
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by brooklyntobangalore and here's what we found interesting.
Average Info
Notes Per Post
15
Likes Per Post
15
Reblog Per Post
0
Reply Per Post
0
Time Between Posts
3 days ago
Number of Posts By Type
Text
17
Last Seen Tumblr Blogs





Fun Fact
Tumblr has been banned in Indonesia for providing people with access to pornographic content.
Text
Pain & Palliative Medicine Rotation
I spent Weeks 4 and 5 with the Pain & Palliative Medicine Department. It was an opportunity to engage with issues pertaining to end-of-life care and to see how culture and class influence medical decision-making for patients with terminal illness. Palliative medicine is a relatively new sub-specialty in India; it didn’t become its own distinct department at St. John’s until 2008. Most low- and middle-income countries, India included, still have little access to palliative care. The St. John’s website describes the philosophy of Palliative Medicine as follows 1:
“Palliative Medicine is a multidisciplinary approach to specialized medical care for people with life-limiting illnesses. It focuses on providing people with relief from the symptoms, pain, physical stress, and mental stress of the terminal diagnosis. The goal of such therapy is to improve quality of life for both the person and their family.”
As such, the focus is on holistic symptom management (esp. pain management) and improving quality of life, rather than on curative interventions – a concept that several attendings remarked is still difficult for patients and families in India (or in the U.S., for that matter…) to accept. Palliative Medicine is a consultative service for the most part, and a majority of the terminal inpatients we rounded on were cancer patients. Still, approx. 80% of the caseload consisted solely of pain management for non-terminal patients – an indication, according to our attending Dr. T, that palliative care is still under-utilized as a service.
The nature of the specialty means that witnessing tragedy is inevitable: a 38 year old lady battling Stage IV ovarian cancer for years and finally succumbing; a small 6 year old boy with an aggressive form of metastatic Wilm’s tumor; colon cancer causing bowel obstruction and extreme abdominal pain; lung cancer making breathing difficult. The families by and large handled their adversity with grace, and I was often moved to see them advocate for their loved ones so adamantly – to ensure that pain and suffering would be minimized even if a cure was elusive or impossible.
Pain management was an important aspect of daily rounds; a lot of care was taken to ensure that dosages of pain meds (usu. opioids) were appropriately titrated. The Palliative team followed the so-called ‘WHO Ladder’ for pain management, whereby pain meds would be escalated from non-opioids (ex. NSAIDS, paracetamol) to weak opioids (ex. tramadol) to strong opioids (ex. morphine, fentanyl) in a stepwise fashion. Given the seriousness of the current opioid crisis in the U.S., this made me wonder about how opioids and other drugs were regulated in India. According to one of the attendings, the Indian Narcotics Bureau designates only certain hospitals as being able to prescribe strong opioids. And within each institution, only Registered Medical Practitioners (RMPs) who have received special training/certification can prescribe opioid medications. Kerala has the most opioid-dispensing institutions (~100-150), with North India having significantly fewer (only a few dozen, according to Dr. T). Bangalore has eight, of which St. John’s is one. There is an interesting tension between wanting to minimize patient exposure to the risk of narcotic dependence on the one hand whilst also striving to ensure that patients have appropriate access to pain meds on the other. A few patients we saw had actually come to St. John’s from out-of-state because they couldn’t otherwise obtain prescriptions for oral morphine 2 to manage their chronic pain 3.
Complicating things further, Dr. T also noted that titrating pain meds was sometimes frustrating because many of the pharma companies that produce generic meds aren’t strictly regulated and have questionable quality assurance. As a result, you can’t always be certain whether a particular drug/pill contains the full listed dose. Thus, if a patient doesn’t respond to a particular dosage/regimen, it’s often unclear whether it’s due to lack of efficacy or whether the pill the patient was given simply doesn’t contain the proper dose. One patient who was given tramadol in its generic form continued to complain of persistent pain; instead of upping the dose, Dr. T decided to try switching to a brand name formulation, and the patient’s pain immediately came down. Referring to some of the generic formulations of commonly prescribed oral pain meds, Dr. T wryly mused, “Is it chalk powder? It could be chalk powder. We don’t know.” On top of all this, the Indian government actively applies pressure on MDs to prescribe generics as a cost-saving measure, to the consternation of doctors, who argue that they cannot possibly provide optimum care if they can’t even be sure of the contents of the generics they are pressured to prescribe.
This got me wondering about how generics were regulated in the U.S., given that many of the generic meds that we prescribe and use are manufactured and sourced abroad in places like India. How does the U.S. ensure that our own markets aren’t flooded with questionable generics? I did some quick digging, and it seems that in order for foreign manufacturers to export their product to the U.S., they have to pass muster with the FDA’s Drug Quality Sampling and Testing Program 4. According to Consumer Reports: “...inspectors from the U.S. and India have ramped up efforts to make sure that plants in India making the drugs exported to the U.S. adhere to the strict manufacturing standards and regulations required by the FDA” 5. As much as we love to collectively complain about inefficient government bureaucracy, these revelations have made me grateful that we have institutions in place to ensure the public interest, as a check on rapacious private commercial practices.
Maybe the biggest takeaway from this rotation was how starkly it underscored inequalities in healthcare access. Unless a patient is very wealthy, healthcare (and esp. care for terminal illness) is often financially ruinous. Every citizen has access to free care at government hospitals, of course, but the general consensus is that these public facilities are under-resourced, under-staffed, and sub-par in terms of care quality. Many patients who can afford to do so therefore seek care at private facilities like St. John’s, where they pay out-of-pocket for every service rendered. Services can be abruptly halted if bills aren’t promptly paid. One patient with Stage III cervical cancer had her chemo and IV pain meds discontinued because of unpaid bills totalling 80,000 Rs. The mother of the aforementioned boy with metastatic Wilm’s tumor had apparently sold land and taken out loans to fund the treatment of her son, only to find out that the tumor was incurable. How she will manage financially after her son passes is unclear. In a market-based, for-profit system like India’s, are there ways to ensure greater healthcare equity and to make access less dependent on individual or familial wealth? 6
++++++++++++++++
[1] See: http://www.stjohns.in/Departments/Palliative%20Medicine/Overview ↩︎
[2] An interesting factoid: oral morphine is ridiculously cheap here – only ~1-2 Rs per pill! ↩︎
[3] Although the question of whether and to what extent opioids should be used to manage chronic pain in the first place is a contentious one. ↩︎
[4] See: https://www.fda.gov/Drugs/ScienceResearch/ucm407277.htm ↩︎
[5] See: https://www.consumerreports.org/cro/news/2014/04/are-generic-drugs-made-in-india-safe/index.htm ↩︎
[6] As with healthcare in the U.S., the problems and their solutions are, in part, a function of politics and political will. India spends less than 2% of its GDP on healthcare, and there is no robust system of health insurance to ensure high quality healthcare for all of its citizens. Certainly greater public sector investment in healthcare could be part of the solution. ↩︎
0 notes
Text
New Delhi & Agra
We took a four-day weekend excursion to New Delhi and Agra! Highlights include: the Taj Mahal, the Agra Fort, the National Museum of Delhi, Parliament, Humayun’s Tomb, and the Raj Ghat (Gandhi’s cremation site). Of note: the temperature in Agra on the day we visited hit 108 degree F, with a humidity of 47%. According to the below heat index chart, that is the equivalent of an apparent temperature > 130 degree F. I ended up getting a pretty severe case of heat exhaustion/heat illness, despite my best efforts to stay cool and hydrated, confirming beyond any doubt that I am just not made for hot weather...

