#got diagnosed as an adult but it definitely explained a whole bunch of things
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has 16.74 million mobile monthly users in the US.
Note
i love how you draw i love how you render i love how you conceptualize your characters and your world...your work is such a huge Autism Resonance Moment for me (have you said whether you have autism? well even if you dont, my autism is resonanting hardcore with everything youre doing here keep it up!!!)

#answered#anonymous#thank you that was such a nice thing to say!#I'm autistic yeah#got diagnosed as an adult but it definitely explained a whole bunch of things#and I'm familiar with the Autism Resonance feeling it's this electrifying “oh snap” sort of moment of appreciation and deeper understanding#at least in my experience#united by neurodiversity#own art
851 notes
·
View notes
Text
Finally had the appointment with the psychiatric specialist. Had to get up at 6am and go to a whole other city but I got it.
He was a guy (not the actual doctor I was supposed to see because she's on medical sabbatical). And he was nice but I am awkward with strangers and there were some things... Look, I just hate medical gender bias and there was a little here.
But most of all, there was... Some ableism?
Don't get me wrong, he was good and proper and did his job, he was also nice (and very young), but I was there for an ADHD and autism screening so I could have an official documented diagnosis and, well, there was quite a bit of gender bias about these disorders... And a significant amount of unconscious ableism too.
I'm already being treated for these things but my current doctors (psychiatrist, psychologist, and GP) don't have expertise in this area because these disorders aren't usually diagnosed in adulthood and that is their field, and this guy is the "expert" so we need his stamp on the matter just to dot the i's.
Turns out we didn't have enough time for all the tests because someone messed up and scheduled this as a follow-up appointment instead of an assessment but we made do. Here's my problem though: he only wanted to focus on the ADHD.
Also, he ignored a lot of details I was trying to put on the table but I might be reading too much into this.
According to him, yes, I definitely have ADHD and it's good that I'm already testing the medication for it but he wants to see what else he can do and if he can fix the side effects, but we didn't really have enough time for a full evaluation so he sent me home with a bunch of written tests to take so he can check them next month and have a more concise idea of my issues.
He also cut some of the older medication I had that is now obsolete with the new stuff.
I'm fine with all that. Grateful even.
But I wanted to talk about the autism diagnosis, I've been trying to approach this with doctors for years, I've desperate to be heard ever since I learned just how strongly the symptoms applied to me every since I was born, I'm been desperate ever since I discovered the gender bias in diagnosing females, I did so much research and talked to other autistic people and associations that gave emotional support, but the doctors keep brushing it off, not because they don't agree but because they literally don't want to talk about autism in general, they don't even wasn't to explain why they don't want to talk about it, the stigma is just too big.
Eventually, this is what this doc said:
"Look, autism is a spectrum and all so it's complicated. You definitely have serious autistic traits for sure but I don't think we should test you for it, there's no point because you're an adult and you've already learned coping mechanisms and masking the hard way, you struggled a lot but you're here, there's really not much else we can do help with and not much treatment we can give for this so why saddle you with a bad label?"
Like, it's so ableist. He totally missed the point? I told him I don't really care about what treatment they can give me, I just want confirmation because:
1. there's safety in labels, much more comforting to know I'm normal zebra and not a failed horse,
2. having the diagnosis gives me access to more information and a better ability to find good coping mechanisms and helpful tools for my daily life,
3. having the diagnosis allows me to find community and get mutual help and support without judgement,
4. having an official diagnosis helps me get certain amenities (or at least understanding) to make my life easier, be it with work or family life, even with social security or at certain events,
5. and finally, just because I survived my childhood without a label and found a way to blend in with neurotypicals doesn't mean that's a good thing (I was horribly bullied and abused for a reason), it doesn't mean that I'm currently happy pretending to be what society expects, doesn't mean it's not fucking exhausting, doesn't mean I don't deserve validation for my struggles.
But noooo, his whole focus was on "we can't medicate to FIX it so why bother" and on "what people would think of you if you had that label".
Bitch, I don't care about either of those, I don't care what people think of me, I care what I think of me, and autistic is not a slur, contrary to what people in this country seem to think! I just want to understand myself and my own struggles, and whenever I get harassed for being different I want to be able to defend myself with this knowledge.
For fucks sake, just test me and show some support!
I stg the doctors in this country are so scared of the word "autism", it's insulting.
#rach rambles#autism#adhd#add#asd#austistic spectrum#diagnosed as an adult#as a kid i was just diagnosed with 'weird/picky/awkward/gifted/antisocial/silly/lazy/etc'#but god 90% of my messed childhood makes so much more sense now with context#and the docs just don't understand the relief that is
3 notes
·
View notes
Text
also, since i am... 100% certain that the chip twitters aren't coming back, i wanna take a few minutes to talk about my experience as a mod for one of the characters (since i doubt it's any surprise that I was one lol)
firstly, i'm not revealing anybodys identities here other than my own, because everyone has fully moved on from the project and don't wanna be assocciated in any way with it anymore. i'm making this post mostly for myself and maybe 2 other people so even if you have inklings of who the other mods are, don't look for them. they will not be happy
with that out of the way-
if it wasn't supremely god damn obvious by this point, i was the most recent mod for bert. from like... what, may 2020? that whole big arc where he got out of the bertputer, that's when i started. definitely a lot of weight on my shoulders with that one.
despite how much i had fun writing for bert though... this whole project was really a nightmare from beginning to end behind the scenes. before we (the new team) could even start actually posting and writing stuff, there was a whole kerfuffle getting the keys (account log in info) from the old team. had to even get david involved for a few things, which we really hated doing just cuz we didn't like bothering him. the old team was also... well, its own thing. i've kinda blocked out most of what happened regarding that but what i do know was that it was very mentally taxing trying to get rid of the old guys and get us logged into the new accounts.
people also certainly had... mixed feelings about the direction we tried to take things in. we were handed a story that was already extremely jacked up with its own weird baggage attached and had to make do with what we could. the story beats set up by the previous team were really hard to work with and we genuinely just did not agree with some of the characterization that was happening. namely bert and otto, they were... something. so, we tried our best to work with it and find justifications or explainations for certain behaviors and actions. i do know for a fact that there were people that did not like what we did with bert, especially. remember seeing stuff saying that we 'aged up' bert for the sole purpose of shipping him with rotten which... is not at all what happened. he was already a grown up character, in his late teens or early 20s, but the previous team had infantilized him to such a degree and for so long that that was just what people knew. we ended up justifying this by basically diagnosing bert with trauma induced age regression. it's a little complicated and a little fuzzy to recall, but that's the intention we were going with, at least.
we did originally have bigger plans for these characters and their arcs and everything, but the team was losing interest and everything surrounding it was genuinely sending some of us into mental crisis. it made us all distance ourselves really far from the project and not wanting to touch chipspeech as a whole with a 10 ft pole. a lot of this stemmed from the sovereign station server too, it was fine like 80% of the time, but shit got weird in there. if you weren't in there then like, good. you've saved yourself the headache. but overall, pretty much everyone has moved on and is doing their own thing now. there's been a few mods that I don't talk to anymore due to other circumstances, but I'm still good friends with a handful of them. they're doing much better now, too.
long story short, the characters just... aren't gonna be coming back, as far as I can tell. it's been pretty obvious due to the 2+ years of radio silence, but just to put the nail in the coffin. i still believe that the twitters are a great springboard for your own interpretations, and that's kind of another reason why we stopped. these characters can honestly be whatever the hell you want them to be. making a rigid sort of canon to apply to them is a little silly, especially when it's a bunch of young adults roleplaying that canon on twitter dot com. do whatever you want. it was a fun enough ride while it lasted.
that being said though, i personally still hold chip near and dear to me. strong interest has definitely faded, but i still like making covers occasionally and drawing the guys and silly stuff like that. i have a lot of myself to thank for chipspeech, and that's not changing, despite the horrors that we faced. thanks for reading all this if you did lol.
and bert is best boy im DYING ON THIS HILL!!!!!!!!!!!!!
10 notes
·
View notes
Text
random headcanons dump - Zach&Eric pt.1
//just a bunch of random facts, i've collected in my notes, let's go
Zach has his right ear pierced and usually wears his Mom's diamond earring. when she lost one earring Zach immediately claimed the other one.
he doesn't like wearing chains/pendants while Eric prefers them. Zach wears many bracelets and, guess what, Eric doesn't like those.
more look-related things; as for his go-to hairstyle:

Zach's existence is a constant coffee overdose and he only switches to matcha when he's in Japan.
never liked watching his parents’ movies, but can’t explain why.
he's mildly autistic, diagnosed as an adult. he's always displayed some autistic traits but they had managed to pass under the radar for years.
neither Zach nor Eric has ever smoked or vaped or anything like that, but they wouldn't mind smoking pot because, unlike cigarettes, it smells nice.
Zach's nickname's origin is obviously music-related; he got it from Duran Duran's album Rio and it was the first cassette he asked his parents to buy him when he got his Walkman. it also means "river" in Spanish, which happens to be Eric's middle name.
Eric got his nickname from not just one but a whole bunch of middle names his Mom wanted to choose from - Deveraux, Denver, Devin. the boys just played with those names, shortened and rearranged them, making fun of their Mom's ideas... until one day they realized Zach started actually using some of them.
although it perfectly describes Eric in general, his "Bad Idea" lightbulb tattoo was inspired by his Dad's reaction to the idea of getting inked.
Eric definitely has more clothes than Zach but they're all black so, welp, you can't tell.
5 notes
·
View notes
Note
Hi! So like five months ago I sent you an ask about applying to grad school and you gave me a super amazing answer. And I'm back now because holy shit I got into grad school (CalArts for Creative Writing) and in the last one you said there was a whole 'nothing list of tips if you actually get into grad school? And I got in and I'm curious what the tips are? If there's anything you've learned in the last few months that changed your perspective on grad school? Thank you so much!
First off, congrats! That’s a big accomplishment! Grad schools in general are competitive, and big names like CalArts even more so.
So, you want my advice, eh? Okay. Let’s do this.
First step is getting organized. You start in the fall (I’m assuming), so you have plenty of time. Find out where important locations are on campus, familiarize yourself with the area you’ll be spending most of your time in (I’d focus on figuring out where the closest bathrooms and places to get food are, personally), and invest in a planner. Keep that planner handy. Use it. It’s easier to stay organized if you start the semester that way than it is to try to organize yourself halfway through the semester. Make a monthly budget. Decide “I will spend X amount on groceries every time I go shopping”. Keep track of the money in your bank account (a lot of banks have mobile apps that make this very easy). Put some of your paycheck into a savings account every time. You never know when you might need a nest egg. Stay up to date on your medical needs (prescriptions, flu shots [for the love of god, get a flu shot], dentist appointments, yearly physicals). You can definitely find resources at your school to help you with some of these tasks. There is no doubt in my mind that you will be able to find a workshop on keeping a budget or other adult skills. Attend workshops for new grad students.
Second, look into different support systems for students. That means student-led organizations, departments that exist to keep the university complying with federal non-discrimination laws, and general resources. Get a support system set up right away, particularly if you are going to be far from family.
Student-led organizations will be able to help you adjust and provide you a sense of community (particularly if you belong to a minority community). Other grad students will be able to offer advice faculty or staff might not be able to. Don’t isolate yourself! That’s what I’ve been doing and it sucks! The only reason I haven’t driven myself completely insane is because I have a roommate who happens to be my best friend. If I could start over, I wouldn’t do what I did and avoid everyone because I was intimidated. I would stroll into rooms with purpose and confidence that I am the baddest b*tch there. Confidence gets you far in life, particularly in grad school.
“Departments that exist to keep the university complying with federal non-discrimination laws” is a very wordy way of saying the Title IX office, disability services, offices for students of color (schools typically have different offices for different racial minorities; find out which one is best suited for you), the LGBT resource center, and the like. If you are part of a demographic minority, find out where you can locate help immediately. If something goes wrong related to your status as a minority, you need to nip it in the bud RIGHT AWAY.
General resources are things like mental health services, university health services, survivor services, etc etc. If you have any history of mental health issues or have been in therapy at any point in your life, I recommend jumping into counseling immediately, even if you feel like you don’t need it. Just talking to a neutral party will help you more than you think. Most schools offer free counseling for students, too. If they don’t, then that’s really fucking weird, but they should be able to help you figure out a method for you to adjust smoothly without it being too much of a drain on your wallet.
Third, learn from my mistakes. Good lord, learn from my mistakes. I had a disastrous first semester at grad school. I was overwhelmed, completely out of my depth, and the one thing I thought I was doing right I discovered I was actually completely fucking up. I entered my second semester on academic probation and probation as a TA. How do you learn from my mistakes? A few ways.
The first time you TA (most grad students TA at some point), insist on someone observing you. The department should automatically observe all TAs, particularly new ones, but it’s possible to slip through the cracks. That happened to me. The head TA was too busy to observe TAs my first semester, and I didn’t find out that I was a shitty TA until I was in a meeting with department and university head honchos, who were effectively accusing me of hating my students and hating being a TA and sucking in general. That’s paraphrasing, and definitely not completely accurate, but that’s how the meeting felt to me. I got by only because I explained to them “I am autistic, I struggle with new social situations”. The extenuating circumstances in my situation allowed me to try to TA again, but this time with some accommodations and outside assistance.
Related: If you are disabled, disclose it to the department. Disclose it to the higher-ups and the professor who will act as your advisor. You don’t need to disclose it to anyone else, but I cannot emphasize enough how important it is to tell the people you will be working for. Even if you have amazing coping skills, disclose it. I’m damn good at pretending to be abled. But my disabilities still bit me in the ass. New situations and stress have a tendency of exacerbating symptoms. You can’t expect everything to go smoothly. And you can’t expect the department to hold your hand or even recognize what’s going on with you. I’m the first diagnosed autistic grad student my department has ever had. They had no clue how to handle that. You’ll be going into a field that tends to be a bit more liberal than STEM (like my area of study), so you might not run into the issue of “uh we don’t know how to help you, please talk to some people at the office of equity”, but it’s best to find out sooner rather than later.
