#'often avoids dislikes or is reluctant to engage in tasks that require sustained mental effort'
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The average Tumblr user visits about 67 pages every month.
Text
me looking at the ADHD diagnostic criteria in the DSM-5-TR since I have access to it for a school paper and being reminded of every weird and annoying thing I do

#adddna#'often fails to give close attention to details or makes careless mistakes'#'often does not seem to listen when spoken to directly'#'often does not follow through on instructions'#'often avoids dislikes or is reluctant to engage in tasks that require sustained mental effort'#'often talks excessively' 'often blurts an answer before the question has been completed'#GODDDD AAUUUUGGGHHHHH . ITS LIKE AN ADHD DIAGNOSIS IN HERE [LITERALLY TOOK STRATTERA THIS MORNING]
210 notes
·
View notes
Text
all the things wrong with lestat de lioncourt according to the dsm-v and psychological theories
In this post, I, a psychologist, will psychoanalyze and diagnose Lestat de Lioncourt, a well-known vampire in gothic literature.
Part I: DSM-V Diagnosis
1.0 Neurodevelopmental Disorders
1.1 Attention-Deficit/Hyperactivity Disorder (ADHD):
ADHD is a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development.
Lestat displays 5 symptoms out of 9 for inattention:
Often has difficulty sustaining attention in tasks: He can’t read.
Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace: He does not ever follow instructions.
Often has difficulty organizing tasks and activities: He fails to keep his house and belongings organized.
Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort.
Is often forgetful in daily activities: He’s bad with doing chores and running errands.
Lestat displays 5 symptoms out of 9 for hyperactivity and impulsivity:
Often unable to play or engage in leisure activities quietly: He’s always making noises.
Is often “on the go,” acting as if “driven by a motor”: He is usually unable to be still for extended time.
Often talks excessively: He is a yapper.
Often blurts out an answer before a question has been completed: He completes people’s sentences and he cannot wait for his turn in conversation.
Often interrupts or intrudes on others: He butts into conversations and he intrudes into or takes over what others are doing.
To be diagnosed with ADHD, one must display at least 10 symptoms out of 18. Therefore, Lestat can be diagnosed with ADHD.
2.0 Schizophrenia Spectrum and Other Psychotic Disorders
2.1 Delusional Disorder:
Delusional Disorder is characterized by the presence of one (or more) delusions with a duration of 1 month or longer. Lestat’s disorder is the Mixed type, meaning that not one single type of delusion predominates, but there’s a mixture. His disorder includes:
Grandiose type: Belief that one is famous, omnipotent, wealthy, or otherwise very powerful: At the end of S2.E8, we see Lestat practicing piano with a block of wood and thinking he’s going on tour.
Jealous type: Belief that their spouse or lover is unfaithful: He constantly watches Louis to see if he will cheat on him or not.
Persecutory type: Belief that they are being conspired against: In S1.E7, we see Lestat thinking Louis and Claudia are conspiring something against him and he makes Antoinette spy on them. (In the persecutory type, it does not matter if the person is actually being conspired against, it’s the obsession that counts.)
2.2 Schizoaffective Disorder:
Schizoaffective Disorder is characterized by an uninterrupted period of illness during which there is a major mood episode (major depressive or manic) concurrent with at least 2 criteria out of 5 of schizophrenia.
Lestat displays 2 symptoms of schizophrenia (A):
Delusions (mentioned above)
Hallucinations: He is haunted by Claudia.
Lestat also displays the main symptom of a major mood episode, which is depressed mood. We can see his depression and the symptoms of his schizoaffective disorder (delusions, hallucinations, and depressed mood) portrayed in several episodes, but mainly S2.E8.
3.0 Bipolar and Related Disorders
3.1 Bipolar I Disorder:
For a diagnosis of bipolar I disorder, it is necessary to meet the following criteria for a manic episode. Lestat displays 5 symptoms out of 7 for a manic episode in S2.E7:
Inflated self-esteem or grandiosity.
More talkative than usual or pressure to keep talking.
Distractibility (attention too easily drawn to irrelevant external stimuli).
Increase in goal-directed activity.
Excessive involvement in activities that have a high potential for painful consequences.
The trial is followed with a depressive episode on his side, therefore, he displays the two distinct ends of Bipolar I: manic episode followed by a depressive episode. Lestat, according to this, can be diagnosed with Bipolar I Disorder.
4.0 Depressive Disorders
4.1 Disruptive Mood Dysregulation Disorder:
Disruptive Mood Dysregulation Disorder is characterized by severe recurrent temper outbursts manifested verbally (e.g., verbal rages) and/or behaviorally (e.g., physical aggression toward people or property) that are grossly out of proportion in intensity or duration to the situation or provocation.
In many episodes, we can see Lestat being verbally and physically aggressive towards Claudia and Louis, let alone many others that he later kills. In the DSM-V, it is concluded that Disruptive Mood Dysregulation Disorder and Bipolar I Disorder cannot coexist, so it is not safe to say Lestat 100% have this disorder, but I thought it was worth mentioning as he displays the symptoms for it.
4.2 Persistent Depressive Disorder (Dysthymia):
Dysthymia is characterized by a depressed mood for most of the day, for more days than not, as indicated by either subjective account or observation by others, for at least 2 years.
Lestat displays 4 symptoms out of 6 for Dysthymia in S2.E8 and later in the song Long Face:
Poor appetite or overeating: ‘I'll get fatter when we break up.’ In this lyric, he mentions how he overeats (or rather overdrains people).
Low self-esteem.
Poor concentration or difficulty making decisions.
Feelings of hopelessness.
In the DSM-V, it is stated that there has not been a manic or hypomanic episode during the period of Dysthymia, which we cannot be sure if that is the case with Lestat, as I diagnosed him with Bipolar I earlier. However, S2.E8 and the Vampire Lestat era happens well after S2.E7, so we can assume that he had not had a manic episode and his mood disorder turned into Dysthymia.
5.0 Anxiety Disorders
5.1 Separation Anxiety Disorder:
Separation Anxiety Disorder is characterized by developmentally inappropriate and excessive fear or anxiety concerning separation from those to whom the individual is attached.
Lestat displays at least 4 symptoms out of 8 for Separation Anxiety Disorder:
Recurrent excessive distress when anticipating or experiencing separation from home or from major attachment figures: He constantly tries to make Louis stay because he is scared of him leaving.
Persistent and excessive worry about losing major attachment figures or about possible harm to them, such as illness, injury, disasters, or death: ‘Did you hurt yourself?’
Persistent reluctance or refusal to sleep away from home or to go to sleep without being near a major attachment figure.
Persistent and excessive fear of or reluctance about being alone or without major attachment figures at home or in other settings: He tries to win Louis back because he is scared of being without him.
Therefore, it is possible to say Lestat can be diagnosed with Separation Anxiety Disorder, as he himself mentions how he does not like being left behind.
6.0 Obsessive-Compulsive and Related Disorders
6.1 Obsessive-Compulsive Disorder (OCD):
OCD is the presence of obsessions, compulsions, or both.
Lestat displays 2 symptoms out of 2 for obsessions:
Recurrent and persistent thoughts, urges, or images that are experienced, at some time during the disturbance, as intrusive and unwanted, and that in most individuals cause marked anxiety or distress: In S2.E8, he mentions his recurrent thoughts about Claudia and how he cannot get over it.
The individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralize them with some other thought or action.
Lestat also displays symptoms out of 2 for compulsions:
Repetitive behaviors that the individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly: He plays the piano as he did with Claudia to get rid of the obsession.
