Juniper Publishers | Journal of yoga and physiotherapy is a multidisciplinary, international peer reviewed journal and is dedicated to promote spread the information in yoga and physiotherapy.
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by juniperpublishers-yoga and here's what we found interesting.
Average Info
Notes Per Post
203
Likes Per Post
111
Reblog Per Post
92
Reply Per Post
0
Time Between Posts
2 months ago
Number of Posts By Type
Text
17
Last Seen Tumblr Blogs





Fun Fact
Tumblr was named as a finalist in Lead411’s New York City Hot 125 in Aug 2010.
Text
Health Promotion Program of Yoga Exercise among Female in Workplace

Authored by Su Ying Tsai
Introduction
Working women are a larger part of workforce than in previous generations. Premenstrual syndrome (PMS) is a common disorder in menstruating females. All women, regardless of race, age, or socioeconomic status, have experienced discomfort during their menstrual periods. Painful menstrual periods or PMS are the most common gynecologic problems as well as the most common reason for increased absenteeism and more workdays with 50% or less of typical productivity per month in female employees [1]. Females with PMS report a poorer perceived quality of sleep [2] and health-related quality of life [3-5], and PMS may result in a depressed mood and greater psychiatric comorbidity [6]. Severe menstrual symptoms lead to increased healthcare utilization, decreased occupational productivity, and absence from work [7].
In recent years, with the rise of educational level and social changes, female labor force has become an indispensable stable foundation for economic development in Taiwan. To our knowledge, when female workers have PMS in the workplace in Taiwan, care personnel in the workplace usually provide heat packs or suggest bed rest at a health center or may provide painkillers. These methods, which merely alleviate female workers’ pain at the time the menstrual cramps occur, are not preventive methods. Recent studies reported an association between exercise and PMS and indicated that a regular exercise habit might be associated with a decrease in some physical and psychologic premenstrual symptoms [8-9]. Exercise is commonly listed as a remedy for PMS. Hence, more and more workplaces and employers are attempting to determine preventive methods or health promotion activities that can ameliorate PMS in female workers during their menstrual periods.
A growing body of evidence indicates that yoga benefits physical and mental health by down regulating the hypothalamic-pituitary- adrenal axis and the sympathetic nervous system [10]. Yoga is a mind and body practice with historical origins in ancient Indian philosophy. Many clinicians treating persistent pain hear about the benefits of yoga from patients who frequent yoga centers. Yoga classes specifically designed for women with PMS have increased, but there is little research about the efficacy of these classes. No research in Taiwan has addressed improvement or changes in female workers’ menstrual discomfort through interventional psychologic and physical yoga activities in the workplace. The research setting was Company C, a large electronics manufacturer requiring highly labor-intensive work in the Tainan Science Park in Southern Taiwan. This company has many female employees of reproductive age, the director of health management pay attention to female employees’ premenstrual disorders and the negative impact of premenstrual symptoms on occupational productivity and attendance. The yoga exercise program was 12 weeks long and featured physically and psychologically interventional yoga activities to determine changes in female workers’ menstrual discomfort.
This study invited all eligible employees (female employees aged 20 to 45 years who were healthy premenopausal women, taking no oral contraceptives, and taking no medication during the last 3 months) and all of them voluntarily participated in this program. Written and signed informed consent was obtained from each participant. The yoga teacher personally guided each participant’s yoga exercise activities at twice-a- week 50-min sessions after work in the plant’s fitness center. There were four yoga classes a week to choose from, allowing participants to select the most convenient time to participate in two yoga classes per week. Each 50-min session comprised a 5-min breathing exercise, 35-min yoga pose practice, and 10-min supine meditation/relaxation. Before starting the yoga exercise intervention programs, we administered a structured self- report questionnaire to the participants to collect information about baseline menstrual pain scores, premenstrual symptoms, and health-related quality of life during the prior 6 months. At the end of the 12-week yoga exercise intervention, we administered the same questionnaire to evaluate changes in the participants’ menstrual discomfort.
A total of 64 participants completed the intervention study. Data revealed that moderate or severe effect of menstrual pain on work was reported by 53.1% participants, with 35.9% subjects reporting the need for analgesics every month during menstruation to relieve menstrual pain. The comparison of characteristics of menstruation before the yoga exercise intervention and after 3 months revealed that 14% participants significantly decreased their use of analgesics during menstruation and the prevalence of a moderate or severe effect of menstrual pain on work significantly declined 23.4% after the yoga exercise intervention. Menstrual pain scores above 80 were reported by 14.1% subjects before the intervention, but after 12 weeks of yoga exercise the prevalence decreased to only 4.7% of subjects. The 12-week yoga exercise intervention was significantly correlated with decreased prevalence of four physical symptoms, including abdominal swelling, breast tenderness, abdominal cramps, and cold sweats.
Based on this data, these findings suggest that yoga exercise in the workplace effectively reduces the symptoms of PMS and can be applied to other woman-friendly workplaces to relief PMS. The results will contribute to our understanding of the current status of a menstrual health-friendly workplace environment for female employees and can be used to establish a model for a healthy lifestyle with a regular yoga exercise to decrease the negative impact of premenstrual symptoms. However, this program has some limitations [11]. Nevertheless, workplaces and employers can help female employees to understand the benefits of regular exercise, such as yoga, which may decrease premenstrual distress and improve the health of female employees. This program may be able to provide a reference for menstrual health promotion of female employees in the future workplace.
For more articles in Journal of Yoga and Physiotherapy please click on https://juniperpublishers.com/jyp/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#karma yoga#physiotherapy#juniper publishers#open access journals#high impact factor journals#physical health#peer review journals#yoga meditation#meditation#yoga
4 notes
·
View notes
Text
Effect of Yoga on the Autonomic Nervous System: Clinical Implications in the Management of Atrial Fibrillation

Authored by Maheswari Murugesan
Abstract
Atrial fibrillation (AF) affects about 1.5% of the U.S. population, especially aging persons, resulting in substantial morbidity and mortality. Although radiofrequency catheter ablation is the accepted treatment for AF, failure of this therapy is common. Given that the onset of AF is preceded by a primary increase in the sympathetic drive followed by marked modulation towards vagal pre-dominance, it is likely that stress precipitates and exacerbates AF. The authors searched the databases of Ovid MEDLINE, Pub Med, APA PsycNET, Alt Health Watch via EBSCO host, and CINAHL to evaluate the effects of yoga as a complementary health approach on the autonomic nervous system and how this mind-body modality, if added to conventional treatment, might contribute importantly to reducing or eliminating stress as a trigger for AF. Articles written in English and published in peer-reviewed journals between 2003 and 2017, reporting on research of yoga on autonomic nervous system, were identified. Twenty articles met the inclusion criteria, revealing that yoga resulted in a significant shift in autonomic balance towards vagal dominance; reduction in heart rate and blood pressure; reduction in indices of ventricular repolarization dispersion in patients with ventricular arrhythmias; significant reduction in stress, anger, depression, and anxiety; and improvements in neuroendocrine release, emotional processing, and social binding. Given these literature review findings, the authors provide an integrative overview of biological mechanisms and substrates that mediate AF, which can be targets for future research evaluating how the practice of selected styles of yoga can mitigate the onset of AF.
Keywords: Yoga; Heart rate variability; Stress; Autonomic nervous system; Atrial fibrillation
Abbrevations: ANS: Autonomic Nervous System; PNS: Parasympathetic Nervous System; HRV: Heart Rate Variability; HF: High Frequency; LF: Low Frequency; VLF: Very-Low-Frequency; ULF: Ultra-Low-Frequency; SDDN: Standard Deviation of Normal-to-Normal; RMSSD: Root Mean Square of Successive Differences; NN50: Number of Pairs of Successive NN (R-R) Intervals that Differ By More Than 50 Milli Seconds; pNN50: Proportion of RR Intervals >50 Msec; FEV1: Forced Expiratory Volume in 1 Second; FVC: Forced Vital Capacity; FEF: Forced Expiratory Flow; PEmax: Maximum Peak Expiratory Flow Rate; PImax: Maximum Inspiratory Flow Rate; GABA: Gamma Amino-Butyric Acid; QOL: Quality of Life; Min: Minute/s; Yr: Year/s; MET: Metabolic Equivalent of Task; AF: Atrial Fibrillation; PAF: Paroxysmal Atrial Fibrillation; QOL: Quality of Life; VAS: Visual Analogue Scale; SD: Standard Deviation; Min: Minute/s
Introduction
Atrial fibrillation (AF), the most common sustained cardiac arrhythmia, is seen in approximately 1.5% of the U.S. population [1] and results in substantial morbidity and mortality [2]. One of the largest U.S. epidemiological studies, the Framingham Heart Study, predicted that AF prevalence doubles with each advancing decade of age, from 0.5% at age 50-59 years to almost 9% at age 80-89 years, independent of the increasing prevalence of known predisposing conditions [2]. Although medical treatment involving radiofrequency catheter ablation has become the well-accepted management strategy for AF [3] failure of this therapy is common, with only two-thirds or less of the patients treated remaining free of AF on long-term follow- up [3]. Early recurrence of atrial tachyarrhythmia, usually defined as arrhythmia recurrence within the first 3 months following ablation, is frequently associated with late recurrence of atrial tachyarrhythmia [4,5]. Acute myocardial injury and the subsequent inflammatory response, as well as modifications of the cardiac autonomic nervous system, provide an early and potentially reversible pro-arrhythmic substrate because of altered atrial myocardial conduction and refractoriness [3]. Research has shown that psychological stressors and imbalance in the autonomic nervous system (ANS) are the most common triggers for paroxysmal AF [6,7]. The mind-body therapy yoga has been shown to reduce stress and maintain autonomic nervous system balance [8]: hence, use of complementary health approaches such as yoga, which are low-cost interventions, might contribute importantly to reducing stress, help individuals maintain balance in the ANS, and thereby prevent recurrence of AF. In this article, the authors provide an overview of AF, the effects of yoga on lessening stress and maintaining ANS balance, and suggest through a psychoneuroimmunological framework the possible mechanisms by which the practice of yoga could mitigate AF episodes and symptoms.
Atrial fibrillation and associated symptoms
Cumulative lifetime risk estimates reveal that AF is primarily a disease of aging. In U.S. and European community-based cohort studies, the estimated lifetime risk of AF is 22% to 26% in men and 22% to 23% in women by age 80 years [9]. The effects of heart failure, valvular disease, myocardial infarction, and ischemic stroke on AF are substantial. Heart failure increases the risk of AF by a 4.5-fold in men and a 5.9-fold in women. Valvular heart disease increases the risk of AF by a 1.8-fold in men and a 3.4- fold increase in women, with myocardial infarction significantly increasing the risk of AF by 40% in men [2]. Likewise, AF is a potent risk factor for ischemic stroke, increasing the risk of stroke 5-fold, thus leading to about 15% of all strokes nationally [10].
The most common AF symptoms include palpitations, shortness of breath, fatigue, dizziness, and anxiety. In a study of 100 randomly selected patients with AF, 88% reported palpitations on exertion, 86% reported palpitations at rest, 70% reported shortness of breath on exertion, 87% reported reduced physical ability, and 59% reported anxiety [6]. Adults with major depression, anxiety, or somatization disorder generally have an associated increase in the severity of their AF symptoms [11].
Quality of life in individuals with AF
AF contributes to increased morbidity in the elderly by adversely affecting their quality of life (QOL) and by deterioration in myocardial function, increasing susceptibility to heart failure, stroke, hospitalization, and mortality [12]. Evaluation of QOL in a group of 264 female patients with AF enrolled in the Canadian Trial of Atrial Fibrillation (N = 403) showed that women had significantly more impaired QOL than men, specifically related to physical rather than emotional functioning [13]. In another study, outpatients with documented AF (N = 152) reported substantially poorer QOL than healthy controls [14]. Three of the four well-known randomized controlled trials (STAF, PIAF, RACE) comparing rate versus rhythm control demonstrated a greater improvement in QOL in patients receiving rate control [15] than those in the rhythm control group. However, the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) trial revealed a similar improvement in QOL for both rate and rhythm control groups [15].
Health care costs associated with AF
A national survey estimated that direct medical costs were 73% higher in patients with AF compared with matched control subjects, representing a net incremental cost of $8705 per patient per year and a national incremental cost between $6 and $26 billion [16]. Retrospective analyses of three federally funded U.S. databases using 2001 data [17] found that approximately 2,34,000 hospital outpatient department visits, 2,76,000 emergency room visits, 3,50,000 hospitalizations, and 5 million office visits were attributable annually to AF. The total annual medical cost for the treatment of AF in the inpatient, emergency department, and hospital outpatient settings estimated at $6.65 billion is likely an underestimate as costs for long-term anticoagulation, stroke prevention, inpatient drugs, and hospital-based physician services were not included [17]. Patients with AF enrolled in the Fibrillation Registry Assessing Costs, Therapies, Adverse events, and Lifestyle (FRACTAL) study who were managed with cardioversion and pharmacotherapy incurred AF and other cardiovascular-related health care costs of $4000 to $5000 per year [18]. Among patients with recurrent AF, the frequency of recurrence was strongly associated with higher resource use, with each recurrence increasing annual costs by an average of $1600 [18]. The cost-effectiveness of catheter ablation is difficult to determine because of differences in the experience levels of centers treating these patients, use of technology, and rates of reimbursement, each of which affects cost calculations [19]. Researchers evaluating the cost- effectiveness of AF ablation compared with rhythm control or anti arrhythmic agents have shown that ablation treatment results in improved quality-adjusted life expectancy, although at a higher cost [18,19].
Atrial fibrillation and stress
Researchers have shown that psychological stressors and imbalance in the autonomic nervous system are the most common triggers for paroxysmal AF [6,7]. Acute life stressors affect the development and spontaneous conversion of AF and are thought to be mediated by the sympathetic nervous system. This hypothesis is supported by increased circulating catecholamine following an acute life stress and by observation that beta-adrenergic blockade prevents abnormal heart rhythm disturbances triggered by acute life stress [5]. In a study of 100 randomly selected patients with idiopathic paroxysmal atrial fibrillation, 54% reported psychological stress as the most common triggering factor for AF [6]. In another study of 116 patients with AF without an obvious cause, acute life stress significantly affected the development and spontaneous conversion of AF [7].
Atrial fibrillation and the autonomic nervous system
The autonomic innervations to the heart from the brain, the spinal cord (extrinsic system) and the ganglion plexi of the heart itself comprise the local ANS (intrinsic system) [20]. This intrinsic cardiac ANS of the heart and the pericardium serves as more than a relay station for the intrinsic projections of the vagal-sympathetic system from the brain and spinal cord to the heart. Supporting this theory is the fact that ablation of the major ganglion plexi at the pulmonary vein atrial entrances either eliminates or markedly diminishes AF inducibility. Also, this intrinsic cardiac autonomic system can act independently to modulate numerous cardiac functions, including automaticity, contractility, and conduction [20].
In addition to the sympathetic component of the ANS, the parasympathetic component has been shown to play a role in AF [21]. Amar et al. [22] showed that the onset of AF was preceded by a primary increase in the sympathetic drive followed by marked modulation toward vagal pre-dominance. The physiologic studies by Patterson et al. [23] further indicate that sympathetic stimulation plays an important modulatory role in the emergence of focal drivers for AF in the presence of an increased vagal tone. The ANS is involved in the genesis of both AF triggers (i.e., ectopic foci that result from interaction between vagal and sympathetic stimulation) and the creation of a more established AF substrate that is needed for the maintenance of AF and is enhanced in the presence of structural heart disease [21]. It has been shown that the abnormal electrical conduction within the pulmonary veins could be sustained only in the presence of isoproterenol or acetylcholine, indicating that sympathomimetic or cholinergic stimulation appears to be necessary to promote the development of sustained focal activity in the pulmonary veins [21].
Relationship between autonomic nervous system and measurement of heart rate variability
Heart rate variability (HRV), the variance between the R-R intervals or complete cardiac cycle on the electrocardiogram, can be used to assess the balance between the sympathetic and parasympathetic branches of the ANS [24]. Efferent sympathetic and parasympathetic activity is integrated in and with the activity occurring in the heart's intrinsic nervous system. Thus, HRV is considered a measure of neurocardiac function that reflects heart-brain interactions and ANS dynamics [25]. HRV is assessed with various analytical approaches, although the most commonly used are frequency domain (power spectral density) analysis and time domain analysis [25]. The European Society of Cardiology and the North American Society of Pacing and Electrophysiology Task Force Report on HRV divided heart rhythm oscillations into 4 primary frequency bands: high- frequency (HF), low-frequency (LF), very-low-frequency (VLF), and ultra-low-frequency (ULF) [24]. It is often assumed that a low LF:HF ratio reflects greater parasympathetic activity relative to sympathetic activity [25]. In contrast, a high LF:HF ratio may indicate higher sympathetic activity relative to parasympathetic activity as can be observed when people engage in meeting a challenge that requires effort and increased sympathetic activation. Alternatively, it can indicate increased parasympathetic activity as it occurs during slow breathing. Time domain indices quantify the amount of variance in the inter-beat-intervals using statistical measures. The three most important and commonly reported time domain measures are the standard deviation of normal-to-normal (SDNN), the SDNN index, and the root mean square of successive differences (RMSSD) [25]. The modulation of vagal tone helps maintain the dynamic autonomic regulation important for cardiovascular health. Reduced parasympathetic (high frequency) activity has been found in cardiac pathologies and in patients under stress or suffering from panic, anxiety, or worry [24].
Yoga as a complementary health approach in treating atrial fibrillation
Yoga, an ancient discipline from India, is a mind-body exercise in which both physical and mental disciplines are brought together to achieve peacefulness of mind and body, resulting in a relaxed state that is useful in managing stress and anxiety. To date, two studies have assessed the impact of yoga on AF. One, a proof-of-concept study [26], revealed that 60-minute Iyengar yoga sessions at least twice a week for 3 months improved symptoms, arrhythmia burden, heart rate, blood pressure, anxiety and depression scores, and several domains of QOL in adults with paroxysmal AF. A second study [27] using mediyoga as the intervention, showed that this style of yoga might potentially lower blood pressure, lower heart rate in patients with paroxysmal AF, and improve QOL compared to a control group.
Given the potential positive impact of yoga on decreasing AF episodes and symptoms as shown in Table 1, the authors conducted an extensive computerized search of diverse databases (Ovid MEDLINE, Pub Med, APA PsycNET, Alt Health Watch via EBSCO host, CINAHL), using key terms of heart rate variability and autonomic nervous system, to assess the effect of yoga on the ANS. These computerized searches yielded 230 studies (Ovid MEDLINE = 25, Pub Med = 31, APA PsycNET = 16, Alt Health Watch = 153, CINAHL = 5), which were then reviewed for eligibility. Inclusion criteria were English language articles reporting on studies that (a) enrolled subjects 18 years and older and (b) were published between 2003 and 2017 in peer- reviewed scientific journals.
The 20 articles that met the inclusion criteria are shown in Table 2. Seventeen were interventional studies with 14 of these using random sampling; 3 used non-randomized sampling techniques. One of the studies included a discussion of the effect of yoga on the parasympathetic and GABA systems [8] and the other study reviewed the health impacts of yoga and pranayama [28]. The review also identified two relevant articles that provided additional information on the impact of yoga on the ANS. One of the articles, provided a review of the health impacts of yoga and pranayama [28] and the second proposed a neurophysiologic model to clarify the mechanisms by which SudharshanKriya yogic breathing balance the autonomic nervous system activity [29].
Sample characteristics
The participants in all 17 interventional studies were adults aged 18 years or older. Three studies included only male participants, with the rationale for excluding females being the tendency in variation of the autonomic variables with the phases of the menstrual cycle in females. However, Markil et al. [30] included 15 women in their study, completing the study during the follicular phase of the menstrual cycle given that the luteal phase causes increase in sympathetic activity. One study did not mention the sex of the participants. Of the 17 interventional studies, 8 were completed in India, 5 within the United States, 1 in each completed in Australia, Germany, Brazil, and Nepal. Women and ethnic minorities were under represented in these studies. Most of the studies except for Dabhade et al. [31] excluded patients with arrhythmias and those on any medications such as beta-blockers and anti-arrhythmic medications that have significant effect on heart rate and rhythm.
The studies reviewed showed that participation in a yoga intervention resulted in a significant shift in autonomic balance towards vagal dominance; a reduction in heart rate and systolic, diastolic, and mean blood pressure; a reduction in the indices of ventricular repolarization dispersion (QTd, JTd) in patients with ventricular arrhythmias; significant reduction in stress, anger, depression, anxiety, and neurotic symptoms; and improvements in neuroendocrine release, emotional processing, and social binding. Both time and frequency domain indices of heart rate variability showed significant changes towards parasympathetic modulation. Bidwell, et al. [32] found that yoga training for females with mild to moderate asthma decreased parasympathetic activity and increased sympathetic modulation as assessed by isometric forearm exercise. Yoga not only causes increased parasympathetic tone but when needed decreases the highly active parasympathetic nervous system to maintain a balanced autonomic nervous system activity.
Right nostril yoga breathing can increase sympathetic tone and cardiac sympathetic activity, resulting in increased blood pressure and heart rate. Left nostril yoga breathing can decrease systolic and mean blood pressure while alternate nostril breathing can decrease both systolic and diastolic blood pressure [33]. Slow breathing exercises can improve sympathetic and parasympathetic reactivity [34]. Slow pace
Bhastrikapranayama exercise has shown a strong tendency towards improving function of the ANS through enhanced activation of the parasympathetic system [35]. Yoga practice of cyclic meditation during the day appears to shift sympatho- vagal balance in favor of parasympathetic dominance during sleep on the following night which promotes improved quality of sleep [36]. Four months of respiratory training in Bhastrika pranayama increased respiratory function and improved cardiac parasympathetic modulation in a group of healthy elderly subjects [37]. The changes during Dhyana (meditation) [38] and guided relaxation [39] resulted in reduced activity of the sympathetic nervous system showing a shift in autonomic balance towards vagal dominance. Laughter yoga therapy for individuals awaiting heart transplant showed improvement in vigor-activity, friendliness, and long-term anxiety. It also improved HRV measures within or close to normal ranges from being low at baseline perhaps related to reduced vagal stimulation [40]. Integrated yoga practice reduced perceived stress and improved adaptive autonomic response to stress in healthy pregnant women [41].
The styles of yoga reported on in the research reviewed include Hatha yoga, viniyoga, Ishayoga, Iyengar yoga, laughter yoga, integrated yoga, yoga nidra relaxation, meditation (cancalata, ekagrata, dharana, dhyana), pranayama (Bhastrika, Kapalbhati, Anilom-vilom, Bhramari, Udgit), cyclic meditation, guided relaxation and yoga breathing practices. Yoga postures, breathing exercises, pranayama, and meditation reportedly led to a significant shift in autonomic balance towards vagal dominance, which can prevent tachycardia, an important goal in the management of AF.
Only 4 studies mentioned the number of participants who completed the studies, with attrition rates ranging from 3.3% to 54.06%. The primary reasons for participants not completing a study were drop outs, irregular attendance at intervention sessions, and relocation following study enrollment. Higher attrition occurred in 'in-person' mindfulness therapy groups (27.3%) compared to the 'online' mindfulness meditation groups (3.8%) [42], giving rise to the need to consider the format and location of yoga interventions. Also, the studies reviewed did not provide an explicit theoretical or conceptual framework to explain the basis for the yoga interventions used with the study population.
A psychoneuroimmunological framework to explain effects of yoga on AF
To address the deficit in the literature regarding theoretical or conceptual frameworks in the studies reviewed, the authors identified a psychoneuroimmunological framework adapted from McCain et al.
[43]shown in Figure 1 to depict the electrical, mechanical, and structural changes in the heart that lead to a stress-related imbalance in the ANS resulting in AF. Yoga interventions can potentially foster the electrical stability of the heart by maintaining ANS balance and lessening AF episodes, AF symptoms (palpitations, shortness of breath, dizziness, and fatigue), stress, depression, and anxiety, thus improving the participants’ health-related QOL. Modulating factors such as stress can cause imbalance in the ANS, which, in turn, can lead to AF. Persistent AF causes inflammation and fibrosis of the atria, resulting in a fixed substrate for re-entry and consequent sustained episodes of AF [21], making treatment options to break this re-entrant cycle challenging. Triggers for atrial fibrosis include the activation of the renin-angiotensin- aldosterone system, inflammation, and oxidative stress [44]. The combination of normal and diseased atrial fibers in conjunction with local fibrosis results in spatial dispersion of atrial refractoriness and causes localized conduction abnormalities, including intra-atrial conduction block and slow conduction [44] . Thus, the interplay of stress (psycho), imbalance in the ANS (neuro), activation of the renin-angiotensin-aldosterone system, inflammation and oxidative stress resulting in atrial fibrosis (immuno) triggers AF and creates a substrate for persistent AF. Mind-body approaches use the concept of body and self-awareness to promote rechanneling of energy within the body thereby maintaining an internal balance. This mind- body balance can further reduce [47] psychological stressors that are important modulating factors in AF and modulate the ANS to parasympathetic dominance in maintaining a stable myocardium, thereby preventing arrhythmias.
Conclusion
Even though the time span of the yoga interventions reported in the studies reviewed ranged from a few minutes to months, all the studies demonstrated some beneficial effect in maintaining nervous system balance and significant impact on selected physiological and psychological factors, thereby improving the participants' overall QOL. Given its impact on modulating autonomic system balance and reducing psychological stress, selected styles of yoga might be considered as cost-effective complementary health approaches in managing AF episodes and symptoms. Further rigorous study is warranted to clarify further the specific mechanisms involved in the use of yoga in patients diagnosed with AF.
For more articles in Journal of Yoga and Physiotherapy please click on https://juniperpublishers.com/jyp/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#karma yoga#yoga#physiotherapy#journal of yoga and physiotherapy#meditation#juniper publishers#physical health#open access journal#high impact factor journals
2 notes
·
View notes
Text
The Problematic Nature of the Third Chapter of the Yoga Sūtras and its Discussion of Powers