Related: If you are disabled, get your ass down to the disability services office and get accommodations. Immediately. Start the process over the summer. Larger schools might have a more complicated process to get accommodations than smaller schools, so you need to get the ball rolling right away. Even if you haven’t felt like you needed accommodations recently, get the ones you had in the past. Don’t assume you’ll be fine without extra help.
Don’t take too many classes your first semester. And make sure the ones you do take aren’t all super difficult. I fucked up my first semester, bc I took three upper-level classes, two of them in chemistry. Yeah, three doesn’t sound like much. But when you’re juggling adjusting to grad school, starting up your thesis, and being a TA, three classes is a huge fucking amount of work. I’d recommend two classes, maybe one of them difficult, the other one sort of medium difficulty. Of course, you have to talk to your advisor for what works best for you, but I highly HIGHLY recommend starting off with a light class load your first semester.
When things start going south, bc they probably will at some point, don’t just keep your head down and try to force yourself through it. Talk to the family members you are closest to (I’m very close with my parents, so I talk to them when I’m having issues, but it could be a sibling or an aunt or uncle or cousin). Talk to friends. Talk to a counselor (PLEASE get a counselor your first semester). Talk to your advisor. Talk to the other grad students in your department. You should be able to find at least one shoulder to cry on, if not a whole bunch.
I said this before, but don’t isolate yourself. Please don’t. It’s easy to avoid people when you’re stressed. Don’t do that. Reach out to other grad students in your department. Make friends. Go with them to coffee shops. I wouldn’t recommend starting out by going to bars, bc that can be a slippery slope, and you shouldn’t have friends who only have fun while they’re drinking (that’s not a healthy behavior). My grad school has a really nasty drinking culture that contributed to my avoidance of other grad students, but hopefully yours doesn’t. And even if it does, you should be able to find someone who won’t want to always go to the bar.
Fourth, be confident. I said that before, but like the “don’t isolate” thing, it’s important. I’ve always been a confident person. I took a huge blow to my confidence when I started grad school, bc I felt like I was surrounded by people with more experience (which is an objective fact, but doesn’t always have to be a bad thing) and more knowledge and more accomplishments and who had their lives together. I was intimidated, for one of the first times in my life! I’ve always been a top-tier person, cream of the crop, A+ honors student, go-getter, award-winner. But in grad school, literally everyone else is that, too. And that’s not a bad thing! Sure, some people might be braggy, but other people will be more humble. Having all this experience in one location is good, bc it means you have more help. You have people you can talk to who have connections, who have run into problems you might run into, who can offer a unique perspective on things. That is SO GOOD. And if you’re still intimidated, think of it like this: You got there, too. You’re just as good as the other grad students, otherwise you wouldn’t be there. You have just as much potential, even if you don’t have as much life experience. You have something unique to offer to the school. If you didn’t, you wouldn’t have been accepted. And it’s not like everyone else actually has it together. Some people might, but most of the other students will be as lost and nervous as you (esp other first year students).
Fifth, toot your own horn. It’s related to being confident, but not quite the same. Talk about your accomplishments. Tell people what you’ve done. Try not to come off too braggy, but don’t hide your light under a bushel. You have to promote yourself if you want to get anywhere. You’ve already succeeded at it once, since you got into grad school. Keep it up! Oh, and don’t be afraid to toot your own horn when someone else is making you feel intimidated. I was at a thing where one guy kept going on and on about how he’d been to this country, and that country, and tried this wine and that food and yadda yadda yadda. I got sick of it, so I cocked my head and stopped him in his tracks by asking him if he’d ever been to Kosovo. He hadn’t. He’d been to a million places, but there was one that I had him beaten on. That was a huge confidence booster. You have your unique experiences. Share them. And don’t be afraid to use them to stop a braggart from controlling a conversation.
Sixth, stay healthy. Mentally and physically. Walk most places (that’s how I get my exercise), bike, do yoga, jog, whatever. Get some exercise. Eat well. Make your own meals, keep track of whether you’ve had a vegetable today. See a counselor, vent to friends, write in a journal. Most schools offer wellness workshops where students can learn how to keep themselves healthy. Look into that, particularly if you struggle to eat well or keep stress down.
Seventh, take a short break if you need to. Grad school culture is intense. People work way too long for way too little recognition. Stress kills. Burn out can make you question your path. Say no to a third side project your advisor wants you to do. Take a day off, or an afternoon. Take a long weekend. Make sure that things won’t fall apart while you’re gone (in my case, I would get lab work done the day before), let your advisor know you won’t be coming in today for health reasons (you can keep it vague), and then spend your day doing anything but work on your thesis. Don’t give in to stress and burn out. It will wreck you.
Eighth, enjoy yourself! Grad school can be hell, but it can also be fun! You’re here to learn and gain experience and, hopefully, not hate every second of it. My own grad school experience has been roughly 92% hell and 8% fun, but I wasn’t prepared when I came. I did the opposite of hit the ground running. I tripped and skinned my knees and my face and I’m still trying to catch up with everyone else. Being prepared, reaching out to people who can help you adjust, those things will ensure your grad school experience goes more smoothly than mine. Just don’t expect everything to go perfectly right off the bat. It’ll take some time before you feel like you truly can enjoy yourself.
…That ended on a weird note, but I hope it was helpful.
You’ve got this! Best of luck!
#whew that turned out long but I knew it was going to be long#again I hope this was helpful#grad school#rant#ask#beatrice-babe
6 notes
·
View notes
Text
Embarrassing admission: I’m a savant. Stick with me and I’ll explain, but it’ll take awhile.
Understand that I’m not saying this to brag. This is not easy for me to admit to myself, let alone anybody else. It’s taken me over a year to write this.It’s actually as difficult for me to discuss this as it is for me to discuss the fact that I actually have coprolalic vocal tics. In fact autistic people’s discussions of savant skills often resemble Touretters’ discussion of coprolalia: There’s a tendency to try to make out like they’re much rarer than they are.
About 10% of Touretters are thought to have coprolalia, that is vocal tics that sometimes involve involve swearing or other offensive words (like slurs). It’s embarrassing to Touretters as a whole because to a lot of people Tourette’s is like a punchline to a joke about cussing. Similarly, about 10% of autistic people are thought to have savant skills (I suspect the number is higher), and autistic people are just as embarrassed by the fact that savant skills have become a stereotype. 10% is one in ten people. That’s not actually the tiny minority that people would have you think it is. And I do believe savant skills are under-reported for reasons I’ll get into later.
Some background about myself
I was first recognized as being autistic at the age of fourteen. I was in a mental institution following a suicide attempt, at the psychiatrist I got was randomly assigned. In other words, he had no reason to be specifically looking for or expecting autism when I first became his patient. I would remain his patient until his retirement and subsequent death in my twenties.
Anyway, after he met me, he asked to meet with my parents. My mother describes him interviewing her extensively about my early development, asking pointed questions about certain things. She said he very quickly said of me, “Your daughter sounds like an idiot savant.”
A note on terminology
Idiot savant sounds outdated or downright rude, depending on your take on things. Even in 1995 when this was taking place. To understand what he was saying, you have to understand the history of terminology around savant skills as well as his own personal history.
So first off -- my doctor was old. He was trained and did his residency at a time when Southern mental institutions were still fully and officially segregated by race. His age and specialty in child psychiatry meant that he had met a lot of children over the years, including a lot of autistic children. It also meant that he used a lot of terminology that would at best be considered quite old-fashioned today, because he learned his clinical vocabulary in probably the early sixties.
Idiot savant does not mean a specific type of savant. It has nothing to do with the outdated classification of idiot which usually meant what today would be referred to as a severe and/or profound intellectual disability. There was never an IQ cutoff for being an idiot savant. Idiot savant meant “wise idiot” and was meant to cover the unevenness of cognitive skills that was characteristic of cognitively disabled people with savant skills.
So him saying I was an “idiot savant” would be the same way that someone today would say “Your daughter has savant syndrome.” He was not making a judgement about my IQ, which at the time had only tested as high, at the age of five, largely due to the effects of hyperlexia, a learning disability involving early reading ability usually combined with comprehension issues, that is in some contexts itself considered a form of savant skill.
People talked about idiot savants, and then it became autistic savants (except that this term would only be applied to autistic people, who are not the only people with savant skills), and these days it’s savant syndrome. You don’t need a cognitive impairment of any kind (such as autism or intellectual disability) to be a savant: There are a lot of blind savants, for instance. Today people mostly just say savant or savant syndrome.
But definitely understand that idiot savant was its own term, separate from both low IQ/intellectual disability in general and the classification of idiot in particular. In fact, very few people identified as savants throughout history, including when the term idiot savant existed, have ever fallen into the official classification of idiot or any of the terms that replaced it.
The confusion people have about the technical term idiot savant (mistakenly relating it to idiot in particular or intellectual disability in general) is very similar to the confusion over the term psychomotor retardation. Psychomotor retardation refers to a mental and physical slowing associated with certain medication side effects as well as a number of conditions such as depression. It has absolutely nothing to do with the category called mental retardation, a recent but now outdated term for intellectual disability. They both have the word retardation in them because it means slow, but they refer to entirely different types of (purported) slowness.
Back to my own history
So he called me an idiot savant before he even used the word autistic to describe me. Both words came up in the first few sentences of that conversation, but idiot savant was the term that came up first. Savant skills were the first unusual thing he recognized in me. Within a month, after further interviews, conversations, interaction, observation, and formal testing, as well as consultation with a team of psychiatric and neurologic professionals, he diagnosed me with autism. Within the description of my diagnosis, he mentioned idiot savant qualities.
The actual autism diagnosis happened in a way that was extremely common in the nineties. He knew that I met the full criteria for autism. He told my mother I was simply autistic. But in the nineties, saying someone was autistic was equivalent to saying “This person will never improve, all therapy is wasted, don’t spend any more money on them than it takes to permanently institutionalize them.” He knew it would be terrible if the insurance company took this take on me -- which they were already trying to do without that encouragement. So on paper, he alternated between saying I had a complex and diagnostically confusing developmental disability, and saying I specifically had PDDNOS or atypical autism. Using PDDNOS/atypical autism as a substitute for a flat-out autism diagnosis was extremely common in the 1990s and had nothing to do with whether you actually met full criteria for autism.
My diagnosis was changed to autistic disorder later on by the same doctor, after the danger had passed and an autism expert had suggested making the change but suggested I go back to the psychiatrist who knew me the best to confirm that this was an accurate thing to do, since the expert in question did not know my family or have years of observation and testing to go on, whereas my psychiatrist did. This was after a bunch of misdiagnoses that would take way too long to explain but that were also quite common in the nineties, in fact some of them were among the most common psychiatric misdiagnoses of autistic people.
The savant thing
So... at the time of my autism diagnosis, autism was an abstraction, and a word I did not understand how it applied to my life. Words like ‘underlying developmental disability’ and ‘pervasive developmental disorder’ and really anything with ‘developmental’ in it might as well have been gibberish. Even when I heard these things over and over, most of the time I ignored them. I’d occasionally read a book by Donna Williams or Temple Grandin, identify to one degree or another, but not grasp what autism was any better for having read these things. And most of the time, while others in my life apparently thought about this diagnosis a good deal, I didn’t. The savant stuff was way under my radar most of the time as well.
I was an adult before I understood why I was diagnosed with autism. I was also an adult before I really saw that I’d been labeled as having savant skills or savant qualities, and before my mother told me the story of my initial diagnosis. And to be honest, I mostly ran away from the label, inside my head, and neither said much about it nor thought about it any more than I had to.
Like many autistic people, I was conscious that the popularity of Rain Man had caused people to view autism as inevitably involving savant skills. Being a savant had become a stereotype. And Rain Man was an unusually talented savant. Most savants have neither his degree of savant skills nor his sheer number of savant skills. He was based on a small number of real people, most notably Kim Peek, who had agenesis of the corpus calosum and a huge number of highly impressive savant skills.
Like many other autistic people, I was very critical of the concept of savant skills. I thought it was just a way of passing off talents as somehow unexpected or pathological or both, when they happened in disabled people. I thought it was just a shorthand for giftedness, a concept I have a great deal of trouble accepting as real or useful, at least not as it’s currently defined. And in many cases it has been used in these ways and autistic people are correct to be suspicious and critical.
And honestly I was afraid of it. For reasons I still can’t articulate, it really terrified me to face the idea that I might be a savant for real. But as I discovered, I am.
What kinds of savant are there?
One of the things that had me confused about savant skills was that, like many people, when I think of savant skills, I think of the most extreme skills. Those are also the rarest kind of savant skills. Prodigious savants, as such people are called, are uncommon. They have never been the most common kind of savant at any stage in the development of the idea of savants in general.
So here are the modern, official classifications of savant. Remember here that I don’t make up the words for each kind of savant skills and may not like them.
Splinter skills are the least spectacular kind of savant skill. They represent talents that are highly impressive specifically when compared with the cognitive difficulties the person has in other areas. They are very common among savants.
Talented savants are savants with talents that are likewise in contrast the person’s difficulties, but they would very obviously be things the person would be considered talented for regardless of disability or lack thereof. They are also pretty common among savants.
Prodigious savants are the rarest kinds of savants. They are people who have skills that would be considered not only highly talented but well beyond the range most people even consider humanly possible for someone to have a skill in. Like the way Stephen Wiltshire can fly over a city once and then do a detailed and almost entirely accurate sketch of he entire panoramic view from memory.
Knowing these categories, I can see that I have a lot of splinter skills and sometimes veer into the realm of talented savant. This is a much better representation of my areas of talent than te concept of giftedness in general is, because the the term savant refers to a talent in a relatively narrow area surrounded by areas of great difficulty. That contrast has been a fact of life for me forever. Like back when my hyperlexia gained me a high IQ at a time when I literally didn’t know what the word test meant.
