
Statistics
We looked inside some of the posts by alert-gayshipsahead and here's what we found interesting.
Average Info
Notes Per Post
3M
Likes Per Post
2M
Reblog Per Post
2M
Reply Per Post
2K
Time Between Posts
1 month ago
Number of Posts By Type
Photo
10
Text
4
Video
3
Last Seen Tumblr Blogs





Fun Fact
US Tumblr user growth rate is estimated to slow down to 4.1%.






Photo








Waller-Bridge believes such lightheartedness is vital in any show because it’s “tied up with pathos and is as usefully disarming as it is entertaining.” In the case of “Killing Eve,” she also thinks it helped her audience root for Villanelle — “because she makes them laugh.” “It forgives a thousand murders!” she says.
8K notes
·
View notes







Text
Watching the horrible and shitty ‘successful, perfect woman who makes her husband/boyfriend feel inferior then later apologizes and puts him above her career’ trope get destroyed by Astrid in Crazy Rich Asians was game changing and added ten years to my life
226 notes
·
View notes
Text
ECG: quick and dirty
I’ve had countless sessions and lectures on ECGs. I don’t know how many websites I have bookmarked, or how many times my eyes glazed over reading Dubin. I’m also terrible at cardiology. I was on my way to accepting my fate of being horrible at ECGs forever, until I had a life changing session on ECGs taught by a great ER doc. I want to post it here because it was probably the most useful thing I learned in med school, and it will stick with me for the rest of my career.
WHEN LOOKING AT ECGs FOR THE FIRST TIME:
1. One ECG is never enough. Always get old ones for comparison. If none available, do another one. Because. One ECG is never enough.
2. RATE. Look at the number on top of the printed ECG. It’s stupid not to use that number. Yes, you should know the rule, 300-150-100-75-60-50. People say you shouldn’t trust the machine because… well, it’s a machine, and it can make mistakes. This is true. I don’t like to look at their “diagnosis” until I have gone through it myself. But the rate is just a number. Plus you should be able to eyeball it and be able to tell if it’s tachy, brady, etc. If the machine is telling you it’s 200 and if it looks tachy, then it’s probably the right number.
3. RHYTHM. Is there a p-wave for every QRS and a QRS for every p-wave? Is the p-wave upright in lead II and down in aVR? Good. Done. BOOM. It’s sinus rhythm. ***if you cannot clearly see the p-waves then you cannot call sinus. move on.
4. AXIS. Again, look at the number at the top of the page. If it’s between 0 and +90, then it’s normal axis. If the number isn’t provided, or if your preceptor doesn’t believe in the convenience of machines/technology, look at the QRS complex of lead I and lead II.
up in lead I, up in lead II: normal axis
up in lead I, down in lead II: left axis deviation (most common causes are left anterior hemi block and left ventricular hypertrophy)
down in lead I, up in lead II: right axis deviation (most common causes are right ventricular hypertrophy…PE)
5. did someone say HYPERTROPHY?
look at V1
is the R wave tall? (greater than 7mm?) right ventricular hypertrophy.
is the S wave tall? (greater than 11mm?) left ventricular hypertrophy.
6. P-waves
look at lead II
is it wide? left atrial enlargement.
is it tall? right atrial enlargement.
7. PR interval
should be between 0.12 sec and 0.2 sec (3-5 small boxes). I used to always get this interval and QRS complex (less than 0.12 sec) mixed up. Think: atria depolarizing + shit getting to ventricles is gonna take longer than ventricles depolarizing. [2 things happening] versus [1 thing happening]. [0.12 sec-0.2 sec] versus [<0.12 sec].
long PR interval means there’s some sort of block at the AV node.
1st deg block. PR interval is long. everything else is normal. cool.
2nd deg block
type I: PR interval progressively gets long. eventually a dropped QRS.
type II: PR interval is constant, but randomly dropped QRS.
3rd deg block “complete block”
there is no association between P waves and QRS. they run separately. **QRS does NOT have to be wide. Just look for P wave/QRS complex disassociation. I sometimes get this and 2nd deg type II mixed up. The only difference I try to remember is that PR interval is constant in 2nd deg type II, but is variable in 3rd deg.
8. QRS complex
narrow or wide?
narrow: good. signal coming from somewhere above ventricles.
wide: think BBB (bundle branch block)
LOOK AT V1 ONLY.
if the last deflection of QRS is DOWN, then it’s a left BBB
if the last deflection of QRS is UP, then it’s a right BBB. super easy. no more of this bunny ears crap.
9. ST segment
always look from J point, and compare with the isoelectric line of T-P segment (NOT PR interval).
elevated/depressed… STEMI… duh. indicates ACUTE ischemic changes.
look for reciprocal changes of the heart. if ST elevation in lateral leads, could see ST depression in the septal leads. PAILS:
posterior up, anterior down
anterior up, inferior down
inferior up, lateral down
lateral up, septal down.
LBBB can look like STEMI. How to tell?
disconcordant changes is normal. (QRS and STEMI on opposite sides of the isoelectric line.)
concordant changes is abnormal.
massive discordance is abnormal. (STEMI is greater than 5mm)
this isn’t that important. Moving on.
Inferior STEMI. Could right ventricle be involved?
DO NOT GIVE NITRO DO NOT GIVE NITRO DO NOT GIVE NITRO.
order a 15 lead
is STE in lead III > lead II? likely RV involvement
INFERIOR MI? 15 LEAD NO NITRO
INFERIOR MI? 15 LEAD NO NITRO
INFERIOR MI? 15 LEAD NO NITRO
10. T waves
is it inverted? indicates recent ischemic changes.
11. Q waves
is it significant? indicates old ischemic changes. will likely be present if followed rule number 1 of reading ECGs. (1 ECG is never enough= look at old ECGs).
I literally go through this list of 11 points in my head when I’m reading an ECG, regardless of whether or not I have an atrial flutter jumping at my face or if I see a massive anterolateral STEMI. Obviously I needed background knowledge on ECGs and the physiology of the heart before constructing this list, but this basic checklist has been very, very useful to me so far. It might look lengthy, but it doesn’t take a lot of time at all- a patient is not likely going to have all these issues with their heart.
Anyway. I still don’t love ECGs, but it feels pretty wonderful to be able to be able to evaluate it in a systematic manner, and get the theory behind interpreting the scribbles of an ECG reading. I don’t get these moments as much as I would like to, but it’s that crosspoint where my classroom learning actually meets real-life applications that gives me happy brain-gasms for days. I love knowing things and more importantly, knowing why.