Authored by Carl Olson
Abstract
Because the Yoga Sūtras compiled by Patañjali devote one entire chapter to siddhas (powers) in a text of only four chapters this has caused scholars to offer various reasons for this problematic aspect of the text. After critically reviewing the opinions of scholars with respect to the imbalance in the text to understand Patañjali's decision, this essay places the text within the historical context of asceticism in India in order to grasp developments that might have shaped the compiler's mind. The historical development of asceticism in India was also accompanied by many narratives that stressed the importance of ascetic powers and helped to shape Patañjali's decision to make a quarter of his text about powers, even though these powers were acknowledged to be a hindrance to an aspirant's final goal.
Around the fourth century CE, the legendary Patañjali, compiler of the Yoga Sūtras, collected elements associated with ascetic practices in order to serve as a guide book for others. In his attempt to bring unity to the various pre-existing yogic traditions, Patañjali gathered together various elements into aphoristic, cryptic, and esoteric statements (sūtras) that lent itself more to remembrance and oral transmission. Because the text was incomprehensible, it invited commentaries by authorities with the intention of rendering the text comprehensible to the uninitiated. The Yoga Sūtras consisted of four parts with about three quarters of the text focusing on technique and the third part of the text concerned with powers gained by yogis practicing the various disciplines. Hence a quarter of the text was concerned with these various supernatural powers called in the introduction to chapter three vibhutis, but called siddhas in the remainder of the chapter.
According to the contents of the Yoga Sūtras and its third chapter, these powers include the ability to know, for example, the past and future, awareness of past rebirths, ability to read the mind of another person, awareness of the approach of one's death, intuiting the location of hidden objects, and intuiting the presence of the purusa (self). These are examples of cognitive (jñāna) powers. Powers (siddhas) that are more physical in nature include, for instance, the ability for a yogi to become invisible, have the strength of an elephant, ability to enter the body of another person, levitation, acute hearing, ability to fly, becoming disembodied, and gaining a perfected body. These various forms of mental and physical powers also find their way into Hindu, Buddhist, and Jain narratives that will be illustrated later in this essay.
A reader of the Yoga Sūtras is informed that these powers are a result of practicing the final three parts (samyama) of the path to liberation that begins with concentration (dhāranā) and includes meditation (dhyāna), and absorption (samādhi), and all major commentators agree that the various powers are results of practicing yoga, and are not the goal of the yogic path. In addition, practitioners are warned not to become attached to the powers gained by yogis because they are a trap that keeps a yogi attached to the world. Nonetheless, within the context of a “how to manual,” it is curious that an entire quarter of the book is devoted to powers (siddhas). Patañjali obviously considered the acquisition of powers to be an essential aspect of the yogic path. This apparent oddity of the text has puzzled scholars, and various attempts have been made by scholars of yoga to attempt to make sense of this feature of the text. This essay proposes to reconsider and attempt to understand what might have motivated Patañjali to devote an entire chapter of his four chapter text to the subject of yogic powers. To meet this purpose of the essay, it is advisable to review interpretations of these powers by different scholars and then to place these powers into their historical context. Thirdly, examples of yogis/ascetics using powers in various narratives will be included because these stories are part of the cultural milieu in which Patañjali worked on the text. Because the yogi has been an ascetic figure traditionally in Indian culture, I have used the terms yogi and ascetic interchangeably.
Go to
Scholarly Interpretations of Ascetic Powers
In his magisterial, multi-volume work on the dharmaśāstra literature, P. V. Kane calls attention to the integral part that the siddhas (powers) play in the Yoga Sūtras [1]. Kane asserts that his opinion is based on the fact that there are 35 references to siddhas in the text out of a grand total of 195 sutrūs. Kane goes on to discuss the origins of the various powers according to Patañjali. And he calls attention to a belief among tantrikas and yogis that mantras had the power to confer supernormal powers.
An early discussion of the importance of ascetic powers in the West is offered by Charles Rockwell Lanman of Harvard University in 1917 for the American Philological Association. Lanman thinks that the practice of asceticism is motivated by the promise of its rewards. Lanman argues that some yogic powers are indubitably instances of hypnosis as in the case of entering another body and gaining power over the will of another person [2]. The role of hypnosis is questionable, although it is a reasonable position to take based on the subject matter that opens itself to speculation about its origins.
Max Weber [3], a preeminent and influential German sociologist, published The Religion of India in 1920 where he discusses the importance of Indian asceticism that he describes as "the most rationally developed in the world [3].” Weber traces its origins to the practice of "magical ecstasy” with the purpose of acquiring magical powers that extended to power over gods, who also practiced asceticism. Indian ascetics are characterized as "possessors of holy charisma and even revered as saints and wonder workers, giving them a power the Brahmans wished to monopolize for themselves [4].” The charisma (a Greek term referring to grace, favor, or gift) to which Weber points is characterized as a charisma of knowledge in the Indian cultural context. For readers of Weber's works, it is not surprising that he would discover something rational about asceticism because rationality plays a pivotal role in his sociological theory by operating on three different levels that include a pattern of individual action and belief, a cultural principle, and a characteristic of social organizations. With respect to individual action and belief, Weber distinguishes between non-rational and rational action. The former arises from deeply held feelings (affectual type) or long held customs (traditional type). The non-rational type of action is more common and is more akin to momentary reactions rather than carefully conceived plans. Compared to the non-rational; the rational response is a more deliberate, self-conscious, calculated response to ways of reaching one's goals, which is true of the yogi.
For Weber [3], a yogi's attainment of powers is a personal achievement that is not confined to any single group status. Weber thinks that the orgiastic-ecstatic features of Indian asceticism points to something irrational, and connects it to neuropathic states, a stance that anticipates the approach of cognitive science to some degree. According to Weber, charisma is a relational notion because it is based on perceptions of others that a particular person is endowed with extraordinary qualities, which renders it an ideal type and gives the charismatic authority to lead others, although such leadership is unpredictable and unstable. Taking what he terms an “other-worldly asceticism,” Weber also writes about a “ this-worldly asceticism,” which he defines as an ordered, diligent, and temperate life that is suited to the development of an economic system such as capitalism. Dumont, a French sociologist, characterizes Weber's theory as “a miracle of empathy and sociological imagination [5].” In spite of Dumont's strong endorsement of Weber’s theory, other thinkers would make their own contributions to the powers acquired by ascetics.
The earliest systematic scholarly study of the powers in Hinduism and Buddhism is Siddhi und Abhiññū: Einestudieüber die klassischen Wunder des Yoga written by Sigurd Lindquist [6] published in 1935. Comparing yogic siddhas with Buddhist rddhis, Lindquist conflates them with his psychological approach, and argues for their equivalence. He argues that powers are mental states brought about by a process of hypnosis, which results in a subjective creation of mental illusions and hallucinations [6]. Therefore, he reduces various types of powers to psychological phenomena. Over by warns against such a conflation of yogic and Buddhist powers because it is misleading, and creates a false impression about the traditional development of these powers. Thereby, Lindquist's approach misses instances of importation and appropriation of the powers [7].
Prior to Lindquist's study of the powers associated with the practice of yoga, JW Hauer [8] published Die Anfange der Yoga: Praxis imaltenlndien in 1922, and in 1958 he published Der Yoga: Einlndischer Wegzum Selbst. In the latter study, Hauer indicates that the powers are part physiological and part psychological [8]. Hauer is also interested with finding the origins of yoga, which he traces to a group of wandering ascetics called Vrātyas, who he identifies as Aryan, although not belonging to the orthodox Brahmanicpriesthood [9]. The Vrātyas are a group that worshiped a primal god known by several names.
Working during the same time of Hauer's second book, Mircea Eliade’s [10] Yoga: Immortality and Freedom, an influential work based on his doctoral research in India published in Paris in 1954 before its translation into English in 1958, reflects the scholar’s approach to the study of religion and his theory of religion. Eliade likens the yogi, for instance, to a magician, the acquisition of powers as anostalgia for a divine condition, and "Yoga leads to a mythological perfection, the very perfection enjoyed by the personages of the Indian pantheon [10].” For someone who writes about initiation, it is not surprising that Eliade also finds an initiatory aspect to the practice of yoga and the attainment of powers. Eliade observes that the knowledge obtained by a yogi is akin to something both grandiose and paradoxical because it is equivalent to an appropriation: "For obtaining direct revelation of the purusa is at the same time to discover, to experience, an ontological modality inaccessible to the noninitiate [11].” As a phenomenologist, Eliade does not raise the question about the literal validity of the various powers by bracketing-out such a question because he wants to understand the powers on their own religious level and not impose his opinions and biases on the textual evidence.
Gaspar Koelman [12], a Jesuit scholar of yoga, is critical of Eliade’s position, although he does agree about the magical quality of the powers. Koelman claims that it is not a yogi's acquisition of perfect knowledge about matter (prakrti) that forms a direct link to the powers, but it is rather "psychological and psychical pacification that matters [12].” Koelman views the acquisition of powers as an ascendancy of spirit over matter and not simply an extraordinary intuitive insight into the nature of reality that Eliade seems to suggest to him, resulting in a recovery of the self,its absolute awareness, and complete freedom.
Similar perspectives on yogic powers are offered by Corrado Pensa, Georg Feuerstein, and Gerhard Oberhammer. Viewing powers as intrinsic to the yogic path, Pensa thinks that they represent specializations connected with the path to liberation, but he also sees them as spurious aspects or magical residues without a textual foundation [13]. Feuerstein agrees with Pensa that powers do not fit into the text, refers to them as the magical aspect of the yogic path, asserts that they conflict with Patañjali’s rationalism, and he wonders why this is the case [14].
According to Oberhammer, Patañjali's compiling of inherited elements of yoga into a consistent discipline represents the attempt to synthesize two forms of meditation: samadhi (concentration) and samapattih (unification), which manifest different structures. In fact, unification is a method intended to appropriate a belief or truth without a real object because it only possesses representations and ideas [15]. In another work, he acknowledges the importance of yogic powers in the Yoga Sūtras that he traces to a foundational stage of the development of the practice of yoga before it is superseded and humanized by Buddhism and Samkhya [16,17].
In contrast to Feuerstein, Pensa, and Oberhammer, Jean Filliozat, a French scholar, argues that the various powers are "not miraculous in the sense of a suspension of the laws of nature, but they are deemed to be realizable through a higher and even integral knowledge of the laws of nature [18]." Filliozat offers a physiological explanation of some powers by the yogi who manipulates his/her external and internal body [19]. According to Filliozat, the yogi gains control by means of his/her practice of the muscular synergies of the body and/or the neuro-vegetative system.
Obeyeskere [20], a psychoanalytic anthropologist of South Asia, argues that yogic powers are reflections of a penetration into the depths of consciousness, and are connected to ego identity. By entering into meditative absorption, the ascetic comes into contact with deep recesses of the unconscious that are interrelated to an area where symbol creating occurs that forms the foundation for culture. What Obeyeskere calls hynomantic states include dream, trance, ecstasy, and concentration, which form models for myths that are logically ordered and coherent, representing ancient forms of knowing with a narrative structure. This implies that a narrative myth is modeled on a dream, yet removed from dream, but the images created in the dream are consonant with the prevailing cultural symbols and meaning [20]. Thus culture and dreams influence each other. Developing the implications of Obeyeskere's position, although he does not mention ascetic powers specifically, we can affirm that powers are a product of hynomantic states developed into narratives.
If the ecstatic person subordinates ordinary, delusional reality to a deeper reality that governs that person's existence, is such a person irrational? Obeyeskere [20] gives two reasons why the ecstatic’s behavior is not irrational: "First, the ecstatic is acting in terms of the supramundane reality that he has constructed for himself; second, the average citizen does not see the behavior of the ecstatic as 'abnormal,' only different from his, but intelligible according to the central values of the culture that both share [21]." Moreover, the ecstatic continues to adhere to the pleasure principle because the new level of reality is meaningful and bearable. By taking into consideration extreme forms of asceticism, it is questionable whether or not the ascetic conforms to the pleasure principle as Obeyeskere claims because the ascetic represents a paradoxical exception to any pleasure principle.
Another scholarly viewpoint about the powers of ascetics is offered by Gerald Larson. After agreeing with previous scholars that Patañjali's assertion about the powers are obstacles to attainment of concentration, Larson acknowledges that the powers are part of the common experience for yogis. Larson cites two Sūtras (YS 3. 37; 3. 51) that embody a skeptical cautionary attitude toward the powers, which he claims proves that the powers are not intended to be taken literally. He concludes that "These powers are most likely imaginative (kalpita) fantasies that arise in the process of doing yoga" [22]. He goes on to claim that the powers do not play any role as signs or marks of progress on the path.
Larson’s evidence does not prove what he claims because the two textual references cited are both warnings and not skeptical expressions about whether or not the yogin actually gains and exercises such extraordinary powers. Moreover, Larson does not take the powers seriously. Why would Patañjali link samyama techniques with specific powers? This is a question that Larson does not answer. It is as if Larson cannot accept the possible reality of the various powers, and injects his personal skepticism into his interpretation, which is perfectly understandable for a person living in the twenty-first century that is far removed from the time period of the text compiled by Patañjali.
A different approach with respect to yogic powers is offered by Steven Phillips in his fine study of yoga philosophy. Since powers are an obstacle to concentration (samādhi), this is an excellent example of voluntarism, according to Phillips, because the "claim that siddhas follow upon thought and emotion coming under the control of the conscious being” [23]. What Phillips means by voluntarism is not simply a goal but also something that is an instrument, which means that concentration is part of the means to powers and not merely a final goal for the basic reason that it leads to something else. Therefore, the powers are a feature of the yogic path that cannot be renounced. From a critical perspective, Phillips argues that Patañjali's dualism of self and matter stands in opposition to his own yogic tradition of siddhas (powers), and the Indian philosopher does violence to the yogic tradition by setting aside the value of powers. Phillips offers the following judgment: "The ties between yoga practice and siddhas are in my judgment intrinsic, both culturally . . . and in psychological fact. No one counts as a master yogin or yoginl who does not possess siddhas”[24]. Phillips thinks that the fundamental message of chapter 3 of the Yoga Sūtras is that various powers flow from the practice of samyama.
Ian Whicher agrees with aspects of Phillips position especially the observation that powers are a natural by-product of the yogin's practice. As any worthwhile yogic instructor, Whicher warns that "Indulging in them only serves to inflate the ego and prevents spiritual growth precisely because the deployment of them presupposes that we invest our attention in the sensorial world or the desire for powers or control over it (reinforcing the subject-object duality, within prakrti that Yoga seeks to overcome) [25].” Whicher's observation is an echo of advice given by many yoga instructors and commentators over the centuries.
Finally, Sarbacker adopts the sociological theory of Pierre Bourdieu and its notion of habitus in order to interpret ascetic acquired powers, along with also contrasting the forces of doxa (worldview) and hexis (body culture) of a yogi. He thus states, “Psychic powers, in this interpretation, would represent the mastery of, or recovery of, the previously unconscious doxa and hexis, both of which in turn are reflected out into the world through communal experience [26].”
Sarbacker thinks that the community shares in the yogic powers of the ascetic, who strives to master his/her, inner psychic and somatic worlds and simultaneously one's relationship to the external world that theoretically gives power, control, and authority. In short, Sarbacker is saying that yogic techniques transform an ascetic internally, and this internal transformation affects the external world of the ascetic along with people who share his/her world. He explains further that "Whether literal or symbolic, actual or mimetic, the demonstration of yoga powers and the representation of such powers in literature encapsulate how the practice of yoga is a vehicle for the transfiguration of the human practitioner into a being of supernormal power and knowledge and a paradigm for a particular type of communal existence [27].” Sarbacker continues by sketching a series of interpretive possibilities.
Each of these learned opinions about the place of powers in the Yoga Sūtras have some merit. But I think that there is an additional way to approach the subject within the Indian religious culture. In order to do this, it is important to briefly review the history of Indian asceticism to actually understand more fully and contextually the compiling of the in the fourth century CE. This historical approach contributes to a tendency to take Patañjali seriously when he affirms that he is merely a compiler of an ancient tradition or several traditions.
A Brief Historical Sketch of Indian Asceticism
A Rg Vedic hymn (10.129) called the Nāradīya Sūkta, a creation hymn, might have been influential on the development of asceticism, but it, at least, provided a context and inspiration for later developments in ascetic life [28]. The puzzling hymn begins by recounting a primordial darkness covering a watery chaos. Then, a life force arises by means of tapas (heat, a term that is also used later to refer to the practice of asceticism) and desire also arises, which forms the first seed of the mind. By means of wisdom, the kavi (seer) establishes the bond of existence within non-existence, suggesting a creation of the world through mind, a primeval consciousness considered divine. Forming an association between the existent within the non-existent, this connection is discovered by seers by means of inspired thinking. Other than this kind of inspired type of thinking, the text does not refer to meditation or contemplation practices.
For whatever reasons, the sacrificial cult of ancient Indian orthodox religion was considered too confining, rigid, and static for some seekers of religious experience. Some practitioners interiorized some Vedic sacrifices, which dispensed with the necessity of priestly expertise as evident in some texts of the Upanisads, such as the mentally performed horse sacrifice in the Brhadāranyaka (1.2.5-7) performed by a person; mention is also made of the mental sacrifice, the offering of bodily parts as oblations, and sacrifice of the breath in the Chāndogya (5. 1923), and the Praśna (4.4) Upanisads where the mind becomes the sacrificer.
The majority of ascetic figures and movements existed outside of the dominant Vedic culture, although it is possible to find references to such groups as the long-haired Keśins and Vrātyas. In addition to their long hair, the Keśinswear dirty, discarded rags, wander naked or wear saffron colored robes that marks them as a renunciant group (RV 10.136.1-4). Reportedly, their alienation from the prevailing society placed them on the social margins much like the deity Rudra, who also resides on the margins of the social world in wild and dangerous places.
Sharing a conscious altering drug with Rudra, the Keśins could transform their condition into sensations of flight, able to read the mind of others, being able to transcend and view their bodies from a transcendent perspective, suggesting ecstatic experiences that are drug induced, although there is some scholarly debate about this point [29,30]. It is very likely that the Keśins, existing outside of the prevailing culture, represent precursors of later ascetic groups and share features with the early Buddhist, Jain, and other sramana (renunicant) movements.
Another marginal social group is the Vrātyas (a term referring to those who have taken vows) identified as wandering warrior ascetics, who practiced self-flagellation and other forms of extreme asceticism, traveling by means of bullock carts. Apparently, Vedic priests attempted to induce them to join the orthodox culture via purification rites. Not previously married or fully adult, these ascetics engaged in raiding expeditions for cattle, fighting, and small scale warfare in order to release their aggressive tendencies [31]. In addition to their martial exploits, they also perform Vedic rites in the forest for their community [32]. Retaining their leadership positions, some Vrātyas remained unmarried, while others played a role expanding the reaches of Vedic culture. They are described in the Atharva Veda (15) as dressed in black with two ram skins over their shoulders and wearing a turban. Their marginal status to Vedic culture is evident in a ritual called the “great vow” (mahavrata), a rite characterized by obscene dialogue and sexual intercourse with a prostitute by a leader that is preceded by breath control exercises [33].
In addition to these obscure groups mentioned in Vedic literature, there are also other ascetic groups referred to by the generic term śramana (renunciant) that are groups that include Jains, Buddhists, and Ājīvikas, originating historically around the fourth-fifth centuriesBCE. Calling attention to the martial imagery in Jain texts, Dundas draws a link between the śramana groups and the Vrātyas, who he thinks may have served as ascetic models [34]. This is disputed by Samuel because the Buddhist and Jain teachings are not martial in spirit and thus not a major predecessor for these movements, even if one grants the influence of some imagery and organizational structure [35].
During the historical period when Buddhists, Jains, and Ajlvikas ascetic movements were developing, Indian culture was experiencing several important changes that increased the chances of individuals adopting an ascetic lifestyle. Probably, the rise of urban life was a central motivating factor because it provided people with more liberty of behavior and thought that contributed to an atmosphere of changing values. The hot, humid climate and closer living arrangements fostered by urban life enhanced the spread of contagious diseases and death. Urban expansion and agricultural innovations were accompanied by population growth.
Economic changes increased job specialization and mercantile activity, which made increased travel necessary between the growing urban centers with their expanding populations. Buddhists and Jains found strong economic support from merchants, bankers, and kings. Political changes placed more power into fewer hands. The political, social, and economic flux caused uncertainty, gave rise to questioning the prevailing social hierarchy, reconsideration of the meaning of life, and contributed to alternative choices about lifestyle.
The types of historical changes affecting early Buddhism and Jainism can also be inferred from ancient Vedic and Upanisadic texts that testify to the existence of a religious skepticism, an anti-priestly bias, acknowledgment of the existence of ascetic groups, and an advocacy of ascetic practice in the form of yogic discipline. Within some Rg Vedic passages, doubts are raised about the existence of the gods based on the claim that no one has seen a particular deity (RV 8.89), and another passage indicates that people have doubts about the existence of gods (RV 2.12). These types of examples from the Vedic literature are indicative of the quest for absolute certainty and the absolute that forms a bridge to the Upanisadic literature and its secret teachings about the relationship between the self and Brahman (identified as the ultimate reality).
The Upanisadic texts overcome the priestly dominance by interiorizing some Vedic sacrifices and transforming them into mental operations performed by the individual without the services of priestly expertise as previously noted. The śramanas (ascetic groups) appear in the Brhādaranyaka Upanisad (4.3.22) in a negative association with thieves, abortionists, and two pariah groups (Chandalas and Pulkasas). A six fold path of yogi is prescribed by the Maitri Upanisad (6.18) that includes breath control, withdrawal of the senses, meditation, concentration, contemplation, and finally absorption, while a briefer version appears in the Mundaka Upanisad (1.2.11) that includes practicing the following two aspects: tapas (austerity) and sraddha (faith) in the forest.
It is difficult to know what the text means precisely with respect to these two practices especially the role of faith. What is remarkable is the close resemblance of the path of the Maitri Upanisad to the classical yogic path contained in Patañjali's compilation of the Yoga Sūtras. Not all Vedic texts are, however, advocates of an ascetic life-style because the Aitareya Brahmana (7.13-18) calls into question, for example, ascetic attire and the conflicting attitudes of householders towards ascetics that run the range of reverence to distrust [36]. And there evolves the widespread figure of the false ascetic, who is depicted as greedy, sexually dangerous, dishonest, and immoral [37].
It is precisely the acquisition of power that functions as a motivating factor for someone choosing an ascetic lifestyle in traditional India along with attempts to eradicate the effects of transgressions and ritual failures, and to secure a place in the afterlife [38]. And the later Upanisads suggest a search for an absolute entity as a motive because it was deemed necessary to go beyond the practice of tapas, which began to be understood to have limitations with respect to achieving a higher goal that embodied gaining control of and maintaining the universe [39,40]. Moreover, it was this historical tradition that shaped a thinker like Patañjali. And an aspect of literary history-verbal or oral-that also shaped Patañjali was the plethora of narratives about ascetics exercising powers gained through their regimen.
Narratives about Power
Besides the development of various ascetic/yogic types of movements that were often motivated by individuals seeking powers, the major epic texts-Mahābhārata and Rāmayāna-of Indian literature contain many narratives about the display and use of ascetic powers. According to the Mahābhārata (12.115119), once there was an ascetic of such goodness that flesh-eating wild animals were akin to his disciples in the forest.
A dog, weak and emaciated from eating only fruits and roots, like the ascetic, became attached to him out of affection, developed a tranquil demeanor, and heart similar to that of a human being. One day, a hungry leopard came to where they were residing and was about to seize the dog as its prey when the dog begged the ascetic to save him. The sage turned him into a leopard, and then, when a tiger attacked, into a tiger, and then a rutting elephant, and a lion. Now that he was carnivorous, all the other animals feared him and stayed away, and finally he wanted to eat the ascetic, who read his thoughts and turned him back into a dog, which was his proper form by birth. The dog moped about unhappily until the ascetic drove him out of the heritage. This narrative captures the ascetic's power to turn another creature into any form. Other parts of the great epic highlight other ascetic powers such as an ascetic’s possession of a divine eye that allows him to see into the future (Mbh 1.111.18-19), the ability to fly (Mbh 3.156.15), power to suddenly disappear (Mbh 3.289.24), or manifests control over nature (Mbh 3,109.6-9).
Similar types of ascetic powers can be found in the Rāmayāna with narratives about an ascetic who possesses power over human biology by being able to create a son for a woman by means of his mind (Ram 1.29.11-18). By means of his powers, another ascetic creates a beautiful pondcalled the pond of the five Apsarases (Ram3.9.11-12). The monkey Hanumān, a devoted servant of the hero Rāma, and his army get lost in a cavern where they encounter a female ascetic, and he asks her for help getting out of the cavern in order to accomplish their task of rescuing S&x012B;tā, wife of the heroic Rama. The female ascetic agrees to use her power to help the floundering monkeys, and instructs them to close their eyes, which frees them instantaneously (Ram 4.52.1-10).
According to the Sāmaññaphalasutta of the Digha Nikāya, the historical Buddha could become one or many, could become visible or invisible, pass through a wall, move through solid ground, remember previous births, walk on water, or travel crosslegged through the sky. The Samyutta Nikāya (2.212; 5.264-65) states that the Buddha can become one of many, suddenly vanish, pass bodily through a wall or mountain, travel like a bird, or touch the moon and sun. His mental powers (telepathy, clairaudience, and clairvoyance) and his wisdom surpass that of even the gods.
Even though these powers were evident of his advanced spiritual status, the Buddha is depicted rebuking a man who displays similar types of powers in the Cullavagga (5.7). According to this account, PindolaBhāradvāja, a disciple of the Buddha, rises into the air, takes a bowl from the top of a pole, and flies three times around the city. The Buddha did not favor such displays because it gave ordinary people the wrong impression about the importance of powers and could potentially distract a practitioner from the path to liberation.
Mahāvīra is no less powerful than the Buddha, according to Jain literature. TheĀkārāhga Sūtra (2.15.260) and the Kalpa Sūtra (121) offer similar accounts of the powers gained by Mahavira when he attains liberation by mentioning omniscience, knowledge of the condition of all worlds, remember former births, and ability to read other minds. What stands out about this list is the emphasis on mental powers over physical prowess. According to the Uttaradhyayana Sūtra (30.7-37), these powers are the by-product of six types of internal and six kinds of external austerities. The external austerities are fasting, five kinds of abstinence, collecting alms, abstention from rich food, mortification of the flesh, whereas the internal forms of practice include expiation of sins, politeness, serving the teacher, study, meditation, and abandoning the body.
Internal forms of asceticism focus on human attitudes, thoughts, and emotions, which cannot be perceived by others, whereas external forms are related to the interaction between ascetics and others, restricting association with worldly objects, and exposing ascetic practices to the gaze of others [41-43]. Any display of these powers is intended to glorify Jain teachings and to assist the flourishing of the religion.
Other bodies of literature relate narratives that highlight the powers of ascetic/yogic figures. A good example of additional literature is Puranas. Before these narratives were composed, they circulated orally within the culture as did the two epics. It does not take much of a leap of imagination to conclude that the historical development of various types of ascetic groups and individuals and the widespread oral and written body of narratives about the existence of powers shaped the mind of Patañjali when he compiled the Yoga Sūtras. Because ascetic powers were closely associated with ascetics and tales about them were prevalent, Patañjali would have been negligent if he had not considered them in his text. From one perspective, Patañjali acknowledges that these powers do arise, are genuine, and not something created by the yogi's imagination. This is an insider’s perspective and stands in sharp contrast to the scholars standing outside of the yogic tradition discussed earlier in this essay. From another perspective, Patañjali asserts that these powers are a hindrance to further spiritual advancement and the achievement of an aspirant's ultimate goal, which is release from the cycle of life.
Concluding Remarks
The narratives about ascetic powers from Buddhist, Jain, and Hindu texts are evidence of the popular folklore and convictions surrounding the life and exploits of ascetics/yogis. Thus, as asceticism in its many manifestations developed in ancient India, its historical evolution is accompanied by narratives depicting extraordinary powers. It is this plethora of narratives both oral and written-about ascetic powers that shape the attitude of Patañjali about the nature of yoga in the fourth century CE as he attempts to compile and systematize its techniques.
Since the association between powers and ascetic life is so pervasive in the culture, it is this pervasiveness and popular, unquestioning assumptions about asceticism to which Patañjali needed to respond. Acting as a compiler of the Yoga Sūtras, if we accept the traditional understanding of his role, Patañjali needed to make sense of a religious phenomenon-extraordinary yogic powers-in order to do justice to an aspect of asceticism that was unquestionably accepted by many Indians. Therefore, Patañjali included an entire section of the text devoted to a discussion and treatment of powers (siddhas) in order to treat his subject in a through manner, which suggests that various kinds of powers are an essential aspect of the ascetic/yogic life style. Moreover, the cultural context in which Patañjali lives, compiles, and writes calls for him to devote some of his text to making sense of ascetic powers. If Patañjali did not consider ascetic powers, he would have been negligent in his vocation. Instead, he takes the folk narratives and oral traditions seriously by devoting an entire chapter to a discussion of ascetic powers in a four chapter book, even though some scholars are perplexed by this alleged over emphasis on powers.
For more articles in Journal of Yoga and Physiotherapy please click on https://juniperpublishers.com/jyp/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#karma yoga#physical health#yoga#physiotherapy#juniper publishers#meditation#juniper publishers high impact journals#high impact factor journals#open access publishers
1 note
·
View note
Text
Sensory Transcendental Therapy

