As much as I love my life, I also care about my level of function🌼🎈
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by love-pauletta and here's what we found interesting.
Average Info
Notes Per Post
1
Likes Per Post
1
Reblog Per Post
0
Reply Per Post
0
Time Between Posts
2 months
Number of Posts By Type
Text
12
Last Seen Tumblr Blogs




Fun Fact
The total number of visits Tumblr.com received during January 2021 is 327 million.
Text
“To my mind, the greatest reward and luxury of travel is to be able to experience everyday things as if for the first time, to be in a position in which almost nothing is so familiar is taken for granted” – this quote was said by Bill Bryson who is an American–British author of books on travel. When I read about him on Wikipedia I thought that he probably said these words when he was traveling for the book he published called I’m a Stranger Here Myself. Community Block provided me with the greatest satisfaction and pleasure of travel by allowing me to experience things for the first time. I wasn't simply enjoying the experience of visiting another community; I was also fully immersed in the current moment of everything that was presented to me, and I found myself in a situation where absolutely nothing felt familiar. NO, it wasn't because I was in a different community impacted by other circumstances than the one in which I am/was born. However, because community block was a DIFFERENT block, it tested my knowledge and abilities gained during my years as an undergraduate working in hospitals.

Before I started this block, I had a preconceived notion that it would be difficult, as most of the students reported. However, I realized that they lacked understanding and that it was a unique block in that it required a different type of critical thinking that required you to step outside of your comfort zone. A shift in perspective was needed, and I'm glad I got it, which was DIFFICULT to DIFFERENT: this came with the understanding that whenever we see an opportunity for change and it appears to be difficult or may be difficult, we often shy away from it because we're afraid of the challenges, of being challenged, and of being out of our comfort zone. The reason I say this is because we were moved from a hospital setting where you only interact with clients in the same setting/environment, which is the hospital, to a community setting where we got to interact with clients in their community, where we explored their home environments and physically came to assess and also interacted with people in the community. One of the things I discovered about people while in this block, particularly from the neighbourhood where I was placed at Inanda, is that once they're given the chance to change, such as by having access to health care resources, they take advantage of it and they tend to reject the opportunity. Why? Because they are afraid of taking the necessary measures, of encountering difficulties, and of failing to be consistent, which may be due to social or family issues.
When (van Stormbroek & Buchanan, 2021) reported on the challenges which are normally faced in community practice he mentioned that “Challenges include’ working with limited resources, language barriers and a patient population faced with costly travel to health care” and these are the same issues we had at Inanda, which made confronting the community's needs challenging and daunting, but it didn't deter us because it motivated us to want to make a difference. Instead of an MDT, we had to learn to work with CCGs, youth mentors, other community or out-of-community clinics, and hospitals to follow up and assure proper treatment delivery. This challenged my thinking, and in the way I generally provide therapy, where all resources are available, needing to problem solve by improvising and being innovative was one of the skills I needed to improve. These challenges led to the introduction of the terms "positionality" and "social location," and an understanding of them made it easier to understand the community better, particularly in terms of its own social location/positionality and how it differs from mine, understanding it and gaining a holistic view of the community, as well as the intervention approach to the community and its members as (Jacobson & Mustafa, 2019), looking at researchers, states that “Understanding our position, particularly in comparison to the social position of our participants, helps us to better understand the power relations imbued in our research and provides an opportunity to be reflexive about how to address this” which also applied in my situation at the community.
This stumbling block forced us to expand our understanding of advocacy beyond what we had been taught, doing, and calling advocacy, which only worked in the contexts we were in ( the hospital). We learned that advocacy demands you, as a therapist, to be strategic in your approach by working with the few resources you have in the community and making them available in sufficient quantities for the patient or community to obtain the treatment they require. Because now you have to be out of your comfort zone, you need to feel the adrenaline and its up to you whether you use it off positively by taking a stand and facing the authorities to ensure proper delivery of treatment. In study of (Jansen van Vuuren et al., 2021) their findings indicated that “highlight the importance of advocacy as a crucial role for African occupational therapy practice, particularly in contexts where there are chronic issues of poverty, violence, social inequality, stigma, and limited resources, and that it should be through education, empowerment, and support, and decreasing stigma through role modelling justice, inclusion, and tolerance. Empowering women, looking at maternal and child health, doing health promotion Advocating “with the aim of facilitating and developing programs and transferring knowledge and skills to community members, educational programs to incorporate CBR skill development, including skills in program development, evaluation and management, particularly through practice placements in local community settings, to ensure therapists are knowledgeable and competent in CBR practice approaches” (Jansen van Vuuren et al., 2021) transferring skills to the CCGs, nurses at the clinic and the youth mentors. One of the difficulties we had especially in advocating for the park we utilize to run our services was the resistance caused by vandalism happening as well as removal of containers, these affected our emotions and made us worry for the future of the community. However, we learnt to put our emotions aside so that it doesn’t influence the spirit we put out in the community and our energy during treatment. WE USED THE RESISTANE GOING IN THE PARK AS THE PRECURSOR FOR PERSISTENCE. Which kept us consistent in advocating for our profession and the community’s health.
“To be effective in delivering within a PHC service, occupational therapists (OTs) have to re-evaluate the models used for practice in the community. They need to refocus their efforts on enabling greater participation for PWDs in daily activities despite their experiences of physical, socio-political and psychological barrier” as stated by (Naidoo et al., 2017). This is the difference and uniqueness this block came with which made the experience so unfamiliar yet understandable and insightful.
References
Jacobson, D., & Mustafa, N. (2019). Social Identity Map: A Reflexivity Tool for Practicing Explicit Positionality in Critical Qualitative Research. International Journal Of Qualitative Methods, 18, 160940691987007. https://doi.org/10.1177/1609406919870075
Jansen van Vuuren, J., Okyere, C., & Aldersey, H. (2021). The role of Occupational Therapy in Africa: A scoping review. Retrieved 22 October 2021, from.
