems who care about the actual medical discussions will get up in arms when someone comes into the chat and says, “every alter is their own person , not even parts of a whole (talking about DIDOSDD) is just infact wrong.” Particularly when many individuals have benefited a lot from recognizing the personhood of their parts.
Why are most Endogenics misinformed about DID and OSDD?
This is a question to Anti-Endos , but Pro can also answear
We now often saw and realized that Endogenics belive DID and OSDD Alters are their own invidiuals and don't let themselfes get convinced otherwhise
We thought that there aren't many of those Endogenics , but it seems to be more than i thought. It can be really bad for people with DID and OSDD because this belief can simply worsen barriers , we shouln't need to show proof to prove this belief is bad.
You can ask any Psychatrist , the belief that Alters are their own invidiual worsens barriers , this is why for recovery the knowlege that they are parts of a whole is needed.
35 notes
·
View notes
Text
the idea of Correct Scientific Terminology when it comes to “what do we call multiple people in one body” is kinda funny
cause like yeah, the most consensus you’re gonna get is “alter” but...
Many terms have been developed to describe the DID patient’s subjective sense of self-states or identities. These include personality, personality state, self-state, disaggregate self-state, alter, alter personality, alternate identity, part, part of the mind, part of the self, dissociative part of the personality, and entity, among others (see Van der Hart & Dorahy, 2009). Because the DSM–IV–TR (American Psychiatric Association, 2000a) uses the term alternate identity, this term is used in the Guidelines for consistency.
gOD
- Ace
#and 'among others' includes a LOT OF OTHERS#remember 'subpersonality components' lmao#also 'correct terminology' is kinda funny#there's correct as in 'saying this suggests you're getting your information from correct sources'#but correct as in 'objectively correct' is...#bipolar isn't more Objectively Correct than manic-depression#shrug
11 notes
·
View notes
Text
Endocannabinoids
Endocannabinoids
The existence of specific receptors in mammalian cells that recognize a plant-derived substance rekindled the question raised two decades earlier, after brain receptors for morphine had been first described, i.e., is there an endogenous ligand? A positive answer was provided in 1992 by the report by Devane et al. describing the isolation from porcine brain of the lipid arachidonoyl ethanolamide, named anandamide, which bound to the brain cannabinoid receptor with reasonably high affinity and mimicked the behavioral actions of THC when injected into rodents (Devane et al., 1992). Three years later a second endocannabinoid, 2-arachidonoylglycerol (2-AG), was discovered independently by Mechoulam et al. (1995) and Sugiura et al. (1995). Since then, a number of related endogenous lipids with endocannabinoid-like activity have been reported (Fig. 1c), but follow-up studies about biosynthesis, cellular transport, metabolism, and biological function have focused on anandamide and 2-AG, with much less information available about the other compounds with endocannabinoid-like properties. The biochemical aspects of endocannabinoids have been recently reviewed by Bisogno et al. (2005).Anandamide is a partial or full agonist of CB1 receptors, depending on the tissue and biological response measured. Although it also binds CB2 receptors, it has very low efficacy and may act as an antagonist (Gonsiorek et al., 2000). The in vivo biosynthesis of anandamide (Fig. 4) is believed to occur through the enzymatic hydrolysis catalyzed by a phospholipase D of a membrane lipid precursor, N-arachidonoyl phosphatidylethanolamide (NAPE) (Schmid et al., 1983), which itself is generated by the enzymatic transfer of arachidonic acid in the sn-1 position in phosphatidylcholine to the amide group of PE (Di Marzo et al., 1994; Cadas et al., 1997). Although a specific transacylase for the latter reaction has not yet been identified, a NAPE-specific PLD has recently been cloned (Okamoto et al., 2004). It is not yet known, however, whether NAPE-PLD is obligatory for the biosynthesis of anandamide, which could make it an attractive target of drug therapy when reduction of tissue anandamide would be of benefit. Indeed, there may be parallel pathways for the generation of anandamide from NAPE. A secretory PLA2 that can catalyze the hydrolysis of N-acyl-PE to N-acyl-lysoPE, which is then acted on by a lysoPLD to generate N-acyl-ethanolamides, including anandamide, was recently identified in the stomach (Sun et al., 2004). An alternative parallel pathway has been identified in our laboratory