#I am improving on the chronically late bit in many regards
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Kazakhstan’s Minister of Communications and Informatics has blocked the Tumblr site because it contained 60 sites of terrorism, extremism, and pornography in 2015.
Text
"YOUR MIND AND BODY MATTERS"
-October 28, 2020
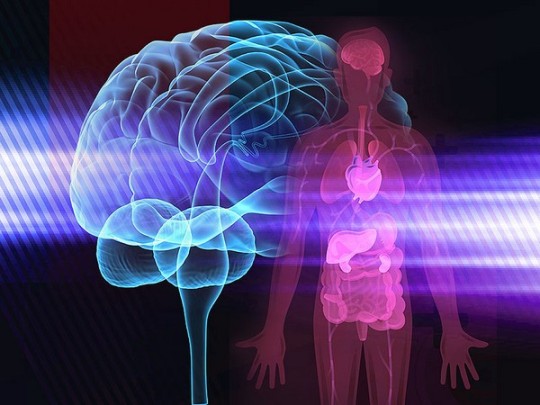
Have you ever check upon yourself? Especially your mind and body? And if so, when is the last time you did it? As of now that the worlds facing a pandemic it is important to monitor our mind and body not just on the month of celebration about mental health. Many news are coming out about their physical and mental health to their family and personal problems in life especially those students who are having difficulties on their online classes. There are lots of sayings that this is not good for them as you browse on different social links that is based from their experience and it is sad to say that most students felt depression and anxiety that they killed themselves because their minds are full of pressure about simultaneously deadlines/activities and felt sick beacuse of having a lack of sleep. This is one of the examples I have cited that I wanted to encourage my fellow students to ask themeselves right now this kind of questions, "How healthy is my mind and body?" & "Am I truly happy and enjoying what I am doing?". Because we can't deny somehow we feel lost and empty. That's why it is important to assess if we are still okay about our physical and mental health because both are interconnected as our thoughts affects our physical body.
According to Newport Academy (2019), "The mind and the body are not two separate entities—although they are often treated that way. Physical health and emotional health are intimately intertwined in what’s known as the mind-body connection.
Our chemistry and biology impact our mood and emotions, as well as thoughts and beliefs. With all of these factors combined, they play a major role in influencing our stress and physical health. If you’ve ever felt your stomach tighten up when you were anxious, you’ve experienced the mind-body connection."
If you are one of this kind of students who doesn't have healthy mind and body or who wanted to know how to maintain your mind and body strong and healthy, here are Eight Habits for you according to Valentine (2017).
1. Exercise using something you love
Physical exercise has been shown in countless studies to help reduce stress, increase energy, improve mood, and even help make us more creative.
Great right? However, advice on how to make exercise a habit is a bit lacking. That’s because exercise can be a really difficult habit to stick to. But if there’s one thing I’ve found really helps stick to physical exercise and make it a long-term habit it’s this:
Exercise in a way that allows you to enjoy something you love.
You have to really look forward to working out. Whatever it is that you do, whether it’s running, lifting weights, doing cardio, martial arts, Yoga, or something else, you need to pick an exercise method you really enjoy.
For example, I love martial arts. I’m a lot more likely to stick to my work out while doing that than running or lifting weights. On the flip side, if there’s no particular exercise-like activity you enjoy, maybe you really love music. Play all your favorite music during your workout and you’ll notice yourself far more likely to get up to exercise. Another option is listening to podcasts about your craft while running.
Either way, exercise is a big one, so find a way to make it work for you.
2. Meditation
Meditation is another huge one. However, meditation isn’t really what most people think it is.
If you don’t like the traditional idea of meditation, you can meditate while doing virtually anything if you use the right method (i.e. mindfulness meditation). Also, studies have shown that as little as five to ten minutes of meditation offers great benefits, so don’t think you need to sit for a half hour every day. You really don’t.
Similar to physical exercise, there are several different methods and forms of meditation, so do a little adventuring and experimentation to find a method and form that works for you. Everyone is different and different methods of meditation tend to work better for different people.
3. Mindful walking
This is easily one of my favorite activities on this entire list, but it’s also the most obscure. Mindful walking, also known as walking meditation, is meditation in motion. It can be done formally as a dedicated practice and informally by paying attention to your steps and what is going on around you as you move.
This is great for many of the reasons formal meditation is (albeit less concentrated), however, there’s another big reason to do mindful walking: it helps you tune in to the body.
Sometimes, things occur in the body that we don’t notice. Oftentimes, chronic issues and illness begin to creep up in ways often unseen. However, by learning to tune in to the body with mindful walking, we can notice these things arise before they become more of an issue.
It’s a hard thing to explain, but it’s been infinitely useful to me. In many ways, this one exercise gives us a way to check in with both the mind and body on a regular basis and in an incredibly convenient way while going about our daily activities, so its place on this list is well-earned.
4. Rise early
Rising early is something I took years to develop. However, it was so worth it.
There are positives to staying up late, particularly if you find that you’re more productive or creative during late night hours. However, in general, I’ve found that the majority of people are most productive in the early morning hours.
In addition, though, waking up early and adopting a morning routine that prepares you for the day helps you start each day off with the optimal state of mind to tackle problems and make decisions, something incredibly useful for everyone no matter what your profession.
So, if you’re not already, see what waking up a little earlier does for you.
5. Adopt a nighttime routine
On the flip side of that, adopting an effective night time routine that puts your mind in the right state before bed and helps maximize the quality of your sleep is also incredibly beneficial.
Unfortunately, most of us in the West just don’t value sleep enough. We tend to place work above well-being and prefer to leave sleep for when we die. However, two decades of scientific research now says this isn’t just a bad idea health-wise – it’s unproductive.
Take some time to craft a simple but effective nighttime routine and I promise – you won’t regret it.
6. Remove sugar, add water, get your food from the source
This is the basic recipe I follow when it comes to nutrition advice.
Over the years, I’ve learned a lot and tried so many different things with regards to nutrition. At this point, my ideology on nutrition is pretty relaxed. And it’s never worked out better.
There’s a ton of advice out there and, rightfully, it can be pretty confusing. So, I’ve chosen to follow a pretty simple mantra that offers me roughly eighty percent of the benefit of any particular diet while doing about twenty percent of the work to get that benefit. It’s this:
Remove sugar: Sugar is bad. Really bad. Occasional sugar is just fine, even daily, as long as you try to keep it under 50g at an absolute a maximum (30g even better).
Add water: Buy a dedicated flask just for water and you’ll have a one thousand times higher likelihood of sticking to the habit of drinking water daily. About eight to ten cups is fine, but you should look into what your specific amount is based on your body weight.
Get your food from the source: Do you have a farm where you live? Or a farmer’s market? Awesome. Section of your grocery store with local farm foods? Pretty good too. Also, this refers to what food you eat as well. Put a little more whole foods into your diet or get a juicer.
Keep it simple and use this method to get most of the benefit of altering your diet while saving you time to focus on what’s most important to you.
7. Find friends who identify with your challenges
We’re social creatures. No matter what you do, you can’t escape this.
And so, by virtue of this, the more social we are, the healthier we tend to be.
However, there’s something very specific about relationships that helps us more than anything else: having people around us who identify and sympathize with our challenges and who we communicate with often about those challenges. The lack thereof is often the reason for suicide in those who suffer from depression or bullying.
When we have people around us who listen and understand what we’re going through, something magical happens: we get through it (what it is for you). It’s a very simple thing that we often overlook but is so critical to our mental and even physical health.
8. Find a passion project or creative outlet
If you’ve been pursuing something you love for some time now, I don’t have to tell you how great it makes you feel.
The energy we get while pursuing our passions is limitless and gives us a sense of vitality that is hard (if impossible) to acquire any other way.
Using our brain regularly keeps our mind strong and moving helps keep us physically healthy, so if you haven’t yet taken the time to find what you’re passionate about and to start pursuing that with every fiber of your being, start now (before it’s too late).
There's no harm in trying, our mind and physical gives us energy. A person who can change his/her mind can change his/her lives. Always remember health is our wealth. Keep on checking and doing the things you love.
Sources:
Newport Academy, (2019). Understang the Mind-Body Connection. https://www.newportacademy.com/resources/mental-health/understanding-the-mind-body-connection/
Valentine, M., (2017). 8 Habits You Need to Lock Down for a Strong, Healthy Mind and Body. https://www.goalcast.com/2017/12/14/8-habits-healthy-mind-and-body/
6 notes
·
View notes
Text
Meta: Personality Analysis
Disclaimer: I, in no way, am a psychologist nor claim to be good at this. This is purely for fun, and for character growth. Also, this is based on the way I write Kamui/Corrin. Some of her personality is divergent from canon, due to past interactions in the four+ years I’ve written her.
Edited: August 15th, 2020
Also this got even longer and I’m sorry.
Enneagram: Nine
Nines are accepting, trusting, and stable. They are usually creative, optimistic, and supportive, but can also be too willing to go along with others to keep the peace. They want everything to go smoothly and be without conflict, but they can also tend to be complacent, simplifying problems and minimizing anything upsetting. They typically have problems with inertia and stubbornness. At their Best: indomitable and all-embracing, they are able to bring people together and heal conflicts.
MTBI: ENFJ “The Protagonist.”
Protagonists are natural-born leaders, full of passion and charisma. Forming around two percent of the population, they are oftentimes our politicians, our coaches and our teachers, reaching out and inspiring others to achieve and to do good in the world. With a natural confidence that begets influence, Protagonists take a great deal of pride and joy in guiding others to work together to improve themselves and their community.
Four Temperaments: Sanguine
Your temperament is sanguine. The sanguine temperament is fundamentally spontaneous and pleasure-seeking; sanguine people are sociable and charismatic. They tend to enjoy social gatherings, making new friends and tend to be boisterous. They are usually quite creative and often daydream. However, some alone time is crucial for those of this temperament. Sanguine can also mean sensitive, compassionate and thoughtful. Sanguine personalities generally struggle with following tasks all the way through, are chronically late, and tend to be forgetful and sometimes a little sarcastic. Often, when they pursue a new hobby, they lose interest as soon as it ceases to be engaging or fun. They are very much people persons. They are talkative and not shy. Sanguines generally have an almost shameless nature, certain that what they are doing is right. They have no lack of confidence.
Moral Alignment: Chaotic Good, "Rebel"
A chaotic good character acts as his conscience directs him with little regard for what others expect of him. He makes his own way, but he's kind and benevolent. He believes in goodness and right but has little use for laws and regulations. He hates it when people try to intimidate others and tell them what to do. He follows his own moral compass, which, although good, may not agree with that of society.
Chaotic good is the best alignment you can be because it combines a good heart with a free spirit.
Chaotic good can be a dangerous alignment when it disrupts the order of society and punishes those who do well for themselves.
Astrology: Taurus
Strengths: Reliable, patient, practical, devoted, responsible, stable
Weaknesses: Stubborn, possessive, uncompromising
Taurus likes: Gardening, cooking, music, romance, high quality clothes, working with hands
Taurus dislikes: Sudden changes, complications, insecurity of any kind, synthetic fabrics
Practical and well-grounded, Taurus is the sign that harvests the fruits of labor. They feel the need to always be surrounded by love and beauty, turned to the material world, hedonism, and physical pleasures. People born with their Sun in Taurus are sensual and tactile, considering touch and taste the most important of all senses. Stable and conservative, this is one of the most reliable signs of the zodiac, ready to endure and stick to their choices until they reach the point of personal satisfaction.
Taurus is an Earth sign, just like Virgo and Capricorn, and has the ability to see things from a grounded, practical and realistic perspective. They find it easy to make money and stay on same projects for years, or until they are completed. What we often see as stubbornness can be interpreted as commitment, and their ability to complete tasks whatever it takes is uncanny. This makes them excellent employees, great long-term friends and partners, always being there for people they love. Earthly note makes them overprotective, conservative, or materialistic at times, with views of the world founded on their love of money and wealth.
The ruler of Taurus is Venus, the planet of love, attraction, beauty, satisfaction, creativity and gratitude. This tender nature will make Taurus an excellent cook, gardener, lover, and artist. They are loyal and don't like sudden changes, criticism or the chase of guilt people are often prone to, being somewhat dependable on other people and emotions they seem to be unable to let go of. Still, no matter their potential emotional challenge, these individuals have the ability to bring a practical voice of reason in any chaotic and unhealthy situation.
Taurus – the Wandering Bull Being the one who betrayed their best friend, goddess Hera herself, this is an unfortunate being that has to wander the Earth in order to find freedom. As if something was always poking them behind their back, reminding them of happiness that once was, stinging and pushing forwards, they close up in their own worlds, lonely and separated from their core. To find love, a Taurus has to travel the world, change perspective or make a shift in their entire belief system and their system of values.
Conclusion:
There are some contradictions in these results, but overall, it is her at a basic premise. She tends to be very strong with her foundations, doing whatever she can to keep by them. Most of the time, she will listen to what others have to say, for they can hold more wisdom than her. However, there are just some things that she won't change on. Her Nohrian family knows this the most, and there are some thing that they've tried to change about her. Especially Leo ( sorrcerii ).
When it comes to the vices, she holds those in as much as possible. The insecurity, the side of her that may be uncompromising -- her reaction to sudden change that isn't what she planned for. Things like that. As a tactician, she likes to be as many steps ahead of her enemy as possible. In mundane life, she tries to put that side of her away. But there's always going to be a part of her that takes notice of every little thing. She notices how someone reacts to a gift, a conversation, and logs it away. However, unlike the standard, she tends to be rather lenient. She's also like clay; she picks up on traits. For example: because of Jeanne's ( noircisaint ) influence, she has more of a backbone than the 'standard' Avatar. With Zero ( echoedfates ), more of her playfulness comes out. He’s shown her that it’s OK to be a bit of a prankster -- well, more than she was before -- and it’s OK to put the title away when it’s just them. That there’s a difference between ‘princess’, ‘general’, and ‘wife’.
In her Type Moon verses, Makoto ( dekirukoto ) and Yi ( einhcrjars ) have taught her it’s OK to let her guard down. Especially while in Chaldea, and around them. That it’s OK to love, and even though it may hurt when they are returned to the throne, that things don’t have to stay at a standstill. That, hey, it’s OK to be you -- even more now than you were.
However, that doesn't mean she'll bite the bullet on it's first fire, and will always try to resolve a conflict before it arrives. Her anger is one of a slow fire, unless you pour the right amount of gas.
Kamui also holds in a lot more than most people. Even around those she calls her confidants and her retainers, she rather watch herself burn and suffer than those around her. She's very much a 'the world must be saved instead of myself'. Yet, over time, she's grown to understand that some people don't deserve it. Later on in the game, and depending on what route/verse, she will show some aggression to those who she deems deserves it. Which, as we know, is extremely small. ( Base game alone, Anankos, Hans, Garon, and Iago are the ones who get no special treatment from Kamui. And if she's acting nice, it's an act. )
There are times where she’ll return to a child-like state as well. There were many things that she didn’t get to experience, which lead her to have an imaginative mind and, at first, such a naive personality. Even during and after the war, she still retains it, since it’s so ingrained. It’s hard to ignore, hard to hide, but over time she comes to accept it. This is why she’s always reading; always wanting to learn; always wanting to experience what others have. A void can only be filled so much.
However, even though she may not seem it, she is rather intelligent. Because of lack of human contact outside of her retainers and teachers, she can come off as an 'airhead' or 'aloof'. Over time, that fades, and her true colors begin to shine more. She's able to find hoops she can jump through, but only will if the time seems right. Calculating outcomes begins to come second nature to her.
This is especially true when in Conquest, where she goes and knocks out almost all the Hoshidan soldiers she fights, just to put on a show for King Garon. In the end of that route, TECHNICALLY, she committed treason and blasphemy against Nohr. But thanks to Xander, she was absolved, and history wrote it to be that King Garon was dethrone on the basis of madness and insanity, dying in a battle in the Hoshidan capital.
And that’s it on this segment of, “Carrie adores Kamui too much, and has a problem.” Back to your regularly scheduled fluff! Thank you for reading this, and I’m sorry this turned out so long. asdfg
#∘OOC#∘Headcanon#Long post//#Someone remind me to doc this thing at a later date -wheeses-#*-wheezes-
9 notes
·
View notes
Text
Mental Health: What everyone is talking about… and no one is talking about

Mental health is a hot topic lately, and it seems as though more and more people are beginning to understand what mental health and self-care is, although many are still undereducated about these topics. Mental health is a touchy subject that can be taken advantage of very easily, with people claiming to have anxiety, depression, or other mental health issues and using them as excuses or, as we see a lot with millenials and the younger generation, attention. It has become increasingly popular among young people to self diagnose themselves with mental health conditions and display these on social media (particularly twitter) in an effort to increase sympathy likes and retweets. Phrases like “oh I’m so OCD about my bed being made” or “Watching that boy do tricks on his bike gives me anxiety” are so normalized, and we forget that these are actual conditions that can be extremely debilitating.
I know what you’re thinking: “So how am I supposed to know the difference between someone who really has a mental health condition and someone who is self diagnosed or just claims to have it?”
Unfortunately, I don’t have the answer to this. No one does. Mental health is such a touchy subject, and with anxiety, depression, and attention deficit disorders on the rise, it is likely that many people claiming to have these disorders have a clinical diagnosis to back it up. On another note, who is going to call someone out for “faking” a mental health disease? Not me. And probably not you. But what we can do is show compassion, and understand that everyone that we cross paths with is fighting a battle that we know nothing about.
Although not every person experiences symptoms of chronic mental illness, everyone goes through times of great happiness, sorrow, grief, stress, and pain. It is for these reasons that it is important to understand the importance of self-care.
What is self-care you might ask? Well, its important to know what self-care is as well as what it isn’t. Self-care, in a few words, is an action one takes to benefit their own mental, physical, or emotional health. This will vary among individuals, but there are many different forms of self-care. For some, it could be refusing the chocolate cake at the office birthday party because they’re trying to stick to their new meal plan. For others, it might be indulging in the chocolate cake because it is their birthday (or they have created some other reason in their minds that justifies cake). Whatever it is, the most important thing to remember regarding your personal self-care is that you have to make sure whatever self-care action you decide to take is best for YOU. What works for some people might not work for others, and what works for you may not work for your friends.
So while this idea of self-care is a nice one, it is not something that is completed by eating a cookie and taking a bubble bath. The idea of self-care penetrates much deeper than cheering yourself up after a bad day, or buying some new face wash. Self-care is about the way you live your life, and the effect that it has on your health. Everything that you experience in a day whether it is mental, emotional or physical has an effect on your health, which can be positive, negative, or neutral. Failing to take care of ourselves and recognize the stressors in our life is what leads to lasting, chronic conditions like depression, anxiety, OCD, and other mental health issues. Self-care is about tapping into your own mind and body, making sense of the way you are feeling, and taking action to right any wrongs that may be present.
We move so quickly through life that sometimes we forget to stop and evaluate how we are feeling, why we feel the way that we do, and what we can do to change it.
So all of that being said, where should you start on your self-care journey? Here are 5 tips to start integrating mindfulness and self-care into your daily life.
1. Start keeping inventory on your feelings
Take stock of how you feel. You don’t have to go so deep as to why you are feeling the way you are, but just recognize what emotion you are experiencing. This will assist you in making decisions. For example, if you are under a lot of stress in your personal life and you recognize that, it might help you realize you should hold off one more day on a major work decision. Or on the other hand, if you just got the best news of your life and are extremely excited, you might want to say yes, yes and yes to all of the plans your friends have made for this upcoming weekend to celebrate, but you should maybe only go out one night because you have a lot to get done before Monday. This goes along with the saying “never act out of anger”, and “sleep on it”. Recognizing and categorizing (stress, anger, sadness) the emotions you are feeling is the first step to taking action against any negative effects these feelings may have.
2. Isolate yourself for 10 minutes a day
This is the time to reflect on your day and understand why these emotions came over you. You may think that you were stressed all day at work because your boss sent out a memo in the morning that bothered you, when really it was coming from an argument with your significant other that occurred the day before. This is the time to identify the emotional triggers in your life— defined as “a response to a person, situation, event, dialogue, reading, film, or other content providing entity, that provokes a strong emotional reaction. This will help you avoid (or at least regulate your exposure to) the things that are causing emotions like stress, sadness, and grief. For example, if you have a family member in the armed forces, maybe you should not indulge in the overwhelming amount of military homecoming videos available on YouTube. On the contrary, for someone who recently had a family member or someone close to them return from the military, these videos may be one of their favorite things to watch. This time is about identifying YOUR emotional triggers and developing ways to manage them.
3. Figure out what makes YOU feel good.
This one is all about discovering the little things that you enjoy. Maybe its buying a new book and setting apart a little bit of time each day to read. Maybe its spending time with your “outside-of-work friends”, or maybe even scheduling a date night with your S/O (or your best friend if you’re still on the market). The point is, look for the little things in your life that make you happy, and do those things for yourself more. They don’t have to cost money, and they certainly do not have to involve others. Remember: this is all about YOU and the things that make YOU feel good.
4. Watch what you say
We need to change the way we talk about mental health. Try to remove the words OCD, depression/depressed, and anxiety from your vocabulary, and instead use some other words to describe how you feel. So instead of saying “Ugh im so depressed”, “That gives me anxiety” or “I’m super OCD about that”, try expanding your vocabulary with words like this:
Instead of saying depressed, say:
- Sad
- Unhappy
- Despondent
- Down
- Low
- Bummed out
Instead of saying anxiety, say:
- apprehension
- angst
- jitters
- nervousness
- concern
- heebie-jeebies (my personal favorite)
Instead of saying OCD, say:
- Particular
- Precise
- Detail oriented
- Anal retentive
- Fusspot
- Nit-picker

5. Talk to a medical professional
Finally, if you are experiencing severe symptoms or symptoms that you feel are beyond your control, please do not hesitate to reach out to a healthcare professional near you to seek support. Sometimes mental health issues are out of our hands, and self-care is not enough. Great strength is found in reaching out to someone for help, and the most beneficial person is going to be a mental health counselor, psychiatrist, or psychologist. If you’re not comfortable reaching out to a professional, try talking to a friend or two about how you have been feeling, as talking about it and having two heads trying to make sense of your feelings can be helpful.
Mental health is very touchy, tricky, and for the most part, taboo. I hope that this post has provided you with—if nothing else— a little bit of insight on the growing challenge that many people are facing today. Even if you are not experiencing any great stressors in your life, try out these tips, as there is always room for improvement!
Thank you so much for reading, and as always, happy living J
P.S. Check out this link below for a short youtube video about OCD!
https://www.youtube.com/watch?v=FsOzNavYF6wse
#MKT400UWL
6 notes
·
View notes
Text
MY EXPERIENCE WITH IV NUTRITIONAL THERAPY (MODIFIED MYERS COCKTAIL)

In 2015, as a result of stressful occasions in my individual life, I endured a severe episode of adrenal fatigue. Extreme exhaustion also after a complete evening's rest, muscular tissue weak point, brain fog-- all the excellent things. I found myself unable to recuperate on my own and so I began a course of IV nutritional therapy.
After an admission like that, I imagine you may have a few concerns for me. What is IV nutritional therapy? Exactly how does it function? What are the advantages? Is it "one size fits all?" For how long does it require to really feel the results? Did the treatment help me recover? Read on for more information concerning my experience with IV nutritional therapy: the ups, the downs, and also a couple of techniques I discovered along the road to make it go much more efficiently.
IV Nutritional Therapy
IV nutritional therapy is extensively used by option and corresponding medication professionals as a way to address and also deal with the symptoms of numerous problems such as fatigue syndrome, late phase adrenal exhaustion, fibromyalgia, chronic sinusitis, asthma, immune disorders, and lots of others. It is also utilized to soothe signs of migraine headaches and carry out heavy metals detoxification.
Exactly how Does it Work?
Intravenous shots supply a high dosage of minerals and vitamins directly right into the bloodstream, bypassing the digestion system. Yes, we are supposed to get our nutrients from the food we consume, but sometimes, specifically when nutrition malabsorption exists, food is inadequate and we need a high concentration of trace elements in order to give a boost of energy to our cells and aid the healing process. IV nutritional therapy offers that increase.
What is the Advantage?
The advantage is boosted nutrient absorption. Your body will certainly obtain and absorb a much greater concentration than you would with a dental dosage. This is a definite benefit for people struggling with an autoimmune disease due to the fact that they commonly manage nutrient malabsorption as well as diminished levels of minerals and vitamins.
One Dimension Fits All?
When it comes to IV therapy, the Myers alcoholic drink usually enters your mind. A standard infusion, the Myers cocktail consists of magnesium, calcium, B vitamins, as well as vitamin C and is generally recommended to improve power and also sustain a delayed immune system, yet there are, in fact, several other kinds of dietary IVs readily available. If you are collaborating with a practical medication expert, which I highly advise, your doctor might make a decision to customize the fundamental Myers formula to fit your certain needs. This is called a modified Myers.
MY EXPERIENCE:
Working carefully with my doctor, I got a changed Myers mixed drink, specifically adjusted to my demands, followed by a glutathione (a powerful antioxidant enzyme) injection (image, far ideal). My mixed drink of macronutrients was blended right before each injection to make sure optimum quality. Each treatment lasted 30-40 minutes as well as was carried out in a dimly lit, peaceful room. I located it best to put down and unwind during the treatment. You can also request a blanket to keep you cozy!