Naidoo, D., Van Wyk, J., & Joubert, R. (2017). Community stakeholders’ perspectives on the role of occupational therapy in primary healthcare: Implications for practice. African Journal Of Disability, 6. https://doi.org/10.4102/ajod.v6i0.255
van Stormbroek, K., & Buchanan, H. (2021). Community Service Occupational Therapists: thriving or just surviving?. Retrieved 22 October 2021, from.
0 notes
Text
“THE SOLUTION WE WANT IS TO BE C0-CREATED BY US”

As I continue down this block, I reflect not only about my own positionality, but also about how I may work around it to accommodate the people in this community. I've been wondering if we're even on the right track to reaching all of our goals for the communities where we're placed; nevertheless, asking several questions won't help; my role is solution-focused, working with and for the community. Giving me a platform to delve deeper into these goals and try to set direction through sustainable development goals will be beneficial for the rest of my time here. Now the question is; HOW CAN WE MAKE THESE GOALS A REALITY?
One of the biggest challenges I've encountered in the community is the high rate of adolescent pregnancy and HIV/AIDS infections among the youth. One of the young people I met was 13 years old and had recently tested positive for HIV; fortunately, I had the opportunity to meet her with the youth mentor. I could tell that this sudden transition in her life was affecting her mental health because she was in a depressed state and didn't want to share her experience. According to family members, she has been having unprotected intercourse with old men, has been exposed to alcohol, and would not sleep at home for more than three days. She claimed it wasn't due to peer pressure, but because it was our first encounter that day and we hadn't established a rapport, she wasn't eager to reveal more. Then I wondered why such a young, lovely girl would put herself in this situation. According to (ODO et al., 2018) “the sexual and reproductive health needs of adolescents are often underserved in many societies yet adolescents constitute large proportion of the population” and “are characterized by series of physiological, psychological and social changes that expose them to unhealthy sexual behaviour such as early sex experimentation, unsafe sex and multiple sexual partners” which is evident at Inanda community because there are less services provided for the youth and they are not educated on the long-term effects . Therefore one of the sustainable developmental goals I’m intending to work on are SDG 5 gender equality and SDG 3 promoting good health and well-being by providing education amongst the youth by having a programme recruiting adolescents from high school especially in lower grades (grade 8), doing health promotions in these schools, making videos and send them on the school WhatsApp group , improve awareness of the services provided at the clinic so that women can have autonomy and right to decision making over their health, provide mental health intervention for those who are exposed to teenage pregnancy, HIV/AIDS infected and carrying the burden of social issues and family dynamics.

With such rapid population growth, health services are in significant demand; nevertheless, fewer people are taking advantage of these services. Because most members of the community have difficulty accessing health care services, in addition to distance and transportation, they also have poor financial management and budgeting skills, which limit their capacity to save money for transportation to these facilities. Aside from low skills, the majority of the population is unemployed, unable to support for their family; some receive grants, while others do not owing to social concerns; all of these factors point to inequality. To reduce these inequalities (Siongco et al., 2020) states that “Promoting fair financing and better health access across LMICs is necessary, as equitable access to healthcare services is a major public health challenge.”, However, because they are receiving free services at the CHC, financing is not an area of concern; however, encouraging and educating the mothers and older members of the community on financial management, particularly during health promotion speeches at the clinic by encouraging budgeting, would be beneficial. Working with CCGs to reach out to the poorer population in the community and working with youth mentors to encourage them to target the unemployed young in the community to participate in the programs they have and to refer them to us, as the population grows (student OTs).
“The health of humans and the environment is in jeopardy. The (SDGs) of the United Nations (UN) set out goals for conserving the planet and improving quality of life by 2030, including a target to ensure everyone's health and well-being” (Salvo et al., 2021). The use of recreational areas has become one of the mediums used to provide therapy and allow for increased community occupational engagement as (Manning, 2014) states that “Parks and protected areas are becoming increasingly important, they offer open, green spaces in our ever-developing world, they are retreats from the hectic lives that many of us lead and they protect wildlife and other elements of biodiversity, as well as historical and cultural resources that are important markers of society” which is what we’ve also observed at Inanda Seminary park as they provided with green space, retreats the lives of the members of the community by the help of OTs. However, because of Covid-19 and other political factors, there have been numerous debates around it, and it is in risk of being closed. Because of the park's inadequate utilization, this could result in deforestation and land degradation. Improving SDG 5 gender equality and promoting SDG 3 good health and well-being through park use (providing services at the park and encouraging gardening among the elderly, which will benefit their families financially and health-wise by reducing undernutrition) will help to increase the park's significance as well as its use. This will assist achieve SDG 15 Life on Land by restoring the ecology, gardening, and restoring the park's greenhouse, as well as fixing garden beds to encourage gardening (Protect, restore and promote sustainable use of terrestrial ecosystems, sustainably manage forests, combat desertification, and halt and reverse land degradation and halt biodiversity loss).
