#Unfractionated heparin
Text


Anticoagulation Pharmacy Lecture
8/23/23
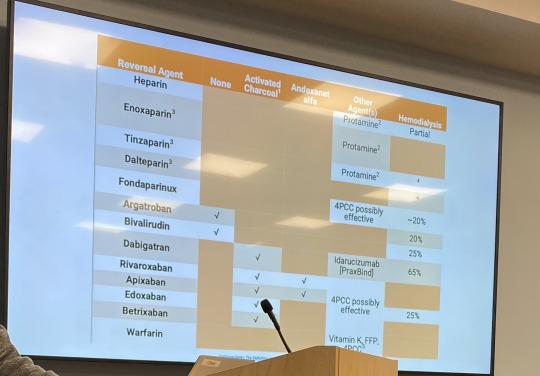
Unfractionated heparin (UFH) work on factors Xa and IIa; it binds to and potentiates the action of antithrombin to facilitate inactivation of factors Xa and IIa. Monitor with activated prothrombin time (aPTT). VTE ppx: 5000 U SubQ q8. VTE tx: 80 U/kg bolus, then 18 U/kg/hr continuous infusion. Adverse effects: bleeding, thrombocytopenia, infusion reactions.
Low Molecular Weight Heparin (LMWH) acts on factor Xa and thrombin a little bit. Works the same as UFH by binding antithrombin, which inhibits factor Xa. More predictable kinetics than UFH. Reversed with protamine. Grouped in with enoxaparin.
Enoxaparin for VTE ppx for pts >120 mg is 40 mg bid
Fondaparinux is a synthetic version of a piece of heparin, works to inhibit factor Xa, no effect on thrombin. Likely safe for pt with HIT. VTE ppx: 2.5 mg qd, unless pt is under 50 kg.
Heparin Induced Thrombocytopenia (HIT) – platelet factor 4 released from platelets binds to heparin and antibodies form against that complex. This activates the plateletsà thrombocytopenia and increased coagulability. 4T score of 0-3 is less than 1% possibility that the pt has HIT. If 4T score is hight, send for SRA (Serotonin-Release Assay). You have to stop heparin and start a different anticoagulant if pt has HIT. Direct thrombin inhibitors are safe to use for AC in pts who have HIT. These are argatroban and bivalirudin. Monitor these with aPTT. There’s no reversal agent for these. These prevent and treat thrombosis in the setting of HIT or if pt doesn’t respond to heparin. Bivalirudin is cleared renally. Argatroban is cleared hepatically.
Oral Anticoagulation
Warfarin – works on factors 7, 9, 10, and 2. It inhibits vitamin K epoxide reductase complex 1. Bridge with heparin because it inhibits proteins C and S, which are anticoagulants. Start 5 mg x2 days then check INR. Can do 2.5 mg if <50 kg; 7.5 mg if >120 kg. Vitamin K or KCentra can reverse warfarin. Warfarin pills have different colors for each strength of warfarin.
INR goals:
Non-valvular AFib: 2-3
DVT/PE: 2-3
Mitral mechanical valve: 2.5-3.5
Coagulopathies: 2-3
Factor Xa inhibitors: apixaban, rivaroxaban, edoxaban – for non-valvular AFib; no monitoring required, safe to use in HIT; reversed with KCentra or Andexanet Alfa (rivaroxaban and apixaban).
Apixaban C/I in severe hepatic disease.
Xarelto should be taken at night with evening meal (or biggest meal of the day to increase absorption); C/I with dialysis (increases bleeding risk). Pts on Xarelto who need dialysis should be on apixaban instead. Apixaban causes less GI and intracranial bleeding.
Savaysa (edoxaban) C/I in pts with CrCl > 95 mL/min
Dabigatran – direct thrombin inhibitor; no monitoring required; safe to use in HIT; reverse with PraxBind (idarucizumab). Dabigatran is very expensive. Expires 6 weeks after bottle opened. Renal adjustment.
Apixaban has been studied in cancer pts.
DOACs for obese pts: conflicting evidence; some evidence of altered kinetics. Modest reduction in AUC in pts >120 kg. AUC reduction doesn’t appear to affect the efficacy of the drug.
Warfarin reversal:
KCentra (prothrombin complex concentrate) has all the factors affected by warfarin and proteins C and S. Dosing: 1500 units for intracranial bleed; 2000 units for DOAC reversal. KCentra is very prothrombotic and dangerous; can cause a thrombotic event. The pharmacy will call you if you order it. KCentra should only be used for emergency bleeding in the ED.
You always give vitamin K (phytonadione) with KCentra. KCentra is short-term benefit. Vitamin K provides long-term benefit. Works in 12-24 hours.
INR 4 to 10, no need to give vit K. If INR >10 and no bleeding – just give vit K. If major bleed, give 5-10 mg IV vitamin K and KCentra. If pt needs urgent procuder, give KCentra.
Vitamin K dosing: 1000 units for intracranial bleed.
Andexanet and KCentra reverse apixaban (Eliquis). Andexanet binds Xa inhibitors.
Bridging: use short acting AC while waiting for long-acting AC to take effect. Can use heparin. Bridge x4-5 days and until INR is therapeutic for 2 measurements.
Heparin needs to be held 4-6 hours prior to surgery, warfarin should be held 5 days prior to surgery.
Resume warfarin 12-24 hours after surgery.
3 notes
·
View notes
Text
Lonopin Injection in Delhi: Uses, Availability, and Benefits
Uses and Indications
Lonopin injections are primarily prescribed for the prevention and treatment of conditions associated with blood clotting. These include deep vein thrombosis (DVT), pulmonary embolism (PE), and other thromboembolic disorders. In clinical settings, Lonopin is often used in hospitalized patients who are at risk of developing blood clots due to factors such as surgery, prolonged bed rest, or certain medical conditions.
