#ukzn
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The total number of visits Tumblr.com received during January 2021 is 327 million.
Text
Community, Occupational Therapy and the Art of Teaching people to fish ( or at least trying)
Being an Occupational Therapist (OT) in a community is like being handed a rusty car with no engine and being told to make it work. I know how dramatic this may sound, forgive me but after our tutorial last Wednesday, I realized how vast the challenges can be in making a meaningful impact in different communities—and honestly, sometimes it feels like we’re pushing that engine-less car uphill with the handbrake on.
At Cato Manor the people there are lovely, warm, and welcoming, but if you've ever tried to introduce a project and then watched it fizzle out as soon as you step away, you know the frustration I’m talking about. It's not that they don’t want the help or the resources—oh, they definitely want something from you—but the spark to keep things running on their own seems to flicker out as soon as we’re gone. Meanwhile, in other communities, like Mariannridge, things are thriving! Projects seem to run on autopilot, and the community is fully invested. What gives? How did they get halfway and we are still at the bottom of the hill ? Having an engine that’s the answer!
Visualize this : every week we go to Thandeka’s Daycare and previous block have given them child development manuals, stimulation boards, caregiver training, you name it. Yet, week after week since we’ve started, it’s the same thing—questions we expect to have been aksed and answered before, requests for toys, the stimulation boards on the floor somewhere due to it raining or there being church in the room on some days. So, what’s happening? Where’s the initiative? Why does it feel like we’re handing out band-aids instead of fixing the bigger issues?
Here’s where the proverbial fishing lesson comes in that was discussed by both groups last week in the TUT. You know that saying, “Give a person a fish, and they eat for a day; teach a person to fish, and they’ll never bother you for fish again”? Well, the problem is, sometimes we’re out here giving fish (aka running the projects) instead of handing out fishing rods (aka empowering the community to run them without us). And it’s not just me coming to this conclusion because I’m being delulu. Research supports this too! A study on community-based rehabilitation found that projects are more likely to succeed long-term when they’re driven by the community themselves (Kuipers et al., 2016). Makes sense, right? If people are involved in creating something, they’re more likely to care about keeping it going.
Now, let’s talk about schools. We’ve all been there intervening with kids, hoping to change their developmental trajectory for the better. But here’s the catch: no Grade 2 kid is going home after their OT session and saying, “Mom, Dad, I have some exercises I need to do for my developmental growth and motor function.” Nope. Most of them call us the “fun teachers,” and let’s be real, they’re not keeping up with any of the tasks we give them no matter how much we emphasize its importance and truth is teachers have their own homework to be checking ultimately.So, why aren’t these interventions sticking? It’s simple. The parents often have no idea what we’re doing with their kids. Because we don’t meet them. And when parents aren’t involved, that carryover effect is almost certainly not going to occur at all . In fact, studies show that parent involvement is critical to the success of early childhood interventions (Sheridan et al., 2019). And it’s not just about following up after appointments. I mean, how many follow-ups can we really do? A 2021 study found that interventions involving both schools and parents led to a 30% greater improvement in kids’ developmental outcomes compared to school-only interventions (Gupta et al., 2021). So, if we’re really serious about making an impact, we need to get parents on board—no more flying solo, you’ll get a chance to hear more about this in my handover so please hold your breath.
The Engine-Less Car (Or Why Community Involvement is Key)
Here’s the thing: not all communities are the same. Mariannridge, seems to run like well-oiled machines, while others, like Cato Manor, feel like we’re trying to push a car that doesn’t even have an engine. And what’s that engine, It’s community pride and involvement. Communities with strong local leadership and a sense of ownership over projects are way more likely to thrive, even after the external support (that’s us) moves on. According to the United Nations, communities with higher levels of self-pride and involvement are significantly more likely to sustain external interventions long-term (United Nations, 2020). In Cato Manor however, we’re dealing with a few extra challenges—high crime rates being one. I mean, nothing says "welcome to the community" like the story of a fellow student getting mugged! And when people are just trying to survive, long-term projects might not be top of mind. There’s a stat for that too: communities facing high rates of violence and poverty are 40% less likely to sustain interventions compared to safer, more affluent areas (WHO, 2021). No wonder things are tough. But here’s where it really starts becoming muddy waters. Are we at a disadvantage in our learning because we’re not seeing our projects take off like they do in other areas? Or is this actually an advantage? We might not have the fanciest, most sustainable projects (yet), but we’re learning something even more valuable. We are learning what it takes to build those projects from scratch. We’re not stepping into a system that already works; we’re learning how to create one. And that’s a skill that’s worth its weight in gold. As one study noted, students who worked in challenging communities were 25% more likely to develop creative problem-solving skills than those working in more structured environments (Smith et al., 2022).
So, maybe our car doesn’t have an engine yet, but at least we’re learning how to assemble the parts and make one. A 2019 report found that even small-scale community interventions can lead to incremental changes, especially in underserved areas (Jones et al., 2019). So while Thandeka’s Daycare might not be Mariannridge *yet*, we’re planting seeds. And sometimes, those seeds take longer to grow. Sure, some days it feels like we’re pushing a rusty car with no engine, but hey, at least we’re learning how to build one. And who knows? Maybe one day, that car will be cruising down the highway on its own.
References:
Gupta, P., Kumar, D., & Sharma, A. (2021). Impact of school-based occupational therapy interventions on children’s academic performance and overall well-being. *Indian Journal of Pediatrics*, 88(4), 355-359.
Jones, M., Harris, L., & Clark, S. (2019). Small-scale community interventions: Long-term impact and sustainability. *Journal of Community Health*, 44(3), 450-461.
Kuipers, P., Kendall, M., & Hancock, T. (2016). Community-based rehabilitation: inclusive development and health. *Disability and Rehabilitation*, 38(1), 33-41.
Sheridan, S. M., Knoche, L. L., & Clarke, B. L. (2019). Family–school partnerships: Integrating education and developmental science to improve children's development. *Developmental Psychology*, 55(5), 1105-1113.
Smith, J., Rogers, T., & Elmer, G. (2022). Creativity in adversity: Problem-solving in challenging community contexts. *Journal of Occupational Therapy Education*, 2(1), 24-38.
United Nations. (2020). *Sustainable Development Goals Report 2020*. United Nations Department of Economic and Social Affairs.
World Health Organization. (2021). *Community-based rehabilitation: CBR guidelines*. WHO Press.
1 note
·
View note
Text
Addressing Sustainable Goals in Occupational Therapy.
In a country like South Africa, there is a huge need for development implementation. People from all walks of life, and professions must work together towards achieving the goal of getting the country more developed. This includes the occupational therapy profession. This blog will explore how I, an occupational therapy student, have been, and plan to continue addressing some of the Sustainable Development Goals in a community like Cator Manor, a community facing a lot of socio-economic challenges such as unemployment, poverty, crime, substance use, and poor infrastructures.

As an occupational therapy student currently in the community blog, my colleagues and I have been doing our part in the movement of implementing some of the Sustainable Developmental Goals in the community we are currently serving. For the sake of this blog, I am only going to mention 5 of the SDGs, namely; No poverty, Zero Hunger, Quality Education, Good Health and Well-being, and Gender Equality United Nations (2023).
For the past 3 weeks, I have had the pleasure and the privilege of serving the community through services I provide in the community clinic, local creches, the primary, and secondary school. Through these services, as minuscule as they may seem, I would personally like to believe that I have been doing my part in bringing positive change in the community, promoting occupational engagement to some of the community members, and somehow enhancing life in the community as a whole.
According to the United Nations (2003), the Sustainable Development Goal of No Poverty aims to alleviate Poverty in all shapes and forms. As an occupational therapist, I have a duty that includes encouraging and enabling community members to develop job skills, rehabilitate the injured, and prepare them for job integration, and encourage the community to consider exploring sustainable incomes through self-employment, such as starting vegetable gardens, all in the name of trying to improve economic independence (Durocher et al.,2016).

The idea of the vegetable garden can ultimately work on another Sustainable Goal, which is Zero Hunger. And in the interest of the sustainable goal, of Zere Hunger, we, as Occupational Therapy students have had the pleasure of helping in the community feeding scheme that serves food outside the community hall.
In a community facing socio-economic challenges, quality education is of significant importance for all willing to receive it. This would ultimately offer the community more opportunities such as getting more people into higher education and bettering their chances of getting more jobs. In a community like Cator Manor, schoolers were reported to be abusing and selling drugs, having behavioral issues, and also facing hardships in their school and personal lives. We, as occupational therapists, have an important role in helping teachers and social workers address the needs of students with learning disabilities to enhance engagement in education (Durocher et al.,2016). We also run groups and individual interventions for psychosocial challenges such as peer pressure and substance use.
While working in the Clinic, I also have the opportunity to address the Sustainable Development Goal of Good Health and Well-Being. My colleagues and I have been doing health promotions almost every day, aimed at informing the public about services Occupational Therapy and other medical professionals in the clinic offer. We worked on raising awareness on Mental Health (anxiety and depression, substance abuse, traumas), and addressing the often-overlooked Maternal Mental Health (Wednesdays at the Philamntwana Clinic). We also looked at barriers the community members face that prevent them from engaging in meaningful occupations, all to promote Good health and Well-being.
In a school with social workers, there were a lot of reports of scholars witnessing and experiencing Gender-based Violence, at home and the school, I had the pleasure of doing a group session that included promoting Gender equality. This was aimed to address social and cultural norms that are unfair to women and provide psychosocial assistance to those experiencing these inequalities.

