
Registered nursing student. Louisiana born and raised (live in Florida). I'm an avid reader, and in a fight for my affection: dogs win. My posts are pretty much medically geared, but if something catches my eye, I'll re-blog.
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by anurseinthemaking and here's what we found interesting.
Average Info
Notes Per Post
36K
Likes Per Post
21K
Reblog Per Post
15K
Reply Per Post
18
Time Between Posts
3 months ago
Number of Posts By Type
Text
6
Photo
6
Note
4
Video
1
Last Seen Tumblr Blogs




Fun Fact
In 2020, 27% of US Tumblr users had an annual household income of over $100,000.
Text
I dug up this blog and A LOT has changed. Since graduating and becoming a RN, I’ve specialized in ER/Trauma. Spent a few years in the ER and I’m now a ER travel nurse.
If anyone is still active, feel free to let me know. I may just convert this blog into an general nursing page, if there’s still some interest!
36 notes
·
View notes
Photo

We tried our hardest to study for GI, but our brains are absolute mush. Taking a bit to myself and catching up on “How to Make a Murderer”. Here’s to the insanity that’s Med-Surg!
12 notes
·
View notes
Note
Hi! I'm wondering what your experience has been like with your instructors, if you've had any really strict or unapproachable ones and how you handled it. We go back to school tomorrow and I just got an email from mine; I've heard bad things about her and she literally introduced herself as "a real stickler". Kill me.
First off, do NOT pay into those comments other students have made. You'll end up going into the situation with a preconceived notion about that instructor, and that will on hinder yourself.I haven't experienced an instructor that's been too difficult. I've often found that if you talk with them during their office hours and share your concerns regarding clinicals, they are usually more than happy to give you advice.We're all human, but the reality of it is, as a nursing student, you're operating under their license and it's their responsibility to ensure you practice safely and throughly. Be open with them; tell them your weaknesses, your concerns, your fears: they will find a way to help you out. I promise. It may not be in the fashion we'd prefer, but try and remain open-minded. You've got this! Just remember you're there to learn and that if something is difficult, try and rise to the occasion or if something upsets you, take a moment to breathe, compose yourself, and have another whack at it.
5 notes
·
View notes
Text
I've been away for a bit, so let's do a Q&A!
Want to get to know more about and my adventures in Nursing School (2nd Semester), here's your chance! Ask away! I'd love to hear from you all!

3 notes
·
View notes
Note
hi there, I start nursing school in January and I was wondering if you have any tips. Just anything you would want to tell yourself before you started! I'm Emily btw, nice to meet you!
Hi Emily!You never think a question such as yours would be difficult to answer, but it is; not that I don't like a good challenge!I would say to prepare yourself for a battle. Nursing school isn't easy, nor should it be. You're ultimately training yourself to be responsible for someone else's care. Now, preparing yourself can be enjoying time with friends, brushing up on Pharmacology or Dosage Safety, or sleeping as much as you can. This part comes from what works best for you as a person.I highly recommend building a small circle of individuals in your life that you can use as a support system. Some of these will come from your nursing class. Don't panic. It truly is going to be okay. Enjoy as much of this ride as you can. It's an uphill battle, but it's one you'll enjoy, even if you want to die a little inside.
17 notes
·
View notes
Text
Uh oh, time for an emotional post.
As I write my last Care Plan for my first semester, I cannot help but feel a pang of sadness. I have been a part of this patient's care throughout these past several weeks and I just don't feel like I've done enough. Sure, I've attempted to pair my care with some creative ideas, but it just does not seem like I've done enough to REALLY make that much of a difference. I get it. We can't make every patient experience/feel that overwhelming sense of care as we'd like, but it definitely hurts a bit more than I anticipated. Did I get a little attached? Yes. Could I have helped it? No. Am I sorry that I did? Absolutely not. I will say this experience has brought to light many aspects of Nursing that I was not aware of, but if there's one thing I have learned, is that I care. It may make my time as a nurse a bit more difficult, but I can't help it. I know I can't fix everyone, but that sure as hell isn't going to stop me from trying.