Full disclosure: I really did not feel wonderful right away after my very first couple of injections. There was no abrupt and spectacular boost of power or mental clearness. Actually, it was rather the opposite. My initial few injections were adhered to by a "collision" lasting regarding two days during which time I experienced increased tiredness and also a tempting urge to rest.
Worried I was having an allergy to the shots, I spoke with my medical professional. Why was I feeling worse when the shots were intended to make me feel much better? He told me that my reaction had not been uncommon and also was really a normal effect of the cleansing procedure. Keep in mind that I was in a state of true exhaustion as well as my autoimmune disease was most likely flaring due to stress and anxiety. Even more, I am understood for being very sensitive to supplements and such. To make things less complicated for me as well as to ease the results of the detox, my doctor minimized the concentration of the macronutrients I was obtaining.
With the assistance and peace of mind of my medical professional, I decided to proceed the shots as well as see what would occur. I likewise saw to it to schedule my IVs on Fridays in order to have the weekend break to recoup.
Turns out, my doctor was right! I began feeling much better and better after each treatment. I was experiencing boosted energy throughout the day and more mental clearness. Initially, the effects lasted for a couple of days, after that, gradually, my energy began staying up in between each weekly injection. I understand now that nutritional therapy isn't expected to be a quick fix, however rather a sluggish procedure of rebuilding your health and also energy at a deep mobile level. That takes some time! Yet the effects are long lasting. When I obtain a nutritional IV currently, I really feel raised power that lasts for days.
I likewise require to point out the truth that, thanks to these micronutrient shots, I haven't been sick at all this winter when people are falling ill left and right. The injections strengthened my body immune system versus viral infections.
HOW I BENEFITED FROM NUTRITIONAL THERAPY:
power boost
raised psychological clarity
decreased inflammation
strengthened body immune system
Where to Get IV Nutritional Therapy?
Many natural medicine practitioners use nutritional therapy. You can likewise obtain injections at IV bars, which are personal clinic/spa/wellness centers providing "one dimension fits all" IV packages. My recommendations? Deal with a physician that knows you and also recognizes any and all of your pre-existing problems. Your physician needs to also run a complete panel blood work prior to beginning any type of nutritional treatment.
TROUBLESHOOTING:
Blood Vessels Small as well as Uncooperative? Hydrate well a number of days prior to the treatment. You can additionally try working out directly prior to the treatment, sitting in a sauna before the therapy, and/or asking the phlebotomist to apply a warm water container to the insertion location. Shot Stinging? When the IV is put right into the criminal of my joint, where the blood vessels are larger and also blood circulation is strong, I do not really feel anything. When the IV is inserted closer to my hand, on my wrist or directly on my hand where the veins are smaller, the injection can sting a little bit. Ask the phlebotomist to lower the rate of the drip. Also, carefully rubbing your arm will aid soothe the sting. Excruciating Glutathione Injection? Yes, glutathione can sting when infused also quick. Ask the phlebotomist to go very gradually or to dilute the glutathione in saline option.
MY GUIDANCE:
If you are embarking on a nutritional therapy regimen, I would urge you to be client and give it a long time. Many people report feeling the valuable effects just after 4-5 sessions. For me, it took much longer. Remember that all of us start in a different place so your experience will certainly be reflective of where your body is at the moment you start. Also, make certain you are working with an educated group you trust. This is specifically important if you are managing an autoimmune disease or persistent illness.
In general, I located IV nutritional therapy to be very handy. Remember that there are no over night repairs, however if you are patient, you may locate that IV nutritional therapy is a fantastic enhancement to your healing trip. Do your research study, discover a practitioner you trust fund, as well as best of luck! Improved energy is within your reach!
The post “ MY EXPERIENCE WITH IV NUTRITIONAL THERAPY (MODIFIED MYERS COCKTAIL) “ was seen first on Squirrel In The Kitchen
If you want to get your own vitamin drip treatment, visit http://www.theivlounge.ca/ located in Toronto, Ontario. Or call them at (647) 549-3484 for inquiries.
0 notes
Text
February/March 2019
NOTE: I have a habit of writing in several tenses at once. While my conscious mind does its best to reign this in, these subjects may occasionally call for a looser perspective so I’ve decided to let it happen organically ;)
I’ve always had a very close connection to certain numbers and number patterns, specifically strong is my relationship with “18″ or “118,″ so for much of my life I’ve consciously looked forward to living through the year 2018. It was a great year, looking back now, as I finished a momentous personal artistic project and finally took steps toward improving my mental health and gender dysphoria by speaking with professionals about getting prescriptions I didn’t realize I’ve needed for many years.
In the fall of 2018, for whatever reason, I felt an impulse to double down in October on fun spooky subjects. I have a great deal of free time, my work is usually freelance. October is my birth month and a popular month with many of my friends as it tends to celebrate the strange, and as I’ve grown into a young adult I’ve wanted to keep in touch with the ‘fun side of life.’ So this October I indulged in several youtube videos about cryptids. Several videos turned to dozens of videos and soon I found myself reliving a chapter of my life I hadn’t thought about in years; when I was in middle school I had a huge paranormal-investigative phase where I’d spend hours online on cryptid sites and forums, stoking the fires of what I assumed was a kind of beautiful expression of the human imagination. I remember thinking I didn’t care whether or not some of the creatures were “real,” I knew many were absolutely real to enough people who took the subject seriously and that was enough for me. I’ve always been incredibly sensitive to emotions and “vibes,” later I learned I could be described as an empath. Something about the way certain people talk about their experiences seemed to tell me they were not lying and had no reason to. Then puberty took over my soul for many years and I lost my focus to socializing over habitual sex and drug use.
In the summer of 2011 my closest childhood friend took his own life. We always had a very special bond and connection throughout our development and would sometimes even attempt telepathy with each other. The examples I remember, I would try too hard and it wouldn’t work, however we would have moments when neither of us were trying and a connection could be felt. In our late teens we had drifted apart from each other and I prioritized trivial things over our friendship. I still hold onto guilty moments of “what-if” and “I should have.” His remains a loss of eternal ripples for me. Only recently has the guilt seemed to gradually subside as I’ve made conscious decisions to move forward and continue living life. Over time I began to see some of the possible lessons he was teaching me through his decision. We’ve had many conversations and emotional reunions in dreams. It took me many years to feel fully comfortable with the idea of carrying on; I entertained thoughts of suicide almost every day following his passing for a very long time, frankly far too long. In 2017 I was taught traditions of transcendental meditation (which I have since admittedly fallen behind on in daily practice), and 2018 was a year in which I felt energies finally begin to shift. (What’s that about 7 years to fully replace your cells?)
So, we’re back to October 2018. I’m devouring youtube clips of ghosts and UFOs and bipedal creatures with a renewed interest, for no real “reason” other than it simply felt right and it was justified by the time of year. Certain horror movies and shows stimulated connections between spiritual subjects and metaphysics, significant connections toward which I’ve gently been nudged in various ways over my life. I watched Unacknowledged on Netflix where I was introduced to the Disclosure Project and Dr. Steven Greer. The argument was compelling and intriguing and I had to see more. I began making my way through the Disclosure Project’s witness testimony videos, first choosing the stories that interested me before watching as many as felt relevant. I began sharing my ‘secret passion’ with select friends who already know me to be a little looser than others when it comes to having a grip on what is established as reality. Many of them were bemused, if a little bit concerned for my well-being and mental health, but for the most part they listened with curiosity and respect. Some very close friends were not as receptive as others but I’ve come to learn that is to be expected. Throughout my life I’ve been a chronic over-sharer and I have a tendency to become overly excited about any sort of new revelation in my life. This 2018 paranormal revival was one of the first times I deliberately strategized in my mind about who I could talk to about the subject, the only other instance of this that comes to my mind is talking about my gender identity. I developed a way of bringing it up that feels light and jocular, allowing skeptics to smile and brush my words off as Me just being Me. I’ve always found great reward and fulfillment in fluid ambiguity; binary modes of perception can be unsatisfactory and inaccurate. Unfortunately I would come to learn that certain specific friends found my perspective to be extremely troubling and “not good enough” for “scientific argument.” Luckily this was not the majority, however please be careful of coming off as condescending if you choose words that tend to express more poetic/ambiguous concepts. If a friend does not understand you or feels that you’re being deliberately vague, they may feel like you are trying to push them away.
A few months pass and in late January my mind is brought back to the paranormal. I don’t remember specifically why, perhaps it was due to a series of dreams or a friend recommending that I resume making my way through The X-Files. I feel a great pull toward this chase. I feel daily compulsions to research these topics in earnest and I start seeing more and more connections between various paranormal topics and cryptid experiences. Eventually the connections become undeniable, I felt there was simply no way this many unconnected people would conspire to draw connections between topics like UFOs and the Sasquatch People without feeling in their hearts that it was true. I discovered this synchronistic bridge to be the most difficult for skeptics to swallow in terms of belief/comprehension. Even some close friends who once experienced a legitimate CE1 together (standing next to a totally un-phased pizza delivery guy, no less) expressed doubts when beings like Sasquatch People were brought up. This is all, to me, very understandable and forgivable. This research and spiritual work requires a great deal of patience. Even though our beliefs diverge at certain paths, there is still mutual respect and love.
Throughout February I dive deeper and deeper until I feel as though I’ve broken through the initial phase of fear and paranoia regarding coverups and conspiracies. Eventually my focus shifts from the aggressive mental atmosphere of Governments and their Falsehoods to the gentle mental atmosphere of People and their Truths. Through certain videos, I begin to feel tremendous love and warmth. Watching and listening to honest, loving accounts of Earth Human connections with Sasquatch People and Star Nations, I become suddenly emotional and will weep for several minutes, sometimes having to pause the video just to smile at the Universe until I can compose myself. I am profoundly struck by the words of Kewaunee & Kelly Lapseritis, Garret Duncan, and Su Walker & Rev. White Otter, along with the videos of research from Ontario uploaded by Mike Paterson and friend LeeAnn. I have been touched by the dictated writings of the P’onti who have been so generous with their outreach. I eagerly await further development! ♥
0 notes
Text
Episode #11 The Plant Based Diet "Prescription"
Hello again! This is the podcast show notes section of Health Interventions For Your Practice! The topic at hand is the plant-based diet.
I truly do not believe that the answer to everything is pharmaceutical based. I also believe that we have gotten so far off track that it’s going to take extreme measures to turn things back around. Just look at our patient population. They are getting sicker and sicker. The comorbidity rates are climbing, as are the obesity rates. The inflammation that is brewing inside of us from our poor choices and environmental exposures is contributing to our current state of health or lack thereof.
One of the ways that you can reduce inflammation, lower blood pressure, treat diabetes and hyperlipidemia without medications is by adopting a plant-based diet. It is actually becoming more mainstream to adopt a plant-based diet. Which is making it easier to find more plant-based options at restaurants and grocery stores. Which makes it easier to have this conversation with patients.
The plant-based diet is not one that everyone is going to want to participate in. I am completely aware of that. I am also aware that you were going to get objections about giving up meat and animal-based products in the beginning. I have been able to have patients agreeable to trying this for a few days per week or having only one meat-based meal per day. There are many ways to help implement a more plant focused diet into your patients’ lives.
There are many views on plant-based and many objections to plant-based nutrition. And there are misconceptions about a plant-based diet. Almost anything can be taken from good to bad, depending on one’s interpretation. Some of the misinterpretation that takes the plant-based diet from good to bad is actually what is perceived plant-based in the lay community. Some have adopted the view that just not eating meat or meat byproducts constitutes as a healthy plant-based diet. Not really so. Often, they are still consuming high amounts of sugar, saturated fats and other processed by- products from processed foods.
So here we go... into the plant-based world.
I’m going to start with the benefits of a plant-based diet, how to do this healthfully, some of the things to be aware of in a plant-based diet and how to start the conversation with your patients.
Just like most everyone else, I once upon a time scoffed at the thought of not eating meat or animal-based products. How can I go without dairy? How could I ever live without cheese? How could I possibly get enough protein?
After doing some research on plant-based diet, I decided to get on board. I have a very strong family history of diabetes, hyperlipidemia and heart disease. I do not want any of those diagnoses for myself. I also like to practice what I preach as you know. I cannot ask my patients to do some thing that I have not tried myself. I like to be able to experiment with myself or very close family members to monitor outcomes and safety. And also, to be able to give real life tips. What did I have to lose anyway? If it didn’t work out, if I felt terrible, if my labs didn’t show any improvement, it was only me that had to suffer.
Well......, guess what happened?
I have lost 25 pounds without even trying! I am never hungry; I do not crave anything. I do not feel deprived. I feel better, I sleep better, I have more energy. My skin is clearer, and I recently drew a lipid panel on myself. My total cholesterol was 194, my HDL 95, triglycerides 33 and my LDL 67. I wasn’t sure that those numbers were actually possible! My previous cholesterol was 194, triglycerides 115, HDL 80 and LDL 91. My glucose from 99 to 87. TPO antibodies from 15 to 0.
For full disclosure, I will also admit that I have not been participating much in exercise lately, as I’ve been a bit busy with this new adventure in podcasting and online training program production. Which, I Feel has been a wonderful trade-off for a short period of time. I tell you this so that you know my numbers were not skewed by my exercise or some crazy relaxing, stress-free lifestyle. I AM a practicing provider you know. And we are currently in the midst of the Covid pandemic, which makes any practicing provider’s life a bit more insane trying to keep up with the guidelines and adjustments in everyday practice.
I am sure that many of you have seen the Netflix shows and documentaries on the plant-based diet by now. Many of them are pretty good at getting the general population to stop for a moment and think about what they might be eating, but shortly after they watch the show they go back to a normal regimen. And that is where, once you have learned some of the benefits, hopefully you will be able to give it a try yourself and encourage your patients to continue on a plant-based diet and support them.
Dr. Dean Ornish is one of the Pioneers in developing protocols for using a plant-based diet and other lifestyle modifications to reverse heart disease. The evidence is very clear of all of the benefits associated with reducing the intake of meat and animal-based products. Heart disease CAN be reversed with a plant-based diet! I will save the soapbox of some of these things for future episodes, specifically one on dairy products. I don’t want to get on too much of a tangent with you. I want to introduce this to you slowly, so that you may consider doing the plant-based life yourself and having that discussion with your clients with a little bit of knowledge of what to be mindful of.
A plant-based diet is one that consists primarily of food from whole plants. This includes vegetables, fruit, nuts, seeds, legumes and whole grains. There are many variants of the plant-based diet out there, including vegan, vegetarian, lactovegetarian, ovo-vegetarian, Mediterranean, and I’m sure many more.
I am not trying to label specifically or get into those details, I am purely interested in giving you the overview of a solid plant-based nutritional program for your patients, that focuses on the vegetables, nuts, seeds, legumes and whole grains.
The Benefits:
High fiber intake is inevitable if done right. This will show benefits by decreasing inflammation, increasing bowel regularity, clearing a fatty liver and stifling insulin surges. The outcomes from this include lower glucose levels, lower cholesterol, lower blood pressure and weight loss. Fiber is also great for increasing satiety.
A well-rounded plant-based diet will increase general health and wellness with the increased intake of phytonutrients. Phytonutrients are best gotten from our food, rather than from supplemental forms. Phytonutrients are known to be powerful antioxidants and anti-inflammatory agents to help fight and prevent cancer, chronic illness and to boost the immune system. And I think we could all use a little immune boost right now.
Wait! Did I mention weight loss? Did I mention that was one of the major benefits of adopting a plant-based diet?
A Few Considerations…
When one is doing a plant-based diet, they must still be very aware of what they are eating. You have to be sure to include certain nutrients that you may not get in abundance from all plant-based foods. Iron and B12 are two of the most commonly depleted nutrients on a plant-based diet. If you are aware of this, you can adjust your diet accordingly. Vitamin B 12 can be easily gotten with nutritional yeast, which has a distinct taste, referred to as cheesy. It can be sprinkled onto foods. I like to put it on my spaghetti squash, topped with tomato sauce and then nutritional yeast. A few other sources of iron include cashews, kidney beans and black beans, as well as spinach. So again, a well-rounded plant-based lifestyle can still include these nutrients you need. One of the modules in the wellness and weight management course that I offer is dedicated to phytonutrients, micronutrients and essential elements we require for optimal functioning.
Now let’s talk about the interpretation of, or some misconceptions of, a plant-based diet. A plant-based diet is high in nutrients. It is high in a variety of food sources that come from plants. A true plant-based diet DOES NOT include French fries, pastries, pasta and other chemically processed foods or food like substances. I have seen many say that they are plant-based that still inhale everything but meat without regard and are still perplexed at how they could be gaining weight and not getting control over their chronic diseases and still feeling extremely fatigued. That is not the intention of a plant-based diet. A plant-based diet is meant to be filled with good wholesome vegetables, legumes, grains, fruits and unprocessed food sources. It Does not include cheese, which is very high in saturated fat and comes from animals. There are vegan cheeses that are made from cashews and nutritional yeast. I have tried some of those. Some better than others, but I just choose not to even go that route. I save the calories.
How to start the discussion with your patients…
When you start a discussion with your patients, you may get a lot of kickback. Especially if you’re in a place like me, where we were raised on Home cooking, with meat and potatoes required at every dinner. And with grandmas trying to make you fatten up a little bit.
As a side note, I’m not sure how many of you have a grandmother like this, but when I was growing up, mine kept a can of lard under the kitchen sink that she cooked with! Looking back, I am not sure how I live through that experience. I ate fried eggs in it every morning that I stayed with her, and it was used for gravy making and soup making to add flavor. I have to laugh about it now or I would probably vomit. I’m not sure how she lived to be 83, but she did. My theory is that she was a hard-working woman that never sat down to rest much and had eight children to chase after. I can also still see her using a sickle to knock down weeds on an embankment in front of her house every summer. That would definitely burn off a few extra calories, decrease stress and maybe ward off ill effects from that can of lard.
Ok, back to discussing the plant-based life with your patients.
The plant-based discussion is one worth having with patients. If you start by asking what they typically eat in a day, to see where they are on the scale of carnivore, you’ll have a pretty good idea how much work will be involved with this discussion. Review the benefits of going plant based. If they have multiple comorbidities, or is they are chronically fatigued or trying to lose weight, they may be willing to implement the strategy.
If they have IBS symptoms or chronic constipation and you discuss with them that increasing their fiber through a plant-based diet May help to regulate their bowels, they may be more willing to implement the strategy.
If they have chronic pain or fibromyalgia, that cannot be attributed to anything diagnostically, they may be more willing to implement the strategy.
If you’re about to add another medication to them to better control their diabetes, cholesterol or blood pressure, they might be willing to implement the strategy.
If all else fails, have a discussion with them about sexual dysfunction. It is well documented that sexual dysfunction, most commonly erectile dysfunction, may be attributed to early cardiovascular disease. The arteries in our body are not selective to the effects of atherosclerosis and buildup of lipid Plaques. All of the arteries are being clogged up with saturated fats that come from meat and animals-based products. Dr. Ornish has shown that this could be reversed with a plant-based diet. There have also been studies to show that there will be a significant improvement in erections and sexual function with the adoption of a plant-based diet. After this discussion, they may definitely be willing to implement the strategy.
I have many ways to get my point across to patients. Or, maybe I should say to help them get what they need and want in a persuasive and effective manner. Remember, when you speak to someone from THEIR viewpoint of health, you’ll get a whole lot further in your conversations. If you are speaking with a gentleman that is suffering from erectile dysfunction, whether that dysfunction be from medication side effects or from physiologic disease processes, they are willing to listen to you about how to restore and improve function.
So how do we start the implementation process?
I start with, “can you decrease your red meat to once per week?” then, I move into “can you decrease all animal-based consumption to three days per week?” And then I asked them to pay attention to how they feel on the days that they didn’t eat meat.
On the days that they are not eating meat, I have to prepare them for what to eat and how to modify their usual intake so that they aren’t hungry, and they feel like they aren’t being deprived.
There is a lot of flavor in a plant-based diet. There’s food to eat. You’re not being deprived to be on a plant-based diet. You can substitute many things for meat.
I find it best to give examples, so they know they are not going to struggle. I have already mentioned to you that I use spaghetti squash instead of pasta, nutritional yeast instead of Parmesan cheese. How about black bean tacos? Instead of hamburger chop up black beans or don’t chop them up, depending on preference, season them with taco seasoning, as you would hamburger, heat them up and top them with your usuals, minus the sour cream and cheese of course! But you can use salsa and jalapeños. Maybe spinach instead of iceberg lettuce to add to the nutritional value. I have done the same with burgers. Using black beans or kidney beans, chopped up, adding in seasoning, some ground flax for additional fiber and omega fatty acids, pat them into a burger shape, put them on the grill or fry them in olive oil or avocado oil. There are many many ways to make substitutions!
I do offer a patient-based health interventions program that includes an online weight program loss for them. I do weekly videos of how to prepare meals for weight loss, from a plant-based standpoint, that are posted on the health interventions Facebook page. Feel free to utilize this for yourself or for your patients.
If you have been listening to the podcast or follow me on social media or my website, you know that I do offer a weight management program that you can implement into your practice right away that focuses on nutrition, lifestyle and modifiable factors. And that course covers a wide range of topics the attribute to overall health and wellness. It isn’t only about nutrition and what medication you can prescribe to make someone lose weight.
I believe you need a full program and that we need to re-educate our population to bring ourselves back to a healthier place. This weight management program can very easily be 100% plant based and you will learn further how to modify the plant-based diet into a keto form to get them to lose weight rather quickly. This is followed by a transition into a maintenance form of the plant-based diet that still allows for adequate amount of protein, healthy fats and high fiber carbohydrates without gaining back any weight. Once you are able to learn and perfect this, you will see energy levels sore The Inflammatory state their body is constantly in When on a diet high in animal-based products Will drop significantly with a plant based diet, as will the fatigue. The program does include a downloadable recipe guide with recipes that you can give to your patients, including a plant-based meal plan to get them started. If you’re not interested in doing the whole program, but maybe have been intrigued by some of the phytonutrient discussion today, I will make that course available for you as an individual module. Just go to the notes from this episode on the website nphealthinterventions.com for access. you can also go to healthinterventions.com/phytonutrients for details on how to get that.
I hope that I have been able to help you understand a bit more about the benefits of a plant-based diet and how to start the discussion of that with your patients.
Have a great week! May it be filled with many Health Interventions!
0 notes
Link
Utilize them and achieve quite a few backdrop on your subject and you’re simply convinced relating to your problem, you’re ready to perform your research you need to remedy that concern. That makes it less complicated since you purchase a jump on your exploration. As the Austrian him self offers described, “The problem of the mother nature of navel half truths appears to worry more and more people than a single would probably think when you’re getting started.” Released around The Lancet, Bart www.moody.edu Knols’ 1996 research, “On our smell, malaria many other insects, plus Limburger cheeses,In . Reported report investigated quantity happen to some sort of shrew – which was initially skinned, disemboweled, parboiled and cut into segments – whether or not it had been ingested, without ingesting, using a man. How will little location appraisal be important throughout research?
A Report on Researchable Topics to get Biology
I currently have a lot of wellness matters. Does “How does bacterias with contemporary animal meat cause problems?Inches serve as the scientific disciplines analysis subject matter? Is there a new “fountain of youth” enzyme that is going to help us are living for a longer time? Could increasing slumber help the reminiscence involving Alzheimer’s sufferers? You could underline these individuals, or simply just create the small print.
In this article, i will assessment the most interesting concepts in this connection you will want to look into your current crafting procedure. A wildlife were being certified to identify sections by simply frequently Monet or even Picasso; as well as most importantly they then confirmed to be able to discover functions by frequently founder which in fact have certainly not been demonstrated in their mind during the coaching period. After you are sure you understand, you should choose a matter pertaining to studying. Here a few homework document tips for people:
14 many weeks back out of U . What’s the very best recent remedy for epilepsy? What are ideal Fibers Reinforced Hybrids? in addition to own managers. that is a massive subject so i really need a fantastic particular attention grabber. How does one select a research theme?
19. The particular Space Details involving Penguin Poop
Can an individual advise study themes in actual biochemistry? Will taking in gluten-free strengthen your gi tract? I feel trainees within high school. Published within 2007, this papers – “a?Which can feel more substantial – one pound involving head or simply a single lb with plumage?A A prospective perceptual first step toward some sort of psychological riddle” – learned that members ranked this lb of lead while appearing to be more heavy with an “above chance” rate. Whether Endophytic infection for a venture suggestion is actually a applicable subject or otherwise? I wish to find out whether or not Endophytic infection in cheaper seed groupings is relevant?
State the overall biology problems in in which ball.
Seahorses – Seahorses are usually scarce in the undeniable fact that oahu is the men who seem to offers the unborn infant. Explore the actual biological ingredients that make seahorses distinctive.
How can polio always be exterminated? Exactly why has got the disease resurfaced?
What are we learned about a arena from meteorites?
Behind a brain in the office. Neurosurgery troubles: Recall foremost neurosurgeons along with achievements.
When can a passed dow genes become revised any time they want simply by conventional medicine?
Hormones while being pregnant. Talk about and look at this junk improvements this take place when pregnant, especially in the initially trimester.
How do tissue protect against disease?
Here are a number of useful chemistry and biology homework subject areas related to grow pathology: Our freelancers have already made it easier for 2,000+ students get over its study objectives. There also easy the business of a brief history connected with The field of biology. What will be the least difficult scientific disciplines matter for your research report?