Availability in Delhi
In Delhi, Lonopin injections are available in multiple strengths and formulations, ensuring healthcare providers can tailor treatment to individual patient needs. Lonopin Injection in Delhi They are typically prescribed by doctors specializing in cardiology, hematology, and internal medicine, among others. Pharmacies across the city stock Lonopin to meet the demand generated by hospitals, clinics, and healthcare facilities.
Benefits of Lonopin Injection
Effective Anticoagulation: Lonopin prevents the formation of blood clots by inhibiting certain clotting factors, thereby reducing the risk of potentially life-threatening conditions like DVT and PE.
Convenient Administration: Lonopin is administered through subcutaneous injection, making it suitable for both inpatient and outpatient settings. This ease of administration enhances patient compliance and ensures consistent therapeutic levels.
Predictable Pharmacokinetics: Unlike unfractionated heparin, Lonopin exhibits more predictable pharmacokinetics, reducing the need for frequent monitoring of coagulation parameters.
Lower Risk of Heparin-Induced Thrombocytopenia: Compared to unfractionated heparin, Lonopin has a lower risk of causing heparin-induced thrombocytopenia (HIT), a potentially severe complication characterized by a decrease in platelet count.
Safe in Pregnancy: Lonopin is considered safe during pregnancy, Folisurge 225 Iu Injection offering an important treatment option for pregnant women at risk of thromboembolic events.
Patient Education and Compliance
Patients receiving Lonopin injections in Delhi are typically educated about the importance of adherence to prescribed dosages and schedules. Healthcare providers emphasize the need for regular follow-up visits to monitor treatment efficacy and safety. Patients are also instructed on proper injection techniques to minimize discomfort and ensure optimal absorption of the medication.

0 notes
Text
The Role of Anticoagulants in Treating Multiple Subsegmental Pulmonary Emboli
In the realm of medical conditions, pulmonary embolism (PE) stands out as a potentially life-threatening condition that requires prompt diagnosis and treatment. While large pulmonary emboli are commonly discussed, the role of anticoagulants in treating multiple subsegmental pulmonary emboli is equally vital. In this blog, we delve into the significance of anticoagulants in managing multiple subsegmental pulmonary emboli and how this treatment plays a crucial role in patient care.
Understanding Multiple Subsegmental Pulmonary Emboli
When discussing pulmonary emboli, it's essential to recognize that these blood clots can vary in size and location within the pulmonary vasculature. While larger emboli are often more easily identified on imaging studies such as CT pulmonary angiography (CTPA), multiple subsegmental pulmonary emboli refer to smaller clots located in the smaller branches of the pulmonary arteries.
The Importance of Anticoagulants
. Preventing Clot Expansion: Anticoagulants play a crucial role in preventing the expansion of existing blood clots. By inhibiting the body's clotting cascade, anticoagulants help stabilize the existing clots, reducing the risk of further clot propagation within the pulmonary vasculature.
. Minimizing Risk of Recurrence: Patients with pulmonary emboli, including multiple subsegmental emboli, are at increased risk of recurrent events. Anticoagulant therapy helps mitigate this risk by maintaining the blood's ability to flow freely, reducing the likelihood of new clot formation.
. Preserving Pulmonary Function: Multiple subsegmental pulmonary emboli can impact pulmonary function by compromising blood flow to affected lung segments. Anticoagulant therapy aims to preserve pulmonary function by preventing additional clot formation and allowing existing clots to dissolve over time.
. Reducing Risk of Complications: Untreated or inadequately managed pulmonary emboli can lead to serious complications such as pulmonary infarction or chronic thromboembolic pulmonary hypertension (CTEPH). Anticoagulant therapy plays a crucial role in reducing the risk of these complications, improving patient outcomes, and overall quality of life.
Types of Anticoagulants Used
. Direct Oral Anticoagulants (DOACs): DOACs such as apixaban, dabigatran, edoxaban, and rivaroxaban offer convenient oral dosing and have demonstrated efficacy in treating pulmonary emboli, including subsegmental emboli. They act by targeting specific clotting factors in the blood.
. Warfarin: Warfarin, a vitamin K antagonist, has long been used for anticoagulation therapy. While effective, warfarin requires regular monitoring of international normalized ratio (INR) levels and dose adjustments, which can be cumbersome for patients.
. Heparins: Both unfractionated heparin (UFH) and low molecular weight heparins (LMWH) are commonly used as initial treatments for pulmonary emboli, especially in acute settings such as hospitalizations. They are administered via injection and require close monitoring of coagulation parameters.
Implementing Anticoagulant Therapy with patientselftesting
At patientselftesting, we recognize the critical role that anticoagulant therapy plays in managing pulmonary emboli, including multiple subsegmental emboli. Our comprehensive range of anticoagulation management services ensures that patients receive personalized care and optimal treatment outcomes.
By partnering with patientselftesting, healthcare providers gain access to advanced anticoagulation monitoring technologies, patient education resources, and ongoing support to facilitate seamless anticoagulant therapy management. Our goal is to empower patients to take an active role in their treatment while ensuring safety and efficacy throughout their anticoagulation journey.
In conclusion, anticoagulants play a pivotal role in treating multiple subsegmental pulmonary emboli by preventing clot expansion, reducing recurrence risk, preserving pulmonary function, and minimizing complications. With advancements in anticoagulation therapy and patient care, individuals can experience improved outcomes and a better quality of life following a pulmonary embolism diagnosis. Partnering with patientselftesting ensures comprehensive anticoagulation management and patient-centric care, ultimately contributing to better health outcomes and enhanced patient satisfaction.