As many of our academics say, as occupational therapists, we are agents of change in communities. Through advocation and promotion, we can address Sustainable Developmental Goals. As much as we cannot address these with every single individual in the community, I believe through engaging with some of the members, we can create a ripple effect that benefits the community. Still, until then, we are going to do what we can, one step at a time.
REFERENCES
Durocher, E., Gibson, B. E., & Rappolt, S. (2016). Occupational justice: A conceptual review. Journal of Occupational Science, 21(4), 418–430. https://doi.org/10.1080/14427591.2013.775692
United Nations. (2023). Sustainable Development Goals. https://sdgs.un.org/goals
0 notes
Text
Classroom Boxes to Community Chaos
As I approach the end of my journey through the UKZN OT curriculum, currently in my second-to-last block, it's been a wild ride. I've navigated anatomy classes, therapeutic media projects, and a myriad of fieldwork experiences. Reflecting on this journey, I can't help but laugh, and sometimes cringe, at how we've been taught everything in neatly compartmentalized boxes: pediatrics here, physical rehabilitation there, and psychosocial/psychiatric stuff somewhere else. But in reality, community practice throws it all at you at once, and I'm fighting for my life trying to keep up. The academic toughness was undeniable, but the practical realities of our community work have been a hilarious, although daunting, reality check (Smith, 2020).
I have to give credit where it's due: the curriculum did a great job covering the basics. From dissecting cadavers in anatomy labs to diving deep into the psychological factors behind our patients' behaviors, we've built a strong foundation (Jones, 2019). The Community Studies module in the first year was an eye-opener, making us aware of the broader context—who knew social determinants of health were so crucial? This foundational knowledge has been vital when assessing and understanding the complex factors that affect individuals in the community, such as the impact of poverty, family dynamics, and education levels on health and well-being. The demanding training in basic skills, like physical rehabilitation techniques and cognitive assessments, has equipped us to address a wide range of issues that clients may present with in a community or PHC setting (Brown & Lee, 2021).
Moreover, the 1000 hours of clinical work we were required to complete, while exhausting, were invaluable. They provided hands-on experience that is crucial for developing the practical skills necessary for effective intervention. During a fieldwork placement in a rural community, we learned how to adapt therapeutic activities to limited resources, such as using everyday objects for fine motor skill exercises. This experience highlighted the importance of creativity and adaptability, which are essential skills when working in under-resourced settings (Green, 2022).
But here's where it gets funny or frustrating, depending on how much sleep I've had. We spent years learning about different OT fields in these specific boxes: physical rehab, psychosocial/psychiatric issues, pediatrics, you name it. Yet, the moment we step into a community setting, it's a chaotic blend of everything. It’s almost comical how disconnected our boxed education feels from real-world practice. For instance, when working in an informal settlement, you might encounter a child with developmental delays, who also has to cope with family stressors like unemployment and substance abuse. Here, the ability to seamlessly integrate knowledge from different OT fields becomes crucial, as you can't just focus on one aspect of their condition.
In this environment, our preparedness for practice is tested. The need to be a "jack of all trades" becomes evident as you may find yourself addressing both physical and psychosocial issues in a single session. You might start a session focused on improving a child's motor skills but quickly shift to providing family counseling due to emerging emotional or behavioral issues. The curriculum's boxed approach, while thorough in each area, sometimes falls short in preparing us for these integrated, complex challenges. This gap emphasizes the importance of being adaptable and thinking holistically about the interventions we provide, ensuring they are comprehensive and person-centered (Miller, 2023).
Going through these 'boxes' has been a crash course in being flexible. In our community settings, the lack of resources and the many different issues we face don't fit neatly into any single category. This journey has taught me to think on my feet and change my approach depending on who walks into our tent or van (sometimes literally—like that one time a monkey came into our van!). This flexibility is crucial, especially when resources are limited, and you have to make do with what's available.
Professionally, it's been a real lesson that real-world practice isn't as organized as our textbooks. This realization has been both challenging and exciting. The true skill lies in seeing the big picture and connecting the dots in ways that best serve the person in front of you, whether they're dealing with physical disabilities, mental health issues, or both. A stroke survivor we worked with during a community intervention. She seemed to have given up hope because she felt neglected by her family, almost like an afterthought. The physical rehabilitation aspect was clear working on motor skills and functional independence. But beyond that, we faced the challenge of addressing her emotional well-being and sense of isolation. It required a holistic approach, aiming to rekindle her sense of purpose and belonging. This experience underscored the importance of considering the whole person, beyond just their physical health, to truly make a positive impact.
Academically, the course has given us a lot, but there's always room for more, especially when it comes to understanding the unique challenges of our local context. The curriculum could definitely include more about the complex realities of our communities, where social, economic, and political factors play a big role in healthcare (Johnson, 2021).
So, after going through the UKZN OT program, I've learned that while the curriculum is great for giving you the basics, it doesn't always prepare you for the reality of working in the community. The challenges are way more complicated than what we learned in class. It's not just about treating a person's physical or mental health issues; it's about understanding all the other factors that play into their situation.
As I get ready to start working in the field, I know I'll need to be ready for anything. Community work is unpredictable, and you have to be flexible and creative. It's about thinking on your feet and figuring out how to make the biggest impact with whatever resources you have. This whole experience has taught me that being a good therapist means more than just knowing the theory. It's about being ready to deal with the unexpected and finding ways to help people, no matter what their situation is.
References
Brown, S., & Lee, J. (2021). Occupational Therapy in Community Settings: A Comprehensive Guide. New Directions Press.
Green, T. (2022). Adapting Therapy in Low-Resource Environments. Community Healthcare Publications.
Johnson, M. (2021). Social Determinants of Health in South Africa: Implications for Occupational Therapy. SAJOT.
Miller, K. (2023). Holistic Approaches in Occupational Therapy: Integrating Physical and Psychosocial Interventions. Occupational Therapy Journal.
Smith, A. (2020). Foundations of Occupational Therapy: Building Blocks for Practice. University Press.
Additional Resources
Reading on Community OT Practices
Link: Community Occupational Therapy and Its Challenges
Reading on Integrating Social Determinants in OT
Link: Addressing Social Determinants of Health in OT
youtube
This video dives into the complexities of community OT practice
#OccupationalTherapy#CommunityHealth#OTStudentLife#UKZN#RealWorldOT#HolisticHealthcare#SocialDeterminants#CommunityPractice#HealthcareInSA#Youtube
0 notes
Text
MA Arts
recently applied once again at UKZN for a masters’ degree. I’d like to research the importance of dramatic tools used in every subject area to try and teach comprehension and understanding.
Over the past 5 years, I’d been blessed enough to be given the opportunity of working with students; young minds eager to learn. My only worry was that majority of children lack the understanding of words, sentences, phrase and meaning. English being the medium of communication, it allows us the ability to converse and understand people from all walks of life. It is then my duty to make this very complicated yet important language easily understood and accessible. Through the conduction of workshops, training and role play of drama, students utilise skills to better analyse texts thus will they be able to fully comprehend given scenarios in assessments
2 notes
·
View notes
Note
hey idk what uni you're going to like you said in the other ask but I think almost all of them have palestine solidarity clubs and work together to organise and fundraise. I know stellies, uct, uwc, ukzn and up have psc's and you can find them on insta and facebook where they frequently post updates and look for volunteers to march and make posters
Hi! So I have applied to three of the universities you've mention (hopefully I get acceptedd into at least one) and joining a solidarity club is definitely something I plan on doing - it's actually one of the things I'm looking forward to most at uni lol
#asks#i'm actually hoping i get into uwc#or at least uct lols#since i plan on studying accounting#which amittedly is one of things i DREAD about started uni
3 notes
·
View notes
Text
Shout-out to Dr. Deepak Mastry from UKZN. Blorbo from my Bachelor Of Arts (Philosophy, Politics & Law). Will never forget that one time after class when you told me to fuck off.
"Blorbo from my shows" no. Blorbo from my BA. Blorbo from my major. Blorbo from my primary source document.
44K notes
·
View notes
Text
A Heartfelt Goodbye: Lessons from Kenville/Sea Cow Lake


Kenville Community OT (Kenville Community OT, n.d.) and Occupational Therapy (UKZN Occupational Therapy, 2021)
On my way out of the Kenville/Sea Cow Lake community with my notes packed up and a lot of goodbyes said, I am filled with gratitude. This block has taught me to be a listener, a collaborator, and, most importantly, a learner. I'll never forget the wide-eyed and big smiles of babies reaching for toys during developmental assessments at the clinic and the sound of children's laughter echoing on the soccer field during the group soccer games. The smell of Igwenya (vetkoek) coming from the tuckshop near the clinic. Our OT space, the once bare shipping container, gradually became home.