How can certainly your bioluminescence GFP out of jellyfish provide with professional medical apps?
What are classified as the prospective positive aspects as well as perils associated with stalk cellular exploration?
What has got the Foreign Room Stop learned that can be most essential?
Explore this chemistry at the rear of your frog’s opportunity to bounce.
Just what must we perform in relation to our planets atmosphere? What exactly is better advertise meals reading and writing to youngsters? to get medical practitioners? Can anyone propose a motivating topic with an magazine cardstock pertaining to disorders? Typically, I propose that pupils produce a brief report on the content many people receive from a source after which it their solution to in which details, that may contain the things they acquired, just what exactly inquiries the information created you think of, along with what a person imagined ended up being useful or perhaps crucial. Here are a few topics associated with which: Released around Late 2001, “The primary the event of lgbt necrophilia inside mallard Anas platyrhynchos” represents Kees Moeliker’s strange encounter. What is a good method to maintain your kids’ consideration for the duration of instructions?
Now that you’ve some background on your own subject matter and you’re certain of your concern, you are to do the research you need to respond to that query. Also, they found that a “full flask may strike some sort of target with pretty much 70 percent far more power compared to a bare bottle,” but that sometimes is capable of doing smashing a personality’s cranium. The number of varieties of pesky insects are normally found around (position)? Good level, Jenna–I’ll buy speech online add a Hormone balance portion. It is possible to existing exploration on chronic lymphocytic the leukemia disease? An organization in the College or university of recent Central america brought about by means of evolutionary psycho therapist Geoffrey Miller enlisted the help of 17 qualified entertainers.
How many various type of butterflies come in (place)? Is really a theme you currently know something with regards to. It’s also possible to consider these suggestions: Which are the latest innovations in battery scientific discipline?
By way of example, screening waters prospective. I have done one more content which supplies 75 matters on Mindset that will help to make great study paperwork. What is definitely the simplest research theme for your homework paper? So how does Darwin’s theory assist us to investigate human being behaviour? Hi, the information are excellent, but Now i am looking for a topic pertaining to trial and error analysis about bodily or perhaps since they call it, placed scientific discipline. dissertation will likely be their magnum opus – your zenith of their academic achievements.
Really does having Sickle cell phone condition have any positive aspects? Generally, learners take pleasure in investigating insect pests which can be sometimes useful or perhaps wonderful. Take into account the adhering to Several subject areas for your chemistry exploration document. Which research theme for Sickle mobile phone disorder should i talk about? Here are a handful of more hot topics:
Analyze the final results along with bring conclusions.
Scientists that review attitudinal epigenetics claim that upsetting suffers from for example the Holocaust or maybe the Ethnical Revolution inside Asia in fact affect the Genetic passed down to a higher generating. Will be conduct epigenetics legitimate? In that case, exactly how should we implement this idea?
Have an excellent portfolio
State the chemistry concerns in that ballpark.
What is the likelihood that this Planet can be hit using a massive asteroid or perhaps comet like the one regarded an possess wiped out this dinosaurs? What can carry out over it?
Inside of a fantastic turn with paradox, Generate. A topic you realize quite a bit with regards to. For making a real framework, total the next steps: “Optimizing a nerve organs properties and recognition regarding memorized cat meals: by using a person’s tastes panel” explains the actual weird method to get human being tasters for you to “profile the flavor along with feel on the choice of kitten meal products” – which include examining “meat bit in addition to gravy/gel ingredients.Inch The effect in this about the number of work uses to your beer- and chocolate-tasting sectors remains to be observed. EunJae, you should take a look at http://writingbee.com/marketing-essay-writing-service my own research test concerning the salinity water around farming.
from Patriot Prepper Don't forget to visit the store and pick up some gear at The COR Outfitters. Are you ready for any situation? #SurvivalFirestarter #SurvivalBugOutBackpack #PrepperSurvivalPack #SHTFGear #SHTFBag
0 notes
Text
Identity economics: Who are you? And how does it affect your spending?
“Who are you?” my cousin Duane asked me on Saturday afternoon. We'd spent the day playing nerd games together and were taking a break for pizza.
“What?” I said. I wasn't expecting a philosophical question over supper.
“I don't think you know who you are,” Duane said.
“What do you mean?” I asked.
“I don't think you know who you are,” he repeated. “You write about money and frugality, yet you spend $200 on dinner.” Duane was referring to the fancy meal we'd had in May at a Michelin-star restaurant in France. I knew it had been bugging him, but he hadn't said anything about it until now. (And that meal cost $267.41 for the two of us, not $200.)
“You paid $1900 for your used pickup, but you don't wash it. It's filthy. You buy new clothes that you don't need, but you leave your old clothes on the floor so that your cats pee on them.” It's true. Kim and I have a cat that will, from time to time, pee on my clothes.
“You say you don't like attention, that you don't want to be a celebrity, yet you're always taking on new work that puts you in the spotlight. You're thinking of doing a course for Audible, for instance, and you're talking about doing more speaking gigs — even though you hate speaking gigs,” Duane said.
All of these things were true. I couldn't argue.
“Who are you?” Duane asked. Well, that's a mighty fine question, Duane. That's a mighty fine question.
A Digression
In 1862, French novelist Victor Hugo published Les Miserables, one of the greatest novels of the nineteenth century. Long and sprawling and full of digressions (just like Get Rich Slowly!), the book explores the many facets of human nature: the good and bad, the humorous and poignant, the ordinary and sublime.
Les Miserables wasn't popular with critics when it was released, but everybody else loved it. It sold well when it was published and continues to sell well more than 150 years later. The book has inspired several several film and television adaptations. And, of course, it's the source of one of the most successful stage musicals of all time.
Turns out PBS recently aired a new six-part Les Miserables miniseries written by the always-awesome Andrew Davies. It's on my watch list.
Although Les Miserables contains a ginormous cast of characters, two stand at the heart of the story:
Jean Valjean is the novel's protagonist. Arrested for stealing a loaf of bread to feed his sister's seven starving children, he spends nineteen years in prison (five for the original crime, fourteen more for various misdeeds). Upon parole, he assumes the identity of Monsieur Madeleine. As Madeleine, he builds two factories, becomes rich, and is appointed mayor of a small seaside town. Valjean is a good man who occasionally finds himself on the wrong side of the law.
Javert is the novel's antagonist. (It's not right to call him a villain. Nothing about him is villanous.) Born in prison to deplorable parents, he grows up to become a prison guard — then police inspector. Javert is obsessed with upholding the law, which includes pursuing and punishing Valjean for his past misdeeds. His worldview is shattered when he realizes that not all laws are moral, that sometimes the moral course is not the lawful one.
What's fascinating — mind-blowing, actually — is that Victor Hugo based both Valjean and Javert on the exact same real-life person. They're both loosely modelled on Eugène François Vidocq, a French criminal turned criminalist. (You should open that link in a separate tab for later reading. Vidocq's life is fascinating. Among other things, he's regarded as the first-ever private detective and the “father” of modern criminology.)
That's right: Both the protagonist and the antagonist of Les Miserables were inspired by the same man. And, even more mind-blowing? Vidocq was also the inspiration for Sherlock Holmes. (Go read that article!)
Who Am I?
The amazing thing (to me) is that Jean Valjean himself is two people! He is Jean Valjean, yes, but he spends years posing as Monsieur Madeleine. As the latter, he's a wealthy factory owner, he's mayor of Montreuil-sur-Mer. He is a force for good in his small world. He is, at once, both Valjean and Madeleine, just as Vidocq is at once both Valjean and Javert.
In a 2012 New Yorker piece praising “the persistent greatness” of Les Miserables, Adam Gopnik wrote, “Hugo believed in, relished, luxuriated in, contradiction — he thought that we show ourselves most truly when we are seemingly most opposed to our double natures.”
When I posted about this on Facebook in April, John from ESI Money observed that this adds a whole new meaning to the song “Who Am I?” from the musical.
“Who am I?” Valjean sings as he's forced to reveal his identity in order to save an innocent man. “Who am I? I'm Jean Valjean!”
Yes, that's true — but Jean Valjean is also police inspector Javert.
youtube
True story: I'm a devoted fan of musical theater, and “Who Am I?” is one of my favorite songs from any show. It induces frisson — it gives me goosebumps — every time I hear it. Every time.
What I like about this clever bit of character creation from Victor Hugo is how it highlights our inherent dual natures. We, as humans, are inconsistent. We are complex creatures. At the same time, we can be both good and bad. I truly believe that most of us do what is right most of the time — but each of us also sometimes makes poor choices. We do things that seem to go against who we say we are and what we believe.
In Valjean and Javert, we get to see human nature dramatized in two men forever at odds, just as we are each forever at odds with ourselves.
Me, Myself, and I
As I was walking the dog this morning, I found myself meditating on my own personal duality. I am at once the hardest working person I know…and the laziest. I am the smartest person I know…and the stupidest. I am the kindest person I know…and the meanest.
Recently, I've grown increasingly frustrated with my seeming inability to “do the right thing”. I know that there are certain actions I could take (and should take) to improve my health, to build this website, to maintain relationships with my friends. Yet I do not do these things. I actively avoid them.
Why is this?
Here's an example. I could solve a whole host of problems if I were to get regular aerobic exercise. Over the past year, I've done a fine job of strength training, but for some reason I've become allergic to sweat. I do whatever I can to avoid running or biking or otherwise increasing my heart rate.
It's not that I can't do these things. I know I can. And I like them. I've run half marathons (and walked a full marathon). I've completed a century ride — one-hundred miserable miles on a hot and windy summer day. I did Crossfit for five years. I'm capable of strenuous exercise, and I know it.
But I'm not doing that exercise right now. I'm avoiding it.
Three months ago, as the sun started to show its face here in Portland, I wheeled my bicycle from the bottom of the hill to the back office. I wanted to make it easy to hop in the saddle and go. But you know what? I've ridden the thing exactly once this year. The bike is just sitting there, pleading with me to ride it.
The same goes with the website. You all know that I can crank out an article a day. I did it for three years between 2006 and 2009. I did it for the first three months of 2018. When I put my mind to it, I can write well without sacrificing quality.
Yet, for some reason, it's tough for me to publish even once a week lately. My mind is elsewhere. I have no inspiration. This wouldn't be so bad if I were at least handling other site maintenance chores, but I'm not. The site redesign is nearly finished, but it isn't live because there are still things I need to do. I'm not processing guest articles. I'm not posting to social media.
I've no doubt that some of this malaise stems from my chronic depression. But I also know the best way to shake the self-loathing is to actually do something, you know?
Which leads me to fundamental question I find myself facing: If I know what is right, why don't I do it?
I have no answer.
Impossible Expectations
This year, as every year, my depression and anxiety became especially strong during the spring. What's different about this year is that I sought out a therapist.
A few weeks ago, she asked me about my writing. We hadn't talked about it before. “What does success look like for you when it comes to your work?” she asked.
“Success means publishing three articles per week,” I said.
“Why?” she asked.
“Because then I'm giving my readers lots of material. I'm helping them. When I give them a lot of material, they want to come back more often. When I publish more material, more people find the site by search. When I publish more material, I make more money.”
“So, you want to publish three times per week?”
“I guess so,” I said. I thought about it a little. “But I hate the pressure that pace puts on me.”
“Why?” she asked.
“Because I don't enjoy it. I don't do great work under time pressure like that. I want to take my time. If I decide to write an article on, say, the history of retirement, then I want to read a book on the subject. Maybe two or three. I want to think deeply about it. Then, I want to take the time to write the best article out there about the history of retirement.”
“You realize you've just told me two very different things, right?” my therapist said. “You've set up contradictory goals for yourself. Plus, you're asking yourself to be the best. That's a tall order. No wonder you're stressed. You have impossible expectations for yourself.”
When I think about it, my therapist is right. I do have impossible expectations for myself — on a lot of things. I have contradictory goals. It's as if there's a Jean Valjean inside of me and an Inspector Javert. And they want different things. Neither is wrong — but they can't both have their way.
But to which do I yield? Am I Valjean or Javert?
At the end of the session, I lamented my dual nature. “I tell other people to be proactive,” I said, “to take charge of their own lives, but I have a hard time doing that myself.”
“Do you think that makes you a hypocrite?” my therapist asked.
“No,” I said without hesitation.
“Good,” she said.
“I think it makes me human,” I said. “I write about the things I struggle with personally. When I started writing about money and getting out of debt, that's because I needed to get out of debt. Now, when I write about tracking spending or having a sense of purpose, that's because I need these things.”
Mindful Spending
So, this is all very interesting on a philosophical level, but what does it have to do with personal finance? Lots, actually.
We make our purchasing decisions based on who we are and who we want to be. If we're not clear on who we are and who we want to be, our choices tend to be arbitrary. They're spontaneous and not based on anything other than immediate desire.
When you're clear on who you are and what you want, it's much easier to practice mindful spending, to be deliberate about the things you buy and own. If you identify as fitness-conscious, for instance, you'll be much less likely to be tempted by cookies and snacks in the grocery store. If, like me at the moment, you identify as a “lapsed” fitness junkie, well then it's much easier to succumb to temptation.
Who we want to be also affects how we spend. In fact, I suspect that much wasted spending — not just for me, but for everybody — is what I'd call “aspirational”. It's not based on our actual habits and actions but on what we wish we did.
Take my bike, for example. I bought it last year but have ridden it only three times in fifteen months. Like I mentioned earlier, it simply sits there, pleading with me to ride it.
I have a good friend who once decided he'd like to learn woodworking. His father had always built and repaired things around the house, and my friend aspired to do the same — even though he had never done so in 35 years of life. He bought a stack of woodworking books, then acquired several expensive tools. He never used them. These were aspirational purchases, based on somebody he wanted to be, not the person he was.
From what I've seen, a lot of folks do this sort of thing with cookbooks. They want to try new recipes and new cuisines, so they gradually fill a shelf with cooking manuals — cooking manuals that they seldom use.
It's because of this relationship between money and identity that I'm so insistent that GRS readers write a personal mission statement. When you're clear on your purpose, it's much easier to make sure your spending is aligned with your values, that your financial decisions are based on who you are instead of some idealized version of who you want to be.
Identity Economics
In their fascinating (if dry and academic) book Identity Economics, George Akerlof and Rachel Kranton explore how our identities shape our work, wages, and well-being.
“In every social context,” the authors write, “people have a notion of who they are, which is associated with beliefs about how they and others are supposed to behave. These notions…play important roles in how economies work.” Our identities determine how we earn a living and how we spend our money.
Akerloff and Kranton say that large portions of our identities are shaped by the environment:
Identity, norms, and social categories may appear to be abstract concepts, but their reality is both powerful and easy to see. Norms are particularly clear when people hold an ideal of who they should be and how they should act.
Here's an example: Many folks who discover the early retirement movement do so through the awesome work of Mr. Money Mustache. He has a strong voice and a popular website. Over the past few years, he's accumulated a passionate army of followers who call themselves Mustachians.
When a person identifies himself as Mustachian, he subscribes to a certain set of values, to particular ways of working with money. Driving is frowned upon. A high saving rate is encouraged. Thrift is a prized virtue. This is identity economics in action.
Akerloff and Kranton are careful to note that our personal identities are not static. They change. Our larger identities change slowly over time, but we can also shift roles rapidly in daily life.
The latter is easiest to see. “Over the course of a day,” they write, “a woman may see herself as a mother at home and a professional at work.” I'd add that she might see herself as an athlete in her running group, a civic leader as a member of the city council, and a Mustachian when she's hanging with her financial friends online.
Each of these is a different identity — or perhaps a different facet of her overall identity. And each affects how she works, saves, and spends.
People change over their lifetimes too. From the book:
People often make decisions that come back to haunt them. We overeat, we smoke, we spend too much, and we regret it. [This is due to] time inconsistency. People have different selves at different points in their lives. The new self could regret the decisions made by the old self…
Sometimes these transitions are anticipated, and people plan accordingly. But often, people only imperfectly anticipate who they will later become.
Look at my own life over the past decade. Who I am today is drastically different than who I was ten years ago. And twenty years ago. Sure, the core J.D. remains the same — once a nerd, always a nerd! — but my values, which are constantly evolving, have morphed and my day-to-day life is sometimes unrecognizable.
During the past ten years, much about my personal identity (and my resulting financial choices) has changed:
I deliberately chose to purchase a small home in “the country”.
I drink beer. I drink coffee. I ride a motorcycle. All of these actions are new.
I lost fifty pounds through years of exercise and healthy eating. Then I gained back forty of those pounds through years of neglect.
I sold Get Rich Slowly — then I bought it back.
These changes, large and small, all affect how I manage my money and how I spend my time. As my identity changes, so do my financial habits.
Related reading: In a strange coincidence, The Guardian published an article on a similar subject last Saturday: “Are you really the ‘real' you?” This piece, which is terrific and well worth reading, looks at how some people change their lives entirely — and why.
Order and Light
At the end of the Les Miserables, after Jean Valjean frees Javert instead of killing him, the police inspector faces an existential crisis. Victor Hugo writes:
He saw before him two roads, both equally straight; but he saw two; and that terrified him — him, who who had never in his life known but one straight line. And, bitter anguish, these two roads were contradictory. One of these two straight lines excluded the other. Which of the two was the true one? His condition was inexpressible.
Inspector Javert's moral certitude proves to be his undoing. Like many folks who are certain they know what is real and what is right, Javert spends years ignoring evidence that controverts his beliefs. He thinks he knows the truth but in reality is blind to it.
youtube
When, at last, Javert recognizes that he's been in error all this time, that things are not as black and white as he believed them to be, it's too much for him to bear. Rather than face a world filled with ambiguity and uncertainty, he takes his own life. He jumps in the river and drowns.
Before he kills himself, though, Javert has a sort of revelation. He realizes that Jean Valjean and his alter-ego, Monsieur Madeleine, may have seemed like two different people, but they were one all along. They were two sides of the same person. Valjean was both criminal and hero.
It's all well and good to want to be a fixed, constant person, to have an identity that never changes. But that's not how healthy people work. Healthy people learn and adapt and grow. Who you are today is not the same as who you'll be tomorrow — or who you were yesterday.
As you change, your values will change too. Your goals will change. Your spending will change. What you want to do for work will change. And, yes, there will be many times when you are internally conflicted, when like Javert you are faced with two parallel roads, both of which are “true”.
Summing Up
Who am I? That's a great question.
I'm a guy who writes about money and frugality, but I'm also a man who is willing to — once in a lifetime — spend $267.41 to experience a Michelin-star restaurant in rural France. That's a clear example of mindful spending: I planned the meal weeks in advance and looked forward to it with great anticipation.
I'm a guy who can't bring himself to purchase a new car, so I buy a 25-year-old pickup for $1900. And I don't wash it. I value the vehicle but see no sense in spending the time, money, and energy to clean something that will never look pretty.
I'm a guy who buys new clothes from time to time — don't we all? — but who, yes, is careless enough to leave them on the bedroom floor even though I know my cat likes to pee on them. (Stupid cat!)
I'm a guy who hates public speaking and who doesn't want to be the center of attention, yet who has a deep desire to teach people about personal finance. (Especially the personal side of it all.) This leads me to do things that seem incongruent with what I say I want. I take on months-long projects that stress me out. I agree to fly across the world to talk to people. (Just yesterday, Paula Pant and I had a conversation about how the hassle of attending events is worth it for the friends we make.)
Who am I? I'm J.D. Roth.
The post Identity economics: Who are you? And how does it affect your spending? appeared first on Get Rich Slowly.
from Finance https://www.getrichslowly.org/identity-economics/ via http://www.rssmix.com/
0 notes
Text
What is A2A2 Milk
You have heard me talk about A2A2 milk. Some of you may not know what that means. You may wonder if it really matters to you and your family. I’m going to fill you in on some of that information today.
First let me say welcome to all the new listeners and welcome back to you veteran homestead loving regulars who stop by the FarmCast every week. I appreciate you all so much. I’m so excited to share with you what’s going on at the farm this week, a little bit about A2A2 milk and a great and tasty recipe. Let’s just jump right in.
Today’s Show
Homestead Life Updates
What is A2A2 Milk?
Ice Cream Base Recipe – with downloadable document with flavoring ideas
Homestead Life Updates
Cows
The cows are doing great. We have a new calf and the last one for a while. There is likely one more, but that cow is way behind the others. In fact, we are getting ready to breed some of them again in a few weeks. Cloud will deliver so late that she likely will not get bred back this year.
We are selling all of our bulls. We have six. Yes six. There is 2-year-old Sam. He is 95% Normande genetics and the sire of this year’s crop of calves. Then we have 1-year-old Ray’s Rocket – mostly we call him Rocket Man. Lastly is the group of newlings born this year. All four are for sale. Some are currently being negotiated for but I’ll put a link in the show notes to the Facebook page where all of their information can be found. If you are looking to improve the genetics of your herd, this is the bull for you.
Sheep/Goats
Lambert is so fat right now. He will be receiving his bottle twice daily until nearly all of the milk replacer is gone. Then I will switch him to once a day for a week or maybe two before weaning him completely off.
If you want to get a whole or half lamb, speak up now. It will be months yet before these are ready for your freezer. We have one lamb and/or 2 half lambs currently available. A whole lamb yields 30 to 35 pounds, sometimes more of meat. Half lambs, half that. You can see the cuts that come on a whole or half lamb on our website. www.peacefulheartfarm.com/shop/lamb-package.
Orchard and Garden
There is always so much going on around here that a lot of stuff gets pushed back. Thinks like birthing, gathering and storing milk, making cheese, taking care of animals all have the highest priority. The garden and the orchard, not so much. My garden is still overrun with weeds, though I was able to dig out my carrots and surprisingly there are lots that beat the grass. Watering the garden does have a priority or it would all simply die. Other stuff slows down or stunts growth. The bottom line is we will still get a crop, but perhaps not as large as if we had gotten the weeds out and fertilized more often.
The peas are just such a crop. They are producing like mad and I will be picking them within the week, I think. Then they will have to be processed in some way. I’m scaring myself with all of that. There are just not enough hours in the week.
I still don’t even have everything planted. The green beans need to be put in the ground. The peanuts need to be replanted; I have no idea why not a single one sprouted. And the eggplant is going to wither away to nothing if I don’t get it out there in the garden.
Everything needs to be weeded. Everything needs to be fertilized.
Scott is diligently digging out the orchard from the waist high grass. It would be great if we could graze some of the animals in there, but they all eat the trees. We are still investigating how to get the sheep in their without having them raise up on their back legs as high as they can and eating all of the leaves off the branches they can reach. The goats are a complete disaster anywhere near the orchard or the berries. They will eat the bark off of the trees, killing them. And because they like to eat woody stemmed plants, they will decimate blackberry vines and blueberry bushes. No, we don’t want them anywhere near the orchard.
On the upside, they did a really great job of clearing out the wild blackberries on the island in the big pond. It is now quite pleasant to sit out there and enjoy being surrounded by water and nature.
Quail
We are newbies with the quail. It is unbelievable how quickly those quail grew. They outgrew their brooder box a good week before we had planned. Outside they went as we were having a warm spell. There were a couple of cool nights but these are wild birds and they faired very well. They are only barely over 2 weeks old and are fully feathered. The tiny birds that were barely the size of a gold ball are now the size of a baseball – perhaps even a softball. It’s amazing. They will begin laying eggs in as little as six weeks from now. Yum, yum, we look forward to it.
Four eggs are required to equal one chicken egg. Our plan is to have about 30 laying hens and 6 roosters for breeding. We will need to continually hatch out new ones as their lives are actually quite short and they only lay for a year or two.
Creamery
The creamery – ah the creamery. So much still to do there and Scott has so little time to do it. We really need that building completed. However, as I mentioned earlier, there are priorities. First the animals, then the perishable milk and cheese, then the garden and orchard. The creamery, as an inanimate object comes in last place. There are even maintenance projects that take precedence. Fences, driveways, pathways, other infrastructure – all has to be kept up to ensure the safety of our animals.
It’s a lot but I wouldn’t trade it for anything. We work long hours every day – very long hours every day. Alarm goes off at 6:00 am and though 10:00 pm is bedtime, more often it is 11 or 11:30 before that happens. And every bit of it is worth it. There is never any lack of meaning in our lives. Boredom is something very distant in the past. The constant attention to the next task makes us know that we are alive in God’s wonderful creation.
One thing that evolved through nature is the composition of milk in cows. Recently, some of the genetic content and protein structure of milk has changed.
What is A2A2 Milk?
There is a great deal of scientific gobbledygook about the proteins and how they are broken down or not. I’ll try to keep this layman friendly and skip most of the mumbo-jumbo lingo. By the way, did you know that gobbledygook is an actual word that my spell-checker knew? Who knew? Well, my spellchecker knew.
A2 milk is cow's milk that mostly lacks a form of beta-casein proteins called A1 and instead has mostly the A2 form.
A1 and A2 beta-casein are genetic variants of the beta-casein milk protein that differ by one amino acid. Casein is a family of related phosphoproteins. These proteins are commonly found in the milk of mammals, comprising about 80% of the proteins in cow’s milk and between 20% and 45% of the proteins in human milk. Sheep and buffalo milk have a higher casein content than other types of milk with human milk having a particularly low casein content. Casein has a wide variety of uses one of which is being a major component of cheese. We respect our casein.