On a happier note, the Taj Mahal (the primary reason for our trip) was well worth it. It was something that we were all a little afraid might not live up to the hype, but it absolutely did and then some. Truly awe-inspiring.



Nataraja, the Lord of Dance:


Scenes from Buddha’s life:

My favorite exhibition at the Delhi museum -- the paintings:

The figure on horseback depicted with the greenish-blue halo is the Mughal ruler Shah Jahan (of Taj Mahal fame). This scene depicts a wedding procession for his son.

































+++++++++++++++++++++++
1 note
·
View note
Text
A Walk in the Park
A short while back, my classmate and I took a trip to see the Tipu Sultan’s summer palace and Cubbon Park, both located roughly in the center of Bangalore. Cubbon Park – known as the ‘lung’ of the city – is an oasis of green replete with winding trails, bamboo thickets, playground space, grassy expanses, and trees tall and dense enough to temporarily muffle the sounds of the surrounding city 1. Unfortunately, getting to the park entailed navigating traffic-congested highways and roads for extended stretches, cutting through a densely-packed commercial district, and being subjected to a constant bombardment of both air and noise pollution 2. Experiencing the tranquility of a quiet stroll through the park was an occasion for me to think about the costs of development, the importance of green space/vegetation for public health, and to draw parallels to my own concrete metropolis of NYC.

One of Bangalore’s nicknames is the “Garden City” due to its reputation for having an abundance of greenery and tree cover. Several Bangaloreans I’ve spoken to, however, have remarked that this term is now a gross misnomer, as hyper-rapid development and land use changes over the past few decades have drastically reduced the amount of vegetation and public green space in the city. Our local neighborhood of Koramangala is fortunate to have relatively bountiful tree cover, but it isn’t too hard to imagine that much of it has been sacrificed to accommodate a ballooning population and growing economy.

Article 39 of the Indian Constitution directs the State to “ensure that...the material resources of the community are so distributed as to best subserve the common good” 3. Surely, parks and public green space ought to be included in the inventory of material resources that subserve this public good. One could argue, however, that economic growth and development are also good for Bangalore. How to strike an appropriate balance?

Eminent domain laws in India allow the State to expropriate private land (much of it formerly agrarian) for ‘public purpose.’ Some scholars 4 complain, however, that loopholes in the law have enabled the State to sell off this land to private commercial interests for the purposes of development. (I imagine that these types of sales have helped catalyze the IT industry/tech boom in Bangalore) 5. The end result: land that was intended to serve as a public resource – a commons for the people – is transformed into a commodity for the profit of private industry. Some may benefit enormously from these land use changes (India’s educated IT professionals, for instance). Others, not so much 6.
To get a sense of what has been lost, I dug up this map from a study conducted by the Indian Institute of Science 7, showing the drastic changes in Bangalore’s land-use over time:
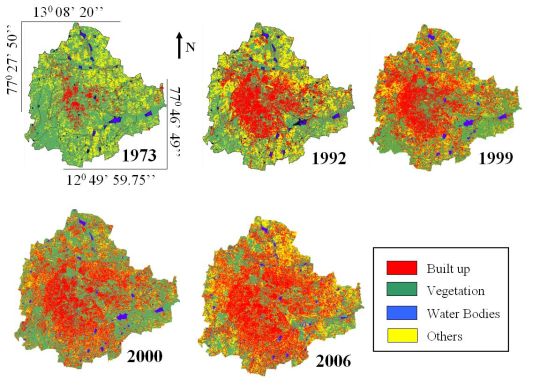
Other public resources that rightly belong to the commons but have been sacrificed in the era of rapid urban development are clean water (which I discussed in a previous post on the so-called ‘water mafia’ and which is quantified in the graph 7 below) and clean air.

As reservoirs have been drained to accommodate developmental build-up, clean water – like green space – has become commodified and sold at markup to those who can afford it. Below is an example of a private tanker truck supplying water to a restaurant near St. Johns, which I suspect is being done without any oversight from a central authority.