Authored by Karen Phillip
Introduction
As my research and practice in the field of counseling expands, I see the clear and positive results of current standard therapies. However, I find a gap in the speed of progression that could be improved with a more developed combination of these therapies. I have therefore developed a Sensory Transcendental Therapy (STT), which aims to engage the person out of their comfort zone; get outside and become aware of how all their senses engage; move physically to stimulate the body, mind and processing and be aware of how the counseling discussion enhances or dims certain sensors of the person. While standard methods of counseling show benefits, it takes too long to get major progressive benefits for some patients. Adding all sensors, stimulating mind and body and challenging them with pattern interrupt will create a more complete therapeutic tool. Many counselors are not trained in this practice at all. I have learned much as a clinical hypnotherapist, and so wish to combine some of those parts with counseling-enhanced skills. The therapy combines aspects of standard therapies such as Cognitive Behavioural Therapy, while considering research which tells us outside environments and movement allow us to process faster and with more clarity.
Research and outline
Sensory Transcendental Therapy (STT) can be described in the following phrase: A psycho-therapeutic counseling session that is held outside the frame of a clinical counseling office. The patient is encouraged to feel more at ease and take in nature (including sight, sounds, feelings, smells of the environment) during a side-by-side walk with a therapist. An outdoor walk takes the person to new and different places, out of their comfort zone, and enables them to more freely discuss their issues.
STT can be likened to Walk and Talk Therapy (WTT), where clients are encouraged to walk side-by-side with the therapist in an outdoor scenario. However, STT takes a more developed and structured approach, incorporating reflective pauses, analysis of body language and Cognitive Behavioural Therapy (CBT) or Solution Focused Therapy, while retaining the benefits of WTT. WTT has reported positive results for psychologists who have practiced it with difficult or ‘closed’ patients, many of whom find the enclosed one-on-one of a counseling room too intimidating to ‘open up’ and understand their issues [1,2].
Movement has long been seen as an excellent supplement to therapy, with research showing vast improvements on the severity of depression diagnoses after periods of prescribed exercise [3]. Building on this theory, simultaneous non-strenuous exercise and counseling has been found to be more effective in treating depressive symptoms than standard counseling [4].
Using the outdoors as a setting for psychotherapy has also been proven to have positive effects on the speed of breakthroughs with patients who find it difficult to ‘open up’ in a formal counseling scenario. When outside and experiencing nature, patients have reported feeling more calm and aware of their own thoughts, and reported a generally more positive frame of mind [5]. The ‘frame’ of psychotherapy is a concept that a therapist has to be very aware of when conducting sessions outside the confines of a designated room. The ‘frame’ describes an image of confidentiality and therapist-client relationships, which must be adhered to in order to keep the safety and integrity of psychotherapy treatment [6]. By taking the ‘frame’ of a session outside, the counselor must ensure that the patient is comfortable with this, and that the experience should be treated no differently than a standard counseling session. STT replicate all of the benefits described.
Therapy session description
A one-hour therapy session could consist of a 10-minute walk, with the client being encouraged to employ all their senses by touching the flowers, smelling the air and viewing the environment. If the client feels any thoughts or feelings rising during this time, they are asked to bring these forward. This could be followed by a five-minute pause, to apply CBT where necessary.
A particular topic could be applied to a session, such as a rise in anxiety or an unexplained drop in mood. There would be a time to stop, sit and look directly at the person to enhance the therapy used, which would be CBT and solution focused. This approach could then be evaluated, and the patient asked if they want to continue walking for longer or if they feel more comfortable stopping after 10-15 minutes. STT sessions can be designed to suit the patient and their particular needs. If the client expresses a major emotional moment during a session, this is when a pause would be suggested to discuss the pattern of the thoughts. The problem would be tackled using traditional therapeutic remedies, and more positive thought processes would be encouraged.
The inherent problem with traditional therapy is that most depressed or anxious people fail to see their available options during a time of panic; this leads to feeling stuck and lost. An outdoor setting is provided to show the patient a more relaxing view of the world, in the hope that they can see the 'bigger picture'. It should also be noted that some patients may also withhold thoughts and feelings from a therapist - this is part of the process and is often alleviated once rapport is established. The patient's body language should be taken into account. Do they appear nervous? Are they interested in the environment, or withdrawing into themselves? These should be noted and discussed at an appropriate time.
Conclusion
There is currently little written on walk-talk therapy and nothing on STT, as this is new, but all research does point to the advantages of the being outside and including movement in sessions. While WTT does include this to a degree, it differs from STT in that it does not seem to engage all sensors. I have used STT now for over 2 years and found clients' responses are enhanced and expedited. About 40 people have used STT against non-STT treatments and results were faster for those using STT; all patients involved had similar issues and needs.
For more articles in Journal of Yoga and Physiotherapy please click on https://juniperpublishers.com/jyp/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#karma yoga#physiotherapy#yoga#physical health#open access journals#high impact factor journals#juniper publishers#meditation
2 notes
·
View notes
Text
Mindfulness Practices that Can be Implemented in the Regular Classroom

Authored by Dorothy Sisk
Introduction
Gandhi's words remind us that as teachers working with children and youth, we are agents of change. Mindfulness can provide insight to enable teachers and administrators to envision and create a new model or approach to education. Mindfulness is not a new idea since William James [1] said, “The faculty of voluntarily bringing back a wandering attention, over and over again, is the very root of judgment, character and will.” This is mindfulness, as James continued, “an education which should improve this faculty would be the education par excellence.”
Mindfulness is being aware of what is happening within us and around us with a clear focus of our attention on moment-to- moment experience in the here and now [2]. Gifted students are sensitive and have great depth in their thinking and feeling, and these characteristics can be positively directed with mindfulness activities. As gifted students engage in mindfulness activities, they can strengthen their inner awareness and vision. However, their sensitivity and depth in thinking and feeling can result in painful experiences when gifted students feel out of sync with other students and their teachers [3].
Mindfulness has ancient roots; but, incredible applications employing mindfulness activities are being made daily in medicine, business and education. Two very different people Thich Nhat Hanh, a Vietnamese Buddhist monk and an American medical physician Jon Kabat-Zinn have worked with mindfulness over the last 40 years, with amazing contributions. More and more educators are viewing mindfulness activities as a viable strategy and practice to use with students to enhance mental, emotional, physical and spiritual wellness.
Thich Nhat Hanh [4] has written five books in the Mindfulness Essential Series including How to sit which provides clear and simple directions for exploring mindfulness. The second book How to relax [5] addresses the daily stress that makes us less productive and less happy. In this book Thich Nhat Hanh shares techniques for bringing your life back into balance. The third book How to walk [6] reminds us that we touch the Earth with awareness, and to stop sleepwalking to arrive fully in the present moment. The fourth book How to Love [7] brings clarity, compassion and humor to the essential question of how to love. The fifth book How to Eat [8] tells how the process of eating can be a joyful and sustainable activity, including preparing the food, and even cleaning up after the meal. In How to Walk [6] Thich Nhat Hanh emphasized love of the Earth, and he said we can express love of the Earth with each step. You can say:
a. With each step
b. I come home to the Earth
c. With each step
d. I return to my source [6].
Jon Kabat-Zinn began his work in mindfulness by establishing the Mindfulness-Based Stress Reduction (MBSR) clinic at the Massachusetts Medical Center in l979. At that time, the word mindfulness was nowhere in the medical lexicon. Today, nearly 23,000 certified MBSR instructors teach mindfulness techniques, including meditation and the clinics are in nearly every state in the United States and in more than 30 countries.
Early on Kabat-Zinn worked with treatment resistant patients of other doctors, and after 8 weeks of mindfulness training, the treatment resistant patients showed remarkable transformation. The MBSR patients had symptom reduction in blood pressure, psoriasis, and fibromyalgia, and patients with chronic pain disorder reported a greater sense of wellbeing [9,10]. Randomized controlled trials and studies show impressive reduction in psychological morbidity, stress and enhanced emotional well-being in non-clinical samples [11] Kabat Zinn reported that participants in MBSR training tend to speak of the mindfulness experience as transformative [12].
Sense of connectedness
Mindfulness builds a sense of connectedness, and recognition of the similarities in people. In today's classroom with the growing diversity of the student population, it is essential that all students are encouraged to develop a respect and connection with others. One powerful mindfulness activity that positively impacts the need for connection is deep listening. Deep listening involves giving full attention to another person and maintaining a present-centered awareness. Gifted students with their many interests and deep passion for their individual projects may find deep listening a challenge. Many gifted students report they give minimal attention to their teachers until they "hear" something they don't already know or are of interest to them. This behavior can be problematic in gifted student-teacher interaction. All students can benefit from deep listening not only for academic achievement, but for greater social awareness and ability to get along with others. Several programs have been developed to help teachers integrate mindfulness into their regular classrooms.
Care
Patricia Jennings [13] a professor from the University of Virginia developed CARE a mindfulness program for students and teachers. The goal was to promote a wholesome way of learning and living. Students reflect on their patterns of behavior, thoughts and emotions in journals. As they engage in reflection, students can see the importance of taking responsibility for building positive interactions with their teachers and other students.
Transformative life skills
Jennifer Frank, a professor at Penn State University collaborated with Niroga Institute to develop the program called Transformative Life Skills (TLS). The program combines mindful yoga, breathing techniques and meditation. The three core practices are action, breathing and centering. Action includes mindful movement and yoga postures; the breathing component helps individuals manage stress; and the centering component brings awareness to the present moment. A pilot study of TLS found the program reduced stress and improved well-being in a sample of 49 high-risk high school students [14].
Learning to breathe
Learning to Breathe was developed by Patricia Broderick [15] and it is based on six themes following the acronym BREATHE. B is for body awareness, R is for reflection and understanding, and working with thoughts, E is for understanding and working with feelings, A is for integrating awareness of thoughts, feelings, and bodily sensations, T is for tenderness, taking it as it is, and reducing harmful self-judgment, H is for habits for a healthy mind, integrating mindful awareness into daily life, and E is for empowerment. Metz et al. [16] in their research found high school students engaged in learning to Breathe reported lower stress levels, negative effect, psychosomatic complaints, and increased levels of efficacy and emotional regulation.
Inner kids
Susan Kaiser-Greenland designed Inner Kids with a focus on attention, balance and compassion. The program seeks to develop awareness of inner experiences, one's thoughts, emotions, and physical sensations; awareness of outer experiences of other people, places and things; and the importance of how these two inner and outer experiences blend together. Inner Kids was found to be particularly helpful in working with students [17]. In addition, Inner Kids helped address the emotional issues that students experience, including their use of intellectual power. Their speed of thought, high level questions and comments often cause rejection by classmates and gifted students may need help in understanding this rejection.
Mind up
MindUp focuses on four areas: 1) How Our Brains Work, 2) Sharpening Your Senses, 3) it’s All About Attitude, and 4) Taking Action Mindfully. MindUp is integrated into most elementary schools in the southern mainland of British Columbia, Canada, and in the United States, the program was adopted by the city of Newark, New Jersey. MindUp was developed by the Hawn Foundation in British Columbia when actress Goldie Hawn lived in Vancouver. Kimberly Schonert-Reichl conducted several research studies of MindUp and reported that students in the program were more optimistic and self- confident and their teachers said they demonstrated more social competence [18].
Kripalu schools
Kripalu Yoga in Schools (KYSIS) works with adolescents to help them learn social and emotional regulation, stress management, self-appreciation and self-confidence and relationship skills. A pilot study of the KYSIS program integrated yoga and mindfulness activities into regular high school programming. Noggle et al. [19] reported that the KYSIS students showed improvement in mood disturbances of students and lessened their anxiety.
Mindfulness activities with high school gifted students
The Texas Governor's School (TGS) is a residential program for high achieving and high ability students from throughout the state of Texas. In 2017, the staff and director decided to plan and implement a mindfulness program for the 73 students attending the three week program using the evidence based research and suggested activities of five Mindfulness programs (Kripalu Yoga, MindUp, Breathe, Inner Kids and Transformative Life Skills. Specific activities were selected including Mindful Walking, Awareness Breathing, Belly Breathing, Mindful Movement, Mindful Eating, Visualization and Loving Kindness Meditations.
Awareness Breathing included the students watching and becoming aware of breathing in and out. They breathed in and counted l-2-3, held the breath 1-2-3 and exhaled 1-2-3. Belly Breathing involved placing an object or pillow on the stomach of each student and watching and feeling it rise and fall with each breath. Mindful Walking involved the students in walking slowly around the track at the University while concentrating on their deep breathing and paying attention to their senses, noting what they were hearing, seeing, smelling or feeling as they walked. The following gatha was used:
a. Breathing in, I am aware of my feet.
b. Breathing out, I smile at my feet.
Mindful movement included several yoga positions including the Sun Salutation which they did with their counselor each morning before breakfast. Mindful Eating involved the students tasting a raisin and holding it in their mouth for several minutes before finally swallowing it. They also tasted a marshmallow with the same intense concentration. A snack meditation with tangerines was used with the students eating the tangerine slowly and mindfully as if it were the most important thing for them to do in their life.
Visualization included a number of visualizations provided by Dr. Sisk involving the classic Three Boxes developed and demonstrated by Maslow [20] and the wise seer on the mountain from the book the Growing Person [21]. Loving Kindness included a number of Loving Kindness mantras using several of Thich Nhat Hanh's gathas in his five books, and a favorite from Goldstein [22] was:
a. May I be happy
b. May I be peaceful
c. May I be free from suffering.
Go to
Participants and Methodology
The students ranged in ages 14-18 in grades 10-12. The mindfulness sessions were 30 minutes daily M-F. Each student was assigned to a counselor and the group of students ranged from 10-12 students in a "family." The counselors reinforced the strategies in evening sessions with their family of students. Observations indicated that most students were able to block out any noise or distractions during the mindfulness exercises. Dr. Sisk, the director trained the counselors in the use of the mindfulness strategies, and she conducted the meditation and visualization sessions. Each of the students wrote a daily reflective journal entry after the mindfulness activities. These entries were examined for themes. Themes that emerged were a feeling of calmness, sensory awareness, enjoyment, and a sense of peace.
The students were administered a Mindful Attention Awareness Scale that was developed by Ruth Baer at the University of Kentucky. In addition, the students were also administered a Leadership Skills and Behaviors Scale developed by Sisk [23] that measures self-concept and motivation.
Results
Pre-test scores in Mindfulness were 3.95 and post-test scores were 4.28. Pre-test scores in self-concept were15.33 and posttest scores were 16.92. Motivation [24] pre-test scores were 23.90 and post-test scores were 25.18. Paired t test results showed significant difference in the three test scores at the .0l level.
Conclusion
In our troubled times, mindfulness offers a strategy particularly suited for gifted students to reduce their anxiety and stress, but mindfulness can be implemented with all students of different abilities. It will be important as teachers approach the use of mindfulness [25] with their students, that they do so with an open-heart, present moment, nonjudgmental awareness. The benefits for both the teacher and the students will be life changing. One easy way to get involved in incorporating mindfulness in your life and in your classroom is to connect with others who are trying to do the same thing. Websites and resources in the references of this article will help get you started, and there are free audio recordings of guided mindfulness practices that you can download. Mindfulness activities and programs can truly transform your classroom.
For more articles in Journal of Yoga and Physiotherapy please click on https://juniperpublishers.com/jyp/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#karma yoga#physiotherapy#yoga#physical health#open access journals#high impact factor journals#meditation#juniper publishers
4 notes
·
View notes
Text
Polymers of Natural Origin in Advanced Study of Research: Fabrication of Pharmaceutical Delivery Device