Sea Cow Lake Clinic (Siqathule, 2023)
Kielhofner (2009) wisely said, "Closure is not an end, but a transition." The words have taken on new meaning for me. How do you properly say goodbye to people who've reshaped your professional identity? I've realised it's not about walking away but ensuring the work continues. I've shown clients simple exercises/ tasks they can do at home using things they already have. At the school, I taught teachers easy ways to keep supporting the kids. For the next students who come here, I've written down everything they'll need to know, not only the official stuff but little tips, too. It's incredible to see how small changes, like teaching a child to hold a pencil differently or showing a mom how to help her baby sit up, can improve everyday life for clients.
The clients here taught me that genuine client-centred care isn't about fancy assessments or perfect treatment plans. It's about listening when they tell me what works in their daily lives. Whalley Hammell meant this when she said that even our best professional intentions could miss the mark if we don't truly partner with clients (Whalley Hammell, 2015). Beagan (2015) echoes this, reminding therapists that cultural humility, not just awareness, is key to effective practice. I understand that good therapy happens when professionals step off their pedestals. It's not about being the expert. It's about creating a space where your clients feel safe enough to say, "Let's try it this way instead" or "I would do it like this." That's when real healing begins.

Children from Kenville/ Sea Cow Lake playing at the Old Clinic (Kenville Community OT, 2022)
I didn't realise how deeply this experience would transform me, not just as a therapist, but as a person. Seeing what people can create with so little opened my eyes in unexpected ways. The reality of people's daily struggles hit me hardest during home visits. Trying to navigate uneven paths with mobility equipment and watching clients adapt small living spaces for their needs, these moments made Duncan's (2020) theories about environmental barriers fall into place. I finally understood what she meant about how physical and social environments can disable people just as much as any condition. These moments made me truly appreciate how someone's environment affects their abilities. What surprised me most wasn't the challenges people faced but how they found ways to thrive and flourish despite them.

Home Visit Commute (Kenville Community OT, 2021)
Sakellariou and Pollard's idea of "occupational justice" used to feel like just another theory I learned in class. Now, after working alongside this community, it's become something much more personal. I can look back and see these small everyday victories and how a small change can become big. It reveals that occupational justice isn't about big gestures but constant, thoughtful advocacy that cuts through barriers and opens doors. They all teach me that justice comes from practical solutions and collective effort. Now, I carry this understanding into every client interaction, knowing my role isn't just to treat but to tear down obstacles and build bridges to fuller participation in life.

Overview of Kenville/ Sea Cow Lake (POST Newspaper, 2017)
This is the real challenge, now to take these lessons with me. Kenville taught me that becoming an occupational therapist is more than a career, it is how you will be in the world, someone who is really seeing people where they are.
References
Beagan, B. L. (2015). Approaches to culture and diversity in occupational therapy. Canadian Journal of Occupational Therapy, 82(3), 150-158.
Kielhofner, G. (2009). Model of human occupation: Theory and application (4th ed.). Lippincott Williams & Wilkins.
Duncan, E. A. S. (2020). Foundations for practice in occupational therapy (6th ed.). Elsevier.
Whalley Hammell, K. R. (2015). Client-centred occupational therapy: The importance of critical perspectives. Scandinavian Journal of Occupational Therapy, 22(4), 237–243. https://doi.org/10.3109/11038128.2015.1004103
Sakellariou, D., & Pollard, N. (2016). Occupational therapies without borders: Integrating justice with practice. Elsevier.
Kenville Community OT. (n.d.). Facebook. https://www.facebook.com/KenvilleCommunOT/photos/pb.100064721198864.-2207520000/101583638366491/?type=3
UKZN Occupational Therapy. (2021). Facebook. https://www.facebook.com/UKZN.OT/photos/pb.100063620298425.-2207520000/106605914754552/?type=3
Siqathule, S. (2023). Patient lament of ‘unhygienic’ conditions at clinic. Rising Sun Newspapers. https://risingsunnewspapers.co.za/211209/patient-lament-of-unhygienic-conditions-at-clinic/
Kenville Community OT. (2022). Facebook. https://www.facebook.com/KenvilleCommunOT/photos/pb.100064721198864.-2207520000/465317378659780/?type=3
Kenville Community OT. (2021). Kenville Community. Facebook. https://www.facebook.com/KenvilleCommunOT/photos/pb.100064721198864.-2207520000/276858000839053/?type=3
POST Newspaper. (2017). Kenville Community. Facebook. https://www.facebook.com/postnewspaper/photos/the-kenville-community-was-outraged-by-a-recent-invasion-of-shack-dwellers-they-/1441847752529606/
0 notes
Text
Choose and present 5 sustainable developmental goals, that you intend to work towards within the community you work in.
In Kenville community, where there are different age groups and people with different challenges, I have learnt that our initiatives are a symbol of hope to people living in the community. I’ve heard this from various people in the community, from the teachers in the primary schools to the carers of the creches emphasizing that they are happy to have another batch of UKZN students in their community. Our approach is not only to provide practical interventions but also touch as many lives as we can in the community through our projects and willingness to put people’s needs and wants in the forefront of what we do to make sure they feel valued and understood by us.
As students working in the community, these are the 5 sustainable development goals that we have started and are working towards achieving. SDG 3, which good health and well-being, we do this by going to creches, the primary school, high school and active aging group to provide intervention. In the creches we do sensory stimulation for the children, promote school readiness by introducing and reinforcing basic concepts using gross motor activities. In the high school we provide intervention every Mondays on topics such as substance abuse, safe sex and study techniques to ensure that they can make informed decisions, and they have knowledge to differentiate between what is wrong and right. For older adults we want to offer intervention that promotes active lifestyles as when people grow older, they tend to not want to be active anymore. We also provide individual intervention at the clinic and do home visits. This is to ensure that even members of the community who cannot travel to the clinic due to physical limitations or financial issues receive intervention as well. This aligns with what the government initiated as they opened a R223 million Meje Community health center in Mbhongweni Village in 2023, they said the aim was to bring health care to people's doorstep to prevent them from spending much while traveling to St Patrick's Hospital in that underprivileged community. According to the article, this project also created 420 job opportunities for the people of the community, which is what we aim to achieve through the KITE project in Kenville community but that will be further discussed in the blog (Luvo Cakata, 2023).
Faith Nedoboni who owns the Konke Academy, initially saw a need to open an after-care facility as she saw children hanging around in the streets after school but after seeing that older children were struggling to read, she decided to turn it into a preschool where she assists them with numeracy and literacy (Savage, 2025). As we saw while assessing primary scholars, there are major issues with writing, following instructions, basic concepts and comprehension amongst other problems noted. Therefore, by using SDG 4, which is quality education, we do this by doing youth expressive groups and doing school-based interventions at the primary school. At the primary schools we provide intervention for learning difficulties by improving the learners' visual perceptual skills, behavioral issues and comprehension issues which are preventing them from grasping concepts in the classroom.This will cause issues for the children when moving to higher grades as they will not be able to perform according the the grades expectations cause them to fail and not be able to achieve their goals in future. In the youth expressive groups, we are hoping to facilitate creative ways for the youth to express themselves and personal development, by doing activities such as role play, journaling, doing crests, and doing poetry.
SDG 8, we recently got a lady in the community who is a KITE volunteer. KITE is a project in the community which is aimed at empowering women in the community by providing them with a way to make an income and support and sustain their families back at home, by teaching them entrepreneurial skills that they can use to start their own businesses. However, I would like to expand this and teach women of the community baking skills, this is a skill that they can use moving forward at any given moment of their lives and be able to use that skill to start their own businesses. Just like how Matebogo Victoria created a platform where deaf people could develop their skills in agriculture to find sustainable work, this was after he was exposed to how he was treated at Tshwane University of Technology as a deaf student. The university did not consider and attend to his needs as a deaf individual as a result he had a drive to start this initiative to support other people who have the same needs as him (Tiisetso Manoko, 2025).

SDG 10, which reduces inequalities. This will be done by turning the container into an Occupational Therapy workspace which is meant to provide interventions to people of all backgrounds in the community. Considering that Kenville’s new clinic did not have equipment to provide intervention for clients, this will help by preventing clients from traveling to far hospitals for Occupational therapy interventions. This has taught me how to be innovative and to consider the economic factors as this is an underprivileged community. Considering that and how to use resources that you have by using evidence that is available and using problem solving skills, to ensure that clients get the intervention they need, this was done outsourcing an examination bed from the physiotherapy department.
SDG11, which is sustainable cities and communities. This will be done by developing a playground for the children which will be used to assess and provide intervention, the activities will be a sand tire, hopscotch using tires, a balance beam and bowling using coke bottles promoting physical activity for the children and community engagement. Improving the OT facility by painting and dividing the container into adult and pediatrics sections to make the space inviting and functional. By using this equipment, it will ensure that the play group is sustainable as most of the equipment used can be replaced easily as it is used in the communities' day-to-day lives.
REFERENCE LIST
1.Luvo Cakata. (2023, October 5). R223 million Community Health Centre officially opened. News24. https://www.news24.com/news24/community-newspaper/mthathaexpress/r223-million-community-health-centre-officially-opened-20231003
2.Savage, R. (2025, March 11). “If you don’t get early years right, children are unlikely to catch up”: why South Africa is trying to reboot its school system. The Guardian; The Guardian. https://www.theguardian.com/global-development/2025/mar/11/children-school-south-africa-early-learning-sector-funding
3. Tiisetso Manoko. (2025, January 4). Deaf farmer champions greater accessibility in agriculture. Food for Mzansi. https://www.foodformzansi.co.za/no-limits-deaf-farmer-advocates-for-accessibility-in-agriculture/
0 notes
Text
FIVE SUSTAINABLE DEVELOPMENT GOALS IN PRACTICE IN COMMUNITY FIELDWORK

