My name is Miranda, 36, (She/Her). I am a writer and I am a chaotic neutral reblogger. Please....Feel free to drop in :) AO3: her_imperius_condessy BlueSky: @boocooblue.bsky.social CashApp: $mirandawrites2013
Last active 4 hours ago
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by her-imperius-condessy and here's what we found interesting.
Average Info
Notes Per Post
3M
Likes Per Post
1M
Reblog Per Post
2M
Reply Per Post
1K
Time Between Posts
4 hours ago
Number of Posts By Type
Text
8
Photo
8
Video
1
Last Seen Tumblr Blogs





Fun Fact
Tumblr’s reach among the 26-to-35-year-olds in the US is 11%.
Text
why does my mother suddenly fail kindergarten whenever she tries to do anything on the computer
#my mother is one of the smartest women I know#She navigated her own divorce settlement and outfoxed my dad's lawyer#But the computer?#Oh no we can't figure that out#I have 'fixed' her computer so many times
110K notes
·
View notes










Photo




“Our clearest memory of the show, we think, will be when Darren broke character a tiny bit, for a moment alone on that stage, saying thank you and goodbye, and that it had been “totally awesome.” Just those two words, he looked the audience in the eye and used his natural voice. That was for us and I don’t think that anyone there will ever forget it, because Darren will always be in StarKid, but things are changing from here on out and he will never be our Harry again.”
6K notes
·
View notes
Text
me, every single time i get a kudos on ao3: someone liked my writing. one real irl human being read something i wrote and enjoyed it. they thought it was good enough to read to the end and click the button. an actual person. they liked it.
47K notes
·
View notes
Text
if youre ever feeling bad just look at pictures of albatross chicks bc theyre adorable but also fucking hilarious like the parents look like they go to pta meetings in full makeup carrying gucci handbags and the babies look like funky little muppets and i love them