Authored by Roy H
Abstract
Polymers assume a noteworthy part in the improvement of medication conveyance innovation by arrival of two sorts of medications like hydrophilic and hydrophobic. In a synchronized way and consistent arrival of plans over broadened periods. There are various favorable circumstances of polymers going about as a dormant transporter. Nonetheless they have their own particular impediments, for example, the polymers regularly delivers undesirable and undesirable symptom, immunogenic enactment potential, should have been surgery after they discharge the medication at the focused in the vicinity and cost additionally a potential element. In such respects, Natural polymers turned out to be the better option limiting the risk of disappointment of medication conveyance framework.
Keywords: Polymers; Hydrophillic; Natural; Immunogenic
Go to
Introduction
Polymers are substances whose particles have high molar masses and compacted of a substantial number of rehashing units. Polymers can shape particles of strong dose frame and furthermore can change the stream property of fluid dose shape. Polymers are the foundation of pharmaceutical medication conveyance frameworks. Polymers have been utilized as a critical instrument to control the medication discharge rate from the definition. They are likewise for the most part utilized as stabilizer, taste-production operator, and proactive specialist. Present day progresses in medication conveyance are currently predicated upon the levelheaded outline of polymers customized particular load and built to apply unmistakable organic capacities. Polymers are both normally happening and manufactured. Among normally happening polymers are proteins, starches, latex and cellulose. Manufactured polymers are created on an extensive scale and have a numerous properties and utilized. Two or three audit articles on normal gums are accessible in literary works. A portion of the surveys secured the compound structure, event and creation of exudate gums, their size and relative significance of the different players on the world market and concentrated on their application in sustenance and different regions. Because of the developing enthusiasm for the utilization of characteristic polymeric materials as pharmaceutical excipients, as exhibited by the quantity of distributed logical papers, it is hard to cover all that may be accessible in a solitary article. It is proposed in this survey to talk about the employments of normal polymers as excipients in pharmaceutical definitions. Particular specify is made of a portion of the normal items as of now being used as pharmaceutical excipients and those being looked into for this reason [1-4].
Go to
Natural Polymeric Materials
Cellulose
In higher plants, cellulose is a basic auxiliary part and speaks to the most plenteous natural polymer. Cellulose is a straight unbranched polysaccharide comprising of β-1,4- connected D-glucose units and many parallel cellulose particles which frame crystalline small scale fibrils. The development of subsidiaries of cellulose is made conceivable by the hydroxyl moieties on the D-glucopyranose units of the cellulose polymer to give an assortment of subordinates. Cellulose subordinates can be made by etherification, esterification, cross-connecting or unite copolymerization. Etherification yields subsidiaries, for example, hydroxyl-propyl-methylcellulose and carboxyl-methyl- cellulose, while esterification brings about subordinates which incorporate cellulose nitrate, cellulose acetic acid derivation and cellulose acetic acid derivation phthalate. These subordinates have discovered application in layer controlled discharge frameworks, for example, enteric covering and the utilization of semi-penetrable layers in osmotic pump conveyance frameworks [5,6].
Pectins
Pectins are non-starch, direct polysaccharides removed from the plant cell dividers. They are prevalently straight polymers of predominantly (1-4)-connected D-galacturonic corrosive buildups hindered by 1,2-connected L-Rhamnose deposits. Smaller scale particulate polymeric conveyance frameworks have been accounted for as a conceivable way to deal with enhance the low bioavailability attributes saw in standard ophthalmic vehicles [7].
Gums and mucilages
Gums are regular plant hydrocolloids that might be delegated anionic or nonionic polysaccharides or salts of polysaccharides. They are translucent, undefined substances more often than not delivered by plants as a defensive after damage. Gums, adhesive, pectins and celluloses are delegated substances that are buildups of pentoses and additionally hexoses. They have various applications as thickeners, emulsifiers, viscosifiers, sweeteners and so on in confectionary, and as covers and medication discharge modifiers in pharmaceutical measurements frames. Be that as it may, the vast majority of the gums in their putative shape are required in high fixations to effectively work as medication discharge modifiers in dose frames because of their high swellability/dissolvability at acidic pH. Henceforth, gums should be changed to adjust their physicochemical properties. For instance, the change of gums through derivatisation of useful gatherings, uniting with polymers, cross-connecting with particles and different methodologies and additionally the variables impacting these procedures in the quest for making them appropriate for altering the medication discharge properties of pharmaceutical dose frames [8,9].
Alginates
Alginates are characteristic polysaccharide polymers secluded from the cocoa ocean weed (Phaeophyceae). Alginic corrosive can be changed over into its salts, of which sodium alginate is the significant shape presently utilized. The scientists officially planned bio-cement sodium alginate microspheres of metoprolol tartarate for intranasal systemic conveyance were set up to dodge the principal pass impact, as an option treatment to infusion, and to acquire enhanced helpful viability in the treatment of hypertension and angina pectoris [10].
Carageenans
The carrageenans are sulphated marine hydrocolloids acquired by extraction from kelp of the class Rhodophyceae, spoke to by Chondruscrispus, Euchemaspinosum. Thinks about have demonstrated that the carrageenans are appropriate in the definition of controlled discharge tablets [11].
Xanthan gum
Xanthan gum, a complex microbial exopolysaccharide delivered from glucose aging by Xanthomonas campestrispv. Xanthan gum has been utilized as a part of an extensive variety of businesses including sustenance, oil recuperation, makeup and pharmaceutical ventures. This wide application is because of its prevalent rheological properties. It is utilized as stabilizer for emulsions and suspensions [12].
Gellan gum
Deacylated Gellan gum (Gellan) is an anionic microbial polysaccharide, emitted from Sphingomonas elodea, comprising of rehashing tetrasaccharide units of glucose, glucuronic corrosive and rhamnose buildups in a 2:1:1 proportion. The physical gelation properties make this polysaccharide appropriate as an organizing and gelling operator in sustenance businesses. Gellan is additionally misused in the field of altered arrival of bioactive atoms. Fluid arrangements of Gellan are utilized as in situ gelling frameworks, for the most part for ophthalmic readiness and for oral medication conveyance [13].
Rosin
Rosin is a low atomic weight (400Da) normal polymer got from the oleoresin of Pinussoxburghui, Pinuslongifolium and Pinustoeda. It has as parts abietic and pimaric acids. Rosin and its subsidiaries have delighted in developing parts in Pharmacy. They have been explored for microencapsulation, film-framing and covering properties, and as grid materials in tablets for managed and controlled discharge [14].
RosHakeagibbosa gumin
The muco cement and maintained discharge properties of the water-solvent gum acquired from Hakeagibbosa (hakea), for the detailing of buccal tablets. Level confronted tablets containing hakea were figured utilizing chlorpheniramine maleate (CPM) as a model medication had been explored [15].
Chitosan
Chitosan is a straight polysaccharide made out of arbitrarily appropriated β-(1-4) connected D-glucosamine and N-acetyl-D- glucosamine. It is made by treating shrimp and other shellfish shells with the soluble base, sodium hydroxide. It is likewise normally exhibit in a few microorganisms and growths, for example, yeast. Analysts are being attempted chitosan as base for arrangement of Micro particulate medication conveyance framework and gadgets [16].
Conclusion
It can be concluded that, there a lot more research awareness should be promoted from primary label to the extent of deep study.
For more articles in Global Journal of Pharmacy & Pharmaceutical Sciences please click on https://juniperpublishers.com/gjpps/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#pharmacy#snorting drugs#juniper publishers#open access journals#high impact factor journals#open access publishers#pharmaceutical#pharma#healthinnovations
0 notes
Text
Be Positive: the Yoga Way

Authored by Subhash Sharma
Our thinking have a profound effect on our physical and emotional health. People who constantly keep focusing, in their routine life, on negative thinking, lead themselves towards low self-esteem and depression, and they are prone to suffering with unrelenting stress. In the situation of negative thoughts and stress the phenomena of flight-or-flight is operating with full swing which creates imbalance in hormonal profile dominated by Adrenaline and Noradrenaline hormones, causing hyper physiological states associated with uncontrolled psychological distortions. Positive or negative thinking are processes not inherited. In fact it depends upon how we perceive any situation. It’s a learned response, a kind of habit we develop over years of absorbing the attitudes of various kind of stimuli around us. Positive thinking helps keeping the physiological functions in the standard range and appropriate mind-body communication, which ultimately leads to the state of good psycho-physiological health. Contrary to that negative thinking causes detorioration in physiological functions as well as break down in the in the pathway of mind-body communication thereby causing various states of psychosomatic disorders. If we intend to achieve the target of happy and healthy living, we should strive to shed negative thinking and remain positive in our thinking and action too.
Major detrimental factors for negative thinking are exaggerating the circumstances, ignoring the positive aspects of the situation, personalizing every issue, either or thinking habit, over generalizing the people around us and premature jumping to conclusions. If we want to address these problems and factors it may involve major three steps- (i) Awareness, (II) Answering every negative thought without any delay or postponement, (III) Appropriate action. Six basic rules are involved in these three steps: (i) To place ourselves in a receptive state of mind, (II) To enlist the strong affirmations, (III) To always live in the present, (iv) To avoid negative phrases, (v) To remain firm on the positive opinion without least doubt, (vi) To remain accommodative. To achieve the above-mentioned target Yoga is a cost effective and easy to learn remedy and have its firm efficacy beyond doubt. Eight steps of Maharshi Patanjali’s Yoga technique are there having the treasure of benefit to create a personality with positive thinking, which may be summarized as under:
1. Yamas & Niyamas (code of conduct): helps the individual to get rid of any kind of fear and/or anxiety or stress.
2. Asanas: Keep the tone of neuromuscular system in dynamic state and modulates the organic functions which helps bringing in the state of homeostasis.
3. Pranayam: fulfills the energy requirement of the individual and brings in the mind and body in very proximity for proper communication between them.
4. Prathyahaar: Helps restraining the special senses from any kind of deviationfrom positive to negative.
5. Dharna: Helps in sitting appropriate goal of action of positive thinking.
6. Dhyan (Meditation): Most effective and vibrant practice promoting mind-body communication.
7. Samadhi: Bringing in the state of tranquility.
All kinds of sufferings, both physical and mental, are having their origin in the negative thinking. Whatever we have in our mind, only that will be exhibited by the body. Hence mind body communication is the key factor of good health and wellbeing, and that can be achieved by positive thinking only, and Yoga is the only tool which bring in the balanced state of mind body communication.
same quantum of light is flowing through every human being. Once we realize Light in our hearts we are ready to take steps and quantum jumps towards higher evolution taking us beyond biological/ Darwinian evolution. This will create a paradigm shift from ‘survival of the fittest to leave behind the rest’ to ‘arrival of the best to lead the rest’. This is also the essential message of VYOMA: Vedanta, Yoga, Meditation and Awakening for all.
For more articles in Journal of Yoga and Physiotherapy please click on https://juniperpublishers.com/jyp/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#journal of yoga and physiotherapy#yoga#physiotherapy#physical health#open access journals#juniper publishers#peer review journals#high impact factor journals#yogaposes#yogaeverywhere#meditation#yogapractice#open access publishers
1 note
·
View note
Text
Light in My Heart

Perspective
Let noble thought come to us from all direction, Rigveda
Let noble thoughts Go from us in all directions, Quantum Rope
Big Bang led to creation of this world from Shunya in the form of light and clouds of waves and particles. Human beings arrived on the earth much later. They arose from the light and clouds of waves and particles. Thus, they are also product of creation from shunya and carry in their heart the sparks of the 'original light'. After their arrival, they were under wonderment and wondered at their own life and origin of the 'Original Light' as well as unfolding of Shunya in terms of matter, mind and consciousness.
Wonderment led to curiosity and later scientists started studying nature of Nature and nature of light. From their study they discovered that light is both wave and particle. Further, light led to an understanding of space and time. Newton concluded that space and time are Absolute. Einstein imagined moving with speed of light and from such an initial imagination came some interesting insights such as mass energy equivalence which found expression in famous equation, e = mc2. Space and time are not Absolute concepts but are relativistic concepts, he concluded. Further, light is the ultimate limit in the universe. His formulations led to a major paradigm shift in human thinking with respect to light, space, time and related concepts. In my book, Quantum Rope (1999) I suggested a more generic equation e = m cn (Sharma 1999), wherein e represents energy, m represents matter and c represents consciousness and n can be 1,2,3, ...representing the expanding circles of consciousness. At the physical level, consciousness (c ) is represented by light and thereby by speed of light (c). While Einstein's equation is at the physical level, e=mcn is at the generic level including all sheaths (koshas) of human existence and it represents equivalence of matter, energy and consciousness from the spiritual perspective. When consciousness expands like the oceanic waves, human beings reach higher levels of consciousness beyond the physical notions of space and time. In fact, e = mcn can be considered as a spiritual equation, as it suggests evolution towards nirvana (n) or 'zone of eternity’ (represented by n in this equation). It also represents the 'ahm brahmasmi' state of consciousness. In this equation, m, e, c, n also represent gross, subtle, supra-subtle and astral states of mind and these are broadly in consonance with waking, dream, deep sleep and trance (Samadhi) states of consciousness. In the equation, e = mcn, we find an interconnectivity among various states of consciousness.
Einstein imagined moving with 'speed of light' and gave us his famous ideas and theories. Once I took liberty of poetic imagination and this led to a poem under the title, “Velocity of Light’ that was published in my book, Quantum Rope (1999, p.13). In Physics, light is considered a scalar quantity, however, when viewed from spiritual perspective, light guides and provides a direction, hence, it can also be considered vector quantity. This provides the reason for title of the poem as “Velocity of light' instead of 'Speed of light’. In this poem Einstein’s idea of twin paradox is also captured. The poem is as follows:
You said long time and no see
I had met you tomorrow near the sea
You said we have met somewhere
I had met you in your future
Because I was travelling with velocity of light
And you were travelling with velocity of kite
I went out on a tour of galaxies
My classmates were still hiring taxies
When I returned home, I was in a younger mould
My classmates had grown very very old
Because I was travelling with velocity of light
And they were travelling with velocity of kite
(Velocity of light, quantum rope: science, mysticism and management, Subhash Sharma, 1999, p.13)
When you light a lamp or candle or switch on light, the darkness is removed. Thus light gives us a lesson that there is no need to Fight. In fact there are three types of individuals viz. those who use 'Fight' approach, those who use 'Flight' (Moving to another space or place/ Flight of Imagination) approach and those who use 'Light' approach to achieve success. Believers in Fight approach tend to give a negative meaning to Flight approach as they equate it with escapism. However, 'Flight' approach can also be a creative as example of Sri Krishna shows us. He took 'Flight' approach (left Mathura to create Dwarika) and used it in a creative way to create a new city and a new perspective. Further he also took the Light approach to enlighten the whole world through his new insights as is evident from Gita. When individuals take the Light approach, they act like the lamp or candle, spreading their ideas and wisdom to remove darkness. Buddha said, become a lamp and remove the darkness. In fact it is up to an individual to follow any of these paths. His/her choice depends on his/her awareness, awakening and self evolution stage. Through light of knowledge, wisdom and consciousness, ignorance is removed. Light is a symbol of noble thoughts. By lighting the lamp of knowledge ('knowledge lamp'), we spread the noble thoughts in all directions.
As I reflected and meditated on the deeper meaning of LIGHT in terms of five letters of its spelling, it led me to a new meaning of LIGHT in terms of Light (L), Infinity (I), God (G), Harmony (H), Truth (T). This LIGHT led me to the following LIGHT Equation:
L = I = G = H = T
Light (L) = Infinity (I) = God (G) = Harmony (H) = Truth (T)
Thus, Light is Infinity, Light is God, Light is Harmony and Light is Truth
This interpretation of LIGHT provides us a new vision and this vision can be expressed in terms of following four principles:
Light is Infinity, Infinity is Light ( L = I)
Light is God, God is Light (L = G)
Light is Harmony, Harmony is Light (L = H)
Light is Truth, Truth is Light (L = T)
It may be observed that Gandhi’s famous quote, God is Truth and Truth is God ( G = T) is a derivative of these principles. Further all religions refer to these principles in one form or other. In fact this interpretation of LIGHT provides us the Oneness vision of all religions and spiritual traditions.
I may indicate that the 'LIGHT Vision’ suggested here is essentially a realization of 'Light in our hearts'. In 1993, I wrote a song titled as 'Light in my Heart' and it was published in my book, Creation from Shunya. This song was adopted in 1996, by first batch students of WISDOM (Women’s Institute for Studies in Development Oriented Management), Banasthali University, Banasthali, Rajasthan, as 'Wisdom song'. This song can also be considered as a 'song of light'. Some lines of this song are as follows:
There is light in my heart
It is there from the start
Its mystery you want to know
It says hello hello ...
It give me a peep
Into things that are deep
It has a beautiful glow
It says hello hello .
It shows silver lines
Bending space and time
In nature's beauty show
It says hello hello .
This light is divine
It makes us fine
Its flow is very slow
It says hello hello ...
(Light in my heart, creation from Shunya, Subhash Sharma, 1993, p. 33)
Let this 'LIGHT Vision' in the form of 'LIGHT in our hearts', spread in all directions for the benefit of all. This vision represents the essence of the 'Wisdom, Consciousness and Light of India’ that many across the world are seeking to create a new vision for the world based on a consciousness shift from fight to light - from lower levels of consciousness to higher levels of consciousness. Realization of 'Light in My Heart' has the potential of transforming the world in to Pragyasthan(A Place of Wisdom), where Science (Scientific temper and scientific approach, Rationalistic worldview), Heart (Heartistic approach, Heart values, Human values) and Spirituality (Spiritual temperament and spiritual approach) find a new integration for the benefit of the whole world. In modern society, Head is given primacy over Heart even though Head owes its vitality to Heart because Heart is the source of blood supply to Head. This implies that science and rationality are incomplete without human values and spirituality. This realization dawns when we realize 'Light in our hearts'
Light in my heart as a step towards higher evolution
Darwin to divinity: Above discussion takes us towards a model of "Arrival of Human Beings and Self evolution". In the beginning of this article, we mentioned about creation of this world from the 'original light' and clouds of waves and particles that took shape in the form of Panchmahabhutas (Five elements). 'Natural interactions’ along with various 'permutations and combinations' among five elements combined with natural 'quantum churning’ arising from natural interactions, lead to creation of life in various forms. This led to 'arrival of human beings’ from the 'clouds’. This perspective based on 'creation from shunya' provides us a new approach to creation and evolution of life including human beings. Original Light is embedded in the heart of every human being and this provides the basis for higher evolution of human being towards realization of this light within. Darwin dealt with evolution through natural selection at the Biological level. It may be indicated that at biological level, human beings are no different from animals and are particularly very close to certain species. However, they differ from animals because of more developed neuron structures in human mind. Sri Aurobindo was concerned with human evolution at the mind and consciousness level. Dasavatara theory of evolution represents an integral approach to evolution wherein we find an integration of the matter, mind and consciousness (mmc) approaches to human evolution. This integration suggests that 'Shunya Unfolding’ (SU)' has been taking place in a natural way in terms of matter (gross level), mind (subtle level) and consciousness (supra-subtle level)) and this 'natural unfolding' is represented by Body, Heart and Spirit (BHS). As we transcend Body (gross), Heart (subtle) and Spirit (supra-subtle) levels, we realize our cosmic/ divine/astral nature that has been referred to as 'aham brahmasmi’. Thus, we have following perspectives on human evolution:
a. Creation from Shunya: Arrival of life from the clouds of waves and particles
b. Darwin’s theory of evolution: Biological perspective on evolution
c. Aurobindo’s perspective of mind evolution
d. Dasavatara 'theory'/ view of evolution
e. 'Aham brahmasmi’/ Divinity/ Divine being view of evolution
'Cloud theory’ of evolution suggests creation of life from the clouds of waves and particles, happens as a result of (i) natural interactions, (ii) permutations & combinations (iii) quantum churning. In contrast, Darwin’s biological evolution is result of nature's selection and biological fitness. Higher evolution among human beings is result of self effort and thereby self selection on the part of human beings. In consonance with the above, there are various stages of human evolution viz. shunya stage, biological stage, heart-mind awakening stage, consciousness enlightenment stage and cosmic being stage. While some persons remain at the biological stage, hence, their behaviour is driven by Biological (B) factors and they remain at Darwinian level of existence and believe in 'survival of the fittest to eliminate the rest’. Some move to next stage represented Heart’s Awakening (HA) and by Human values, heartfulness and heartistic approach to life and human existence, some move further to the next stage represented by Spiritual (S) values and spiritual temperament and a few reach the cosmic being level as they have inner desire for 'cosmic realization' of reaching Harmonic Oneness (HO) stage represented by 'aham brahmasmi’. YOGA, when defined as "Yearning for Oneness and Gaining Advancement" (Sharma 1996, in “Western Windows Eastern Doors’), helps our self evolution towards Harmonic Oneness (HO). According to Swami Vivekananda, every human being is potentially divine and aim of human, beings is to manifest this divinity within. Thus, human journey is a journey from 'Shunya Unfolding' (SU) through Biological (B), Heartfulness (H), Spiritual (S) stages and finally reaching Harmonic Oneness (HO) stage. In essence this represents evolution from Biological (B) being to Human (H) being ('being human’), Spiritual (S) and Cosmic being representing Harmonic Oneness (HO) with everything around us. These stages represent the expanding circles of human consciousness from biological state to cosmic/ divine being state. Hence, we refer this model as 'Darwin to Divinity’ and this four circles model of human evolution is presented in Figure 1.
Above presented model of human evolution is also captured in the following poem titled as 'I Am a New Religion’ (Shunya Poems, Subhash Sharma, 2010, p. 43):
I am a new religion, Higher than every religion,
A religion of being, being a human being,
Being a higher being, being a cosmic being,
I am a new science, Higher than every science,
A science of being, being a human being,
Being a higher being, being a cosmic being,
I am a new ism, Higher than every ism,
An ism of being, being a human being,
Being a higher being, being a cosmic being,
I am a new identity, Higher than every identity,
An identity of being, being a human being,
Being a higher being, being a cosmic being,
I am a new consciousness, a consciousness of being,
Being a higher being, being a cosmic being.
(I am a New Religion, Shunya Poems, Subhash Sharma, 2010, p. 43)
It may be indicated that this poem also traces the journey of human society since 'shunya unfolding' and the arrival of human beings on earth. This journey is a journey from Religion (s) to Science to Ideologies in the form of many Isms that originated in 19th and 20th century with their intellectual foundations in conflict and violence and to current focus on Identities (e.g. national identity, regional identity etc.). It also suggests future evolution towards a new consciousness of being a cosmic being. Realizing 'Light in our hearts' is a step in this direction.
For more articles in Journal of Yoga and Physiotherapy please click on https://juniperpublishers.com/jyp/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#journal of yoga and physiotherapy#physiotherapy#physical health#juniper publishers#open access journals#juniper publishers high impact journals#high impact factor journals#peer review journals
2 notes
·
View notes
Text
Yoga in School Education