Hyperlexia is something that’s sometimes considered a savant skill and sometimes not. In my case, I feel like it is, because it’s an extreme and isolated talent that came seemingly out of nowhere and that is accompanied by extreme cognitive difficulties in areas that most people would assume to be related to the areas of talent.
I also had musical savant skills. Perfect pitch is another thing that’s considered a savant skill some of the time and not others. But the fact that I was first chair, first violin in the junior high orchestra by the age of seven, I can’t read that as anything other than an obvious foray into the realm of talented savant.
Up until I was in my early twenties, I had a spatial (not visual -- closer to kinesthetic, or the way blind people map space) map in my head of every place I had ever been, indoors or outdoors. I never got lost. Ever. I don’t know why I lost this but while I had it, I can’t see it as anything but a savant skill. My mother, who has severe spatial awareness problems (she’s very visual -- she and I are opposite kinds of proof that visual and spatial are not the same skill), has used me as a navigator since I was a small child,
I also have something that I feel like must be extremely common and not usually recognized at all. I would call it a partial savant skill. It’s a skill that isn’t quite a skill because it has no outlet. I am constantly composing detailed, complex, original cello music without even trying. But with no way to play it in realtime, and no way to write it down (translating to musical notes is a laborious, slow process for me), the music remains in my head and never shared with the world. So I don’t know that this counts as a “real”savant skill by objective measures, but it feels like a savant skill with a crucial piece missing. I wonder how many people have partial and/or unexpressed savant skills like this.
I think my art (specifically, painting in recent years) falls somewhere in the category of either splinter skill or talented savant skill. Which may always be a subjective thing, and it’s difficult to judge the quality of your own work. But this has less to do with some objective measure of quality, and more to do with the way in which the art takes place and the way the skill developed and functions. Savant skills are more than just the presence of an unexpected skill, there’s specific ways they are learned and function in a person that mark them out as different from your average talent of the same level.
And people do hide their savant skills sometimes, even when they are obvious savant skills. I am not open about all of my savant skills. Additionally, not all savant skills are in areas where people normally look for savant skills. The current savant experts focus almost entirely on certain areas for savant skills, to the exclusion of other skill areas.
Additionally, many disabled people develop skills that are entirely unknown to nondisabled people and therefore unmeasured and not accounted for in descriptions of possible savant skills. It is entirely possible, in fact probably common, for people to have savant skills in these unmeasured skill areas. I am no exception to this. I have savant skills I can’t even describe because nobody has ever acknowledged the existence of the skills in question never mind come up with language for them.
Anyway, I eventually realized it was important that I face the fact that I have savant skills. It’s more than a little embarrassing. It’s not something I wanted to admit to myself. I’ve spent over a year agonizing about how to articulate what I’d found out about myself. As well as whether to tell anyone about it at all.
I know a lot of people don’t believe savant skills are a thing. I have read several books on the topic and concluded that they are a thing. And that they apply to my life. I’m not capable of explaining all the details. And calling something a savant skill is and should be very different than just a way of saying that someone disabled has a talent or qualifies for some definitions of giftedness. (In fact, I don’t believe in any common concept of giftedness that I’ve ever heard of. I do, however, now believe in savant skills. They’re entirely different ideas.)
Anyway, I can’t explain why this was so hard to believe, herd to face up to, and hard to admit. But it was. I still can’t escape the fact that I have savant skills, and I’m better off not trying to escape or deny it any longer. I have to admit that the doctor who first categorized me as autistic was right about the savant thing as well. As I said, i’m not bragging. I’m simply publicly admitting that my combination of skills and difficulties -- both current and past, since some skills have vanished and others have appeared over time -- fits the savant pattern perfectly, both in areas that are usually widely recognized as common savant skills and in areas they would never even notice.
#actuallyautistic#actuallysavant#savant#savant skills#savant syndrome#long post#personal#difficult to admit#talents#splinter skills#talented savants#prodigious savants#actuallyDD#savants#developmental disability#cognitive disability#autism#personal history#diagnosis#psychiatrist
183 notes
·
View notes
Text
It was hard not to be affected by the keyboard warrior backlash Kylie Jenner got last week after announcing that her new skincare line would include a walnut facial scrub. Being a 90s teen I didn’t really think too much of it at first. I came of age in an era before political correctness, when nobody questioned where you put your nuts but hey, times have changed and so have I!
So what’s going on?

Picture from here.
Walnuts, that’s what.
If you read even a handful of the comments online it leaves you with the impression that there is nothing worse for your skin than a dollop of walnut face scrub. As a cosmetic chemist that is often asked to incorporate natural scrub particles into cosmetic products I wanted to dissect this backlash a little, flesh it out, play with these ideas a little, work out where the truth lies. I did this first from my perspective as a cosmetic chemist and then by chatting to the lovely Amy Erbacher, facialist-to-the-stars and someone with heaps of up-close-and-personal insights into what people do to their skin and how the skin takes it. Chemists don’t really have that sort of insight you see.
The backlash – a semi-scientific appraisal.
So what people seem to be upset most about are these things called ‘micro tears’ that allegedly form on the skin after you scrub it with walnut particles.
After thinking on this for a moment, I found myself wanting to form a mental picture of how ‘this’ rates against ‘that’. What that means is, if I assume that the people are right, that Walnut does form micro tears on the skin and that they are bad, how does that compare with other exfoliating particles, with harsh towelling of the skin, with environmental factors (sand, wind, dust etc) and with other things we might do to our skin (needling, microdermabrasion, lasers etc).
Walnut particles are abrasive. They are abrasive because they are hard and un-yielding (they aren’t squishy like a sponge) and they also have some jagged rather than smooth edges. It is likely that these jagged edges could cause tiny skin tears.
Here are two microscope images of some Walnut scrub particles that came out of St Ives Apricot Scrub. The left side is at 4 x magnification and the right side is 10x. You can see some big particles and some small, some clumps and some individual particles. You can see the rough edges but generally these are just bulky and woody with little spiked bits.
A while a go, I looked at a whole bunch of other exfoliant particles. They are shown below. Looking at this you can see a range of natural and an un-natural particle. The Jojoba beads are round and soft-edged. These also melt at around 45-50C which is face-wash temperature. The micro-plastic is somewhat round but with little jagged bits in the background. The other materials, sugar excepted, are quite jagged and un-even.

How can looking at this help with understanding micro tears?
If it is true that walnut particles cause micro tears to the skin, looking at the above range of exfoliant particles it would seem reasonable that at least some of the above could also cause the same. This to me is interesting as the response online to Kylie Jenner’s launch was very emotional and ultra specific about Walnut shell. Some early responders also cited a law suit brought against St Ives that got into the USA court system late last year. As fairly typical of people trying to drive home a fast point, they neglected to inform their readers that the law suit application failed. Maybe looking at the above gives us some idea of why…

So what does using scrubs like this do to the skin?
This is where I couldn’t really answer and is why I got Amy Erbacher involved.

Amy came to me a few years ago when she wanted to develop her own range of skin cleansers based on what she had learned from years in the beauty trade. Amy explained that she often picks up visual signs that a clients skin has been treated too harshly during her practice as a facialist. Typical signs of past trauma include hyper pigmentation, irritation, adult acne and/or hypersensitivity. Of course, being a facials Amy doesn’t give any medical diagnoses but it is her job to attempt to bring the skin back to looking and feeling good.
So they are the symptoms but what about the causes?
Amy thought it entirely possible (even probable) that the habitual use of harsh abrasives, especially when applied vigorously and often to the skin, could be contributing to the symptoms she sees. However, she felt it unlikely that physical exfoliant of the type purchased over-the-counter are the only cause of clients woes with UV exposure, lifestyle habits such as smoking and a poor diet, over-use of AHA’s and Enzymes and our addiction to instant results also playing a part. On that front, as a facialist, Amy has observed clients growing appetite for cosmeceuticals as a potential double-edged sword. Demands for stronger AHA products, faster-acting serums and deeper dermal delivery have (potentially) pushed the skin barrier to its limits for some clients resulting in various symptoms of premature ageing. When talking to Amy there was a clear vibe coming from her that the best approach to skin care was to take it gently and…care for it.
Stopping there for a moment there are clearly some subtleties to the case of ‘nut gate’ that we must address. Maybe it’s time for a little self-analysis and therapy?
Going back to my teenage years I just could not get enough facial scrub into my life. I had acne and part of that was blocked pores and blackheads. I was convinced that a good old scrub was the best way to get that dirt out. Coming into modern times I’ve had more than one client send back the scrub samples I sent them for a bit of ‘toughening up’ when I went a bit too easy (gentle) on the physical exfoliation. So while Amy is clearly telling me to calm it down in one ear, my other ear is hearing ‘give it to me hard baby’. Who do I listen to!
Balance, perspective and application.
Amy clearly has a point. The skin (and remember, we are talking facial skin here) is delicate but it is not pathetic. This report looks at how skin resists tearing and by looking at that we can clearly see that a little exfoliation isn’t likely to cause long-term damage when used sparingly and with care. As we have eluded to above, there are many cosmetic procedures and practices that leave our skin slightly traumatised, indeed, that’s often how we get fast results. Acids, needles and microdermabrasion treatments all stimulate the skin, instructing them to repair, re-build and restore the skin hopefully to its brighter, smoother and more youthful self. In that way we could say that our trauma led to personal growth – what doesn’t kill us makes us stronger. So maybe the only trouble when it comes to exfoliating our skin is knowing when enough is enough…
When exfoliation has to stop.
Acne.
In Amy’s professional practice she recommends only the gentlest of scrubbing in all cases and never for skin with live acne pustules – see that’s where I used to go wrong. I had the mindset that the scrub would set the pimple free and leave my skin clean and un-clogged. Looks like all I was doing back then is spreading the germs around! So that’s one down-side of physical exfoliants – spreading microbes around the skin. Are there any more?
Sensitive types.
Amy points out that another down-side of harsh scrubbing is the disturbance of the micro biome. We are only just starting to learn how our few Kg’s of microbes that live in and on us keep us safe and well. While exfoliants won’t damage the microbiome per se, they do ‘clean’ a bit more thoroughly than a product without them and for some people this can leave their micro biome a little scattered and when that happens, the skin can become more sensitive. Again, it is a case of ‘less is more’.
Damaged Skin.
Amy points out that it is really tempting for those with sun-damaged thickened skin to go crazy with exfoliants but again this isn’t recommended. The skin is thickened due to sun damage and so scrubbing that off won’t really help long-term as you are just layering more stress onto already stressed skin. From my perspective these probably are the clients that ask for harsher scrubs. From now on I’ll be talking to them more about cosmetic retinol products and gentle chemical exfoliants as safer alternatives.
When you have an addiction to harshness.
I have had several conversations with Amy over the years and there definitely does seem to be a section of the population that just can’t get enough when it comes to beauty treatments. I think I was semi-addicted to the ‘freshly scrubbed’ feeling I used to get from my walnut exfoliant even though it was probably not doing me any good. This behaviour is definitely going to result in long-term skin complications if it is kept up but it pays to remember that this is NOT, I repeat NOT the nuts fault.
The bottom line in nut-gate.
Amy is clearly in the ‘treat it ultra gentle’ camp whereas I like it a little rough (probably based on my earlier facial abuse) so who is right?
Amy is coming from a strong evidence-based mindset that over-exfoliating is one of the contributing factors leading to skin issues down the track. Because of that she strongly warns her clientele against harsh scrubs. This advise is backed up by many other facialists, dermatologists and skin professionals.
When I look at the St Ives Apricot Scrub I see that it suggests using it 3-4 times a week, the Kylie Jenner product is apparently gentle enough to use every day or, as the pack suggests, 2-3 times a week. I don’t know if the exfoliation rate is equivalent for these two products but having worked with Walnut exfoliant as an ingredient for many years it is unlikely to deviate much from the general shape, size and hardness typical of this ingredient. What could vary is the dose, the cushioning effect of the base and potentially the formula pH, perfume and preservative, all of which can contribute to the overall harshness or gentleness of a formulation.
Do we do what the packet says?
Looking back to my most addicted period I think I used the St Ives scrub 1-2 times a day in my bid to ‘clean my pores’. Clearly it would be reasonable to expect a difference in results between people that over-use a product and those that follow the normal/ recommended use pattern. That said, Amy was strongly of the opinion that 2-3 times a week would be too much, in general for skin to handle and I feel inclined to agree. Maybe the days of exfoliating the shit out of our faces should be resigned to history, like the Spice Girls, Shell Suits and Cherry Coke…
So where does that leave nut-gate?
Ummmm, I think it is all a bit more nuanced than the good folks of the inter webs would like us to believe. There is a clear ‘OMG NO, are you trying to kill us Kylie’ vibe going on online at the moment but maybe that’s all a smart publicity ploy, one never knows.
Traumatising the skin is a strategy that some cosmetic products and procedures use to their advantage so to single out walnut scrub as the worst thing to have ever happened to the skin is a bit silly really and does nothing to progress the conversation. Micro tears are a type of trauma that a scrub could produce, but physical exfoliants won’t tear up your skin to any noticeable degree unless you scrub like a daemon, have skin that is already damaged or use the product in excess (and excess is going to differ for everyone) – all things being equal. If you are an abusive scrubber then you should not just be wary of walnut scrubs, you should be wary of any hard-particulate scrub agent that can generate sufficient friction. There is nothing inherently worrying about walnut when compared to other natural exfoliants unless you are allergic to nuts and nut products.
I think the last word has to be to plead to our sense of balance.
If, like me, you like exfoliating scrubs then use them carefully, sparingly, gently and in a way that doesn’t damage your skin or spread infection. I can see why the skin professionals hate them and I do agree that a gentle approach to skin care is most likely the best plan.