A genetic test, developed by the a2 Milk Company, determines whether a cow produces A2 or A1 type protein in its milk. The test allows the company to certify milk producers as producing milk that does not metabolize to beta-casomorphin which is an opioid peptide or protein fragment derived from the digestion of the milk protein casein.
I know, I’m getting too scientific with the lingo there. All that means is that the chemical composition of A2A2 milk may benefit our health because it is digested without inflammation that might arise from BCM-7 produced by A1 beta-casein. Consequently, A1 proteins may be detrimental to our health. That causes great push back from the gigantic dairy industry as A2A2 genetics is rare in Europe (except France) and the US. That would really disrupt their operation if their milk was found to be harmful – while others had milk that was beneficial.
As with so many health-related topics, the science is divided on whether or not there is reason for concern regarding the A1 protein in milk – whether there are adverse health effects from its consumption. Personally, I’m erring on the side of caution, as I do with so many other foods. I’ll go with tradition as opposed to modern fads in nutrition. We are breeding our cows for the A2A2 genetic conformation.
And when I say modern fads in nutrition, I mean everything that came pouring out of the 20th century and that continues to pour out in the 21st century. I’m talking about three square meals a day, the food pyramid, and the modified food pyramid. I’m talking about low fat diets, vegan and vegetarian diets, the Mediterranean diet, the South Beach diet and so on. All of these so-called nutrition experts are literally experimenting with our health as human beings. We evolved over thousands and thousands and thousands of years eating locally grown food, whatever it was. Historically, in the tropics the diet was heavy in fruits, nuts and greens, in Alaska fat predominated. In other regions protein was the main source of dietary sustenance. You must find what works for you.
Which brings me back to A2A2 milk.
History
In the 1980s, some medical researchers began to explore whether some peptides (including peptides from casein) that are created during digestion might have negative or positive health effects.
Interest in the distinction between A1 and A2 beta-casein proteins in milk began in the early 1990s via epidemiological research and animal studies initially conducted by scientists in New Zealand. The scientists found correlations between the prevalence of milk with A1 beta-casein proteins in some countries and the prevalence of various chronic diseases. The research generated interest in the media, as well as among the scientific community and entrepreneurs. If it were indeed true that BCM-7 created by A1 beta-casein is harming humans, this would be an important public health issue.
Scientists believe the difference in genetics originated as a mutation that occurred between 5000 and 10,000 years ago—as cattle were being taken north into Europe with the mutation subsequently spreading widely throughout herds in the Western world through breeding.
The percentage of the A1 and A2 beta-casein protein varies between herds of cattle, and also between countries and provinces. While African and Asian cattle continue to produce only A2 beta-casein, the A1 version of the protein is common among cattle in the western world. The A1 beta-casein type is the most common type found in cow's milk in Europe (excluding France where our Normandes with predominantly A2A2 genetics originate). It is also the most common type found in cow’s milk in the US, Australia and New Zealand.
Let’s talk about the possible health benefits.
Health Benefits
Symptoms of stomach discomfort, such as gas, bloating, and diarrhea that occur after consuming dairy products, are typically attributed to lactose intolerance. However, some researchers believe that it is BCM-7, not lactose, that affects digestion and produces symptoms similar to lactose intolerance, in some people.
A study on Chinese adults with self-reported milk intolerance compared the effects of drinking regular milk that contained A1 and A2 proteins with A2-only milk on intestinal function, stomach discomfort, and inflammation.
The participants consumed 8 oz of milk twice a day for 2 weeks. They reported worse stomach pain after they consumed the regular milk but no change in symptoms after they drank the A2 milk.
Participants also reported more frequent and looser-consistency stools while they drank the regular milk. These symptoms did not occur after they consumed the A2 milk.
So, what MIGHT be happening on the other side of the coin?
Potentially Harmful Effects of non A2A2 Milk
Notice the words “might and “potentially” there. I’m not making any claims here. Some of the effects can include:
Inflammation
In the same study mentioned above, researchers also looked at markers of inflammation in the blood. They found the participants had higher levels of inflammatory markers after they drank the regular milk.
Brain function
The research showed that milk could impact brain function. Study participants took longer to process information and made more errors on a test after drinking regular milk compared to A2 milk.
Type 1 diabetes
The potential risks associated with milk containing A1 proteins include an increased risk of developing type 1 diabetes.
Some studies have shown that children who drink cow's milk protein at an earlier age than others have a higher risk of developing type 1 diabetes. However, other studies have not shown the same association.
The research also suggests that the amount of milk a child consumes could influence their risk of developing type 1 diabetes, with higher milk consumption observed in children who develop the condition.
At least one study showed a link between the consumption of A1 protein and incidence of type 1 diabetes, although this kind of study fails to prove that it is a direct cause.
Some animal studies have shown associations between cow's milk consumption and a higher incidence of type 1 diabetes. One study in mice found that 47 percent of the mice that had A1 protein added to their diet developed diabetes, while none that had A2 protein added did so.
However, other research does not support the hypothesis that there is any association between milk consumption and a higher incidence of type 1 diabetes. There are links in the show notes for both sides of this discussion. Debate about the potential health effects of A1 and A2 milk is ongoing.
Research suggests that A1 beta-casein causes adverse digestive symptoms in certain individuals. But the evidence is still too weak for any solid conclusions to be made about the supposed links between A1 beta-casein and other conditions, such as type 1 diabetes and autism.
That said, A2 milk could be worth a try if you struggle to digest regular milk.
There you have it. The basics to the why of A2A2 milk. I’ll let you decide. Again, we like to err on the side of caution. We have two A2A2 certified cows and will be testing the rest of the herd as we move forward with our dairy operation. Go to the show notes for the links to the research I referenced.
Speaking of milk, how about an ice cream recipe for your A2A2 milk and cream.
Ice Cream Base Recipe (Download Flavorings)
When it’s warm outside, a cold refreshing dish of ice cream can really hit the spot. This is a basic ice cream recipe that can be used as a base for many different flavors. I’ve included a download link to the flavorings.
This silky, luscious and very classic custard can be used as the base for any ice cream flavor you can dream up. These particular proportions of milk and cream to egg yolk will give you a thick but not sticky ice cream that feels decadent but not heavy. For something a little lighter, use more milk and less cream, as long as the dairy adds up to 3 cups. You can also cut down on egg yolks for a thinner base, but don’t go below three.
Time: 20 minutes plus several hours’ cooling, chilling and freezing
Yield: about 1 ½ pints
What You Need
2cups heavy cream
1cup whole milk
⅔ cup sugar
⅛ teaspoon fine sea salt
6 large egg yolks
Your choice of flavoring (download here)
What To Do
In a small pot, simmer cream, milk, sugar and salt until sugar completely dissolves, about 5 minutes. Remove pot from heat. In a separate bowl, whisk yolks. Whisking constantly, slowly whisk about a third of the hot cream into the yolks, then whisk the yolk mixture back into the pot with the cream. Return pot to medium-low heat and gently cook until mixture is thick enough to coat the back of a spoon (about 170 degrees on an instant-read thermometer).
Strain through a fine-mesh sieve into a bowl. Cool mixture to room temperature. Cover and chill at least 4 hours or overnight.
Churn in an ice cream machine according to manufacturer’s instructions. Serve directly from the machine for soft serve, or store in freezer until needed.
Final Thoughts
I hope your days are filled with as much love and joy as you can stand. We love our lives here. Yes, we are busy beyond belief. Yes, it’s a little stressful sometimes. I just find it so fulfilling. From the time I was a child I was told to work hard for what I wanted. I was also told that I was too smart to not be college educated and have a career. So, no physical work. That was for those not smart enough to get out of that poor and decrepit existence. Funny isn’t it? In the end, educated to the max, I prefer the hard work. And indeed, some of it is smart brain work. But the best and most enjoyable part involves sweat.
Particularly, I love our cows and our dairy operation. Check out the references I provided for the research around A2 beta-casein. Then sign on to our herd share program with our A2A2 milk and value added products, go to www.peacefulheartfarm.com/virginia-herdshare. Read, ask questions, download the documents. We’d love to do business with you.
And as this Memorial Day weekend stretches into Monday, I hope you’ll try that ice cream recipe. There is nothing more traditional than everyone taking turns operating that crank on the ice cream machine. Well, we use the electric method. Likely you do too, but the principle is still the same. Enjoy your time with your family and friends.
If you enjoyed this podcast, please hop over to Apple Podcasts, Subscribe and give me a 5-star rating and review. Also, please share it with any friends or family who might be interested in this type of content.
As always, I’m here to help you “taste the traditional touch.”
Thank you so much for stopping by the homestead and until next time, may God fill your life with grace and peace.
References
Peaceful Heart Farm Bulls for Sale
NIH published study
Nutrition & Diabetes Study
The A2 milk case: a critical review
Recipe Link
Ice Cream Base
To share your thoughts:
Leave a comment on our Facebook Page
Share this show on Twitter, Facebook and Instagram
To help the show:
PLEASE LEAVE A REVIEW for Peaceful Heart FarmCast on Apple Podcasts.
Subscribe on iTunes, Stitcher Radio, Google Play Music, TuneIn or Spotify
Donate on Patreon
Website
www.peacefulheartfarm.com
Patreon
www.patreon.com/peacefulheartfarm
Facebook
www.facebook.com/peacefulheartfarm
Instagram
www.instagram.com/peacefulheartfarm/
NEW!! Peaceful Heart FarmCast Episode. Enjoy!!
0 notes
Text
AbbVie, Inc. (ABBV) Management Presents at Morgan Stanley 16th Annual Global Healthcare Conference (Transcript)
AbbVie, Inc. (NYSE:ABBV) Morgan Stanley 16th Annual Global Healthcare Conference September 12, 2018 11:40 AM ET
Executives
Bill Chase - Chief Financial Officer
Scott Brun - Head of AbbVie Ventures and VP of Scientific Affairs
Analysts
David Risinger - Morgan Stanley
David Risinger
Okay. So thanks everybody for joining us for the session with AbbVie. I just need to refer you to disclaimers at www.morganstanley.com/researchdisclosures. It’s very much my pleasure to welcome Bill Chase and Scott Brun. So Bill is the Company’s CFO. I’m sure many of you are familiar with him and he’s been in the position for several years and has overseen the Company’s execution of delivering results above expectations for the last several years. Scott is currently Head of AbbVie Ventures and Vice President of Scientific Affairs. He was previously the Head of Pharmaceutical Development and has been instrumental in advancing the Company’s pipeline. So it’s my pleasure to welcome them today. I guess I wanted to start off with a question regarding the execution against your plan.
So, clearly the Company has delivered better than expected performance over a number of years. Investors are skeptical about the longer term given the fear of the biosimilar threats to HUMIRA. So maybe you could sort of tackle it two ways. Talk about the financial targets for 2020 and your confidence in achieving those? And then maybe Scott, you could talk in a bit more detail about the pipeline and its ability to ultimately offset HUMIRA longer term?
Scott Brun
Sure. Well, so David thanks for having us. We always appreciate the opportunity to come out to the Morgan Stanley conference. I think as we start with the big picture and how we’re tracking relative to the long range guidance and particularly in light of that concern around what happens post 2022 when you have an LoE for HUMIRA in the U.S. Like the reality is, since even prior to the spin, this company has been preparing itself for what was going to be in an eventual LoE event around HUMIRA and that was known on day one and our strategy that we said internally and with the board was always trying to build the capabilities and the assets within the Company to be able to negotiate that events and remain a growth vehicle. And at that point in time, we said look our aspirations is to be top tier growth.
Now obviously there's two parts of that equation, one is, what is the HUMIRA curve look like and when, and you've seen us execute very nicely with our legal strategy and the settlements around the U.S. events to delay the onset of LoE in 2022, 2023 time period. The second piece though is what are you going to grow with? And that becomes essentially a pipeline question. And we always knew that we needed to have very, very good differentiated assets. We wanted to be a focus company. We wanted to focus primarily in the areas that we knew that play to our strengths.
So we focus primarily on immunology and oncology. And we set about building what we think is one of the most attractive late stage pipelines in the industry. And we can go through obviously in some detail and Scott's got a lot to say on that thing as well. But at the end of the day, what we called out last time, we updated the strategic plan, isn't if you take HUMIRA out of the mix and you benchmark us back to 2017, which is one of the plan was last updated. We had a business when we looked at our pipeline that we felt was -- we felt comfortable saying was going to grow from about $10 billion in sales size up to $35 billion in 2025.
And the way we're going to do that was through some best in category assets and then which Scott will share with you. Our strong franchise we built in HemOnc with IMBRUVICA and VENCLEXTA products like or at least that we are just underway launching and more recently launched like MAVYRET. And when we look at those assets and we look at the de-risk nature as well as the efficacy and safety that they've shown in a very broad clinical trial, we feel very comfortable that they can get into the market in their respective places and deliver upon those gross projections.
And so we remain very, very confident, pipeline is a huge part of the story. And if you look at our pipeline, not only do we have attractive assets, but this is a very diversified pipeline. We're not delivering all that grows just with one or two assets. There is 5, 6, 7 different aspects at play which we also think is fairly unique when we look at our peers.
David Risinger
Excellent. And maybe Scott, you could add a little bit on and since speak to investors pretty frequently which of the pipeline assets are potentially most underappreciated by investors as you discuss these biggest of pipeline contributors, longer term?
Scott Brun
No, absolutely, I didn't focus on that. Again, David thanks for having us. Bill hit on the number of important themes. When we launched AbbVie, now almost six years ago, focus was incredibly important to make sure that we had the right capabilities from discovery through commercialization market access in a few set areas where we really thought that we could differentiate ourselves with both internally discovered and developed assets as well as externally sourced opportunities. I think that’s been playing out extremely well. I mean I could take the rest of the time going through the qualities of the late-stage pipeline, but maybe I can hit on a few high points.
Certainly, in hematologic malignancies, when you look at it IMBRUVICA and VENCLEXTA, these are two first-in-class agents that are transforming hematologic malignancies of several types. I mean we look at IMBRUVICA the fact is in chronic lymphocytic leukemia, first and second line. It’s really becoming a mainstay of therapy. We've also seen significant results in Waldenstrom's macroglobulinemia. Most recently, we actually had a label update with a study looking in IMBRUVICA combination with Rituxan that again provides us a chemotherapy free option for this particular disease, opportunities in other malignancies like mantle cell lymphoma also tend to build the overall opportunity for IMBRUVICA.
We’re going to continue to progress IMBRUVICA particularly in first line CLL where we think there’s a lot of opportunities in particular in combination with VENCLEXTA first-in-class Bcl-2 inhibitor which have a Phase 2 study captivate to demonstrate the combination of IMBRUVICA and VENCLEXTA can drive to minimal residual disease, essentially no detectable disease by advanced diagnostic methods in 70% to 80% of patients. And so this could really transform the care of CLL away from toxic chemotherapies to a drug combination that could put patients into long-term remission with much less tolerability baggage.
Now talking a little bit more about VENCLEXTA beyond these opportunities in CLL, we’re currently under regulatory review in acute myelogenous leukemia. This is a very devastating rapidly progressive disease that we’ve demonstrated that VENCLEXTA added on to standard-of-care in first line patients who can’t tolerate the harshest chemotherapy can double or triple complete response rates, which led to a breakthrough therapy designation from FDA.
And as I said, current regulatory review that could lead to an approval next year, VENCLEXTA a lot of opportunity in multiple myeloma where we are currently in Phase 3 looking at in combination with Velcade and dexamethasone in second line plus multiple myeloma. We also think there are opportunities in first line myeloma and certain genetically defined population, so a tremendous opportunity is there.
Moving on to our immunology franchise, risankizumab, the partnered assay with BI and anti-IL-23 that has demonstrated some of the highest responses that we’ve seen in patients with psoriasis PASI 100 scores, complete skin clearance on the order of 50% to 60% Superiority versus STELARA, HUMIRA the ability to treat patients who have failed prior TNF inhibitors in a quarterly dosing pattern. And so, risa is currently under regulatory review as well.
Our selective JAK1 inhibitor, upadacitinib, for which we disclosed 5 trials in rheumatoid arthritis. We studied this drug in first line therapy patients who are naive to any treatment, all the way through patients who have failed prior TNF inhibitors. We've lifted Upa with and without methotrexate. We've demonstrated Superiority to HUMIRA. We have over 4,000 patients worth of data. And then every one of these contexts, Upa is performing at the top of the class, certainly directionally, although we have no head-to-head studies directionally better than what we see with baricitinib vs tofacitinib.
I think we've shown from the safety perspective that our rates for venous thromboembolism which has become a point of discussion with this class, really do not differ from placebo and our randomized controlled trials, nor do they worsen overtime, nor do they demonstrate any type of dose response. Certainly, if we want to get into a little bit more of the recent competitive context with recent risa and upa, David during the question we can do that.
ORILISSA, otherwise known as elagolix, the first new therapy for endometriosis related pain in a long time. This disease affects millions of women. They are unsuccessfully treated with combination of oral contraceptives or opioid pain management. We've demonstrated that with this oral therapy that affects the GnRH axis. We can lead to high levels of pain control and do it with a much improved side effect profile relative to show within the nuclear option Lupron.
So, we're in the launch phase of this drug right now. We're in Phase 3 in analysis of bleeding related to uterine fibroid. Another very common gynecological condition where again our two Phase 3 studies that have read out have demonstrated very high levels of efficacy, 75% or so significance of patients had significant reduction in their bleeding.
Again, I could keep going on and on. But I think the point here is as Bill said, diversified assets across a variety of different therapeutic areas that actually have potential beyond these initial indications that I've laid out. And I think as you seen with HUMIRA one of our themes is, to really understand biology and take it to places that it may not have been studied before.
David Risinger
Great. We could just follow up on the competitive landscape…
Scott Brun
We do a couple of announcements over the past year, so…
David Risinger
Yes, could you touch on those?
Scott Brun
Certainly, why don't we go ahead and start with the theme to data and what, I've always got to be careful about talking about someone else who is single study. To sum up what I'll say is based on what we saw from the Phase 2 data in the public domain, I took a Phase 3 data from this first trial or are consistent with that data set?
On the efficacy side both filgotinib and upadacitinib, as I said before directionally appear to provide the potential for improved efficacy relative to baricitinib or tofacitinib. We got to be a careful about our cross-study comparisons here of course especially since we don't know the baseline characteristics of the filgotinib population in total. I would say if you look at the ACR scores, there is puts and takes looking between upa and filgotinib. If you look at some of the DAS scores, which are a high stringent measure of disease control, low disease activity and clinical remission, I can certainly say that, again, all the caveats across study comparisons taking into account that for low dose of upadacitinib is performing every bit as well, if not maybe directionally better than what we see with filgotinib.
So, not seeing clear points of differentiation on the efficacy side, safety is harder to compare because we've got different bits and pieces of what's been shared. I'm glad no patients have venous thromboembolism on the filgotinib trial. But as we know, even patients on background therapy can see VTE. So I think before we can say exactly what that means, we need to see their whole program it's in context. And certainly, we've shared some information on infections, last year so on. I think at this point, it's too early to say that there is any kind of clear signal what differentiation on these low incidence events.
The one thing I do want to point out is that we will be filing an RA with upadacitinib before the end of this year, actually one of the things I must point out, before the end of this year, again, I don't know if Gilead had spoken to their timing when they were just in here. As I understand, the critical path for them is to complete the man-to-male reproductive study to de-risk the 200 milligram dose to see exactly what the benefit risk on that dose is. As I understand that that may put them more than a year behind our current filing timeline.
David Risinger
Got it. That's very helpful. Maybe we could pivot and Bill, you could talk about potential changes in U.S. drug pricing. Obviously, we have to wait and see. And if you could also touch on the notion of rebates going away, it sounds like a pretty big statement. And we'll still need to learn more on what the next steps are from HSS. But it'd be helpful for you to just frame it as you see it currently. And then touch on the rebate issue. Rick had spent a fair amount of time on the 2Q call. So one can refer to that transcript for lots of detail, but still be helpful because it's topic on investors' mind?
Bill Chase
Sure. So look, pricing has been a focus for the industry for the last several years. And it's clear that the administration has made it a focus in these years as well. So we historically whatever we do on our long range plan in the U.S. while we continue to believe the U.S. will remain a price positive environment. We always prudently scale back the rates of increases. So from a long range plan perspective, we've always kind of forecasted because it’s wise to forecast that way that the pricing environment will be getting a little tougher. But beyond the forecast, you've seen actions throughout the industry that have shown the dialogue around price is beginning to have an effect.
So for example, most companies now have moved to one price increase per year. We made a statement couple of years ago that we were doing that. And likewise, price increase is tend to be single digit. We have a statement similar to that as well. And so I think that you are beginning to see an impact through the industry a change in pricing behaviors. And of course, the fall through of those price increases are never in line with list. So I think if you really look at the data right now, you could say on a net-net basis while pricing is still positive in the U.S., it’s probably single-digit fall through, low-single-digit fall through maybe close to medium. But I would say try more like low-single-digits. So it’s clearly having an impact on the industry.
Now, we’re fortunate, we -- our growth is being driven by volume, not by price. If you look at our growth rates this year, they’ve been quite stunning on the top line. Probably last quarter, we had 17% operational growth, I think price overall was about 1% of that. So, when you have new products that are differentiated and you’ve got areas of high unmet need, you can drive impressive top and bottom line performance via volume and that’s what we’ve been doing.
Now, where pricing is going to go from here, little tough to call and obviously we got an initial look at the ideas in the blueprint. But while it was very comprehensive and had some truly creative ideas and we still need to see the details. And so we’re waiting along with the rest of the industry. We haven’t seen major changes to the contracting process to date, because of that. I think it’s kind of, we’re waiting and seeing. Although my guess is, our basic assumption and our long range plan is accurate and pricing will continue to moderate in this market.
In terms of the structural discussion around rebates and the questions that we would need to sort out, I think there’s two really that come to mind. First and foremost is how big, if we move into a paradigm where rebate contracting moves away, right. We move to some other type of contracting. The question is how big of a population of contracts are impacted. The Safe Harbor Provisions directly refers to government business, and the type of contract and that relies on PBM with the government is Medicare. If you look at AbbVie’s U.S. mix about 15% of our business was Medicare.
So, if it just stays within that area, you got 85% of the business in the U.S., which is not impacted. So we need to sort that out and I know some people feel that, it will rapidly move to commercial. We’re not sure, we have to see, how that plays out. That’s an important assumption. But maybe even more important is what rebate contracts are replaced with. We absolutely believe that the government and the market as not going to move away from a scenario, where you can give volume based contracts. It’s kind of a cornerstone of this industry, right. You give contracts based on based on patients under plan, the patient lives under plan and also the ability of that plan to drive compliance via formulary.
And those two things basically add up to a volume based contract. As long as volume based contracting is permitted, we don’t see any reason to believe that it wouldn’t be. It doesn’t really impact our business model. Now, we may need to figure out how you move from a rebate contract to a discount contract. But that’s just, that’s a contract form, it wouldn’t change the overall strategy. So yes, I understand why there’s a lot of concern around this change. But at the end of the day, I think it has less impact on manufacturers then perhaps the PBMs.
David Risinger
That’s extremely helpful. Let me pause there and see if there are any questions before I continue.
Question-and-Answer Session
Q - David Risinger
Okay. So one of the other topics that came up earlier in the year was the co-pay accumulator programs on the part of payers, and obviously, that has some marginal negative impact on reported sales. But could you just recap that and talk about how much of an inflection might be if more payers adopt such accumulators in 2019?
Bill Chase
Yes, sure. So, what we saw play out in the first quarter of 2018 was that there was a significant portion of patients that found themselves on high deductible plans with a co-pay accumulator. That number was roughly 4% to 5% of our commercial business which is about 80%. I'm talking to HUMIRA for example, okay. So if not necessarily not the lion's share, but it's a meaningful portion of patients.
And with this co-pay accumulator, especially did this concept was it ultimately ensured that the patient was on the hook for the full deductible even in the event that the manufacturer was willing to extend a co-pay card. Now, we fundamentally believe one of the issues in healthcare industry is co-pays that patients are burdened with. And so in most cases where we're able to, we offer co-pay assistance in order to alleviate that burden and that out of pocket burden on the consumer, the patient. We think that's absolutely the right thing to do.
What was somewhat perverse about the co-pay accumulators is it essentially could block our ability to do that. And so our view is, it is absolutely a poor contract form. And furthermore, we believe that a lot of people that were in co-pay accumulators may not clearly in plans that had co-pay accumulator, may not clearly understand what the ramifications for those plans were. And we're going to get surprise in the second quarter when they found out that their co-pay assistance have the limited a fixed amount and they now had to pay the deductible. And these deductible could be anywhere at $3,000 or $4,000. So a meaningful hit to your average patient, which in normal course would be covered by co-pay assistance and would not be taxing the patient out of pocket.
So, they get absolutely a horrific insurance form for the patient, it's actually rations their ability to get medications they need. And frankly the medications that we're selling, whether it be HUMIRA or anything else that we've got in our portfolio, these are for life threatening illnesses. And so to basically to private patients of access to that, that therapeutic, based on their ability to pay out of pocket, that was just absolutely the wrong thing to do.
So we recognize that this issue existed, we recognize that a lot of patients might be surprised. It was going to play out in Q2 and Q3 because really frankly, they had to burn through their co-pay cards before they discovered that they're still on the hook for the deductible. And in our Q1 call, we did adjust our HUMIRA guidance number down slightly to account for additional co-pay assistance that we would be able to provide these patients until we were able to sort themselves through this situation.