The behaviors or mental acts are aimed at preventing or reducing anxiety or distress.
To be diagnosed with OCD, any of these 4 symptoms is necessary, and Lestat, arguably, displays all of them, so he is diagnosed with OCD by me.
7.0 Trauma- and Stressor-Related Disorders
7.1 Post-Traumatic Stress Disorder (PTSD):
PTSD is a disorder that develops in some people who have experienced a shocking, scary, or dangerous event. There are several criteria to be diagnosed with it.
Lestat displays 3 symptoms out of 4 for exposure to actual or threatened death, and serious injury:
Directly experiencing the traumatic event: Claudia and Louis attempted to kill him.
Witnessing, in person, the event as it occurred to others: He was there to watch the Trial and he witnessed Claudia dying.
Learning that the traumatic event occurred to a close family member or close friend: He learned that Louis tried to harm himself.
Lestat displays 4 symptoms out of 5 for presence of intrusion symptoms associated with the traumatic event:
Recurrent, involuntary, and intrusive distressing memories of the traumatic event: He cannot get the death of Claudia out of his mind. He also still thinks about Louis harming himself.
Dissociative reactions (e.g., flashbacks) in which the individual feels or acts as if the traumatic event were recurring.
Intense or prolonged psychological distress at exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event.
Marked physiological reactions to internal or external cues that symbolize or resemble an aspect of the traumatic event.
Lestat’s PTSD is multifaceted, as there have been several different traumatic events that had shocked him and endangered him (e.g., Magnus, the Trial, S1.E7, the death of Nicki). According to Sam Reid, Claudia will haunt Lestat in S3, so we will see more of his reactions to his PTSD.
8.0 Feeding and Eating Disorders
8.1 Pica:
Pica is characterized by persistent eating of nonnutritive, nonfood substances over a period of at least 1 month. Which is, pretty much, seen in every vampire. It does not take a psychologist to diagnose vampires with Pica. They are Pica.
8.2 Avoidant/Restrictive Food Intake Disorder:
ARFID is characterized by an eating or feeding disturbance as manifested by the person avoiding certain foods. As can be seen in many episodes, Lestat constantly judges Louis for feeding only from animals instead of humans. Lestat prefers human blood only, making him a restrictive food intaker.
8.3 Binge Eating Disorder:
Binge Eating Disorder is characterized by recurrent episodes of binge eating.
Lestat displays 2 out of 2 symptoms for an episode of binge eating:
Eating, in a discrete period of time, an amount of food that is definitely larger than what most people would eat in a similar period of time under similar circumstances.
A sense of lack of control over eating during the episode.
In the song ‘Long Face’, Lestat talks about binge feeding after a breakup in which he eventually gains weight from the amount of blood he consumes. Do vampires get overweight? I don’t know, but that’s what he says, so I diagnose him with Binge Eating Disorder.
9.0 Disruptive, Impulse-Control, and Conduct Disorders
9.1 Oppositional Defiant Disorder:
Oppositional Defiant Disorder is a pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness lasting at least 6 months.
Lestat displays 6 symptoms out of 8 for Oppositional Defiant Disorder:
Often loses temper: e.g. when playing chess with Claudia, when Claudia came back and he beat up Louis.
Is often touchy or easily annoyed.
Is often angry and resentful.
Often deliberately annoys others.
Often blames others for his or her mistakes or misbehavior.
Has been spiteful or vindictive at least twice within the past 6 months.
Therefore, it can be easily said that Lestat is not a bad person, he is just mentally ill.
9.2 Intermittent Explosive Disorder:
Intermittent Explosive Disorder is characterized by recurrent behavioral outbursts representing a failure to control aggressive impulses.
Lestat displays 2 symptoms out of 2 for failure to control aggressive impulses:
Verbal aggression or physical aggression toward property, animals, or other individuals: Going crazy after losing in chess, choking Claudia, beating up Louis.
Three behavioral outbursts involving damage or destruction of property and/or physical assault involving physical injury against animals or other individuals occurring within a 12-month period: It possibly happens more for Lestat.
10.0 Personality Disorders
10.1 Borderline Personality Disorder:
BPD is a pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, beginning by early adulthood and present in a variety of contexts.
Lestat displays 7 symptoms out of 9 for Borderline Personality Disorder:
Frantic efforts to avoid real or imagined abandonment: He does everything in order to keep Louis.
A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation.
Identity disturbance: markedly and persistently unstable self-image or sense of self.
Impulsivity in at least two areas that are potentially self-damaging: Cheating on partners, money spending, substance abuse can be seen in Lestat.
Affective instability due to a marked reactivity of mood.
Chronic feelings of emptiness.
Inappropriate, intense anger or difficulty controlling anger (as mentioned in Disruptive & Impulse-Control Disorders).
As guessed by many people, BPD is the disorder that Lestat relates to the most. He obviously displays a lot of symptoms of it and therefore easily can be diagnosed with it by any professional.
10.2 Histrionic Personality Disorder:
Histrionic Personality Disorder is characterized by a pervasive pattern of excessive emotionality and attention seeking, beginning by early adulthood and present in a variety of contexts.
Lestat displays 6 symptoms out of 8 for Histrionic Personality Disorder:
Is uncomfortable in situations in which he or she is not the center of attention.
Interaction with others is often characterized by inappropriate sexually seductive or provocative behavior.
Displays rapidly shifting and shallow expression of emotions.
Consistently uses physical appearance to draw attention to self.
Shows self-dramatization, theatricality, and exaggerated expression of emotion.
Considers relationships to be more intimate than they actually are.
Lestat can easily be seen as ‘the life of the party’ and if he is not the center of the attention, you best believe he will do something about it. He displays enough symptoms to be diagnosed with HPD.
11.0 Paraphilic Disorders
11.1 Voyeuristic Disorder:
Voyeuristic Disorder is characterized by recurrent and intense sexual arousal from observing an unsuspecting person who is naked, in the process of disrobing, or engaging in sexual activity, as manifested by fantasies, urges, or behaviors.
In S1.E1 we see that Lestat likes watching Louis having sex with another woman. Louis asks Lestat, ‘That’s your thing? You like to watch?’.
11.2 Sexual Masochism Disorder:
Sexual Masochism is recurrent and intense sexual arousal from the act of being humiliated, beaten, bound, or otherwise made to suffer, as manifested by fantasies, urges, or behaviors.
When Dreamstat comes back to Louis, there is a scene in which Lestat provokes Louis by saying ‘Kill me again.’, and he laughs as Louis hits him, chokes him, and although that is Louis’ dream of Lestat, I think it’s safe to say Lestat had enjoyed that kind of behavior before. When Louis takes Lestat back, we also see how beaten up Lestat is, and it happens after they have sex.
Part II: Psychological Theories
1.0 Social Exchange Theory:
Social Exchange Theory is a concept based on the idea that social behavior is the result of an exchange process. According to this theory, people weigh the potential benefits and risks of their social relationships. When the risks outweigh the rewards, they will terminate or abandon the relationship. The purpose of this exchange is to maximize benefits and minimize costs.
Lestat lives his life by this theory. He is often driven by his desires and passions. He craves companionship and love but also seeks dominance and control over others.
Costs:
Emotional Turmoil: Lestat's intense relationships often lead to emotional conflicts and suffering, both for him and his companions.
Risk of Rejection: His desire for deep connections makes him vulnerable to rejection and betrayal, as seen with Louis.