But what about clean air? That is every person’s birthright and can’t possibly be expropriated and commodified, right? Well peep this Fortune article from 2016, which I originally thought was an Onion article: Smog in China and India Have Given Birth to a New Industry: Bottled Air.
“In May, a Canadian company that claims to sell “100% Pure Rocky Mountain Air” announced that it would start distributing its product in twin packs of 3 and 8-liter bottles to the Indian market, for around $20 and $40 respectively.”
Writer and cultural critic Matthew Crawford has argued that even our very sense of mental peace and calm – relatively abundant, coincidentally, in places like parks – are things that we increasingly have to pay for. He uses the example of airports: the wealthy pay for the privilege of enjoying the quietude and privacy of the business-class lounge, while the rest of us are forced to contend with the noise and the constant stimulation of the airport proper 8. Another example: in the hospital, if you want the privacy and quiet of your own room, it will come at a steep price – a situation that has many parallels to ‘VIP suites’ in American hospitals.
One of the attendings I met during my first week in Bangalore described the city colorfully as a ‘sensory assault.’ Public parks like Cubbon are great because they are reservoirs of peace and tranquility – respites from the daily sensory onslaught that everyone ought to be able to enjoy (for free!). Whilst walking through Cubbon, I was reminded of how lucky I was to grow up across the street from a park and playground in NYC and how fortunate I’ll be to be steps away from Central Park during my residency. I was so glad to learn, via Wikipedia, that “the roads around [Cubbon Park] are closed for traffic from 5:00 to 8:00 am every day to provide more safety and fresh environment for morning walkers and exercisers” 9. Finally, a victory for Bangalore’s pedestrians (who I feel are generally shafted in favor of drivers/cars...)!
One last note about the environmental consequences of destroying urban green space – it tends to make a city hotter. Check out the below map 10 of NYC, showing a pretty direct correlation between areas of denser vegetation and lower average temperatures. Some life-long Bangaloreans I’ve chatted with have noted wistfully that when they were kids, the temperatures in the city were significantly cooler, to the point where they would need to put on a sweater in the morning to stave off the a.m. chill. Those days, it seems, are long gone.

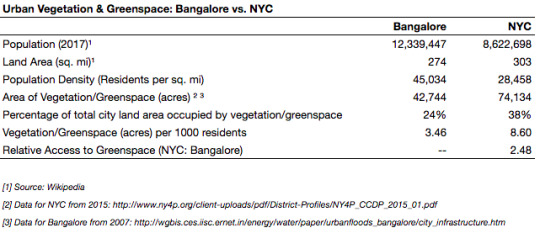
To place things in perspective, here is a comparison of green space/vegetation in Bangalore vs. NYC:
Speculating on why preservation of public resources/the commons has been under-prioritized as a political issue, Dr. Koshy noted – quite provocatively, I thought – that “Indians… do not understand the nature of societal or social responsibility which is not just taking care of yourself and your family…We have to put the cart before the horse. This means enough water, food, shelter, clothing, education, jobs, power, transport, etc., for everyone, not just for some” 4 11. I thought his assessment of the Indian public was perhaps a bit harsh, and didn’t adequately account for the sometimes difficult tradeoffs between acquiring things like ‘jobs’ and ‘power’ (often attained via economic growth) and securing resources like water (often achieved via responsible environmental stewardship and conservation). His sentiment did, however, seem to be consistent with the overall spirit of Article 39, which defends a sense of collective responsibility and collective destiny in India.
+++++++++++
[1] St. John’s is a similar oasis, as I’ve mentioned previously. ↩︎
[2] This of course exists in NYC too, to a lesser degree. ↩︎
[3] See: https://indiankanoon.org/doc/555882/ ↩︎
[4] From: Wake Up, India! Essays For Our Times by Dr. Koshy A.V. and Dr. Bina Biswas ↩︎ ↩︎
[5] See: https://www.commonfloor.com/guide/no-letting-out-land-to-industries-kiadbs-latest-move-31494.html ↩︎
[6] The loss of vegetation/green space – and the environmental degradation that it signifies – can thus be considered an externality whose costs are borne collectively by Bangalore’s citizens. ↩︎
[7] See: http://wgbis.ces.iisc.ernet.in/energy/water/paper/urbanfloods_bangalore/city_infrastructure.htm ↩︎ ↩︎
[8] See: https://www.nytimes.com/2015/03/08/opinion/sunday/the-cost-of-paying-attention.html ↩︎
[9] See: https://en.wikipedia.org/wiki/Cubbon_Park ↩︎
[10] From: https://earthobservatory.nasa.gov/IOTD/view.php?id=6800 ↩︎
[11] I have heard similar accusations levied against China in its own parallel quest for rapid economic development vis-a-vis unfettered capitalist investment/growth. ↩︎
1 note
·
View note
Text
Dermatology Rotation
“Leprosy work is not merely medical relief but it is transforming the frustration of life into joy of dedication and personal ambition into selfless services.” - Mahatma Gandhi
+++++++++++
Week 3 was spent rotating through the Dermatology department, which is primarily an outpatient service. Much of the pathology I saw was similar to what might be encountered back at Downstate, for instance: psoriasis, urticaria, dermatophytosis, acanthosis nigricans, warts, paronychia, rosacea, scabies, and vitiligo. But one of the main reasons I wanted to spend a week in Derm was the opportunity to see and learn about leprosy (aka Hansen’s disease), an infectious disease affecting the skin and peripheral nerves. India accounts for approx. 60% of the global burden of leprosy, with over 120,000 new cases per year 1. A significant percentage of cases stem from the northeastern and central regions of the country.


Caused by the bacterium Mycobacterium leprae, it’s a disease that’s been historically misunderstood and unfairly stigmatized. Europeans up through the colonial period believed it to be a moral scourge as much as a physical ailment – a result of both sin and squalor. These attitudes led to the enactment of colonial laws mandating the banishment of leprosy-affected patients into segregated colonies/asylums. These laws also sanctioned other forms of discrimination against leprosy patients. For instance, the 1898 Lepers Act in India 2 – introduced during British colonial rule – barred such patients from holding certain jobs and gave police officers the right to arrest them without a warrant. The law wasn’t officially repealed until 2016. And though officially off the books, the legacy of these discriminatory attitudes is still felt in present-day India, where stigma is a significant barrier that hinders patients from seeking treatment 3. The great irony is that although these laws were enacted (presumably) to secure the public health, leprosy is not known to be highly contagious and, in fact, most individuals do not develop the disease following exposure 4.
Given that cases of leprosy are likely underreported as a result of stigma and suboptimal care-seeking, the Indian government launched the Leprosy Case Detection Campaign in 2016 – an initiative that mobilized almost 300,000 ASHA community health workers in a door-to-door effort to detect unreported cases of leprosy. A total of 320 million Indians were screened in this campaign, which I thought was an utterly remarkable public health feat 5!
I ended up seeing one patient with leprosy during my Derm week. The patient was a 47 y/o farmer who presented with multiple hypopigmented patches all over his body. He also exhibited ear thickening, ulnar nerve hypertrophy, and cranial neuropathy (the patient had signs of facial droop and nasolabial flattening, similar to a Bell’s palsy presentation). He did not, however, have the characteristic ‘leonine facies’ that you see in textbooks.
Characteristic facial lesions of advanced leprosy 6:

Nerve damage resulting in poorly-healed wounds/lesions/deformities in the hands and feet _6: _

It was interesting to palpate the patient’s ulnar nerve and note its increased size. (I had to ask the St. John’s med students to show me how to do this). The attending mentioned that palpation of an enlarged ulnar nerve is actually quite sensitive for the detection of leprosy. I did some digging afterwards, and according to one study 7 of 357 patients with untreated multibacillary leprosy, sensitivity of nerve palpation for the detection of leprosy was as high as 88% (although specificity was significantly lower). As with pulmonary TB, prolonged treatment (up to or exceeding 12 months) with a multi-drug regimen (dapsone + rifampin + clofazamine) can make adherence difficult.
Other barriers stymying the eradication of leprosy include: lack of expertise amongst primary care providers in identifying and treating leprosy; the absence of a robust referral network to link patients to specialist care; and a lack of access to dermatologists. Also, per the Kumar editorial cited earlier: “Over the last few years involvement of dermatologists in vertical programme has diminished in India and moreover, dermatologists are also now more focused towards lucrative branches of dermatology” 1. I suppose it’s not so different from the U.S., where market incentives compete with public health priorities to drive overall practice patterns.
+++++++++++
[1] Kumar, B. (2015). "World Leprosy Day 2015: renewing commitment for a leprosy free world!" Indian J Med Res 141(1): 1-4. ↩︎ ↩︎
[2] See: http://www.rfhha.org/images/pdf/Hospital_Laws/Lepers_%20act_1898.pdf ↩︎
[3] See: https://www.leprosymission.org.uk/news-and-resources/news/indias-repeal-of-1898-lepers-act-is-positive-step/ ↩︎
[4] Source: UpToDate ↩︎
[5] See: http://www.who.int/neglected_diseases/news/India_massive_leprosy_case_detection_campaign_reaches_320_mill/en/ ↩︎
[6] Illustrations taken from: The Sick Rose: Disease and the Art of Medical Illustration by Richard Barnett. ↩︎ ↩︎
[7] Khambati, F. A., et al. (2009). "Sensitivity and specificity of nerve palpation, monofilament testing and voluntary muscle testing in detecting peripheral nerve abnormality, using nerve conduction studies as gold standard; a study in 357 patients." Lepr Rev 80(1): 34-50. ↩︎
1 note
·
View note
Text
Shravanabelagola/Belur/Halebid
Our next weekend day-trip took us to the towns of Shravanabelagola and Belur/Halebid – approx. 3.5 hours and 4.5 hours west of Bangalore by bus, respectively (Belur and Halebid are neighboring towns only ~10 miles apart).
+++++++++++
Shravanabelagola is home to Vindhyagiri Hill, at the summit of which sits a Jain temple with a majestic, 57-foot monolithic statue of the god Bahubali, built circa 983 AD. According to Jain texts, Bahubali is said to have meditated motionless for an entire year in a standing position; after his year of meditation he was able to attain omniscience/enlightenment. It’s probably one of the coolest, most impressive sculptures I’ve ever seen – the power and grandeur conveyed by the scale of the statue somehow in perfect consonance with the quiet serenity expressed in Bahubali’s face and posture. Per Wikipedia 1:
“The statue depicts the prolonged meditation of Bahubali. The motionless contemplation in kayotsarga (standing still) posture led to the growth of climbing vines around his legs. The image...has curly hair ringlets and large ears. The eyes are open as if he is viewing the world with detachment. His facial features are perfectly chiselled with a faint touch of a smile at the corner of the lips that embody a calm inner peace and vitality.”







Every twelve years, the Mahamastakabhisheka festival takes place, in which priests and worshippers climb atop the scaffolding around the statue to anoint it with milk, sugarcane juice, saffron paste, sandalwood, turmeric, and vermilion. The last festival took place in February 2018, but we got to witness (what I assume to be) a smaller version of it during our brief visit.



+++++++++++
Belur/Halebid were sites of two temples – Chennakeshava Temple (Belur) and Hoysaleswara Temple (Halebid), dedicated to the Hindu gods Vishnu and Shiva, respectively.








Of the two, the Hoysaleswara temple was slightly more impressive, containing stonework of mindboggingly intricate complexity. The temple artwork mainly consisted of detailed friezes/reliefs that depicted, in stunning detail, scenes from both daily life and Hindu mythology. These friezes are organized in bands on the outer wall of the temple. Wikipedia 2 has a very helpful diagram explaining what each band depicts/represents:






Two lovers stealing a kiss?

The bull Nandi, the vahana, or "vehicle" of Lord Shiva:

Well that looks unpleasant...


+++++++++++
[1] See: https://en.wikipedia.org/wiki/Gommateshwara_statue ↩︎
[2] See: https://en.wikipedia.org/wiki/Hoysaleswara_Temple ↩︎
1 note
·
View note
Text
History of Medicine Museum
Tucked away in a corner of the St. John’s Research Institute is a delightful museum dedicated to the history of medicine (officially, the S. L. Bhatia History of Medicine Museum). Recommended to me by one of the Community Health residents, the museum contains two floors of exhibitions covering the history of both Indian and general allopathic medicine, as well as a medical humanities library. Super cool that a medical school has this type of museum space (which you seldom see in the U.S.)! The museum featured old medical equipment/tools, 19th century medical texts, and other quirky ephemera. It’s quickly become my favorite place on campus.

An old device for performing nerve conduction studies:

Old-school spirometer:

Apparatus for assessing ABGs:

An alembic (device for distilling medicines).

Women pioneers:




Prognosis for TB meningitis in the late 19th/early 20th C.

Outdated thoughts on the etiology of epilepsy:

Curare -- a treatment for tetanus that we still use!

Old remedies for sore throat:


1 note
·
View note
Text
Neurology Rotation
My second week at St. John’s was spent rotating through the Neurology department. The patient cases were interesting and included a variety of pathology, some which I had never seen before (ex. neurocysticercosis; neuromyotonia 1 ) but many which were at least familiar (ex. myasthenia gravis; autoimmune/paraneoplastic encephalopathy; epilepsy; stroke; (possible) ALS).