in RAW246.7 macrophages. This involves hydrolysis of NAPE to phosphoanandamide by a PLC, followed by dephosphorylation through a phosphatase (Liu et al., 2006). This latter pathway rather than PLD is the target of regulation by bacterial endotoxin, which increases anandamide synthesis in macrophages (Varga et al., 1998; Liu et al., 2003a). The existence of this pathway may also account for the recent finding that anandamide tissue levels are unchanged in NAPE-PLD knockout compared with wild-type mice (Leung et al., 2006).Fig. 4Schematic representation of the endocannabinoid system in pre- and postsynaptic neurons. The presynaptic terminal is located in the top, whereas the postsynaptic neuron is located in the bottom. EMT, endocannabinoid membrane transporter; MAGL, monoacylglyceride...2-AG is generated from diacylglycerol (DAG) by DAG lipase selective for the sn-1 position (Fig. 4). DAG, an intracellular second messenger that activates protein kinase C, can be generated from phosphoinositides by a phosphoinositide-specific PLC or from phosphatidic acid by phosphatidic acid phosphohydrolase (Bisogno et al., 2005). Two DAG lipase isozymes, α and β, have been cloned (Bisogno et al., 2003). In the adult brain they are localized in the postsynaptic plasma membrane, in line with their putative role in generating 2-AG involved in retrograde transmission.Basal levels of 2-AG in the brain are approximately 2 orders of magnitude higher than the levels of anandamide. Despite this, stimulus-induced release resulting in detectable extracellular levels could be demonstrated only for anandamide and not for 2-AG in an in vivo microdialysis study (Giuffrida et al., 1999). This finding illustrates that, despite growing interest in endocannabinoids and their roles as retrograde neurotransmitters (Wilson and Nicoll, 2002; Chevaleyre et al., 2006), the mechanism of their release is not well understood. Like prostanoids, endocannabinoids are not stored but generated on demand in response to a depolarization-induced rise in intracellular calcium or activation of various metabotropic receptors (Varma et al., 2001; Kim et al., 2002; Witting et al., 2004; Di et al., 2005a,b). A putative membrane endocannabinoid transporter involved in the cellular uptake of endocannabinoids (see below) may also be involved in their release. This is suggested by the ability of a transport inhibitor to prevent the release of intracellularly applied anandamide (Maccarrone et al., 2000a; Gerdeman et al., 2002).Anandamide present in the extracellular space is accumulated by neurons and other cells by facilitated diffusion. This process is driven by its transmembrane concentration gradient, is saturable and temperature-dependent, and does not require ATP or sodium ions. Most importantly for the topic of the present review, anandamide uptake is selectively inhibited by a variety of structural analogs, which suggests the existence of a saturable cellular component involved in anandamide transport (Beltramo et al., 1997; Bisogno et al., 1997; Hillard and Jarrahian, 2000; Maccarrone et al., 2000a). However, a specific anandamide transporter protein has yet to be cloned, and it has been proposed that intracellular degradation of anandamide by fatty acid amide hydrolase (FAAH) is sufficient to account for anandamide uptake in long incubation periods (Glaser et al., 2003). Studies with cells isolated from FAAH+/+ and FAAH−/− mice did not resolve this issue, as the absence of FAAH was found not to affect anandamide uptake (Fegley et al., 2004) or to reduce it substantially (Ortega-Gutierrez et al., 2004), albeit under different experimental conditions. Nevertheless, a FAAH-independent component of anandamide uptake, inhibited by the compound UCM707, was detected in the latter study, supporting the notion of a protein other than FAAH being involved. This notion is also supported by the emergence of a number of synthetic transport inhibitors, the potencies of which to inhibit anandamide uptake does not correlate with their affinities for CB1, CB2, or TRPV1 receptors or their potencies to inhibit FAAH (Fig. 3). However, in view of the important role of FAAH in generating the transmembrane concentration gradient for anandamide, the possibility that a noncatalytic region of FAAH or a FAAH-associated protein may act as anandamide transporter cannot be excluded. Interestingly, the elucidation of the crystal structure of FAAH revealed several channel-like regions in the enzyme, granting it simultaneous access to both the cytosolic and membrane domains (Bracey et al., 2002). Against this possibility, however, is the recent report that the novel, high affinity anandamide transport inhibitor LY2318912 binds with similar Kd and bmax values to