Loneliness: Despite seeking companionship, Lestat frequently finds himself isolated due to his nature and actions.
Rewards:
Companionship: Lestat values the presence of others, particularly those who can understand his nature and share his experiences.
Power and Control: He often derives satisfaction from having power over others, which boosts his sense of significance and dominance.
Excitement and Adventure: Lestat’s relationships often bring new experiences and adventures, which he craves as part of his rebellious spirit.
His interactions are driven by the pursuit of rewards such as companionship, power, and adventure, while also dealing with the costs of emotional turmoil, conflict, and isolation.
2.0 Maslow’s Hierarchy of Needs:
This psychological theory posits that human motivations are structured in a hierarchy, ranging from basic physiological needs to self-actualization. Lestat’s actions and motivations often reflect his quest to fulfill these needs, from the basic physiological requirement for blood to his pursuit of self-actualization through personal growth and creative expression.
Needs:
Physiological:
Vampiric Thirst: As a vampire, Lestat's primary physiological need is the consumption of blood. This need drives many of his actions, ensuring his survival.
Immortality: Unlike humans, Lestat doesn't need food, water, or shelter in the traditional sense. His physiological need is centered around obtaining blood and ensuring his physical survival as an immortal being.
Safety:
Physical Safety: Lestat seeks to protect himself from threats, both from humans and other vampires. This includes avoiding vampire hunters and rival vampires who may wish to harm him.
Existential Safety: Lestat grapples with the existential nature of his immortality and seeks to find stability in his long existence. This often involves creating and maintaining secure environments where he can exist without threat.
Love and Belongingness:
Companionship: Lestat's relationships with Louis, Claudia, and others highlight his deep need for companionship and belonging. Despite his often domineering nature, Lestat craves intimate connections.
Vampire Family: His creation of a vampire family with Louis and Claudia is an attempt to fulfill his need for love and belonging. He seeks to create a close-knit group that can understand and share his experiences.
Esteem:
Respect and Recognition: Lestat desires recognition and respect from both humans and vampires. His flamboyant and rebellious behavior often serves as a way to assert his presence and command attention.
Self-Esteem: Lestat struggles with his self-esteem, oscillating between grandiosity and self-doubt. He seeks validation through his actions and the admiration of others.
Self Actualization:
Personal Growth: Lestat's journey throughout the series is marked by his pursuit of knowledge, self-discovery, and personal growth. He constantly seeks to understand his place in the world and the meaning of his existence.
Art and Music: Lestat's involvement in the arts, particularly his passion for music, is an expression of his self-actualization. These creative pursuits allow him to explore and express his individuality and inner world.
Transcendence: At times, Lestat seeks experiences that go beyond his own existence, exploring the metaphysical and spiritual aspects of being a vampire. This includes his encounters with ancient vampires and other supernatural beings.
3.0 The Myers-Briggs Test (MBTI):
The MBTI categorizes personalities into 16 types based on four dichotomies:
Extraversion (E) vs. Introversion (I)
Extraversion (E): Lestat is highly extraverted. He thrives on interaction with others and seeks out social engagement, whether with humans or other vampires. He loves being the center of attention, often drawing others to him with his charm and charisma.
Sensing (S) vs. Intuition (N)
Intuition (N): Lestat is intuitive, often looking beyond the surface to understand deeper meanings and possibilities. He is driven by his curiosity and desire for new experiences and knowledge.
Thinking (T) vs. Feeling (F)
Feeling (F): Although Lestat can be calculating and strategic, his decisions are often influenced by his emotions and personal values. He experiences intense emotions and is deeply affected by his relationships and experiences.
Judging (J) vs. Perceiving (P)
Perceiving (P): Lestat is spontaneous, adaptable, and often prefers to keep his options open. He is not one for strict plans or routines and enjoys the freedom to explore and act on impulse.
Lestat's personality aligns well with the ENFP type in the Myers-Briggs framework. His extraversion, intuition, emotional depth, and spontaneous nature define his character and drive his actions.
4.0 Freud’s Ego Psychology:
Freud's model of the psyche is composed of three main elements: the Id, the Ego, and the Superego. Each of these components plays a critical role in shaping an individual's actions and interactions. Through this psychology, Lestat can be understood as a dynamic interplay between his Id-driven desires, his Ego's attempts to navigate reality, and his Superego's moral contemplations.
The Id:
Desires and Instincts: Lestat's Id is strongly represented by his vampiric desires and instincts. His need for blood, thrill-seeking behavior, and hedonistic pursuits are driven by the Id's demand for immediate gratification. Lestat’s frequent indulgence in bloodlust, his desire for power, and his pursuit of pleasure without concern for consequences highlight his Id-driven actions. His transformation into a vampire amplifies these primal desires.
The Ego:
Reality Principle: Lestat’s Ego attempts to balance his powerful Id with the demands of reality. This is evident in his strategic thinking and ability to navigate the complexities of human and vampire societies. Lestat's efforts to create a successful career as a rock star and his ability to form and maintain complex relationships (despite their tumultuous nature) demonstrate his Ego at work. He often calculates his actions to achieve his desires while managing external realities.
The Superego:
Moral Conscience: Lestat’s Superego is less dominant than his Id, but it is still present. His reflections on morality, guilt, and his existential musings show the influence of his Superego. Lestat's internal conflicts and occasional guilt over his actions indicate the presence of his Superego. His moments of introspection, particularly when he questions the morality of his vampiric existence, highlight this aspect of his psyche.
Lestat experiences significant internal conflicts between his Id, Ego, and Superego. His hedonistic desires often clash with his moments of moral contemplation and the need to adapt to reality. He often projects his own desires and frustrations onto others, such as Louis and Claudia. His complex relationships involve elements of transference, where he relives past traumas and desires through his interactions with them.
5.0 Jung’s Archetypes:
Jung's theory of archetypes suggests that there are universal, archaic symbols and images that derive from the collective unconscious. These archetypes manifest in literature and myths, often embodying fundamental human experiences and traits.
The Self:
Integration and Wholeness: Throughout the series, Lestat's journey can be seen as a quest for integration and self-understanding. He seeks to reconcile his various aspects and achieve a sense of wholeness.
The Shadow:
Dark Aspects: Lestat's Shadow includes his violent tendencies, selfish desires, and the darker aspects of his vampiric nature. He often grapples with these parts of himself, leading to internal conflict and moral ambiguity.
The Anima:
Feminine Qualities: Lestat's Anima is reflected in his deep emotional connections and his capacity for empathy and love, despite his often ruthless behavior. His relationships with Louis and Claudia reveal his nurturing and protective sides.
The Persona:
Public Face: Lestat's Persona is highly cultivated, presenting himself as charismatic, charming, and flamboyant. He is a performer both literally (as a rock star) and metaphorically, often masking his deeper, more troubled self.
The Hero:
Quest and Challenges: Lestat embodies the Hero archetype through his constant quest for meaning, adventure, and self-discovery. He faces numerous challenges and often acts as a catalyst for change in the vampire world.
The Trickster:
Mischief and Chaos: Lestat often plays the role of the Trickster, causing disruption and challenging societal norms. His rebellious nature and tendency to create chaos reflect this archetype.
His public Persona, the dark Shadow, the nurturing Anima, the heroic quest, the Trickster's chaos, and the journey towards the Self all contribute to his multifaceted character.
6.0 Attachment Theory:
Attachment theory, developed by John Bowlby and later expanded by Mary Ainsworth, examines how early relationships with caregivers shape an individual's patterns of attachment and behavior in later relationships.