20 notes
·
View notes
Video
instagram
Let’s be thankful for the heart that works tirelessly for us.
Happy Thanksgiving!!
2K notes
·
View notes
Note
Hi there! So I am a first semester nursing student and I am currently failing my theory class...I have failed 2 exams so far and am to the point of giving up. �� I guess I am having a hard time testing, especially since I am not used to these questions. Is there any advice you can give on how to study? I really don't want to fail this class and retake it.
Try reviewing some study videos online or via YouTube. Often times, it takes several different combinations of different techniques to find one that works best for you. Keep it up! I have faith that you'll pull out of this!
5 notes
·
View notes
Text
13 test taking tips
1. Eliminate answers you know are not right 2. WHO WILL DIE FIRST? An yourself this question with priority questions. Who needs immediate attention? 3. How to answer ‘what do you do first’ questions - first think about your ABCs but pay attention to the question because airway is not always the answer. A patent Airway is definitely important, but giving oxygen is not always the solution. Also, what is the simplest thing you can do right now. More then likely a,b,c, and do are all correct answers so put them in order in your head. 4.‘priority questions’ - think about your ABCs and pain. 5. Do not change your answer answer; usually your first choice is the right one, unless you misread the question. 6. Double check to make sure that you have copied the math problem correctly from the test. 7. Look at the central idea of each question. What is the main point question mark site exactly what the question is asking; 1 response is clearly best. 8. Statements that begin with always, never, done, except, most, or least are probably NOT the answer. 9. Examine all answer choices, are three similar while one is different? 10. Find the keywords or phrase in the question that will help you choose the correct answer. 11. If the test requires you to read passages and then answer a question, read the question first. By doing this, you will know you’re looking for as you read. 12. Remember, your first guess is usually right. 13. Psychosocial and psychological questions are sometimes asked in nursing. The answer usually relates to restating the patient’s feelings are asking open-ended questions. Example, tell me how you feel? Or share what you know about the procedure you are having today.
This is not definite but can offer assistance with taking exams. All 13 items do not apply to every test but every item can assist with evaluating questions.
I received this from one of my nursing instructors, and thought it was valuable enough to pass on!!
128 notes
·
View notes
Photo

I have been toying with the idea of converting my SnapChat into a "Nursing School Chronicle", now that I'm nearly done with my first semester. If you're interested, like this post! If there's enough of a demand, I'll send out my SnapChat username and y'all can come along on the ride!
40 notes
·
View notes
Text
Basics for the Wards: How to Read EKGs
I’m on cardiology right now, and yesterday the fellow taught us some basics for interpreting EKGs. The trick is the have a thorough algorithm and do it every time so you don’t miss anything.
Disclaimer: Obviously this is just a cursory intro so folks won’t look like complete fools like me- who, when asked to interpret an EKG, went into a cold sweat and said, “Well, it looks like the heart is beating.” Attendings do NOT like that.
INTRO

This is what a normal lead II EKG one beat reading should look like. TAKE NOTE LITERALLY EVERYONE STOP CALLING YOUR SQUIGGLY LINES HEARTBEATS IT IS WRONG GAAAHHHH.

Normal EKG.


What the various leads are monitoring.
1. Rhythm: Sinus or not- aka, is the SA node talking to the AV node correctly? Check in leads V1 and II- if there is a P wave before every QRS you have sinus rhythm. If this is not the case, you do not have sinus rhythm! A whole discussion on things messing up sinus rhythm will come when I have a better grip on it myself.
2. Rate: How fast is the heart beating- aka, how fast are the ventricles depolarizing? So EKGs are little tiny boxes in bigger boxes, right? There are several methods for calculating rate using the boxes, but the one that works for my brain is to count the big boxes between R’s and divide that by 300. So, 1 big box between R = 300/1 = 300 bpm. 2 big boxes between R= 300/2= 150 bpm. And so on.

In general, any heart rate above 100 is tachycardia, and any heart rate below 60 is bradycardia. These values may vary (ex: SIRS criteria counts heart rate above 90 as tachy). Normal heart rate is around 75 (exceptions include athletes- look up athletic heart syndrome)
3. QRS Complex: Wide or narrow- aka, is the Bundle of His bossing the ventricles around? Basically, a nice narrow QRS complex generally indicates the bundle of His is intact and operating how it is supposed to. A wide QRS complex indicates something is awry with the Bundle of His- could be an organic pathology, could be a medication side effect (ex: antiarrythmics, TCAs, quinidine, to name a few), could be an electrolyte imbalance (ex: hyperkalemia), could be other things.
4. Axis: Is the heart depolarizing the way it should- aka right shoulder to left nipple. I, personally, am still sorting out the axis system, and it’s hard to do in this format. The first, most basic place to start is checking if lead I and aVF are POSITIVE, meaning their QRS complexes go ABOVE the isoelectric line. If that is the case, you are probably ok axis-wise.


Essentially, lead I’s vector goes from left to right, and aVF’s vector goes from head to toe. So the average of those vectors is the general path of depolarization of the heart. You want the axis to be between -30 and +90. So, if aVF is positive, but lead I is negative (the QRS is below the isoelectric line) that means it is going from left to right instead and would be classified as a right shift. Likewise, if lead I is positive, but aVF is negative, that means it is going down to up and would be classified as a left shift. There is soooo much more to axis interpretation, this is just a starting point.
5. Intervals: Again with the conduction system, it’s, like, totally important that it obeys all the rules every time. PR= <.2 seconds, or one big box QRS= <.12 seconds, or 3 small boxes QT= < ½ the RR interval

6. ST segment changes: checking for CAD- aka, is the myocardium getting enough blood/oxygen? Since the folks in the South seem to consider butter a food group and know that if it can’t be fried it’s not worth eating, CAD is a huuuuuuuuge issue here. When blood supply to the myocardium is compromised, there will usually be characteristic EKG changes. Note- not every episode of angina/MI will have EKG changes though! - Inferior leads –> right coronary artery. - lateral leads –> circumflex artery - anteroseptal leads –> left anterior descending. Disclaimer: does not apply to everyone all the time, some folks have variant coronary anatomy.