Photo credit: Biobin, 2025
In 2015, the 2030 Agenda for Sustainable Development, was adopted by all United Nations Member States (UN, 2025). This agenda includes 17 goals to which each country must strive to eradicate life challenges faced by many in the world (UN, 2025).
For my Community Theory and Fieldwork block in the 4th year of Occupational Therapy (OT), I can see that we work toward the following 5 goals which are zero hunger, good health and well-being, quality education, decent work and economic growth, and reduced inequalities.
Zero Hunger involves ending hunger, achieving food security, and promoting sustainable agriculture. Good Health and Well-Being involves ensuring healthy lives and promoting well-being for all at all ages. Quality Education is to ensure inclusive and equitable quality education and promoting lifelong learning opportunities. Decent Work and Economic Growth promotes inclusive and sustainable economic growth, employment, and decent work. Reduced Inequalities involves reducing inequality within and among countries (UN, 2025).
The project that targets good health and well-being is working at the Cato Manor Clinic, seeing clients and performing health promotion talks. Also screening children at the Philamtwana Clinic and performing maternal mental health promotion talks there. These activities promote good health and well-being by treating clients and getting them to seek help if they are unwell.
Quality education is done through a programme with the Mayville Secondary grade 9s where they learn life skills, career development and coping skills. This promotes lifetime learning opportunities by showing them options to study further and how to handle the stresses of school and daily life. We also try for inclusive education by targeting students with developmental delays in the Mayville Primary School and Golden Future creche and to rectify it by planning treatment activities with them.
Decent work is done through career talks with the high school children to showcase careers that would secure them good jobs. Also, I worked one-on-one with a client to prepare her business pamphlet and advised her on where she could join a business incubator for her craft products.
For partnership, the UKZN OT department has partnered with the Denis Hurley Centre to assist with their programmes for the homeless, refugees and drug users. We currently assist at their Dalton Creche with education, fine and gross motor and social interaction skills.
Through implementing all of the above programmes we are trying to reduce inequalities by giving people and children access to better health care and opportunities for learning and growth.
Therefore, these are the ways that I see us using 5 of the SDGs to further its mission in the Community Theory and Fieldwork Block in Cato Manor and the Denis Hurley Centre.
For further details on the 17 goals on the 20230 Agenda of Sustainable Development please visit the following website https://sdgs.un.org/goals
If you would like to get involved with the Denis Hurley Centre their details can be found on the following website https://www.denishurleycentre.org/page/volunteering-in-durban
A good place to start if you would like assistance with your business is the Small Enterprise Development Agnecy (SEDA). They can found at https://www.seda.org.za/
References
Biobin South Africa. (2025). Our commitment to the Sustainable Development Goals. https://biobin.co.za/our-commitment-to-the-sustainable-development-goals/
Denis Hurley Centre. (2025). Volunteering in Durban. https://www.denishurleycentre.org/page/volunteering-in-durban
Small Enterprise Development Agency. (2025). Home. https://www.seda.org.za/
United Nations. (2025). The 17 goals. United Nations Sustainable Development Goals. https://sdgs.un.org/goals
0 notes
Text
Reflecting on the pros and cons of the UKZN’s OT Curriculum: Are We Truly Ready for Community? PHC Practice?
“Tell me and I forget, teach me and I may remember, involve me and I learn.” – Benjamin Franklin.
Imagine stepping into a very busy community, eager to make a difference as an aspiring occupational therapist, only to realize that some of the tools you need are missing from your kit. You have the theory, the passion, and the drive, but do you really have the practical experience to back it up? As a 4th year OT student at the University of KwaZulu Natal, looking at the previous years, I had come across times when I knew what I was doing and also times when I felt I didn’t know anything. Sometimes, I couldn’t help but ask myself: Am I truly prepared for the realities of the community practice?
One of the biggest advantages of our UKZN curriculum is the early exposure to community settings in the first year, which is more like shadowing. However, it does not fully prepare students for the community fieldwork block. From second year onwards, we engage with real cases through the physical and psychosocial fieldwork modules, and we gain hands-on experience in conducting assessments, developing treatment plans, and working with clients. This practical exposure allows us to learn a lot and build confidence and competence in handling clinical cases with physical and psychological conditions. The psychosocial and physical aspects are well integrated into our learning, making it easier to manage clients presenting with conditions related to these fields.
This makes treating the physical and psych clients we find in the community block easier because it integrates everything, consolidates our knowledge from various OT domains and allows us to apply what we have learned in real-world settings. In our case, working in the Mariannridge community has given us significant exposure to how it actually feels to be in the community as we work with children, clients with chronic conditions, and those affected by social determinants of health. This experience will enhance our problem-solving skills and adaptability as emerging health practitioners.
Despite these strengths, there are notable gaps in how the curriculum prepares us for community settings. One of the major concerns is the limited integration of paediatrics into practical training; while we learn the fundamentals of paediatrics in theory, we do not have the opportunity to apply this knowledge in practice until the fourth year. By then, the information is difficult to retain and apply effectively, especially when dealing with paediatric clients in community settings like Mariannridge. Then, the comprehensive paediatrics content is condensed into a short two-week period in fourth year, weeks before we start practicals, making it overwhelming and difficult to absorb.
There’s a lack of early exposure to community-based practice as well. We only start learning about the basics of community OT in the fourth year, yet we are expected to deliver interventions effectively in these settings. Without prior structured community fieldwork practicals, navigating the complexities of working in under-resourced communities, such as Mariannridge, addressing health promotion and implementing sustainable interventions becomes challenging.
“The purpose of education is to replace an empty mind with an open one.” –Malcolm Forbes
To better prepare UKZN OT students for the community block, the curriculum should be revised to include earlier and more structured fieldwork experiences in both paediatrics and community practice. This could include introducing paeds and community blocks from first to fourth year, allowing students to gradually build their competencies in these areas rather than being overloaded with information in final year. To improve community OT training early in the curriculum, introduce community OT concepts and practices from previous years. This will help students build a deeper grasp of the role of OT in PHC and CBR.
If the UKZN OT program aims to produce well-rounded future practitioners who can thrive in any setting, then it’s time to rethink how the OT department trains students for community practice. While the foundation is strong, the gaps in paediatric and community-based training cannot be overlooked. So, here’s a thought: what if the department restructured the curriculum to ensure that we know and feel ready for the communities we serve by the time we graduate?
"Education is not the filling of a pail, but the lighting of a fire." — William Butler Yeats
0 notes
Text
Bridging the Gap: A Critical Reflection on UKZN’s OT Curriculum and Community Practice Preparation
South Africa’s public healthcare system is based on levels which offer services at tertiary, secondary, district and Primary Health Care (Naidoo, Van Wyk & Joubert, 2016). As primary healthcare serves as the first level of care, it is depended upon by 86% of South Africa’s population, due its cost-effectiveness, accessibility, inclusivity, efficiency and equitability (Health Hosts South African Primary Health Care Conference, South African Government, 2023). This statistic highlights relevance to the importance of suitable and efficient Occupational Therapy (OT) services for the prevalent needs of this population at this level of care.
Challenges in students defining their roles in PHC settings
Occupational Therapists play a vital role in Primary Health Care (PHC) settings in South Africa, particularly in providing accessible, community-based rehabilitation services. Despite the importance of this role, there remains a significant gap in the understanding of occupational therapists’ contributions to PHC among students. This lack of clarity is especially evident among occupational therapy students during their community service years, where they often struggle to deliver effective services due to limited knowledge and practical application of the PHC approach. An additional concern is the limited opportunity for students to engage in interprofessional practice and collaboration, which are essential components of effective PHC service delivery. Occupational therapists within the District Health Services (DHS) are expected to align their services with PHC principles, emphasizing community-level interventions. This challenge is further exacerbated by the current occupational therapy curriculum, which emphasizes remedial hospital-based rehabilitation, and provides limited preparation for the demands of PHC practice (Naidoo et al., 2017).
The incomplete integration of occupational therapy services into PHC settings in South Africa can be attributed to resource constraints, lack of awareness, and educational gaps. This results in an ongoing lack of clarity regarding the role of occupational therapists in PHC, ultimately limiting their potential contribution toward addressing the diverse health needs of communities and achieving universal health coverage.
Anecdotally, the occupational therapy curriculum has been criticized for being overly packed, leaving students with limited time and opportunities to fully integrate theoretical knowledge with practical application (Naidoo et al., 2017). At the University of KwaZulu-Natal (UKZN), PHC principles are introduced in the first, second, and third years of study through theory-based learning. However, the practical application of these principles is confined to a single six-week community-based fieldwork placement in the fourth year. This fieldwork, conducted at selected community clinics in KwaZulu-Natal, such as Cato Manor, Mariannridge, and Kenville, is critical for translating theoretical knowledge into effective practice at the PHC level. The limited duration of this placement, coupled with the diverse needs of patients in PHC settings, places significant pressure on students to deliver effective and contextually appropriate services within a short timeframe.
Pros of the UKZN OT Curriculum in Preparing Students for Community and PHC Settings:
• Early Introduction to Community Engagement: First-year occupational therapy students participate in the HLSC116 Community Studies module, which includes approximately three observational visits. Additionally, there are four weekly community engagements, providing early exposure to community settings.
• Theoretical Foundation in PHC Principles: Throughout the first three years, the curriculum introduces PHC principles, providing students with a foundational understanding of community health dynamics.
• Community-Based Fieldwork Placement: A six-week placement in the fourth year at community clinics, such as Cato Manor, Mariannridge, and Kenville, offers students exposure to real-world PHC environments, facilitating the application of theoretical knowledge.
Cons of the UKZN OT Curriculum in Preparing Students for Community and PHC Settings:
• Limited Practical Exposure in Early Years: In the second year, there is no community engagement, leading to a gap in continuous practical exposure to community settings.
• Short Duration of Community Engagement in Third Year: During the third-year psych block, students attend community settings once a week in the second semester, but the sessions are brief (12 PM to 3 PM) and primarily involve assisting fourth-year students, limiting active participation.
• Hospital-Centric Training: An emphasis on hospital-based rehabilitation can leave students underprepared for the distinct challenges of community-based settings.
• Curriculum Overload: The dense curriculum may restrict opportunities for students to integrate theoretical knowledge with practical application, particularly in community contexts.
• Insufficient Interprofessional Collaboration: Limited opportunities for interprofessional practice during training can hinder the development of collaborative skills essential for comprehensive PHC delivery.
Reflecting on my own experiences, the limited community exposure throughout the curriculum has left me feeling inadequately prepared for PHC settings. The observational nature of first-year community visits and the brief third-year exposure may not be sufficient for developing hands-on skills in community settings. Extended and more interactive community placements could enhance our practical experience. Opportunities for working alongside professionals from other disciplines appear limited and could be enhanced by collaborative learning experiences with students from other health disciplines to foster a team-based approach, essential for effective PHC delivery. Integrating interprofessional practice into the curriculum could enrich our understanding of collaborative care in PHC. Regular evaluations to ensure that course content and fieldwork opportunities are tailored to meet the evolving needs of PHC can better prepare us students for real-world challenges.
To better equip graduates for PHC settings, OT educational programs should aim to produce ethically grounded and socially responsible practitioners. This involves shifting the curriculum focus from predominantly hospital-based individual care to promoting wellness and population health within community settings (Naidoo & Van Wyk, 2023). Curriculum designers must consider the needs of all stakeholders, integrating opportunities to develop, model, and assess competencies relevant to PHC. While acknowledging existing curriculum constraints, such as content overload, these adjustments are essential for aligning educational outcomes with the evolving demands of South Africa’s healthcare landscape (Naidoo & Van Wyk, 2023).
References
Health hosts South African Primary Health Care Conference, 15 to 16 Nov | South African Government. (2023, November 14). Www.gov.za. https://www.gov.za/news/mediaadvisories/conferences-summits-seminars-and-workshops/health-hosts-south-african-primary
Naidoo, D., & Van Wyk, J. M. (2023). Competencies Required to Deliver a Primary Healthcare Approach in the Occupational Therapy: A South African Perspective. Occupational Therapy International, 2023, 1–14. https://doi.org/10.1155/2023/4965740
Naidoo, D., Van Wyk, J., & Waggie, F. (2017). Occupational therapy graduates’ reflections on their ability to cope with primary healthcare and rural practice during community service. The South African Journal of Occupational Therapy, 47(3), 39–45. https://doi.org/10.17159/2310-3833/2017/v47n3a7
Naidoo, D., Van Wyk, J. V., & Joubert, R. W. E. (2016). Exploring the occupational therapist’s role in primary health care: Listening to voices of stakeholders. African Journal of Primary Health Care & Family Medicine, 8(1), 9. https://doi.org/10.4102/phcfm.v8i1.1139
0 notes
Text
UKZN OT Curriculum, preparing students for Community Practise
According to a quick internet search, there are 7 different Universities in South Africa that offer the Bachelor of Occupational Therapy Degree, with the University of KwaZulu Natal being the only one situated in KZN. Like most Health Sciences degrees, the Occupational Therapy Degree period of study is 4 years, with the students graduating with an Honors Degree. Occupational Therapy students are fortunate enough to be allocated to places to do Community Service for the year after completing their degree. That certainly takes a load off