Lestat's early life as a human was marked by complex relationships with his family, particularly his mother, Gabrielle. His father was neglectful and abusive, while his mother was more supportive but distant due to her own struggles. These early experiences likely influenced Lestat's attachment style, contributing to his complex and often tumultuous relationships later in life.
Disorganized Attachment: Lestat exhibits traits of disorganized attachment, characterized by a mix of anxious and avoidant behaviors. His relationships are marked by intense emotions, fear of abandonment, and difficulty maintaining stable bonds. This theory highlights his struggles with intimacy, fear of abandonment, and need for control.
7.0 Social Identity Theory:
This theory explores how individuals derive a sense of identity and self-esteem from their membership in social groups, and how these group dynamics influence intergroup behavior.
Social Categorization:
Vampire Identity: Lestat categorizes himself primarily as a vampire, which becomes a core aspect of his identity. This categorization distinguishes him from humans and other supernatural beings. Lestat's transformation into a vampire and his subsequent embrace of vampiric traits and behaviors mark his entry into this distinct social category. He frequently identifies himself as part of the vampire world, even when challenging its norms.
Social Identification:
Group Membership: Lestat identifies strongly with the vampire community, despite often rebelling against its rules and leaders. His identity as a vampire shapes his actions, relationships, and self-perception. Lestat’s relationships with other vampires, such as Louis, Claudia, Armand, and even ancient vampires like Akasha, reflect his deep connection to the vampire identity. His desire to understand and sometimes reshape the vampire world shows his commitment to this group.
Social Comparison:
Ingroup vs. Outgroup: Lestat often compares himself and his vampire companions to humans and other supernatural entities. This comparison reinforces his sense of superiority and uniqueness.
His categorization as a vampire, identification with the vampire community, and comparison with humans and other vampires shape his actions and self-perception. The intragroup dynamics, including power struggles, status seeking, and identity crises, further highlight the complexities of his social identity.
8.0 Five Factor Model of Personality:
The Five-Factor Model includes five broad dimensions of personality:
Openness to Experience:
High Openness: Lestat exhibits high levels of openness. He is curious about the world, adventurous, and willing to explore new experiences, both as a vampire and in his human endeavors.
Conscientiousness:
Low to Moderate Conscientiousness: Lestat demonstrates lower levels of conscientiousness. He often acts impulsively and disregards conventional norms or plans.
Extraversion:
High Extraversion: Lestat is highly extraverted. He thrives on social interaction, enjoys being the center of attention, and is energized by engaging with others.
Agreeableness:
Low to Moderate Agreeableness: Lestat shows varying levels of agreeableness. While he can be charming and charismatic, his actions often reflect self-interest and a lack of empathy.
Neuroticism:
Moderate to High Neuroticism: Lestat exhibits moderate to high levels of neuroticism. He frequently experiences emotional turmoil, existential angst, and inner conflict.
Lestat’s personality, as analyzed through the Five-Factor Model, reveals a complex character with high openness and extraversion, but lower conscientiousness and agreeableness, alongside significant neuroticism. These traits contribute to his charismatic, adventurous, and often tumultuous nature.
In conclusion, I diagnosed Lestat with 18 mental disorders (according to DSM-V) and analyzed his personality through 8 different psychological theories. I don't necessarily say that I am right, but given the psychology degree I have, I am pretty much sure of what I have concluded here with this.
Much love,
Zenith
#lestat de lioncourt#iwtv lestat#the vampire lestat#rockstar lestat#amc iwtv#iwtv#iwtv s2#iwtv season 2#interview with the vampire#psychology#mental health#diagnosis
39 notes
·
View notes
Text
Do you know this (noncanon) ADHD character?

Evidence below the cut! (As in, an entire DSM-V diagnosis xD)
Submitter provided the following diagnosis:
HC, there is a beautiful analysis by @rena-rain as well as many posts all over the internet; over all it is a common headcanon in the fandom. out of the dmsv traits she displays:
a. Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or during other activities (e.g., overlooks or misses details, work is inaccurate).
b. Often has difficulty sustaining attention in tasks or play activities (e.g., has difficulty remaining focused during lectures, conversations, or lengthy reading).
c. Often does not seem to listen when spoken to directly (e.g., mind seems elsewhere, even in the absence of any obvious distraction).
d. Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., starts tasks but quickly loses focus and is easily sidetracked).
e. Often has difficulty organizing tasks and activities (e.g., difficulty managing sequential tasks; difficulty keeping materials and belongings in order; messy, disorganized work; has poor time management; fails to meet deadlines).
f. Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (e.g., schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers).
g. Often loses things necessary for tasks or activities (e.g., school materials, pencils, books, tools, wallets, keys, papenwork, eyeglasses, mobile telephones).
h. Is often easily distracted by extraneous stimuli (for older adolescents and adults, may include unrelated thoughts).
i. Is often forgetful in daily activities (e.g., doing chores, running errands; for older adolescents and adults, returning calls, paying bills, keeping appointments).
a. Often fidgets with or taps hands or feet or squirms in seat.
b. Often leaves seat in situations when remaining seated is expected (e.g., leaves his or her place in the classroom, in the office or other workplace, or in other situations that require remaining in place).
c. Often runs about or climbs in situations where it is inappropriate. (Note: In adolescents or adults, may be limited to feeling restless.)
d. Often unable to play or engage in leisure activities quietly.
e. Is often “on the go,” acting as if “driven by a motor” (e.g., is unable to be or uncomfortable being still for extended time, as in restaurants, meetings; may be experienced by others as being restless or difficult to keep up with).
f. Often talks excessively.
g. Often blurts out an answer before a question has been completed (e.g., completes people’s sentences; cannot wait for turn in conversation).
h. Often has difficulty waiting his or her turn (e.g., while waiting in line).
i. Often interrupts or intrudes on others (e.g., butts into conversations, games, or activities; may start using other people’s things without asking or receiving permission; for adolescents and adults, may intrude into or take over what others are doing).
Several inattentive or hyperactive-impulsive symptoms are present in two or more settings (e.g., at home, school, or work; with friends or relatives; in other activities).
D. There is clear evidence that the symptoms interfere with, or reduce the quality of, social, academic, or occupational functioning.
only feature not shown is evidence of it happening before 12 YO since the show starts when she's 13 i think?
in addition she also presents a classic case of limerance towards adrien prior to actually falling in love with him, and on-screen hiperfocus episodes, as well as a hiiiigh possibility of comorbid GAD (analysis also by gentil-minou) and a few signs that could point towards comorbid ASD
#poll#noncanon adhd character#miraculous ladybug#mlb#marinette dupain-cheng#marinette dupain cheng#ml ladybug#ml marinette#youre so right submitter. shes so adhd#i havent watched mlb in a long time i should catch up#im also so impressed by you straight up diagnosing her#that is some SOLID evidence
36 notes
·
View notes
Text
A Look at Nightcord at 25:00 and Neurodivergency (Part 3)
Follow up to part 1 and 2
Warning for r-slur in criteria from DSM
Shinonome Ena

Shinonome Ena is the artist of the group, she cam appear easy to anger or teasable but she's also very caring to her friends. What she wants the most is for her art to get recognized and while she enjoys the attention she gets from her selfies, she'd still prefer for her art to get attention more than or over her selfies. Now let's look at her symptoms:
Attention-Deficit/Hyperactivity Disorder
ADHD for short is a disability charactherized by inability focus especially when needed or the task is not interesting to the indivual and/or hyperactivity such as inability remain still and impulsivity to sum it up roughly. Now let's look at the symptoms:
A. A persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development, as characterized by (1) and/or (2):
Inattention: Six (or more) of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic / occupational activities: Note: The symptoms are not solely a manifestation of oppositional behavior,defiance, hostility, or failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required. a. Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or during other activities (e.g., overlooks or misses details, work is inaccurate). b. Often has difficulty sustaining attention in tasks or play activities (e.g., has difficulty remaining focused during lectures, conversations, or lengthy reading). c. Often does not seem to listen when spoken to directly (e.g., mind seems elsewhere, even in the absence of any obvious distraction). d. Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., starts tasks but quickly loses focus and is easily sidetracked). e. Often has difficulty organizing tasks and activities (e.g., difficulty managing sequential tasks; difficulty keeping materials and belongings in order; messy, disorganized work; has poor time management; fails to meet deadlines). f. Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (e.g., schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers). g. Often loses things necessary for tasks or activities (e.g., school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones). h. Is often easily distracted by extraneous stimuli (for older adolescents and adults, may include unrelated thoughts). i. Is often forgetful in daily activities (e.g., doing chores, running errands; for older adolescents and adults, returning calls, paying bills, keeping appointments).
