
27 // MD Class of 2021 // medblr+studyblr // Happy to answer any questions about the medical school process in the US.
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by humanitymed and here's what we found interesting.
Average Info
Notes Per Post
555K
Likes Per Post
313K
Reblog Per Post
241K
Reply Per Post
838
Time Between Posts
17 days ago
Number of Posts By Type
Text
17
Last Seen Tumblr Blogs




Fun Fact
In February 2021, Tumblr had 518.6 million blog accounts.

Text
This kinda turns into a ramble, but I was listening to a podcast that was recorded in 2015 about how technology would be impacted by a variety of apocalyptic events.
One of them was a pandemic that caused a reduction in population.
And one of the things they mentioned was that in a reduction in population, we couldn't replace a workforce with labor-saving robots quickly enough to shore up important facets of modern life like the power grid or healthcare systems, and that those systems would have a limited number of days before total collapse occurred.
Which of course we know to be accurate- while we're not at the point of total collapse (yet) you don't even need black plague numbers to reduce the workforce to the point of a substantial reduction in service.
Except that instead of people going "oh well, seeing as there are fewer living, able-bodied people capable of working due to the pandemic we are currently experiencing together, I can't really have the same expectations of service I did 5 years ago because it took a lot more people to provide that level of service" they're complaining about how people "no longer want to work" and that service has become "completely unacceptable".
Like, I've been yelled and cussed at, fired (by a patient, which means (and has always meant) literally nothing in the grand scheme of things), and told that my service was outright negligence (when it was actually far above the crisis standard of care we are operating under, and will be operating under I assume indefinitely because I don't see us coming back from this for a few solid generations).
Talk to a few bedside nurses (or literally anyone in the service industry, I just happen to be in healthcare) and you'll learn that people got mean in February of 2021. That time when the confluence of a staffing crisis and people running out of emotional energy to care about the multiple simultaneous crises that were (and continue to be) going on all the time. And a lot of them just started yelling.
Like, I'm rambling now, but it's not even about reminding everyone that everyone is doing their best, working flat out doing 2 or 3 people's jobs at a minimum and that's beyond anyone's ability to do well.
It's about asking people to remember that the reason for this now permanent reduction in service is not some nebulous personal failing of an individual who is serving you inadequately, it's that too many people are dead or disabled to provide 2019 service, and that's going to be ever again in your life.
So if you don't want to be constantly angry at service industry people for literally the rest of that life, accept that you're living through the hellish alternate ending of Contagion where the EIS personnel were spit on and the population refused to isolate and get the vaccine, thus creating an unthinkable superbug that people proceeded to completely ignore until they caught it and became disabled or died.
And we get to listen to podcasts from a time before where such things were laid out as "could be's" of an apocalyptic future.
120 notes
·
View notes
Text
It’s weird when you find out your attending is twitter famous...
4 notes
·
View notes
Text
It’s odd. I’d say 95% of the time when a patient becomes a CMO or hospice candidate you know what decision the family is eventually going to make, they’re just not ready to make it. Kind of feels like a pseudo choice, you know? We make families have these big conversations where we talk about how a patient is dying and we recommend keeping them comfortable...I guess theoretically the option is to “do everything we possibly can” or keep them comfortable, but it’s hard to present that option as a HCW because often in my head it’s really keep them comfortable or make them suffer before they die.
When we have disagreements with family members in these scenarios it’s almost always because the family wants to keep going with aggressive measures and we don’t see any utility in that. It’s always shocking, I mean genuinely takes us aback when a family wants us to stop being aggressive when we want to keep going. It’s so unusual, so rare...it makes it harder when we are at a stalemate in the other direction with a family because you want to say, look. we never say no to doing more if we thought we could do more. our default is to want to do more. if we’re saying we want to keep them comfortable it’s because we believe there is zero utility in continuing as we’re doing.
There are always people though that will say, hey, the doctors told us my uncle wouldn’t live 3 more weeks and he lived three more months! that’s why I can’t give up on mom! And sometimes I just want to shake them and say, were those three good months? How many of those weeks were in a hospital? How often were the nurses holding down the patient so the doctor could shove a NGT down their nose? Were you there when they were crying from needlesticks every morning? Were you there when they kept ripping off the O2 mask because they didn’t want it on their face anymore?
Not to downplay the burden of that decision for families. It’s hard. It’s really hard. It’s just...also hard to watch. It’s hard to do. I feel for the nurses most of all, who are often the ones who have to do the physical work of carrying out a plan for someone who is clearly suffering to those who know what suffering looks like.
Phew! that became a rant.
there’s a really morbid type of anticipatory waiting that comes with someone advancing to end of life care, especially when you’re in healthcare and can interpret what the writing on the wall says
22 notes
·
View notes
Text
Dear intern,
You are doing awesome. There are no mistakes, only opportunities to learn. Just remember that no one walks into intern year knowing WTF they’re doing. You’re not alone. If others got to the other side of training intact, so can you. You’re doing great.
301 notes
·
View notes