0 notes
Text
Is Fondaparinux an Effective Alternative Anticoagulant in Patients With Heparin-Induced Thrombocytopenia Type II? A Case Report and Review of the Literature
Heparin-induced thrombocytopenia (HIT) type II is an acquired, transient, prothrombotic disorder and a life-threatening complication of unfractionated (UFH) and low-molecularweight heparin (LMWH) therapy presenting with thrombocytopenia and/or complicating venous or arterial thromboembolism that is associated with increased in vivo thrombin generation.[1,2] It is generally recognized that HIT can be divided into two types: HIT type I non-immune mediated HIT) and HIT type II (immune-mediated HIT).[3] For the remainder of this paper the term HIT indicates HIT type II. Heparin-induced thrombocytopenia is a clinicopathologic condition and adverse drug reaction caused by platelet-activating antibodies of IgG class which are directed against a molecular complex formed by heparin and platelet α-granule protein, platelet factor 4 (PF4).[4,5] Heparin-induced thrombocytopenia occurs in 3% to 5% and 0.5% of patients receiving UFH and LMWH, respectively.[6] In the absence of alternative anticoagulation, the risk of thrombosis is ~5% to 10% per day in the first few days after cessation of heparin[7] and mortality from HIT range from 18% to 50%.[3] Currently, direct thrombin inhibitors (argatroban, lepirudin) and danaparoid are approved agents as nonheparin anticoagulants for the prevention and treatment of HIT.
Although they are effective, all of this drugs have their limitations and adverse affects. The synthetic pentasaccharide fondaparinux, a subcutaneously administered indirect acting factor-Xa inhibitor, offers a new alternative for both prevention and treatment of HIT, especially where licensed drugs are not available. Here we report the successful use of fondaparinux in the treatment of a patient presenting with acuteon-chronic renal failure requiring hemodialysis and HIT associated with thrombosis (HITT). We also review the current role of fondaparinux in the treatment and prophylaxis of thrombosis in patients with HIT.
0 notes
Text
Increasing Aging Population to Boost Heparin Market Growth
As per Inkwood Research, the Global Heparin Market is set to progress with a CAGR of 4.01% in terms of revenue during the forecasting years 2024-2032.
“Browse 58 Market Data Tables and 51 Figures spread over 160 Pages, along with an in-depth TOC on the Global Heparin Market Forecast 2024-2032.”
VIEW TABLE OF CONTENT LINK - https://inkwoodresearch.com/reports/heparin-market/#table-of-contents
Heparin, an organic compound composed of a diverse array of molecules associated with carbohydrates, is primarily employed in laboratories to prevent blood coagulation in collected blood samples. Naturally occurring in the lungs and liver, heparin exists in two main forms: unfractionated and low molecular weight heparin.

REQUEST FREE SAMPLE LINK – https://www.inkwoodresearch.com/reports/heparin-market/#request-free-sample
Surging Geriatric Populace to Boost Global Heparin Market Growth
With the global population aging, there’s an increasing demand for healthcare solutions tailored to older individuals’ specific needs. According to the World Health Organization, the proportion of older adults is projected to nearly double from 12% to 22% between 2015 and 2050, with 1 in 6 people worldwide aged 60 or older by 2030.
Common age-related conditions like chronic obstructive pulmonary disease (COPD), atrial fibrillation, and coronary artery disease necessitate anticoagulant therapy, making heparin a crucial medication and contributing to market expansion.
Low Molecular Weight Heparin: Key Heparin Type by 2032
Light-molecular weight heparin (LMWH) is an anticoagulant medication designed to minimize the risk of blood clots, including conditions like pulmonary embolism and deep vein thrombosis (DVT). Derived from unfractionated heparin (UFH), LMWH has smaller molecules, enhancing ease of use and reducing the likelihood of certain adverse effects compared to regular heparin.
North America: Significant Region During the Forecast Period
The incidence of thromboembolic and cardiovascular conditions is increasing in North America, with CVD alone claiming one life every 33 seconds in the US, according to the Centers for Disease Control and Prevention (CDC). The market in North America benefits from the prominent positions of key pharmaceutical companies like Pfizer and Baxter, driving the growth of the heparin market in the region.
Some of the leading companies operating in the market include Dr. Reddy’s Laboratories Ltd, Aspen Pharmacare Holdings Limited, Opocrin SpA, etc.
Request for Customization: https://inkwoodresearch.com/request-for-custom-report/
About Inkwood Research
Inkwood Research specializes in syndicated & customized research reports and consulting services. Market intelligence studies with relevant fact-based research are customized across industry verticals such as technology, automotive, chemicals, materials, healthcare, and energy, with an objective comprehension that acknowledges the business environments. Our geographical analysis comprises North & South America, CEE, CIS, the Middle East, Europe, Asia, and Africa.
Contact Us
https://www.inkwoodresearch.com
1-(857)293-0150
Related Reports:
GLOBAL ANTICOAGULANTS MARKET
0 notes
Text
Balancing the Risks and Benefits of Anticoagulation During Pregnancy

Pregnancy is a unique physiological state that brings about numerous changes in a woman's body, including alterations in hemostasis. For women with pre-existing conditions that predispose them to thrombosis, such as deep vein thrombosis (DVT) or atrial fibrillation, the management of anticoagulation during pregnancy poses a complex challenge. Striking the right balance between preventing thrombotic events and avoiding potential harm to both the mother and the fetus is crucial. This article explores the intricate task of balancing the risks and benefits of anticoagulation during pregnancy.