203K notes
·
View notes




Text
A doctor discovers an important question patients should be asked
This patient isn’t usually mine, but today I’m covering for my partner in our family-practice office, so he has been slipped into my schedule.
Reading his chart, I have an ominous feeling that this visit won’t be simple.
A tall, lanky man with an air of quiet dignity, he is 88. His legs are swollen, and merely talking makes him short of breath.
He suffers from both congestive heart failure and renal failure. It’s a medical Catch-22: When one condition is treated and gets better, the other condition gets worse. His past year has been an endless cycle of medication adjustments carried out by dueling specialists and punctuated by emergency-room visits and hospitalizations.
Hemodialysis would break the medical stalemate, but my patient flatly refuses it. Given his frail health, and the discomfort and inconvenience involved, I can’t blame him.
Now his cardiologist has referred him back to us, his primary-care providers. Why send him here and not to the ER? I wonder fleetingly.
With us is his daughter, who has driven from Philadelphia, an hour away. She seems dutiful but wary, awaiting the clinical wisdom of yet another doctor.
After 30 years of practice, I know that I can’t possibly solve this man’s medical conundrum.
A cardiologist and a nephrologist haven’t been able to help him, I reflect,so how can I? I’m a family doctor, not a magician. I can send him back to the ER, and they’ll admit him to the hospital. But that will just continue the cycle… .
Still, my first instinct is to do something to improve the functioning of his heart and kidneys. I start mulling over the possibilities, knowing all the while that it’s useless to try.
Then I remember a visiting palliative-care physician’s words about caring for the fragile elderly: “We forget to ask patients what they want from their care. What are their goals?”
I pause, then look this frail, dignified man in the eye.
“What are your goals for your care?” I ask. “How can I help you?”
The patient’s desire
My intuition tells me that he, like many patients in their 80s, harbors a fund of hard-won wisdom.
He won’t ask me to fix his kidneys or his heart, I think. He’ll say something noble and poignant: “I’d like to see my great-granddaughter get married next spring,” or “Help me to live long enough so that my wife and I can celebrate our 60th wedding anniversary.”
His daughter, looking tense, also faces her father and waits.
“I would like to be able to walk without falling,” he says. “Falling is horrible.”
This catches me off guard.
That’s all?
But it makes perfect sense. With challenging medical conditions commanding his caregivers’ attention, something as simple as walking is easily overlooked.
A wonderful geriatric nurse practitioner’s words come to mind: “Our goal for younger people is to help them live long and healthy lives; our goal for older patients should be to maximize their function.”
Suddenly I feel that I may be able to help, after all.
“We can order physical therapy — and there’s no need to admit you to the hospital for that,” I suggest, unsure of how this will go over.
He smiles. His daughter sighs with relief.
“He really wants to stay at home,” she says matter-of-factly.
As new as our doctor-patient relationship is, I feel emboldened to tackle the big, unspoken question looming over us.
“I know that you’ve decided against dialysis, and I can understand your decision,” I say. “And with your heart failure getting worse, your health is unlikely to improve.”
He nods.
“We have services designed to help keep you comfortable for whatever time you have left,” I venture. “And you could stay at home.”
Again, his daughter looks relieved. And he seems … well … surprisingly fine with the plan.
I call our hospice service, arranging for a nurse to visit him later today to set up physical therapy and to begin plans to help him to stay comfortable — at home.
Back home
Although I never see him again, over the next few months I sign the order forms faxed by his hospice nurses. I speak once with his granddaughter. It’s somewhat hard on his wife to have him die at home, she says, but he’s adamant that he wants to stay there.
A faxed request for sublingual morphine (used in the terminal stages of dying) prompts me to call to check up on him.
The nurse confirms that he is near death.
I feel a twinge of misgiving: Is his family happy with the process that I set in place? Does our one brief encounter qualify me to be his primary-care provider? Should I visit them all at home?
Two days later, and two months after we first met, I fill out his death certificate.
Looking back, I reflect: He didn’t go back to the hospital, he had no more falls, and he died at home, which is what he wanted. But I wonder if his wife felt the same.
Several months later, a new name appears on my patient schedule: It’s his wife.
“My family all thought I should see you,” she explains.
She, too, is in her late 80s and frail, but independent and mentally sharp. Yes, she is grieving the loss of her husband, and she’s lost some weight. No, she isn’t depressed. Her husband died peacefully at home, and it felt like the right thing for everyone.
“He liked you,” she says.
She’s suffering from fatigue and anemia. About a year ago, a hematologist diagnosed her with myelodysplasia (a bone marrow failure, often terminal). But six months back, she stopped going for medical care.
I ask why.
“They were just doing more and more tests,” she says. “And I wasn’t getting any better.”
Now I know what to do. I look her in the eye and ask:
“What are your goals for your care, and how can I help you?”
-Mitch Kaminski
Source
119K notes
·
View notes
Photo
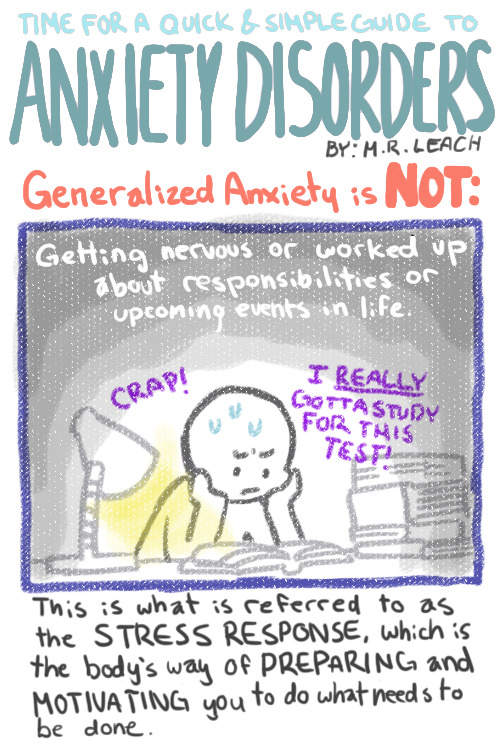