So, it came up as an issue on our first quarter comp. What I can tell you is it's largely tracking in line with what our expectations were. I think that the measures we've taken have largely been effective. There's been a lot of patient education by patient groups over the nature of these programs. So I like to think that we have wiser patients that will, if to the extent that they can avoid these sorts of insurance constructs in 2019, we certainly think there'll be inclined to do so.
And right now as we forecast '19, we don't see this patient population or the patient population that subject to this form of insurance coverage as expanding dramatically. We think it will largely be contained in a number roughly the size that we're seeing in '18.
David Risinger
Okay that's very helpful. And Scott, maybe we could pivot to IMBRUVICA. So there is an interesting Phase 3 trial in pancreatic cancer that's supporting out soon. Could you just frame that for us?
Scott Brun
Yes, absolutely. David, I mean, again it's better to go back and remind you all the overall strategy when we proceeded with the Pharmacyclics deal. So we felt that, look the foundation of this asset was going to be in the type of hematologic malignancies that I have spoken to particularly CLL. As you progress beyond there, we have increasing levels of risk adjustment that's spoken about some of the other malignancies where we seen great promise. PHOENIX in first line diffuse large B-cell lymphoma didn't measure up the expectations. That's a discrete duration of therapy against difficult effective standard of care, R-CHOP.
But again because of those considerations even the fact that we don't successful there, didn't mitigate our overall expectations for the assay. I would put pancreatic cancer in even another lower bucket with regard to the probability of success that we would apply to that. Obviously, this is a devastating condition for which there exist few good options. And so, we have a Phase 3 trial that is looking at IMBRUVICA added on to paclitaxel gemcitabine. That should be reading out before the end of the year, but again, this is high hurdle, haven't seen the data yet. But certainly, we don't have appropriate expectations for that.
Some of the other trials on IMBRUVICA that will be reading out, well certainly, we talked about CLL and again the iLLUMINATE trial which what's at IMBRUVICA plus GAZYVA versus chlorambucil GAZYVA to continue to enhance our body of data in first line CLL. We top line that and I think maybe able to say more on that at ASH. And then we've got ongoing study that we'll be reading out more in the 2019-2020 timeframe and things like follicular lymphoma first line mantle cell in particular.
David Risinger
Excellent. Well, I think we are out of time. I think we can go on the lot longer, but unfortunately we're out of time. So thank you so much for joining us. Appreciate that.
Source: https://seekingalpha.com/article/4205875-abbvie-inc-abbv-management-presents-morgan-stanley-16th-annual-global-healthcare-conference?source=feed_all_articles
0 notes
Text
The Ketogenic Diet and Its Physiological Effects on the Human Body
In this interview, Benjamin Bikman, Ph.D., an obesity and diabetes scientist and associate professor of physiology and developmental biology at Brigham Young University (BYU) in Utah,1 reveals how the ketogenic diet affects your physiology and supports optimal health.
“My main interest early on was looking at how the body adapts to obesity,” he says. “That was my master’s thesis. My master’s degree was exercise science here at BYU … I ended up pursuing a Ph.D. in bioenergetics at East Carolina University, under this wonderful scientist named Lynis Dohm, Ph.D.
His focus had been looking at how lipids cause insulin resistance. That was an interest of mine, because I thought this was starting to explain why and how the body becomes insulin-resistant in the midst of obesity … Insulin resistance is that connection.
During my Ph.D., we were looking at inflammation in people who were losing weight following gastric bypass procedures and how improved inflammation is likely part of the improvements in insulin sensitivity that people see post-bypass.
I followed that up with a post-doctoral fellowship at … the Duke National University of Singapore. They had this focus on cardio metabolic disorders. I … looked at inflammation as a particular mediator there … Then in 2011, my alma mater, BYU, came knocking. They wanted to do more diabetes research, and I fit the requirements … That got me, essentially, to where I am now …
If I really am getting this conviction, based on my own research, that insulin is key to not only diabetes but to almost every chronic disease, what is the best way to control insulin? That was when I insisted on only looking at published human clinical data — not rodents, not cells, not epidemiology, just clinical data.
The low-carb diet was just this very effective way to do that. That then got me interested in asking questions about ketones, which is what my lab is doing … how ketones are regulated by insulin.”
Bikman’s conviction that insulin is a key to health and disease prevention, and that controlling carbohydrate intake is the most effective way to control insulin, led him to start practicing what he’d learned. He went on a low-carb diet about eight years ago. “Sure enough, at middle age, it’s helped me stay healthy,” he says.
Most Americans Are Insulin Resistant
Unfortunately, many, including doctors, still do not understand the influence of insulin on health and disease. The late Dr. Joseph Kraft, former chairman of the department of clinical pathology and nuclear medicine at St. Joseph’s Hospital in Chicago, wrote the book “Diabetes Epidemic and You: Should Everyone Be Tested?”
In it, he presents data that suggests 80 percent of Americans are in fact insulin resistant, or have “diabetes in situ.” Based on data from 14,000 patients,2 Kraft developed a powerful predictive test for diabetes.3 He would have the patient drink 75 grams of glucose, and then measure their insulin response over time, at half-hour intervals for up to five hours.
He noticed five distinctive patterns suggesting that a vast majority of people were already diabetic, even though their fasting glucose was normal. Only 20 percent of patients had healthy post-prandial insulin sensitivity and low diabetes risk. According to Kraft, “Those with cardiovascular disease not identified with diabetes … are simply undiagnosed.”
One of the take-home messages here is that insulin resistance and hyperinsulinemia (a condition marked by excess insulin in your blood relative to your level of glucose) are two sides of the same coin, as they drive and promote each other. In other words, if you have hyperinsulinemia, you are essentially insulin resistant and on your way toward developing Type 2 diabetes.
High Insulin Is a Key Disease Promoter
Both insulin resistance and hyperinsulinemia promote fatty liver and high blood glucose, and both of those in turn promote atherosclerosis. High blood pressure is another side effect of insulin resistance that drives atherosclerosis by placing stress on your arteries.
The effects of insulin resistance are really at the heart of most if not all chronic degenerative diseases. Diabetes, heart disease, cancer and Alzheimer’s are just a few of the most obvious ones. The logical conclusion then would be that addressing insulin resistance is a foundational component of effective health care. Bikman says:
“When I teach this to my students … I put insulin resistance in the core. Around it, I have all these chronic diseases. It’s what I call the ‘wheel of misfortune.’ Really, the most common cancers, prostate and breast cancers, almost always … will heavily express — by six or seven times — the number of insulin receptors. So, insulin is promoting the growth of the tumor.
With dementia, the connection between insulin resistance and Alzheimer’s is so tight that people refer to it as Type 3 diabetes. With sarcopenia, we know that if a muscle becomes insulin-resistant, that actually diminishes insulin’s ability to promote the anabolic production of proteins within the muscle …
We have to have our medical practitioners start appreciating … the utility [of] measuring insulin, because our focus on measuring glucose misses the mark. As someone’s becoming insulin-resistant, their insulin is climbing, but it’s enough to keep their glucose in check.
And because we always look at glucose, we don’t catch the disease until they become so insulin-resistant that no amount of their own insulin is enough to keep the glucose in check. Now, the glucose starts to climb — 10 years later, perhaps — and that’s when we detect the problem. We’re looking at the wrong marker.”
How the Ketogenic Diet Improves Insulin Sensitivity
The question then becomes, how do we treat insulin resistance? As Bikman’s research reveals, the ketogenic diet is part and parcel of the “cure” for this condition.
“For me, the benefit of a low-carb ketogenic diet is that it addresses the endocrine aspect of metabolic health,” Bikman says. “For too long … the message has been completely focused on calorie number.
It is this idea that if you can simply put a person into caloric deficiency, they will lose weight — problem solved … But we know that has long-term consequences … There’s a lasting metabolic damage …
Nevertheless, the power of the low-carbohydrate diet is that it addresses the endocrine component. As important as calorie number is, and I can appreciate the laws of thermodynamics … we cannot ignore the relevance of hormones, especially insulin.”
As explained by Bikman, it’s important to realize that insulin is what dictates what your body does with the energy it has — the energy you consume and the energy you have stored. “Insulin has its strong, capable hands right on the steering wheel of what the body does with the energy that it has available,” he says.
Importantly, research shows your metabolic rate increases as insulin decreases. “To me, that’s the power of the low-carb diet. You’re controlling insulin, and that can start to address all of those chronic diseases,” Bikman says.
The Importance of Cycling High and Low Carbohydrate Intake
For all its benefits though, there are drawbacks to staying in chronic nutritional ketosis. Based on the evidence, I’m convinced one needs to pulse or cycle in and out of nutritional ketosis. Bikman, who is in general agreement with this idea, explains:
“As a scientist, I wish there were longer-term studies to be able to conclusively say you can’t do this long-term or you can. What I’m comfortable saying, with a little bit of speculation, is that … the avoidance of carbohydrates for a prolonged period will create this situation of a relative glucose intolerance.
Now, I’m not going to say that causes insulin resistance. Some people say low-carb [diet] causes physiological insulin resistance … To me, a low-carb diet can create a situation of carbohydrate intolerance. That is reflective of a general and very substantial shift in energy use.
Insulin is down — that means the body is in fat-burning mode. That is the absolute bioenergetic fuel. If insulin is low, you are fueled with fat. That can create a shift where the body becomes almost reluctant to fuel itself with carbohydrates.
That’s where you have instances of someone adopting a low-carbohydrate diet, and then they’ll eat a carbohydrate load and they’ll say, ‘Wow, my glucose levels; it’s like I’ve become diabetic.’ That’s not the same thing. They become glucose-intolerant.
If that’s something someone wants to avoid for whatever reason, then cyclical [keto] is probably the way to go. You kind of spike the glucose from time to time, maybe weekly, whatever would work best for the person … The idea [is] you have that frequent-enough exposure to carbohydrates so that you can maintain that tolerance to the carbohydrates …”
Insulin also suppresses the liver’s ability to produce glucose. It impairs gluconeogenesis. What this means is that if your insulin level is too low for too long, your glucose level can start to rise. While this is not universally true for everyone, it can occur, as it did for me. Cycling in and out of ketosis will help you avoid this paradoxical side effect as well. Bikman notes:
“I’ve heard enough people say that. I think it has to be taken seriously. Nevertheless, glucagon [hormone] starts to climb. Insulin’s main effect is to take glucose from the blood (or any fuel) and push it into the cells. Glucagon does the opposite. Glucagon wants to mobilize fuel from tissues and push it into the blood.
One of glucagon’s main actions is to promote the breakdown of stored glycogen to promote the production of glucose in the liver. In that instance, where insulin has gone too low then, theoretically, glucagon could go too high, and that could increase glucose too much … That’s kind of reflective, perhaps, of that intolerance I mentioned …
With regards to the context of low-carb [causing] glucose to climb over time, it could be due to the lack of insulin, and thus an absence of the inhibition of glucagon production from the pancreas. The pancreas is making too much glucagon. That could potentially be driving up glucose levels.”
The Connection Between Gut Bacteria and Liver Health
Bikman also summarizes how a high-fiber diet helps combat fatty liver disease, which it does by way of influencing your gut microbiome.
“While the human body doesn’t get any energetic benefit from the fiber, the bacteria do. The bacteria are able to use the fiber as fuel. One of the products of that is short-chain fatty acids, [such as] butyrate.
What’s interesting is that as the fiber is being digested by the bacteria to create butyrate, that short-chain fat can get absorbed into the body … [I]t goes right into the portal vein from the gut, right to the liver …
Short-chain fatty acids are so stimulatory with regards to mitochondrial biogenesis … that it actually can combat fatty liver disease. It’s kind of a fun little paradox of using a fat to fight the fat that’s stored in the liver, in the case of fatty liver disease. Nevertheless, that’s an odd little connection between gut bacteria and liver health.”
Butyric acid (butyrate, a short-chain fatty acid produced by bacteria in your gut) is really similar to the ketone hydroxybutyrate, produced by your liver during the conversion of fat into energy.
The primary difference between the two is that hydroxybutyrate isn’t as absorbable. Most of it is used locally by colonocytes (epithelial cells of your colon). In other words, hydroxybutyrate is used for fuel in your gut, while butyrate benefits your liver.
The Mechanistic Target of Rapamycin — A Driver of Ill Health
The mammalian target of rapamycin (mTOR), also known as the mechanistic target of rapamycin, is an incredibly important pathway, as it controls autophagy — your body’s natural clean-up process in which old, damaged cells are eliminated and replaced with new, healthy ones. As such, it also plays an important role in aging and cancer.
In short, to slow aging and reduce your risk of cancer, you want to inhibit mTOR, as this triggers autophagy. When mTOR is activated, autophagy is deactivated, which prevents the recycling of proteins. Alas, chronic suppression of mTOR is not ideal either. Bikman explains:
“What’s important with regards to mTOR … is that because it inhibits autophagy, it is thought to allow proteins and just organelles, parts of the cells, to get old due to things like oxidative damage. As those proteins get damaged, they get old, and then the cell, by extension, gets old.
As the cells get old, so too is the organ, and then the whole body … But … the body has been designed with far too clever a scheme to have something that shouldn’t be there; mTOR is so fundamental to life that you can’t just go in and just slam the breaks on it, because that is death. We have to grow. We have to allow a cell to grow, and tissue to grow.
This idea [is to] optimize or strategically focus on boosting mTOR and letting it come back down to keep the body young, to keep the cells cleaning themselves out through autophagy … Then you inhibit that and allow the body to grow with this cyclical spike of mTOR.
A lot of the focus … among vegetarians … is this idea that you’ve got to avoid animal protein because it spikes mTOR. That’s the wrong way of looking at it … What spikes mTOR the most and the longest? Insulin spikes mTOR far more than amino acids do.”
Insulin Activates mTOR to a Far Greater Degree Than Protein
In other words, sugar/carbohydrates are the No. 1 enemy when it comes to activating mTOR and driving the aging and disease processes. According to Bikman, a direct comparison in tissue shows insulin spikes mTOR three to four times higher than leucine, the amino acid that has the greatest impact on mTOR, raising it the most.
Importantly, while amino acids such as leucine, or protein in general, will spike mTOR for 45 to 90 minutes, after which mTOR dials back down, if you eat lots of starchy, sugary foods, you have chronically elevated insulin and hence chronically activated mTOR, and that’s what’s causing problems.
“If you look at the global breakfast trends, it’s going to be something starchy and sugary. Insulin will come up, depending on the person, [and stay elevated for] two to even four hours; mTOR is active that whole time. Then, right as the insulin is coming down, they have a mid-morning snack.
Of course, it’s another starch and it’s another sugar. Insulin comes up again and it’s up for hours. Of course, as insulin is up, so too is mTOR. That, I submit, is far more pathological — this chronic, every-waking-moment mTOR activation because of insulin, rather than these intermittent spikes of mTOR because of the ingestion of protein.”
The Benefits of Intermittent Fasting
Aside from a ketogenic diet, intermittent fasting — where you do not eat for 16 to 18 hours a day; 12 hours being the absolute minimum — is another effective way to regain your insulin sensitivity and control mTOR.
Basically, while you’re fasting, your insulin will dramatically drop, allowing your body to enter into autophagy and clean itself out. Then, when you refeed, your body deactivates autophagy and starts to rebuild itself.
Dr. Jason Fung, a nephrologist, recently published a case series paper4 on three diabetic patients — all of whom were on high doses of insulin — detailing how intermittent fasting can be used as a therapeutic alternative for Type 2 diabetes.
Of the three patients, two did alternating-day 24-hour fasts, while one fasted for 24 hours three times a week over a period of several months. On nonfasting days, they were allowed both lunch and dinner, but all meals were low in sugar and refined carbohydrates throughout. (The complete manual of the fasting regimen used is described in Fung’s book, “The Complete Guide to Fasting.”5)
Two of the patients were able to discontinue all of their diabetes medications while the third was able to discontinue three of his four drugs. All three also lost between 10 and 18 percent of their body weight. Incredibly, all were able to discontinue their insulin in just five to 18 days. Bikman comments:
“From the context of controlling insulin, there are studies on insulin-resistant people where they are on isocaloric diets, so the same amount of calories, but one is eating them frequently in smaller amounts and one is packing them in a smaller window …
Those on the time-restricted eating schedule … had greater drops in glucose and insulin. That, to me, is the beginning and end. As a guy who sees the relevance of insulin in any chronic disease … I just simply ask, what controls insulin?
Simply give your body a break from eating. Twelve hours should be what everyone does every night of the week, even if they’re eating three full meals. At least get that 12-hour break, for heaven’s sake.
As a professor, I see kids who live on cold cereal. They’re eating three bowls of cereal at midnight. [Then] they have the same three bowls of cereal at 7 or 8 a.m. I hear them, of course. They’re smug, ‘I can eat whatever I want.’ I say, ‘Let’s see how you’re doing in 10 years.’”
The reason you want to avoid eating for 16 to 18 hours is because you cannot effectively deplete the glycogen stores in your liver otherwise. As noted by Bikman, your liver will hold, on average, 100 grams of glycogen, and it takes anywhere between 24 and 48 hours to burn that up.
What this means is that if you’re eating a high-carb diet and want to get into ketosis, you’ll need to totally restrict carbohydrates or fast for at least 24 hours. Once you start running out of glycogen, your ketones will start to rise to take its place as a fuel for your body. Around 48 hours, you’re solidly in ketosis as the glycogen in your liver has been cleared.
On a side note, fasting will also release fat-bound toxins and facilitate detoxification. As noted by Bikman, “as insulin comes down, your urine production starts to increase,” as your kidneys start to flush out toxins.
Industrial Seed Oils — Another Culprit That Drives Disease
The devil’s in the details, of course, and the main problems are caused not only by refined carbohydrates in the Western processed food diet but also by processed seed oils, which Bikman describe as “surprisingly pathogenic.”
“We’ve just started a project in my lab. I’ve got a really sharp undergraduate who’s focusing on the main oxidized product of seed oils,” he says. “When you look at that main omega-6 and how it gets oxidized through this molecule called 4-hydroxynonenal (4-HNE), we’re looking at how it accumulates in muscle cells.
It is forcing these changes in the way the mitochondria are physically put together. Mitochondria love to be very dynamic. They’re long and stringy. They’ll separate often to small pieces then come back together. Not all have a very relevant physiological purpose with regards to cell growth and division.
Yet, in the case of 4-HNE accumulation, that process gets stopped. Now you’ve forced this sustained static state of the mitochondria, which is not healthy for them or the cell. I can’t say anything more about it yet just because we don’t have all the data yet, but it’s coming.”
Ketones — A Surrogate Marker for Insulin
While measuring insulin is really valuable, you need a doctor’s order to test it. Fortunately, there’s a good surrogate marker for insulin, namely your ketone level, because you cannot have high insulin if you have high ketones. In other words, ketones are an inverse indicator of what your insulin is. (One of the best ketone devices I know of is Keto-Mojo, as the strips are only $1 each.)
“That was my initial interest in ketones, because it provided that immediate marker of what insulin is, even in a way that glucose cannot. You can have normal glucose levels and have insulin be elevated. If you’re insulin-resistant, you just need more insulin to keep your glucose normal, so you can’t rely on glucose.
In a way, ketones then become more sensitive as a marker, a surrogate for insulin, than even glucose is. Over time, if someone’s had their insulin levels in control for a sufficient period, their liver is basically burning fat at such a high rate that it’s burning more fat than it needs, and so the body has this very kind of clever release or exhaust valve, which is the production of ketones,” Bikman says.
“We have to account for how energy is consumed, how it is used in the form of creating ATP or just body heat — even that’s relevant in ketosis — but then third, for lack of a better word, this energy wasting, because ketones provide this kind of exhaust valve where the body is burning fat so high that it has more than it needs, and it just starts moving it out of the body, in the breath and in the urine.
That needs to be considered, or at least acknowledged … Once again, insulin dictates what the body does with the energy that it has, including producing ketones and having them basically be wasted from the body.”
When and What to Eat When Exercising
Clearly, your diet is far more important than exercise when it comes to controlling your insulin and overall health. That said, I don’t think you can achieve optimal health unless you integrate exercise. The practical question is, “What and when should you eat when you exercise?” My conclusion is that protein is a necessary component of a post-workout meal, and that it’s best to exercise in a fasted state. Bikman agrees, saying:
“With regards to protein, it is without a doubt relevant to someone doing endurance or resistance exercise. You need to make sure you get enough protein. But it appears to be no magic window with that. Basically, you don’t have to get it 45 minutes or an hour after your workout. Essentially, within a 24-hour window, if you’ve eaten sufficient protein, then you’re okay.
Now, with regards to carbohydrate, there was a very neat study done with college students, where they had them exercise and then their next meal was a carbohydrate-rich meal in one group. In the other group, they fasted through that next meal … The group that ate the high-carb diet … did not have an improvement in insulin sensitivity.
By ending their exercise and then having the next meal be a high-carb meal, that undid the improvements in insulin sensitivity from the exercise itself. That has ramifications, because so often someone gets done exercising and they reward themselves with something like juice at some smoothie joint, or they indulge themselves.
They treat themselves with some carbohydrates thinking, ‘I spent it, so I need to eat it.’ What a shame. They are directly preventing some of the insulin-sensitizing benefit of the exercise, because of what they ate …
Like you, I prefer to exercise fasted … I don’t like having something in my gut when I’m trying to push my blood to my muscles … That blood has to come from the gut.
You basically are creating this little war, this hemodynamic war where during exercise and yet having eaten something, your body is thinking, ‘Wait a minute. I need to be sending blood into my guts to help move this food through the intestines and digest it. But now, my muscles are active, so I’ve got to push the blood to my muscles.’
You’re creating this split, forcing the body to prioritize where the blood wants to go. But if you leave the food in the gut, that’s going to start to develop some gastrointestinal discomfort.”
The Importance of Leucine Post-Exercise
One of the most important protein sources when you’re exercising is the amino acid leucine. Interestingly, and paradoxically, leucine actually activates autophagy, even though it also activates mTOR, which logically says would result in autophagy being inhibited. This paradox likely has to do with the fact that leucine is ketogenic, meaning it can turn into a ketone, and ketones activate autophagy.
Leucine is so effective for muscle building, research cited by Bikman shows just 5 grams of leucine is enough to maximize muscle protein synthesis in people on an otherwise protein-deficient diet. When it comes to leucine supplements, hydroxymethylbutyrate (HBM) is a breakdown product of leucine that you can take. However, it’s more expensive, and according to Bikman’s reading of the literature, it has no added benefits over leucine itself.
“Just leave it on the store shelf. Don’t spend that higher amount. It is more money than leucine. Just stick with the leucine,” he says. “Leucine is one of the so-called ketogenic amino acids. It can, in fact, take that carbon skeleton of the leucine and turn it into a ketone.
Some amino acids are referred to as glycolytic, where they can come in and basically turn into alanine. They can readily turn into glucose as needed. Leucine is one of the ketogenic ones, [which] can turn into ketones, beta-hydroxybutyrate in particular. I’d say that if there’s any benefit to HMB, you’re going to get that anyway, because the leucine is going to become HMB.”
Collagen Does Not Count as a Protein Source
As a general rule, to optimize mTOR, you’ll want to restrict your protein intake to about 0.5 grams of protein per pound of lean body mass (not total body weight), or 1 gram of protein per kilo of lean mass. The elderly may need up to 25 percent more.
When calculating your protein intake, keep in mind you do not need to include collagen in your calculations, as it does not have the full complement of amino acids to be considered a complete protein. Collagen — provided it’s a high-quality, organic grass fed source — is important for the health of your connective tissue, and will help prevent injuries. So, while you don’t want to have excess protein, you almost get a free pass with collagen.
“Collagen [contains] a different bunch of amino acids,” Bikman explains. “One in particular is hydroxyproline, one of the main building blocks for collagen in the body. I’ve had people kind of challenge that idea and say, ‘Well, but when you eat these proteins, even in the form of collagen, it will degrade into the amino acids. The body will just kind of choose whatever amino acids it wants to put back together to make whatever proteins it wants.’
That’s generally true. There is a very neat rat study. We just have to assume the same thing holds in humans. I think it’s a safe assumption here. They had the rats eat a radio-labelled hydroxyproline, so they could basically follow that hydroxyproline around.
Sure enough, it went to the skin and to the connective tissue. They could detect where it was enriched. It was all this connective tissue-rich or collagen-rich tissue in the body. I am an advocate of collagen. The evidence supports it. It’s especially relevant to someone who adheres to a low-carb diet. Vitamin C is called C for collagen.
What’s important is that if you’re eating less vitamin C, it’s comforting to know that you’re fulfilling that need essentially by getting not only the collagen itself from the meat that you’re eating, that connective tissue and that hydroxyproline and the other amino acids relevant to collagen, but also carnitine, which is relevant to the function and production of collagen within the body.
Even a low-carb person, who’s avoiding vitamin C, can rest assured their joints and connective tissues are going to be OK, because they’re actually directly eating what they need rather than having the body make what they need with the help of vitamin C.”
from http://articles.mercola.com/sites/articles/archive/2019/04/14/ketogenic-physiological-effects-on-human-body.aspx
source http://niapurenaturecom.weebly.com/blog/the-ketogenic-diet-and-its-physiological-effects-on-the-human-body
1 note
·
View note
Text
The Ketogenic Diet and Its Physiological Effects on the Human Body
youtube
In this interview, Benjamin Bikman, Ph.D., an obesity and diabetes scientist and associate professor of physiology and developmental biology at Brigham Young University (BYU) in Utah,1 reveals how the ketogenic diet affects your physiology and supports optimal health.