The Physiological Changes of Pregnancy:
Pregnancy induces various physiological changes, particularly in the cardiovascular and hemostatic systems. Plasma volume and cardiac output increase, while procoagulant factors rise concurrently. This hypercoagulable state is a protective mechanism to prevent excessive bleeding during childbirth. However, it also poses a heightened risk of thromboembolic events for women with pre-existing conditions, necessitating careful consideration of anticoagulation therapy.
Risks of Untreated Thrombosis:
For pregnant women with a history of thrombosis or those at high risk, the consequences of untreated thrombosis can be severe. Deep vein thrombosis can lead to pulmonary embolism, a life-threatening condition that poses a significant risk to both the mother and the developing fetus. Balancing the need for anticoagulation to prevent these complications with the potential risks to the fetus is a delicate process that requires a multidisciplinary approach.
Anticoagulation Options and Their Risks:
Several anticoagulant medications are available, each with its own set of benefits and risks. Heparins, such as unfractionated heparin and low molecular weight heparin, are commonly used during pregnancy due to their limited placental transfer. Warfarin, an oral anticoagulant, crosses the placenta and is associated with fetal complications, such as embryopathy and central nervous system abnormalities. Choosing the appropriate anticoagulant involves considering the efficacy in preventing thrombosis and minimizing potential harm to the developing fetus.
Risk of Bleeding Complications:
While preventing thrombosis is crucial, anticoagulation therapy inherently increases the risk of bleeding complications. Striking a balance between preventing thrombotic events and minimizing the risk of bleeding is essential for both maternal and fetal well-being. Careful monitoring of coagulation parameters and adjustment of anticoagulant dosages are integral components of managing these delicate balances.
Individualized Treatment Plans:
Managing anticoagulation during pregnancy is a complex task, highlighting the necessity for personalized treatment plans. When devising a treatment strategy, factors such as the type of thrombophilia, history of previous thrombotic events, and gestational age must be carefully considered. It is essential to consult with high-risk pregnancy treatment in Indore for expert guidance. Collaborative decision-making involving obstetricians, haematologists, and other relevant specialists is crucial to tailor therapy to each patient's unique circumstances.
Monitoring Fetal Well-being:
Regular monitoring of fetal well-being is paramount in the management of anticoagulation during pregnancy. This includes assessing fetal growth, monitoring for signs of placental insufficiency, and conducting periodic ultrasounds to detect any congenital abnormalities associated with anticoagulant use. The benefits of preventing maternal thrombotic events must be weighed against the potential risks to the fetus, and adjustments to the treatment plan may be necessary as the pregnancy progresses.
Achieving a balance between the risks and benefits of anticoagulation during pregnancy calls for a personalized and meticulous approach. The intricate physiological changes induced by pregnancy and the complexities of maternal-fetal health require careful consideration of multiple factors. For expert guidance, consult with a gynecologist in Indore. Successful management entails collaborative efforts between healthcare professionals and open communication with the expectant mother. Healthcare providers aim to optimize both maternal and fetal outcomes by evaluating the risks of untreated thrombosis against the potential harms of anticoagulation.
#high risk pregnancy treatment in indore#painless normal delivery in indore#normal delivery in indore#heavy periods treatment in indore#gynecologist in indore#gynecologist indore#best gynecologist in indore
0 notes
Text
Data Bridge Market Research analyses a growth rate in the heparin market in the forecast period 2023-2030. The expected CAGR of heparin market is tend to be around 5.50% in the mentioned forecast period. The market is valued at USD 1.3 billion in 2022, and it would grow upto USD 2 billion by 2030. In addition to the market insights such as market value, growth rate, market segments, geographical coverage, market players, and market scenario, the market report curated by the Data Bridge Market Research team also includes in-depth expert analysis, patient epidemiology, pipeline analysis, pricing analysis, and regulatory framework.
#Asia-Pacific Heparin Market#Asia-Pacific Heparin Market Share#Asia-Pacific Heparin Market Size#Asia-Pacific Heparin Market Growth#Asia-Pacific Heparin Market Trends#Asia-Pacific Heparin Market Players#Asia-Pacific Heparin Market Competitors#Asia-Pacific Heparin Market Industry Size#Asia-Pacific Heparin Market Industry Trends#Asia-Pacific Heparin Market Industry Growth#Asia-Pacific Heparin Market Industry Share#Asia-Pacific Heparin Market Industry Players
0 notes
Text
0 notes
Text
0 notes
Text
Global Low Molecular Weight Heparin (LMWHs) Market Unidentified Segments – The Biggest Opportunity Of 2022
Latest added Low Molecular Weight Heparin (LMWHs) Market research study by AMA Research offers detailed outlook and elaborates market review till 2027. The market Study is segmented by key regions that are accelerating the marketization. At present, the market players are strategizing and overcoming challenges of current scenario; some of the key players in the study are Aspen (South Africa)
Sanofi-aventis (France)
Pfizer (United States)
Teva (Israel)
Leo Pharma (Denmark)
Amphastar Pharmaceuticals (United States)
Abbott(United States)
Intrapharm Laboratories (United Kingdom)
Opocrin (Italy)
Dongying Tiandong Pharmaceutical (China)
Techdow (United Kingdom)
Yantai Dongcheng Pharmaceutical Group (China) etc.
Low molecular weight heparin is obtained from unfractionated heparin the procedure of obtaining is through enzymatic or chemical depolymerization of unfractionated heparin. It is highly used as it shows low side effects compared to other available medications. It is used for various blood related and heart-related treatments. The above product it is safe for pregnant women as it don’t shows any complications ahead. It is easily available and also can be used by your own, no need to visit hospitals every time once you know how to use it.