A few weeks ago, I, a 4th-year occupational therapy student, also found myself having to apply for various possible placements for CommServe 2025, in case I pass of course. And yes, it could go either way. I suffer from a lot of things as a student, but ‘Dilulu’ isn’t one of them. I am not going to pretend like it's been a walk in the park and that I have this in the bag. It has been quite a struggle with honestly, more downs than ups. I have shed more tears for this degree than I have ever shed for anything, and probably acquired lifetime traumas along the way…. Sorry, my subconscious self took over there for a minute. What were we even talking about? Oh yeah, the Occupational Therapy Curriculum.
Okay, before we delve into the curriculum, can I just say just how much respect I have for this profession and the discipline? According to multiple conversations I have had with students (both within the Occupational Therapy Discipline and in other Disciplines), a lot report that they feel that the Occupational Therapy discipline is arguably one of the most hard-working disciplines in the UKZN Westville Campus. Inkosi impela baqinisile uma bethi “le Degree akuyona eyolamthumthu ripped arm emoji”(it is not for the weak or faint-hearted.
From the very first step in the first year, being introduced to 4 Anatomy modules, after not having gone any further than human reproduction in the 12th grade, that is quite a leap. But before I go any further, I have to be honest.
In the topic of the UKZN OT curriculum preparing students for practice, I don’t think I'm part of the best generation to comment accurately on that topic. As part of the COVID-19 student generation, we probably did not experience the OT curriculum at its very best. As the pandemic was relatively new in 2021, everyone was still integrating into online learning. Almost every lecture and class was held online, including Anatomy spotters and ironically, Community Studies lectures. Get it? Community Studies lectures online, with students not able to visit the community they are training to serve rolling eyes emoji. So that’s how we began our journey, with online classes and online tests, robbing us of a true university experience.
Fast forward to the 2nd semester of the second year, where we were integrated back into normal university life. A huge transition, from barely ever attending contact lectures to attending full-time. With no time to ease into it, we were thrown into the deep end.
I recently took a look at a research study by Thavanesi Gurayah (2022), which aimed “to explore facilitators and barriers to completing an occupational therapy degree at the University of KwaZulu-Natal” by interviewing 7 graduates from the Class of 2015. According to said study, the graduates interviewed found the OT curriculum “academically challenging”. However, the study concluded by saying that the participants reported that the experience gave them the “opportunity for personal growth.”
I am afraid to report, that I do not share the sentiment. Personal growth, at what time? Under the UKZN OT curriculum, the students are overworked, with barely any chance to recover from one block to another. As for preparing students for working in the community level, it is hard to say given that we were not exposed to working in/with actual communities until the very last year, and for a 6-week block, like that’s supposed to be enough?
I have to be honest, I envy the Class of 2015. From the study, they seem like they have positive remarks to make about The UKZN OT curriculum. I wish I could also say despite all the rollercoasters, I found a way, an opportunity for “personal growth”. I wish I could talk about anything other than the traumas, self-doubt, and emotional scars I have acquired under this discipline. I don’t know. Maybe someday I might look back and find great things to say about the experience here. Maybe someday, but that day is not today.
REFERENCES
Thavanesi Gurayah. (2022). An Exploration of the Facilitating Factors in Completing an Undergraduate Occupational Therapy Degree at the University of KwaZulu-Natal, South Africa. Africa Education Review, 19(3), 1–18. https://doi.org/10.1080/18146627.2023.2278050
0 notes
Text
The Future of Occupational Therapy and My Journey to Prepare.
I’m a 3rd-year Occupational Therapy (OT) student at the University of KwaZulu-Natal (UKZN), and I’m passionate about the field. Over the past 12 weeks, I’ve had the opportunity to visit various clinical sites and put the theory I’ve learned into practice. It’s been an eye-opening experience, and I feel more connected to OT than ever before. As I look ahead to my final year and beyond, I’m excited about where the profession is heading and how I’m preparing for it.
Why Occupational Therapy Has a Bright Future?
Occupational Therapy is increasingly recognized as an essential part of healthcare. Historically known for physical rehabilitation, OT has expanded to include mental health, cognitive rehabilitation, and more. The future is promising because OT helps individuals live full and meaningful lives, whether they’re recovering from physical injuries or managing mental health conditions. According to the World Federation of Occupational Therapists (WFOT), OT plays a crucial role in promoting health, well-being, and independence across all ages.

Mental health is a growing focus within OT. As awareness of mental health issues increases globally, so does the recognition that OT has a unique role in this area. Through therapeutic activities and a client-centered approach, OT helps individuals develop coping skills, improve emotional regulation, and reintegrate into everyday life. This makes OT vital in the broader mental health field.
Technology is also revolutionizing OT practice. The use of telehealth, for example, is allowing occupational therapists to reach clients in remote areas. Research shows that telehealth has been effective in providing OT services for individuals who have limited access to traditional in-person care, especially during the COVID-19 pandemic. Assistive technologies, such as adaptive devices, are helping clients achieve greater independence, another key trend driving the future of OT.