Peace, justice and strong institutions SDG 16 which includes “Promoting peaceful and inclusive societies for sustainable development, provide access to justice for all and build effective, accountable and inclusive institutions at all levels” goes hand in hand with SDG 5 and SDG 10 , by improving and achieving these goals we will be promoting peace within the community, and promoting access to Justice, as states that “SDG integration and interdependence are critical for advancement and successful implementation of individual and collective SDGs. Integration refers to each SDG viewed in the context of the other SDGs, i.e., not in isolation. “ I will also work on these goals interdependently and integrated because “An exclusive focus on a specific SDG without considering the other SDGs will constrain progress” as stated by (Cerf, 2019)

References
Cerf, M. (2019). Sustainable Development Goal Integration, Interdependence, and Implementation: the Environment–Economic–Health Nexus and Universal Health Coverage. Global Challenges, 3(9), 1900021. https://doi.org/10.1002/gch2.201900021
Manning, R. (2014). Research to guide management of outdoor recreation and tourism in parks and protected areas. Koedoe, 56(2). https://doi.org/10.4102/koedoe.v56i2.1159
ODO, A., SAMUEL, E., NWAGU, E., NNAMANI, P., & ATAMA, C. (2018). Sexual and reproductive health services (SRHS) for adolescents in Enugu state, Nigeria: a mixed methods approach. BMC Health Services Research, 18(1). https://doi.org/10.1186/s12913-017-2779-x
Salvo, D., Garcia, L., Reis, R., Stankov, I., Goel, R., & Schipperijn, J. et al. (2021). Physical Activity Promotion and the United Nations Sustainable Development Goals: Building Synergies to Maximize Impact. Journal Of Physical Activity And Health, 1-18. https://doi.org/10.1123/jpah.2021-0413
Siongco, K., Nakamura, K., & Seino, K. (2020). Reduction in inequalities in health insurance coverage and healthcare utilization among older adults in the Philippines after mandatory national health insurance coverage: trend analysis for 2003–2017. Environmental Health And Preventive Medicine, 25(1). https://doi.org/10.1186/s12199-020-00854-9
0 notes
Text
Positionality In research, why not in community health care workers?
Have you ever been deep in thought, reflecting about a circumstance in which you reacted and addressed it differently than everyone else who was also exposed to the same situation with you? Have you ever pondered why you reacted the way you did, or why you approached the situation differently than others? And what were the underlying influences and factors that led to that particular reaction? If you haven't already done so, consider your environment and the people you live with. What causes you and them to respond or approach situations in the same way? And if you've found yourself in this circumstance, it's important to go further and figure out what's causing these unusual reactions/approaches, as they may have an impact on your judgement.
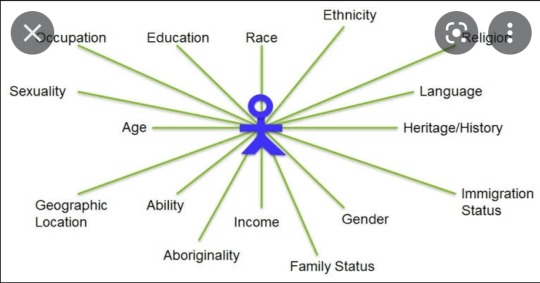
Positionality have been thoroughly evaluated and described in research qualitative studies where (Secules et al., 2021) describes it as how a person's socially significant identity characteristics define him or her in a dynamic manner and continues to say that it has been defined as reflexivity, which is the process by which a researcher recognizes, evaluates, and owns their own origins, viewpoints, experiences, and biases in order to improve study quality. This further means, especially out of context of research, examining your own feelings, reactions, and motives and how they influence what you do or think in situations. Class, citizenship, ability, age, race, sexual orientation, cis/trans status, are just a few of the many dimensions that make up our social identities. Age, gender, sexuality, color, social class, culture, religion, and other factors all influence how we see and interpret the world around us, as well as how the world perceives and interprets us as stated by (Jacobson and Mustafa, 2019).
Whenever I'm in a situation, one of the things I've discovered about myself is that the way I perceive, interpret, and choose to react to a situation is heavily influenced by a variety of elements, including culture, religion, race, and the other factors described above. I wouldn't consider myself as a religious woman just because I am a woman who grew up in a very religious family (Christian) that acknowledges its culture but does not follow cultural beliefs and rituals. However, growing up in a family like that has influenced my judgment and the way I perceive situations. However, my age (21), gender (female), and sexuality (LGBTQI+) have a strong influence on how I react to and handle situations as well. And the setting I grew up in, a township known as "lokshin," played a significant effect, particularly in terms of cultural norms, the types of crimes I was exposed to, and the township's views. Now that I'm in the community block and thinking about my role as an occupational therapy student, I'm starting to question my positionality. Positionality is important in social work because it determines how one conducts client work, community participation, and decision-making. As a result, I'm starting to evaluate myself whenever I have to do a home visit, conduct assessments, exposed to severe home/diagnoses related problems or provide intervention etc.
The community I am placed in is also a township, it connects with my hometown as they share the same challenges, I have had no difficulty understanding the settings, contextual factors such as informal settlements that are seen within this community, its culture, religions, and other factors such as race of the people in the community as all of this is quite similar to my hometown. When (Berkovic, Ayton, Briggs and Ackerman, 2020) conducted a research on one of the topics they have a lived experience on, they were referred to as a “research insider”, and they noticed the advantages and disadvantages of this which raised a concern to me as it sort of applies to my situation as well. I have an understanding of these people and the factors that create them and factors which come as challenges, I understand them on a personal level which places me as an insider when providing intervention. (Berkovic, Ayton, Briggs and Ackerman, 2020) states that an insider position’s advantages, include facilitating a clear perspective that creates credibility with people, “promoting an equalized connection between the researcher and the participants, and fostering rapport between the researcher and the participants.” Which are one of the advantages I have also noted since I have began working in this community. However, disadvantages such as participants' misunderstanding of a researcher's ability to provide health advice, as well as compromised researcher objectivity and professionalism haven’t been noted while I’m at the community. (Saidin, 2017) also suggested that the insider researcher's comparable background to the participants could sway his readings of the findings in his study causing them to be biased because of the great impact of his prior experiences with the topic, as opposed to an outsider researcher who has no prior knowledge of the topic. These are on the challenges I am not willing to face as they may place my intervention at risk and to be bias.

Just as researcher’s positionality in qualitative research is questioned and evaluated, it is quite significant to also evaluate positionality of community-based health practitioners. As (Holmes, 2020) state that it has an impact on how research is conducted, as well as the outputs and outcomes, this also applies to the health practitioners working with communities, their positionality will have an impact on how intervention is conducted/planned as well as the outcomes of intervention. Therefore, it is quite significant to have reflexivity as a community health-worker, as It has the potential to guide our thinking so that we may better adapt to complicated and contextually placed health challenges, as well as unanticipated circumstances in health promotion practice that cannot be predicted through formal training (Alexander et al., 2020).