Influencing Trend: Growing Use In Heart Disorders And Blood Clotting Over Other Medications
Challenges: Loss Of Bone Strength
Opportunities: Low Weight Heparins Are Safe Complications In Pregnancy When Compared To UFH
Market Growth Drivers: Growing Demand As It Can Self-Administered At Home Via Subcutaneous Injection, Reducing Or Eliminating Hospital Stays
The Global Low Molecular Weight Heparin (LMWHs) segments and Market Data Break Down by Type (Enoxaparin, Dalteparin, Tinzaparin, Fraxiparine), Application (Treatment of Venous Thromboembolism, Complications of Pregnancy, Anti-coagulation Therapy, Cardioversion of Atrial Fibrillation/Flutter, Others), Route of Administration (Intravenous, Subcutaneous, Intramuscular), Packaging (Multi vials, Prefilled syringes), Weight (0.4ml injections, 100mg/mL (3mL vial), 30mg/0.3mL, 40mg/0.4mL, 60mg/0.6mL, 80mg/0.8mL, 100mg/mL, 120mg/0.8mL, 150mg/mL, Others), End User (Hospitals, Clinics, Pharmacies)
Presented By
AMA Research & Media LLP
0 notes
Text
0 notes
Text
The lecture we had today was about perioperative care.
Geriatric Preop:
Cognition - dementia, delirium, depression
Capacity - Aid to Capacity Evaluation
Function - ADLs (bathing, dressing), IADLs (money management, shopping)
Mobility & fall risk screening
Frailty - Fried criteria (if at least 3/5 are positive, they’re frail; should do PT before surgery)
Nutrition - Mini Nutritional Assessment
EtOH & tobacco use - CAGE questionnaire (pts who have EtOH use disorder are at risk for withdrawal; look for tongue fasciculations). Pts who smoke should have patch and gum while in the hospital.
Cardiac evaluation 9- 2014 ACC/AHA algorithm for noncardiac surgery
Med room review - STOPP/START criteria, Beers criteria
Confusion Assessment Method (CAM) screens for delirium.
More than 4 METS = climbing 2 flights of stairs; walking up a hill, walking at 4 MPH on level ground
Duke Activity Status Index
Surgery is ok if HR is controlled (HR 50-100 or 110)
Predicting post op pulmonary complications- Gupta postoperative respiratory failure risk
D/c warfarin 5 days prior w/o bridging for AFib
If mechanical valve, d/c warfarin with heparin bridge once INR falls outside therapeutic range
Stop LMWH 24 hours before surgery; hold unfractionated heparin 4-5 hours before surgery
Hold ASA 7 days prior for primary prevention. Those on it for secondary prevention, continue it unless surgery has high bleeding risk.
Post op VTE ppx - 2019 American Society of Hematology Guidelines. For hip/knee surgeries start 8-12 hours after surgery. Duration is 14 days or until pt is fully weight bearing. Duration is up to 6 weeks for total hip arthroplasty.
LMWH (doesn’t alter PTT), low dose DOACs (work as well as or better than LMWH). ASA can be used, but it’s not as good as LMWH or DOACs. ASA alone is inferior to LMWH or DOACS alone. Can do ASA after 5 days of DOACS.
1 note
·
View note
Text
HEPARIN MARKET Growth, Industry Size-Share, Global Trends, Key Players Strategies and Upcoming Demand
Data Bridge Market Research analyses that the HEPARIN MARKET will project a compound annual growth rate (CAGR) of 5.6% during the forecast period of 2022-2028.
A world class HEPARIN MARKET research report is formulated with the finest and advanced tools of collecting, recording, estimating and analysing market data. With the systematic and comprehensive market research study, this market research report offers the facts associated with any subject in the field of marketing for Healthcare industry. It gives superior ideas and solutions in terms of product trends, marketing strategy, future products, new geographical markets, future events, sales strategies, customer actions or behaviours. This HEPARIN MARKET report has been prepared by considering several fragments of the present and upcoming market scenario.
HEPARIN MARKET Scope and Market Size
The heparin market is segmented on the basis of product type, mode of administration, source, ingredients, availability, treatment, application, therapeutics, strength, type, container, packaging, end user and distribution channel. The growth amongst these segments will help you analyse meagre growth segments in the industries, and provide the users with valuable market overview and market insights to help them in making strategic decisions for identification of core market applications.
On the basis of product type, the heparin market is segmented into unfractionated heparin, low molecular weight heparin (LMWH) and ultra-low molecular weight heparin (ULMWH).
On the basis of mode of administration, the market is segmented into oral administration and parenteral administration.
On the basis of source, the heparin market is segmented into bovine and porcine.
On the basis of ingredients, the heparin market is segmented into sodium and calcium and others.
On the basis of availability, the heparin market is segmented into raw, and processed.
On the basis of treatment, the heparin market is segmented into deep vein thrombosis, pulmonary embolism, arterial thromboembolism and others.
On the basis of application, the heparin market is segmented into pre-surgical procedures, post-surgical procedures, kidney dialysis, diagnostic tests and others.
On the basis of therapeutics, the heparin market is segmented into cardiovascular, respiratory, oncology, nephrology, CNS and others.
On the basis of strength, the heparin market is segmented into 10 unit, 100 unit, 1000 unit, 5000 unit, 10000 unit, 25000 unit and others.
On the basis of type, the heparin market is segmented into generics and brands.
On the basis of container, the heparin market is segmented into bottles, bags, vials and others. On the basis of packaging, the market is segmented into glass and plastic.
On the basis of end user, the heparin market is segmented into hospitals, clinics, homecare, ambulatory surgical centres and others.
On the basis of distribution channel, the market is segmented into hospital pharmacy, retail pharmacy & drug store, online pharmacy and others.
Get the Free sample copy of the report here:
Some of the key questions answered in this report:
How has the HEPARIN MARKET performed so far and how will it perform in the coming years?