But the most interesting aspect of the rotation, however, was witnessing how thoroughly the principle of paternalism suffused medical practice on the wards. Our attending – though warm and congenial towards his patients – nevertheless tended to rush through explanations, announce treatment plans without any patient input 2, and was generally unavailable to have more than a cursory discussion with family members. In one memorable exchange, he offered this terse ultimatum to a patient’s family after they had expressed some concern regarding the treatment plan: “You listen to me, or you go.”
Most of the other patients/families we saw adopted a more deferential attitude, whereby they treated the doctors with unquestioned reverence. This particular family, though, seemed to be wealthier, more educated, and thus (I assume) more emboldened to interrogate physician authority. Indeed, our attending actually joked that a patient’s level of education is inversely proportional to physician happiness: more education means more demands for explanations 3, which ultimately places constraints on both the physician’s massive authority and limited time.
To be fair, I think this approach was partly attributable to patient volume rather than physician callousness: it was a busy service, and there simply wasn’t time to sit down and address every single question/concern. In this setting, paternalism seemed like the more efficient option. In discussing with my classmates, we also speculated on the extent to which Indian cultural norms and generational differences were at play.
We learn in medical school that paternalism is bad and that the ideal practice paradigm is a deliberative-interpretative strategy that splits the difference between the patronization of paternalism and the hands-off approach of the informative model 4.

As doctors, we are granted the right and authority to wield the tools of our profession as we see fit, only to have that power constrained by a healthcare model that (rightly) holds patient autonomy and shared decision-making 5 to be sacrosanct. How do we respect a patient’s agency, decision-making capacity, and fundamental values whilst retaining the freedom to practice in ways that we deem to be most appropriate for the patient’s and the public’s welfare 6? How are we to respond when those imperatives conflict with one another?
Our hand-wringing over paternalism is not, then, merely a function of a generational or cultural disconnect. It may instead be emblematic of a more universal frustration about physician power and our (in)abilty to exercise it. We chose to become doctors, after all, in order to act – to be able to do things that we consider medically appropriate and even life-saving. To have agency, in other words. But we sometimes forget that it is not our agency that is paramount, but the patient’s 7. And that though a patient’s demands may be unreasonable, the values that inform those demands aren’t.
I recently finished reading Paul Kalanathi’s memoir When Breath Becomes Air, in which he describes feeling a profound loss of agency as he transitioned from the role of doctor to the role of cancer patient – from one who acts to one who is acted upon 8. None other than Osler himself warned that we mustn’t get so caught up in our own hubris – in our paternalistic certainty that we know how best to act – that we forget that other cherished value of our profession – humility:
“The Art of Detachment, the Virtue of Method, and the Quality of Thoroughness may make you...successful practitioners…, but your character may still lack that which can alone give permanence to powers – the grace of Humility.” – William Osler, Aequanimitas

[1] Neuromyotonia = peripheral nerve hyperexcitability causing spontaneous muscular activity. See: https://youtu.be/-ovFTl77N50?t=50s. Note the ‘bag of worms’ appearance of the fasciculations in the calf muscle – this is exactly what it looked like in the patient we saw. ↩︎
[2] The junior residents were reduced to the role of glorified secretaries who took down and subsequently executed the attending’s orders, without much discussion or teaching. ↩︎
[3] Isn’t this just accountability?? ↩︎
[4] The ‘Emanuel & Emanuel’ model. See: Ezekiel J. Emanuel and Linda L. Emanuel. "Four Models of the Physician-Patient Relationship." JAMA 267:2221-6, 1992. ↩︎
[5] Not to mention cost-containment... ↩︎
[6] Some researchers have advocated for a dynamic model of physician-patient interaction (rather than a ‘one-size-fits-all’ approach) that varies according to each individual patient’s extent of medical knowledge; health-related values; and degree of autonomy. See: Agarwal, A. K. and B. B. Murinson (2012). "New Dimensions in Patient–Physician Interaction: Values, Autonomy, and Medical Information in the Patient-Centered Clinical Encounter." Rambam Maimonides Medical Journal 3(3): e0017. ↩︎
[7] Even when we believe their choices and demands to be inconvenient and foolhardy. ↩︎
[8] Indeed, Kalanathi explains the etymological roots of the word ‘patient’ as meaning, in part, ‘the object of an action.’ ↩︎
1 note
·
View note
Text
Mysore
The Downstate crew took a weekend day-trip to Mysore (aka Mysuru) – a city in Karnataka about 90 mi. southwest of Bangalore. Took a train there and a bus on the way back. Highlights included: hiking up 1,008 steps to the top of Chamundi Hill to see the Chamundeshwari Temple 1; statue of the bull Nandi 2; panoramic views of the city at the hill’s summit; statue of the demon Mahishasura 3; south Indian thali for lunch; mischievous monkeys; and a VIP tour of the Mysore palace 4.




















[1] This was physically challenging in a way that my out-of-shape body had not anticipated. ↩︎
[2] The vahana, or "vehicle" of Lord Shiva. ↩︎
[3] According to Hindu legend, the Buffalo Demon Mahishasura had terrified the local population of Mysore, until he was eventually killed by the goddess Chamundi – an event that is annually commemorated/celebrated in Mysore. See: https://en.wikipedia.org/wiki/Mahishasura. ↩︎
[4] Since Robin, our injured compatriot, was in a wheelchair, we were actually assigned an attendant who personally led us around and gave us an explanatory tour of the palace. ↩︎
1 note
·
View note
Text
Community Health Rotation
I spent my first week doing a rotation in the Dept. of Community Health – a primary care specialty that is probably most analogous to Family Medicine in the US. There is a heavy emphasis in the department on patient outreach and preventative/public health. Public health and population-level outcomes are departmental priorities, and there (refreshingly) seemed to be less of a disciplinary/epistemological separation between clinical medicine on the one hand and public health on the other (compared with the US). Both urban and rural health were emphasized. We spent the week at either: (1) an urban health center on the outskirts of a slum called Austin Town about a 20 min drive south of St. John’s or (2) a rural health center in the village of Mugalur, about a 1 hour drive east of St. John’s.
++++++++
On the morning of day one, we (i.e. Dr. J, a St. John’s 2nd year post-grad 1, a Downstate classmate, and I) took an autorickshaw to Austin Town.