REFERENCES
Secules, S., McCall, C., Mejia, J., Beebe, C., Masters, A., L. Sánchez‐Peña, M. and Svyantek, M., 2021. Positionality practices and dimensions of impact on equity research: A collaborative inquiry and call to the community. Journal of Engineering Education, 110(1), pp.19-43.
Jacobson, D. and Mustafa, N., 2019. Social Identity Map: A Reflexivity Tool for Practicing Explicit Positionality in Critical Qualitative Research. International Journal of Qualitative Methods, 18, p.160940691987007.
Berkovic, D., Ayton, D., Briggs, A. and Ackerman, I., 2020. The View From the Inside: Positionality and Insider Research. International Journal of Qualitative Methods, 19, p.160940691990082.
Saidin, K., 2017. INSIDER RESEARCHERS: CHALLENGES & OPPORTUNITIES. Proceedings of the ICECRS, 1(1).
Alexander, S., Jones, C., Tremblay, M., Beaudet, N., Rod, M. and Wright, M., 2020. Reflexivity in Health Promotion: A Typology for Training. Health Promotion Practice, 21(4), pp.499-509.
0 notes
Text
COME ON HEALTH CARE WORKERS!! LET'S CHANGE OUR MINDSET AND ALLOW COMMUNITY DEVELOPMENT
“There is no equality without empowerment. There is no empowerment without knowledge. Our job is to foster the opportunities so that every woman, child and adolescent can own- and demand-their rights” These words were said by the president of the Foundation of Community Development Mrs. Graca Machel, who is also an advocate, Mozambican politician and humanitarian. She did not say these words to make an impression however she applied them in her life from a very young age, living through them as principles, advocating and fostering opportunities for women, children, and adolescents especially in Low-Middle Income Countries (LMIC) for Community Development. A short while after I read up on her on Wikipedia I questioned her dedication, where was it coming from? I also wished that it could be transferred or shared with our current health care workers and organisations that work in rural communities. While I was on that thought I had a realization that she understood that “maternal mortality is not only a health indicator but also a key indicator in the country development as it has social and economic impact” (M. Bauserman, V.R. Thorsten, C. Bose, J. Patterson, 2020), which is the same understanding and knowledge that needs to be instilled to our health care workers.

LMIC have been constantly mentioned in every article I’ve read concerning maternal and child health, and they are reported to have an increase in maternal and child health mortality rate. (M. Bauserman, V.R. Thorsten, C. Bose, J. Patterson, 2020) state that “Maternal mortality disproportionately affects women in LMICs where most of the maternal deaths are from preventable causes, with MMR of 479 for LMICs compared to 41 in high income countries (HICs)”. Looking at these statistics made me realise that our communities are losing out on an important dime that represents the future of our communities, because women and children are the future of our societies. This increased loss of children and women places these communities at high risk of not developing and reaching the full health optimal outcomes and stealing away their rights. When I read on (K.W. le Roux et al, 2020) they acknowledged the poor context and infrastructure of the health care facilities especially in rural areas, where they mentioned that “they are under-resourced, poorly maintained and lack essential medicine” I questioned the role of authorities and organisations that work with the health facilities in rural areas. Why are low-middle income countries disregarded especially when there are tons of research and literature on maternal and child health? Why are they not considered as priority especially women and children in these communities? But then I realised that asking these questions won’t bring any change or provide with a different lens however a better question could be How can we as OT’s assist the members of these communities, how can we improve their quality of life and maintain community development?
Women empowerment used as a catalyst to yield improvement in heath and wellbeing for women and children and for community development is one of the conceptions that should be considered in maternal and child health. And according to (S.K Abreha & Y.A. Zereyesus , 2020) “women's empowerment in developing countries, particularly in South Asia and sub-Saharan African countries, remains low compared to other regions in the world, and this is a barrier to development and human capital formation, it contributes to poor child health and growth”. This is also observed at Inanda community there is less intervention provided for women and children, the staff at the clinic are not skilled and equipped, they are not motivated to implement women empowerment within the community through education. Occupational Therapist use empowerment as an educational process to help clients develop the knowledge, skills, attitudes, and self-awareness required to effectively assume responsibility for their health-related decisions, they help clients change from being passive to being actively involved in their personal health care process. How do they do this? By designing programs and providing services for members of the community especially women using sights such as parks to provide occupation-based therapy however due to COVID-19 some programs are placed on hold and according to (T. Ahmed et al, 2021) “LMICs with poor MNCH indices suggests that current corona restrictions lead to more than 30% additional maternal and new-born deaths due to reduced access to relevant essential services such as family planning, antenatal care (ANC) and adequately supervised community and facility-based deliveries”. And “Up to 20% of women experience perinatal mood disorders (including anxiety) which affect daily function. These numbers have increased dramatically during the Covid-19 pandemic” (C.V. Farewell, J Jewell, J Walls & J.A. Leiferman, 2020)

However it is important to not that even before the onset of COVID-19 there were problems which increased MMR as (K.W. le Roux et al, 2020) reports that “there is scarcity of trained and skilled healthcare workers in rural areas, including doctors, pharmacists and nurses leading to suboptimal health outcomes” this is another challenge we find at Inanda, and it actually makes a lot of sense; firstly because I’ve been exposed to Inanda community and Inanda seminary clinic where there are no skilled and educated health care workers such as speech therapists, social workers, optometrists etc and it’s very hard to access them due to long distances and this limits the chance of community development; secondly it’s because I have gained insight on how health care workers are not motivated to apply for posts in rural areas. As I am doing my final year, we were required to apply for Community Service placements for 2022, and a number of students applied for available posts in urban areas and when you checked on the posts available for hospitals in rural compared to urban they were 3 times more, and then I questioned the rationale behind this. (P agyei-baffour, S.R Kotha, J.C Johnson, & Mawuli Gyakobo, 2011) states “Retaining health staff in rural areas has proven extremely difficult as young professionals increasingly prefer urban postings and health systems do not reward and rural exposure, poor working conditions, low job satisfaction, political and ethnic problems, and sometimes, civil strife and poor security in most underserved areas, predispose new graduates to select cities.”. I honestly understand that perspective however I believe another answer to this it is because they lack this concept and understanding that Mrs. Graca Machel had, which made me realise that HCW are not focused on community development and the importance of women and children, however we’re driven by our intrinsic motivation. If we as health professionals don’t understand the importance and role of women and children in communities, we’ll most definitely won’t see the need to carry all the burden with them.