How I’m Preparing for This Future.
During my 12 weeks of practical experience, I’ve worked with a variety of clients, including those with intellectual disabilities and mental health conditions like schizophrenia and Bipolar Mood disorder. These experiences have not only helped me develop clinical skills but also taught me how to be adaptable and empathetic in diverse situations. As OT moves toward a more holistic and individualized approach, these skills will be crucial.
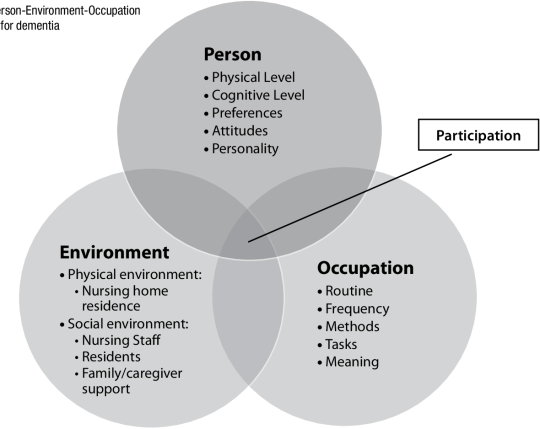
I’m also learning to apply different models of care. The Person-Environment-Occupation-Performance (PEO-P) model has been particularly useful in understanding the complex interactions between individuals, their environments, and their daily activities. By considering these factors together, I can better plan interventions that are both client-centered and goal-oriented.
Cultural sensitivity is another area I’m focused on. In South Africa, many people hold traditional beliefs that influence how they view health and healing. Learning how to respect and integrate these beliefs into OT practice will be essential as the profession continues to expand into more diverse and multicultural settings. Cultural competence has been shown to improve therapeutic outcomes and build trust with clients.
Next year is my final year of the 4-year OT degree, and I’m excited to continue building on what I’ve learned. I’ll take on more responsibilities in my clinical placements, further refining my skills as I prepare to enter the workforce. Whether I end up working in mental health, paediatrics, or community-based settings, I’m committed to making a meaningful impact in people’s lives.
The future of OT is full of possibilities, and I’m ready to be part of it. With a combination of hands-on experience, theoretical knowledge, and a passion for helping others, I believe I’m well-prepared to face the challenges and opportunities ahead.
REFERENCES.
Davis, R., & Smith, L. (2019). Cultural competence in occupational therapy: A guide for practitioners. OT Practice, 24(5), 24-30.
Hayes, L., & Lannin, N. (2020). The role of OT in mental health recovery. Journal of Mental Health Therapy, 15(3), 45-57.
Law, M., Cooper, B., Strong, S., Stewart, D., Rigby, P., & Letts, L. (1996). The person-environment-occupation model: A transactive approach to occupational performance. Canadian Journal of Occupational Therapy, 63(1), 9-23. https://doi.org/10.1177/000841749606300103
O’Brien, J., & Hussey, S. (2022). Telehealth in occupational therapy: Access and outcomes in remote areas. OT International, 8(2), 101-115.
World Federation of Occupational Therapists. (2021). Promoting the profession of occupational therapy worldwide. World Federation of Occupational Therapists. https://www.wfot.org
0 notes
Text
Cynthia Chiang Is Searching For Signs of The Universe's First Light
The cosmologist builds her own equipment, and deploys it to the edges of the Earth, to get a hint of how the cosmos came to be.
— July 24, 2024

Cynthia Chiang. Photograph By Mark Thiessen, National Geographic
“It was written in some sense,” that National Geographic Explorer Cynthia Chiang would end up in observational cosmology — the study of the origin and development of the universe using specialized detectors and telescopes. “I’m not going to lie, my father was a physicist. My mother’s an astronomer. But no kid wants to be like their parents,” she jokes, semi-seriously.
Chiang always enjoyed building things. It wasn’t unusual for her to experiment with her father’s research equipment; disassembling vacuum chamber components and putting them back together like a child engineer. She thanks, in part, her short attention span for her evolving curiosity: “I am always looking for something.”
For the last few years, Chiang has been looking for signs of the universe’s early existence — from the birth of the first stars more than 13 billion years ago, to the preceding “cosmic dark ages” — and she’s building her own equipment to do it. As a professor of physics at McGill University, she focuses on peering beyond the universe as it is known today, into its distant past, using novel radio technology.
Since 2017 Chiang and her team at McGill have been engineering and planting radio telescopes in two of the Earth’s most remote (and quietest) places for the best shot at hearing the earliest groans of the cosmos.
Initially, Chiang planned to do her PhD in particle physics but switched direction after a visit to a lab at the California Institute of Technology. “It was complete chaos. There is cryogenic equipment everywhere, tools everywhere. I didn’t know about observational cosmology at the time but thought ‘Whatever this is, I want to do that.’”
She spent a year as a winter-over scientist at the Amundsen-Scott South Pole Station after working on a few experiments in Antarctica during her PhD and postdoc. One was a balloon-borne microwave telescope that was launched from McMurdo. She could have familiarized herself with telescopes in Hawaii; it was a competing opportunity when she was first offered to go to the South Pole.
“That really catalyzed my love of remote places because it didn’t take me a second to decide…To this day I still have not been to Hawaii.”
Chiang worked as a Dicke postdoctoral fellow with a team of telescope scientists at Princeton University monitoring the cosmic microwave background (CMB) — the remnant radiation left over from the Big Bang.
Eventually, she wanted to engineer her own instruments. After her year at the South Pole Station, she accepted a job at the University of KwaZulu-Natal (UKZN) in South Africa. At that time, the site decision was made for the largest radio telescope array on Earth — the Square Kilometre Array — and two-thirds of it was awarded to South Africa.
“If We See These Childhood Photos of The Universe, Then We Can Understand The Factors That Affected Its Growth and How It Evolved To Be What We Call Home Now.” — Cynthia Chiang
“This was also a leap of faith because I really couldn’t continue the work I was doing before,” Chiang recalls. “I had never done radio before but I thought, ‘Let me give this a try and see how it goes.’”
It was her entry point to cosmic radio waves, from cosmic microwaves.
A Matter of Tuning In
Chiang is wearing a glow-in-the-dark, constellation-adorned dress. To be clear, she is not an astronomer, though her mother is and probably would have loved for her to be too. “Astronomers study stars and planets, fine details in the sky. They can tell you what the constellations are. Please don’t ask me that,” she jokes. Chiang has her own specialty. As a cosmologist, she’s interested in the bigger picture. “We do statistics. And for a long time we did not have data, we were just doing simulations. It really started with Edwin Hubble.”
Hubble’s Telescope kicked things off in the 1900s, and precision cosmology wouldn’t come into existence until the 1980s.
To date, cosmologists have been able to make direct observations as far back as the Big Bang afterglow, the cosmic microwave background. Chiang describes it as “a snapshot of the universe when it was born.”
What can be seen of this time, which was before the birth of the first stars, otherwise known as the “cosmic dawn”, is “like a photo, a two-dimensional thing,” around 400,000 years after the explosive genesis of the universe.
Six years ago, Experiment to Detect the Global EoR Signature, a radio observation experiment based in Australia, may have captured the only verified record of the cosmic dawn, but what they detected needs a cross-check to confirm it was real.
“We’re motivated to resolve this question because the payoff would be huge,” Chiang says.
She compares the age of the universe when the first stars ignited to a human toddler: “And a toddler looks different than an adult. If we see these childhood photos of the universe, then we can understand the factors that affected its growth and how it evolved to be what we call home now.”
It’s really hard to obtain what she and other scientists are after. The portal is hydrogen. Chiang breaks down how the universe evolved during the cosmic dark ages, before the first stars turned on:
“The universe was filled with, to good approximation, nothing but hydrogen. Some helium as well but mostly hydrogen. It was dark and boring. It turns out that if you can measure where hydrogen lives during this period of darkness, it’s like getting a three-dimensional scan instead of a two-dimensional photograph.”
Similar to an FM car radio, Chiang’s telescopes measure light at radio wavelengths. Though ideally, they don’t pick up all the human-generated noise, just the signals emitted by hydrogen when the universe was giving birth to itself. Hydrogen emits a unique glow and its wavelength is directly proportional to its distance from Earth. The further away the light is, the older it is.
“So if we want to study any part of the universe’s history, we can tune into the right wavelength. The wavelengths we want to catch are very, very faint,” and very, very old.
Hence why Chiang has to plant her instruments away from it all, at the ends of the Earth.