membranes from HeLa cells devoid of FAAH or transfected with FAAH, pointing to a binding site independent of the FAAH molecule (Moore et al., 2005). Arguments for and against the existence of a bidirectional anandamide transporter have been recently reviewed (Hillard and Jarrahian, 2003; Fowler et al., 2004; Mc-Farland and Barker, 2004; Glaser et al., 2005).Fig. 3The structure and pharmacological specificity of inhibitors of FAAH and of endocannabinoid membrane transport.In some in vivo studies, treatment with transport inhibitors unmasked cannabinoid-like tonic effects on pain sensitivity, anxiety-like behaviors, locomotor activity, and muscle spasticity, which is an indication of the potential therapeutic usefulness of such compounds (Moore et al., 2005; Bortolato et al., 2006; La Rana et al., 2006). Similar and more pronounced effects have been reported in response to treatment with FAAH inhibitors, as discussed below.In contrast to the unsettled status of anandamide transport and a putative transporter protein, the unique role of FAAH in the in vivo degradation of anandamide has been extensively documented (reviewed inMcKinney and Cravatt, 2005). Initial evidence for a membrane-associated enzyme in the liver that hydrolyzes N-N-acyl ethanolamides (Schmid et al., 1985) was followed by the cloning of FAAH (Cravatt et al., 1996) and the identification of its crystal structure in complex with an active site-directed inhibitor (Bracey et al., 2002). The unique role of FAAH in terminating signaling by anandamide was indicated by the phenotype of FAAH knockout mice, which displayed 10 to 15 times elevated levels of anandamide across the brain, supersensitivity to the actions of exogenous anandamide, and the appearance of tonic signaling by endogenous anandamide, resulting in CB1 receptor-mediated hypoalgesia (Cravatt et al., 2001; Lichtman et al., 2004b), reduced anxiety (Kathuria et al., 2003), antidepressant activity (Gobbi et al., 2006), and lowering of blood pressure in different models of experimental hypertension (Bátkai et al., 2004b). Cravatt et al. (2004) were able to resolve the relative roles of central versus peripheral fatty acid amides by generating mice deficient in FAAH in peripheral tissues only. These mice did not display the hypoalgesia observed in mice with global deficiency in FAAH, but had a similar anti-inflammatory phenotype, indicating that the latter was mediated by elevated fatty acid amides in peripheral tissues (Cravatt et al., 2004). Interestingly, another amidohydrolase catalyzing the same reaction as FAAH but at acidic pH was recently identified and cloned (Tsuboi et al., 2005). This lysosomal enzyme is structurally unrelated to FAAH and is widely distributed in tissues, with highest levels in the lung, and has been recently shown to contribute to the physiological degradation of anandamide in macrophages but not in the brain (Sun et al., 2005).Although 2-AG is also hydrolyzed by FAAH under in vitro conditions (Goparaju et al., 1998; Lang et al., 1999), in vivo it is not a substrate of FAAH, as indicated by the unchanged brain levels of 2-AG in wild-type and FAAH−/− mice (Osei-Hyiaman et al., 2005a). 2-AG is hydrolyzed in vivo by a monoacylglyceride lipase (MGL) (Dinh et al., 2002a,b; Saario et al., 2004). A study of the ultrastructural distribution of FAAH and MGL revealed that in the hippocampus, cerebellum, and amygdala, FAAH is located postsynaptically, whereas MGL is localized in presynaptic axon terminals, including terminals of GABAergic interneurons (Gulyas et al., 2004). Correspondingly, functional studies in hippocampus indicate that depolarization-induced suppression of inhibition (DSI) is unaffected by pharmacological blockade of FAAH (Kim and Alger, 2004), but it is potentiated by blocking MGL (Kim and Alger, 2004; Makara et al., 2005), in agreement with an earlier study implicating 2-AG rather than anandamide in synaptic plasticity in the hippocampus (Stella et al., 1997). Further evidence supporting the role of 2-AG as the retrograde transmitter involved in synaptic plasticity is the preferential postsynaptic distribution of the major 2-AG biosynthetic enzyme, diacylglycerol lipase α, in hippocampus and cerebellum (Katona et al., 2006;Yoshida et al., 2006).However, the behavioral consequences of DSI and its modulation remain unclear: selective knockout of CB1 receptors from GABAergic interneurons was found to abolish DSI and long-term depression (LTD) of inhibitory synapses, whereas the classic behavioral responses to THC remained unaffected in these animals (Monory et al., 2005). Therefore, at this point it is difficult to predict the potential therapeutic usefulness of selective MGL inhibitors. http://www.ncbi.nlm.nih.gov/pmc/art...
0 notes