Most of us don’t know how to ‘do’ moderation but that’s not Kylie or the professionals fault, that’s ours. That said, in telling us that she uses this product (which I haven’t tested) 2-3 times a week but that you COULD use it daily to achieve a skin like hers (which is kind of perfect) is somewhat irresponsible especially given that her audience is quite young, potentially acne prone and highly susceptible to celebrity marketing messages.
So should you keep your nuts off your face?
Probably.
Amanda x
Should you keep your nuts off your face? It was hard not to be affected by the keyboard warrior backlash Kylie Jenner got last week after announcing that her new skincare line would include a walnut facial scrub.
#beauty#Cosmetic Science#exfoliation#Kylie Jenner#microdermabrasion#Realize Beauty#Scrub#skin care#Walnut Scrub
0 notes
Text
[Transcript] – Should You Or Your Kids Get Vaccinated? One Doctor’s Surprising Answer To Making The Big Decision On Vaccines.
Podcast from: https://bengreenfieldfitness.com/podcast/lifestyle-podcasts/should-kids-get-vaccinated/
[0:00:00] Podcast Intro
[0:00:55] Podcast Sponsors 1
[0:04:15] Autoimmunity and Chronic Diseases
[0:05:16] Introduction to Dr. Thomas Cowan
[0:08:15] The Kid Who Has Asthma and Numbers
[0:12:59] Coley and Coley’s toxins
Get The Low Carb Athlete - 100% Free!Eliminate fatigue and unlock the secrets of low-carb success. Sign up now for instant access to the book!<![CDATA[ #_form_64_ font-size:14px; line-height:1.6; font-family:arial, helvetica, sans-serif; margin:0; #_form_64_ * outline:0; ._form_hide display:none; visibility:hidden; ._form_show display:block; visibility:visible; #_form_64_._form-top top:0; #_form_64_._form-bottom bottom:0; #_form_64_._form-left left:0; #_form_64_._form-right right:0; #_form_64_ input[type="text"],#_form_64_ input[type="date"],#_form_64_ textarea padding:6px; height:auto; border:#979797 1px solid; border-radius:4px; color:#000 !important; font-size:13px; -webkit-box-sizing:border-box; -moz-box-sizing:border-box; box-sizing:border-box; #_form_64_ textarea resize:none; #_form_64_ ._submit -webkit-appearance:none; cursor:pointer; font-family:arial, sans-serif; font-size:14px; text-align:center; background:#eb7000 !important; border:0 !important; color:#fff !important; padding:10px !important; #_form_64_ ._close-icon cursor:pointer; background-image:url('https://d226aj4ao1t61q.cloudfront.net/esfkyjh1u_forms-close-dark.png'); background-repeat:no-repeat; background-size:14.2px 14.2px; position:absolute; display:block; top:11px; right:9px; overflow:hidden; width:16.2px; height:16.2px; #_form_64_ ._close-icon:before position:relative; #_form_64_ ._form-body margin-bottom:30px; #_form_64_ ._form-image-left width:150px; float:left; #_form_64_ ._form-content-right margin-left:164px; #_form_64_ ._form-branding color:#fff; font-size:10px; clear:both; text-align:left; margin-top:30px; font-weight:100; #_form_64_ ._form-branding ._logo display:block; width:130px; height:14px; margin-top:6px; background-image:url('https://d226aj4ao1t61q.cloudfront.net/hh9ujqgv5_aclogo_li.png'); background-size:130px auto; background-repeat:no-repeat; #_form_64_ ._form-label,#_form_64_ ._form_element ._form-label font-weight:bold; margin-bottom:5px; display:block; #_form_64_._dark ._form-branding color:#333; #_form_64_._dark ._form-branding ._logo background-image:url('https://d226aj4ao1t61q.cloudfront.net/jftq2c8s_aclogo_dk.png'); #_form_64_ ._form_element position:relative; margin-bottom:10px; font-size:0; max-width:100%; #_form_64_ ._form_element * font-size:14px; #_form_64_ ._form_element._clear clear:both; width:100%; float:none; #_form_64_ ._form_element._clear:after clear:left; #_form_64_ ._form_element input[type="text"],#_form_64_ ._form_element input[type="date"],#_form_64_ ._form_element select,#_form_64_ ._form_element textarea:not(.g-recaptcha-response) display:block; width:100%; -webkit-box-sizing:border-box; -moz-box-sizing:border-box; box-sizing:border-box; #_form_64_ ._field-wrapper position:relative; #_form_64_ ._inline-style float:left; #_form_64_ ._inline-style input[type="text"] width:150px; #_form_64_ ._inline-style:not(._clear) + ._inline-style:not(._clear) margin-left:20px; #_form_64_ ._form_element img._form-image max-width:100%; #_form_64_ ._clear-element clear:left; #_form_64_ ._full_width width:100%; #_form_64_ ._form_full_field display:block; width:100%; margin-bottom:10px; #_form_64_ input[type="text"]._has_error,#_form_64_ textarea._has_error border:#f37c7b 1px solid; #_form_64_ input[type="checkbox"]._has_error outline:#f37c7b 1px solid; #_form_64_ ._error display:block; position:absolute; font-size:13px; z-index:10000001; #_form_64_ ._error._above padding-bottom:4px; top:-41px; right:0; #_form_64_ ._error._below padding-top:4px; top:100%; right:0; #_form_64_ ._error._above ._error-arrow bottom:0; right:15px; border-left:5px solid transparent; border-right:5px solid transparent; border-top:5px solid #f37c7b; #_form_64_ ._error._below ._error-arrow top:0; right:15px; border-left:5px solid transparent; border-right:5px solid transparent; border-bottom:5px solid #f37c7b; #_form_64_ ._error-inner padding:8px 12px; background-color:#f37c7b; font-size:13px; font-family:arial, sans-serif; color:#fff; text-align:center; text-decoration:none; -webkit-border-radius:4px; -moz-border-radius:4px; border-radius:4px; #_form_64_ ._error-inner._form_error margin-bottom:5px; text-align:left; #_form_64_ ._button-wrapper ._error-inner._form_error position:static; #_form_64_ ._error-inner._no_arrow margin-bottom:10px; #_form_64_ ._error-arrow position:absolute; width:0; height:0; #_form_64_ ._error-html margin-bottom:10px; .pika-single z-index:10000001 !important; @media all and (min-width:320px) and (max-width:667px) ::-webkit-scrollbar display:none; #_form_64_ margin:0; width:100%; min-width:100%; max-width:100%; box-sizing:border-box; #_form_64_ * -webkit-box-sizing:border-box; -moz-box-sizing:border-box; box-sizing:border-box; font-size:1em; #_form_64_ ._form-content margin:0; width:100%; #_form_64_ ._form-inner display:block; min-width:100%; #_form_64_ ._form-title,#_form_64_ ._inline-style margin-top:0; margin-right:0; margin-left:0; #_form_64_ ._form-title font-size:1.2em; #_form_64_ ._form_element margin:0 0 20px; padding:0; width:100%; #_form_64_ ._form-element,#_form_64_ ._inline-style,#_form_64_ input[type="text"],#_form_64_ label,#_form_64_ p,#_form_64_ textarea:not(.g-recaptcha-response) float:none; display:block; width:100%; #_form_64_ ._row._checkbox-radio label display:inline; #_form_64_ ._row,#_form_64_ p,#_form_64_ label margin-bottom:0.7em; width:100%; #_form_64_ ._row input[type="checkbox"],#_form_64_ ._row input[type="radio"] margin:0 !important; vertical-align:middle !important; #_form_64_ ._row input[type="checkbox"] + span label display:inline; #_form_64_ ._row span label margin:0 !important; width:initial !important; vertical-align:middle !important; #_form_64_ ._form-image max-width:100%; height:auto !important; #_form_64_ input[type="text"] padding-left:10px; padding-right:10px; font-size:16px; line-height:1.3em; -webkit-appearance:none; #_form_64_ input[type="radio"],#_form_64_ input[type="checkbox"] display:inline-block; width:1.3em; height:1.3em; font-size:1em; margin:0 0.3em 0 0; vertical-align:baseline; #_form_64_ button[type="submit"] padding:20px; font-size:1.5em; #_form_64_ ._inline-style margin:20px 0 0 !important; #_form_64_ position:relative; text-align:left; margin:0px 0px; padding:20px; -webkit-box-sizing:border-box; -moz-box-sizing:border-box; box-sizing:border-box; *zoom:1; background:transparent !important; border:0px solid #b0b0b0 !important; width:300px; -moz-border-radius:0px !important; -webkit-border-radius:0px !important; border-radius:0px !important; color:#000 !important; #_form_64_ ._form-title font-size:22px; line-height:22px; font-weight:600; margin-bottom:0; #_form_64_:before,#_form_64_:after content:" "; display:table; #_form_64_:after clear:both; #_form_64_._inline-style width:auto; display:inline-block; #_form_64_._inline-style input[type="text"],#_form_64_._inline-style input[type="date"] padding:10px 12px; #_form_64_._inline-style button._inline-style position:relative; top:27px; #_form_64_._inline-style p margin:0; #_form_64_._inline-style ._button-wrapper position:relative; margin:27px 12.5px 0 20px; #_form_64_ ._form-thank-you position:relative; left:0; right:0; text-align:center; font-size:18px; @media all and (min-width:320px) and (max-width:667px) #_form_64_._inline-form._inline-style ._inline-style._button-wrapper margin-top:20px !important; margin-left:0 !important; #_form_64_ ._form_10 text-align:center !important; #_form_64_ ._x20518276 label,#_form_64_ ._field10 label text-align:left; #_form_64_ ._form_31 width:100% !important; ]]>
[0:21:25] How does the Immune System Work?
[0:28:34] Podcast Sponsors 2
[0:31:34] Getting Vaccinated
[0:34:00] Rethinking Cell Biology
[0:37:00] Gary Ling’s Criticisms
[0:42:54] Why Do We Get Sick?
[0:48:40] Dr. Cowan’s Protocol
[0:51:30] Overcoming the Effects of Vaccinations
[0:53:50] Low-dose Naltrexone
[1:00:04] How Colostrum Helps
[1:01:06] Dr. Cowan’s Organ Preparations
[1:04:32] Rudolf Steiner’s Cosmology of Our Development
[1:11:13] What Do You Do with Your Kids?
[1:12:24] Closing Remarks
[1:14:42] End of Podcast
Ben: I have a master’s degree in physiology, biomechanics and human nutrition. I’ve spent the past two decades competing in some of the most masochistic events on the planet from SEALFit Kokoro, Spartan Agoge and the world’s toughest mudder, the 13 Ironman triathlons, brutal bow hunts, adventure races, spearfishing, plant foraging, free diving, bodybuilding and beyond. I combine this intense time in the trenches with a blend of ancestral wisdom and modern science, search the globe for the world’s top experts and performance, fat loss, recovery, gut hormones, brain, beauty, and brawn to deliver you this podcast. Everything you need to know to live an adventurous, joyful, and fulfilling life. My name is Ben Greenfield. Enjoy the ride.
So, I have this crazy habit that when my wife makes bone broth at home, I actually take all the bones after they’ve been in the crock-pot and I keep them in there for another day. And then, I take them out of the crock-pot and I put them in this Cast Iron Skillet and I cover them with olive oil and salt and black pepper and turmeric, and I put a little bit yoghurt on them. I know this sounds gross but I eat the bones. They just melt in your mouth and I suck the marrow out and I feel like a man. I get all of the critical vitamins and amino acids and collagen that you get from animal bones and connective tissues.
But, if you don’t want to go to all of that trouble and you still want organic grass-fed bone simmered bone broth that’s been simmered for over 20 hours and then sealed into these special cartons without any preservatives mixed with a whole bunch of organic vegetable extract, then you should get Kettle & Fire bone broth. It is certified gluten-free, Whole30 Approved, whatever that means, non-GMO. It’s paleo-friendly. It’s got all the body-loving goodness you want and nothing you don’t. And they actually make this super simple. They got chicken, they got beef, they’ve got one with like nootropic mushrooms in it.
Kettle & Fire is really good bone broth. My wife actually has a whole carton every single day, like we make bone broth at home but then she takes it to the next level. She drinks an entire carton of Kettle & Fire bone broth every day. None of you have seen my wife lately but she’s hot. That’s why, because she drinks bone broth every day. So, if you want to be hot like my wife, drink bone broth every day. Anyway, so you get 15% off of anything that the good folks at Kettle & Fire make. Very simple. You go to kettleandfire.com/ben. That automatically gives you 15% off. You could use coupon code BEN but I think if you go to kettleandfire.com/ben, it’ll automatically save you.
I also wanted to tell you about a really good one-two combo for muscle building or muscle maintenance. I know a lot of you are interested in this and this is something I’ve been doing a lot more of these days. It’s like rocket fuel before workout. You take creatine. And creatine, if you take it the right way in the right form like a good pure creatine supplement and you blend that with a little bit of water, and then the second component I’ll tell you about in little bit, it actually gives you a huge shot in the arm for any workout, and it’s really great again for mass building and muscle maintenance as well.
Well, what I’ve been doing is stirring in a scoop of the cool lime Kion Aminos into the Thorne Creatine. This is a really good pre-workout that also still allows you to simulate a fasted state while you’re working out. So, you get that growth hormone and testosterone response. You can find the Thorne Creatine at 10% off and the Kion Aminos at 10% off right now if you just go to getKion.com. There’s a whole bunch of supplements over there but the two for muscle building I really like right now. It makes the aminos with the creatine. So, all of that, the automatic discount included, is over at getKion.com. That’s getK-I-O-N.com.
Over the past 50 years, the rates of autoimmunity and chronic diseases have exploded. A ton of kids has allergies. As you’re no doubt aware, 1 in 11 has asthma, 1 in 13 has food allergies, 1 in 36 has autism, and then there are all these other things that are autoimmune related conditions that even adults have like acne and eczema and joint pain and thyroid issues and leaky gut. Many people will attribute this rise and all these autoimmune conditions to simple, increased awareness and more diagnosis because we’re aware of these issues, kind of similar to how more and more, especially young boys these days are diagnosed with ADD and ADHD. I don’t know if it’s a growing epidemic of ADD and ADHD as much as it is that people are just creating names for diseases that boys just naturally grow up with.