So the EKG changes to look for must be seen in two contiguous leads, aka, two inferior leads or two lateral leads. - Ischemia (low oxygen) = ST depression or T wave inversion (EXCEPT T wave inversions are ok in leads V1 and aVR)


- Injury = ST elevation

- Old infarct/dead myocardium = pathologic Q waves. Basically that first negative vector (aka, the Q of the QRS complex) should never be bigger than one tiny box.

And, that, friends, is a basic algorithm for reading EKGs! There is a lot more, but if you follow these steps every time, you will look like a rock star on wards. Good luck!

5K notes
·
View notes
Photo




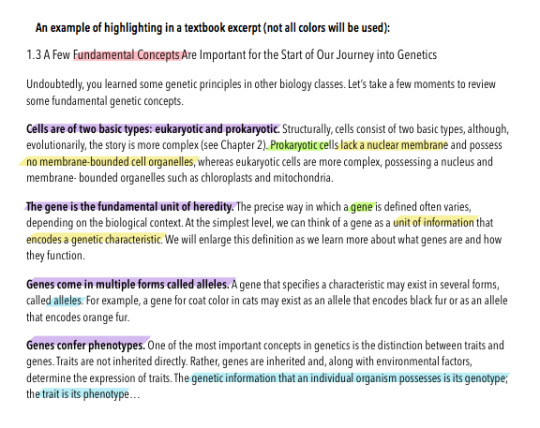
Since an Anon asked how he/she may improve their grades, I decided to share my “Process of Attempting to Know What I’m Doing in Nursing School”.
Top Left Image: An overall view of my “study zone”. It’s nothing fancy, nor do I want it to be. Its simple, decently organized, and it serves its purpose.
Top Right Image: The left side of my desk. You’ll notice my desk organizer (where I store pens, pencils, sticky notes, paper clips, etc.) My Medical/Surgical book with highlighting and sectioned off with smaller sticky notes to quickly reach the chapter I need (dammit, if this book cost over $200, you better believe I’m writing in it), and a small black notebook. This is what I use during clinicals (apart from my black HIPAA-compliant clipboard for quick notes, such as my patient’s lab values).
Third Image: Simply my computer. We’re currently covering the Introduction to Fluids, Electrolytes, and Acid-Bases and I have clinicals on Tuesday, which is when my Care Plan Map is due.
Final Image: The right side of my desk. This contains my lamp, fossilized wood (because why wouldn’t you find it fascinating?!) index cards with dividers for my drug cards (a requirement for clinicals when administering medications, albeit we are only passing PO meds). Figured if I’m already doing the work to write everything down, might as well keep them for reference, and finally…
MY BRAIN BOOK.
This small black book is where I store my notes. It’s small, which allows me to take it anywhere. I use a highlighting system to quickly decode the data:
Pink - Topics Yellow - Definitions Orange - Nursing Safety Priorities Green - Additional Pertinent Information.
I use the PowerPoints for guidance, extract more specific data from my textbook/lectures, and will print out necessary tables to tape in the book for easy access.
Whether this helped you or not, at least now you know a little bit more about myself.
82 notes
·
View notes
Note
Hi there so I'm in medsurge right now and I'm passing with a C but I really really am trying to get a B. I read the chapters multiple times study with groups but I can't ever get higher than a 78 on exams. What do you do to get Bs
What I've learned, and am still learning, each class requires some variation of adaptability when it comes to studying. Some methods I've used are: adaptive quizzing, color coding highlights (diagnoses = blue, QSEN/Critical = red, definitions = yellow, etc.) I have also interviewed a few other of my fellow nursing students to see if they're utilizing some other form of studying I may be able to try.Another component I like to use, is to teach the material to someone else. Albeit a significant other, parent, sibling, or hell, your dog (don't judge, my pup could easily pass the NCLEX-RN at this point).Be confident in your skills thus far! Keep persevering and press on! I know you've got this!Good luck, Anon!
6 notes
·
View notes
Photo

It was a blast! Not only did I learn a good bit in the field, but it was amazing to hear the stories from the IRONMAN athletes while I cared for them.
13 notes
·
View notes
Photo

Or put them in descending order, most orange to least orange.
1K notes
·
View notes
Text
I made my first "C" on my test today...
I thought I'd be more upset with myself. I'm definitely disappointed, but it shows how much more I need to study, since clinicals and paperwork have been thrown in the mix. Here's to kicking ass and taking names on this next test! P.S. Pardon my language. In case you haven't noticed, I have a potty mouth.

15 notes
·
View notes