Text
It makes me want to cry reading this. You can’t imagine the hoops physicians in the US have to jump through to get care for their patients. Of course you have already seen how frustrating it is from the patient side of things. We too are exhausted by it. My co resident the other day was asked to do a peer to peer with an insurance company about an echocardiogram. An echo of all things!

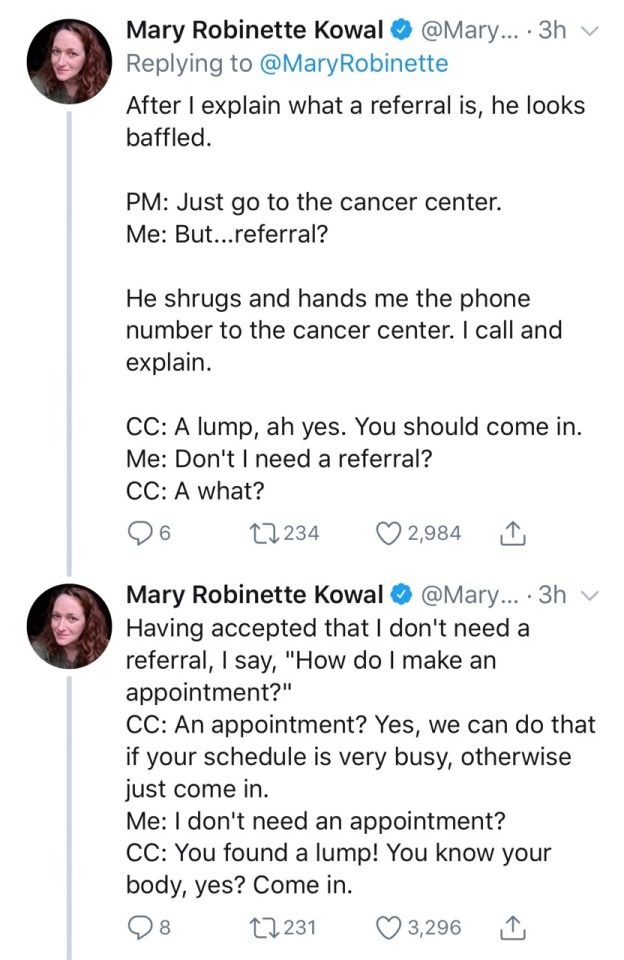
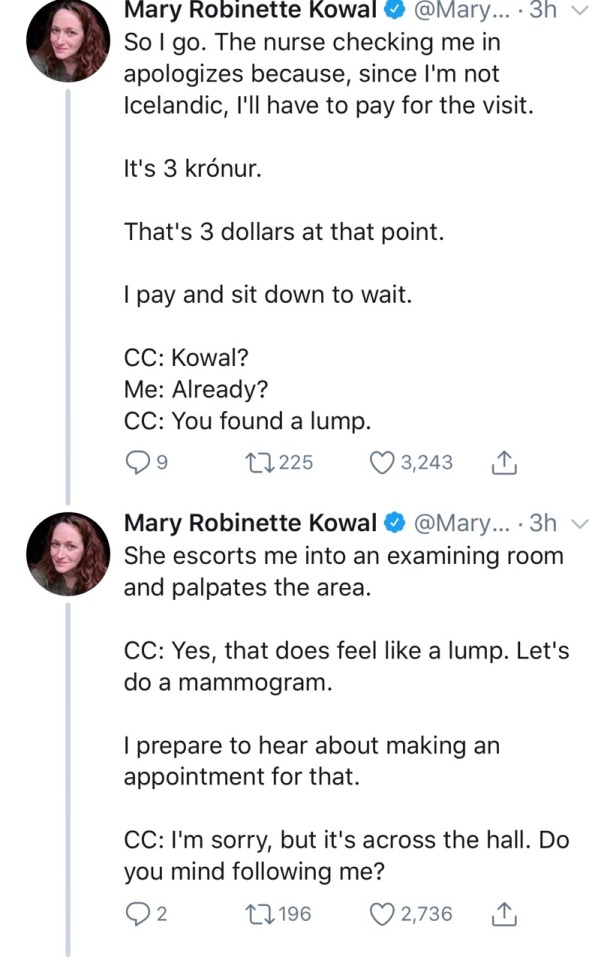
The next time they tell you Americans are “happy” with their employer provided health insurance remember that that “happiness” is fueled by willful ignorance of what the alternatives are really like and fear of losing what little crappy health care they currently have.
347K notes
·
View notes
Text
What I don’t understand is how they see things while scrolling so quickly...
“Why do radiologists always find the smaller things? Is it really their trained eyes, or do they just have ridiculously big screens?”
112 notes
·
View notes
Text
Pure sadness, especially when it’s a drink you actually paid good money for. I got a free cup of coffee the other day and I was so excited about it...immediately got swamped and by the time I was able to drink it, it was cold. Cold and in a non-microwaveable cup, too. Ugh.