One of the antenna stations of the ALBATROS radio astronomy experiment, installed at the McGill Arctic Research Station. Photograph By Anthony Zerafa
“Impulsiveness and a bit of mischief,” she says, have characterized her journey through the cosmos. “And a lot of coincidences afterward. It was not too long after I started radio in South Africa that we found out about Marion Island.”
Dodging Human Noise
About halfway between South Africa and Antarctica, 2,000 kilometers (1,243 miles) from anything else, Chiang found a researcher’s paradise. Chiang’s husband and collaborator spotted Marion Island in an in-flight magazine while the two were en route to South Africa.
One of the most remote regions on Earth, Marion Island is an ideal place to get away from radio foreground contamination. In 2018, Chiang and a team of scientists planted Probing Radio Intensity at high-Z from Marion (PRIZM). Designed by the team at McGill and UKZN, PRIZM is an instrument looking for a 21-centimeter signal emitted by hydrogen, stretched to the frequency of the universe’s first billion years.
PRIZM collected data through 2023 as weather permitted on Marion. At times the conditions were too dangerous to hike to the site of the telescope, which was intentionally set up several kilometers away from the island’s main research base. Throughout the year, the instruments, and their caretakers, were battered by wind, salt spray and invasive species. “If it’s not the salt water, it’s the mice.”

Marion Island is a South African research base located in the sub-Antarctic. The island is uniquely radio quiet for astronomical observations. Chiang’s radio telescope installations are sited behind the central hill in the photo, a few kilometers away from the research base that is visible in the foreground. Photograph By Mohan Agrawal
The data analysis is still in process, but so far, Chiang has high expectations for its pristineness. As a follow-up, Chiang works as a co-investigator on Mapper of the Intergalactic Medium Spin Temperature (MIST). The new-generation experiment, developed in 2020, is being conducted from the Arctic. “The MIST analysis is going to be super fun. We normally have a wall of radio stations just killing our cosmic dawn signal. This is wide open for us and it’s clean.”
On another side of the planet relative to Marion, the team identified a different radio-quiet base in the Canadian High Arctic to plant MIST and another telescope array that will look even further back in time. MIST's companion experiment “is part of a longer, crazier frame I have,” Chiang explains. “The cosmic dark ages.” This epoch has never been observed and is uncharted territory in the universe's history.
Array of Long Baseline Antennas for Taking Radio Observations from the Sub-Antarctic/Seventy-ninth parallel, or ALBATROS for short, is a network of antennas the team is building up now. The array is sprinkled across Axel Heiberg Island, and the idea is the antennas will work together to take pictures of the radio sky. “That means the timing has to be consistent. We have to have a common heartbeat between antennas that are separated by many kilometers. That’s a huge engineering challenge.”
So far there are four in place, and the team is aiming for eight. Each year the goal is to install between three and four, but the reality of the challenging landscape keeps bringing the number down. “Last year it was because of a helicopter crash. Everyone’s okay, thankfully. Two years before it was because of weather delays,” Chiang says.
“Our ‘station’ — I say station in quotes because it’s three buildings — it’s a slapdash operation. We try to make the best of it by going one step at a time,” Chiang says. “The upshot is there is no winter population,” and thus, no noise. In general, there’s not much.
“The first question I usually get asked about working in the Arctic is ‘Do you get to shower? What are the toilets like?’ We don’t have to dig holes. There is a spot, up the hill, around the corner, a really nice view of a glacier while you’re contemplating life and other things,” she reassures.

In this remote researcher's paradise, Axel Heiberg Island in the Canadian High Arctic, the team's outhouse is equipped with an ice axe toilet paper holder. Photograph By Cynthia Chiang
Because of the weather, the instruments are set up and left to run autonomously for a year. It’s also important that ALBATROS, which is trying to pick up the lowest frequencies, runs through the Arctic winter — when solar activity is at a minimum and interferes least with the Earth’s ionosphere. This provides the highest chance for clean data. “The ionosphere basically scrambles and blurs radio signals as they travel through, and the lowest frequencies are blocked entirely,” Chiang explains.
Some instruments, expectedly, have died part way through the winter. Some things have survived. “For me, that’s a huge win. It’s beyond what I could have ever dreamed before,” says Chiang. The team is still installing the array, so pictures haven’t been made yet, but overcoming technical challenges while building instruments from scratch is a successful start.
“Our credit really goes to our amazing students. They have spent countless hours, years, testing software and hardware to make sure it survives for a year, that if there is a glitch in a computer it will reboot on its own and take care of itself. It’s a huge amount of work.”
The first picture ALBATROS is aiming for will be of the closest view from Earth — the Milky Way galaxy — which is just clutter in the foreground when trying to peer billions of years into the past. “The Milky Way is much brighter than anything from the dark ages. We want to see if it’s even possible to get a nice picture of the Milky Way to start,” Chiang explains. Then effectively, subtract the Milky Way from the bigger picture.
“The state of the art we have in terms of what the Milky Way looks like at the lowest frequencies dates from the ’60s. That’s the best we have.”

McGill students Tristan Ménard, Larry Herman, and Joëlle Bégin install an ALBATROS radio antenna at the McGill Research Station on Axel Heiberg Island. Photograph By Anthony Zerafa
What sets Chiang’s instruments apart from larger telescopes, like the infrared vision James Webb Space Telescope, also trying to peer into the formation of the first stars, is that they do broad strokes. Even as small-scale experiments, MIST and ALBATROS gather big-picture data that complement the detailed view from the world’s largest telescopes.
Over the next few years, Chiang and her team will continue installation and observation in hopes of getting a good look at the universe in its infancy. The sun’s activity cycle will also play a part. When the solar minimum arrives in a few years, that’s when the best pictures will be taken. In the meantime, Chiang will work on imaging the Milky Way, and refine her instrumentation.
“That’s a fun aspect about building the instruments ourselves, we get to customize.”
Chiang estimates the science may be a decade off if not more when it comes to detecting the cosmic dark ages, “but you start one step at a time,” and leave room for surprises.
She references a quote by mathematical physicist Freeman Dyson: “What we’re really hoping for is new and unexpected discoveries because nature’s imagination is richer than ours.”
1 note
·
View note
Text
A Course of Bricks, Ticks and Info that will Stick (hopefully) 🧳
The last four years I spent carrying around my eye suitcases (they've upgraded from being eyebags) trying to keep up with the curriculum better be worth whatever is to come in the future.
The University of KwaZulu-Natal (UKZN) is an institution that prides itself on offering a diverse range of courses to complete, good facilities to offer practical experience and great opportunities to network with others through the various events that take place. What it does not account for is the potential burnout that students may be experiencing, as well as the threat of failure that hangs over their heads.
The UKZN OT degree is a four-year degree that includes an Honors year. What the three undergraduate years consist of is various practical blocks focusing on engaging the learner in interventions regarding physical conditions and psychological conditions. While the exposure to these conditions is helpful and good for experiential learning, the environment in which we learn is often quite restricted and limited. (Undergraduate Programmes - Discipline of Occupational Therapy, 2019)
Do I, personally, feel like UKZN OT degree has prepared me for working at a community and primary healthcare level?
No, not at all, and this is my evaluation of it.
Pros:
Comprehensive Understanding of Community Health, at least, in theory:
The curriculum includes modules that focus on community-based questions and practical experience, as well as, primary healthcare. This module is the clinical studies done in first year, along with the OT fundamentals module being incorporated this year. This creates a good theoretical fundation in order to understand the community in terms of the social determinants of health, their assessments and heath promotion stategies. By using tools like the CBR matrix or PESTLE analysis taught in class, my practical group will be able to provide good analysis of the community. (Lysack et al., 1995)
Inter-professional Education and Collaboration (IPE):

IPE is emphasized in every lesson by the lecturers, citing that collaboration between different parts of the health science field will benefit us in the future and will provide a more holistic, conclusive report about the client’s presentation. This prepares OT students to work effectively in multidisciplinary teams (MDTs). (MacQueen et al., 2001)
This was evident on our first Wednesday in the community. Upon reaching the clinic, we had a short meeting with the Community Health Workers (CHWs) about the area and had a short orientation to the area. What we learned was that substance use is a common condition amongst the youth in the community and gained referrals for adult clients as well.
Focus on Advocacy and Policy:

OT education at UKZN includes components that educate students about advocacy for social justice and healthcare policy. This empowers us as the future to the health science field to advocate for improved healthcare services and policies that benefit underserved communities. In this way, UKZN teaches us that we are capable of creating a ripple on the surface of a system that has been running since before we were born, but also that we need to respect the space that the community has given to us.
One of the most important lessons that I have learned is that it is best to communicate with the people you are trying to help instead of making the project independently as it is best to receive some feedback on the activities that will be included in order to make it more client-centred.
Cons:
Limited Exposure to Rural Health Challenges:

The curriculum often incorporates clinical placements in semi-urban and urban areas. This hands-on experience allows students to apply theoretical knowledge in real-world contexts, develop essential clinical skills, and understand the challenges and dynamics of working in community settings. Despite efforts, there may be limited exposure to the unique challenges faced by rural and remote communities in South Africa. More emphasis on rural health issues and specific strategies for overcoming geographical barriers could better prepare us for practice in these settings. (Harper et al., 2022)
For example, my first psychosocial block was in a private facility. Had I not been placed in a semi-urban area for my second block, the shock of coming to the community for the first time in fourth year would have affected my treatment for the first week as I would still need to become familiar with certain ideas.
In conclusion, the UKZN curriculum for OT provides an idea of what working in the community and in primary healthcare is like and provides essential theoretical information about skills that are needed in community. Due to a lack of experience in different types of areas in the clinical environment in previous blocks and a poor control of who goes to which placement during the three undergraduate years, not everyone is able to have the same exposure to different areas and have never experienced a different sense of community.
There are no words to describe what being part of the community feels like, even if it just for six weeks, therefore, my suggestion is to continue with the exposure to community that the first and third years are currently experiencing as it gives them an idea of how the block will be completed instead of being thrown in the deep end with a heavy suitcase filled with theoretical information that is hard to process, let alone implement in a completely new environment.
But what happens if I let the suitcase fly open?