IAuthored by Kalpana Venugopal
Introduction
Yoga makes a note worthy difference in the sense of well being of children of all ages and from all backgrounds. Regular practice of yogic postures enhances the ability of students to concentrate, to deal with impulsive behaviour, and to think more clearly. It helps mental equilibrium and self-control. Yoga teaches children to be gentle with themselves and others. It generates positive emotions and compassion. Furthermore, yoga reduces stress and helps children to release tension and relax. It helps children develop lifelong health habits (both physical and mental), i.e. acquaints them with the option of healthy practice of exercises for the body and brain [1]. Yoga offers students a balanced and safe way for them to relate with themselves and to their surroundings, both through inner & outer awareness. Practising yoga intensifies self-confidence as the students measure their own individual success and improvement. Yoga promotes group cooperation & accelerates the learning of vocabulary in a playful manner [2]. It has an exhilarating and calming effect, which in later life could lead to a marked reduction of stress, blood pressure problems postural and nervous disorders. Children enjoy associating the name of a pose with the characteristics of the animals and other aspects of nature it represents, thus relating to the oneness of creation [3]. Recognising all these benefits, which are based on sound research and practice most countries have recommended for yoga in school education.
A distinctive aspect of Yoga is the attention and mental focus that children learn to exercise while doing the postures. The result is the toning up of both the body and mind. In adopting and maintaining a posture there is a certain co-ordination between the muscular system and the nervous system, that influences the physical and mental behaviours. Yogic postures do not just invigorate the body but also aid immensely to keep the mind healthy and calm thus bringing a feeling of refreshment. The physical benefits are improvement of flexibility, freedom of movement, better posture & gait, improved digestion, circulation, nervous, & endocrine systems and stronger resistance, coordination of body and mind through postures [4] . Improved concentration, self-control; self confidence; focus upon one thing at a time, awareness of themselves, their abilities & individual differences; persistence & perseverance to attain; observation & self assessment; appreciation of silence; seeking for perfection, are all learned through control of breath and body postures [1]. This has great implication for academic learning [5] . The mental benefits of yoga are immense such as relaxation, calmness of mind, increased concentration, appreciation of silence, self-control, better coping with stress & tension, and generates positive emotions. It also harnesses mental energy & effort, helps deal with impulsive behaviour and enables to think more clearly [2]. Yogic practices can remove the psychological blocks in the minds of children and also make them aware of the psychological changes that happen in their body and brain. It can make them aware of their own distractions and give them the ability to focus on the theme of the subject they are studying. It can improve their responses, creativity, receptivity, memory, willpower and behavior [6]. Awareness and consciousness of body and mind makes them to be aware of their own abilities. Alertness and mindfulness makes them to be aware of meaningful learning and to seek meaning in learning. Visualization in meditation aids in stimulating the senses and promotes creativity [3]. Children will be more relaxed, focused, one-pointed and tranquil and less destructive, restless, violent and distracted, in class. All this accelerates learning and improves performance in school. It costs virtually nothing to set up a time for yoga lessons. A 10-minute yoga session per day is adequate and it does not require any equipment. Any open classroom is sufficient for conducting a yoga class. Yoga is not a religious practice, nor does it conflict with any religion, it is a way of life. The sooner it is learned and practiced in life the quality of life is assured. Therefore it is imperative to begin this early in life and school is the best agency to do so.
In India, Yoga has been an integral part of Health and Physical Education that has been a compulsory subject up to the secondary school stage, since 1988. The National Curriculum Framework 2005 [5] adopted a holistic definition of health in which yoga is an integral part of it. Yoga has been introduced from Class VI onwards, though yogic activities may begin in an informal way from primary classes onwards. The success of this effort depends on the steps that school principals and teachers take to encourage children to practice Yoga and reflect on their learning. It has been observed that yoga and physical education have not been given the due importance in school education and neither has their contribution to the health and overall development of the child been adequately acknowledged [7]. The constraints faced by yoga and physical education is related to a number of factors that affect the quality of school education in general and health and physical education in particular. In order to make this subject on par with other subjects of school education, it is important in advocating it as having a strong experiential learning component and not just instructive [5]. Therefore, emphasis should be on preparing and training teachers in yoga by focusing on the comprehensiveness of the area of health and physical education.
The experience of initiating yoga in school curriculum has been a mixed experience. There is a tendency of reducing yoga to a mere physical exercise, which defeats the very essence of this practice. Presently there is shortage of trained yoga teachers, which is related to the non-availability of adequate number of institutions that have the capacity and expertise for this purpose. The role of the National Council for Teacher Education in this regard is laudable [8]. The modules prepared by the NCTE on Yoga Education for the Diploma, Bachelor and Masters programs in Education are intended to fulfill the great expectations that the society has placed on teachers and teacher educators in respect of development of composite personality in teacher educators and teachers, and in turn in the students. It is indeed gratifying that Yoga Education has been made a compulsory paper/area of study for more than 18,000 teacher education institutions teaching above 14 lakh teachers through above 3 lakh teacher educators/ faculty members. This is historic for India, for this is the first time that Yoga Education has been made compulsory nationally for all the teacher educators and student teachers in the country. [7] Yoga is the single most area of learning, which is capable for effecting the holistic development of the human personality. Yoga has its roots in Indian traditions and culture, and it is scientific in method, content and verifiable like any other academic discipline. In view of the above, the NCTE developed learning materials, which is authentic and secular, and free from any sectarian biases [8]. The materials developed satisfy the criteria of secularism and democracy and, in most cases, possess research-based authenticity.
Yoga aims at the total development of the human personality, impacting upon its different dimensions and facets-the individual and social; emotional and cognitive, psychomotor and behavioral, and eventually moral and spiritual [6]. If regularly and properly practiced, Yoga has the potential to transform an individual into a vibrant personality, full of energy and enthusiasm. It can give poise and tranquility, a sharp memory, concentration, a creative mind, resistance against diseases and holistic health [3]. All of these needs to be worked upon from childhood for fuller benefits and therefore it should be a part of school life. Second, it is a truism that for spreading the message of Yoga and making it a mass movement no other agency, except that of the school and the teachers can be most effective; therefore, inclusion of Yoga education in school and teacher education cannot be over emphasized.
For more articles in Journal of Yoga and Physiotherapy please click on https://juniperpublishers.com/jyp/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#yoga#physical health#physiotherapy#Juniper publishers high impact journals#Juniper Publishers#peer review journals#open access journals#High impact factor journals
0 notes
Text
Hatha Yoga Effect on Airway Resistances of Tobacco Smokers with Allergic Rhinitis

Authored by Chellaa R
Abstract
Background: There have been limited studies on Hatha yoga training as a complementary therapy to manage the symptoms of Allergic Rhinitis and also to check the effect of yoga on airway resistances in tobacco smokers with Allergic Rhinitis.
Aim: The main Aim of the study was to check the effect of Hathayogasanas on the Airway resistances in tobacco smokers with allergic rhinitis.
Materials and Methods: This is a prospective non blinded study of 20Tobacco smokers with allergic rhinitis. In the age group of (18-30). The subjects chosen for the study underwent an ENT examination and Hatha yoga training was giving for a period of 90 days. The objective analysis for upper airway resistance and lower airway resistance was done using a Rhino manometer and Spiro meter. The subjective analysis was done using a SF-12 Health survey questionnaire and a SNOT questionnaire. Both the objective and subjective analysis was done before and after the practice of Yogasanas. The compiled data was analyzed with the paired (2-tailed) T-Test, using SPSS (Software package for social sciences) version 16.
Results: The total nasal airway resistance was found to be increased before doing yoga and it was significantly reduced at 150 Pa pressure after doing yoga. The mean FEV1/FVC% before doing yoga was less when compared with the post yoga measurement. The mean Physical component score (PCS) and Mental component score (MCS) of the SF-12 health survey questionnaire had significantly improved and the mean SNOT questionnaire score had significantly reduced after the practice of yoga.
Keywords: Hatha yoga; Tobacco smokers; Allergic rhinitis; Rhino manometer; Spiro meter; SF-12 Health survey questionnaire; Snot questionnaire
Abbreviations: AR: Allergic Rhinitis; SF-12: Short Form 12 Health Survey Questionnaire; SNOT: Sino Nasal Outcome Test Questionnaire
Opinion
Allergic Rhinitis (AR) is the most common allergic disease, affecting 30% of population around the world. The disease is predominantly associated with exposure to some aeroallergens like cigarette smoking [1]. Allergic Rhinitis (AR) is usually defined as the presence of at least one or more of the symptoms of congestion, rhino rhea, sneezing, nasal itching, and nasal obstruc-tion [2,3]. The disease is an Immunoglobulin E (IgE) medi-ated reaction of Th2-type T cell response [4,5]. Due to the chronicity of disease and the variable response to therapy, a large number of patients resort to complimentary and alternate medication for Allergic rhinitis. Nasal breathing exercise is a simple and cost effective measure to reduce symptoms of Allergic Rhinitis and improve patient satisfaction [6].
Yoga is an alternative to traditional (Western) aerobic exercise that may have promise as a complementary treatment for smoking cessation. Yoga contains a number of components that contribute to stress reduction including asanas, yoga postures that have been shown to improve mood and well-being similar to the effects of traditional Western exercise, [7-10] and pranayama, breathing exercises that involve regulation of breath and conscious deep breathing that stimulates pulmonary stretch receptors similar to the deep in halation associated with smoking [11]. While yoga is associated with health benefits similar to exercise, the goal of yoga practice is also to create a calm state of mind through the combination of physical postures, breathing techniques, and directed meditative focus [12,13]. Several studies have shown that the practice of yoga reduces perceived stress and negative effect. Thus, the practice of yoga may also improve the chances of successful smoking cessation [14-17].
Yoga training can readjust the autonomic imbalance, controls the rate of breathing, and thus alters various physiological variables. These changes are attributed to the decreased sympathetic reactivity and relaxation of voluntary Inspiratory and expiratory muscles [18,19]. The proportion of adolescents with symptoms of asthma or allergic rhinitis who reported smoking experimentation is a cause for concern, because there is strong evidence that active smoking is a risk factor for the occurrence and increased severity of allergic diseases [20]. Passive and active smokings are both risk factors for asthma and allergic rhinitis in adolescents [21-23]. Cost effective options and alternative therapy such as yoga will serve as a solution to manage Allergic rhinitis. The ancient science of yoga includes physical postures, voluntarily regulated breathing, and meditation, among other techniques [24]. Practicing yoga can bring positive effects on well-being and human health with respect to biological and physiological parameters [25]. Voluntarily regulated yoga breathing techniques have been found to increase the oxygen consumption (and correspondingly the metabolic rate) both as an immediate effect [26,27] and as a longitudinal effect [26]. Certain yoga voluntarily regulated breathing techniques offer an opportunity to study the effects of changes in the respiratory pattern on metabolism [28]. Voluntary regulation of breathing in yoga alters autonomic activity with an improvement in cardiovascular and psychological health [29]. Nose is the main channel for the entry of air to the respiratory system, but this also exerts a resistance to the airflow. This nasal airflow resistance consists of half to 2/3rd of total airway resistance [30]. Nasal resistance is defined as resistance offered to the air entry by the nasal cavity [31]. This resistance is rather important as it prevents catastrophic collapse of lung [32]. Nasal airway resistance accounts for more than 50% of total airway resistance [33].The nasal cavity has been modeled as 2 resistors in parallel [34,35]. The 3 components of nasal resistance are as follows: the nasal vestibule, nasal valve, and nasal cavum [33].Information regarding nasal resistance is essential for management of anatomic and physiologic diseases of the na-sal airway. However, there are often inconsistencies between subjective nasal obstructive symptoms and the objective appear-ance of the nasal cavity [36]. Due to this discrepancy, objective diagnostic tools for the assessment of nasal patency or resistance are needed [37].The upper airway resistance can be measured with the help of a rhino manometer and lower airway resistance can be measured with a spiro meter. Anterior active rhino manometer is the most frequently used method in clinical practice according to the International Standardization Committee of Rhinomanometry, ICSR [38, 39]. The word rhinomanometry means 'rhino' for nose and 'manometer' for measurement of pressure [40]. Spirometry is a safe, practical and reproducible maximum breathing test that can be used in primary care to objectively determine the ventilatory capacity of the lungs. As already emphasised earlier in this article, it is the 'gold standard’ for detecting and quantifying airflow obstruction [41]. A spiro meter is a medical device that allows measurement of how much air is expelled and how quickly the lungs can be emptied, in a maximal expiration from full inflation [42]. The test is relatively quick to perform, well tolerated by most patients and the results are immediately available to clinician [43]. Sofar there has not been much studies done to check the efficiency of Hatha yogasanas on the airway resistances of tobacco smokers with allergic rhinitis. Hence Hatha yogasanas comprising of breathing exercises were taught to the recruited subjects in the study and effect of these asanas on the airway resistances of tobacco smokers with allergic rhinitis was studied.
Materials and Methods
This study was conducted at the Department of Otorhinolaryngology, St. John's national academy of health sciences, Bangalore. The study is a prospective non blinded study. 20 Tobacco smokers with Allergic rhinitis between the age group of 18-30, willing to practice yoga for a period of 90 days and with full compliance and reduce the number of cigarettes were recruited for the study. The Nasal resistance was measured at day0, that is before the start of practicing yoga and then after a period the 90 days. Written and informed consent was taken before the procedure. A thorough otorhinolaryngologicalexamination of all subjects was done prior to the study. The subjects were taught Hatha yogasanas by a trained yoga tutor. The following are the list of specific asanas which were taught
a) Tadasana (mountain pose)
b) Ardhachakrasana(Half-Wheel Posture )
c) Ardhakatichakrasana (Lateral arc posture)
d) Bhujangasana ( Cobra Pose )
e) Vrksasana ( Tree Pose )
f) Veerabadrasana(Warrior Pose)
g) Gomukasana ( Cow Face Pose )
h) Ustrasana ( Camel Pose )
i) Dhanurasana ( Bow Pose )
j) Surya Namaskara
k) Nadi Shodhana Pranayama ( Alternate Nostril Breathing Technique )
l) Bhastrika Pranayama ( The Bellows Breathing )
m) Bhramari Pranayama ( Humming Bee Breathing Technique )
n) Kapalabhati ( Hyperventilating Practice )
o) Jalaneti
The rhino manometer and spirometer was used to assess objectively the effect of Hatha yogasanas on the airway resistance. Regular calibration was ensured. The technique of the whole procedure was explained in full detail to all subjects. Series of trial recordings were performed with an intention that they were familiar with the technique and equipment thereby eliminating any anxiety which is a known factor for reducing nasal resistance. Rhinomanometry examination was performed during quiet breathing with close mouth in an upright sitting position and the following parameters were recorded [44].
Equipment used had following features:
1. During spontaneous respiration transnasal pressure differences and nasal air flow were recorded simultaneously.
2. Nasal air flow and pressure curve was displayed on a visual display unit (VDU) which allowed controlling the regularity of patients breathing.
3. Data obtained in the form of printed graph which contained nasal airflow and pressure-flow relation at 150mm Pa pressure [30].
Nasal resistance was kept static at 150 Pa because at this pressure difference both laminar and turbulent airflow were prevailed and nasal resistance can be assessed with minimal physical effort. Calculations of transnasal resistance were made according to Ohm's law. Nasal resistance to airflow was calculated by following equation
R = ∆P/V
R is total nasal airflow resistance in Pa/cm3/s,
∆P is 150 Pa pressure, V is nasal airflow (sum of left and right) during inspiration.
Total nasal airflow resistance reflects the resistance of both side of nasal cavity. The advantage of measuring the total nasal airflow resistance is to avoid the effect of nasal
Cycle over unilateral nasal airflow resistance as the nasal cycle may lead to a change of 4-fold in unilateral nasal airflow resistance [45]. The subjective analysis was done using the SF- 12 Health survey questionnaire and SNOT questionnaire.
Result
The Objective analysis parameters pre yoga and post yoga was found to be as follows, Total Nasal Airway Resistance in the 20 subjects was 0.44 Pa/cm3/s pre yoga and 0.39Pa/cm3/s post yoga at 150Pa with P<0.05. Pulmonary function test parameter FEV1/FVC% pre yoga was 66.12 and 79.51 post yoga with P<0.001***. . The subjective analysis parameters was found to be as follows, the Physical component score of the SF-12 health survey questionnaire was 38.62 pre yoga and 41.99 post yoga with P<0.05* and Mental component score of the SF-12 health survey questionnaire was 40.04 pre yoga 45.07 post yoga with P<0.01**, and the SNOT questionnaire score was 12.77 pre yoga and 10.05 post yoga P<0.001***.
Discussion
Allergic Rhinitis (AR) is defined as inflammation of the membranes lining the nose, and is characterized by nasal congestion, rhino rhea, sneezing, itching of the nose and/or post-nasal discharge [46]. It is often viewed, as a trivial disease but can significantly affect the quality of life (QOL) by causing fatigue, headache, sleep disturbances and cognitive impairment [47] Allergic Rhinitis is also closely related to asthma and, 10-40% of people with rhinitis have concomitant asthma [47]. According to WHO (2007), the global burden of allergic rhinitis was estimated to be 400 million [48] and the prevalence among adults ranges between 10% and 32% in Asia Pacific region [49]. Despite the high burden, there is paucity of community based studies in India, determining the burden and factors associated with allergic rhinitis. Medications provide some relief, but improvement is only partial. Anti-IgE shots show better efficacy, but are still very expensive [50].
Tobacco smoke exposure remains common and has been linked with an increased risk of multiple upper respiratory conditions in various age groups. Significant associations have been suggested between tobacco smoke exposure and chronic sinusitis [51], asthma [52] and allergic rhinitis [53]. In developing countries such diseases pose a serious socio economic burden. Cost effective options and alternative therapy such as yoga will serve as a solution to manage Allergic rhinitis. Pranayama is an integral part of Hatha yogasanas. As a deep breathing technique, pranayama reduces dead space ventilation and decreases work of breathing. It also refreshes the air throughout the lungs, in contrast with shallow breathing that refreshes the air only at the base of the lungs [54]. Regular practice of pranayama improves cardiovascular and respiratory functions, improves autonomic tone toward the parasympathetic system, decreases the effect of stress and strain on the body and improves physical and mental health [55-57]. Pulmonary function parameters (PFT) provide important clinical information to identify and quantify the defects and abnormalities in the functioning of the respiratory system. A study by Dinesh etal ,after 12 weeks of fast pranayama training FEV1 /FVC, PEFR, and FEF25-75 were significantly improved (P = 0.02, P< 0.001, and P< 0.001, respectively) compared with the values at baseline. Yadav and Das attributed that improvement in the PFT parameters by yogic practices due to increased respiratory muscle strength, clearing of respiratory secretions and using the diaphragmatic and abdominal muscles for filling the respiratory apparatus more efficiently and completely. Furthermore, the improvement in the PFT parameters may be due to rise in thoracic - pulmonary compliances and broncho dilatation by training in Nadisodhana pranayamas [58]. Stimulation of pulmonary stretch receptors by inflation of the lung reflexely relaxes smooth muscles of larynx and tracheo bronchial tree. Probably, this modulates the airway caliber and reduces airway resistance [59]. Previous investigators demonstrated the effect of pranayama on enhancement of the respiratory muscle efficiency and lung compliance due to reduction in elastic and viscous resistance of lung [60]. Furthermore, pranayama acts as stimulus for release of lung surfactant and prostaglandins into alveolar spaces, which increases the lung compliances [61]. Total nasal resistance gives an overall measure of nasal functions and also reflects the degree of nasal obstruction during breathing [45].
In our study Table 1 shows the Total Nasal Airway resistance in 20 subjects where in during preying it was 0.44 and post yoga it was 0.39 with the p value <0.05*. Graph 1 shows the decrease in total nasal airway resistance post yoga. Table 2 shows the Spiro metric measurements i.e, FEV1/FVC% during pre yoga it was 66.12 and post yoga it was 79.51 with the p value <0.001***. Graph 2 shows the significant improvement of the FEV1/FVC% parameter post yoga in the 20 subjects. Table 3 shows the SF- 12 Health survey components i.e the physical component score during pre yoga was 38.62 and post yoga was 41.99with the p value <0.05* and the mental component score during preying was 40.04 and post yoga was 45.07 with the p value <0.01**. Graph 3 shows the significant improvement in the physical and mental component scores post yoga. Table 4 shows the SNOT scores which was 12.77 during pre yoga and 10.05 post yoga with the p value 0.001***. Graph 4 shows the significant reduction in the SNOT score post yoga.
Conclusion
The study shows that there is decrease in the total nasal airway resistance and the FEV1/FVC% parameter also show significant improvement in 20 tobacco smokers with allergic rhinitis after the regular practice of yoga. The Quality of life of the subjects has been better as per the SNOT and SF 12 Questionnaire. There have been no scientific studies concerning the effect of yoga on the airway resistances of tobacco smokers with allergic rhinitis. Thus this study may form a basis for future studies focused on the effect of yoga on the tobacco smokers with allergic rhinitis.
For more articles in Journal of Yoga and Physiotherapy please click on https://juniperpublishers.com/jyp/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#open access journals#yoga#physical health#physiotherapy#Juniper publishers high impact journals#High impact factor journals#peer review journals
1 note
·
View note
Text
Yoga and Meditation