My medical professional followers/friends will know this look - aka you bought a drink into work and it was pure chaos as soon as you clocked in so you didn’t get to drink it and when you finally do it is in a…questionable state. The flavoring is back to the bottom and the ice has melted so the coffee is watered down. This is a very specific experience and I hope all of medblr can taste this photo. It tastes like stress. And shame.
25 notes
·
View notes





Text
Every time I consult cardiology and nephrology at the same time for a CHF + CKD patient, I enjoy sitting back to watch the ensuing chaos I created.
217 notes
·
View notes
Text
The world stands with Ukraine

Tbilisi, Georgia

St. Petersburg, Russia

London, England

Paris, France

Thessaloniki, Greece

Rome, Italy

Berlin, Germany

Tokyo, Japan

Montenegro

Mumbai, India
87K notes
·
View notes
Text
I don’t even understand how this happens. Every time I’ve accidentally started to present a med student’s patient as an intern I’ve either remembered the med student was assigned that patient or either the attending or resident cuts in to remind the room it’s the med student’s patient. I LOVE when med students present my patients - less work for me! Seriously it’s the resident’s responsibility to remember things like that. I’m sorry that happened to you.
Yesterday one of the residents presented my patient before I could (something that has happened daily on this service), and when another resident noticed I was a little annoyed, she said “you’ll get em next time, tiger!” Ma’am I am 25.
30 notes
·
View notes
Text
ur early 20s are about being obsessed with kindness and mary oliver and seasonal fruits and recreating comfort foods you ate as a child and learning how to love and crying because you have no choice but to live the life before you and finding god on the bus back from the grocery store
44K notes
·
View notes
Text
If you can report, report. There is no place for mistreatment of students in academic medicine. That attending can work at a non-teaching hospital if he wants.
Literally had the worst consult experience today.
Let me explain. It's my first day on a rotation that I've never done before but the block is set up as if I had prior experience with additional duties, responsibilities and patients. I was feeling a little overwhelmed, but honestly doing okay and managing things despite feeling very timid and unsure. I started the day with a positive attitude and was open to learning and feedback because I know I have a lot to figure out in the next 4 weeks.
Things in the morning were a little rushed but going fine overall. But then I go to make a consult and the attending at the other end of the phone just utterly berates me. Because, how dare he, an attending, have to answer a phone call from a student.
Never mind that I didn't get any farther than introducing myself and never even brought up the patient that I was wholly prepared to present. Nevermind that his service routes consults to the attendings and not to residents as a standard protocol therefore consults from trainees around be expected.
I have never had anyone talk to me so unprofessional at work before. I've put up with a fair amount of shit. From inappropriate behavior to bad attendings to rude coworkers, this guy was by far the worst.
I was working so hard to make a good impression and do well today. Despite feeling so uncertain about it all, I did recognize that I was actually doing pretty well for an overwhelming first day. I felt like even though I didn't actually want to be on this block when all my classmates are taking fun or easy electives (or even a month off), the extra work would pay off next year so I hopefully wouldn't feel like I'm drowning at the start of intern year. I didn't choose this rotation because I wanted to do it or thought it was fun. I did it because I knew figuring out this crap now would pay off exponentially next year when my workload would practically double.
And some asshole attending with a gigantic ego thought that it was beneath him to talk to a student. Like I was the scum of the earth. He just absolutely ripped me a new one. How dare a trainee talk to faculty at an academic institution?!
If I could drop this block, I would. I had no desire to be here before today but have even less of a desire to go back.
I know what program is dead last on my rank list. Easiest decision all year.
30 notes
·
View notes