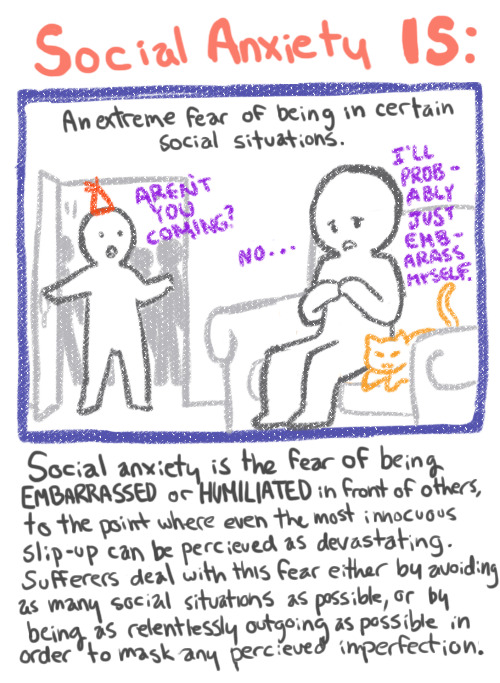

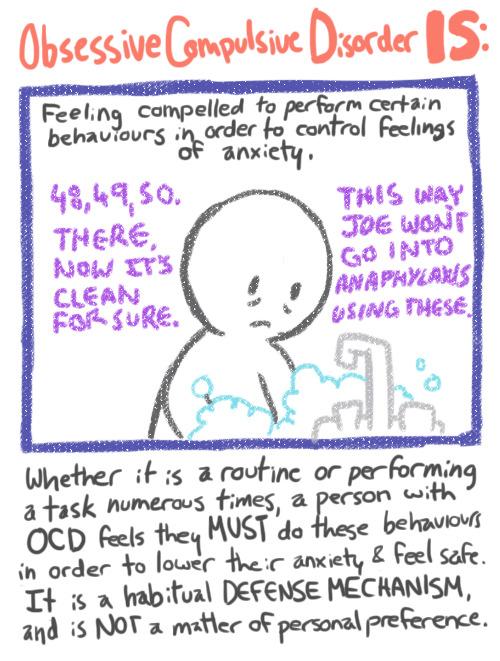
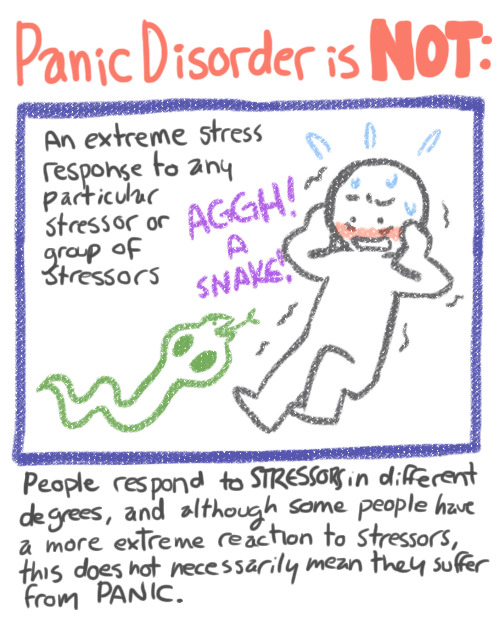


Some things I’ve learned in the CBT clinics I’ve been going to regarding anxiety that I thought might be helpful to some.
415K notes
·
View notes
Text
if we want to stop the patriarchal concept of surnames being passed down the male line, we have a few options options that i’d be 100% fine with:
children get whichever surname is cooler, to eliminate uncool surnames over the generations
children get whichever surname is rarer, to achieve a utopian future in a few centuries where all surnames are more or less equally common
children’s surnames are randomly generated: say, heads for parent #1’s surname, tails for parent #2’s surname
parents pick the first names first, and then a court decides which surname fits it better. so if a couple named mr. madison and mr. liu want to name their daughter alison, she’ll get the surname liu, because alison madison sounds ridiculous
everyone stops having children right now
108K notes
·
View notes
Photo
SPIDER-MAN: INTO THE SPIDER-VERSE + letterboxd reviews (x, x, x) insp.
38K notes
·
View notes

Text
I love the concept of Tooks. "Everybody in the Shire is very very businesslike and respectable and has no use for adventures except for this one entire family of mad lads who also run the municipal government"
39K notes
·
View notes
Video
342K notes
·
View notes
Photo



“Work was hell today.” (comic by AxbyMag)
444K notes
·
View notes