But there’s definitely something going on when it comes to autoimmunity. My guest on today’s show, Dr. Thomas Cowan, who has been a guest on this show multiple times–this is his fifth appearance, I believe, fourth or fifth appearance on my show. Usually, when someone appears on my show that much, it’s because anytime they release a book or anytime that they write an article, I pay attention because they’re forward-thinking people who are far ahead of the curve when it comes to medicine and Dr. Cowan definitely falls into that category.
Case in point, he has a new book. It’s called “Vaccines, Autoimmunity, and the Changing Nature of Childhood Illness.” He actually highlights how there’s a direct causal relationship to the increase in the number of vaccines that kids get and autoimmune diseases, provocation of the immune response. The book is fantastic. I have a bunch of stuff underlined that I wanted to ask Dr. Cowan. So, here he is on the show with us. Just fun fact for you guys, if you heard me on the Joe Rogan podcast where I was talking about why the heart is not a pump and Joe definitely raised an eyebrow on me when I was trying to explain that, Dr. Thomas Cowan actually wrote the book that describes all of that to you in detail. It’s called, “Human Heart, Cosmic Heart.”
So, that’s a good one to read as are all of his books, frankly. I’ll link to all of them in the show notes. But Dr. Cowan, welcome back to the show, man. It’s old hat for you. You’re almost like a podcast sidekick now.
Thomas: That’s right. Well, it’s always a pleasure to talk to you, Ben.
Ben: Yeah. Yeah. You’re always a wealth of knowledge, man. I enjoy the occasional meals we get to have together at the Weston A. Price Conference when I can make it over there. You’re a good guy to eat grass-fed butter and lard with.
Thomas: Yeah. And I appreciate all your support through the years.
Ben: Yeah. And one thing I neglected to mention, by the way, for those of you who may not be familiar with this part of Dr. Cowan’s life is he makes these fantastic vegetable powders that me and my family use on all of our sautés, in our stews. They’re all based on this idea that Dr. Cowan and I delved into when he was on my podcast called How to Eat More Vegetables, about these organic heirloom vegetables and threefold blend powders and dark turmeric and kale and leek powders that he actually makes and packages in the Miron glass jars and ships all over the US.
I’ll link to that stuff in the show notes as well. So, everything that we talk about today, you can find over at BenGreenfieldFitness.com/autoimmunity. That’s BenGreenfieldFitness.com/autoimmunity because that is indeed the topic of the day. And I think a perfect point for us to start, Dr. Cowan, would be this story that you tell about when you were growing up in the ’60s and how there was a kid you knew who had asthma. Can you get into that story?
Thomas: The point of that story was–and people who have–old people around in their lives like me or grandparents or parents, if you ask them, how many children did you know growing up with food allergies and peanut allergies and asthma and eczema, childhood cancer and juvenile rheumatoid arthritis and on and on and on? What I remember was one child in our whole elementary school. And it isn’t like we were the paragons of healthy eating. We ate frozen food, and basically, crap. But still, there was only one child I remember because as I said in the book, he was teased, although I would add, not by me. That’s just not my style, I guess, teasing other people. But he was teased and he was teased because it was like, “How dare you be sick?”
Now, if you’ve fast forward from that ’til 2016, 2017 or now, I’ve heard statistics that Detroit Public Schools, which is where I grew up, something like 40% of the children carry an inhaler to school. So, maybe they’re teasing the so-called normal people now.
Ben: Seriously.
Thomas: Like, “What’s wrong with you? You don’t have any medicine to take.” So, the whole situation has changed. You can’t go to a ballgame and eat peanuts. You can’t go to a birthday party everybody has food allergies. I don’t know the percentage. The CDC came out with a 46% of current American children have a diagnosed chronic disease that needs at least intermittent medication.
Ben: And adults. I went to dinner the other night. I was in–where was I? I was in Chicago. I went to this fantastic Italian restaurant. I was with about 20 people. And when the waiter came out and asked if we had food allergies or sensitivities, freaking half the hands in the room shot up and this person was like, “I’m not eating gluten,” and this person says, “I have a sensitivity in lactose.” And I realized that part of that is the nature of just having dinner with, as I often do, people who are intensely aware of health. But there is an increasing number of adults who have an enormous number of allergies and skin conditions and all manner of things that frankly are autoimmune issues. Thyroid is another big one. But you’re right. We didn’t see a lot of this and I don’t know if you have any stats, because I mentioned earlier that a lot of people do say that this is just increased diagnosis, increased awareness of the condition. But do you have anything to say to that argument?
Thomas: Well, I mean even if you actually believe the CDC and the Health and Human Services’ numbers, they say it was about 6% of the childhood population had a diagnosed chronic disease in 1980 and it’s now 46%. So, that’s one way to look at it. Another way and one of the diseases that is now being questioned, whether there’s an actual increase or whether it’s all about diagnosis, is of course autism. So, now, there’s a whole movement to say that autism is normal and we just diagnose it more. But the problem with that is–I’ve spent a lot of my life around autistic people because I worked at camps and I was in anthroposophical doctor working with Camphill Villages where there are a lot of autistic people. Something like 75% of people with a diagnosis of autism ends up being institutionalized. And I don’t know about you, Ben, but if I think how many 60/70-year-olds do I know with autism and how many institutions there are for autistic people who are in their 50s, 60s and 70s, it’s basically zero. So, where are they all? If they were just as many autistic people 50 years ago as there are now, we would expect a million autistic adults that are institutionalized and we see almost none.
Ben: You tell another story in the book that I think is perfect for kind of beginning to delve into the changing nature of childhood illness and autoimmune and vaccines, and that’s the story of this guy named William Coley. I hadn’t really heard of this dude before ’til I read your book. But can you go into Coley and Coley’s toxins?
Thomas: So, when I was first becoming a doctor, and at that time, I was learning about anthroposophical medicine, I would say if you wanted to encapsulate the entirety of the medical philosophy, it’s of course complicated. But it goes back to Paracelsus who sometimes considered the Father of Medicine saying, “Give me a medicine to produce a fever and I can cure any disease.” So, the example that you gave of William Coley is a perfect example of that. So, here was a guy who was a trained oncology surgeon specializing in a kind of cancer, which is a bone cancer called osteosarcoma, which is a very aggressive and deadly form of cancer, and he was actually working at Sloan Kettering Hospital in New York. He was working under the tutelage of a guy named Ewing for whom Ewing sarcoma is named after. So, Ewing is as big as it gets in the history of sarcoma. So, he was the state of the art in 1910/1920 treating sarcomas. At one point then, he has John Rockefeller’s “friend” who came to him with a sarcoma and he did the usual treatment which was amputation and then she died 68 weeks later. That was an important patient for him probably for all kinds of reasons and it just apparently very discouraged him. And so, he decided to look through the records of the hospital to see where this sarcoma center of the world, how are we doing with treating sarcoma. And, his answer was basically, dismally.
Now, there was one exception in the records this dockworker guy named, Stein, who–all it said in the notes was, “Discharged free of disease.” So, Coley had the good sense to go and track this guy down, this was nine or so years later, and he said, “What happened to you?” He said, “Well, they never did do the surgery or any other treatment because while I was in the hospital, I got this disease called erysipelas, which is a very bad strep infection of the skin, which typically causes very high fevers. And I had a fever for a month at which time the sarcoma was gone and never came back.”
So, again, a lot of doctors would hear that and say, “Well, that’s anecdotal and I don’t have to pay any attention to that” or “I don’t know what happened.” But there was a movement all over the world at the time of treating cancer with fever therapy. Coley knew about this so he decided to give all his sarcoma patients erysipelas because he knew the usual way they treated them wasn’t working, and he ended up saying that approximately 40% of the people who got erysipelas got better after a month of high fevers. 40% died of the erysipelas, this was in the pre-antibiotic era, and 20% interestingly, no matter what he did, never would get erysipelas and then they would just die of their sarcoma.
That’s in some ways a great result because 40% of incurable cancer patients got better far better than anything we can do now. But it’s also had a high risk because 40% died of this infection. So, that’s a high mortality rate. So, he said, “Well, maybe I don’t need the infection. Maybe I just need the fever.” So, he figured out how to use attenuated, essentially non-infective bacteria in just a certain part of them that would provoke a fever without actually giving them an infection. That’s what became Coley’s toxins. It was the main adjunctive treatment for cancer for the next 30 or 40 years.
Ben: And it was just causing people to get fevers that somehow were killing off the cancer.
Thomas: Exactly. Now interestingly, when I became a doctor, I was contacted by his granddaughter, a woman named William Coley Nauts, who gave me this manuscript. It had never been published. There was, I don’t know, thousands of pages with all of case studies that Coley treated. I went through them all and there were literally hundreds, thousands of people who were cured. And by this time, he was not causing infection because he was not using live bacteria. It wasn’t 100% but it was a huge success. I was looking at this and then I saw some articles that Sloan Kettering was developing an immune therapy program where they would take the chemicals that are made when you have an infection and they would give them to cancer patients to see if they could stimulate their immune response and get rid of their cancer.
Now, the amazing thing about this–and they isolated something called tumor necrosis factor and they would give this. And then you inject somebody with tumor necrosis factor and you get a fever. Shockingly to me, they would give them Tylenol to bring the fever down and then the whole thing wouldn’t work and they said, “Well, I guess immune therapy doesn’t work.”
The bottom line was it’s not the tumor necrosis factor or the interferon or the interleukin themselves that are a positive effect to the therapy. It’s like Hippocrates said, “Give me a medicine to produce a fever and I can cure any disease.” You have to have the fever as unpleasant as it may be and you have to have it to 105 degrees or so for a month, and that causes no problems in itself. But unfortunately, since the ’60s, Coley’s toxins have been outlawed in the United States. That whole approach is unavailable.
Ben: Why were they outlawed?
Thomas: I don’t know. I mean, they said it was an unproven therapy and I think it was basically pennies and they just didn’t want it.
Ben: But you don’t really need Coley’s toxins if you have a child that is allowed to actually get sick so that the normal–I believe it’s called the–is it the humoral immune system is able to actually kick in and be trained in the right way?
Thomas: Well, it’s the cell-mediated. Literally back then, since that day, every single time I’ve seen a child, a sick child in my practice with a fever, I literally think to myself, “I am preemptively treating their cancer to be.” In other words, if I can get them through somehow this febrile illness without suppressing the fever, then I know that I have just, literally for their entire life, pushed them in a direction away from cancer. That’s why I’m doing that. If it takes a day of a fever, that’s good. If it takes a week of a fever, that’s fine. My job is to somehow help them undertake this process so at the end of the day, they’re at this funny word that we say after you’re sick, “Now, I’m better,” because literally, you’re better than what you were when you started.
Ben: So, what are the types of conditions that a kid would get when they’re young that would allow that proper cell-mediated immune response to kick in so that the body is able to mount its normal immune response, get a fever, and then remember that specific antibody or toxin or sickness so that the person doesn’t get it again?
Thomas: Right. So, maybe we should just go through that for a minute, if that’s okay, just to put that in context?
Ben: You mean like how that immune system is actually working?
Thomas: Yeah.
Ben: Yeah. I think that would be valuable because I think a lot of people don’t really even understand that there are two main branches of the immune system that we’re talking about here.
Thomas: Right. So, here’s the way it works. Let’s just take in like a measles infection. So, if you’re a child and you’ve never been exposed to measles and you get exposed to this virus and it gets in and it gets inside your cells, probably millions of them or certainly thousands, and your body is now looking at these infected cells, so the first thing it does is it mounts a cell-mediated, meaning it’s based in the white blood cells, response that’s whose job it is is to essentially attack and digest these infected cells and then clear them out of the body. Now, it does this through the mechanism of fever and rash and mucus and cough and diarrhea, and all the things that we call being sick. And if there’s anything people will remember from hearing me or reading my book, it’s that that which we call being sick, fever, rash, cough, all that, that’s not the virus. It’s not the measles virus, it’s your cell-mediated immune system essentially eliminating the virus. Now, the virus provoked the cell-mediated response but the actual symptoms are from the cell-mediated response getting rid of the infected cells.
Ben: Right. The rhythm of your body.
Thomas: Yes. I know that because if you inhibit your cell-mediated response, you can infect people and even kill them and they’ll never be “sick.” Sick means your cell-mediated response is working.
Ben: Wait, wait. What do you mean you could infect people and kill them and they wouldn’t get sick?
Thomas: So, if you give people a measles infection and then give them prednisone so that they don’t have a fever or a rash, the infection will continue and it could even kill them but your body has been thwarted in its attempt to get rid of it and that’s a dangerous situation. You don’t want to stop your body from using its natural mechanisms to clear the infected cells. That’s a bad strategy. Now, once that happens, it usually takes seven to ten days, and then you’re back to normal. The body in its evolutionary wisdom says, “I don’t want to do this over and over again. So, I’m going to tag one of the pieces of the measles virus and make antibodies against it, that’s the humoral or antibody arm of the immune system so that if I ever encounter that virus again, I can keep it from infecting my cells without getting my cell-mediated immune system involved.” And because the humoral antibody immune system is not associated with symptoms, you don’t know anything’s happening. You never get sick again from that virus. And when those two things happen in that sequence, infection, cell-mediated clears it, antibodies remember it. It’s unbelievably almost 100% foolproof nobody ever gets measles twice in their life.
Ben: So, you’re saying we should just let kids get measles and let measles run its course?
Thomas: Well, I’ll get to that.
Ben: Okay.