After checking in at the urban health center (the Arogya Raksha Yojana or ‘ARY’ clinic) 2, we ventured out to the anganwadi 3 in the heart of the Austin Town slum. Anganwadi roughly translates to "courtyard shelter." They are government-funded child care centers for children up to age 5. They provide rudimentary healthcare services, meals, and informal education to local under-5 children, under the supervision of one or two anganwadi workers (akin to pre-school teachers). There are approx. 13.3 million anganwadis in operation in India. The anganwadi we visited was a one-room windowless structure, quite small (approx. 12’ x 12’), serving 11 children. We were told that most of the children were migrants from Tamil Nadu and thus spoke Tamil rather than Kannada. Our role for the day was to help Dr. J take measurements of the children’s height, weight, and mid-arm circumference and then plot the results on WHO growth charts to screen for malnutrition/underweight/growth stunting. Several of the children were mildly underweight, one had significant stunting, and the rest were more-or-less normal.



We also saw a child with a cleft palate + repaired cleft lip of indeterminate age. One of the attendings later told us that if the cleft palate doesn’t affect feeding, parents may opt to only have the cleft lip repaired, for both cost and cosmetic 4 reasons. Dr. J examined and wrote notes for all of the patients, with plans to refer the children with pressing issues to the ARY clinic. Milk fortified with protein powder was one of the therapies for malnutrition/stunting +/- albendazole tablets to ensure that helminth infection was not a cause of malnourishment.


One thing I was curious about was whether the WHO growth charts were adjusted for a country’s relative level of wealth/development. I figured they must be – the charts represent the normal distributions of the heights & weights of the population’s healthy children, and these distributions would be vastly different for the children of developing countries vs. developed ones. But I was wrong! Apparently the WHO pooled data from six countries (Brazil, Ghana, India, Norway, Oman, and the US) to produce an international standard, stating that, “children born anywhere in the world and given the optimum start in life have the potential to develop to within the same range of height and weight. Naturally there are individual differences among children, but across large populations, regionally and globally, the average growth is remarkably similar. For example, children from India, Norway and Brazil all show similar growth patterns when provided healthy growth conditions in early life.” 5 These ‘healthy growth conditions’ include: “recommended infant and young child feeding practices 6, good healthcare, mothers who did not smoke, and other factors associated with good health outcomes.” Thus, the WHO growth standards are essentially a normative formulation of what healthy growth from birth to age 5 ought to look like (ex. breastfeeding, moms who abstain from smoking, etc.). 7
++++++++
The following three days were spent at the rural health center in Mugalur village, which was fully staffed and run by St. John’s clinicians. The trip to Mugalur took about an hour by van, and it was nice to transition from the congested traffic of urban Bangalore to the lush greenery of the agrarian countryside.

Post-grads interested in going into Community Health spend 6 months of their PGY2 year living in Mugalur and overseeing the daily clinics. Each day was dedicated to a different subspecialty clinic (ex. maternal/child health, NCD clinic, psychiatry (‘Manasi clinic’), geriatric clinic). Patients were drawn from the surrounding villages. I learned that patients paid user fees for lab services 8, medications, and procedures (including minor surgery), but that St. John’s provided them at discounted cost (ex. ~1500 Rs for cataract surgery; 25% subsidy for medications).

On the first day, we were driven to a smaller neighboring village close to Mugalur called Madapanahalli. There, the post-grads/residents ran the day’s geriatric clinic in a makeshift space just outside the village temple. The village homes were small, colorfully painted, and surrounded by acres and acres of lush farmland. We were joined by one of the ASHA workers (i.e. community health workers) whose job it was to regularly visit patients at their homes to ensure that they showed up on clinic day and to remind them to take their meds. The post-grads carried around a large metal box that essentially served as a portable pharmacy – packed with common, mostly generic medications for chronic conditions like HTN, DM, anemia (ex. ACEi, ARBs, calcium channel blockers, metformin, pain meds, a few antibiotics, iron tablets, multivitamins).






We saw a few patients at the temple and also made a few home visits, where we observed the post-grads performing basic H&Ps on the patients. Not speaking the language, I simply sat and watched politely whilst awkwardly munching on a Yelakki banana (i.e. baby banana) that I was offered. One patient had a surprisingly modern and ornate home near the village center, which I later learned from the residents was likely purchased with money secured from selling their land. As a result, the wealthier villagers all had nice homes, but ultimately possessed a diminished capacity to generate new revenue/wealth. The post-grads mused that these villagers’ children/grandchildren likely moved away from the village and into urban Bangalore to look for work – part of the accelerating urbanization of the region, I suppose.
On our walk around the village we were also shown the large, government-maintained water tank that supplies filtered potable water for the entire village. It was essentially a ‘water ATM’ in which villagers would insert 1 Rs to get ~20L of water.

We also got to visit a Grama Hiriyara Kendra (GHK) Program – essentially a senior citizen center established by St. John’s that serves the village’s over-60 population 9.


It was a moderate-sized, one-room structure in which about 12 women 10 gathered to receive basic health education, engage in physical activity, have meals/milk/tea, and enjoy one another’s company. I was served a cup of cold buttermilk with cilantro & spices as the ladies stared bemusedly at their pale-faced visitors. We were told that the concept of a senior center was not widespread in India, and that the GHK Program was, in part, intended to be a pilot initiative to demonstrate to the government the value of having senior-centered programming to bolster the physical and psycho-emotional well-being of India’s elderly 11.

++++++++
For the Maternal/Child Health (MCH) Clinic, we started our day by making a pit stop at a regional Primary Health Center (PHC) en route to Mugalur to pick up vaccines. The vaccines (incl. IPV, OPV, measles, rubella, a few others) were kept refrigerated at the government-run PHC and were re-stocked by the government approx. monthly. The St. John’s crew would come pick them up and temporarily store them in plastic coolers for the trip to Mugular.



The maintenance of the vaccine cold chain is an interesting logistical challenge. I brought up the operational model of Project Last Mile, which seeks to leverage the distribution and cold-chain apparatus of Coca-Cola to deliver medicines and vaccines to the farthest reaches of the globe 12. Dr. N, one of the attendings, responded by discussing the benefits of engaging the private sector, but also the drawbacks (ex. giving Coke a veneer of do-gooderism so that they can sell more soda, eventually necessitating the use of their cold chain to deliver insulin to the world’s latent diabetics...).