What has been the impact of COVID-19 on the HEPARIN MARKET?
What are the key regional markets?
What are the key driving factors and challenges in the industry?
What is the structure of the HEPARIN MARKET and who are the key players?
Market Analysis and Insights: HEPARIN MARKET
Rising prevalence of pulmonary embolism and venous thromboembolism is leading to the rise in the heparin market value. Data Bridge Market Research analyses that the heparin market will exhibit a CAGR of around 5.6% for the forecast period of 2021-2028.
Heparin is an injectable anticoagulant that is especially used in surgical procedures to prevent blood clotting in the veins and arteries. Otherwise, it is also used to treat blood clotting disorders. It is also used to treat and diagnose pulmonary embolism, venous thromboembolism and arterial thromboembolism. Heparin is also commonly known as unfractionated heparin. Heparin is an animal-derived product, derived from the tissues of slaughtered meat.
The rising number of accidents and medical surgeries is the root cause for the rise in demand for heparin. Also, rising disorders like cardiovascular disorders will multiply the demand for heparin. A rise in the expenditure to improve healthcare infrastructure coupled with rising patient awareness is also expected to boost up the market demand. Research and development proficiencies will too foster the market growth rate.
HEPARIN MARKET - Regional Level Analysis
The countries covered in the heparin market report are U.S., Canada and Mexico in North America, Germany, France, U.K., Netherlands, Switzerland, Belgium, Russia, Italy, Spain, Turkey, Rest of Europe in Europe, China, Japan, India, South Korea, Singapore, Malaysia, Australia, Thailand, Indonesia, Philippines, Rest of Asia-Pacific (APAC) in the Asia-Pacific (APAC), Saudi Arabia, U.A.E, South Africa, Egypt, Israel, Rest of Middle East and Africa (MEA) as a part of Middle East and Africa (MEA), Brazil, Argentina and Rest of South America as part of South America.
HEPARIN MARKET - Share Analysis:
The heparin market competitive landscape provides details by competitor. Details included are company overview, company financials, revenue generated, market potential, investment in research and development, new market initiatives, global presence, production sites and facilities, production capacities, company strengths and weaknesses, product launch, product width and breadth, application dominance. The above data points provided are only related to the companies’ focus related to heparin market.
Key player - HEPARIN MARKET
Some of the major players operating in the HEPARIN MARKET are OPOCRIN S.P.A., Baxter., Aspen Holdings, B. Braun Medical Inc., Pfizer Inc., GlaxoSmithKline plc., LEO Pharma, Sanofi, Fresenius SE & Co. KGaA, Teva Pharmaceutical Industries Ltd., F. Hoffmann-La Roche Ltd, Mylan N.V., Changzhaou Qianhong Bio-pharma Co., ltd., Eisai Co., Ltd., Fresenius Kabi AG, Hikma Pharmaceuticals PLC, Nanjing Jianyou Biochemical Pharmaceutical Co., Novartis AG, SARIA SE & Co. KG, Shanghai Fosun Pharmaceutical(Group)Co., Ltd. and Hepalink Group
Get Full Access of Report@
MAJOR TOC OF THE REPORT
Chapter One: Introduction
Chapter Two: Scope and Market Size
Chapter Three: Analysis and Insights
Chapter Four: Country Level Analysis
Chapter Five: Share Analysis
Chapter Six: Key player
Get TOC Details:
Top Trending Reports:
Global Autoclave Market
Global Proctoscope Market
Global Molecular Methods Market
Global Wound Debridement Market
Global Human Papilloma Virus Testing Market
Global Non-Small Cell Lung Cancer Market
Global CPAP Market
Global RNA Markers Market
Global Healthcare Cloud Computing Market
Global Medical Image Management Market
Global Pharmacogenetic Testing Market
Global Hemodialysis Services Market
Global Hemostatic Wound Dressing Market
Global Interventional Radiology Products Market
Global Lab Accessories Market
Global Label-free Array Systems Market
Global Laboratory Gas Generators Market
Global Life Science Analytics Market
Global Mediastinoscopes Market
Global Medical Alert System Market
Global EDS, WDS, EBSD, Micro-XRF Instruments Market
Global Direct-to-Consumer (DTC) Genetic Testing Market
Global Q- Polymerase Chain Reaction and D- Polymerase Chain Reaction Devices Market
Asia-Pacific (APAC) Q-PCR and D-PCR Devices Market
Europe Q-PCR and D-PCR Devices Market
About Us:
Data Bridge Market Research set forth itself as an unconventional and neoteric Market research and consulting firm with unparalleled level of resilience and integrated approaches. We are determined to unearth the best market opportunities and foster efficient information for your business to thrive in the market
Contact:
Data Bridge Market Research
Tel: +1-888-386.8-2818
Email: [email protected]
0 notes
Text
Global Heparin Market is projected to expand at a CAGR of ~5% by 2026

Heparin is an injectable anticoagulant prescription medicine used to treat and prevent the symptoms of blood clots caused by medical conditions or medical procedures. Additionally, it is utilized to make an anti-clotting surface inside a variety of medical devices, including test tubes and renal dialysis machines.
The Global Heparin Market is expected to grow at a rate of ~5% by 2026. The rising prevalence of chronic diseases such as venous thromboembolism, pulmonary embolism, renal diseases, and cardiovascular disorders, increasing geriatric population, high demand for anticoagulants, growing application of heparin in various surgeries such as orthopedic and heart surgeries, and the expanding availability of synthetic and semi-synthetic heparin mimetics that help in the treatment of cancer, coagulation, and inflammatory diseases are a few of the main factors driving the global heparin market.