As I conclude this blog, I come to a realization that the community block that we have in Occupational Therapy at UKZN builds this conception of women empowerment, it instils this understanding that Mrs Graca Machel had by changing our mindset and dive deeper into our scope of practice especially in community practice. I just hope we grasp it, putting our intrinsic motivation aside.

References
C.V. Farewell, J Jewell, J Walls & J.A. Leiferman. (2020). A Mixed-Methods Pilot Study of Perinatal Risk and Resilience During COVID-19. Journal of Primary care and community health, 12.
K.W. le Roux et al, E. A.-K.-B. (2020). Community health workers impact on maternal and child health outcomes in rural South Africa – a non-randomized two-group comparison study. Nature partner Journal, 15.
M. Bauserman, V.R. Thorsten, C. Bose, J. Patterson. (2020). Maternal mortality in six low and lower-middle income countries from 2010 to 2018: risk factors and trends. Reproductive Healt, 10.
M.F.E.Munar, M. T.-V.-G.-Á.-M. (2021). The Effectiveness of Community Occupational Therapy Interventions: A Scoping Review. International Journal of Environmental Research and Public Health, 15.
Meyers, S. (2009). Community practice in Occupational therapy: What is it. In S. Meyers, Community Practice in Occupational therapy: a guide to serving the community (p. 32). LLC: Jones and Barlett Publishers.
P agyei-baffour, S.R Kotha, J.C Johnson, & Mawuli Gyakobo. (2011). Willingness to work in rural areas and the role of intrinsic versus extrinsic professional motivations - A survey of medical students in Ghana. BMC medical education, 11.
S.K Abreha & Y.A. Zereyesus . (2020). Women’s Empowerment and Infant and Child Health Status in Sub-Saharan Africa: A Systematic Review. Maternal and child health journal, 12.
T. Ahmed et al, A. E.-P. (2021). The effect of COVID-19 on maternal newborn and child health (MNCH) services in Bangladesh, Nigeria and South Africa: call for a contextualised pandemic response in LMICs. International Journal for Equity in Health, 15.
Z.S Lassi, R. Kumar, & Z.A Bhutta. (2016). Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, Third Edition (Volume 2). Washington DC: World bank group.
0 notes
Text
" Acceptance is the ability to unconditionally value all parts of who you are. That means you acknowledge all of yourself--the good and the things that need improvement. For most of us, self-acceptance can be hard. We tend to be critical of ourselves, but there are a number of ways to learn to accept yourself and your life. It all begins with your state of mind."

How long did it take for you to accept your roots, the teachings from your parents? How long did it take for you to accept yourself for who you are, accept your true self? It varies for all of us, some people take their whole life, others take half their life, others need validation from their peers to be able to accept themselves, others accepted themselves from when they were little, etc... Personally it was easy for me to accept myself as my behavior is mostly shaped and guided by my roots and the teachings I received from my parents. As my father would say "we all make mistakes but it is important to learn from them and change our thinking as well as behaviors". The way we think also guides our behaviour therefore this is just one of the advices I would give to my future self. "Be mindful of your thoughts, because they can influence your behavior and make your roots". My future self...
One of the things I never wish to neglect are the teachings which I received from my parents especially my father, from when I was little. That man played a huge role in creating and shaping me into the person I am today. I am a proud daughter because I strive every day to adhere to those teachings and live life according to the principles which were presented/introduced to me. However, I don't always get it right, I fumble and fall, and that's okay because we make mistakes and we learn from but I should always remember who I am in whatever situation nor circumstance, I should always remember my roots. "How can you forget your self, your true self? How can you disregard your roots? Go back home black child, to your family and friends, find yourself.", this what I always ask and tell myself whenever I face circumstances that are above my energy and soul, I go back to my roots, family and friends and that's where I gain back my strength and my true self. This is the same thing which happens in my profession Occupational Therapy, according to my experience, sometimes I face challenges whereby I feel like I don't know what I am doing or I don't know what I have to focus on because the client which I'm treating would present with various problems which all affect their function in different ways, which happened during this block. However I would be able to remind myself to not be too hard on myself and go back to my roots and family(which in this case is theory and my supervisors) to be able to guide my thoughts, behaviour, intervention plan and find myself and focus as a therapist. This is the same advice I would give to my future self and as a therapist, that it is okay to make mistakes, fumble and fall but don't forget who you are, don't forget your roots (theory), go back to your mentor and forgive yourself for the mistakes you did in the past.
Additionally, as we grow older we go through various stages and in some of these stages we experience some sort of change or we gain new information which influence our behaviour to change, it is important to allow these changes and accept them and explore more on them and see the effects of these changes into our lives. Meaning there is always new theory established each and every year as the world is changing each and every day therefore it essential to accept this new theory and apply it during treatment, it is essential to to do research now and again to improve your skills and knowledge as a therapist in order to be aware of the changes done in our profession. That is one of the advices I'd give to my future self. This was also emphasized by my supervisor especially in this block, that research, experiential learning and growing our knowledge through others is important. These are important especially when you are treating a different or unusual diagnoses, it is important to see other theorists or therapists perspectives.