Hyperactivity and impulsivity: Six (or more) of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/ occupational activities: Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or a failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required. a. Often fidgets with or taps hands or feet or squirms in seat. b. Often leaves seat in situations when remaining seated is expected (e.g., leaves his or her place in the classroom, in the office or other workplace, or in other situations that require remaining in place). c. Often runs about or climbs in situations where it is inappropriate. (Note: In adolescents or adults, may be limited to feeling restless.) d. Often unable to play or engage in leisure activities quietly. e. Is often “on the go,” acting as if “driven by a motor” (e.g., is unable to be or uncomfortable being still for extended time, as in restaurants, meetings; may be experienced by others as being restless or difficult to keep up with). f. Often talks excessively. g. Often blurts out an answer before a question has been completed (e.g., completes people’s sentences; cannot wait for turn in conversation). h. Often has difficulty waiting his or her turn (e.g., while waiting in line). i. Often interrupts or intrudes on others (e.g., butts into conversations, games, or activities; may start using other people’s things without asking or receiving permission; for adolescents and adults, may intrude into or take over what others are doing).
B. Several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years. C. Several inattentive or hyperactive-impulsive symptoms are present in two or more settings (e.g., at home, school, or work; with friends or relatives; in other activities).
Now let's look at Ena's symptoms:
1a- Honestly I don't remember if this ever happened, especially in school work since it's not mentioned too much and Ena doesn't seem to help around the house a lot however if there were any instances of it happening, please do let me know.
1b- Ena does struggle with sustaining attention, even at her passion; art. Often getting artblock and struggling to draw something she doesn't like as much.
1c-This doesn't seem to be present.
1d-Ena works mostly with her own freedom and niigo and I don't remember much on how her school work goes so I'm not sure on how I could judge this symptom.
1e- Ena's workspace is indeed often messy and have often even missed deadlines on niigo work with one time Kanade not waiting for Ena anymore.
1f-Ena seems to struggle with this, even with art even if she manages to finish and she doesn't often seem to do schoolwork so it could be related however I'm not too sure.
1g- If i remember correctly she lost a few items for drawing if I remember correctly however this doesn't happen too often.
1h-This does seem to happen, especially when something worrying happens like a niigo member not feeling well, she struggles to focus on her artwork or if I remember correctly even school in My Footprints Your Destination event however it's been a while since I read a lot of this so i might be wrong or this might be treated more like a specific instance.
1i- She does often seem to be late to school and its activities but other than that I haven't seen that much.
2f- Ena does have moments where she does talk a lot however rest of this criteria is hard to tell from 2D Models in game.
B- Most of Ena's past scenes focus on her trauma so I'm not sure if these were present however that seems to be the case. On top of that, ICD states ADHD can sometimes be developed later in life too however that's a controversial topic.
C-I focused mostly on the niigo work in this review so I'm also not sure if it's present however knowing her personality and struggles, it like is.
So Ena does seem to show some symptoms however since I don't remember or know much about her school life but she indeed shows some symptoms however it's debatable whether she could actually be diagnosed or not but I of course can see why people would see her as such if they do.
Some other common traits Ena shows are:
easily frustrated
really bad at time management
Dyslexia
A disability under Specific Learning Disorder in the DSM is charactherized by difficulties reading, writing and spelling to sum it up. More specifically the symptoms are:
Inaccurate or slow and effortful word reading (e.g., reads single words aloud incorrectly or slowly and hesitantly, frequently guesses words, has difficulty sounding out words).
Difficulty understanding the meaning of what is read (e.g., may read text accurately but not understand the sequence, relationships, inferences, or deeper meanings of what is read).
Difficulties with spelling (e.g., may add, omit, or substitute vowels or consonants).
Difficulties with written expression (e.g., makes multiple grammatical or punctuation errors within sentences; employs poor paragraph organization; written expression of ideas lacks clarity).
Now Ena doesn't seem to show any of these as far as I remember however I can see why dyslexic people would headcanon her as such, especially with her being an artist and many people with learning disabilities being good at creative activities.
Bipolar, Cyclothymic and Major Depressive Disorder
Bipolar Disorder which is often shortened as BD, BP or Bipolar is a disorder consisteng of high and/or low mood episodes called manic or hypomanic and depressive to put it roughly. There are 2, or 3 in some sources that include cyclothymia, of this disorder with Bipolar I having at least one manic or mixed (major depressive and manic) episode and Bipolar II having at least one hypomanic and one major depressive episode. if there's no (hypo)manic episode present and only a major depressive one, it could be diagnosed as Major Depressive Disorder or MDD instead so now let's take a closer look at the symptoms and these episodes:
(Hypo)Manic episode:
Inflated self-esteem or grandiosity.
Decreased need for sleep (e.g., feels rested after only 3 hours of sleep).
More talkative than usual or pressure to keep talking.
Flight of ideas or subjective experience that thoughts are racing.
Distractibility (i.e., attention too easily drawn to unimportant or irrelevant external stimuli), as reported or observed.
Increase in goal-directed activity (either socially, at work or school, or sexually) or psychomotor agitation.
Excessive involvement in activities that have a high potential for painful consequences (e.g., engaging in unrestrained buying sprees, sexual indiscretions, or foolish business investments).
C. The mood disturbance is sufficiently severe to cause marked impairment in social or occupational functioning or to necessitate hospitalization to prevent harm to self or others, or there are psychotic features. (For it to be considered a manic episode rather than hypomanic.)
Major depressive episode:
Depressed mood most of the day, nearly every day, as indicated by either subjective report (e.g., feels sad, empty, or hopeless) or observation made by others (e.g., appears tearful). (Note: In children and adolescents, can be irritable mood.)
Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day (as indicated by either subjective account or observation).
Significant weight loss when not dieting or weight gain (e.g., a change of more than 5% of body weight in a month), or decrease or increase in appetite nearly every day. (Note: In children, consider failure to make expected weight gain.)
Insomnia or hypersomnia nearly every day.
Psychomotor agitation or retardation nearly every day (observable by others, not merely subjective feelings of restlessness or being slowed down).
Fatigue or loss of energy nearly every day.
Feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day (not merely self-reproach or guilt about being sick).
Diminished ability to think or concentrate, or indecisiveness, nearly every day (either by subjective account or as observed by others).
Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.