“My main interest early on was looking at how the body adapts to obesity,” he says. “That was my master’s thesis. My master’s degree was exercise science here at BYU … I ended up pursuing a Ph.D. in bioenergetics at East Carolina University, under this wonderful scientist named Lynis Dohm, Ph.D.
His focus had been looking at how lipids cause insulin resistance. That was an interest of mine, because I thought this was starting to explain why and how the body becomes insulin-resistant in the midst of obesity … Insulin resistance is that connection.
During my Ph.D., we were looking at inflammation in people who were losing weight following gastric bypass procedures and how improved inflammation is likely part of the improvements in insulin sensitivity that people see post-bypass.
I followed that up with a post-doctoral fellowship at … the Duke National University of Singapore. They had this focus on cardio metabolic disorders. I … looked at inflammation as a particular mediator there … Then in 2011, my alma mater, BYU, came knocking. They wanted to do more diabetes research, and I fit the requirements … That got me, essentially, to where I am now …
If I really am getting this conviction, based on my own research, that insulin is key to not only diabetes but to almost every chronic disease, what is the best way to control insulin? That was when I insisted on only looking at published human clinical data — not rodents, not cells, not epidemiology, just clinical data.
The low-carb diet was just this very effective way to do that. That then got me interested in asking questions about ketones, which is what my lab is doing … how ketones are regulated by insulin.”
Bikman’s conviction that insulin is a key to health and disease prevention, and that controlling carbohydrate intake is the most effective way to control insulin, led him to start practicing what he’d learned. He went on a low-carb diet about eight years ago. “Sure enough, at middle age, it’s helped me stay healthy,” he says.
Most Americans Are Insulin Resistant
Unfortunately, many, including doctors, still do not understand the influence of insulin on health and disease. The late Dr. Joseph Kraft, former chairman of the department of clinical pathology and nuclear medicine at St. Joseph’s Hospital in Chicago, wrote the book “Diabetes Epidemic and You: Should Everyone Be Tested?”
In it, he presents data that suggests 80 percent of Americans are in fact insulin resistant, or have “diabetes in situ.” Based on data from 14,000 patients,2 Kraft developed a powerful predictive test for diabetes.3 He would have the patient drink 75 grams of glucose, and then measure their insulin response over time, at half-hour intervals for up to five hours.
He noticed five distinctive patterns suggesting that a vast majority of people were already diabetic, even though their fasting glucose was normal. Only 20 percent of patients had healthy post-prandial insulin sensitivity and low diabetes risk. According to Kraft, “Those with cardiovascular disease not identified with diabetes … are simply undiagnosed.”
One of the take-home messages here is that insulin resistance and hyperinsulinemia (a condition marked by excess insulin in your blood relative to your level of glucose) are two sides of the same coin, as they drive and promote each other. In other words, if you have hyperinsulinemia, you are essentially insulin resistant and on your way toward developing Type 2 diabetes.
High Insulin Is a Key Disease Promoter
Both insulin resistance and hyperinsulinemia promote fatty liver and high blood glucose, and both of those in turn promote atherosclerosis. High blood pressure is another side effect of insulin resistance that drives atherosclerosis by placing stress on your arteries.
The effects of insulin resistance are really at the heart of most if not all chronic degenerative diseases. Diabetes, heart disease, cancer and Alzheimer’s are just a few of the most obvious ones. The logical conclusion then would be that addressing insulin resistance is a foundational component of effective health care. Bikman says:
“When I teach this to my students … I put insulin resistance in the core. Around it, I have all these chronic diseases. It’s what I call the ‘wheel of misfortune.’ Really, the most common cancers, prostate and breast cancers, almost always … will heavily express — by six or seven times — the number of insulin receptors. So, insulin is promoting the growth of the tumor.
With dementia, the connection between insulin resistance and Alzheimer’s is so tight that people refer to it as Type 3 diabetes. With sarcopenia, we know that if a muscle becomes insulin-resistant, that actually diminishes insulin’s ability to promote the anabolic production of proteins within the muscle …
We have to have our medical practitioners start appreciating … the utility [of] measuring insulin, because our focus on measuring glucose misses the mark. As someone’s becoming insulin-resistant, their insulin is climbing, but it’s enough to keep their glucose in check.
And because we always look at glucose, we don’t catch the disease until they become so insulin-resistant that no amount of their own insulin is enough to keep the glucose in check. Now, the glucose starts to climb — 10 years later, perhaps — and that’s when we detect the problem. We’re looking at the wrong marker.”
How the Ketogenic Diet Improves Insulin Sensitivity
The question then becomes, how do we treat insulin resistance? As Bikman’s research reveals, the ketogenic diet is part and parcel of the “cure” for this condition.
“For me, the benefit of a low-carb ketogenic diet is that it addresses the endocrine aspect of metabolic health,” Bikman says. “For too long … the message has been completely focused on calorie number.
It is this idea that if you can simply put a person into caloric deficiency, they will lose weight — problem solved … But we know that has long-term consequences … There’s a lasting metabolic damage …
Nevertheless, the power of the low-carbohydrate diet is that it addresses the endocrine component. As important as calorie number is, and I can appreciate the laws of thermodynamics … we cannot ignore the relevance of hormones, especially insulin.”
As explained by Bikman, it’s important to realize that insulin is what dictates what your body does with the energy it has — the energy you consume and the energy you have stored. “Insulin has its strong, capable hands right on the steering wheel of what the body does with the energy that it has available,” he says.
Importantly, research shows your metabolic rate increases as insulin decreases. “To me, that’s the power of the low-carb diet. You’re controlling insulin, and that can start to address all of those chronic diseases,” Bikman says.
The Importance of Cycling High and Low Carbohydrate Intake
For all its benefits though, there are drawbacks to staying in chronic nutritional ketosis. Based on the evidence, I’m convinced one needs to pulse or cycle in and out of nutritional ketosis. Bikman, who is in general agreement with this idea, explains:
“As a scientist, I wish there were longer-term studies to be able to conclusively say you can’t do this long-term or you can. What I’m comfortable saying, with a little bit of speculation, is that … the avoidance of carbohydrates for a prolonged period will create this situation of a relative glucose intolerance.
Now, I’m not going to say that causes insulin resistance. Some people say low-carb [diet] causes physiological insulin resistance … To me, a low-carb diet can create a situation of carbohydrate intolerance. That is reflective of a general and very substantial shift in energy use.
Insulin is down — that means the body is in fat-burning mode. That is the absolute bioenergetic fuel. If insulin is low, you are fueled with fat. That can create a shift where the body becomes almost reluctant to fuel itself with carbohydrates.
That’s where you have instances of someone adopting a low-carbohydrate diet, and then they’ll eat a carbohydrate load and they’ll say, ‘Wow, my glucose levels; it’s like I’ve become diabetic.’ That’s not the same thing. They become glucose-intolerant.
If that’s something someone wants to avoid for whatever reason, then cyclical [keto] is probably the way to go. You kind of spike the glucose from time to time, maybe weekly, whatever would work best for the person … The idea [is] you have that frequent-enough exposure to carbohydrates so that you can maintain that tolerance to the carbohydrates …”
Insulin also suppresses the liver’s ability to produce glucose. It impairs gluconeogenesis. What this means is that if your insulin level is too low for too long, your glucose level can start to rise. While this is not universally true for everyone, it can occur, as it did for me. Cycling in and out of ketosis will help you avoid this paradoxical side effect as well. Bikman notes:
“I’ve heard enough people say that. I think it has to be taken seriously. Nevertheless, glucagon [hormone] starts to climb. Insulin’s main effect is to take glucose from the blood (or any fuel) and push it into the cells. Glucagon does the opposite. Glucagon wants to mobilize fuel from tissues and push it into the blood.
One of glucagon’s main actions is to promote the breakdown of stored glycogen to promote the production of glucose in the liver. In that instance, where insulin has gone too low then, theoretically, glucagon could go too high, and that could increase glucose too much … That’s kind of reflective, perhaps, of that intolerance I mentioned …
With regards to the context of low-carb [causing] glucose to climb over time, it could be due to the lack of insulin, and thus an absence of the inhibition of glucagon production from the pancreas. The pancreas is making too much glucagon. That could potentially be driving up glucose levels.”
The Connection Between Gut Bacteria and Liver Health
Bikman also summarizes how a high-fiber diet helps combat fatty liver disease, which it does by way of influencing your gut microbiome.
“While the human body doesn’t get any energetic benefit from the fiber, the bacteria do. The bacteria are able to use the fiber as fuel. One of the products of that is short-chain fatty acids, [such as] butyrate.
What’s interesting is that as the fiber is being digested by the bacteria to create butyrate, that short-chain fat can get absorbed into the body … [I]t goes right into the portal vein from the gut, right to the liver …
Short-chain fatty acids are so stimulatory with regards to mitochondrial biogenesis … that it actually can combat fatty liver disease. It’s kind of a fun little paradox of using a fat to fight the fat that’s stored in the liver, in the case of fatty liver disease. Nevertheless, that’s an odd little connection between gut bacteria and liver health.”
Butyric acid (butyrate, a short-chain fatty acid produced by bacteria in your gut) is really similar to the ketone hydroxybutyrate, produced by your liver during the conversion of fat into energy.
The primary difference between the two is that hydroxybutyrate isn’t as absorbable. Most of it is used locally by colonocytes (epithelial cells of your colon). In other words, hydroxybutyrate is used for fuel in your gut, while butyrate benefits your liver.
The Mechanistic Target of Rapamycin — A Driver of Ill Health
The mammalian target of rapamycin (mTOR), also known as the mechanistic target of rapamycin, is an incredibly important pathway, as it controls autophagy — your body’s natural clean-up process in which old, damaged cells are eliminated and replaced with new, healthy ones. As such, it also plays an important role in aging and cancer.
In short, to slow aging and reduce your risk of cancer, you want to inhibit mTOR, as this triggers autophagy. When mTOR is activated, autophagy is deactivated, which prevents the recycling of proteins. Alas, chronic suppression of mTOR is not ideal either. Bikman explains:
“What’s important with regards to mTOR … is that because it inhibits autophagy, it is thought to allow proteins and just organelles, parts of the cells, to get old due to things like oxidative damage. As those proteins get damaged, they get old, and then the cell, by extension, gets old.
As the cells get old, so too is the organ, and then the whole body … But … the body has been designed with far too clever a scheme to have something that shouldn’t be there; mTOR is so fundamental to life that you can’t just go in and just slam the breaks on it, because that is death. We have to grow. We have to allow a cell to grow, and tissue to grow.
This idea [is to] optimize or strategically focus on boosting mTOR and letting it come back down to keep the body young, to keep the cells cleaning themselves out through autophagy … Then you inhibit that and allow the body to grow with this cyclical spike of mTOR.
A lot of the focus … among vegetarians … is this idea that you’ve got to avoid animal protein because it spikes mTOR. That’s the wrong way of looking at it … What spikes mTOR the most and the longest? Insulin spikes mTOR far more than amino acids do.”
Insulin Activates mTOR to a Far Greater Degree Than Protein
In other words, sugar/carbohydrates are the No. 1 enemy when it comes to activating mTOR and driving the aging and disease processes. According to Bikman, a direct comparison in tissue shows insulin spikes mTOR three to four times higher than leucine, the amino acid that has the greatest impact on mTOR, raising it the most.
Importantly, while amino acids such as leucine, or protein in general, will spike mTOR for 45 to 90 minutes, after which mTOR dials back down, if you eat lots of starchy, sugary foods, you have chronically elevated insulin and hence chronically activated mTOR, and that’s what’s causing problems.
“If you look at the global breakfast trends, it’s going to be something starchy and sugary. Insulin will come up, depending on the person, [and stay elevated for] two to even four hours; mTOR is active that whole time. Then, right as the insulin is coming down, they have a mid-morning snack.
Of course, it’s another starch and it’s another sugar. Insulin comes up again and it’s up for hours. Of course, as insulin is up, so too is mTOR. That, I submit, is far more pathological — this chronic, every-waking-moment mTOR activation because of insulin, rather than these intermittent spikes of mTOR because of the ingestion of protein.”
The Benefits of Intermittent Fasting
Aside from a ketogenic diet, intermittent fasting — where you do not eat for 16 to 18 hours a day; 12 hours being the absolute minimum — is another effective way to regain your insulin sensitivity and control mTOR.
Basically, while you’re fasting, your insulin will dramatically drop, allowing your body to enter into autophagy and clean itself out. Then, when you refeed, your body deactivates autophagy and starts to rebuild itself.
Dr. Jason Fung, a nephrologist, recently published a case series paper4 on three diabetic patients — all of whom were on high doses of insulin — detailing how intermittent fasting can be used as a therapeutic alternative for Type 2 diabetes.
Of the three patients, two did alternating-day 24-hour fasts, while one fasted for 24 hours three times a week over a period of several months. On nonfasting days, they were allowed both lunch and dinner, but all meals were low in sugar and refined carbohydrates throughout. (The complete manual of the fasting regimen used is described in Fung’s book, “The Complete Guide to Fasting.”5)
Two of the patients were able to discontinue all of their diabetes medications while the third was able to discontinue three of his four drugs. All three also lost between 10 and 18 percent of their body weight. Incredibly, all were able to discontinue their insulin in just five to 18 days. Bikman comments:
“From the context of controlling insulin, there are studies on insulin-resistant people where they are on isocaloric diets, so the same amount of calories, but one is eating them frequently in smaller amounts and one is packing them in a smaller window …
Those on the time-restricted eating schedule … had greater drops in glucose and insulin. That, to me, is the beginning and end. As a guy who sees the relevance of insulin in any chronic disease … I just simply ask, what controls insulin?
Simply give your body a break from eating. Twelve hours should be what everyone does every night of the week, even if they’re eating three full meals. At least get that 12-hour break, for heaven’s sake.
As a professor, I see kids who live on cold cereal. They’re eating three bowls of cereal at midnight. [Then] they have the same three bowls of cereal at 7 or 8 a.m. I hear them, of course. They’re smug, ‘I can eat whatever I want.’ I say, ‘Let’s see how you’re doing in 10 years.’”
The reason you want to avoid eating for 16 to 18 hours is because you cannot effectively deplete the glycogen stores in your liver otherwise. As noted by Bikman, your liver will hold, on average, 100 grams of glycogen, and it takes anywhere between 24 and 48 hours to burn that up.
What this means is that if you’re eating a high-carb diet and want to get into ketosis, you’ll need to totally restrict carbohydrates or fast for at least 24 hours. Once you start running out of glycogen, your ketones will start to rise to take its place as a fuel for your body. Around 48 hours, you’re solidly in ketosis as the glycogen in your liver has been cleared.
On a side note, fasting will also release fat-bound toxins and facilitate detoxification. As noted by Bikman, “as insulin comes down, your urine production starts to increase,” as your kidneys start to flush out toxins.
Industrial Seed Oils — Another Culprit That Drives Disease
The devil’s in the details, of course, and the main problems are caused not only by refined carbohydrates in the Western processed food diet but also by processed seed oils, which Bikman describe as “surprisingly pathogenic.”
“We’ve just started a project in my lab. I’ve got a really sharp undergraduate who’s focusing on the main oxidized product of seed oils,” he says. “When you look at that main omega-6 and how it gets oxidized through this molecule called 4-hydroxynonenal (4-HNE), we’re looking at how it accumulates in muscle cells.
It is forcing these changes in the way the mitochondria are physically put together. Mitochondria love to be very dynamic. They’re long and stringy. They’ll separate often to small pieces then come back together. Not all have a very relevant physiological purpose with regards to cell growth and division.
Yet, in the case of 4-HNE accumulation, that process gets stopped. Now you’ve forced this sustained static state of the mitochondria, which is not healthy for them or the cell. I can’t say anything more about it yet just because we don’t have all the data yet, but it’s coming.”
Ketones — A Surrogate Marker for Insulin
While measuring insulin is really valuable, you need a doctor’s order to test it. Fortunately, there’s a good surrogate marker for insulin, namely your ketone level, because you cannot have high insulin if you have high ketones. In other words, ketones are an inverse indicator of what your insulin is. (One of the best ketone devices I know of is Keto-Mojo, as the strips are only $1 each.)
“That was my initial interest in ketones, because it provided that immediate marker of what insulin is, even in a way that glucose cannot. You can have normal glucose levels and have insulin be elevated. If you’re insulin-resistant, you just need more insulin to keep your glucose normal, so you can’t rely on glucose.
In a way, ketones then become more sensitive as a marker, a surrogate for insulin, than even glucose is. Over time, if someone’s had their insulin levels in control for a sufficient period, their liver is basically burning fat at such a high rate that it’s burning more fat than it needs, and so the body has this very kind of clever release or exhaust valve, which is the production of ketones,” Bikman says.
“We have to account for how energy is consumed, how it is used in the form of creating ATP or just body heat — even that’s relevant in ketosis — but then third, for lack of a better word, this energy wasting, because ketones provide this kind of exhaust valve where the body is burning fat so high that it has more than it needs, and it just starts moving it out of the body, in the breath and in the urine.
That needs to be considered, or at least acknowledged … Once again, insulin dictates what the body does with the energy that it has, including producing ketones and having them basically be wasted from the body.”
When and What to Eat When Exercising
Clearly, your diet is far more important than exercise when it comes to controlling your insulin and overall health. That said, I don’t think you can achieve optimal health unless you integrate exercise. The practical question is, “What and when should you eat when you exercise?” My conclusion is that protein is a necessary component of a post-workout meal, and that it’s best to exercise in a fasted state. Bikman agrees, saying:
“With regards to protein, it is without a doubt relevant to someone doing endurance or resistance exercise. You need to make sure you get enough protein. But it appears to be no magic window with that. Basically, you don’t have to get it 45 minutes or an hour after your workout. Essentially, within a 24-hour window, if you’ve eaten sufficient protein, then you’re okay.
Now, with regards to carbohydrate, there was a very neat study done with college students, where they had them exercise and then their next meal was a carbohydrate-rich meal in one group. In the other group, they fasted through that next meal … The group that ate the high-carb diet … did not have an improvement in insulin sensitivity.
By ending their exercise and then having the next meal be a high-carb meal, that undid the improvements in insulin sensitivity from the exercise itself. That has ramifications, because so often someone gets done exercising and they reward themselves with something like juice at some smoothie joint, or they indulge themselves.
They treat themselves with some carbohydrates thinking, ‘I spent it, so I need to eat it.’ What a shame. They are directly preventing some of the insulin-sensitizing benefit of the exercise, because of what they ate …
Like you, I prefer to exercise fasted … I don’t like having something in my gut when I’m trying to push my blood to my muscles … That blood has to come from the gut.
You basically are creating this little war, this hemodynamic war where during exercise and yet having eaten something, your body is thinking, ‘Wait a minute. I need to be sending blood into my guts to help move this food through the intestines and digest it. But now, my muscles are active, so I’ve got to push the blood to my muscles.’
You’re creating this split, forcing the body to prioritize where the blood wants to go. But if you leave the food in the gut, that’s going to start to develop some gastrointestinal discomfort.”
The Importance of Leucine Post-Exercise
One of the most important protein sources when you’re exercising is the amino acid leucine. Interestingly, and paradoxically, leucine actually activates autophagy, even though it also activates mTOR, which logically says would result in autophagy being inhibited. This paradox likely has to do with the fact that leucine is ketogenic, meaning it can turn into a ketone, and ketones activate autophagy.
Leucine is so effective for muscle building, research cited by Bikman shows just 5 grams of leucine is enough to maximize muscle protein synthesis in people on an otherwise protein-deficient diet. When it comes to leucine supplements, hydroxymethylbutyrate (HBM) is a breakdown product of leucine that you can take. However, it’s more expensive, and according to Bikman’s reading of the literature, it has no added benefits over leucine itself.
“Just leave it on the store shelf. Don’t spend that higher amount. It is more money than leucine. Just stick with the leucine,” he says. “Leucine is one of the so-called ketogenic amino acids. It can, in fact, take that carbon skeleton of the leucine and turn it into a ketone.
Some amino acids are referred to as glycolytic, where they can come in and basically turn into alanine. They can readily turn into glucose as needed. Leucine is one of the ketogenic ones, [which] can turn into ketones, beta-hydroxybutyrate in particular. I’d say that if there’s any benefit to HMB, you’re going to get that anyway, because the leucine is going to become HMB.”
Collagen Does Not Count as a Protein Source
As a general rule, to optimize mTOR, you’ll want to restrict your protein intake to about 0.5 grams of protein per pound of lean body mass (not total body weight), or 1 gram of protein per kilo of lean mass. The elderly may need up to 25 percent more.
When calculating your protein intake, keep in mind you do not need to include collagen in your calculations, as it does not have the full complement of amino acids to be considered a complete protein. Collagen — provided it’s a high-quality, organic grass fed source — is important for the health of your connective tissue, and will help prevent injuries. So, while you don’t want to have excess protein, you almost get a free pass with collagen.
“Collagen [contains] a different bunch of amino acids,” Bikman explains. “One in particular is hydroxyproline, one of the main building blocks for collagen in the body. I’ve had people kind of challenge that idea and say, ‘Well, but when you eat these proteins, even in the form of collagen, it will degrade into the amino acids. The body will just kind of choose whatever amino acids it wants to put back together to make whatever proteins it wants.’
That’s generally true. There is a very neat rat study. We just have to assume the same thing holds in humans. I think it’s a safe assumption here. They had the rats eat a radio-labelled hydroxyproline, so they could basically follow that hydroxyproline around.
Sure enough, it went to the skin and to the connective tissue. They could detect where it was enriched. It was all this connective tissue-rich or collagen-rich tissue in the body. I am an advocate of collagen. The evidence supports it. It’s especially relevant to someone who adheres to a low-carb diet. Vitamin C is called C for collagen.
What’s important is that if you’re eating less vitamin C, it’s comforting to know that you’re fulfilling that need essentially by getting not only the collagen itself from the meat that you’re eating, that connective tissue and that hydroxyproline and the other amino acids relevant to collagen, but also carnitine, which is relevant to the function and production of collagen within the body.
Even a low-carb person, who’s avoiding vitamin C, can rest assured their joints and connective tissues are going to be OK, because they’re actually directly eating what they need rather than having the body make what they need with the help of vitamin C.”
from Articles http://articles.mercola.com/sites/articles/archive/2019/04/14/ketogenic-physiological-effects-on-human-body.aspx source https://niapurenaturecom.tumblr.com/post/184171638036
1 note
·
View note
Text
My Whole 30 Experience
Like many others, I have struggled with weight and the concept of “healthy eating”. While I do love sweets and “cheat meals”, I have always truly enjoyed fruits, vegetables and home cooked meals. Growing up, we ate pretty healthy but desserts were a fairly regular thing which probably doesn’t help me as an adult. While dabbling in various sports and activities, I did not find the true sport of “fitness” until I tried Crossfit. Now, everyone has their perceptions and opinions of Crossfit (many of which I have heard), however I have never found an activity that truly challenges me both mentally and physically in a way that I enjoy so much. The community, camaraderie, successes and failures, are all part of the process. I digress but, the moral of the this rant is, I have always strived to be healthy and active but have not always been the most successful in feeling the best I could be. My significant other has heard a lot about the “Whole 30” and bought me the book which I was only mildly offended by (kidding). I was super interested in it as I have had a lot of success with lower carb and macro (protein/fat/carb) lifestyles and thought this would be a great adventure. I didn’t have a ton of time to read the book before starting as I had a goal. We were heading to Europe at the end of February and I wanted to be done the whole 30 before then. The day after he left, I was going to embark on this mission. Several friends\family members were surprised and some even had their doubts about it “being too hard”. While I am always up for a challenge, I did have my concerns about this lifestyle as it seemed a bit extreme at first with many steep learning curves along the way. I haven’t even really explained what the Whole 30 ® is. This program has been tried and tested my millions of people since its inception in about 2009. Now, I am not in any way shape or form endorsing a diet or lifestyle change that does not appeal to you or that has not been approved by your md, but this one seemed pretty legit. The premise is to eat all whole foods for 30 days- seems simple enough. Many people who chronic health issues including IBS, allergies, skin issues, arthritis and a whole range of emotional concerns have found that when they cut out many of the irritants (e.g gluten, sugar, dairy, legumes etc), they have a resolution or at least improvement in their symptoms. While I do not suffer any chronic health conditions, I do have some MSK pain along with some mood swings (probably from hormones or sugar) and thought I would give this lifestyle adjustment a chance. Since this was such a challenging, amazing experience, I thought I would document it and share. Of course, I am well aware that everyone will have their own opinion and input (heck, that is if anyone reads this!) but I figured it would be nice to share the tips and tricks that I have learned in this roller-coaster month. Week 1 (Jan 21-27): Since I didn’t have a ton of time to read the book from cover to cover like I would have wanted to prep, I did my best to read the “what not to eat list” before prepping for my first few days at work. The Whole 30 ® book is super helpful with a step by step guide on basically what it is that I would be embarking on, tips, meal plans, recipes, Q&A and so much more. The website is even more helpful! Once I started taking a look at what the website had, I had a lot more confidence in the process. They had tons of FAQs regarding lots of different foods and help with various topics such as going out to eat, substitutes for basic stuff etc. In terms of meal prepping, this is one of my fave things to do to prepare for the work week so I didn’t see this as much of a challenge. While I won’t go into detail about each day or anything, I will mention each a few successes as well as a few struggles for each week along with some suggestions or learning points that I found helpful. Successes: meal prepping and getting right into it, decrease appetite at times while maintaining the sense of feeling full longer. Having meals prepped is key. Improved energy around day 7
Struggles: cravings- the sugar detox on about day 5 was not nice. Super foggy, headache, lethargic etc. new bowel habits . That sulphites are literally in everything (vinegars, nuts, dried fruit etc.).