"Personal freedom is a state of being where we love ourselves for who we are. We accept ourselves for who we want to be, who we were and where we're headed. Personal freedom is about responding to life rather than reacting. It's about healing your past, loving yourself and doing what's best for you, loving yourself and doing what's best for you and yours. It's about living a life you desire and creating the discipline and desire you want. "
https://www.inc.com/lolly-daskal/how-to-accept-yourself-your-life-your-reality.html#:~:text=Acceptance%20is%20the%20ability%20to,self%2Dacceptance%20can%20be%20hard.
https://pin.it/7EKZiog

0 notes
Text
Look at this... 👀
Look at this... 👀 https://pin.it/1iGEiuc
To stop being shy and begin to confidently show your real character and feelings can be defined as coming out of your nutshell, moving out of your comfort zone not disregarding your values and beliefs but finally accepting and acknowledging your them but most importantly your skills and influence as an individual. However this should be based on your role as an individual and your understanding of the responsibilities that specific role implies, failure to do so may cause problems and lead to one seem like they they do not want to come out of their comfort zone /nutshell, like they don't have skills that specific role require them to have. For example understanding your role in the workplace, according to research "Understanding your role in the workplace is knowing where you fit within the culture of your organization. It is where you will have the best opportunities to directly influence the various areas of your workplace" therefore it is important to have this basic understanding in order to be influential in whatever position you're in and come out of your nutshell.
Yes I wouldn't compare my experience in the Fieldwork block as a student to someone else's experience in a workplace as a qualified Occupational Therapist and say they are similar however the skills which are required in the workplace are similar to the ones which are required and developed in this Fieldwork block. Therefore the experience was quite similar but very challenging as it's been a long time since I've focused on the Psychosocial part, essentially it was difficult to figure out what exactly was required from me especially when I received my client, as it was difficult to know which assessments are appropriate and what to observe for during activities, all of this was due to lack of understanding of my role as an OT in the psychosocial block. However creating rapport with my client and getting a clear holistic overview of him was one of the things which helped my focus of intervention, as well as coming up with appropriate and effective principles of treatment when planning sessions, I noticed some changes in my way of thinking. I was able to utilize my skills during treatment using a client-centered approach as there was noticeable improvement in the client’s level of performance and self awareness, understanding that improving a specific client factor influences the improvement on occupational performance, this helped me realize that understanding your role influences your effectiveness of your services /treatment on your clients which is how I came out of my nutshell.
The feedback I received from my supervisor was based on the effectiveness of therapy as she also observed a lot of improvement from my client, even though she didn't focus more on how I applied my skills as an OT but she emphasized that it quite surprising on how the client improved in 2 weeks which is evident that I did come out of my nutshell and found myself.
covalentcareers.com/resources/6-things-expect-your-first-week-occupational-therapist/
powertools.hh2.com/post/understanding-your-role-in-the-workplace#:~:text=Your%20company%20role%20is%20not,various%20areas%20of%20your%20workplace.
0 notes
Text
*The links for the quotes included in this blog are at the bottom*
COVID COVID COVID!!
The only thing that's been dominating our lives, mental health and our well being since the beginning of this year. Am I tired of it? Hell yea. Do I want it to stop spreading? You don't even have to ask twice and I'm sure the feeling is mutual with you too. Just think about it, how many doors did it close for you? I know right. Yea I agree with you, It should definitely pack its bags and leave!!! But here's a trick question, was it a trick or a treat?
The pandemic has made a lot of modifications in our lives especially our daily routines, our behavior and how we normally conduct certain tasks/the way we do things. It took a hard knock having to adapt to the changes and having to create a new routine that is suitable for our environment as well as our well being. Besides these changes mentioned, which mostly apply in our personal lives, even in the health sectors/hospitals there had to be strict regulations to maintain the work environment and there was zero access to them which made it hard for people to continue with their treatment especially in OT because it required one on one sessions as well as group sessions which are impossible to run because of "social distancing"
"For our residential clients, Functional Life Skills (FLS) staff now provide treatment in group homes that would normally have been provided at our day program/outpatient facility.Staff follow a daily health and safety protocol, including having their temperature checked at the beginning of their shift, monitoring the temperature and O2 saturation level of all clients, and following a strict routine of cleaning equipment and high-touch surfaces"
Having to go through these changes and getting to experience them have been nerve wrecking and it brought up a lot of emotions because I felt like there was little hope for the future, well my future to be quite specific. Not given the chance to go to school, attend lectures and go to prac felt like a punishment, the Virus literally became a threat that I had little power over in fact zero power.
Since we've been back to campus and having pracs my mood has been a little elevated even though it is still quite horrifying but feeling like things are slightly getting back on track bring a little hope. Especially since I was in the group Work block, it was quite difficult choosing appropriate activities which didn't go against the restrictions and maintaining social distancing. At first it didn't feel like it was going to be a good learning experience since we didn't have actual clients to work with however working with my peers was very helpful and improved my insight in a lot of things. I learnt a lot from them especially my partner and a lot of handling techniques as well as communication skills. And to be quite honest, thou the virus brought a lot of negativity, losses and changes, it did come with a lot of benefits, I believe it was a learning experience.
"Being positive isn't pretending that everything is good - it's seeing the good in everything"
Multiple people established a lot of skills/creative skills which they had little insight on and they weren't aware that they had them and some of us we had to learn and adapt in order to survive and complete all we had planned for the year. For example, one of the skills which I obtained through this pandemic were computer based skills through the use of Zoom meetings to attend lectures and a lot of alternatives were introduced to maintain and achieve treatment goals especially in OT like Telehealth.
"As for our outpatient clients, they too receive services via telehealth delivery, both for cognitive and licensed therapies, whether on personal devices or on company-supplied iPads. Family members are typically available to assist with schedule reminders and technology issues."
The point that I'm trying to make out of this is we might have viewed covid 19 as a threat most of the time but maybe it is time we view it in a different perspective and approach it with smart strategies in order to survive because there's a lways a light at the end of the tunnel. It was more of a trick than a treat. Just a matter of adapting to change.
"You can't go back and change the beginning, but you can start where you are and change the ending "
https://pin.it/5qUdxez
https://www.biausa.org/public-affairs/media/how-service-delivery-has-changed-the-effect-of-covid-19-on-occupational-therapy
https://pin.it/3D9yCla
0 notes
Text
NB: the references of each quote written on this blog will be at the bottom of the blog.