For cyclothymic disorder:
A. For at least 2 years (at least 1 year in children and adolescents) there have been numerous periods with hypomanic symptoms that do not meet criteria for a hypomanic episode and numerous periods with depressive symptoms that do not meet criteria for a major depressive episode. B. During the above 2-year period (1 year in children and adolescents), Criterion A symptoms have been present for at least half the time and the individual has not been without the symptoms for more than 2 months at a time. C. Criteria for a major depressive, manic, or hypomanic episode have never been met.
Now let's look at Ena's symptoms:
(Hypo)mania:
1-This is present, especially upon recieving supply however so some might attribute it to another disability which I'll cover later.
2- This symptom isn't present, she seems to need a lot of sleep most of the time.
3-She also again seems to be more talkative as I already covered in ADHD section, especially at times.
4-She has times where she feels like she suddenly get lots of ideas too if I remember correctly.
5-I don't exactly remember this but as I already covered in ADHD section, she can get distracted rather easily at some things?
6-She also gets really determined to draw or get better at it at times unlike others where she seems really discouraged about it.
7-She can impulsively buy things from what I've seen but this too can be attributed to something else I'll mention later.
C: These don't cause marked impairment, harm to anyone besides symptom 7 and she doesn't experience psychosis either.
Ena shows almost all the symptoms however these constitute for a hypomanic episode rather than a manic one so Bipolar II is still in question so let's look at her depressive symptoms:-
1-This has been present as we've seen many times especially in her focus events.
2-Again this has happened, both in main story and her focus events, especially in pale color event.
3-This hasn't been mentioned much but it seems not to be present.
4-She does experience hypersomnia nearly everyday it seems from the stories, sometimes even only through 1 am to 7 am.
5-Once again this is hard to inspect from 2D models.
6-She seemed low on energy most of the time during these episodes too.
7-This is also present, especially on her low times, ESPECIALLY when she doesn't reciever the supply she needs.
8-She does become really indecisive at times, especially on low moods if I remember correctly.
9-She does experience suicidal ideation as indicated in many stories like the main story where she says she indeed wants to disappear.
She does fit the diagnostic criteria for a major depressive episode too so she could indeed be seen as bipolar or more specifically bipolar and I can see why someone would see MDD just looking at the depressive episodes as well, the only issue is if these are present for long enough to constitude for episodes which brings me to cyclothymia which Ena has been like this for years however she does meet the diagnostic criteria for either episode so it's likely not cyclothymia.
Other common traits of bipolar and MDD seen in Ena:
poor judgement of others
rapid mood shifts
impulsive
has difficulty finding the motivation to clean or do other household tasks
sometimes probably feels like she's not really depressed, that maybe she's just lazy
experiences a restlessness occasionally and has to move around physically, such as pacing or spinning around in a chair or changing clothes
sometimes can get moody or snappy
sometimes feels very numb, like she has no feelings at all
seems to have a skewed perception of time
Social Anxiety Disorder
Also known as Socialphobia, SAD or social anxiety for short is a disorder charactherized by anxiety, often intense, in social situation to sum it up.
Let's look at the symptoms again:
"A. Marked fear or anxiety about one or more social situations in which the individual is exposed to possible scrutiny by others. Examples include social interactions (e.g., having a conversation, meeting unfamiliar people), being observed (e.g., eating or drinking), and performing in front of others (e.g., giving a speech).
Note: In children, the anxiety must occur in peer settings and not just during interactions with adults.
B. The individual fears that he or she will act in a way or show anxiety symptoms that will be negatively evaluated (i.e., will be humiliating or embarrassing: will lead to rejection or offend others).
C. The social situations almost always provoke fear or anxiety.
Note: In children, the fear or anxiety may be expressed by crying, tantrums, freezing, clinging, shrinking, or failing to speak in social situations.
D. The social situations are avoided or endured with intense fear or anxiety.
E. The fear or anxiety is out of proportion to the actual threat posed by the social situation and to the sociocultural context.
F. The fear, anxiety, or avoidance is persistent, typically lasting for 6 months or more."
Rest are about it causing distress to indivual and is not better explained by another disability.
Let's look at Ena's symptoms:
To cut it short, Ena does seem to do well in most social situations, interacting with others well and not having anxiety about embarassing herself however does have about people looking down on her, she also doesn't go out that often though so it's hard to judge her symptoms.
Generalized Anxiety Disorder
Or GAD for short is a disorder charactherized by anxiety in various things that might occur in daily life.
The symptoms are:
"A. Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance).
B. The individual finds it difficult to control the worry.
C. The anxiety and worry are associated with three (or more) of the following six symptoms (with at least some symptoms having been present for more days than not for the past 6 months); Note: Only one item is required in children.
Restlessness or feeling keyed up or on edge.
Being easily fatigued.
Difficulty concentrating or mind going blank.
Irritability.
Muscle tension.
Sleep disturbance (difficulty falling or staying asleep, or restless, unsatisfying sleep)."
Now onto Ena:
A.Ena does seem to find daily activities stressing or worrying as shown in stories a few times however judging that as anxiety or not is mostly up to interpetation.
B. Ena does struggle to control these worries
C1, C2 as being easily tired in these worrisome situations, maybe C3 and C4 can be seen in Ena generally; especially C4.
So some may see Ena as having GAD however it is mostly up to interpatation.
Some other GAD traits Ena shows are:
avoids events and situations which may trigger my anxiety
had anxiety attacks if I remember correctly
often worry about the future
when she's stressed, she can become snappy with others
constantly worries about the quality of her performances for niigo
Obsessive-Compulsive Disorder
OCD for short is a disorder charactherized by either obsessions, compulsions or both. Obsessions in this case refer to intrusive aka unwanted thoughts and compulsions to reduce anxiety caused by them. Intrusive thoughts can be a number of things like "What if my family gets sick", "what if i hurt my brother" or "my pet" and compulsions might be directly related to this such as compulsive hand-washing, hiding the sharp objects or avoiding being near your brother or pets to avoid "hurting" them or sometimes unrelated like "i have to flip the light switch 10 times exactly so my brother won't die". It's a complex disorder with many different characteristics and its own spectrum of disabilities however this is diagnostic criteria with either obsessions or compulsions taking at least one hour out of your day to be diagnosed.
Now onto Ena, some could see her obsessions as being throughts about being inadequate and her compulsions as needing to keep drawing since she often said "i need to keep drawing, drawing, drawing" back to back in stories or perhaps drawing is more than a passion and reduces other intrusive thoughts in their headcanon as well.
Other OCD traits Ena has are:
is constantly checking on things to make sure they’re working properly or are okay
sets higher standards for herself than she does for other people
can repeat herself a lot
had anxiety attacks
(Complex) Posttraumatic Stress Disorder
Or C/PTSD for short is a disorder quite literally in the name, it includes experiencing a traumatic event and many issues in your daily life in the aftermath.
Symptoms are: "A. Exposure to actual or threatened death, serious injury, or sexual violence in one (or more) of the following ways:
Directly experiencing the traumatic event(s).
Witnessing, in person, the event(s) as it occurred to others.
Learning that the traumatic event(s) occurred to a close family member or close friend. In cases of actual or threatened death of a family member or friend, the event(s) must have been violent or accidental.
Experiencing repeated or extreme exposure to aversive details of the traumatic event(s) (e.g., first responders collecting human remains: police officers repeatedly exposed to details of child abuse). Note: Criterion A4 does not apply to exposure through electronic media, television, movies, or pictures, unless this exposure is work related.