Thomas: But at this point, I want to point out that that’s the way our immune system always worked until about 50 years ago. The theory of vaccines is–well, the cell-mediated part is the sickness part. We don’t want the sickness part. So, we’re just going to take a piece of that measles virus or kill it or so-called attenuate it, and we’re going to stimulate you to make antibodies. Sometimes we actually have to give you, essentially, toxins to make you make antibodies. So, we’re going to embark on an antibody-only strategy. That’s the theory of the vaccine. No more cell-mediated immune system, only antibodies. And so, that’s what they do. They give you pieces of the virus or pieces of toxins or killed viruses and then they have to mix it with things like aluminum and formaldehyde and mercury and fetal DNA cells and glyphosate and all kinds of things to make you make antibodies. And it works. So, now you have people who’ve skipped the cell-mediated part and have an accelerated antibody response.
Now, I would point out two things about that strategy. In number one, there is zero possibility of getting lifelong immunity through an antibody-only strategy. And for people who don’t believe me, it’s simply the reason why every vaccine has to have boosters because the immunity that you get, when you only stimulate the antibody part, the first time lasts seven to ten years, the subsequent boosters last two to three years. So, when you’re 30 or 25, you no longer have antibodies. You’re just as susceptible to it as when you were a newborn baby.
The second thing I would point out about an antibody-only strategy is just like you eloquently talked about the rise in autoimmune disease. An autoimmune disease is defined as the situation of accelerated antibodies that are targeting your own tissues. So, if you ask the question, how did we end up with like what Yehuda Shoenfeld says 150 million people who have autoimmune disease. Well, an autoimmune disease meaning too many antibodies. This is maybe a funny way to say it but that’s the whole point of the vaccine program. So, it worked.
Ben: Hey, I want to interrupt today’s show to tell you why my face is as smooth as a baby’s bottom. It’s because I use these blades that are made by a company called Harry’s. Harry’s bought a German-engineered factory that’s been making some of the highest quality blades for shaving, I don’t know what else you’d use blades for, in the entire world. For over 95 years, this factory has been making these blades. Harry bought them and they started churning out these five blade razors with a lubricating strip, and also this weighted ergonomic handle. It’s like the Cadillac of razors. They have these wonderful paraben and phthalate-free, rich lathering shave gels. They have a really great travel blade cover so these blades stay in fantastic shape if you’re on the road. And they have all this put together in a really great kit. They call it their trial set. So, you get travel blade cover, you get the shave gel, you get the five-blade razor with the lubricating strip and the trimmer blade, you get the weighted ergonomic handle and all of that you can actually get. It’s a $13 value but you can get it for free if you just go to harrys.com/greenfield. That’s harrys.com/greenfield. You’ll automatically get the entire kit for free. This makes shaving a breeze. I mean, the hair just literally almost falls off. I used to use Nair when I was a bodybuilder but this is probably a way healthier way to actually get a nice close, close shave for men or for women, because women like to shave their legs and some women like to shave their face, too. Some women need to do that, believe it or not.
This podcast is also brought to you by Zip Recruiter. Zip Recruiter makes hiring a breeze, kind of like Harry’s was making shaving a breeze. You see all this stuff is about making your life easier. What they do is you post a job on Zip Recruiter. They do all the work for you. They spot like the strongest applicants. They collect all the information. They identify the people with the right experience. They invite them to apply to your job. They’re like this freakishly smart online software that allows you to get hooked up with the right candidate, literally, in a day. Eighty percent of the employers who post a job on Zip Recruiter get a quality candidate through the site in just one day. It’s that easy. No more piles of resumes on your desk and spending all your life on LinkedIn, stalking people, which is awkward because a lot of times, they could see if you viewed their profile and you got to have an incognito browser and all of that. No, you don’t even need to do it. You just go to ziprecruiter.com/green. That’s ziprecruiter.com/green. And when you do that, you get to try Zip Recruiter for absolutely free. That’s right, free. Zip Recruiter. There’s a reason they call it the smartest way to hire. So, you get to try it for free, ziprecruiter.com/green.
So, the problem is though that all of these people who get that humoral system stimulated early in life from the vaccines never get a chance to actually get sick from that particular illness and mount a natural immune response to that illness that then causes the body to remember that illness and not get it again.
Thomas: Correct. And there have been study after study showing that children who get chickenpox have less glioblastoma, kind of brain cancer. Children who get measles have less osteoarthritis, have less arteriosclerosis, have less heart disease, have less dementia. There’s study after study showing that children who get febrile childhood disease have less chronic disease later in life, period. Anybody who doesn’t know that just simply doesn’t know the history of medicine or the current literature on the relationship of childhood illness and chronic disease.
The other thing I would point out is that when people say, “Well, it’s fine to not go through these illnesses.” The fact of the matter is I happen to know the exact date the CDC says anybody born in 1956 or before is considered immune to measles. That happens to be the year I was born. So, anybody, 62 or older, by definition had measles. So, we have no idea whether a human being can actually get to be 65 who didn’t have measles when they were a child because there’s nobody like that. Could be it’s fine, could be it’s not fine. We don’t know.
Ben: So, when it comes to the whole idea behind vaccines and actual cellular function, there’s a section in your book that kind of blew my mind because everything I learned in exercise physiology and a lot of my coursework at University of Idaho seems to be relatively incomplete, specifically when it comes to cell biology and the cell membrane. I realize that this might sound completely separate from any consideration of autoimmune or vaccination but I think you can probably pretty elegantly weave this into this discussion because you have a whole chapter in the book about why we need to rethink cell biology. We’ve got time to unpack this but can you get into what we currently believe about cell membranes or what medicine and science currently believes is the way that a cell operates and why that could be a flawed pattern of thinking?
Thomas: The basic premise of cell biology all came from trying to understand the central paradox of mammalian including human cells which is, “How does a cell live in a sodium-rich environment yet has a sodium-poor internal milieu?” Now, that may sound like a mouthful but if you put a cell in a high salt concentration, it will equilibrate and the sodium will be balanced on either side. But that’s clearly not the case with any mammalian cell. The sodium stays on the outside, the potassium collects on the inside, and this causes a separation of charges which is fundamental to allowing the cell to be a charged entity like a battery that can actually do work. So, if you lose the charge because you lose this separation of sodium-potassium, you’re talking about a dead cell.
Ever since–it’s literally 200 years of research into how the cell accomplishes that. Nobel Prizes were given and the answer is you have this cell which is a membrane-bound sac of water and it has a pump in the membrane which pumps the sodium out and the potassium in. And that’s how it happens. And here’s the pump and we studied it and we’ve got our prizes for it.
Ben: I remember the little spheres in my textbooks in college showing the NA and the K moving in and out of the cell membrane based on that sodium-potassium pump.
Thomas: Right. And that creates the charge of the cell. It’s the most fundamental part of cell biology you could imagine. Now, here’s the problem with that. I have to acknowledge a guy named Gilbert Ling, who was a biologist who really spent four decades critiquing this system and showing that it’s basically baloney. The first problem is, okay, a cell is a sac of water with stuff in it. I often tell the story when I was an ER doctor and we’re told that 70% of the intracellular content is liquid water. And I would see people with bullet wounds and bayonetted and shot and all kinds of stuff. And I never saw puddle of water on the floor next to them or water squirting out of a human being. So, I asked myself, “Where is the water here?” I know there’s blood but that’s different. Supposedly, these cells are 70% water yet there’s no water in the human body. So, that’s one problem with that model.
The second problem is Ling actually ran the energetics of this sodium-potassium pump, and absolutely conclusively determined that in order to create this differential, you would need approximately 40 times the energy that a human being or the human cell has available to it just to run the pump. That’s like if you have a mortgage on your house that’s 20,000 a month and your salary is 1,000 a month, it’s not going to work. A, you’re not going to be able to pay the mortgage, and B, you’re not going to have enough money for food. You cannot run that pump given the amount of energy it takes and why he was the only one to understand that as I have no idea.
Ben: So basically, there isn’t actually enough ATP available to be responsible for the proper distribution of sodium and potassium based on the pump model.
Thomas: Exactly. The other part of that is–and I’m glad you said that because he also pointed out very clearly that unlike what seemingly everybody thinks, ATP is not the energy molecule that we think it is. There is no more energy in an ATP molecule than any other common molecule. So, the system does not run by ATP as some energy source fueling this pump pumping the potassium in and the sodium out. So, the question then is, how does it work and what does that have to do with autoimmune disease? The answer is our cells are made of this fourth phase structured water or gel water that I know you’ve got into a lot with Dr. Pollack and other people. It’s structured similarly to how Jell-O is. You take proteins, you add water, you put energy source, in the case of Jell-O, it’s heat, that unfolds the proteins, allows them to interact with water. When it cools down, it forms a gel. A hundred percent of the water in our cells is in this gel form, not a liquid form, even though people say there is no gel form but there is. And the way that it’s structured, similarly to Jell-O, is you take the intracellular proteins. The ATP interacts with the ends of the proteins and unfolds them. It allows them to interact with water to create what I call the perfect gel. The perfect gel, now think of it like it has a sort of mesh, like a mosquito netting. The mesh is so constituted so that by itself, it attaches to potassium and repels the sodium. So, there’s no pump needed. All you have to do is use ATP to unfold the protein, structure the water. That structured water by definition collects the potassium, expels the sodium, and that creates work on the cell that the cell can do and everything is good.
Ben: Yeah. That’s actually Gerald Pollack who I interviewed. And I’ll link to all of this again if you go to BenGreenfieldFitness.com/autoimmunity. He gets into how all of this fourth phase water, this so-called structured water that surrounds–would you describe that as surrounding ourselves or would you say that it is–
Thomas: No, it’s the very nature of the water in our cells.
Ben: Inside the cells.
Thomas: Inside the cells and even around DNA, in the nucleus, there’s a small amount of structured water which determines which part of the DNA will be expressed. The structured water does everything. The reason it’s water is because it has infinite binding sites, and so it can interact with thoughts, emotions, hormones, vitamins, every–
Ben: Sorry to interrupt but if you have a negative electric charge, essentially, you have almost a crystalline structure that can absorb different forms of information or energy or signals, and this relates to the whole concept of the body being a human battery, and also relates to the concept of how we’re affected by–as Bruce Lipton goes into in his book, “Biology of Belief” or Joe Dispenza outlines in his book, “You Are the Placebo,” how we can and our cells can even respond to things like energy and emotions and sound frequencies, and all manner of things that go beyond simple, I guess we would call atoms. And it can instead interact with subatomic particles and then interact with waves and vibrations as well.
Thomas: Yes. All that is because of the perfect crystalline negatively charged water gel. Now, that gets into the next thing. So, why do we get sick? And in particular, I often joke that the reason I wrote this book was because I wanted to understand for myself the sequence of events that happens to me, and I don’t think I’m the only one, when you get sick. Here’s the sequence. A, I’m fine, then I don’t feel well and I get a fever, and then, it sort of breaks down and then I get snot and then I snot out the snot and then I get better. So, why does it happen like that? Nobody ever told me, nobody ever said anything. Why that sequence of events? But here’s why.
Let’s say you have this perfect gel. So, now you’re a perfectly tuned radio and you can accept all the influences that a human being is supposed to. And then you dissolve arsenic in your gel. So, that distorts the gel. So, now you have an out-of-tune radio that can’t accept signals and you’re going down a bad path here. You can’t make an energy charge. That’s what we call being sick. So, your body says to itself, “I’ve got to get rid of that arsenic but I got it interspersed in my gel. So, what I’m going to do here is heat up the gel so it make it back into a liquid, and then I’m going to make it run out of the cells and I’m going to snot it out of my body, and then, I’m going to reconstitute a more perfect gel.” So, that’s what we do.
Ben: In a case of something like an autoimmune condition that would involve inflammation, these cells actually get into this pathological state. Is that based on some kind of an inhibition of this negative charge or the inability of water to basically move in and out of a cell?
Thomas: The way I would put it is let’s say you have like with chickenpox or measles. So, your gels are healthy, you get an infection, you clear it out, you reconstitute perfect gels, and now you’re fine. But let’s say it’s not a chickenpox virus that’s distorting your cells but aluminum being injected into your cells and that happens over and over again. So, you clear it out, you get sick, and then you get more. And then you clear it out and you get more, and at the end of the day, you end up with a distorted cell which is weak in its ability to accept impulses and it’s weak in its ability to create this charge. And now you have a chronic inflamed situation because your body is continually trying to clean itself out of whatever was put in there, but you keep putting it in there and you keep inhibiting your body from doing this housecleaning. I mean, what else would you expect to happen but you end up with chronic sickness.
Ben: It’s interesting because this is similar to our discussion of the heart in our last episode about how the heart actually pumps less than what we think, very similar to this sodium-potassium pump being possibly something that isn’t even from a pure biochemical standpoint feasible. And when we talked about the heart, you talked about how water, particularly the charges of water, allow it to move through a well-designed shape of the heart, I believe you called it a tetrahedron structure, without the heart necessarily needing to pump but rather the heart relying upon the vortices like movement of water through that structure of the heart. And in the same way that water moves through plants and the vasculature in plants, without the plants needing a heart, water and fluids can move through the human body in a similar way. And what you’ve just described is very similarly, almost like this self-sustaining system that doesn’t rely upon a lot of outside energy for accomplishing movement but in fact allows for the cell to operate, assuming a state of adequate hydration and an adequately charged body, which we’ll get into in a second, without necessarily requiring say the ATP.
Thomas: Exactly. I couldn’t put it any more succinctly. That’s exactly right. These pump models are from a–the reason we think that way is because Descartes said, “From now on, only mechanical ideas will influence how we think about the human being.” That’s why we think that.
Ben: But it’s more than just mechanics. It comes down also to electricity charges and frequencies.
Thomas: Yes, exactly. It’s more than the camps. And in fact, when you get into the mechanics, it can’t possibly be the heart pushing the blood. It mechanically doesn’t work, and similarly, it can’t possibly be this sodium-potassium pump creating this charge. The energy just doesn’t add up. There is a whole another way and that gets into a lot of things but basically, unfortunately, our biology is based on inanimate, inorganic principles. We don’t know the difference between life and death. Therefore, we can’t study life.