I remember when I was doing my second year I used to be a bit confused about how the Multidisciplinary team is organized and how it works. During the beginning of my third year Fieldwork block I started understanding that there is no set of organization in the MDT but one health practitioner should ask for another professional's expertise to help improve the client by planning intervention and achieve the patient's goals. "Several studies found that stuff often lack understanding of their precise roles and responsibilities and/or lack a shared appreciation of the goals and objectives of the Multidisciplinary team." and I think that's what happened to me this week, I became a little confused about my role as an OT in the case which will be discussed in this blog.
My treatment plan was to incorporate the nurses to encourage/motivate the client to engage in activities independently (transfers, bed mob), which I did, as well as recommend that the hospital OT ensures continuity of the routine we created with the client, which I also did. But then I realized that even though my client have been told by every member of the MDT that she'll never be able to walk again she still haven't accepted her condition (paraplegia), her culture and family play a huge role in giving her hope that she might walk again, I understood where the client was coming from since we're from the same culture but I saw the need for intervention because this was affecting the client’s emotional insight and volition to engage in activities independently (occupational performance). I was uncertain on whether a referral to a psychologist was required or I had to just leave the client like that, it was overwhelming.
Using a client-centered and when working as a Multidisciplinary team it is essential to plan interventions using that approach, working with the patient, understanding them holistically and establishing goals/aims with them and their carer. I tried using this approach and it was pretty hard because "Successful joint working requires clear, realistic and achievable aims and objectives..." and at this point the client's aim were unachievable and unrealistic and I really believed that she required some counseling from a psychologist to help her go through the acceptance stage.
The feedback I received from my supervisor was that I should be more understanding towards the situation because this is a new phase in her life and will need time to accept and move on, I should make use of activities to improve her level of independence and challenge her so that she can know her capabilities. I began to understand my role as an OT in MDT which was to improve her volition to engage in activities by reminding the client the importance of attending therapy as well as use of positive reinforcement during sessions. I also saw the need for care giver training with the family to incorporate them more into therapy and in helping the client to improve.
I can be a health advocate by motivating the client to have a specific routine which includes exercises or activities which she can do to promote and maintain health. Being a health advocate goes hand in hand with being OT because it promotes a healthy life and being in control of your life and establishing healthy habits therefore as an OT student I am a health advocate.
0 notes
Text
Occupational Therapy is a very multifaceted profession, the more your profoundness grows in it the more you realize the complexity of it. "Clinical reasoning is crucial in occupational therapy because it is the means by which the therapists identify the clients' problems accurately and determine effective treatment protocols", (M.N Ikiugu, Psychosocial Conceptual practice Models in Occupational Therapy, 2007). Basically it guides the therapist to be able to formulate goals, plan and implement intervention, evaluate the effectiveness of intervention and review. It's not rocket science when you think about it or when you explain it but when you put it into practice it's not a cakewalk.
In terms of putting clinical reasoning cycle into practice I was able to consider the client's situation as she is hospitalized and separated from family as well as the environment in which she is in. I was able to review the information I found on the client's file especially the history of the diagnoses and the cause of injury, as well as previous interventions she had received from other therapists. I had to be able to understand the client's diagnoses, though I was a bit overwhelmed by the fact that it was spinal cord related (paraplegic) as it was my first encounter therefore a lot of research was done to further my knowledge. I had to understand that the client's injury is a year and 4 months long, she is still adjusting to this new phase of her life therefore a lot of depression or anxiety may be present. I gathered new information through assessments and interviews.
As mentioned above that the client had received intense intervention from different therapists therefore a lot of improvement was observed especially on the upper limb and seemed independent in most ADLs which made it difficult for me to identify problems. A meeting with the therapist was done whereby we had to discuss her personal problems as well as the problems I've observed, formulate goals and set a daily routine suitable for her whilst she is in the hospital. As much as I was focusing on the client's residual impairments (weakness in the lower limb) as well as client factors like muscle strength on the upper limb, physical endurance and balance which are the most essential factors that prevent the client from being independent, my focus was also on the client's roles and responsibilities in order to formulate goals based on the activities she is required/expected to perform in the hospital and at home after discharge.
This week I had to plan my sessions according to the findings and problems I've identified to achieve the client's goals and the therapists (me) using an occupation-as-means approach. I realised, especially during dressing, that a lot of adaptations had to be done to accommodate the client as she had to use bed rails to lift her hips due to lower limb weakness, and I didn't consider all of that during my planning as I had expected the client to perform a movement which is facilitated by the lower trunk and buttocks which are weak. My aim for this week was on improving physical endurance and muscle strength by doing multiple activities in a day which resulted in overexhausting the client and ended up thinking that my aim wasn't met only to realise, through my supervisor's feedback, that my aim was actually achieved.
My supervisor was able to construct my thoughts, guide and improve my clinical reasoning by the feedback I received,commenting on that the choice of activities I do should relate to the client's goals not my personal goals as a student therapist. I should also consider the client's anxiety of falling during activities as well as paying attention to the muscles responsible for each movement that I expect the client to perform during activities. Therefore, I learnt the importance and the role of Clinical Reasoning as well as considering the client's goals using a client-centered approach and giving them autonomy. The client and I are from the same culture therefore we are able to relate to one another and I'm aware of the all the cultural morals therefore cultural humility was not used.
"Never, never be afraid to do what's right, especially if the well-being of a person or animal is at stake. Society's punishments are small compared to the wounds we inflict on our soul when we look the other way." - Martin Luther King Jr.