B. Presence of one (or more) of the following intrusion symptoms associated with the traumatic event(s), beginning after the traumatic event(s) occurred:
Recurrent, involuntary, and intrusive distressing memories of the traumatic event(s). Note: In children older than 6 years, repetitive play may occur in which themes or aspects of the traumatic event(s) are expressed.
Recurrent distressing dreams in which the content and/or affect of the dream are related to the traumatic event(s). Note: In children, there may be frightening dreams without recognizable content.
Dissociative reactions (e.g., flashbacks) in which the individual feels or acts as if the traumatic event(s) were recurring. (Such reactions may occur on a continuum, with the most extreme expression being a complete loss of awareness of present surroundings.) Note: In children, trauma-specific reenactment may occur in play.
Intense or prolonged psychological distress at exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event(s).
Marked physiological reactions to internal or external cues that symbolize or resemble an aspect of the traumatic event(s).
C. Persistent avoidance of stimuli associated with the traumatic event(s), beginning after the traumatic event(s) occurred, as evidenced by one or both of the following:
Avoidance of or efforts to avoid distressing memories, thoughts, or feelings about or closely associated with the traumatic event(s).
Avoidance of or efforts to avoid external reminders (people, places, conversations, activities, objects, situations) that arouse distressing memories, thoughts, or feelings about or closely associated with the traumatic event(s).
D. Negative alterations in cognitions and mood associated with the traumatic event(s), beginning or worsening after the traumatic event(s) occurred, as evidenced by two (or more) of the following:
Inability to remember an important aspect of the traumatic event(s) (typically due to dissociative amnesia and not to other factors such as head injury, alcohol, or drugs).
Persistent and exaggerated negative beliefs or expectations about oneself, others, or the world (e.g., “I am bad,” “No one can be trusted,” ‘The world is completely dangerous,” “My whole nervous system is permanently ruined”).
Persistent, distorted cognitions about the cause or consequences of the traumatic event(s) that lead the individual to blame himself/herself or others.
Persistent negative emotional state (e.g., fear, horror, anger, guilt, or shame).
Markedly diminished interest or participation in significant activities.
Feelings of detachment or estrangement from others.
Persistent inability to experience positive emotions (e.g., inability to experience happiness, satisfaction, or loving feelings).
E. Marked alterations in arousal and reactivity associated with the traumatic event(s), beginning or worsening after the traumatic event(s) occurred, as evidenced by two (or more) of the following:
Irritable behavior and angry outbursts (with little or no provocation) typically expressed as verbal or physical aggression toward people or objects.
Reckless or self-destructive behavior.
Hypervigilance.
Exaggerated startle response.
Problems with concentration.
Sleep disturbance (e.g., difficulty falling or staying asleep or restless sleep).
F. Duration of the disturbance (Criteria B, C, D, and E) is more than 1 month."
Now onto Ena:
a1-Ena's dad telling her she has no talent and will never be a proper artist seems to have traumatized her a lot.
b1- She often thinks that she's not enough or is not a good artist.
b3- She tends to dissociate often when she remembers these events and there are often flashback sequences to her dad telling her she doesn't have talent which I wasn't sure if it belongs to b1 or b3.
b4/5-She does seem disstressed whenever something reminding her of her dad telling she has no talent happens as well.
c1- She does her best to avoid the thoughts of that moment she asosicates with her trauma the most as well as
c2- She avoids dad whenever she can because of this as well.
d2- She constantly believes she's not good enough due to her father's words.
d3- She often blames her dad however she did sometimes blame on it her not being good enough too if I remember correctly.
d4- She's prone to anger and has negative or complicated feelings towards art in general
d5- Switched to night school because of her dad
e1- She's prone to anger, especially with even little things like being reminded of her dad or her dad mentioning art
e5- She can struggle concentrating when being reminded of those memories or especially when drawing
F- These have lasted for years
So while Ena's trauma is somewhat unusual, well not unusual actually since being told you're not good enough is traumatic many people but not as "extreme" as some people would expect, she still seems really affected and disstressed by it so it's reasonable that it caused some issues for her; one of these, people might see it as ptsd or cptsd among other things.
Besides that, common PTSD traits Ena shows are:
sometimes feels completely emotionally numb
experienced prolonged periods of sadness or hopelessness
is unable to keep up with my daily routine, such as going to work or school or doing chores around the home (especially school-wise here)
Hypersomnolence Disorder
Hypersomnolence Disorder or hypersomnia is a disorder causing an excessive need for sleep to sum it up. The symptoms are:
"A. Self-reported excessive sleepiness (hypersomnolence) despite a main sleep period lasting at least 7 hours, with at least one of the following symptoms:
Recurrent periods of sleep or lapses into sleep within the same day.
A prolonged main sleep episode of more than 9 hours per day that is nonrestorative (i.e., unrefreshing).
Difficulty being fully awake after abrupt awakening.
B. The hypersomnolence occurs at least three times per week, for at least 3 months"
If we look at Ena, A2 seems to be present the most with her sleeping most of the day. In criteria B, this seems to happen most of the time with Ena's sleep schedule too so if these symptoms are not better explained by something else, she might have hypersomnia.
Borderline Personality Disorder
BPD for short, is a disorder categorized by marked impuslivity, instability in relationships and sense of self as well as fear of abandonment to cut it short.
Symptoms are:
Frantic efforts to avoid real or imagined abandonment. (Note: Do not include suicidal or self-mutilating behavior covered in Criterion 5.)
A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation.
Identity disturbance: markedly and persistently unstable self-image or sense of self.
Impulsivity in at least two areas that are potentially self-damaging (e.g., spending, sex, substance abuse, reckless driving, binge eating). (Note: Do not include suicidal or self- mutilating behavior covered in Criterion 5.)
Recurrent suicidal behavior, gestures, or threats, or self-mutilating behavior.
Affective instability due to a marked reactivity of mood (e.g., intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days).
Chronic feelings of emptiness.
Inappropriate, intense anger or difficulty controlling anger (e.g., frequent displays of temper, constant anger, recurrent physical fights).
Transient, stress-related paranoid ideation or severe dissociative symptoms."
Now let's look at Ena:
1.We don't see this much I'd assume she's quite afraid of Kanade leaving her.
2.When Mafuyu disappointed her, she did quickly switch between seeing her as a friend to hating her in the main story though she did touch a very sensitive place for her.
3.She doesn't quite know who she is, building her self esteem and identity on how well her art or selfies are recieved.
4.She's quite impulsive and if I remember correctly, does go on spending sprees however since this is still a game mostly for kids, there aren't any other given examples of her impulsivity.
5.Again since this is a family-friendly gamethis is a limited topic however; as we already covered, she's suicidal, gets thoughts and feelings about wanting disappear which should count as suicidal behavior.
6. Ena's mood is quick to shift, often to worse like hopelessnes or anger which is common in BPD.
7.Ena's whole sense of identity and self esteem relies on art so yes she does feel chronically empty as she would have nothing left if she lost art.
8. She's prone to anger as I've stated before.
9.When she's under stress, Ena sees the whole world as against her as well as well dissociating rather easily so this symptoms is present as well.
Many people see or headcanon Ena as having BPD and because she shows many symptoms and traits; it's undertsnadable why, especially why people see themselves in her.