Indian physicians follow the WHO vaccination schedule, with a few adjustments for the local context (ex. BCG vaccine for childhood TB). Unlike us, they don’t routinely vaccinate against mumps or VZV. Dr. N explained that the incidence of those infections simply wasn’t high enough to warrant inclusion in the routine immunization schedule, and that a cost-benefit consideration factored into the decision. Another example of how a public-health orientation informed decision-making. Also reminded me of this recent NYT article about how challenging it is for individual US physicians to engage in a similar cost-benefit calculus when deciding on treatment options for their own patients. As a provider, do you decide to forgo an expensive (but marginally more effective) treatment in order to decrease overall costs? Important to consider, given how crucial cost containment is in the US.
++++++++
The last days of the rotation were spent in the NCD and Manasi (i.e. psychiatry) clinics. It seemed that many of the diabetic patients had never before seen a physician before coming to the NCD clinic. Thus, the initiation of treatment with a simple regimen of metformin + a low-dose sulfonylurea (in addition to counseling re: diet & exercise) turned out to be extremely high yield. Many of the patients saw a dramatic decrease in their random glucose (300s –> 100s) within a few months of therapy initiation, which must have been extremely gratifying for the docs. Most of the patients seen at Manasi clinic had mixed psychiatric and neurological complaints, including epilepsy and headache. The most common psych disorders were depression and anxiety.
Finally, on our last day, the Mugalur clinic hosted a group from the Indian Institute of Science (IISc) 13. This group seemed to be marketing a new augmented reality ultrasound technology for use in low-resource settings. In the course of their discussion, I learned that transcranial ultrasound could be used to measure the degree of midline shift in the setting of intracranial mass effect, with good correlation to the measurements obtained from head CT. Really neat, especially in settings where head CT is not readily available! Did some more digging and stumbled on this paper 14, which described the theory and technique in patients with space-occupying stroke.

[1] Akin to a PGY-2 in the US. ↩︎
[2] The urban health center is jointly funded by St. John’s (who provides the clinicians) and by Biocon (who provides generic medications at discounted cost). Biocon is the largest biopharma company in India. Interestingly, it began as a two-person operation in the 1970s with 150 USD in startup capital, before growing into the pharma behemoth it is today. ↩︎
[3] See: https://en.wikipedia.org/wiki/Anganwadi. ↩︎
[4] This is especially true for the girls, as their parents will be concerned about their marriageability. ↩︎
[5] See: http://www.who.int/mediacentre/news/releases/2006/pr21/en/ ↩︎
[6] i.e. breastfeeding ↩︎
[7] I then wondered whether this universal formulation could serve as a proxy indicator for class/SES since, for instance, poor mothers may have decreased capacity to regularly breastfeed their children and, in general, are less able to provide the optimal environment for growth as outlined by the WHO. In other words, screening for stunted growth in children is tantamount to screening for extreme poverty. ↩︎
[8] Contracted out to a private company. ↩︎
[9] See: http://www.stjohns.in/Special_services/SeniorCitizensProgramme ↩︎
[10] Apparently, there were initially men involved in the program, but we were told by the senior post-grad that they all eventually opted out because they felt uncomfortable with the high female:male ratio, perhaps suggesting (at least amongst the older generations) the novelty of gender-integrated social activities. ↩︎
[11] Reminds me of something Atul Gawande said in Being Mortal: that as formerly agrarian societies modernize, the task of taking care of the elderly becomes socialized – that is, the duty shifts from being the private responsibility of an elderly person’s family to the public responsibility of the government/state. ↩︎
[12] See: http://www.coca-colacompany.com/stories/projectlastmile ↩︎
[13] Part of a group attempting to research and manufacture affordable medical devices. ↩︎
[14] You’re essentially measuring the degree of lateral shift of the third ventricle. See: Stolz, E., et al. (1999). "Comparison of transcranial color-coded duplex sonography and cranial CT measurements for determining third ventricle midline shift in space-occupying stroke." AJNR Am J Neuroradiol 20(8): 1567-1571. ↩︎
1 note
·
View note
Text
Coffee?
Mildly surprised and super impressed at the number of good third-wave coffee places in Koramangala. :) A lot of the coffee I’ve had here thus far is a coffee/chicory blend. It’s pretty tasty, but it’s nice to know I can also have 100% arabica coffee while here.


1 note
·
View note
Text
St. John’s

St. John’s Medical College was established by the Catholic Church in India in 1963. It’s situated on a beautiful, tree-lined 140 acre campus in the heart of Koramangala – an oasis from the bustling, congested city beyond its walls. It is part of the broader St. John’s academic medical complex that, in addition to the medical school, comprises a teaching hospital, a college of nursing, a research institute, and an institute of ‘Health Management and Para-Medical Studies’ 1 2. The hospital (where I’ll be rotating as a foreign elective student) is a large, private, 1350+ bed tertiary care referral center that, like teaching hospitals back home, professes a tripartite mission of clinical service, academics/teaching, and research. Depending on which source you cite, the Medical College hovers somewhere between 14th and 4th in the rankings of best medical schools in India 3 4.



Robert Koch was the German physician and microbiologist who identified Mycobacterium tuberculosis as the causative agent in TB. (Apparently, TB was previously thought to be inherited) 5.
[1] See: https://en.wikipedia.org/wiki/St._John%27s_Medical_College ↩︎
[2] See: http://www.stjohns.in/About/Overview ↩︎
[3] See: https://www.outlookindia.com/magazine/story/top-25-medical-colleges-in-2017/298918 ↩︎
[4] See: https://www.indiatoday.in/bestcolleges/2017/medical-bestcollege ↩︎
[5] See: https://en.wikipedia.org/wiki/Robert_Koch ↩︎
1 note
·
View note
Text
Let’s Go To The Mall...Today!

Went to check out the Forum Mall in the heart of Koramagala, which I learned was Bangalore’s first full-fledged mall 1. It offered a ton of Western retail shops/brands, as well as a great food court and an 11-screen multiplex on the top floor screening both Hindi and English films.


My mango ice cream from the food court:

There was also a fabulous all-purpose market a few blocks down the road (‘Star Bazaar’), where I picked up an awesome pair of black chinos for ~700 Rs as well as a bunch of household items. My classmate referred to it affectionately as ‘the Kmart of India.’ :D
[1] See: https://en.wikipedia.org/wiki/The_Forum_(shopping_mall) ↩︎
1 note
·
View note
Text
Water Mafia?