This is Husna, signing OuT!
References:
Harper, K. J., McAuliffe, K., & Parsons, D. N. (2022). Barriers and facilitating factors influencing implementation of occupational therapy home assessment recommendations: A mixed methods systematic review. Australian occupational therapy journal, 69(5), 599–624. https://doi.org/10.1111/1440-1630.12823
Lysack, C., Stadnyk, R., Paterson, M., McLeod, K., & Krefting, L. (1995). Professional Expertise of Occupational Therapists in Community Practice: Results of an Ontario Survey. Canadian Journal of Occupational Therapy, 62(3), 138–147. https://doi.org/10.1177/000841749506200305
MacQueen, K. M., McLellan, E., Metzger, D. S., Kegeles, S., Strauss, R. P., Scotti, R., Blanchard, L., & Trotter, R. T. (2001). What Is Community? An Evidence-Based Definition for Participatory Public Health. American Journal of Public Health, 91(12), 1929–1938. https://doi.org/10.2105/ajph.91.12.1929
Undergraduate Programmes - Discipline of Occupational Therapy. (2019, July 18). Ot.ukzn.ac.za. https://ot.ukzn.ac.za/undergraduate-programmes/
Picture References:
370+ Muslim Nurse Illustrations, Royalty-Free Vector Graphics & Clip Art - iStock. (n.d.). Www.istockphoto.com. https://www.istockphoto.com/illustrations/muslim-nurse
Andy Milne. (2022, June 6). Teaching Health Advocacy. #Slowchathealth. https://slowchathealth.com/2022/06/06/teaching-health-advocacy/
Interprofessional teamwork: Nursing - Osmosis Video Library. (2022). In osmosis.org. https://www.osmosis.org/learn/Interprofessional_teamwork:_Nursing
The Integrated Urban Development Framework (IUDF) – Cooperative Governance and Traditional Affairs. (2016). Cogta.gov.za. https://www.cogta.gov.za/index.php/the-integrated-urban-development-framework-iudf/
0 notes
Text
The end or the beginning?

(Msethnablog, 2017)
I have been a student at UKZN for almost four years now, and I have experienced a rollercoaster of experiences. I feel as if I have trekked up a steep rocky hill and have the peak in my view where I jump into the waters below. I have experienced online learning, working in extremely privileged and underprivileged facilities, which assisted in preparing myself for the unknowns in the communities in which I have worked; I have had to change my own perspective on the practice and hearing the community experience through whispers in the wind to now experiencing it on my own. I ask myself, am I prepared for primary health care practice? Walk this journey with how primary health care has moulded me as an Occupational Therapist as I emerge as an aspiring primary healthcare practitioner in community practice.
What is primary health care? “Primary health care is a whole-of-society approach to effectively organize and strengthen national health systems to bring services for health and wellbeing closer to communities.” (World Health Organization, 2019).
See the links below to watch a video to learn more about what primary health care is, an FAQ that I found helpful in understanding it.
youtube
youtube
How has the UKZN curriculum prepared me for it? There are definitely pros to the curriculum, but there are also cons. Let us start with one of the pros: having lecturers who would provide extra readings despite not being obligated. I would find myself becoming curious about the topic due to the one reading that was recommended. One AFR piqued my interest, which was mentioned in passing. Little did I know that months later, I would preach the principles and implement them into my practice with substance use cases to prioritize the client's needs. It evolved the view of therapy as the client was more engaged and applying the psychoeducation, highlighting that “I see you”.
I started the degree during lockdowns and other school disruptions, such as floods and load shedding. This required a dramatic shift in the curriculum to accommodate safety regulations while delivering lectures. So, I did not experience being in a community from the start; I had to rely on people's opinions and images. This did not provide much on the community and I did not get to actually experience the communities, observe the people, the environment, and the interactions between them. Having such a subjective view of community practice did not prepare me for community practice. I have not heard much about the academic aspect of PHC practice. It has always been an idea on a page. However, I must note that this may not be a true reflection of the standard curriculum since this was during the pandemic.
We have been taught in silos. We would have a semester dedicated to the different aspects of Occupational therapy. In the final year, we had 4 blocks. This then “taught” us to have different Occupational therapy hats. One for paediatrics, one for physical, and one for psychosocial. As a student, I struggled to switch hats because there were short (or no) breaks between blocks. Community practice requires you to tap into all 3 hats to provide therapy and understand the community and how to treat within the community. This then limited me in the flexibility and adaptability of my thinking of practice, which is divided rather than holistic in the community.
In the other blocks, we mostly worked in hospitals. Which are quite resourced; there is a hospital bed that can be adjusted, step stools, and useful items just waiting to be used. “South Africa is a country in deep organic crisis, requiring interventions that can help developments and social justice challenges; and yet the higher education system prioritises research and teaching to the exclusion of CE.” (Dube, 2023). The lack of resources to intervene sustainably limited me in the choices of what therapy I could then provide to the individuals in the MR community. I have had to use to fight a battle between sustainability and effectiveness, asking myself if I am doing enough?
A huge pro is the decentralised training. I was placed in Manguzi Hospital, a rural hospital with a firm stance on practising primary health care. I could tag along on multidisciplinary home visits, which the hospital funded, which, in my opinion, all hospitals or health services should aim to do as the country is moving to a shift to primary health care. I stayed longer hours than other blocks willingly. I was tired, but I was fulfilled. I discovered a rural rehab organisation I would like to join once I am qualified. See the link below to read more about RuReSA.
I had come to realise how you can encourage the community to take charge of their own health by simply being in a space they are comfortable in. This also started the thought: How can I make my own therapy spaces more comfortable?
In this discipline, little to no therapy is set in stone. The techniques, principles, and models are the same, but how each individual treats a client is different. In some cases, the learnings I have taken from previous blocks were completely shut down by the supervisor for that block. I had found myself in a state of uncertainty and questioning what I should do as I want to do my job as a therapist, but I am also a student. I have had to learn how to justify my means and explain the theory behind my actions. This also pushed me to read further and better understand the theory behind the actions. So, essentially, this is a pro.
This was achieved by changing to become more self-directed. Now, what is self-directed learning? To my understanding, it is self-motivated learning. I am taking the initiative to learn more and read more. “Self-directed learning is an approach to education that empowers learners to lead their own learning journey.” (Germeroth, 2024). Adjustment is what I needed. How was I supposed to fly when my wings could not support my weight? I talk about coping and adaptability in therapy. It called me to shift from a spoon-fed the first year to becoming a self-directed learner aiming to strive in community rehab. Rather than calling it guidance, it was a shove onto the right path of growth and diverse skills to ensure that the therapy is meaningful and client-centred.

(Beveridge, 2021)
See the link below, which explains more about lifelong learning.
To conclude, I feel that this curriculum has its ups and downs; on a subjective level, one would sometimes feel frustrated. However, it has reinforced that I have to be a self-directed learner, and it has tested my confidence in my own skills and pushed me to do better. I have learnt that in order to bring the therapy to the community I have to flexible, be adaptable and be a quick thinker, and importantly read more about what I have seen in order to have more of an understanding of community practice. To feel, see, be and become part of the community. Therefore, I feel that the curriculum does prepare us for community practice. But who knows where I will stand in the future once I have experienced more and reflected on it.
REFERENCES
Beveridge, B. (2021, August 12). Importance of Life Long Learning, a student perspective. Medium; Medium. https://rebecca2021.medium.com/importance-of-life-long-learning-a-student-perspective-5598182e9d2f
Dube, N., & A, H. E. (2023). The praxis and paradoxes of community engagement as the third mission of universities. a case of a selected South African university. South African Journal of Higher Education, 37(1), 131–150. https://doi.org/10.20853/37-1-5643
Germeroth, K. (2024, April). What is self-directed learning and what are its benefits? Moodle US. https://moodle.com/us/news/what-is-self-directed-learning/
Kuzmina, julia. (2022, February 17). Lifelong Learning: Meaning, Importance, Benefits & Examples. Valamis. https://www.valamis.com/hub/lifelong-learning
Msethnablog. (2017, December 4). When Life Gets in the Way…and the Importance of Reflection. For the Love of Books, Tech, Coaching, and More; For the Love of Books, Tech, Coaching, and More. https://msethnablog.wordpress.com/2017/12/04/when-life-gets-in-the-way-and-the-importance-of-reflection/
World Health Organization. (2019). Primary health care. Who.int; World Health Organization: WHO. https://www.who.int/health-topics/primary-health-care#tab=tab_1
World Health Organization. (2019). Primary health care throughout our life [YouTube Video]. In YouTube. https://www.youtube.com/watch?v=QX7Q0a8GxaA&t=3s
World Health Organization . (2022). Primary health care: Bringing health services closer to communities [YouTube Video]. In YouTube. https://www.youtube.com/watch?v=_htX-EdAyuc&t=97s
0 notes