Increasing Usage of Heparin in Various Applications Drives the Heparin Market
Anticoagulants work by decreasing the clotting ability of the blood. It helps to prevent the formation of clots as well as stop the further expansion of any existing clots. As a result, it may be used in a variety of applications, including:
Prevent or treat certain blood vessel, heart, and lung conditions
Prevent blood clotting during open-heart surgery, bypass surgery, kidney dialysis, and blood transfusions
Prevention of deep vein thrombosis
Prevention of a blood clot following percutaneous coronary intervention
Growing Adoption of Low Molecular Weight Unfractionated Heparin Over Heparin to Prevent Deep Vein Thrombosis or Pulmonary Embolism Fuels the Demand
Low-molecular-weight heparins have several advantages over UFH that have led to their increasing use for several thromboembolic indications such as deep vein thrombosis (DVT) and pulmonary embolism (PE) as well as atrial fibrillation (AF). In comparison to heparin, LMWH provides better bioavailability and a longer half-life, streamlined dose, predictable anticoagulant response, a reduced risk of heparin-induced thrombocytopenia (HIT), and a reduced risk of osteoporosis.
Explore Premium Report on Heparin Market @ https://meditechinsights.com/global-heparin-market/
The Potential Role of Heparin in Covid-19 Patients Boosts the Heparin Market Growth
Many patients with COVID-19 develop a clinically significant coagulopathy. COVID-19 infections can lead to an increased risk of blood clots. These blood clots can lead to individuals being admitted to hospital, or, unfortunately in severe cases, death. Similarly, patients with COVID-19 are at high risk for developing clinically significant large-vessel thrombosis. Thus, early usage of anticoagulation may reduce the risk of coagulopathy, microthrombus formation, and organ damage.
Key Challenges/ Constraints: Heparin Market
The main factors limiting the market's growth are the side effects associated to the usage of heparin drugs and the availability of another anticoagulant on the market.
North America Holds the Largest Market Share but APAC is Set to Witness Strongest Growth
North America holds the largest market share of the heparin market followed by Europe and the Asia Pacific. This can be primarily attributed to the high burden of chronic diseases, the presence of advanced and robust healthcare infrastructure, increasing demand for heparin in various surgeries, and rising incidences of cardiovascular disorders in the region.
Companies Adopt both Organic & Inorganic Growth Strategies to Increase their Market Share
Players operating in the heparin market are adopting organic and inorganic growth strategies such as collaborations, acquisitions, and expansions to garner market share.
For instance,
In February 2022, Techdow USA Inc. announced the launch of its Heparin Sodium Injection, USP in the United States market
In January 2022, Ohio-based biotechnology company Optimvia Pharmaceuticals announced the development of a synthetic method for creating large quantities of heparin, which is used to make a common blood thinner at a reasonable price
Competitive Landscape Analysis of Heparin Market
The global heparin market is marked by the presence of established key players such as Baxter International Inc., B. Braun Holding GmbH & Co. KG, Dr. Reddy’s Laboratories Ltd., and Fresenius SE & Co KGaA among others.
For More Detailed Insights, Contact Us @ https://meditechinsights.com/contact-us/
About Medi-Tech Insights
Medi-Tech Insights is a healthcare-focused business research & insights firm. Our clients include Fortune 500 companies, blue-chip investors & hyper-growth start-ups. We have completed 100+ projects in Digital Health, Healthcare IT, Medical Technology, Medical Devices & Pharma Services.
Contact:
Ruta Halde
Associate, Medi-Tech Insights
+32 498 86 80 79
0 notes
Text
EHR-based decision support system helps prevent VTE in hospitalized patients
Increasing thromboprophylaxis
“A big proportion of venous thromboembolism in the community is due to hospitalization for recent medical illness,” Spyropoulos told Healio. “By far, more severe and fatal VTE events occur in nonsurgical medically ill patients. There are approximately 8 million hospitalized medically ill patients in the United States every year. Thromboprophylaxis for this heterogeneous, difficult population is misused or underused, especially in the post-discharge period. Data show only 4% of hospitalized medically ill patients receive any kind of post-discharge prophylaxis. We know that about one in four hospitalized medically ill patients are at high risk of thrombosis, not just in the hospital but after discharge.”
Existing systems to improve VTE prophylaxis in this population are either inefficient or very expensive, he said.
“Our institute developed a novel universal clinical decision support platform that was able to integrate clinical decision support into any electronic health record using an EHR-agnostic capability,” Spyropoulos told Healio. “This tool was effective in altering clinician behavior, which was not easy. We garnered that technology and incorporated a validated VTE risk model called IMPROVE-DD. I call it the CHA2DS2-VASc score for medically ill patients. We hoped that using this tool would increase rates of appropriate thromboprophylaxis as a marker of change in clinician behavior. The home run would be to reduce hard outcomes, which are major thromboembolic events.”
All patients were older than 60 years and were hospitalized for one of five reasons: exacerbation of congestive HF, acute respiratory insufficiency, acute infectious disease including COVID-19, acute inflammatory disease including rheumatic disease, and acute stroke with or without paralysis, Spyropoulos said during a presentation.
The IMPROVE-DD VTE score, developed and validated over 10 years, covers a scale of 0 to 12, and designates patients with a score of 0 or 1 as low risk, those with a score of 2 or 3 as moderate risk (who benefit from appropriate in-hospital prophylaxis) and those with a score of 4 to 12 as high risk (who benefit from appropriate in-hospital and post-discharge prophylaxis), Spyropoulos said. It is compiled as follows: 3 points for previous VTE; 2 points for known thrombophilia, current lower-limb paralysis, cancer, or D-dimer at least two times the upper limit of normal; and 1 point for immobilization for at least 1 day, an ICU or coronary care unit stay, or being older than 60 years.