Fascinating and disturbing read: India’s Silicon Valley Is Dying Of Thirst. Your City May Be Next. Apparently, Bangalore’s rapidly expanding population, combined with frequent droughts and a poorly maintained municipal water system have conspired to create a water crisis in the city. To meet the growing demand for clean water, an informal network of private companies owning fleets of tanker trucks have had to travel farther afield and dig deeper bore wells to find and deliver water to Bangalore’s citizens, often upcharging for the water in the process. The men who control the largest of these companies essentially control the water supply of Bangalore and can use this monopoly power to raise prices ever-higher. They are known derisively by Indian public officials as a “water mafia.” This is a Vice article, though, so perhaps a bit sensationalized/alarmist? Here’s another, more optimistic take by the water management authorities in Bangalore: http://bengaluru.citizenmatters.in/bangalore-water-scarcity-solutions-2018-23160.
1 note
·
View note
Text
Tula Kalnnaar Nahi – “You will not understand”

On the flight from Newark to Mumbai (the first leg of my journey), I watched a 2017 Marathi language film called Tula Kalnnaar Nahi, which told the story of a married couple on the brink of divorce who rediscover their love and affection for one another over the course of the film. The title roughly translates into “You will not know/understand.” Though the phrase was referring, of course, to the ups and downs of marriage, I also thought it was an apt summation of my ambivalence about being a foreign interloper in India. How much will I fail to know? What understanding (of India’s health care, of its people) can possibly be established in six weeks?
One of the objectives of my elective, as outlined by SUNY Downstate, is “to have a cross-cultural experience.” 1 My role here is, in part, ethnographic in nature – to observe Indian medical care and to better understand the cultural/social/economic variables that inform how that care is delivered. Sometimes I fear, though, that superficial cross-cultural exchanges of brief duration engender stereotyping, ethnic/cultural essentialization, and misunderstanding rather than true knowledge. There is substantial literature in the US documenting how racial and ethnic stereotyping continue to be persistent problems in American medicine that potentially contribute to population-level disparities in healthcare 2. Which begs the question: is it possible to really ‘know’ another culture (and provide care appropriately) without substantial/lengthy immersion?
[1] Speaking of cross-cultural exchange, one of the other movies I watched on the plane was a 2017 Shah Rukh Khan vehicle called Jab Harry Met Sejal – clearly a reference/homage to the iconic 1989 Billy Crystal/Meg Ryan film When Harry Met Sally. Left me wondering about the extent of cross-pollination between Bolly- and Holly-wood. Unfortunately, SRK’s star power couldn’t save the movie from horendous reviews: https://www.rottentomatoes.com/m/jab_harry_met_sejal/. :P ↩︎
[2] See, for instance: https://journals.lww.com/lww-medicalcare/Abstract/2008/07000/Physician_Implicit_Attitudes_and_Stereotypes_About.6.aspx. Also: http://www.pnas.org/content/113/16/4296.full. ↩︎
1 note
·
View note
Text
Yum!

Best butter chicken + naan I’ve ever had, hands down. :D From a restaurant down the street called Hasini that advertises itself as an Andhra-style restaurant 1. According to some quick Wikipedia research 2, this cuisine is the “spiciest in all of India” due to its generous use of chili. I was certainly sweating up a storm. 😅
[1] A type of South Indian Telugu cuisine native to the Telugu people from the states of Andhra Pradesh and Telangana. ↩︎
[2] See: https://en.wikipedia.org/wiki/Telugu_cuisine ↩︎
1 note
·
View note
Text
Day 1
TL;DR: Uber, AirBnB studio apartment, initial impressions
I was somewhat surprised to see that Uber had such a significant presence at the Bangalore airport. I had intended on taking a local cab company from the airport to my studio in Koramangala (a neighborhood about an hour’s drive south of the airport), until I saw the following article in a copy of the Mumbai Mirror on the plane.

Apparently India has quickly become Uber’s third largest market (behind the US and Latin America), with plans for massive future investments and five-to-tenfold growth in ridership over the next decade. My ride went pretty smoothly despite some minor communication difficulties with the driver.
I’m staying in a decent-sized AirBnB studio off one of the main roads, approximately a 10 minute walk to the St. John’s campus. It has all the creature comforts of home (Wifi, A/C, fridge, hot water) to make living here for the next six weeks relatively stress-free. In general, there are a lot of stately-looking houses in this part of town. Here’s a picture of my room:

And here’s an example of one of one of the houses in the neighborhood:

My room faces the main road, so there is constant noise from traffic and horn-honking 1 at all hours of the day (which I actually don’t mind, as it reminds me of the ambient noise in Brooklyn :)). It’s in an area of town that is densely packed with restaurants, cafes, and shops, thus making grabbing a bite to eat relatively easy. My first meal in India was a traditional English breakfast from a hip restaurant down the street called “The Hole in the Wall,” populated mostly by couples and young people (students?).

There are abundant signs that Bangalore is a hip, “up-and-coming” city but also hard-to-ignore signifiers of poverty and hyper-rapid urbanization (ex. generally poor roads/sidewalks/infrastructure; congested traffic; piles of uncollected trash (which sometimes cows will rummage through and nibble on); non-potable tap water 2).

The weather is definitely muggy, but not too uncomfortable – Bangalore is apparently famous for its (relatively) temperate weather, due to its significant elevation (~3000 ft. above sea level). Temperatures at night dip into a comfortable range in the mid-70s to low-80s F. Some quick internet research 3 quickly revealed, however, that April is Bangalore’s hottest month, with average highs in the mid-90’s F, so we’ll see how long I last before I start complaining about the heat....

:)
[1] One of the first things I noticed was how drivers here utilize their horns nearly constantly to alert other cars, Vespa-riders, and pedestrians that they are nearby and/or intend to pass them. It was a wonder to me how folks didn’t succumb to ‘honking fatigue’ and become desensitized to the sound of car horns (akin to how medical professionals often experience ‘alarm fatigue’ and learn to ignore the constant noises and alerts emanating from patient monitoring devices). ↩︎
[2] This is apparently a huge issue in Bangalore – in large part a function of its hyper-rapid development. More on this later. ↩︎
[3] From: https://en.wikipedia.org/wiki/Bangalore#Climate ↩︎
1 note
·
View note