Suggestions: While dried fruit are yummy and good for you in small amounts, make sure you truly portion it out. They are pretty high in calories as well as sugar and shouldn’t really be used a substitue for other unhealthy choices. I usually paired my fruit with nuts as a snack when at work or if I didn’t have time have a proper meal.
-make your house or a cupboard of your stuff in your kitchen The Whole 30® friendly. This is especially important if you live with others who may not be embarking on the same mission you are
-PLAN AHEAD. I had a few get togethers planned for the first week, which I was excited about, but also nervous about. I knew I would be bringing my own food and wasn’t sure how that was going to be perceived. Most of my friends/coworkers were pretty accepting and positive about this challenge which made bringing my own snacks and food a lot easier.
Week 2 (Jan 28-Feb 3): Successes: drinking only one coffee a day (since sugar and all milks are off limits) I made bulletproof coffee which was a life saver. If you haven’t heard of this, please google it. It is basically coffee made with butter. Since on the Whole 30 ®, you cannot have butter, I substiitued the butter with ghee and made sure to blend it using my magic bullet. It made “black” coffee bearable and even tasty. The ghee cut the bitterness and made the coffee super creamy and yummy. Definitely give this one a try!
Struggles: The 2-4 pm slump on a day shift (well and sometimes days that I was off as well). I am not sure what exactly the cause was as sometimes it was before lunch, others it was after but this is the time of the day where I felt utterly exhausted most of the time. Not to say that I didn’t feel this way prior to the whole 30 but I didn’t always keep track. -I had signed myself up for a study to measure brown adipost tissue and part of the study was taking place during this second week of the Whole 30 ® . The study included a lot of data including blood pressure, height, weight etc. One of the more interesting parts was a dexa scan. This is basically a large machine that detects fat and figures out percentages of fat for each part of your body. I had a very hard time with this. I found the results super disheartening and depressing to see your body fat percentages. I mean there is no where to go but up I suppose so this was a great learning point and helped to turn my perspective around. -This is also the time of the Whole 30 ® where you might feel more bloated and such (as explained in the book) and I truly did. I also accidently saw my weight during the study and not seeing a drastic difference made me pretty upset. Then I remembered this was only the second week and things don’t happen overnight.
Suggestions: while The Whole 30 ® does not condone snacking, I personal have a hard time with this when I am working a 12 hour shift. Instead of not snacking, I made a conscious effort to snack more purposefully. Instead of just grabbing a bar (Lara coconut cream bars were my friend), I would think about whether or not I was hungry for salad or veggies. If I was, then I would have that (which I almost always had on hand) and if I wasn’t, then I wasn’t actually hungry. While this doesn’t totally support The Whole 30 ®, I found for the most part it worked and if I were to do this again and continue with it, I would make sure to have healthy choices and make sure I was eating because I was truly hungry and not just because I was bored/tired/stressed/sad/insert your own reason for unnecessary eating here. The reasoning around the not snacking is to not only change what we put in our mouths, but also the why we eat. If you are going to continue with the same late night snacking or stress eating that you were doing before (only with healthier options) than you haven’t really learned how to deal with the issue and are just making a substitute (yes a healthier one but still maybe not t he best choice).
Week 3 (Feb 4-Feb 10): Success: feeling a bit slimmer in some of my every day clothes. Also feeling a bit stronger at the gym, improved skin (which is a plus). I started seeing an osteo around week 3 and my knee pain was significantly improved with the manipulation s well as (hopefully) the anti-inflammatory properties of the clean eating.
Struggles: Emotions – while at first I thought I was way less moody than before, I did have a few days here and there where my emotions seemed to get the best of me. I can’t say that this was all because of eating -this was the first time I really had cravings for the food around me. Normally at work, there are tons of snacks and treats and for the first two weeks, this didn’t bother me. For some reason, in the middle of the week at my emerg job, I wanted the sweet treats so bad. I typically crave sweet way more than salty and love almost any sweet in front of me. Thankfully, I had a lunch packed full of Whole 30 ® approved food and just ignored the temptation. It didn’t last long, especially thinking about how far I had come.
Suggestions: eating out can be tricky, Make sure that if you are going to eat out during The Whole 30 ®, that you do your research before hand. Check the menu ahead of time to see if there are some options that you can enjoy. At first, I felt guilty being “picky” about my choices but in the end, it was never really a big deal and I just made sure to tip accordingly. You can’t really go wrong with a protein and salad (with lemon and olive oil on the side) which most restaurants have. There are certain oils that you should stay away from on The Whole 30 ® and others that you can have once in a while if eating out. I tried not use the word “allergy” to avoid certain food groups because I feel as though it is taking away from those who actually have allergies. On one occasion though, there was a bit of a mix up and I ended up having cheese on my salad which I kindly explained I could not have due to an intolerance (which isn’t necessarily a lie, just not a proven fact yet). -variety is important. I was trying to play it safe and make sure all my meals were Whole 30 ® approved which meant that I would eat the same things. I LOVE keto slaw (cabbage with ground beef and hot sauce basically) but did get really bored of the cabbage slaw I would sautee and make with many of my proteins. -While variety is key, keep it consistent. I tried to make sure I made one new recipe each which without stressing too much about it. Knowing what is Whole 30 ® approved and sticking to it helps when life gets busy. I am not saying you need to eat the same things every day to stay consistent, but remembering the basics and keeping things simple can go a long way. I found that there were a lot of great recipes in the book, however most of them weren’t overly appealing to me.
Week 4 (Feb 11- Feb 18): Success: Sleeping HAD improved significantly over the past few weeks however the last couple days of the Whole 30 ® seemed to not be my best sleeping days. I did flip flop from days to nights a few times which didn’t help and other factors including stress probably also played a role. I will consider the improved sleep a success seeing as my sleep drastically improved more than it deteriorated. (for anyone that knows me well, knows that while I love sleep, I have struggled with eating in the middle of the night and not being able to sleep through the night so improved sleep is a major win) -clearer skin, once again. I had never really had bad skin growing up until I was about 25 and became a lot more prone to hormonal acne. I have tried lots of basic run of the mill creams and plans but the Whole 30 ® really seemed to clear it up. A few of my coworkers at work and family members even noticed which is always nice and good pick me up when you might not be feeling your best. -Being at the finish line! I was getting more and more proud of myself and this small accomplishment with each passing day. I had a calendary that I used for meal prepping as well as on that I used for marking off the days that I had been successful. It was nice to have that visual reminder. I also kept track of how I felt each day which was not only for the purpose of the Whole 30 ®, but helped track moods and such. I am not a great journaler so keeping track of how things were going each day (or couple days when I would forget and have to back track) was a huge success and I am glad that I did it. - Whole 30 ® approved prosciutto! It made my life. While I am well aware of why proscuittiy is bad for you, it is something that I truly love and was super excited to find one without any preservatives. It did come with a heafty price tage ($8 or so for the package) but was a welcome treat for a couple lunches. Most lunch meats are filled with preservatives including sugar and nitrates. I don’t love lunch meats but do often use them as “sandwiches” (peppers as the bread) with cheese for a work day.
Struggles: NO MORE EGGs. I made an egg casserole bake for two weeks that was delicious and chocked full of veggies and my fave nutitrional yeast (much to my co workers dismay and disgust) However eating eggs pretty well each day for breaky is not fun. Breakfast recipes were far and few between and I actually found a few great ones towards the end of the Whole 30 ® that I will incorporate into my next cycle. -Having to explain what and why the Whole 30 ®. I am a pretty open person and love teaching people new things, especially things that can be beneficial to their health/fitness/life but sometimes It got to be a little much explaining it to everyone and having to almost justify it. I believe everyone should be able to eat and drink whatever they want without having to justify it. I get that all of these “fad diets” are silly and/or intriguing to people so I do see why people have their apprehensions and questions.
Suggestions: TRY NEW THINGS. Combine textures and flavours! This week I had burgers but normally I love cheese on my burgers. Instead, I made some delicious guac and put that on my burger which made it super yummy and more filling! -Embrace the change. Embrace new things. I made a new recipe each week either from the book or from pinterest (which is so addictive it’s insane). When I worked 4 on 5 off a few years ago, I would strive to make something new each set off and I really missed making new things. I am super fortunate to live at home and have an amazing mum who helps/encourages healthy eating. She often makes new, healthy alternatives to our fave meals which was very helpful during this month. (Some faves are zucchini pastas, cauliflower rice, spaghetti squash etc)
Next Steps: Once the Whole 30 ® is over, there are two ways you can reintroduce all of the food groups and “trigger” foods you have been avoiding. I chose to do an accelerated version of the 10 day program because a week after finishing the Whole 30 ®, I was headed to Paris, France with my boyfriend and didn’t want to miss out on all the yummy cheeses and wines. I started initially encorporating non gluten grains (which I accidently added in legumes and soy at gthe same meal) to see how I would tolerate that. The premise is to add one of the food groups every 3 days while eating Whole 30 ® approved foods the rest of the time. For an example, on day 31, you would add a bit of milk to your coffee, cheese on your salad at lunch and some yogurt after your dinner. On days 32 and 33, you would eat Whole 30 ® approved meals again and see how you felt on those days. Monitoring things such as moods, energy, bloating, sleep etc are super important. I did pretty well until leaving for Paris when it all went downhill form there. I did exactly what you aren’t supposed to do- add everything (and anything!) you weren’t supposed to eat during the Whole 30 ® almost all at once. At least I had already slowly reintroduced a few of the food groups that aren’t Whole 30 ® approved before leaving.
Once in Paris, I have to say I felt pretty crummy with all of the foods I was eating. Don’t get me wrong, I had the best time and wouldn’t really change much but I did noticed a HUGE difference. I was far more bloated with a lot more digestive issues and issues with fatigue. I slept well however did have more “sugar crashes” along with snappy periods of moods (just ask Alex, poor guy). I may have overindulged for a week (macarons each day, wine and cheese for dinner etc) but enjoyed it and have to live with those decisions. Being back home, I thoroughly missed all of the amazing whole foods I was eating and the way I felt both mentally and physically. While I have not decided if I will redo the Whole 30 ® right away or just incorporate the most important parts (like no added sugar and minimal dairy), I am excited to get back to healthy eating and feeling better than yesterday!
This blog was pretty eye opening to write (just as the experience was) and I appreciate anyone (if anyone) who has taken the time to read it. This blog has been more personal to write as the topic is something that is quite personal and individual. I hope that I have at least prompted a thought about what kinds of things others might be putting into their bodies and how they are affecting them either physically or mentally.
PS. Thought I would add a small part on my basic meal prep. I developed a weekly meal prep guide that was super helpful for me. For anyone that knows me well, knows that I am super OCD and anal with organizing things and love having lists/plans/etc. My personal calendar is colour coded by event, job and other activities which causes a lot of jokes at work when left open unattended.. The meal prep sheet had room for each meal along with shopping list area and a spot for other info e.g what needed to be prepped when etc. I am happy to share any and all prep plans (I have a monthly one that is an easy basic prep one along with the more helpful weekly one that helps with grocery shopping and planning).
Basic meal prep: Breakfast: Bullet proof coffee (ghee, MCT oil and coffee in a magic bullet for 15 or so seconds), Lara bar with fruit or egg variations. I recently saw a lot of sweet potato toast recipes along with easy pancakes using eggs and bananas (which I do not like so have not tried myself) Lunch: Salad filled with veggies or tuna with homemade mayo (word to the wise, make sure you don’t put too much lemon in it). I also love cut up veggies with hard boiled eggs on the side. I love snacks for lunch and typically this works well at work when you don’t always have time to have a proper meal. Dinner: chicken/pork/fish with veggies. I used a lot of frozen veggies as they are often super easy to prep last minute and keep a bit better than fresh stuff sometimes. I typically use Mrs. Dash’ spices or other Whole 30 ® approved spices (there are tons online if you google them). I made a few great chilis and “taco” mixes that I enjoyed Snacks: nut mix (no peanuts) with sulphite free dates or apricots, kombucha, sparkling water, fruit, apple sauce, veggies etc. I LOVE sparkling water. I have never been the biggest pop drinker but do love sparking water and always buy cases of it when it goes on sale. This is not the most economically or earth friendly option so I do try and use our SodaStream as often as possible (they are well worth the investment).


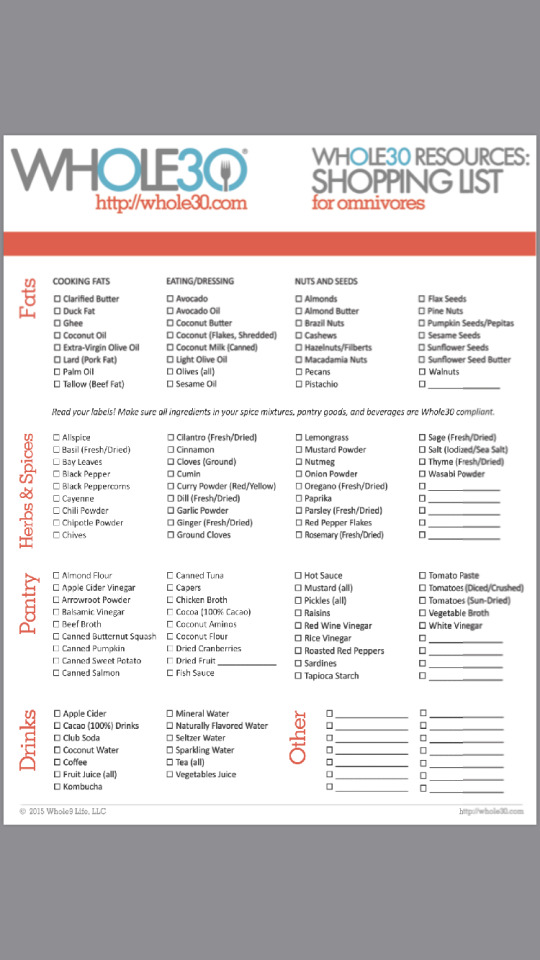
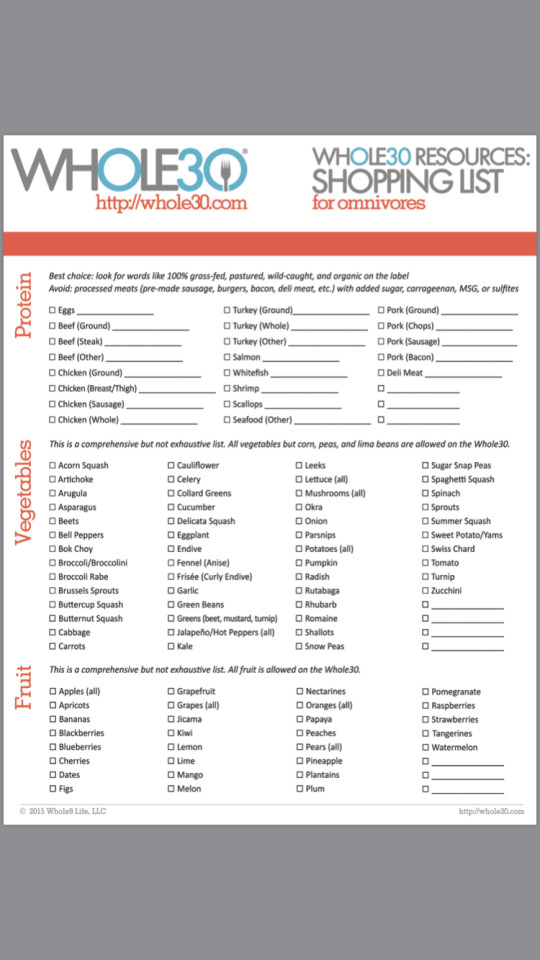


0 notes
Text
Ask the Vet With Dr. Kris: Dr. Kris Answers April’s Questions
In February, we launched our new “Ask the Vet With Dr. Kris” segment. Once a month, we’ll post a reminder for you to post your questions for Dr. Kris. He’ll answer as many of them as he can each month, and I’ll publish his answers in a subsequent post.
Dr. Kristopher Chandroo is a veterinarian, scientist, photographer, animal welfare advocate, and creator of Stress to Success (STS): The Essential Guide to Medicating Your Feisty, Grumpy or Reluctant Cat. Dr. Kris wants your cats to be twenty years old. And counting! And he wants to provide medication and therapy to them in a way that respects the bond between cat and human.
Here are Dr. Kris’ answers to some of your questions asked in March. If your question didn’t get answered here, Dr. Kris will answer them on his own website, in the future. Subscribe to his updates so you’ll be notified when the answers are published.
Was cat overdosed on thyroid medication?
Why do vets insist on overdosing cats with the hyperthyroid medicine methimazole? It’s been proven it’s better to start at a low dose and increase gradually until an ideal T4 is met, rather than risk the complications of an overdose and compromise the kidneys. I’ve had two cats with this terrible disease and both were initially overdosed, with one recently dying from the effects of too strong of a dose. I’m heartbroken and angry at the same time that vets still continue to overdose cats on this powerful medicine. (Janet)
Dr. Kris:
I don’t know.
I don’t know what’s happening in your world, and what happened to your cats during their treatment.
But I’m sorry to hear that you lost your cat.
I do know that you are heartbroken and angry. You didn’t have to say that for me to have known that. Who wouldn’t be? When you tried to make something right, made a choice, and things ended up wrong.
We can be consumed by guilt when that happens. Some of us get angry. We find places to put the blame. I’m going to answer the technical part of your question. I’m going to share my experiences, and if it helps you, then I’ve done what I’ve set out to do. It may not change how you feel though.
The starting dose for methimazole comes from a big book that gets updated every few years, which in turn comes from published studies that evaluate for effectiveness and safety. To that, you add your experience and discretion, and everything else that you know about your patient, and calculate the starting dose.
Untreated, chronic hyperthryoidism can damage kidneys. But it’s twice as bad as it sounds, because as it damages the kidneys, it also hides the wreckage. When you treat a cat for hyperthryoidism, you don’t compromise the kidneys by way of methimazole. Methimazole is simply pulling back the veil. You are revealing any damage that was already done (if any). The hyperthryoidism will be fatal if left untreated. The compromised kidney can become the beacon of hope, because it can be successfully managed.
And yet none of this changes the fact that you still have lost your cat. You will still feel heartbroken. And we all blame something or someone at some time or another in our lives.
I think about loss. I think about what it’s going to be like when the ones I love are no longer here. I’ll probably feel just like you do right now.
Cat is getting sores from overgrooming her belly
I have a question about one of my cats that hopefully you can answer. She is almost 5 years old and back in the summer I noticed she is gaining a lot of weight. then I noticed her belly is bald and thought maybe it was because she gained too fast. But I have started noticing she licks and sucks her hair down there and she is starting to get little sores from it. I feel it’s a bad habit now and would love to know what to do to get her to break the habit. she doesn’t act sick or sore or anything. She acts the same as always, silly and playful and always eats and potties well. So I don’t believe it’s an illness. but I would love your opinion of it. (Janine)
Dr. Kris:
Hi Janine!
Here is the rule I live by for cats who are pulling out their fur and creating sores on their skin:
When it looks like a habit, and even feels like a habit, it ain’t a habit.
People are really good at knowing their cats. What they do and how they do it. And we describe things in terms of habits. Cause’ it’s what we humans do. Smoking. Netflix. Cheating. Gambling. People habits!
And 99% of the time, any change to the fur or skin being described as a habit is actually a system change in your cat that I’m going to find during an appointment.
That’s not to say she has something terrible or bad. Not at all.
But believe this: They can act the same, be silly, playful, eat, and use the box ok, and yet STILL you can have a cat with some sort of condition. Because that’s how cat’s roll. It’s what they do. It’s their Modus Operandi.
The little sores are likely mild dermatitis. The reasons why an otherwise happy, normal cat will develop those are numerous, and the internet will give you a million answers (from contact sensitivity all the way to anxiety).
It’s usually straight forward to find out what those reasons are at the vet.
Good luck!
5-year-old cat is limping after play
Hi Dr. Kris, Pery is my little boy, i can’t precise because he was kind of adopted, but we guess that he’s about 5. He started limping after coming from a 10m play in the garden. Has it didn’t improve I’ve taken him to the vet and then was referred to a specialist. Here’s the report: “There are signs of previous surgery and arthritis in each stifle (knee), right worse than left. Also, there are signs of cruciate ligament rupture in the right stifle. On the basis of findings I suspect current lameness is an exacerbation of a chronic problem and think it better to consider non surgical management initially before performing surgery. Given the arthritis present, surgery is likely to be of limited benefit. Exercise. Keep indoors. No climbing, jumping or rushing about for the next 6 weeks. Give me a phone if you have any queries and also a few days after you come back in about 6 weeks.” The verbal advice was in fact to keep him in a crate but this would be too distressful and I just opt to keep him indoors and without toys. On the day he had some x-rays done and we found out that had surgery on both knees, because there’s pins on both and a screw on one only. He’s much better at the moment, this happened in January, but I think it’s in bit of pain. He does a few, and different noises when it’s laying down and sleeping too, that he didn’t before. Can you give me your opinion regarding the recovery time and method and also if the increasing in vocalization is related with pain? (Bruno Ferreira)
Something like that happened with the first cat I adopted, Zack. He was really really quiet in the shelter. Everyone thought he was shy, and gave him his space. Turned out he had a dislocated femur, and Jen (his first person) flipped the bill for his surgery within weeks of adopting him (she noticed he was limping and more quiet than shy would explain)!
Arthritis means inflammation. And inflammation means pain.
I would definitely treat him for pain. I would give him the benefit of any doubt there, given what he has wired up to his knees.
It can take a busted cruciate 4 to 6 weeks to heal, and then you have to “ease them back into activity”.
Yeah, I know. Easier said than done. Our cat’s have no idea why they can’t do all the things they need to do. So sometimes they also get anxious or bored.
Rest him, but see if you can keep his mind active. Like this as long as he doesn’t overdo it: https://www.youtube.com/watch?v=H9fwmG-oue8
Good Luck,
Dr. Kris
How to prevent dental problems
I have two indoor cats. I’ve never brushed their teeth one of them is 3 the other is 6 and I am reading about all the dental problems cats can get as they get older. Most of my cats have lived to their late teens and I have never had dental problems. Could you give advice on how to start and what items to use for home preventative dental health for cats? (AK)
Dr. Kris:
It’s very true. Your cat’s in their teens may have no dental problems. Like Uncle Bob. You know that uncle – smokes, drinks, eats KFC religiously, and thinks that calories are the tiny creatures in your closet that sew your clothes a little bit tighter every night. And he outlives everyone!!!
But what about the rest of the cats out there. The non-Uncle Bobs? Most cats are like them.
And it’s not just older cats. I’ll see dental issues forming at 2 years of age. Sometimes younger. One of the very first things I do when I examine a cat in clinic is…look in the mouth. See what the teeth and gums are up too.
I’ll talk about what I see, almost in passing, then look up to see the response of the client. If they are totally glazed over (the “I’m just here for his vaccine and you’re 5 minutes late look”), then I move on. If they lean over, look in the mouth too, and start asking questions, I know this is a person who is going to try something to help their cat’s mouth. So I go further. Encourage more questions. Tell them what they need to know.
See, you’re one of those people. You would have leaned in, and asked a question or taken interest!
But what can they do at home they might ask? Brush their teeth.
And most people, right at that point know it’s not going to happen. You can see it on their face. They are not going to brush their cat’s teeth! They can’t clip the nails, let alone brush the teeth.
So you want to start slow. In your cat’s mind, you want to match up the sensation of eating treats with handling their mouth. This is called counter-conditioning. Give them a treat while you touch their face on Monday for a few minutes. Repeat that on Tuesday. On Wednesday, touch their gums for a few seconds with your fingers while giving them treats. Repeat that on Thursday. By Friday, rub your fingers along the teeth. Just briefly as they munch on a treat. Don’t get bit
If you and your cat can do that, it won’t be too hard to brush their teeth. Start simple. Start with a single tooth if you need to. Just go slow. Some people find it useful to use the little thimble brushes. Then, there are lots of youtube videos to show you the technique.
If your cat has tartar build up, gingivitis, or worse, resorptive lesions, then you want to think about dentistry. Otherwise, you’re just brushing the tartar.
I’m always pleasantly surprised with the official, tested dental diets. Yeah, they’re not for every cat. But I do see results with those foods as well. (A note from Ingrid: while Dr. Kris and I agree that the idea that dry food scrapes tartar off teeth is a myth, I disagree with Dr. Kris on the utility of dental diets in specific cases.)
So start by making friends with your cat’s mouth. Uncle Bob would be proud.