He said the appropriate thromboprophylaxis strategies are, for an inpatient with IMPROVE-DD VTE score of 2 or more, subcutaneous unfractionated or low-molecular-weight heparin, and for a post-discharge patient with IMPROVE-DD VTE score of 4 or more, rivaroxaban (Xarelto, Janssen/Bayer) 10 mg once daily for 30 days.
For the trial, two hospitals were randomly assigned to the usual care and two hospitals were randomly assigned to the EHR-based decision support system. There were 5,249 patients (mean age, 75 years; 48% men) in the intervention group and 5,450 patients (mean age, 74 years; 46% men) in the control group, enough to power the trial for hard clinical endpoints, Spyropoulos told Healio.
“We used the tool at admission, which is the normal clinical workflow, but we also created a brand-new workflow that doesn’t exist in U.S. hospitals, which is the tool being brought up at discharge as well, during the medication reconciliation process,” he said in an interview. “Using the tool took all of about 10 seconds, so it was not a difficult thing for the clinicians to do. The tool calculated a score and a 3-month risk, and when the user recorded those results, both the IMPROVE-DD score and an appropriate thromboprophylaxis recommendation were displayed in the EHR. It forced the providers to do something about it.”
The primary outcome was the rate of appropriate in-hospital and post-discharge thromboprophylaxis in moderate-risk and high-risk patients. Secondary outcomes included rates of VTE, arterial thromboembolism, VTE plus arterial thromboembolism, major bleeding, all-cause mortality, death/all-cause readmission and death/VTE readmission, all at 30 days after discharge.
‘Big numbers’
The in-hospital primary outcome occurred in 80.1% of patients in the intervention group and 72.5% of patients in the control group (OR = 1.52; 95% CI, 1.31-1.67; P < .001), whereas the post-discharge primary outcome occurred in 13.6% of patients with IMPROVE-DD VTE score of 4 or more in the intervention group and 7.5% of those patients in the control group (OR = 1.93; 95% CI, 1.6-2.33; P < .001), Spyropoulos said.
“The tool did exactly what it was supposed to do,” he told Healio. “Six percent to 8% absolute increases in prophylaxis are big numbers and have consequences in terms of outcomes and quality improvement metrics.”
Of note, the 72.5% in-hospital prophylaxis rate in the control group was “very high,” Spyropoulos said, noting that it far exceeded the rate in nonacademic hospitals, which is about 55%.
“The thinking is, there should be a greater benefit in nonacademic hospital settings,” he told Healio.
At 30 days after discharge, compared with the control group, the intervention group had lower rates of VTE (OR = 0.8; 95% CI, 0.64-1; P = .048), arterial thromboembolism (OR = 0.35; 95% CI, 0.19-0.67; P < .001) and VTE/arterial thromboembolism (OR = 0.71; 95% CI, 0.58-0.88; P = .002), but a higher rate of all-cause mortality (OR = 1.32; 95% CI, 1.15-1.53; P < .001), according to the researchers. There were no significant differences between the groups in major bleeding, death/all-cause readmission and death/VTE readmission.
“By increasing in-hospital and at-discharge thromboprophylaxis, the tool was able to reduce major thromboembolism,” Spyropoulos told Healio. “And we didn’t pay a price for this in terms of bleeding.”
The tool should be freely available in the library of tools of the Agency for Healthcare Research and Quality, which gave a grant to the informatics and clinical team of Spyropoulos’ group at the Feinstein Institutes for Medical Research to develop it, he said, noting the IMPROVE-DD risk model will soon be available for those who want to use it individually on most apps that physicians use.
Technical Doctor's insight:
Contact Details :
[email protected] or 877-910-0004
www.technicaldr.com
0 notes
Text
New Treatment Horizons for Deep Vein Thrombosis in Cancer Patients
Mini Review
Venous thromboembolism (VTE), clinically manifested as deep vein thrombosis (DVT) or pulmonary embolism (PE). It is the third most common acute cardiovascular syndrome behind acute myocardial infarction and stroke [1]. It may occur before, during or after cancer diagnosis, with a relatively high incidence in cancer patients, ranging from 15 to 50% [2]. Thrombotic events are reported as the second leading cause of mortality in these patients; the main cause is death due to cancer itself [3]. VTE treatment when associated with cancer is complex, related to the high risk of bleeding and recurrent VTE [2]. The basis of acute VTE management in patients with or without cancer is generally equal. However, an individual management is necessary due to comorbidities, drug interactions and other kinds of approach. For therapeutic decision, patient choice, treatment goals and life expectancy should be taken into consideration [4]. Cancer patients without contraindications and kidney failure, low molecular weight heparin (LMWH) is recommend in the immediate anticoagulation - first five days - as monotherapy. In case of a glomerular filtration rate lower than 30 milliliters per minute, intravenous unfractionated heparin (UFH) is indicated, but it’s also accepted an approach of LMWH guided by anti-Xa levels. If anticoagulation needs to be suspended or reversed in a short time, UFH should be preferred [5].
Read More about this article: https://irispublishers.com/acrci/fulltext/new-treatment-horizons-for-deep-vein-thrombosis-in-cancer-patients.ID.000534.php
Read More about Iris Publishers Google scholar Articles: https://scholar.google.com/citations?view_op=view_citation&hl=en&user=d1PdB38AAAAJ&cstart=20&pagesize=80&authuser=1&citation_for_view=d1PdB38AAAAJ:ZeXyd9-uunAC
1 note
·
View note
Last Seen Blogs

girlfailurefelix
professional yapper

todaviamadrid
Todavía Madrid

waywardkaz2y5
Follow the Spiders

live-simply-free
Live On Till the Energy Fades

ephanah-sin
Black Blood