6K notes
·
View notes
Photo
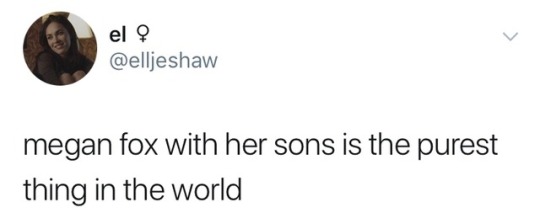




she just lets them wear whatever tf they want :’)
158K notes
·
View notes

Video
She bless the rains down in Africa
131K notes
·
View notes

Video
222K notes
·
View notes

Text
No, I’m serious, if women all got together and went into electrical engineering or automotive repair en masse, then ten years later people would be talking about how it was a “soft field” and it would pay proportionately less than other fields.
Likewise, if men moved en masse to bedeck themselves in sparkles and make-up, then suddenly you’d get a bunch of editorials talking about how classy they look.
None of these things are inherently masculine or feminine; none of these things inherently elevate you or drag you down. But whatever women are seen to do is automatically seen as being inherently more frivolous than anything men do. And shaming women for not pigeonholing themselves into a narrow range of acceptable “masculine” behaviours is just going to result in the goalposts getting moved once again.
263K notes
·
View notes




Text
Piscatella’s backstory in Orange is The New Black wasn’t included to make you sympathize with him. It was a reference to a real life event. On June 23, 2012, four correction officers locked black prisoner Darren Rainey in a shower and raised the temperature to 180 degrees. He kicked the door and begged to be let out, and they laughed and asked if it was warm enough. They left him in there for two hours. When he was pulled out, his internal body temperature was too hot to register with a thermometer. His skin was peeling off. Burns covered 90% of his body. Despite all of this, the official statement was that cause of death was “undetermined” and on March 17, 2017 it was announced that the four COs involved will not face any charges.
His name was Darren Rainey. Say his name. Remember his name.
14K notes
·
View notes