Authored by Susan Visvanathan
Introduction
These two yoga and meditation are indivisible, since even those who are secular, enter into deep states of reflection, while engaging in yoga. The day begins well when one is able to contemplate, and do one’s exercises simultaneously. The energy that is released is substantial, the mind is calm, one lets go of all the negativism that might have accumulated because of the disturbing events all of us are constantly exposed to. Best of all, the predatory instincts we have, as human beings, constantly engaged in competition with others, is muted.
Yoga helps to build up immunity, as our nervous systems are affected very badly by the noise pollution, the contaminated processed food that we all eat, and the way in which we live our lives, generally without stoppers. We move, as metropolitan citizens from one excitement to another, often stopping to merely draw breath, before we begin another excruciatingly exhausting assignment. The carbon trail we leave behind is as reminiscent of our own absorption of it, as we stand next to aero plane exhausts while disembarking, as frequently as we get stranded next to a spewing truck or bus or SUV in traffic jams, which last up to ten minutes at a time. How do we get rid of this carbon which accumulates in our blood, always making us yawn through the day, as we work endlessly? A good diet helps, and the free radicals are washed out by our drinking quantities of water and eating well washed salads and fresh fruit.
Yoga makes us, through its initial emphases on breathing exercises, spill out the air which is locked in our lungs, and by concentrating on the breathing, as we pull air in and push it out, it clears our brain. The concentration that is evident, as we do pranayama is probably the first step to meditation, since our mind and body becomes integrated in this preliminary exercise. The integration of body and mind, which yoga brings to us is its greatest benefit. As we proceed with the exercises that our guru teaches us, we find them appropriate to our age and physical condition. The guru selects exercises that are necessary for our well being. Even in a group setting, where there are people of different ages, it is the guru’s wisdom that allows us to participate in some, and not in others. If our age and physical circumstance does not permit us to do some exercises, we should not feel incompetent. I had an uncle in Kerala, who did head stands at the age of 90, and he always did his yoga and meditation before leaving for a twelve hour day at his shop, where he had been a spice merchant since his early youth. So age, by itself is not a determinant, but for those of us, who suffer from multiple sclerosis, the paralysis maybe so subtle, that even the simplest of exercises, such as lifting one’s spine while lying on the floor, may take some time. Multiple sclerosis is a neurological illness, which is neither genetic nor infectious.
However, living in polluted cities, eating food which has been loaded with pesticides does affect one’s chances of developing it. The similarities with rheumatoid arthritis and with diabetes are compelling. Many of the symptoms of MS, which is the slow or rapid loss of faculties and the deadness of nerves in the brain and spine, may result in blindness, loss of hearing and of course, paralysis. MS patients live with the dread of these, waking up in the morning, finding an eye inflamed, or ears blocked, or a body part stiff, without apparent cause. Yoga and meditation calm the body, and the mind. Shava Asana, like Pranayama, is excellent for returning the body to its accustomed tranquil space. For the galloping form of MS, where loss of limbs is immediate, meditation is calming, since the body accepts the context in which it has been placed. Most MS patients, whether it is the slow or rapid form of degradation, know that time is of the greatest essence, that what they have may well be taken away from them by the end of the day. They suffer exhaustion, which is almost continuous, and of course, fear, despair, anxiety. Care givers find their lack of attention to every day tasks, or their hypersensitivity to these, annoying in turn. They also suffer from the need to be attended to immediately. Meditation helps in controlling this need to be understood and attended to, as often, caregivers are busy with other tasks.
Yoga builds up those muscles which are in danger of atrophy due to the lack of blood circulation in such patients. Even flexing hands and feet, while in bed, or at the computer, can go a long way in releasing the blood, where it has jammed or coagulated. Many times, MS patients wake up, in the middle of the night, with some limb gone completely dead on them. Ayurvedic treatment is a great boon, and sometimes, the patient emerges completely free of pain for a couple of months. The food that helps MS patients most are fruit and salads, cooking in sesame oil. Of course staying clear of butter, meat, chocolates, cakes, pickles and oily food does help in slowing the onset of illness. Since heat is the catalyst, those foods which are heating, trigger off MS episodes, or aggravate existing conditions. The heat rash and the inflamed eye is the first symptom. If the patient reads the sign that the body is overheated, and attends to it, then the chances are that she or he will work to cooling the metabolism down. Some are allergic to dairy products, some to meat. Each patient has to find out which is the catalyst to the exacerbation of their condition. Yoga, Ayurveda, Meditation and Diet are the most important in tailoring the palliative measures useful to controlling the disease, as its tumultuous appearance disturbs everyone equally, without being very visible. MS patients, before paralysis sets in, look like everyone else, but deep within they are trying very hard to lead normal lives, and they experience the world much more dramatically than others. Homeopathy has great remedial doses for each symptom, as it appears differentially for every patient.
It is tailor made to the person according to the situation in which he or she finds himself or herself to be in, at any given time. The odd thing about MS is that every week, the patient finds a new body part is acting up, and standardized allopathic medicines like cortisone of interferon, are not equally available to all patients, and come with their own side effects, and are not custom made to the individual and unique nature of each afflicted person. Yoga, essentially, is a preventive system of therapy, which handles the pitta in the person's metabolism with its ability to understand that our relationship to the cosmos is constantly being divined by our attitude to it.
For more articles in Journal of Yoga and Physiotherapy please click on https://juniperpublishers.com/jyp/index.php
For more about Juniper Publishers please click on https://juniperpublishers.com/index.php
#Yoga#High impact factor journals#peer review journals#open access journals#physiotherapy#physical health#Juniper Publishers
1 note
·
View note
Text
Epilepsy and its Association with Depression | Juniper Publishers

Juniper Publishers-Open Access Journal of Toxicology
Authored by Sukaina Rizvi
Abstract
Depressive disorder is a frequent comorbid psychiatric condition in patients with epilepsy. It is more common in patients with temporal lobe epilepsy and frontal lobe seizures. Research has revealed a strong correlation between these two conditions. The early recognition of depressive symptoms in an epileptic patient is a predictor to improve quality of life. Besides treating epilepsy, antiepileptics have a role in treating nonepileptic conditions like mood disorders and pain syndromes. However, it is to be considered that certain antiepileptics decrease seizure threshold and increase seizure frequency.
Introduction
Over the years, a significant amount of research has been conducted showing relationship between epilepsy and depression. Epilepsy and depression are common conditions and often they occur together. Approximately, 40-60% people with epilepsy are affected with depressive symptoms [1]. This is a review article highlighting a strong association between two entities. The main idea behind this review article is to encourage practitioners to keep a close eye on symptoms of depression in people with epilepsy and to treat them accordingly which can impact positively on their quality of life.
Discussion
what is epilepsy? It is important to understand epilepsy on individual basis before moving on further. Epilepsy or a “seizure disorder” is a neurological condition affecting people of all ages. It involves a spectrum of various kinds of seizures, each presenting in a unique way in person to person. The two terms Epilepsy and seizure are used interchangeably; however, these are different in a context of frequency of occurrence as seizure is a single occurrence and epilepsy is two or more unprovoked seizures. According to Epilepsy foundation there are about 3.4 million people in United states who have epilepsy and there are 150,000 of new cases of epilepsy in the United States each year. It is also evident from a systemic review and meta-analysis research by A. K Ngugi, et al that median incidence of epilepsy as almost twice as high in low income countries than of high income countries [2]. The cause of epilepsy could be familial or could be secondary to stroke, brain infection, traumatic brain injury or idiopathic. Diagnosis requires a multidisciplinary approach including clinical presentation along with EEG, CT scan head, MRI, Neuropsychological testing, blood work. There are some seizures which present with normal finding on EEG. These are called pseudo-seizures and require a detail evaluation by a psychiatrist.
Epilepsy tend to impact a person on physical and psychological grounds as the occurrence of seizure is often uncertain. This could lead to an increase risk of mood disorders, physical trauma, cognitive issues, behavioral disturbances, depression, hospitalizations and mortality [3]. It is evident from a survey in UK that people with epilepsy tend to suffer from anxiety and sleep disorders more than the people without epilepsy [4]. This sleep disturbances and anxiety can significantly affect the quality of life in a negative way predisposing a person to develop depression.
As the focus of medicine has transitioned to research, we are now able to uncover that depression and epilepsy often coexist together. It is approximated that life time prevalence of depression in correlation with epilepsy is about 55% [5]. The exact cause of this association is still debatable as various mechanisms explain this link. People with depression have sleep deprivation which can decrease seizure threshold and increase seizure frequency. Preictal psychiatric symptoms usually consists of a constellation of symptoms preceding seizure and can last from minutes to days including prodromal symptom of depressed mood and irritability which is relieved after the onset of seizure or in some cases after few days of seizure activity [6]. Inter Ictal depression or dysphoria consist of brief episodes of crying spells, feeling of worthlessness, anhedonia, helplessness, hopelessness which usually last less than 30sec. In addition, inter ictal depression is also manifested by agitation, psychotic disturbances and impulse control issues which can ultimately predispose to increased suicidal tendencies [5,7]. It is important to recognize all these phases as their prompt recognition and their immediate treatment can lead to prevention of a seizure activity and would also improve quality of life.
It is stated that Depression affects some parts of limbic system of brain which includes amygdala which is a center for emotional/stress responses and hippocampus which has a role in cognition. This results in reduced hippocampal volume and functional or physical alteration of amygdala. Research publication have demonstrated increased risk of depression in patients with temporal epilepsy [5].
This is supported by the temporal lobe epilepsy refractory to antiepileptic medications that could lead to hippocampal sclerosis [8]. Studies have shown some correlation showing that people who have hippocampal sclerosis had a history of febrile convulsant seizure in childhood. Also, there is a study on infants with complex febrile seizures validating that sometimes complex prolonged febrile seizures can lead to acute hippocampal injury which later evolves to hippocampal atrophy [9]. This phenomenon could also explain an association between epilepsy and depressive symptoms secondary to reduced hippocampal volume.
Antiepileptics also have a significant role in various psychiatric disorders where they are primarily used for mood stabilization and for treating anxiety. However, effects of antiepileptics in terms of their therapeutic benefits and side effect profile varies from person to person. It is important to consider that studies performed on one group of people on AEDs should not be implied to another group. This is even more of significance in patients with epilepsy where there is a considerable variation in response to these drugs based on different reactions. Research has shown that people with epilepsy on antiepileptics are more predisposed to increased risk of depression as compared to the other populations [10]. According to Siddhartha, certain antiepileptics are notorious for this behavior which includes levetiracetam, ethosuximide, phenytoin, topiramate etc., which may precipitate underlying depression or anxiety. However, it is interesting to note that some AEDs like lamotrigine have beneficial effects of antidepressants [10,11]. It is stated in publications that each of AEDs act through unique mechanisms which alters the electrochemical gradient resulting in positive or negative behavioral changes. These mechanisms include GABAergic modulation either through stimulating chloride channels or inhibiting GABA uptake and inhibition of voltage gated sodium channels [12]. Landolt hypothesis of forced normalization should also be taken into consideration regarding behavioral manifestation of AEDs which states possibility of depressive symptoms after diminution of epilepsy either through surgery or use of AEDs [5].
There is evidence suggesting that tricyclic antidepressants and MAOI have a dose- dependent potential to decrease seizure threshold. Bupropion has also shown to decrease seizure threshold at all doses. Now there are cases reported in which Bupropion has led to seizure activity even at its extended release formulation. Alternatively, second generation antidepressants SSRI like sertraline, paroxetine, escitalopram does not lower seizure threshold and can be safely used for treating depression in epileptic patient [13,14]. There could also be a strong connection among depression, epilepsy and suicide as a people with MDD harm themselves by over ingesting antidepressants which could be lethal causing seizures or on the other hand, a people with epilepsy can become depressed over time with their illness and try to commit suicide.
Conclusion
In the light of above review article, it is concluded that epilepsy and depression share a unique bidirectional relationship as depression is a most frequent comorbidity in patients with epilepsy. Given their strong correlation a clinician should use a holistic approach to identify depressive symptoms in epileptic patients. There is also a need to investigate about any history of seizure disorder as there is evidence suggesting hippocampal changes in these patients predisposing to depression in later life. It is imperative for practitioners to obtain a through drug history, monitor their drug levels and to make correct choice of antidepressants if treating epilepsy. This also necessitates a need of collaboration between a neurologist and a psychiatrist to manage these conditions.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Toxicology please click on: https://juniperpublishers.com/oajt/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/oajt/OAJT.MS.ID.555616.php
37 notes
·
View notes
Text
SVM based Prediction of Major Histocompatibility Complex Binders: Identification and Analysis of Dracunculus medinensis Peptide | Juniper Publishers
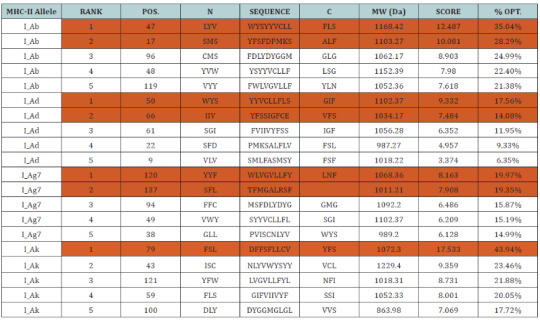
Juniper Publishers-Open Access Journal of Organic & Medicinal Chemistry
Authored by Sonu Mishra
Abstract
The largest human infecting parasite causes guinea worm disease, known as the disease and cause of poverty due to unavailability of the sanitized water. This is not lethal but causes the long term morbidity and motility in the infected human. In this research work, we predict the peptide binders of antigenic protein from D. medinensis sequence to MHC-I molecules are as 11mer_H2_Db, 10mer_H2_Db, 9mer_H2_Db, 8mer_H2_Db.Also study integrates prediction of peptide MHC class I binding; proteasomal C terminal cleavage and TAP transport efficiency by using sequence and properties of the amino acids. We also found the binding of peptides to different alleles by using Position Specific Scoring Matrix. NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis is 145 residues long with 137 nonamers having antigenic MHC binding peptides. PSSM based server will predict the peptide binders from D.medinensis of NADH dehydrogenase subunit 6 sequence to MHC-II molecules are as I_Ab.p, I_Ad.p, I_Ag7.p,I_Ak.p which are found antigenic epitopes region in NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis.
Keywords: Antigen; MHC; TAP; PSSM; NADH dehydrogenase subunit 6; Peptide
Abbreviations: MHC: Major Histocompatibility Complex; TAP: Transporter Associated with Antigen Processing; PSSM: Position Specific Scoring Matrices; SVM: Support Vector Machine
Introduction
The unique life cycle of the D.medinensis takes almost one and half years to complete with unusual six stages. This infection remains asymptomatic during the incubation period. This is one of the largest known human parasites which cause the high rate of the motility and morbidity in infected individuals for long time especially among the school going children’s.
The female worm released the larvae after the incubation period. Cyclops (intermediate host) eats infected larvae which gets entry into the human while drinking the contaminated water where the larvae gets mature and complete their six stages of the life cycle and finally the infectious female releases the infectious larvae which induces a painful blister (1 to 6cm diameter) on the skin of lower limbs; the person develop a slight fever, local skin redness, swelling and severe pruritus around the blister. Other symptoms include diarrhea, nausea, vomiting and dizziness. The severity of the wound infections in the infected individual led to a more complications such as redness and swelling of the skin (cellulitis), boils (abscesses), generalized infection (sepsis), joint infections (septic arthritis) that can cause the joints to lock and deform (contractures), lock jaw (tetanus). The blister burst within 1 to 3 days and female worms one or more slowly comes out from the wounds which causes an excoriating burning sensation and pain .Immersing or pouring water over the blister provide pain reliever. But this the moment that adult female is exposed to the external environment. During emergence of the limbs in open water sources it recognizes the temperature difference and releases the milky white liquid in the water which contains millions of immature larvae, when larvae released in water are ingested by copepods where they mount twice and become infective larvae within two weeks [1-7]. However, Identification of MHC [Major Histocompatibility Complex] binding antigenic peptide molecule will improves the understanding of specificity of immune responses against the pathogen, which is one of the important steps for vaccines discovery.
MHC class I antigen
The presence of the Major histocompatibility complex class I (MHC-I) molecules has been seen on the on the surface of all nucleated cells and display a large array of peptide epitopes for surveillance by the CD8+ T cell repertoire. CD8+ T cell responses,which are essential for the disease or infection control. The CD8+ T cells are actively and efficiently discriminate between the healthy and the infected cell through the recognition of peptides which are associated with MHC-I molecules present on the cell surface. The peptide with the length range of the 8-11 amino acids , are typically derived from protein antigens in the cytosol that arise from conventional as well as cryptic translational reading frames [8]. Proteins which are classically synthesized in the cytosol undergo proteasomal degradation and the resultant peptides are later on transported into the Endoplasmic Endoplasmic Reticulum (ER) and loaded onto MHC-I molecules [9]. Due to the loading of the peptide the class I MHC stabilizes and pass through to the cell surface where the circulating CD8+ T cells scans the complexes which is known as ‘immune surveillance’ [10-19]. Therefore, prediction of TAP binding peptides is important for identification of the MHC class-1 restricted T cell epitopes.
Proteasomal degradation
Proteasomal degradation is important step in the antigenpresentation process to regulate the balance between intracellular proteins [20]. Inside the proteasome by the action of proteinase the antigenic protein NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis are cleaved into oligopeptides [21] and then these oligopeptides are binds to the TAP, which transports these peptides into the ER.
TAP mediated peptide transport into ER(Endoplasmic Reticulum)
TAP is heterodimeric transmembrane protein, is a family of ABC transporter that transports antigenic peptide (NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis into ER [22] because most of the MHC binding peptides are unable to diffuse across membrane, but TAP protein is capable of transporting the peptide inside the ER where it binds to MHC class I molecules. These MHC-peptide complexes will be translocate on the surface of antigen presenting cells [23] and are recognized by T-cell receptors to elicit an immune response.
MHC class II antigen
The prediction of peptides binding to a MHC class II molecule is difficult due to different side chains and longer length found in the extracellular antigen presentation [24-26]. In the MHC class II antigen presentation process, antigenic protein NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis are ingested by antigen-presenting cells through the process of endocytosis or phagocytosis, then cleaved by cathepsins a class of protease into oligopeptides in the endosomes, than are fuse with lysosomes containing MHC class II molecules [27] and present them at the cell surface for recognition by T cells [28-36]. Where T helper cells trigger an immune response by inflammation and swelling due to phagocytes or may lead to an antibody-mediated immune response via B-cell activation. Since MHCs have a key role in immune system by stimulating cellular and humoral immunity against NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis and are used for controlling specific immunological processes by creating peptides to bind to specific MHC alleles and this binding affinity to specific peptides are used for designing synthetic peptide vaccines [37-40].
Materials and Methods
Predictions of MHC class I binding peptide
MHC binding peptide is predicted using neural networks trained on C terminals of known epitopes. By using RANKPEP we predict peptide binders to MHCI molecules from protein sequences or sequence alignments using Position Specific Scoring Matrices (PSSMs) whose C terminal end is likely to be the result of proteosomal cleavage.
Prediction of antigenic peptides by cascade SVM based TAPPred method
By using TAPPred we predict TAP binders on the basis of sequence and the properties of amino acids. We found the MHCI binding regions. The binding affinity of NADH dehydrogenase subunit 6 (mitochondrion) from D.medinensis having 145 amino acids shows 137 nonamers.
Predictions of MHC class II binding peptide
MHC peptide binding of NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis predicted using neural networks trained on C terminals of known epitopes. By using RANKPEP we predict peptide binders to MHCII molecules from protein sequences or sequence alignments using Position Specific Scoring Matrices (PSSMs). MHC molecule binds to some of the peptide fragments generated after proteolytic cleavage of antigen.
Results and Interpretation
In this research work, we predict the peptide binders of NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis sequence to MHC-I molecules are as 11mer_H2_Db, 10mer_H2_ Db, 9mer_H2_Db, 8mer_H2_Db (Table 2). MHC molecule binds to peptide fragments which are generated after proteolytic cleavage of antigen tend to be high-efficiency binders. TAP is an important transporter that involved in the translocation of peptides from cytosol to ER. TAP binds and translocate selective peptides for binding to specific MHC molecules. Therefore, predicting binding affinity of those peptides toward the TAP transporter is crucial to identify the MHC class-1 restricted T cell epitopes. Cascade based support vector machine shows 42 High affinity TAP binder residues at N and C termini using sequence and properties of the amino acids of NADH dehydrogenase subunit 6 (mitochondrion) from D.medinensis (Table 3). This method integrates prediction of peptide MHC class I binding; proteasomal C terminal cleavage and TAP transport efficiency by using sequence and properties of the amino acids. We also found the binding of peptides to different alleles by using Position Specific Scoring Matrix. NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis is 145 residues long with 137 nonamers having antigenic MHC binding peptides. PSSM based server will predict the peptide binders of NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis sequence to MHCII molecules are as I_Ab.p,I_Ad.p,I_Ag7, I_Ak which are found antigenic epitopes region in NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis (Table 1).
* The RANKPEP consists of a list of selected peptides binding potential (score) to the MHC molecule from the query given at a selected threshold. Peptides shown here contain a C-terminal residue that is predicted to be the result of proteasomal cleavage and also focus on the prediction of conserved epitopes that help to avoid immune evasion resulting from mutation. Proteasomal cleavage options are only applied to the prediction of MHCIrestricted peptides.
* TAPPred showing Cascade SVM based High affinity TAP Binders sites, their sequence, rank, position and scores are displayed in the tabular output are to be found 42 High affinity TAP Transporter peptide regions which represents predicted TAP binders residues which occur at N and C termini NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis.
Conclusion
NADH dehydrogenase subunit 6 (mitochondrion) an antigenic proteins from D. medinensis involved multiple antigenic components to direct and empower the immune system to protect the host from the pathogenesis. Major histocompatibility complexes I and II (MHC-I and MHC-II) display specificity to bind with their respective epitopes. MHC class molecules are cell surface proteins that take active part in host immune reactions to response for almost all antigens. This knowledge of the immune responses to an antigen protein NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis clear that the whole protein is not necessary for raising the immune response, but a small fragment of antigen can induce immune response against whole antigen. This means the increase in affinity of MHC binding peptides may result in enhancement of immunogenicity of NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis hence are helpful in silico to design and develop highly predictive computational tools for the identification of T-cell epitopes. Finally, accurate prediction remains vital for the future to design synthetic peptide vaccine.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Organic & Medicinal Chemistry please click on: https://juniperpublishers.com/omcij/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/omcij/OMCIJ.MS.ID.555557.php
39 notes
·
View notes
Text
Multimodal Exercise as Intervention for School-Aged Children and Youth with Emotional and Behavioral Disorders-Juniper Publishers
Juniper Publishers- Journal of Yoga and Physiotherapy