Ben: Now, I want to get into your whole protocol for supporting the immune system based on supporting the innate immune system response, especially in childhood rather than vaccinations. But to bring things full circle, what you were saying is when we look at aluminum and mercury or formaldehyde or any of these other chemicals or metals that are in a vaccine, what those do is they can actually insert themselves into the intracellular matrix and interfere with the actual charge generating ability of the cell itself.
Thomas: Right, or any toxin. Anytime you live in a toxic world or nutritionally depleted world, you’re going to interfere with the formation of your gels, which is how we interact with the world. That’s what collects and processes information, which, in a sense, is what a human being or a living system is. It’s an information communication device with the rest of the world. And now, we’re human beings whose radios are out of tune.
Ben: Yeah. And this is important too because this is one of the things that I explain to people when they ask me what are the top things they could do to maintain ideal health and wellness. And a lot of it comes down to supporting this natural gel matrix within the cell and the natural negative charge of the structured water in the body. That comes down to very good water intake, preferably structured water but water that has maintained its normal negative charge. I have a structured water filtration system installed in my own home. And, although I don’t get a lot of structured water when I travel, there are even ways you can bring structured water when you travel, like I have these little liquid shots called Oral IV, for example, that I can throw in my travel bag and bring with me. And then, in addition to the structured water, adequate mineral intake. I mean, we’ve got trace liquid minerals and Celtic Sea Salts and all sorts of things here at our house that my kids and my wife and I use, and then getting outside barefoot on the ground with adequate sunshine. I mean water, minerals, the earth and sunshine are–you know, before you go and buy a bunch of colostrum and liver capsules, all these things that do support the immune system, I mean you have to take care of that low-hanging fruit.
Thomas: Exactly. You just outlined exactly the plan on how to maintain healthy gels and a healthy body right there. That was it.
Ben: Now, in terms of the actual immune system itself and this idea of alternatives to vaccines, I know that you have kind of a basic autoimmune treatment protocol. I think this is important because a lot of adults, especially, have been vaccinated. A lot of adults have children or people are listening in who might even be children who have been vaccinated, I mean is it really a hopeless scenario for a lot of these folks, their humoral immune system being triggered when they were young without the innate immune system or are there things that we can do to heal the body?
Thomas: Yeah. I mean, basically, there’s no human being who’s hopeless. That is not even the way to look at it. It’s always just taking one step at a time. So, if you’re sick, these dynamics that you just talked about and that we’re talking about are in play. And so, what’s needed is to put together a cellular gel restoration program. Now, the four basic, water and sunlight and earthing and movement, that’s the basic for any plan. And then, I would say the next most basic is at some point in your life, your cell-mediated immune system will start to rear its head again and say, “Remember that I’m still here.” At that point, you have to honor it. You have to go through the illness, if you need to, have somebody who knows how to do that help you and you’ve got to let your body do its own housecleaning. Now, some of the strategies that I outlined in the book were different diets, and like you say, colostrum, and you can use vitamin C and you can do the GAPS diet, and you can use low-dose naltrexone. All these things are attempts to bring this back into balance. But the rubber hits the road, when your child eventually will get sick again because their cell-mediated immune system will say, “Now, we’re strong enough to do this and you have to squire it through. If you need help, that’s fine, so that they get to the end of the day in a better shape than when they started.”
Ben: Now, I want to actually explore a few of those things that you just brought up as far as ways to kind of heal the body and to quell this autoimmune response. One that you just mentioned was low-dose naltrexone, and it’s pretty rare that all have docs on like you who are using a lot of natural healing protocols who will mention a pharmaceutical drug like that. But what is it that you like about this low-dose naltrexone?
Thomas: So, naltrexone was originally discovered as an opiate receptor inhibitor, meaning if you took an overdose of heroin, this naltrexone inhibits the attachment of the heroin to your opiate receptors and basically will save your life within seconds. So, it’s called Narcan and it’s used in all the emergency rooms probably all over the world. So, then they started giving it to addicts, 50 milligrams a day, and that would inhibit the ability of the heroin to make you high, which I guess is good. But it also made you feel so lousy that people didn’t take it, and so it failed as an addiction drug. And that’s because when you block opiates like heroin, you’re also blocking endorphins which are endogenously produced opiates. And life without endorphins is not much fun. So, that would have been the end of it except there was a number of doctors, a guy named Bihari, in particular, who said, “These people with autoimmune disease, they have a low endorphin state. That’s why they feel so lousy. So, if I can improve their endorphins, I can make them feel better and their whole immune system will function better.” So, he ended up giving them very small doses of naltrexone which essentially tricks your body into making endorphins, and that rebalances your immune system. It lowers the humoral, it stimulates cell-mediated immunity, and that can make an unbelievable difference for people suffering from autoimmune disease. I have cases in the book of people with Graves’ disease, people with pemphigus. I’ve got story after story of people who do all those things that you say plus eating low-antigen diets so they’re not overreacting, like paleo or GAPS or something like that, and take low-dose naltrexone and they finally get a rebalancing of their immune system, and if we’re lucky, an actual remission of their autoimmune disease.
Ben: Now, I know that that’s something that you would normally have prescribed by a physician but it is LDN. Is low-dose naltrexone something that one could buy online?
Thomas: There is a pharmacy out of Israel. I don’t remember the name of it but you can actually buy it although it takes a little bit of expertise to get the dose right. So, it would be best to work with somebody who uses low-dose naltrexone regularly. I was going to say you’re right. It’s the only pharmaceutical medicine in a typical month that I actually use.
Ben: My friend Grace Liu, who I worked with when I was healing my gut a couple of years ago, uses that and also mistletoe as a very similar treatment that apparently works quite well along with LDN for not just gut issues that come along with autoimmune disease but also a lot of the inflammation that comes along with that. Have you ever done much with mistletoe?
Thomas: I’ve done a lot with mistletoe. Mistletoe is basically Rudolf Steiner’s fever therapy. It’s like Coley’s toxins in a shot and it stimulates the cell-mediated immune system. So, fever is not the only way but there’s also hyperthermia. People have come up with various ways of cleaning the gels and stimulating–Steiner called it the etheric body or the water body which is sort of the same thing. And when Steiner was asked what does mistletoe do, he said, “It simulates a bacterial infection.” In other words, Coley’s toxins in injection form.
Ben: Interesting. Okay. So, you’ve got LDN and mistletoe as two things for people to look into who are experiencing autoimmune issues. And then another one that you mentioned, and I’ve had this guy in the show before, is this lignite stuff. Are you recommending lignite as something one would use short-term or is that just something based on glyphosate exposure that you have patients just taking almost like a daily multivitamin?
Thomas: Right. And that comes because there’s a number of ways to get into this autoimmune situation, meaning you have too many antibodies and you’re reacting to yourself. The too many antibodies is often and largely a consequence of vaccines but it’s also a consequence of absorbing antigens which are proteins from your gut, and then your body has to react against them by making antibodies. So, if you can seal the pores in your gut, then you will be less exposed to antigen so, therefore, make less antibodies, therefore, have less autoimmune disease. And this stuff that you mentioned called Restore is one of the ways and maybe the best way that I know of to seal the gut. So, I use it with people with autoimmune disease and gut issues until they’re clear of it, basically.
Ben: Yeah. You just take a shot like about a half hour before you eat a meal, right?
Thomas: Yeah.
Ben: Okay.
Thomas: Exactly.
Ben: Got it. And then another one that seems to act similarly in terms of tight junctions in the stomach and lowering the activity of this zonulin protein that seems to be able to open these tight junctions and cause more of this autoimmune food allergy, food intolerance, other inflammatory conditions, is colostrum. So, colostrum is another one that I’ve talked about before on the show quite a bit, but in terms of that, are you also recommending that for both children and adults who are having autoimmune issues?
Thomas: Yeah. I mean colostrum, again, one of the ways you get into this autoimmune disease is because you’re absorbing antigens from the gut, and that’s because you have a disordered gut flora and too much zonulin and the pores are too open. So, what colostrum does is it’s basically the first milk that’s there to stimulate the implantation of the healthy gut flora. So, if you give that to a person and give them a diet that includes fermented foods and maybe probiotics if needed, then you encourage the implantation of healthy gut flora that prevents leakage into the bloodstream and that helps the autoimmune disease.
Ben: Okay. Got it. And then the last one I want to talk to you about was these organ preparations that you use. What are those?
Thomas: So, one of the reasons why autoimmune disease, let’s take say Hashimoto’s, becomes chronic is–so you stimulate antibodies. You have these antigens stimulating antibodies. You have these adjuvants in vaccines stimulating antibodies. One of the antibodies cross-reacts with say your thyroid and it causes an inflammatory reaction in your thyroid, which means it puts out proteins from the thyroid into the bloodstream. Now, that, of course, makes your body make more antibodies to these antigens floating in your bloodstream. And so those antibodies then cross-react with your thyroid, create an inflammation, more antigens in the bloodstream, more antibodies, more inflammation, and that’s why it becomes a chronic situation. So, in order to break that cycle, the organ that you’re attacking, so in this case the thyroid, if you eat a desiccated thyroid from a grass-fed cow, the hope is that your body’s antibodies will go after the thyroid that you just ingested and leave your own thyroid alone. This has been used in the Brigham and Women’s Hospital for about 40 years. They call it oral tolerance therapy because many of the antibodies are made in the Peyer’s patches around your gut. So, if you eat what cartilage then your antibodies attack that, leave your own thyroid alone, that your thyroid can heal and that breaks the cycle.
Ben: Now, these types of glandulars, are these similar to something like low-dose naltrexone that you would need to get a prescription for or are these the same type of things you could find, say on Amazon when you go there and you see like grass-fed desiccated beef organs and desiccated liver? And I know NOW Foods is one brand that’s recommended as far as like a good safe source of liver extract. Are these the type of things that people can use just in order on their own?
Thomas: Yes. They’re similar. I mean, I use the ones mostly from Allergy Research because they seem like they’ve tested them and they worked with a friend of mine named, Nick Gonzalez, who basically directed them how to do it, whether they’re so much better than any other one, I don’t really know.
Ben: Yeah. But even the Allergy Research stuff, you can order that off Amazon, right?
Thomas: Yeah, right. It’s not going to hurt you, so that’s fine. I mean, it’s always good to work with somebody who’s done this before but I’m not saying it’s imperative. It’s certainly imperative if you’re having a horrible time with rheumatoid arthritis or Graves’ disease. I wouldn’t want somebody doing that on their own.
Ben: Okay. Alright. Now, I want to come full circle and I will of course link to Dr. Cowan’s book for those of you who want to delve into his autoimmune protocol even more deeply and some of the dosages and uses of some of the things we talked about like colostrum and LDN and some of these organ extracts. But one of the things that I find fascinating that I didn’t have a chance to ask you yet is this idea behind Rudolf Steiner, somebody who you mentioned earlier, and the fact that there are actual identified developmental stages that a normal, healthy human child should be almost like allowed to go through. And he has kind of outlined these different stages of life where you’re supposed to get sick, you’re supposed to get some of these diseases that we’re trying to eradicate. Can you explain what that, I believe he calls it the cosmology of our development would be in respect to that?
Thomas: Normal science and normal medicine says we have a body, meaning a physical body and there’s nothing else to a human being but them. That’s the way we’re taught. Now, that’s why even why sometimes I bristle at saying even the word science because–I mean, there’s no doubt everybody wants to get the truth and do that as carefully as possible. But if the definition of science is the belief that only material stuff exists in the universe, I’m not sure I can agree with that. Or let me put it another way, I don’t agree with that because what about like love that I don’t know anybody who can measure love and yet everybody knows it exists.
Now, Steiner took that into a more, I would say particular or scientific way, and it’s hard to know how he got these things but let’s just say whatever method he used–and he said, “Well, we not only have a physical body but we have three other bodies, one is a water body and one is an air body and one is a warmth body. He gave them different names like etheric body and astral body and ego, but that’s what he meant. And he said, “Just like the physical body gets born, the etheric body or water body gets born, and the soul body or air body gets born, and then the warmth body or ego gets born, and they get born by going through certain illnesses.”
So, the etheric or water body gets born when you’re 7, and that’s when you go through measles. Your air body, your soul body, sort of the whole puberty thing gets born when you’re 12 to 14, and then you go through rheumatic fever or strep infection. And then, your ego gets born when you’re 20, 21 and then you go through mono. When you’re born, your physical body gets born through interacting with the air. The Greek said, “When you interact with the air, that’s the birth of the physical body.” And that happens through overcoming pertussis or whooping cough. So, that’s this sort of scheme he laid out. I think the point for anybody to realize is that a strategy of keeping children from overcoming obstacles is fundamentally a strategy of creating weak human beings.
Ben: It’s so inconvenient though to have to get scarlet fever and the measles and take the more, shall we say stoic approach to sickness rather than just trying to nuke it with the vaccine.
Thomas: Yes, maybe, but if you realize, as I’ve come to, that there’s no other choice, A, and that with proper care. And so, some of what you learned in anthroposophical medicine is the proper care of these illnesses. But even if they weren’t, the mortality rate from measles in the decade prior to the measles vaccine had dropped to almost zero. So, there was very little case to be made that this was a dangerous disease to the American population before the measles vaccine. So, now, we have a whole lot of hysteria about it, but the bottom line was–I mean, we had measles parties my parents brought me when they wanted me to get measles so I didn’t miss so much school, and it’s a whole different world of how we think about these things. People then had a sense that you cannot prevent children from experiencing challenges because that’s not how human beings develop.
Ben: Yeah. It kind of just comes full circle, honestly, to everything that is wrong with the way that we raise our kids from antibacterial hand soaps to soy milk formulas to the built-up protective covering on the floor of all the playgrounds at the schools. It’s just sacrificing kids’ muscle mass, their bone density, their immune systems, and then we carry that into adulthood at which point then we have to pull out all those fringe things we talked about earlier like LDN and mistletoe and colostrum and these soil extracts are digging up from the earth like Restore. A big part of it is, sure, a little bit of the glyphosate and the herbicide and the pesticide and the modern battle we’re fighting in an era where our food is compromised. But another big part of it is the way that our immune systems have been treated when we’re babies.