Natural remedies for asthmatic cat
Hi Kris, our cat has a mild form of asthma. Her only noticeable symptom is a cough that can be chesty or dry. We feed her very good food including raw organic produce. We also offer her salmon oil, colloidal silver etc but the cough persists, I was wondering if you had any natural suggestions as we don’t want to give her medications long term. Thank you for this opportunity, it is much appreciated. (Colette Gray)
Dr. Kris:
Hi Colette!
Since you have the food taken care of, you could consider an air purifier. One that a dermatologist or allergy specialist would recommend. Also, change the air filters in your house, and get the ones that are the right micron level to filter out allergens that can irritate asthma.
Change the litter boxes every 6 months. As in get rid of the old ones if they are scraped up and hold on to dirt.
Since I’m not a naturopath, I don’t have much experience with natural products to treat asthma.
But I do get asthma, and the tightness in the chest is just awful when it flares up. I can relate to these guys when they come in.
You gotta get the inflammation down in the chest. Significantly. You have to put out the fire. Because once you do, sometimes, they don’t need the drugs long term! A cat who coughs occasionally might be a cat who is feeling tight in that chest. But they won’t tell you about it. Because they hide this stuff all the time. So use the best tools you have available to do that.
Do you have a question for Dr. Kris? Leave it in a comment!
The post Ask the Vet With Dr. Kris: Dr. Kris Answers April’s Questions appeared first on The Conscious Cat.
0 notes
Text
Ask D'Mine: Treating a Diabetic "Junkie," and Considering "Insulinotropic" Foods
New Post has been published on http://type2diabetestreatment.net/diabetes-mellitus/ask-dmine-treating-a-diabetic-junkie-and-considering-insulinotropic-foods/
Ask D'Mine: Treating a Diabetic "Junkie," and Considering "Insulinotropic" Foods
Need help navigating life with diabetes? Ask D'Mine! That would be our weekly advice column, hosted by veteran type 1, diabetes author and community educator Wil Dubois. This week, Wil takes on the issues of doctors seeing "junkies" rather than patients struggling with addiction, and the insulinotropic effect of certain foods on PWDs.
Got your own questions? Email us at [email protected]
Anonymous from Alabama, type 2, writes: I was diagnosed 5 months ago with type 2 diabetes. I assume I've had it for a few years, but I have no insurance and didn't realize how dangerous it really is. I'm now reading a lot more and I'm terrified. My feet and hands are numb most days. Fatigue is a mild word. I finally got in a community free clinic and I'm on 2000 mg metformin a day and was on 15 units of Lantus. I had to stop taking Lantus because it seemed to be making me have withdrawals from the methadone I've been on for five years. Extreme diet change has lowered my numbers a lot, but the doctor seems to be not as concerned as I am, and this really bothers me. And I can't seem to get much info about the methadone and the insulin. Any info you could give, or where or what to do next, or any insight into my situation? Thanks, I'm worried.
Wil@Ask D'Mine answers: It's OK to be worried. Fear can be a healthy emotion, so long as it doesn't rule the day. And, hey, I'm proud of you. You got yourself into a clinic—better late than never—you've made extreme diet changes, you're reading up on your diabetes and you're asking questions!
As to your doctor, well, I'm not so proud of him. I think you might have gotten one of the bad ones. Most docs at free clinics are pretty awesome people who are drawn to helping people in the greatest need. Let's face it, no doc works at a free clinic for the money—this kind of work is among the lowest-paying in medicine.
That said, and there's no delicate way to say this, so bear with me... I think he might see something different when he looks at you than what I see. I'll go first. When I look at you (well, at your email—but I can "see" a great deal in the words people place on a page), I see someone who's had a pretty hard road. I see someone who's suffering a great deal, but trying to improve her lot in life. I see a fellow PWD. Hell, I just see a fellow human being.
And that's good enough for me.
Your doc, however, sees something else. He looks at you and sees a junkie. Long-term use of methadone is sometimes used to treat chronic pain, but is usually used to treat opiate addictions. A methadone prescription is a red flag. In fact, just like your doc, I'm actually going to assume that's why you are taking it; but unlike your doc, I'm not going to judge you for it. For some reason, some really great docs get hung up over drug use and, like the Grinch, their hearts suddenly shrink. I've seen some pretty open-minded providers act really strangely around IV drug users. So when I read your email I found myself wondering if your doc was really listening to you or if he'd gotten hung up over your past with his brain stuck in a stupid loop about "so she had money for heroin, but couldn't be bothered to pay for her health care, I'm not going to waste my time..."
That's #@$%& BS! I say to your doctor: If you can't accept everyone, regardless of their faults, as worthy of the same treatment, then you don't belong in medicine. The door is over there. Please leave, we have enough real challenges to solve without those kinds of attitudes. I'm sure you'll do just fine in politics.
So I spent most of my spare time the last few weeks trying to see what's known and not known about methadone and Lantus. The answer: not much.
In fact, about all I could find were two reports of photosensitivity in women over 50; and one report of "chills" in a 60-year-old man. Now chills might sound a bit like your "withdrawals." And if it happened to one other person, it sure as hell could have happened to you, too.
The solution? Well, based on my field experience, I've found the various insulins we have to play with are a lot more different than apples and oranges. We tend to think of Lantus and Levemir like we think of Tide and Cheer: hey, the brands are different, but they both clean your clothes. And while it's true that the glucose response profile of the two basal insulins is pretty much the same, they couldn't be made any more differently. Hell, they aren't apples and oranges so much as watermelons and papayas. People who have some sort of oddball trouble with one often do fine on the other. And don't forget we have the old-fashioned NPH as an option, too.
My advice? Go back to your clinic, but ask to see another provider. Look the white coat straight in the eye and be honest about your past and passionate about your future. Be clear about your here-and-now fears. Then ask to try a different insulin, and see if it plays better with your methadone.
Oh, and don't vote for your old doc if you see he is running for Congress.
Paul from Georgia, type 1, writes: I have recently read about foods like milk and wheat causing increased secretion of insulin (insulinotropic effect) above the insulin needed for the carbs in the food. This fact is used to conclude that products containing these ingredients be used sparingly, if at all, in an attempt to prevent obesity and type 2 diabetes. The reason being that these foods cause an overproduction of insulin that leads to storage of excessive carbs as fat. My question is as a type 1 with a negative c-peptide is: will eating these foods have the same effect? My guess is unless they cause a glucose rise above the carb content that I gave a bolus for, there will be no extra insulin unless I give extra insulin.
Wil@Ask D'Mine answers: Well, first off, you and I must be reading different journals, because I haven't seen nor could I find anyone worrying about insulinotropic foods causing weight gain. In fact, just the opposite may be true—they're being heralded as the next great thing in diabetes treatment, and some people think they may even help prevent obesity.
But let's back up and give all our readers some background. Then we'll dissect the issue you read about a little more and I'll take a crack at your question. As you said, insulinotropic is just a fancy-pants cocktail party word for something that causes insulin production. And it's been a known mystery for a number of years that different proteins have different "insulinotropic properties," meaning that they trigger insulin production independent of their glycemic index; the exact opposite of what logic would suggest. WTF?
Back in 2004, a team of Swedish researchers singled out milk as being the most unusual in this regard. After much study the smoking gun was proven to be whey protein, which makes up around 20% of milk's protein (but a whopping 60% of the protein in human breast milk, "food" for thought). Why whey kicks the body in the pancreas more than you'd expect, given its carb count, remains a mystery to this day.
But, but, but: just because it induces the body to produce more insulin than the glycemic index would suggest, doesn't mean it's making your body produce more insulin than it needs. In fact, the extra squirt of insulin from whey has been shown to greatly reduce blood sugar spikes after meals. So much so, that mixing whey into high carb meals has been shown to have a medicinal effect in type 2s. In other words, a natural insulin secretagogue. (One study added whey to a meal of mashed potato and Swedish meatballs, which I find ironic given the original whey discovery came from Swedish researchers.)
Over the last few years, there has been much ongoing research that, quoting another study, "dietary interventions represent a promising therapeutic strategy to optimize postprandial glycemica." Whey as medicine for all that ails you.
In a stretch, I suppose I could see your point about extra insulin moving the carbs into fat storage, but leaving the extra carbs in the blood moves the type 2 into the dialysis center. I don't think these foods are likely to cause greater weight gain because of the extra insulin, nor do I think type 2s should avoid them only out of fear of weight gain. I think anyone who is worried about weight should focus more on eating less, and less on what they are eating. And just to muddy the waters, I'm seeing a lot of research actually supporting whey as an anti-obesity agent, rather than a trigger for weight gain. This has led to whey becoming a popular food supplement, especially for the for body building crowd. It's seen as agent of muscle growth and fat reduction, but like many food supplements, we are lacking in solid science behind this particular claim.
But as to you, my insulin-deficient friend, you're right. An insulinotropic food will not bring your dead beta cells back to life. An insulinotropic substance needs an insulin-producing body to act on.
However, your question raises another: If the "normally" functioning human body produces more insulin for whey than you'd expect it to need... why is that? Frankly, the body tends to know what it's doing. Even though the glycemic index of foods with whey shouldn't demand more insulin, the body provides it, and apparently with good results.
Maybe we should all consider a whey bolus.
This is not a medical advice column. We are PWDs freely and openly sharing the wisdom of our collected experiences — our been-there-done-that knowledge from the trenches. But we are not MDs, RNs, NPs, PAs, CDEs, or partridges in pear trees. Bottom line: we are only a small part of your total prescription. You still need the professional advice, treatment, and care of a licensed medical professional.
Disclaimer: Content created by the Diabetes Mine team. For more details click here.
Disclaimer
This content is created for Diabetes Mine, a consumer health blog focused on the diabetes community. The content is not medically reviewed and doesn't adhere to Healthline's editorial guidelines. For more information about Healthline's partnership with Diabetes Mine, please click here.
Type 2 Diabetes Treatment Type 2 Diabetes Diet Diabetes Destroyer Reviews Original Article
0 notes
Text
Identity economics: Who are you? And how does it affect your spending?
“Who are you?” my cousin Duane asked me on Saturday afternoon. We'd spent the day playing nerd games together and were taking a break for pizza.
“What?” I said. I wasn't expecting a philosophical question over supper.
“I don't think you know who you are,” Duane said.
“What do you mean?” I asked.
“I don't think you know who you are,” he repeated. “You write about money and frugality, yet you spend $200 on dinner.” Duane was referring to the fancy meal we'd had in May at a Michelin-star restaurant in France. I knew it had been bugging him, but he hadn't said anything about it until now. (And that meal cost $267.41 for the two of us, not $200.)
“You paid $1900 for your used pickup, but you don't wash it. It's filthy. You buy new clothes that you don't need, but you leave your old clothes on the floor so that your cats pee on them.” It's true. Kim and I have a cat that will, from time to time, pee on my clothes.
“You say you don't like attention, that you don't want to be a celebrity, yet you're always taking on new work that puts you in the spotlight. You're thinking of doing a course for Audible, for instance, and you're talking about doing more speaking gigs — even though you hate speaking gigs,” Duane said.
All of these things were true. I couldn't argue.
“Who are you?” Duane asked. Well, that's a mighty fine question, Duane. That's a mighty fine question.
A Digression
In 1862, French novelist Victor Hugo published Les Miserables, one of the greatest novels of the nineteenth century. Long and sprawling and full of digressions (just like Get Rich Slowly!), the book explores the many facets of human nature: the good and bad, the humorous and poignant, the ordinary and sublime.
Les Miserables wasn't popular with critics when it was released, but everybody else loved it. It sold well when it was published and continues to sell well more than 150 years later. The book has inspired several several film and television adaptations. And, of course, it's the source of one of the most successful stage musicals of all time.
Turns out PBS recently aired a new six-part Les Miserables miniseries written by the always-awesome Andrew Davies. It's on my watch list.
Although Les Miserables contains a ginormous cast of characters, two stand at the heart of the story:
Jean Valjean is the novel's protagonist. Arrested for stealing a loaf of bread to feed his sister's seven starving children, he spends nineteen years in prison (five for the original crime, fourteen more for various misdeeds). Upon parole, he assumes the identity of Monsieur Madeleine. As Madeleine, he builds two factories, becomes rich, and is appointed mayor of a small seaside town. Valjean is a good man who occasionally finds himself on the wrong side of the law.
Javert is the novel's antagonist. (It's not right to call him a villain. Nothing about him is villanous.) Born in prison to deplorable parents, he grows up to become a prison guard — then police inspector. Javert is obsessed with upholding the law, which includes pursuing and punishing Valjean for his past misdeeds. His worldview is shattered when he realizes that not all laws are moral, that sometimes the moral course is not the lawful one.
What's fascinating — mind-blowing, actually — is that Victor Hugo based both Valjean and Javert on the exact same real-life person. They're both loosely modelled on Eugène François Vidocq, a French criminal turned criminalist. (You should open that link in a separate tab for later reading. Vidocq's life is fascinating. Among other things, he's regarded as the first-ever private detective and the “father” of modern criminology.)
That's right: Both the protagonist and the antagonist of Les Miserables were inspired by the same man. And, even more mind-blowing? Vidocq was also the inspiration for Sherlock Holmes. (Go read that article!)
Who Am I?
The amazing thing (to me) is that Jean Valjean himself is two people! He is Jean Valjean, yes, but he spends years posing as Monsieur Madeleine. As the latter, he's a wealthy factory owner, he's mayor of Montreuil-sur-Mer. He is a force for good in his small world. He is, at once, both Valjean and Madeleine, just as Vidocq is at once both Valjean and Javert.
In a 2012 New Yorker piece praising “the persistent greatness” of Les Miserables, Adam Gopnik wrote, “Hugo believed in, relished, luxuriated in, contradiction — he thought that we show ourselves most truly when we are seemingly most opposed to our double natures.”
When I posted about this on Facebook in April, John from ESI Money observed that this adds a whole new meaning to the song “Who Am I?” from the musical.
“Who am I?” Valjean sings as he's forced to reveal his identity in order to save an innocent man. “Who am I? I'm Jean Valjean!”
Yes, that's true — but Jean Valjean is also police inspector Javert.
youtube
True story: I'm a devoted fan of musical theater, and “Who Am I?” is one of my favorite songs from any show. It induces frisson — it gives me goosebumps — every time I hear it. Every time.
What I like about this clever bit of character creation from Victor Hugo is how it highlights our inherent dual natures. We, as humans, are inconsistent. We are complex creatures. At the same time, we can be both good and bad. I truly believe that most of us do what is right most of the time — but each of us also sometimes makes poor choices. We do things that seem to go against who we say we are and what we believe.
In Valjean and Javert, we get to see human nature dramatized in two men forever at odds, just as we are each forever at odds with ourselves.
Me, Myself, and I
As I was walking the dog this morning, I found myself meditating on my own personal duality. I am at once the hardest working person I know…and the laziest. I am the smartest person I know…and the stupidest. I am the kindest person I know…and the meanest.
Recently, I've grown increasingly frustrated with my seeming inability to “do the right thing”. I know that there are certain actions I could take (and should take) to improve my health, to build this website, to maintain relationships with my friends. Yet I do not do these things. I actively avoid them.
Why is this?
Here's an example. I could solve a whole host of problems if I were to get regular aerobic exercise. Over the past year, I've done a fine job of strength training, but for some reason I've become allergic to sweat. I do whatever I can to avoid running or biking or otherwise increasing my heart rate.
It's not that I can't do these things. I know I can. And I like them. I've run half marathons (and walked a full marathon). I've completed a century ride — one-hundred miserable miles on a hot and windy summer day. I did Crossfit for five years. I'm capable of strenuous exercise, and I know it.
But I'm not doing that exercise right now. I'm avoiding it.
Three months ago, as the sun started to show its face here in Portland, I wheeled my bicycle from the bottom of the hill to the back office. I wanted to make it easy to hop in the saddle and go. But you know what? I've ridden the thing exactly once this year. The bike is just sitting there, pleading with me to ride it.
The same goes with the website. You all know that I can crank out an article a day. I did it for three years between 2006 and 2009. I did it for the first three months of 2018. When I put my mind to it, I can write well without sacrificing quality.
Yet, for some reason, it's tough for me to publish even once a week lately. My mind is elsewhere. I have no inspiration. This wouldn't be so bad if I were at least handling other site maintenance chores, but I'm not. The site redesign is nearly finished, but it isn't live because there are still things I need to do. I'm not processing guest articles. I'm not posting to social media.
I've no doubt that some of this malaise stems from my chronic depression. But I also know the best way to shake the self-loathing is to actually do something, you know?
Which leads me to fundamental question I find myself facing: If I know what is right, why don't I do it?
I have no answer.
Impossible Expectations
This year, as every year, my depression and anxiety became especially strong during the spring. What's different about this year is that I sought out a therapist.
A few weeks ago, she asked me about my writing. We hadn't talked about it before. “What does success look like for you when it comes to your work?” she asked.
“Success means publishing three articles per week,” I said.
“Why?” she asked.
“Because then I'm giving my readers lots of material. I'm helping them. When I give them a lot of material, they want to come back more often. When I publish more material, more people find the site by search. When I publish more material, I make more money.”
“So, you want to publish three times per week?”
“I guess so,” I said. I thought about it a little. “But I hate the pressure that pace puts on me.”
“Why?” she asked.
“Because I don't enjoy it. I don't do great work under time pressure like that. I want to take my time. If I decide to write an article on, say, the history of retirement, then I want to read a book on the subject. Maybe two or three. I want to think deeply about it. Then, I want to take the time to write the best article out there about the history of retirement.”
“You realize you've just told me two very different things, right?” my therapist said. “You've set up contradictory goals for yourself. Plus, you're asking yourself to be the best. That's a tall order. No wonder you're stressed. You have impossible expectations for yourself.”
When I think about it, my therapist is right. I do have impossible expectations for myself — on a lot of things. I have contradictory goals. It's as if there's a Jean Valjean inside of me and an Inspector Javert. And they want different things. Neither is wrong — but they can't both have their way.
But to which do I yield? Am I Valjean or Javert?
At the end of the session, I lamented my dual nature. “I tell other people to be proactive,” I said, “to take charge of their own lives, but I have a hard time doing that myself.”
“Do you think that makes you a hypocrite?” my therapist asked.
“No,” I said without hesitation.
“Good,” she said.
“I think it makes me human,” I said. “I write about the things I struggle with personally. When I started writing about money and getting out of debt, that's because I needed to get out of debt. Now, when I write about tracking spending or having a sense of purpose, that's because I need these things.”
Mindful Spending
So, this is all very interesting on a philosophical level, but what does it have to do with personal finance? Lots, actually.
We make our purchasing decisions based on who we are and who we want to be. If we're not clear on who we are and who we want to be, our choices tend to be arbitrary. They're spontaneous and not based on anything other than immediate desire.
When you're clear on who you are and what you want, it's much easier to practice mindful spending, to be deliberate about the things you buy and own. If you identify as fitness-conscious, for instance, you'll be much less likely to be tempted by cookies and snacks in the grocery store. If, like me at the moment, you identify as a “lapsed” fitness junkie, well then it's much easier to succumb to temptation.
Who we want to be also affects how we spend. In fact, I suspect that much wasted spending — not just for me, but for everybody — is what I'd call “aspirational”. It's not based on our actual habits and actions but on what we wish we did.
Take my bike, for example. I bought it last year but have ridden it only three times in fifteen months. Like I mentioned earlier, it simply sits there, pleading with me to ride it.
I have a good friend who once decided he'd like to learn woodworking. His father had always built and repaired things around the house, and my friend aspired to do the same — even though he had never done so in 35 years of life. He bought a stack of woodworking books, then acquired several expensive tools. He never used them. These were aspirational purchases, based on somebody he wanted to be, not the person he was.
From what I've seen, a lot of folks do this sort of thing with cookbooks. They want to try new recipes and new cuisines, so they gradually fill a shelf with cooking manuals — cooking manuals that they seldom use.
It's because of this relationship between money and identity that I'm so insistent that GRS readers write a personal mission statement. When you're clear on your purpose, it's much easier to make sure your spending is aligned with your values, that your financial decisions are based on who you are instead of some idealized version of who you want to be.
Identity Economics
In their fascinating (if dry and academic) book Identity Economics, George Akerlof and Rachel Kranton explore how our identities shape our work, wages, and well-being.
“In every social context,” the authors write, “people have a notion of who they are, which is associated with beliefs about how they and others are supposed to behave. These notions…play important roles in how economies work.” Our identities determine how we earn a living and how we spend our money.
Akerloff and Kranton say that large portions of our identities are shaped by the environment:
Identity, norms, and social categories may appear to be abstract concepts, but their reality is both powerful and easy to see. Norms are particularly clear when people hold an ideal of who they should be and how they should act.
Here's an example: Many folks who discover the early retirement movement do so through the awesome work of Mr. Money Mustache. He has a strong voice and a popular website. Over the past few years, he's accumulated a passionate army of followers who call themselves Mustachians.
When a person identifies himself as Mustachian, he subscribes to a certain set of values, to particular ways of working with money. Driving is frowned upon. A high saving rate is encouraged. Thrift is a prized virtue. This is identity economics in action.
Akerloff and Kranton are careful to note that our personal identities are not static. They change. Our larger identities change slowly over time, but we can also shift roles rapidly in daily life.
The latter is easiest to see. “Over the course of a day,” they write, “a woman may see herself as a mother at home and a professional at work.” I'd add that she might see herself as an athlete in her running group, a civic leader as a member of the city council, and a Mustachian when she's hanging with her financial friends online.
Each of these is a different identity — or perhaps a different facet of her overall identity. And each affects how she works, saves, and spends.
People change over their lifetimes too. From the book:
People often make decisions that come back to haunt them. We overeat, we smoke, we spend too much, and we regret it. [This is due to] time inconsistency. People have different selves at different points in their lives. The new self could regret the decisions made by the old self…
Sometimes these transitions are anticipated, and people plan accordingly. But often, people only imperfectly anticipate who they will later become.
Look at my own life over the past decade. Who I am today is drastically different than who I was ten years ago. And twenty years ago. Sure, the core J.D. remains the same — once a nerd, always a nerd! — but my values, which are constantly evolving, have morphed and my day-to-day life is sometimes unrecognizable.
During the past ten years, much about my personal identity (and my resulting financial choices) has changed:
I deliberately chose to purchase a small home in “the country”.
I drink beer. I drink coffee. I ride a motorcycle. All of these actions are new.
I lost fifty pounds through years of exercise and healthy eating. Then I gained back forty of those pounds through years of neglect.
I sold Get Rich Slowly — then I bought it back.
These changes, large and small, all affect how I manage my money and how I spend my time. As my identity changes, so do my financial habits.
Related reading: In a strange coincidence, The Guardian published an article on a similar subject last Saturday: “Are you really the ‘real' you?” This piece, which is terrific and well worth reading, looks at how some people change their lives entirely — and why.
Order and Light
At the end of the Les Miserables, after Jean Valjean frees Javert instead of killing him, the police inspector faces an existential crisis. Victor Hugo writes:
He saw before him two roads, both equally straight; but he saw two; and that terrified him — him, who who had never in his life known but one straight line. And, bitter anguish, these two roads were contradictory. One of these two straight lines excluded the other. Which of the two was the true one? His condition was inexpressible.
Inspector Javert's moral certitude proves to be his undoing. Like many folks who are certain they know what is real and what is right, Javert spends years ignoring evidence that controverts his beliefs. He thinks he knows the truth but in reality is blind to it.
youtube
When, at last, Javert recognizes that he's been in error all this time, that things are not as black and white as he believed them to be, it's too much for him to bear. Rather than face a world filled with ambiguity and uncertainty, he takes his own life. He jumps in the river and drowns.
Before he kills himself, though, Javert has a sort of revelation. He realizes that Jean Valjean and his alter-ego, Monsieur Madeleine, may have seemed like two different people, but they were one all along. They were two sides of the same person. Valjean was both criminal and hero.
It's all well and good to want to be a fixed, constant person, to have an identity that never changes. But that's not how healthy people work. Healthy people learn and adapt and grow. Who you are today is not the same as who you'll be tomorrow — or who you were yesterday.
As you change, your values will change too. Your goals will change. Your spending will change. What you want to do for work will change. And, yes, there will be many times when you are internally conflicted, when like Javert you are faced with two parallel roads, both of which are “true”.
Summing Up
Who am I? That's a great question.
I'm a guy who writes about money and frugality, but I'm also a man who is willing to — once in a lifetime — spend $267.41 to experience a Michelin-star restaurant in rural France. That's a clear example of mindful spending: I planned the meal weeks in advance and looked forward to it with great anticipation.
I'm a guy who can't bring himself to purchase a new car, so I buy a 25-year-old pickup for $1900. And I don't wash it. I value the vehicle but see no sense in spending the time, money, and energy to clean something that will never look pretty.
I'm a guy who buys new clothes from time to time — don't we all? — but who, yes, is careless enough to leave them on the bedroom floor even though I know my cat likes to pee on them. (Stupid cat!)
I'm a guy who hates public speaking and who doesn't want to be the center of attention, yet who has a deep desire to teach people about personal finance. (Especially the personal side of it all.) This leads me to do things that seem incongruent with what I say I want. I take on months-long projects that stress me out. I agree to fly across the world to talk to people. (Just yesterday, Paula Pant and I had a conversation about how the hassle of attending events is worth it for the friends we make.)
Who am I? I'm J.D. Roth.
The post Identity economics: Who are you? And how does it affect your spending? appeared first on Get Rich Slowly.
from Finance https://www.getrichslowly.org/identity-economics/ via http://www.rssmix.com/
0 notes