Abstract
Many school-aged children and youth experience emotional and behavioral struggles that diminish their educational outcomes. One of the thirteen categories of disability recognized in the Individuals with Disabilities Education Improvement Act-the federal law that provides for special education services to students with disabilities is emotional disturbance (ED). Although ED is the actual label under the law, most school- based practitioners and educational researchers prefer the term emotional and behavioral disorder (EBD). Recently, researchers have begun to explore the use of multimodal exercise (e.g., yoga) as an intervention for students with and at risk for EBD to see how it may influence students' emotional and behavioral outcomes. The purpose of this review was to summarize the yoga intervention literature to determine what effects, if any, these interventions have had for students identified with EBD in a school setting. Two studies were identified. Discussion of the two studies is presented and future directions for research are suggested.
Keywords: Yoga, Emotional and behavioral disorders, Intervention, Behavior, Engagement, Self-Regulation
Abbreviations: EBD: Emotional and Behavioral Disorder
Introduction
Many school-aged children and youth experience emotional and behavioral struggles that diminish their educational outcomes. One of the thirteen categories of disability recognized in the Individuals with Disabilities Education Improvement Act [1]-the federal law that provides for special education services to students with disabilities - is emotional disturbance (ED). Although ED is the actual label under the law, most school- based practitioners and educational researchers prefer the term emotional and behavioral disorder (EBD). An EBD is characterized by externalizing behaviors, internalizing behaviors, or a combination of both (i.e., co-occurring disorders). Externalizing behaviors are directed towards the social world outside of the person and include aggression, disruption, violence, noncompliance, and delinquent acts [2]. Internalizing behaviors are characterized by depression, phobias, eating disorders, anxiety, and other inward, somatic complaints [3].
School personnel often struggle to support students with EBD, given the myriad of their behavioral, emotional, and social needs [2]. Many students with EBD drop out before graduation because their behaviors become incompatible with the goals of school [4]. When compared to peers with a physical or learning disability, students with EBD perform worse academically, drop out of school at higher rates, and experience higher unemployment [5]. Considering post-secondary outcomes, students with EBD have the highest rate of criminal arrest (49.4%) when compared to other students served in special education [6]. Although many academic [7] and behavior [8] interventions have been developed and found to be successful in supporting the needs of students with EBD, secondary and postsecondary outcomes for this group are still relatively negative [6]. Recently, researchers have begun to explore the use of multimodal exercise (e.g., yoga) as an intervention for students with and at risk for EBD to see how it may influence students' emotional and behavioral outcomes. The purpose of this review is to summarize the yoga intervention literature to determine what effects, if any, these interventions have had for students identified with EBD in a school setting.
Review of Studies
In a review of research focused on relaxation techniques for students with disabilities, Zipkin [9] explained that yoga "can calm disruptive students and stimulate tired ones" (p. 286). Yoga is a multimodal practice that typically includes deep and purposeful breathing, meditation, and physical poses intended to stretch and balance the body [10]. Yoga may be beneficial to students with and at risk for EBD because previous research has shown yoga to be associated with improved emotional regulation and prosocial behaviors among children and youth [11,12]. In a review of research utilizing yoga as an intervention in school settings, Serwacki & Cook Cottone [13] identified 12 peer-reviewed, published studies. Of these 12, only 4 studies (33%) were focused on students with disabilities. Of these four studies, only one included students identified with EBD [14]. In their quasi-experimental study, Powell and colleagues reported on the effectiveness of the Self-Discovery Programme (SDP), a multi-pronged approach that incorporates massage, yoga, and relaxation techniques. The sample in the study included 107 children in England, ages 8-11 (45% female) identified with EBD and/or a learning disability.
Approximately 95% of the participants were Caucasian. Intervention students (n=53) received 45-minute SDP sessions once per week for 12 weeks. Students participating in SDP exhibited significant improvements in confidence (in self and in social situations) and engagement in class (e.g., more contributions), and a significant decrease in total behavior difficulties (i.e., a composite of internalizing, externalizing, hyperactive/inattentive, and peer problem behaviors). Overall, SDP was well received by children in the intervention group and teachers reported seeing their students utilize skills learned during the intervention throughout the school day.
As a follow-up to the review by Serwacki & Cook Cottone [13], I conducted a systematic search of the literature in an attempt to identify any recent (2013-2017) peer-reviewed studies that have used yoga as an intervention for school-aged children and youth identified with EBD. Only one study was located. Using a pre/post design, Steiner, Sidhu, Pop, Frenette, and Perrin [15] included 74 children ages 8-11 (41% female) identified with EBD in the United States. Racial/ethnic demographics were as follows: 49% African-American, 24% Hispanic, 20% Caucasian, 12% Native American, and 5% Asian-American. All children received a 1-hour yoga session twice per week during the school day for 3.5 months. According to teacher reports, after receiving the intervention the children exhibited improved attention and adaptive skills, and reduced externalizing and internalizing symptoms. Regarding satisfaction with the intervention, 64% of teachers and the vast majority of student responses were positive. Seventy-two percent of parents of student participants indicated the intervention had a positive impact on their child.
Conclusion
Given the myriad of needs common among students with EBD, it is encouraging to see that researchers are beginning to utilize yoga as an intervention for these youth. Although both studies indicated yoga was effective in helping children and youth with EBD, two studies does not provide a strong enough foundation to classify yoga as an evidence-based practice for this population. More studies are needed with more diverse samples. In fact, it was somewhat surprising to find how similar the samples of children were from the two reviewed studies in terms of age and sex. Although, racial/ethnic demographics were quite different in the two studies, with one sample being fairly homogenous [14] and the other being racially diverse [15]. Larger sample sizes in randomized controlled trials would be ideal in an effort to evaluate the true power of yoga to support the mental health needs of students with EBD. Still, the potential for yoga to improve students' behavior, especially their internalizing symptomology, is reason to be hopeful. Effective interventions for internalizing behaviors are far fewer than those for externalizing behaviors [16]. As more and more students with EBD find themselves in inclusive, general educational settings, schools must be prepared to offer these children the emotional and behavioral supports they need to be successful. Incorporating yoga into a weekly routine for these students may be a worthwhile investment for schools to make.
For more articles in Journal of Yoga and Physiotherapy please click
on https://juniperpublishers.com/jyp/index.php
For more Journals in Juniper Publishers
please click on https://juniperpublishers.com/index.php
To know more details regarding our Juniper publishers please click on
https://juniperpublishers.business.site/s
0 notes
Text
Beauty, A Social Construct: The Curious Case of Cosmetic Surgeries | Juniper Publishers
Juniper Publishers-Open Access Journal of Dermatology & Cosmetics
Authored by Vandana Roy
Abstract
In this article we deconstruct the social norm of beauty and cosmetic beauty treatment, an issue that is seldom discussed in medical circles and is often lost to popular rhetoric. In doing so, we also reflect on the institutionalized system of social conditioning.
A Historical Perspective
Cosmetic surgery, as with reconstructive surgery, has its roots in plastic surgery (emerging from the Greek word ‘plastikos’, meaning to mold or form). The practice of surgically enhancing or restoring parts of the body goes back more than 4000 years. The oldest accounts of rudimentary surgical procedures is found in Egypt in the third millennia BCE. Ancient Indian texts of 500 BCE outline procedures for amputation and reconstruction. The rise of the Greek city-states and spread of the Roman Empire is also believed to have led to increasingly sophisticated surgical practices. Throughout the early Middle Ages as well, the practice of facial reconstruction continued. The fifth century witnessed a rise of barbarian tribes and Christianity and the fall of Rome. This prevented further developments in surgical techniques. However, medicine benefited from scientific advancement during the Renaissance, resulting in a higher success rate for surgeries. Reconstructive surgery experienced another period of decline during the 17th century but was soon revived in the 18th century. Nineteenth century provided impetus to medical progress and a wider variety of complex procedures. This included the first recorded instances of aesthetic nose reconstruction and breast augmentation. Advancements continued in the 20th century and poured into present developments of the 21st century.
Go to
Desires and Demands in Contemporary Times
In recent years, the volume of individuals seeking cosmetic procedures has increased tremendously. In 2015, 21 million surgical and nonsurgical cosmetic procedures were performed worldwide. In the United Kingdom specifically, there has been a 300% rise in cosmetic procedures since 2002. The year 2016 witnessed a surge in the number of such treatments with the United States crossing four million operations. Presently, the top five countries in which the most surgical and nonsurgical procedures are performed are the United States, Brazil, South Korea, India, and Mexico. Such demand can be viewed from different perspectives. At one end it is a product of scientific progress, growing awareness, economic capacities and easier access and on the other, something on the lines of a self-inflicted pathology. This article dwells on the latter and attempts to address a deep-rooted problem of the social mind.
Lessons from History
History is witness to a number of unhealthy fashion trends, many of which today appear extremely irrational and even cruel. Interestingly, the common thread connecting all of them is the reinforcement of social norms and stereotypes. Forms of socialization which lie at the intersection of race, class and gender-based prejudices. To elaborate, hobble skirts and chopines restricted women’s movement and increased their dependence on others. Corsets deformed body structures, damaged organs and led to breathing problems. The Chinese practice of binding women’s feet to limit physical labor was regarded as a sign of wealthiness. Dyed crinolines and 17th century hairstyles made people vulnerable to poisoning and fire related injuries. Usage of makeup made of lead and arsenic, eating chalk and ‘blot letting’, reflected a blatantly racist obsession with white and pale skin. Lower classes faked gingivitis to ape tooth decays of the more privileged who had access to sugar. Furthermore, other practices like tooth lacquering, radium hair colors, mercury ridden hats, usage of belladonna to dilate pupils and even men wearing stiff high collars, all furthered societal expectations and notions of class superiority. Till the 1920’s, there was rampant usage of side lacers to compress women’s curves. Even today many ethnic tribes continue with practices which inflict bodily deformations. In the urban context as well, trends like high heels, skinny jeans and using excessive makeup dominate the fashion discourse. Cosmetic procedures are the latest addition to the kitty.
The Social Dilemma
What is it that leads the ‘intelligent human’ of today to succumb to archaic and regressive notions of beauty? What motivates them to risk aspects of their lives to cater to selflimiting rules of ‘acceptance’? The surprising part is that this anomaly is often placed in the illusory realm of ‘informed consent’. In common parlance, ‘to consent’ implies voluntary agreement to another’s proposal. The word ‘voluntary’ implies ‘doing, giving, or acting of one’s own free will.’ However, when the entire socio-cultural set up and individual attitudes validate certain behaviors, there is very less space left for an alternate narrative. Let alone free will.
Pierre Bourdieu once argued that nearly all aspects of taste reflect social class. Since time immemorial, societal standards of beauty have provided stepping stones to social ascent and class mobility. Better ‘looking’ individuals are considered to be healthier, skillfully intellectual and economically accomplished in their lives. Such an understanding stems from well entrenched stereotypes in complete disregard of individual merit and fundamental freedoms. An inferiority complex coupled with external pressures and self imposed demands, subconsciously coerce individuals into a vicious cycle of desire or rejection. Active and aggressive media has played a key role in forming societal perceptions of what is attractive and desirable. In addition, lifestyle changes reflect an image obsessed culture, reeking of deep-rooted insecurities. At the root of a submissive and conformist attitude lies a subconscious mind lacking selfesteem and self-worth. People continue to look for remedies in the wrong places. The only difference is that corsets and blot letting have given way to surgeries and cosmetic products. The biggest question is, how have ideas otherwise seen as deviant, problematic and inadequate retained control over minds of millions of individuals?
A Gendered Culture
‘Beauty’ is understood as a process of ongoing work and maintenance, its ‘need’ unfairly tilted towards the fairer sex. History has demonstrated the impact of dangerous beautification practices on women. Contemporary ideals aren’t far from reaching similar outcomes. Today, there is a powerful drive to conform to the pornographic ideal of what women should look like. There has been a growth in the number of adolescents who take to cosmetic surgeries to become more ‘perfect’. In many countries, the growth of the “mommy job” has provoked medical and cultural controversies. Presumably there is an underlying dissatisfaction which surgery does not solve. Furthermore, where does the disability dimension fit in here? What happens to the ‘abnormal’ when the new ‘normal’ itself is skewed? For those with dwarfism and related disorders, new norms become even more burdensome.
The massive pressure to live up to some ideal standard of beauty, particularly for women, reeks of patriarchal remnants of a male dominated society. This kind of conformity further nurtures objectification and sexualization, reducing women to the level of ‘chattel’ to feed the male gaze. There is a also a power struggle at play where biased standards help maintain the unequal status quo. Today, there is idolization of celebrities, beauty pageants and advertisements by cosmetic companies over sane medical advice. They set parameters of size, color and texture to be followed by the world at large. Moreover, people who deviate from such norms are made to feel stigmatized or ostracized from social spheres. The existence of male-supremacist, ageist, hetero sexist, racist, class-biased and to some extent, eugenicist standards reflect a failure of society as a whole. It is thus high time that we revisit and deconstruct skewed standards of beauty.
Mind Over Matter: Psychological Dimensions
Culturally imposed ideals create immense pressure of conformity. Consequently, they have been successful in engendering insecurities via their influence on perception of self and body image. Such perceptions often become distorted and discordant with reality, leading to serious psychological disorders. One such disorder is the body dysmorphic disorder (BDD). This is a psychiatric disorder characterized by preoccupation with an imagined defect in physical appearance or a distorted perception of one’s body image. It also has aspects of obsessive-compulsiveness including repetitive behaviors and referential thinking. Such preoccupation with self-image may lead to clinically significant distress or impairment in social and occupational functioning. With reference to cosmetic surgeries, patients with BDD often possess unrealistic expectations about the aesthetic outcomes of these surgeries and expect them to be a solution to their low self-confidence. Many medical practitioners who perform cosmetic surgery believe themselves to be contributing towards construction of individual identity as well. The notion that beauty treatments can act in much the same way as psychoanalysis has led countries like Brazil to open its gate of cosmetic procedures to lower income groups. This happens while the country continues its battles with diseases like tuberculosis and dengue. The philosophy behind such ‘philanthropy’ is that ‘beauty is a right’ and thus should be accessible to all social groups. While on one hand we may applaud such efforts of creating a more ���egalitarian’ social order, on the other hand it is hard to overlook the self-evident undercurrents of social prejudice and capitalistic propaganda.
Medicalization of Beauty
Traditional notions of beauty embody a kind of hierarchy and repression which alienate individual agency and renders them as powerless victims. Such is the societal pressure which normalizes cosmetic procedures and subverts serious health effects. These include adverse effects due to cosmetic fillers like skin necrosis, ecchymosis, granuloma formation, irreversible blindness, anaphylaxis among others. Other dangers like heightened susceptibility to cancer and increased suicide rates. However, patients are often unaware of the risks which are hidden behind a veil of expectations and reassurances. Furthermore, quackery and inadequate standards such as lack of infection control also compound the problems of this under regulated field.
Role of Stakeholders
At the heart of any successful social transformation lies the power of united will and collective action. Thus, the consolidated and sustained effort by all stakeholders is the key to realizing an ecosystem conducive to tackle negative social norms. At the outset, government regulation is needed with respect to cosmetic procedures and the cosmetics industry. These regulations should encompass all private and public avenues and should also work against misleading advertising. Spreading awareness is the key to a better informed society. The state should fund and run specialized awareness sessions pertaining to psychological problems and aid mechanisms, gender sensitization as well as those aiming at spiritual and introspective personal development of individuals. NGO’s, medical professionals, academicians and members of the civil society, must come together to eradicate forms of social discrimination which undermine social institutions and individual agency around the world. This would help facilitate discussion, data collection, coalition building, and action that may eventually lead to behavioral changes.
Aesthetic surgery today seems to be passing through an ethical dilemma and an identity crisis. And rightly so for it strives to profit from an ideology that serves only vanity, bereft of real values. Nevertheless, there are exceptional cases where medical-aesthetic inputs have been vital in restoring morale by subverting stigmatization.
The Way Ahead
Beauty is unfair. The ‘attractive’ enjoy powers gained without merit. The perfectionist in humans seeks outward validation of external beauty over inner virtues. Scientific progress and an increase in human expertise to manipulate natural phenomena has paved the way for these desires to become a reality. There is no denying that advances in plastic and reconstructive surgery have revolutionized the treatment of patients suffering from disfiguring congenital abnormalities, burns and skin cancers. However, the increased demand for aesthetic surgery falls short of a collective psychopathology obsessed with appearance. This article expresses trepidation about such forms of social consciousness that first generates dissatisfaction and anxiety and then provides surgery as the solution to a cultural problem.
We have to work towards a social order which embraces people as they are and facilitates free choice, individual liberty and informed decision making. This is particularly pertinent when these decisions work towards framing cultural perceptions and expectations for millions around the world. We should open our hearts to diversification of beauty and aesthetic. Let our entertainment, fashion, capital and media revolve around heterogeneity of ideologies and cultures. In the words of Eleanor Roosevelt, “No one can make you feel inferior without your consent”. So, let us all come together and create a better society. A society, where principles of justice, equity, good conscience and humanity override primitive and archaic ideologies of naive men. A society where individual will be truly free and, discourse a product of informed thought.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Dermatology & Cosmetics please click on: https://juniperpublishers.com/jojdc/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojdc/JOJDC.MS.ID.555556.php
31 notes
·
View notes
Text
Severity of Hip Displacement in Relation to Subtypes and Motor Function in Cerebral Palsy- Role of Hip Surveillance | Juniper Publishers

Juniper Publishers-Open Access Journal of Orthopedics and Rheumatology
Authored by Kunju PAM
Abstract
Background: Hip dislocation in children with cerebral palsy (CP) is a common and often over looked problem by the treating pediatricians. Though it can be diagnosed early by using radiographs, knowledge about the standardized methodology and need for periodic surveillance is lacking among primary care pediatricians. Hip surveillance by X-ray pelvis can identify early hip dislocation and it is shown that early intervention may prevent the need for surgery [1].
Methods: The study was done in a tertiary care hospital as a onetime radiological evaluation of children with CP between the age group of 4-9 yrs. One hundred and one children with CP formed our study population.Clinical evaluation for details regarding CP type and assessment of motor ability by gross motor function classification system (GMFCS) was done. A hip X-ray was done for calculation of, migration index for establishing or ruling out hip displacement. Migration percentage (MP) in relation to CP subtypes and GMFCS grades were done.
Results: There were 48 boys and 53 girls (mean age 4.80 years). 12 children were Gross Motor Function Classification System (GMFCS) level 5, while 26 were GMFCS level 4. Out of 36 hemiplegic CP only one had MP > 40. out of 6 children with spastic quadriplegia, 5 (83%) had MP > 40%. Spastic diplegic and choreoathetotic subtypes showed MP >40% in 9 out of 43 and 7 out of 16 respectively.According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40% compared to only 4.76% in GMFCS I and II put together.
Conclusion: All the children in this study did not undergo a hip X-ray prior to this study. 22 out of 101 children had severe degree of hip displacement. The maximum number of hip displacements was seen in children with spastic quadriplegia; Spastic diplegic and choreoathetotic subtypes showed intermediate risk of hip displacement and hemiplegia had very low risk. According to the gross motor function classification system,GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40%. The study showed the relationship between the CP subtypes and the severity of the motor involvement. It also emphasized the need for early hip surveillance.
Keywords: Hip dislocation; Cerebral palsy; Lateral Displacement; Hip surveillance
Introduction
In children with spastic cerebral palsy reduced activity of the hip abductor muscles in comparison to the spastic adductors leads to diminished growth of the greater trochanter of femur results in pathologic deformities of the hips-femoral anteversion and coxa valga antetorsa [2]. If untreated, dislocation of the hip typically occurs at age 2–7 years with a maximum at the age of 6 years. The incidence of hip displacement in cerebral palsy is related to the severity of involvement; varying from 1% in children with spastic hemiplegia, up to 75% in those with spastic quadriplegia [2,3]. So periodic evaluation of hip function is essential for early intervention and preventive measures.
Hip surveillance is defined as: “The process of monitoring and identifying the critical early indicators of hip displacement” [4].Hip displacement refers to the displacement of the femoral head laterally out of the acetabulum and is measured using a migration percentage (MP). Hip subluxation refers to hip displacement where the femoral head is partially displaced from under the acetabulum while hip dislocation refers to hip displacement where the femoral head is completely displaced from under the acetabulumn [5,6].Hip surveillance is important, to prevent morbidity of spastic hip disease-The aim of the management in children with spastic hip displacement is to maintain flexible, well-located and painless hips with a symmetrical range of movement. The key to achieving this goal is early identification and intervention.
Periodic hip surveillance also helps to reduce the need for extensive surgical procedures which is highly specialized area of orthopedics which may not be available in every center. So primary care pediatrician has a role for hip surveillance and timely referral.
Patients and Methods
The study was done in a pediatric neurology department of a tertiary care hospital as a onetime radiological evaluation of children with CP between the age group of 4-9 yrs prior to the referral to orthopedics. One hundred and one children between the age group of 4-9 yrs. with the diagnosis of CP formed our study population.A pediatric neurologist and physiotherapist in the department examined the children and completed an assessment form. Clinical evaluation for details regarding CP subtype and assessment of motor ability by gross motor function classification system (GMFCS) [6] was done. Winters, Gage, Hicks (WGH) gait type was determined, in addition to inquiring regarding pain during history taking. Orthopedic consultations done whenever required.
Radiographic Examination
Decision for referral for surgery depends on the degree of displacement of the femoral head and acetabular dysplasia. The migration percentages as described by Reimers and the acetabular index described by Hilgenreiner are the conventional measurements of displacement of the hip and acetabular dysplasia in young children with cerebral palsy.Radiographic assessment consists of measurement of migration percentage (MP) from a supine AP pelvis radiograph with standardized positioning [7] (Figure 1). Reimers Hip Migration Percentage is the percentage of body width of femoral capital epiphysis displaced out of the acetabulum (which falls lateral to perkins line) [8].Measurement of migration percentage of femoral head was done as given in the (Figure 2).
In the adult or older child, where the triradiate cartilages are fused and therefore inapparent, the inferior margin of the pelvic teardrop is used instead.The acetabular angle using Hilgenreiner’s line should be less than 28°at birth. The angle should become progressively shallower with age and should measure less than 22° at and beyond 1 year of age.
Present study an anteroposterior (AP) pelvic radiograph at the time of first visit was done. Any decrease in the range of movement at the hip or presence of scoliosis was a definite indication for further detailed radiological examination & immediate referral. In the present study 101 children were assessed between 4 and 9 years of age. Children with MP > 33% and > 40% were compared in relation to those with MP below these limits. Migration percentage (MP) in relation to CP subtypes and GMFCS grades were done.
Results
There were 48 boys and 53 girls (mean age 4.80 years). Distribution of Cerebral Palsy sub types were as follows. Hemiplegic 36 (35.64%), Quadriplegic 6(5.94%), Diplegic 43(42.57%) and Choreo athetotic 16(15%). 12 children were Gross Motor Function Classification System (GMFCS) level 5, while 26 were GMFCS level 4. Results of hip displacement by radiography as measured by MP in relation to CP subtypes and motor severity are presented in (Tables 1&2) and (Figure 3).
Only one child out of 36 children with spastic hemiplegia developed MP > 40%. The maximum number of hip displacements was seen in children with spastic quadriplegia, where 5 of 6 children (83%) had MP > 40%. Spastic diplegic and choreoathetotic subtypes showed intermediate risk of hip displacement (9 out of 43 and 7 out of 16 respectively had MP >40%). In the present study onset of hip displacement could not be assessed as hip surveillance was not done in a periodic basis. Figure 4 shows x-ray hip of 4-year-old with very minimal displacement (MP 33.33%) and Figure 4 shows severe hip displacement in an 8-year-old child.
According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40% compared to only 4.76% in GMFCS I and II put together.
Discussion
The natural history of spastic hip disease of CP is progressive lateral displacement of the hip secondary to spasticity and muscle imbalance in the major muscle groups around the hip. Displacement may progress to severe subluxation, secondary acetabular dysplasia, deformity of the femoral head, dislocation and painful degenerative arthritis [4,5]. The long-term effects of dislocation of the hip can be disastrous for individual patients leading to pain and loss of the ability to sit comfortably in up to 50% of cases [6]. Other problems include difficulty with perineal care and personal hygiene, pelvic obliquity and scoliosis, poor sitting balance and loss of the ability to stand and walk [7-11].
A hip is usually considered to be subluxed,if the migration is equal to or greater than 33%. Reimers [17] found that among normal, the 90th gentile for migration percentage at four years was 10% with spontaneous migration of less than 1% per year. An unstable migration percentage is when progression is greater than or equal to 10% over 1 year [12-16]. Present study has shown that even a single radiological evaluation could identify hip displacement in children after the age of 4 yrs. Majority of (5 out of 6) quadriplegic CP, had severe type of hip displacement compared to hemiplegic CP (1 out of 36). Compared to other bilateral types of CP diplegia had lower rate of hip displacement (9 out of 43). This may be because of the less motor function impairment. So GMFCS may be a better predictor for early prediction of hip structural impairment. It is seen that there is direct correlation between the GMFCs class and severe hip displacement. According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40% compared to only 4.76% in GMFCS I and II put together.
Subtyping of CP may have a role in predicting occurrence of severe hip displacement as shown by the almost complete occurrence in quadriplegic CP. However, a mere clinical examination and subtyping will not help in identifying severe hip disease in other type of CP. So, a systematic analysis of GMFCS is required for intensified screening of hip dysfunction. Moreover, as described in various guide lines periodic hip surveillance is mandatory for better ambulation and avoidance of surgery. This can be attained by early intervention measures. Figure 4 itself shows the importance of early surveillance. AACPDM - (American Academy for Cerebral Palsy and developmental medicine) recommends following schedule of hip surveillance (Table 3).
Conclusion
Need for hip evaluation in children with CP is emphasized by this study. All the children in this study did not undergo a hip Xray prior to the study. 22 out of 101 children had severe degree of hip displacement. The maximum number of hip displacements was seen in children with spastic quadriplegia and hemiplegia had very low risk. According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40 %. The study showed the relationship between the CP subtypes and the severity of the motor involvement in producing hip displacement. Referral to an orthopedic surgeon with experience in treating hip displacement in children with CP is recommended when there is presence of hip pain on history and/or physical examination. Periodic hip surveillance is mandatory for early detection of hip displacement. When the migration percentage is greater than 30% and/or there is less than 30 degrees of hip abduction with or without other findings, referral to an orthopedic surgeon is recommended [1,17].
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Orthopedics and Rheumatology please click on: https://juniperpublishers.com/oroaj/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/oroaj/OROAJ.MS.ID.555848.php
50 notes
·
View notes
Text
Hepatocurative and Gluco-stabilizing Potentials of Ethanol Extract of Stem bark of Flacourtia indica in Aluminium Chloride induced Toxicity in Albino Wistar rats | Juniper Publishers