Thomas: We’re babies. And it’s the lucky ones who can just use those things. It’s the unlucky ones who get all the really life-altering horrible situations that we have in literally epidemic levels, whether it’s MS, and ALS, and autism, and breast cancer at age 35 that was never seen before. So, if that’s the way we want to go, then we’ve got a perfect strategy for that right now.
Ben: Yeah. And I guess I would close with this because a lot of people will ask me, “Well, what do you do, Ben, with your kids?” We did a lot of international travel with our kids. We got a couple of vaccines that if I could go back and do it again, as you and I discussed in our last podcast, I would probably use a lot more natural defense mechanisms like Thieves essential oil and vitamin D and all these other ways that you can support the immune system or fight off infection. But then, the other thing–I mean my kids, every morning, they’re taking, especially during cold and flu season where they’re surrounded by sick kids at school, they’re taking double the amount of vitamin D and K. They take glutathione with PQQ and coenzyme Q10 for mitochondrial support before they go off to school. We have chaga tea, vats of chaga tea in the refrigerator that the kids are drinking. Everybody in our house takes colostrum. If there’s any type of flu or immune system issue going around, we take a shot of Restore each time before we eat a meal. And all this might sound laborious. For us, it’s like taking a shower, brushing our teeth. These are the ways that we protect ourselves. And for me, and especially for my children, doing this rather than putting a bunch of metals and toxins into their body is a far superior approach.
For those of you listening in who have questions, who have comments about this kind of stuff, I would recommend that you not only read Dr. Cowan’s book, “Vaccines, Autoimmunity, and the Changing Nature of Childhood Illness” because admittedly, we skim the surface of the gel matrix inside of the cell and also some of the politics and the science behind vaccinations and things like measles and smallpox. It’s a wonderful resource that I think anybody who has an immune system or children should own. So, I’m going to link to that one in the shownotes along with everything else that Dr. Cowan and I talked about and my previous three or four, I don’t remember, podcast episodes with him all over at BenGreenfieldFitness.com/autoimmunity. That’s BenGreenfieldFitness.com/autoimmunity.
And, Dr. Cowan, I want to thank you again for coming on the show and for all this forward-thinking work that you’re doing.
Thomas: Thank you, Ben. I just want to say again, I think I’ve said this before, but I so appreciate your thoughtfulness and your wonderful way that you ask questions and sort of process this because it makes it much easier for me. And believe me, not everybody can do that.
Ben: Well, I mean I’ve said this before on shows but one of my favorite parts about my job is when the book from whatever, Victory Belt or Chelsea Green or any of this other kind of forward-thinking publishers show up at my doorstep because they know I want advanced copies. And I get to lay in bed at night and read them, and my wife gets sick of me just like–it sounds like this when I’m reading, “Oh-huh, huh. Interesting, huh. Hey, babe, listen to this.” And I underline everything. But the coolest part is as I’m sitting there reading the book, folding pages, underlining, and occasionally with the Kindle, dragging my finger across, I’m highlighting that once I assimilate all of those questions, I get to get a guy like you on the phone and actually pick your brain about the book that you wrote. That’s my favorite part about my job. So, yeah, it’s hopefully doing some people some amount of service. So, anyways, thanks for your time, man. I appreciate it.
Thomas: Okay, Ben. Thank you.
Ben: Alright, folks. I’m Ben Greenfield along with Dr. Thomas Cowan signing out. All the show notes are at BenGreenfieldFitness.com/autoimmunity. Have an amazing week.
Over the past fifty years, rates of autoimmunity and chronic disease have exploded.
Currently, 1 in 2.5 American children has an allergy, 1 in 11 has asthma, 1 in 13 has severe food allergies, and 1 in 36 has autism.
While some attribute this rise to increased awareness and diagnosis, my guest on today’s show, Thomas Cowan, MD, argues for a direct causal relationship to a corresponding increase in the number of vaccines American children typically receive – approximately 70 vaccine doses by age eighteen. The goal of these vaccines is precisely what we’re now seeing in such abundance among our chronically ill children: the provocation of immune response.
In his new book Vaccines, Autoimmunity, and the Changing Nature of Childhood Illness, Dr. Cowan looks at emerging evidence that certain childhood illnesses are actually protective of disease later in life; examines the role of fever, the gut, and cellular fluid in immune health; argues that vaccination is an ineffective (and harmful) attempt to shortcut a complex immune response; and asserts that the medical establishment has engaged in an authoritarian argument that robs parents of informed consent. His ultimate question, from the point of view of a doctor who has decades of experience treating countless children is…
…what are we really doing to children when we vaccinate them?
Dr. Cowan, MD, is a veteran family physician who has studied and written about many subjects in medicine, including nutrition, homeopathy, anthroposophical medicine, and herbal medicine. He is the author of Human Heart, Cosmic Heart: A Doctor’s Quest to Understand, Treat, and Prevent Cardiovascular Disease and the new book Vaccines, Autoimmunity, and the Changing Nature of Childhood Illness from Chelsea Green Publishing. He is also a founding board member of the Weston A. Price Foundation, and a frequent lecturer throughout the US and Canada.
He’s also the same doctor I mentioned in this Joe Rogan episode when I talked about how your “heart is not a pump”.
During our discussion, you’ll discover:
-Dr. Cowan’s experience with a childhood friend with asthma, and how it turned him onto medicine…8:00
The child was teased by classmates. “How dare you be sick…” He was way out of the norm.
Asthma is far more prevalent now than in the 60’s.
Increasing number of adults with autoimmune issues.
A large number of people diagnosed with autism become institutionalized.
-The story of William Coley’s Toxins…12:50
“Give me a medicine to produce a fever, and I can cure any disease.” –Hippocrates
Coley was an oncology surgeon, specializing in osteosarcoma.
Realized his conventional treatment of sarcoma (cancer) was not effective.
Came upon a former patient who was scheduled to be treated for sarcoma.
Wound up getting treated for erysipelas (induced fever); sarcoma went away and never returned.
Experimented with induced fever treatment on his own patients. 40% were cured with this treatment. 40% mortality rate.
Inducing fever was killing the cancer.
Coley’s Toxins has been banned as a practice in the U.S. since the 1960’s.
“When I’m treating someone for a condition whose symptoms include a fever…If we can cure that condition without alleviating the fever, I am preemptively pushing this individual away from cancer for the rest of their life.” –Dr. Thomas Cowan
-The two branches of the immune system…21:20
You get exposed to measles.
Body is looking at infected cells.
Mounts a white cell response: attack and digest infected cells and clear out of the body.
Fever, rash, diarrhea. Basically what we call “being sick.”
“Being sick” is not the virus; it’s your body rejecting the virus.
If you inhibit the cell-mediated response, you can infect and even kill people.
By eliminating the symptoms (fever, rash, diarrhea, etc.) you allow the virus to continue its attack on the immune system.
Theory of vaccines: Purely antibody strategy.
No cell-mediated immune system.
Inject the virus along with aluminum, mercury, formaldehyde, etc. to force your body to produce antibodies.
You end up with an accelerated antibody response.
2 problems with this strategy:
You have zero possibility of developing lifelong immunity to a virus after it has passed.
Every vaccine needs to have boosters.
Just as susceptible as a newborn as an adult.
Autoimmune disease is the situation of accelerated antibodies that are targeting your own tissues.
Children who get chickenpox and measles have less major chronic disease later in life.
CDC: Anyone born before 1956 is considered to be immune to measles.
-Why the way current science believes cells operate in the immune system is flawed…31:30
The central paradox of mammalian cells: How does a cell live in a sodium-rich environment, yet has a sodium-poor internal milieu.
Balance of sodium and potassium “charges” the cell like a battery.
Lose the charge, you have a dead cell.
Each cell has a “pump” that balances the sodium and potassium.
Two problems with this way of thinking:
Cells are supposedly 70% water, but there’s no water in the human body.
In order to create the supposed differential, a cell needs 40x the amount of energy a normal cell has just to run the “pump,” let alone its other normal functions.
There’s not enough ATP available to be responsible for the proper distribution of sodium and potassium
-The real reason we get sick…42:50
The sequence: You feel good, then get a fever, then a bunch of snot, then you feel better.
Your body is like a gel; then it gets corrupted by a virus.
Your body heats up, softens the gel, gets rid of the virus, the waste of which ends up in your hanky. The gel hardens again and is immune to that disease.
Introducing foreign substances as you find in vaccines weakens the immune system; you keep getting sick over and over; you experience inflammation.
-Dr. Cowan’s protocol for supporting the immune system based on the innate immune system response…48:40
Substances such as aluminum and formaldehyde interfere with the charge of the actual cells.
A human being is an information communication device with the rest of the world; our “radios” are out of tune with vaccines.
Adequate water, minerals, outside barefoot, adequate sunshine. Low hanging fruit to take care of before turning to vaccines.
-What we can do to reverse or overcome the effects of vaccinations if we’ve been vaccinated already…51:15
No one is beyond hope. Take it one step at a time.
Create a “cellular gel restoration program.”
You may need to experience the illness again. Let your body do its own house cleaning.
-The one pharmaceutical drug of which Dr. Cowan is an advocate, and why…53:45
Low doses of Naltrexone.
Discovered as opiate receptor inhibitor. (OD on heroin.)
When you block opiates, you block endorphins. You’re not a happy camper.
Naltrexone tricks your body into making endorphins; makes a huge difference in people suffering from AI disease.
-How colostrum helps both children and adults with autoimmune issues…59:45
Stimulates healthy gut flora.
Prevents leakage into the bloodstream.
-And MUCH more…
Resources from this episode:
My previous episodes with Dr. Cowan:
–Dr. Thomas Cowan’s vegetable powders
–Why Your Heart Is Not A Pump (& What Most Doctors Don’t Know About The True Cause Of Heart Disease).
–How (& Why) To Eat More Vegetables, Why A Plant Is Like An Upside-Down Human, Little-Known Superfood Plants & More!
–The Shocking Story Of Vaccines, The Toxicity Of Ultrasounds, Why You Shouldn’t Play With Your Child & Much More With Dr. Thomas Cowan
–The Insulin Of The Heart: A Little-Known Seed Extract That May Be The Future Panacea For Heart Disease.
-Book: Vaccines, Autoimmunity, and the Changing Nature of Childhood Illness
-Book: Human Heart, Cosmic Heart: A Doctor’s Quest to Understand, Treat, and Prevent Cardiovascular Disease
–Gilbert Ling’s books
–Gerald Pollack’s books
–GreenfieldNaturals Whole House water filtration unit
–The LDN book by Linda Elsegood
–OralIV for structured water during travel
–Restore by Dr. Zack Bush
–Kion Colostrum
–Allergy Research desiccated organ extract
Episode Sponsors:
–Kettle and Fire Get 15% off your order using my link.
–Kion Aminos and Thorne Aminos. 10% off both.
–Harry’s Razors Get their trial set for FREE (a $13 value) when you use my link.
–Zip Recruiter A better way to hire! Use my special link and try Zip Recruiter for free.
Ask Ben a Podcast Question
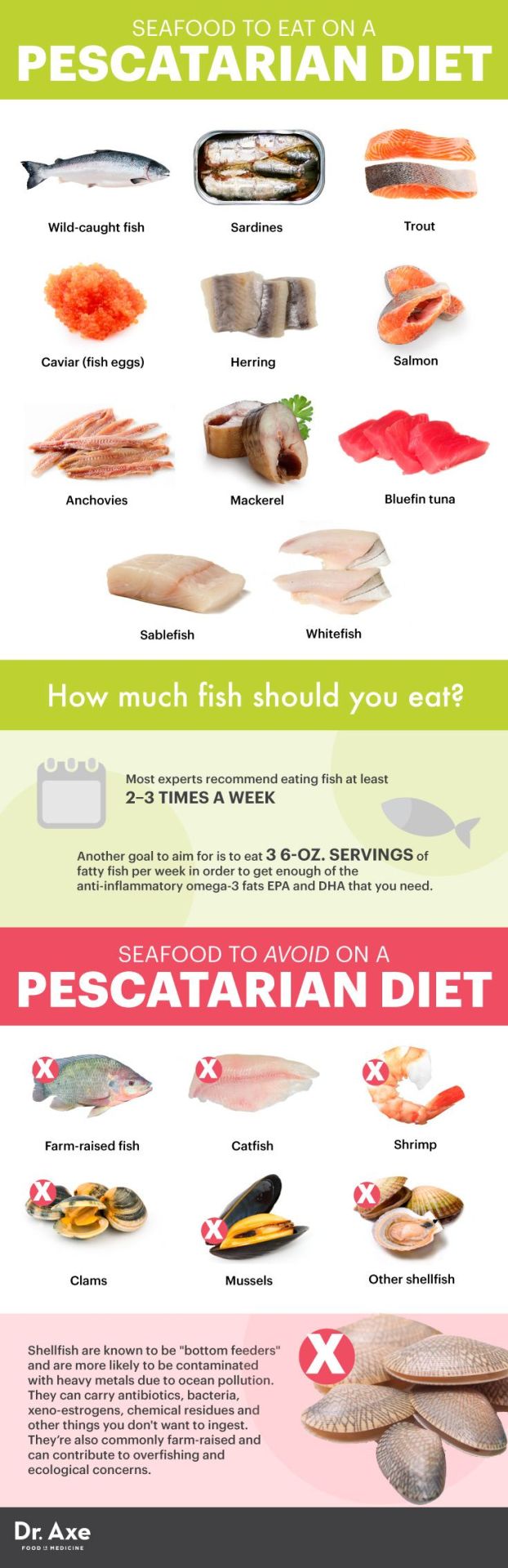
Source: https://bengreenfieldfitness.com/transcripts/transcript-should-kids-get-vaccinated/
0 notes