0 notes
Text
"To imagine oneself playing a role in an epic story is exhilarating but to actually step into an epic story is terrifying. And the problem is that imagination might be safe but being safe doesn't write any stories worth reading" - Craig. D Lounsbrough
It is essential to understand your role as a person, whether your role at home, work or community. This helps you structure your actions and intervention ls when your problem skills are required in different environmental settings. But the most crucial aspect of this is understanding the role of people in your surroundings, this is essential as it guides your interaction with them and it allows you to grow insight in terms of your boundaries with them. To be able to grow good and successful relationships with them, good communication skills are required. Many people struggle to communicate effectively sue to many factors, this can lead to misunderstanding and conflicts in a multidisciplinary team. To avoid problems as such all team members should remember the importance of good communication and remain calm even during stressful work periods.
As an OT understanding your role, : 1. As a therapist to your client and 2. As a multidisciplinary team member is important. For example building rapport with your client and utilizing questioning skills to your client's condition, personal thought, interests, likes, home environment etc is essential as it allows you to come up with a suitable treatment plan/intervention. On a personal level, my ability as a student therapist in understanding my role required a lot of research so that I can be able to structure myself in the place I'm placed in. My communication skills are being gradually improved as I get to interact more and more with my clients but in terms of communication skills with my clients I grow each and every day as I get to witness them grow comfortably during our treatment sessions and this allows me to incorporate in treatment planning and setting goals of treatment. Also this creates an opportunity to understand them on a personal level as this was one of the feedback received from my supervisor as she was motivating a client-centred approach in terms of planning.
When people work on multidisciplinary teams, they have different but complementary skills and experience that contribute to the overall effort. However, they might not share the same communication preferences and styles. Without good communication, confusion and misunderstanding can deminish the team's ability to achieve its goals. This is why it's important to develop goals and strategies to improve communication (D. Tara, Multidisciplinary Team Communication, 2020). Having to learn my role and other professional's roles was a bit of a challenge for me as I didn't know on how to work with them and having to create and maintain communication led up to a misunderstanding. Due to the client's which I have, which are chronic patients, it was a challenge for me to re-refer to other professionals as they have already completed treatment with them months ago. The assessment findings for one of my clients pointed a need for physiotherapy intervention and having to refer the client caused conflict and misunderstanding, that alone made me to negatively criticise my skills as a communicator and affected my treatment planning. Feedback from the supervisor helped me realize that you have to improvise and think out of the box in terms of treating this client. And that helped me to evaluate myself as a therapist.
Picturing yourself performing the required responsibilities of your role is much easier than physically fulfilling them. And establishing a foundation first and proving through your words and actions that you understand yours and other people's strengths and weaknesses improve your skills as a communicator.
"if you think communication is talking, you haven't been listening" - Debra-Ann Tanne
0 notes
Text
"Basically our role regardless of the setting is to get people back to the activities they love, whether it's after a physical or psychological injury" - Joel Pilgrim, founder of Waves of Wellness
Critical thinking is the highest level of cognitive function or ability which does not only require an individual to carefully or thoughtfully carry various evidences but to additionally appraise or identify the structural contexts in which this evidence have risen. It is also essential during Occupational therapy assessment and treatment sessions
Being able to incorporate critical thinking in your assessment and treatment sessions enhances your ability as a therapist to critically plan treatment using a client-centred approach. As occupational therapists aims on improving their client's independence in daily activities and enhance the individual's quality of life, they also need to consider their client's occupational performance.
On a personal level, incorporating critical thinking and use of client centered approach have been a bit of an obstacle for me as my clients are unable to independently formulate treatment goals for themselves due to poor cognitive skills and have no leisure pursuits. Also they both have no support system which I can communicate with in terms of goals, progress and what should be happening at home after discharge to maintain progress, bearing in mind that they're both a social case.
This week I had to meet with the social worker so that I can be able to critically plan for treatment. Therefore during my last interaction with my clients I was able to involve them in the intervention decisions I made by providing them with my aims of treatment to allow them to prioritize them into a list/prioritize their goals whilst they're in the hospital setting. This was done to aid client-centred approach.
Looking at the feedback received from my supervisor which was to focus more on the client's problems and priorities them so that I can clearly plan treatment I would say that it improved my insight as a therapist on how I can critically evaluate myself as a student therapist and on which areas to focus on when treating. Self evaluation would be I still need to learn how to cope with two clients and also how I can critically plan for treatment also provide the same service and not be bias.
(Roger's, 1961) "The client-centred approach focuses on the client's responsibility and capacity to discover ways to more fully encounter reality. The client who knows himself or herself best, is the one more appropriate behavior for himself or herself.". What I learnt is, understanding your client's phenomenal world and premorbiddaily routines to motivate execution of activities after injury is essential. It requires you to not only bring back different aspects of your client's premorbid world view and skills but to also modify their environments in order to stimulate execution, make it adaptable to clients and be realistic.
Therefore getting people back to the activities they love after a physical or psychological injury is essential and also including critical thinking and using a client-centred approach in your treatment plan.
"Because critical thinking demands a readiness to restructure one's thinking and decreases the risk of acting on faulty assumptions, it is an essential component of client centred practice" (KRW Hammel, 2015)
0 notes
Text
How Does Treating Make me feel?
As soon as I knew my client's diagnosis I pictured their clinical presentation and the assessments needed to be conducted. Most of the assessments conducted were client related as I had already observed him in the ward and was able to assess one of the basic ADLs (dressing), his level of functioning and the collateral information.
As further assessments were planned and conducted, I noticed that I fail to properly plan and structure assessment and treatment session as I didn't plan them accordingly and they weren't realistic. I had to change a lot of structuring due poor planning but that improved my insight as a student therapist.
I also learnt that you can also incorporate treatment in your assessment session, incorporate it in such a way that you can educate the client functional movements for activity completion (this was observed during dressing of the UL & LL and during feeding). It is also motivating to observe the client do the movements independently after teaching them, without assistance. It made to look forward into doing more assessments and treatments with the client.
The feedback which I received from my supervisor improved my insight as a therapist in terms of writing a write up and preparing for a treatment session as he specified that I wasn't clear and specific on my aims of assessments. Looking forward into doing more mistakes and learning from them.. And also gaining more knowledge about OT treatment 🌼😊🎈
1 note
·
View note