Juniper Publishers-Open Access Journal of Biomedical Engineering & Biosciences
Authored by Idoko A
Abstract
Herbal therapies have been used to manage liver diseases resulting from hepatotoxicity and hyperglycemia. The study investigated the hepatoprotective and gluco-stabilizing abilities of ethanol extracts of stem bark of Flacourtia indica in albino Wistar rats. Thirty-one rats of mixed sex, weighing 165-285g were used and divided into five groups of A to E. Acute toxicity study of the plant’s stem bark was conducted on group E (20 rats). At phase 1, group A (negative control) was made up of 3 rats administered no AlCl3 and no leaf extracts while groups B (positive control), C and D (test) made of 4 rats each, administered 260mg/kg body weight AlCl3 only, for 7 days. At phase 2, groups C and D were treated with stem bark extract of Flacourtia indica for 7 days. Activities of Alanine aminotransferase, Aspartate aminotransferase, Alkaline phosphatase, concentrations of Bilirubin, Albumin, Total protein and blood glucose were assayed with histopathological study on euthanized rats’ liver.
Results of phase 1 showed significant (p˂0.05) increase in the liver function enzyme and blood glucose after induction with AlCl3 compared with (phase 2) values of liver function enzyme and blood glucose with significant (p˂0.05) decrease after treatment with stem bark extract. Histopathology results in phase2 showed regeneration and healing of damaged hepatocytes of phase1. In conclusion, the liver injury induced by AlCl3 was found to be effectively managed by the treatment with Flacourtia indica’s ethanol stem bark extracts, with blood glucose stabilized. This could be as a result of the antioxidants and phytochemical contents of the plant, with diver’s potency to scavenge free radicals and reactive oxygen species.
Keywords: Flacourtia indica; Gluco-stabilizer; Hepatic function; Hepatoprotective; Hyperglycemia; Stem bark
Abbrevations: ALT: Alanine Aminotransferase; AST: Aspartate Aminotransferase; WHO: World Health Organization; BIL: Bilirubin; TP: Total Protein
Introduction
The liver, a reddish – brown heaviest and largest internal organ weighs about 1.5 – 1.6 kg in an adult male and is about the size of an American football [1]. It is located behind the ribcage on the upper right side of the abdomen and is divided into four lobes with multiple lobes containing hepatic cells (hepatocytes). A normal liver enjoys an adequate blood supply and ability to regenerate its own tissues within few days [2]. The liver is known to perform over 500 functions in the body which include detoxification, excretion, digestion, metabolism, storage and homeostasis. It detoxifies harmful substances that are toxic to the body such as drugs, chemicals, heavy metals, alcohol and pesticides [3]. The liver excretes toxic chemical substances in the bile as well as xenobiotics, hormones and other by-products [4]. The liver plays a major role in homoeostasis stability of trace elements [5]. The liver is a major store house of glucose (in form of glycogen), iron and vitamins such as vitamins A, folate (B9), B12 and D [6]. Enzymes such as alanine aminotransferase (ALT), Aspartate aminotransferase (AST) and hormones are synthesized by the liver [7]. However, the liver is adversely affected by overloaded toxic substances, resulting in hepatotoxicity [8].
Hepatotoxicity is implicated with chemical induced liver damage resulting in chronic and acute liver diseases. Over 800 chemicals causing hepatic injuries abounds. They include drugs used to suppress pain and reduce inflammation such as ibuprofen, acetaminophen or paracetamol, naproxen and aspirin (Non-Steroidal Anti-inflammatory Drugs), alcohol, industrial and laboratory chemicals such as Aluminum trichloride AlCl3 and carbon tetrachloride CCl4 and natural toxins such viruses, aspergillus flavus [6,9,10]. Meanwhile, AlCl3 has demonstrated high potency in exerting hepatotocity, the mechanism by which AlCl3 exert its injury on the liver is not yet clear [9]. These induced toxic chemicals in the hepatic tissue, render the liver disease with malfunction including hepatitis, liver cancers, fatty liver, primary biliary cirrhosis, primary sclerosing cholangitis, hemochromatosis, hyperoxaluria and oxalosis and Wilson’s disease [11,12]. The earth is made up of about 8.13% of aluminium. The metal has got wide utilization, therefore increasing the chances of exposure into the body through the intestinal tract and the lung. It is a used in manufacturing cosmetics such as roll-on and deodorant, cooking utensils, food additives and drugs such as antacids. In water purification, aluminium salts are also used [13].
The practice of traditional medicine, using plants and plants products for the treatment of ailments is an age long practice. Several medicinal plants with their herbal functions have been discovered and more are still be researched on [14]. Medicinal plants have been found to possess several activities such as hepatoprotective, nephroprotective, antimicrobial, anticancer, anti-inflammatory, hypoglycemic, antihypercholesterolemia, hypoglycemia, heamatinic and antioxidant activity [15-17]. These beneficial therapeutic properties and efficient pharmacological impacts of medicinal plants on man and animals are not farfetched from the numerous bioactive compounds they contain [18]. The availability of herbal alternatives for the management of liver disease and other ailments is been encourage by world health organization (WHO) to be better developed for improved efficacy, safety of use, cheap to purchase and accessible for patronage [19].
Flacourtia india is a wide spread medicinal plant, of Salicaceae family, tribe of Flacourtiaceae, genus of Flacourtia and specie of Indica [20, 21]. It is known as Governor’s plum in English, kondai or Katai in India, Cilimu in China and in Nigeria: it is called Akpuru in Igbo, Isada in Hausa and Iyeye in Yuroba [22]. The plant is tropical specie with a natural geographical occurrence in Africa and Asia. Predominantly, Flacourtia india is said to be a native to both Africa and East Asia [23]. Flacourtia indica is a bushy small shrub like tree, having a spiny, erect, rough, strong stem bark, that extend with branches. It spines branched and spread up to 12cm long and to a maximum height of about 15cm (50 feet) [22]. Several pharmacological abilities of Flacourtia indica have been exploited with the whole plant, leaf, seed, fruit, stem, bark and root. These include hepatoprotection against AlCl3, paracetamol and CCl4 induced hepatic damage [9,24], anti-diabetic, anti-anxiety, antimicrobial, anti-malaria, anti-asthmatic, diuretic, antioxidant, analgesic/anti-inflammatory and anti-hyperlipidemia [18,25- 27]. The plant has been reported by previous researchers in their phytochemical analysis to contain several bioactive compounds, including phenolic compounds, flavonoids, saponins, carbohydrate, Coumarin Glycosides [28].
Blood glucose concentration is an important index handled by the liver in monitoring and stabilizing blood glucose levels. In post absorptive state, the fasting blood glucose concentration of a healthy (normal) individual is 70 – 100mg/dl (4.5-5.5mmol/l). However, after eating a carbohydrate meal, the level of blood glucose may rise to 120-140mg/dl. It is generally established that the value for plasma concentration is about 15% slightly higher than the value of blood glucose. Hypoglycemia implies a decrease in blood glucose concentration from the normal and hyperglycemia is an increase in blood glucose concentration from the normal [29,30]. Plants have been reported to have herbal ability in reducing high glucose concentration, not necessarily causing an unhealthy hypoglycemia, but attempting to stabilize blood glucose level in albino wistar rats [30]. Thus, in view of these, it became imperative to investigate the hepatocurative and gluco-stabilizing effects of stem bark of Flacourtia indica using ethanol solvent extraction in order to ascertain the previous claim and establish new fact.
Materials and Methods
Chemicals
Aluminium trichloride AlCl3 was purchased from BDH Laboratories/Chemicals Ltd, Poole, England. Kits used for the liver function assay were obtained from Randox Laboratories Ltd, 55 Diamond Road, Crumlin, country Antrim, BT29 4QY, United Kingdom. They include; Bilirubin (BIL), Alanine Aminotransferase (ALT), Aspartate Aminotransferase (AST), Albumin (ALB), Total Protein (TP). All other chemicals used are pure and of analytical grade.
Collection and Preparation of Plant Samples
Fresh plant materials of Flacourtia indica (Governor’s plum) were collected from around Emene jurisdiction in Enugu state, Nigeria. The required plant stem bark was authenticated and a voucher number of PSB/109-12. A was given by Mr. Okafor, C.U., a botanist in plant tissue culture and biotechnology department, Faculty of Biological Science, University of Nigeria, Nsukka. The plant extract was prepared by pilling the bark from the stem of the plant and cut into pieces for easy air drying. The dried samples were ground into powder using an electric grinder. The powdered parts were soaked in ethanol and allowed to stay for 48 hours at room temperature after which they were filtered. After filtration, the samples were then taken and evaporated to dryness using water bath at 80oc. The evaporated extracts were reconstituted with distilled water relative to the weight of the evaporated extract. The volumes of the extracts to be administered were calculated according to the body weight of the rats using the formula:
Collection and preparation of blood sample
Three milliliter (3mls) of blood was collected from the rats by capillary pressure insertion into the side of the eye using capillary tubes into a plain bottle, for the collection of serum used for biochemical assay (liver function test). The samples in bottles were stored at room temperature.
Acute Oral Toxicity (LD50) Study
Twenty (20) rats were used for oral acute toxicity study (LD50) of the plant. The acute toxicity study of ethanol stem bark extract of Flacourtia indica was evaluated in two phases as described by [31]. In the 1st phase, doses of 10mg/kg, 100mg/kg, and 1000mg/kg were administered to 3 rats each. The body weight of rat was noted before and after extract administration. Single dose of ethanol extract was administered orally and observed from the time of administration, for toxic symptoms, such as behavioral changes, loco-motion, convulsion and mortality, then overnight and finally for a time period of five days. In the absence of mortality in the first phase, higher doses of 1500mg/kg, 2500mg/ kg, 3500mg/kg and 5000mg/kg were then administered on 1 rat each of which one mortality was observed in the 2nd phase of the experiment at 3500mg/kg body weight. LD50, the amount or lethal dose of materials given all at once, which causes the death of 50% of a group of test animals was calculated with the formula below;
Study Animals
Albino Wistar rats of 165-285g weight, of either sex were obtained from university of Nigeria Nsukka. Animals were housed at an ambient temperature and relative humidity in the animals’ house of natural sciences, Caritas University, Amorji – Nike Enugu. The rats were allowed to acclimatize for one week prior to the experiment and had access to standardized pelletized finisher feed and clean water within the period the acclimatization. The principle of laboratory animals’ care and ethical guidelines for investigation of experimental pain in conscious animals were followed respectively [32,33].
Experimental Design
Experimental design was carried out in two phases thirty five (35) Wistar albino rats were used, divided into A, B, C, D and E as follows; at phase 1,
Group A: Control (negative control) consist of 4 rats, no Aluminum chloride (AlCl3 were administered.
Group B: Test control (positive control) consist of four (4) rats, were administered orally with 260mg of Aluminum chloride (AlCl3) without extract given.
Group C: Consist of four (4) rats, were orally administered with 260mg/kg body weight of rats.
Group D: Consist of four (4) rats were orally administered with 260mg/kg body weight of rats. At phase 2, groups C and D were treated with ethanol stem bark as follows;
Group C: Consist of four (3) rats, were treated with stem bark extracts of 500mg/kg body weight of rats.
Group D: Consist of four (3) rats were treated with stem bark extract of 700mg/kg body weight of rats.
At the end of phase 1 and 2, one rat from each group was randomly selected and sacrificed by euthanization using chloroform and liver removed for histopathology study.
Induction of Liver Injury
Liver injury was induced in rats of group B – D by single oral administration with 260mg/kg body weight of AlCl3 respectively.
Liver Function Assay
After collection of blood sample from rats serum was collected by clot retraction. Serum ALT, AST, ALP, Albumin, Total protein and Bilirubin were assayed with the use of kits from Randox Laboratories Ltd, 55 Diamond Road, crumlin, country Antrim, BT29 4QY, United Kingdom, following the manufacturer’s procedure.
Histopathological Studies
The selected models were sacrificed and dissected after which the liver organs were excised and fixed in a buffer medium of 0.9% of formalin solution in plain tissue bottles. The tissues were embedded in paraffin, solid section was cut 5um and stained with hemotoxin and eosin, the sections were examined and analyzed by the distant Specialist of histopathology, University of Nigeria under high microscopy instrumentation having photomicrographic attachment.
Statistical analysis
Results were expressed as mean ± standard deviation and analyzed using one-way ANOVA (analysis of variance, p value (p<0.05) was considered significant. A component of graph pad instat 3 software version 3.05 by graph pad Inc. was employed [34].
Results
Acute toxicity results
The oral administration of ethanol extract of F. indica stem bark resulted in behaviour changes and mortality up to the dose of 3500 mg/kg body weight at the second phase. Though, the LD50 of F. indica ethanol stem bark extract was calculated to be 4183mg/kg (higher than 3500 mg/kg). Table 1 shows the result of the acute toxicity in phase 1 and 2. The liver function test of rats after induction with 260mg AlCl3, for liver injury is shown in Table 2. A significant (p<0.05) increase was observed in TP, ALB, BIL, ALP, ALT and AST of control compared to test control and test groups.
Table 3 shows liver function indices of rats administered various dose of stem bark (500mg and 700mg) extract of flacourtial- Indica for 0ne week. A significant (p<0.05) increase was observed in all parameters assayed in the test groups compared to the test control and control group. The significant increase (p<0.05) in Table 2 when compared to Table 1, reveals the potential hepato- healing effect of Flacourtia indica not necessarily in a dose dependent manner.
Results are mean ± standard deviation, Values in the same column bearing similar superscripts are significantly different at P<0.05. (n=4).
Key: A: Control Group; B: Test Control; C and D: Test groups.
TP: Total Protein; ALB: Albumin; BIL: Bilirubin; ALP: Alkaline Phosphatase; ALT: Alanine Transaminase; AST: Aspartate Transaminase
Results are mean ± standard deviation, Values in the same row bearing similar superscripts are significantly different at P<0.05. (n=4).
Key: A: Control Group; B: Test Control; C and D: Test groups; TP: Total Protein; ALB: Albumin; BIL: Bilirubin; ALP: Alkaline Phosphatase; ALT:
Alanine Transaminase; AST: Aspartate Transaminase
Table 4 presents the blood glucose concentration of rats after induction with AlCl3 and after Treatment with stem bark extracts of Flacourtia indica. After administration (treatment), with Flacourtia indica, the blood glucose concentrations of test groups (C and D) decreased significantly (p<0.05) compared to after induction with AlCl3 in a dose dependent pattern, thus acerbating induced hypoglycemia.
Results are mean ± standard deviation, Values in the same row bearing similar superscripts are significantly different at P<0.05. (n=4).
Key: A: Control Group; B: Test Control; C and D: Test groups
Result of Histopathology Analysis
The results of histopathological study of liver tissue of rats at induction (group A and B), after induction with AlCl3 and after treatment with F. indica ethanol stem bark extract (group C and D) as cross sections are shown in Figure 1 & 2. Photomicrograph of liver showed cytoplasm containing empty (black arrow) and fluid filled (red arrow) appearing vacuoles which pushed out the nucleus and then formed a signet-ring like appearance. H&E. mag. 400X (Figure 3). Photomicrograph of liver showed minor distortion of the hepatic cords leading to enlarged sinusoids (black arrow), also macrophages (red arrow) and focal necrosis (star) were also observed. H&E. mag. 100X (Figure 4). Photomicrograph of liver showed massive influx of inflammatory cells (black arrow), damaged hepatocyte (red arrow), degeneration of the hepatocyte cords and the affected hepatocytes are aligned in deformed cords which compresses the lumen of the sinuses. Zonal fatty changes occurred in the liver lobules, diffusely affecting the same zone. The fatty degeneration, vacuoles appeared in the cytoplasm around the nucleus, because the lipid content may be dissolved in the course of embedding. The vacuoles are empty with absence of inflammatory cells (black arrows) and regenerated hepatocytes (white arrows). H&E. mag. 400X.
Discussion
The significant increase that was observed in the liver function indices in Table 2 of groups C and D, as compared to Table 3 was as a result of aluminium chloride administration. This result is consistent with other researchers’ who reported that aluminium chloride is capable of inducing hepatic injury (hepatotoxicity), using a minimal dose of 34 mg/kg body weight administered in rats’ diet [35] and oral exposure in drinking water of 40 male Wistar albino rats of 0, 64mg/kg, 128mg/kg and 256mg/kg body weight AlCl3 for 120days, respectively [9]. AlCl3 induced toxicity has been reported to have toxic effects on liver, kidney, biochemical dysfunction and general health challenge [13]. A significant increase was seen in blood glucose concentration of rats after induction with AlCl3 compared to after treatment with Flacourtia indica (Table 4). This increase could have resulted from the inability of the liver to secret insulin owing from the hepatic damage caused by AlCl3. The mechanism through which this was done was taught to be linked to hepatic-stress related release of epinephrine, a factor inhibiting insulin secretion [36].
The potent inducement of liver injury by AlCl3 was supported by histopathology results (Figures 1, 2, 4 & 5). The underlying mechanism through which AlCl3 induces hepatic damage, as hepatic toxicant, as shown by the histopathology results could be associated to fatty liver incidence as a result of accumulated triacylglycerols and lipoprotein [36]. The histopathological results’ examination of liver tissues reveals intact hepatocytes, distinct architecture of kupffer cells and cytoplasmic aligning of the negative control group. Induction by AlCl3 in test groups revealed several degrees of hepatic injuries including; infiltration of mixed infiltrates in the sinusoid, diffused fatty changes, focal necrosis, massive influx of inflammatory cells, damaged hepatocyte, degeneration of the hepatocyte cords and the affected hepatocytes are aligned in deformed cords which compresses the lumen of the sinuses (Figures 2, 4 & 5). Treatment with Flacourtia indica’s ethanol extract stem bark with 500 mg/kg and 700 mg/ kg in rat’s liver revealed regeneration of hepatocytes, absence of inflammation, with almost healed hepatic architecture (Figures 3 & 6). This is also consistent with [28], supporting the claim that Flacourtia indica protects the liver against AlCl3 hepatic damage in treated groups with healing features, typified by absence of damaged and degenerated hepatocytes, necrosis and inflammation.
Treatment of the AlCl3 induced hepatotoxic rats with the stem bark extract of Flacourtia indica revealed a significant decrease in AST, ALT, BIL, TP, ALP and blood glucose concentration and a slight significant increase in serum albumin, implying that hepatic tissues are regenerating and healing. This observation was supported by the histopathology analysis of the liver tissues which shows recuperation of hepatic cells after administration of the stem bark extract. This is in support of the work of [28], who reported that Flacourtia indica prevents and protect AlCl3 and CCL4 induced rats’ hepatic damage through augmentation of antioxidant enzyme activity. Flacourtia indica appears to prevent the increase in the activities of the main liver function enzymes (ALP, AST, ALT, BIL and TP) by a counter and effective action against the hepatoxic damaging effects of AlCl3. This action might be due to Flacourtia indica’s potentials as an indirect antioxidant promoter and free radical scavenging abilities in preventing membrane failure and cellular necrosis [20].
Table 4 shows the blood glucose concentrations and effect of oral administration of the different doses after induction with 260 mg AlCl3 and 500 mg/kg and 700 mg/kg body weight of Flacourtia indica on blood glucose concentrations of rats. After administration of stem bark extract of Flacourtia indica, the blood glucose levels of test groups (C and D) decrease significantly (p<0.05) compared to after induction with AlCl3 in a dose dependent pattern, thereby bringing the concentration of blood glucose to a stabilized level from the AlCl3 induced hepatotoxic level. Reduction in blood glucose by Flacourtia indica’s stem bark could be due to the presence of both micro and macro mineral elements and phytochemicals, having antioxidant and blood glucose enzyme regulating and stabilizing control [19,28,37,38], reported the mineral elements composition in Flacourtia indica to include magnesium, manganese and zinc. Thus, the mechanism behind the stability of blood glucose by Flacourtia indica could be understood from the role of these mineral elements as cofactors to glycolytic enzyme especially hexokinase and phosphofructose [17]. The blood glucose level stabilizing effects of Flacourtia indica appears to be maintained by the constant furnishing of these mineral elements [37,38].
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Biomedical Engineering & Biosciences please click on: https://juniperpublishers.com/ctbeb/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/ctbeb/CTBEB.MS.ID.555971.php
28 notes
·
View notes