Some other common BPD traits Ena shows are:
has trouble sleeping, or sleeps too much
has an extreme need for acceptance
very much lives in the moment, to the point where past actions don’t matter. How she judges others (and herself) depends entirely on what is happening right now.
is often defensive.
reacts very strongly to mundane experiences
can have a difficult time making decisions
often feels misunderstood, mistreated, or victimized
When she's upset, she's unable to calm down without help.
seems to have a favorite person (Kanade) which she heavily relies on for emotional support and approval
Histrionic Personality Disorder
HPD for short is a personality disorder characterized by excessive emotionality and attention seeking to sum it up roughly. The symptoms are:
Is uncomfortable in situations in which he or she is not the center of attention.
Interaction with others is often characterized by inappropriate sexually seductive or provocative behavior.
Displays rapidly shifting and shallow expression of emotions.
Consistently uses physical appearance to draw attention to self.
Has a style of speech that is excessively impressionistic and lacking in detail.
Shows self-dramatization, theatricality, and exaggerated expression of emotion.
Is suggestible (i.e., easily influenced by others or circumstances).
Considers relationships to be more intimate than they actually are.
Now onto Ena:
She's often uncomfortable when she's not the center of attention whether that be in their nightcord circle or among their fans.
This isn't present again once again as this is still a family-friendly game.
Her emotions do rapidly change however I'm not sure if I'd call them shallow.
She does pay attention her physical apperance and use selfies to draw attention to herself.
This is sort of true, especially in early story from what i remember but I also read the stories in Japanese and don't remember all of her speech style.
It is intense, "dramatic" however I'm not sure if that's intentional.
Actually is not and often stands her ground unles it's Kanade.
She was quick to warm up to all of Niigo and seems really friendly with others too, even in main story she considered Mafuyu to be a close friend while she didn't even consider a friend at all then.
Ena needs a lot of attention and does things that make her gather attention often like posting selfies, especially when she's struggling according to a 4koma and her emotions are often rapidly shifting so it's understandable why many would see her as hpd-coded too. However it's upto interpatation if her symptoms are hpd-coding or something else once again.
Other than that, some more HPD traits Ena has are:
Unless she's directly interacting with someone who is giving her attention, she feels unappreciated
is very enthusiastic and can be very exciting to be around
is a very open person and enjoys forming close bonds with others
often “fishes” for compliments
can be easily distressed by pictures of her that she finds unflattering
doesn’t respond well to criticism and can be incredibly distressed by it
Narcissistic Personality Disorder
Also called NPD for short is a personality disorder charactherized by a grandiose sense of self, need for admiration and lack of empathy however many of these are a coping mechanism to hide the person's actually really low self-esteem. So then, let's look at the symptoms:
Has a grandiose sense of self-importance (e.g., exaggerates achievements and talents, expects to be recognized as superior without commensurate achievements).
Is preoccupied with fantasies of unlimited success, power, brilliance, beauty, or ideal love.
Believes that he or she is “special” and unique and can only be understood by, or should associate with, other special or high-status people (or institutions).
Requires excessive admiration.
Has a sense of entitlement (i.e., unreasonable expectations of especially favorable treatment or automatic compliance with his or her expectations).
Is interpersonally exploitative (i.e., takes advantage of others to achieve his or her own ends).
Lacks empathy: is unwilling to recognize or identify with the feelings and needs of others.
Is often envious of others or believes that others are envious of him or her.
Shows arrogant, haughty behaviors or attitudes.
Now if we look at Ena:
1.She does seem to have a grandiose sense of self, wants to be recognized as great as she's dependent on it for her self-esteem.
2.She also seems to be preoccupied with fantasies of success such as her art recieving a lot of attention, as much as her selfies and being recognized as a great artist.
3.She wants to believe she's special once again because her self esteem is dependent on it. As stated by the name of her focus chapter in the main story; she doesn't want to be an ordinary person, she wants to be a special person with art many love.
4. Read back to the previous symptom, she requires excessive admiration to keep hher self-esteem at a high point. Whether that be niigo's praise, niigo fans praising her art or people praising her selfies, she need supply (as I mentioned before) from somewhere.
5.Honestly I don't remember this as stated here but please let me know if she had done something that indicated instant compliance with her requests at any point in story that I still haven't mentioned.
6. This also doesn't seem to be present.
7.She lacks empathy, affective empathy at least, as while she understood Mafuyu was in a hard situation, she didn't understood how she felt or why she couldn't just do x thing to help her situation though that ended up helping Mafuyu at times.
8.She's often envious of others, primarily Mafuyu as she has talent unlike Ena.
9.Most of what I said like wanting to be recognized as great or constantly admired are already haughty or arrogant attitudes.
Ena's incredibly NPD-coded, it's no wonder many people headcanon her as such. Ena's a good look into the inner world of a narcissist, she's not a manipulative abuser like people tend to paint narcissists as but instead a really insecure person who's dependent on painting herself as great and talented to maintain her self-esteem. Not to mention her first focus card featured narcissius flowers.
Some other common NPD traits Ena has are:
can have either low or high self-esteem. It depends on the people she's with and how they’re treating her at the time
tend to overestimate herself, which can often lead to disappointing herself
can become anxious and spiral into a depression if she doesn’t receive praise or admiration
hates being alone for too long
compares herself with others often, having no other means of defining herself unless she can use someone else as sort of a “measuring tape”
often feels incredibly misunderstood by others
likes to constantly be moving up and making progress and can become obsessive with it
is incredibly sensitive to criticism. Being criticized can leave me feeling humiliated, degraded, and empty and she event left art course due to criticism before
when upset, she tends to withdraw from others
is often depressed and/or anxious
This was all for Ena, this took some time haha but please do let me know if there's anything else you want me to look into, well then see you everyone at Mizuki aka the last part!
#プロセカ#project sekai#proseka#25時、ナイトコードで。#25 ji nightcord de#nightcord at 25:00#kanade yoisaki#yoisaki kanade#宵崎奏#asahina mafuyu#mafuyu asahina#akiyama mizuki#mizuki akiyama#ena shinonome#shinonome ena#暁山瑞希#東雲絵名#朝比奈まふゆ#mental health#neurodivergent#neurodiversity#depression#ocd#bpd#adhd#bipolar#hypomania#hypomanic#b#bipolar 2
14 notes
·
View notes
Text
Attention Deficit Hyperactivity Disorder – ADHD
Introduction:
Attention Deficit Hyperactivity Disorder – ADHD is one of the most common disorders encountered in children and most of the times the disorder is misunderstood and as a result is badly managed. ADHD can be described as a developmental disorder characterized by varying degrees of inattention, overactivity and impulsivity, arising in childhood. Sensory, language or motor impairment, mental retardation or emotional disturbance with deficits of behaviour and performance may also be seen in children suffering from ADHD.

Signs & Symptoms of ADHD -
ADHD begins in childhood. The symptoms of inattention and/or hyperactivity need to occur in a manner and degree which is inconsistent with the child’s current developmental level. That is, the child’s behavior is significantly more inattentive or hyperactive than that of his or her peers of a similar age.
Several symptoms must be present before age 12. This age requirement supports ADHD/ADD as a neurodevelopmental disorder. It is often difficult for adults (e.g., parents) to look retrospectively and establish a precise age of onset for a child.
A person can present with predominantly inattention, predominantly hyperactivity-impulsivity, or a combination of the two. To meet the diagnosis of ADHD and thereby be tagged as a child suffering from ADHD, the child must show at least 6 symptoms from the appropriate categories below:-
Symptoms of Inattention:
Failure to give close attention to details.
Makes careless mistakes in schoolwork, work, or other activities.
Difficulty in sustaining attention in tasks or play activities.
Does not listen when spoken to directly.
Fails to follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace.
Difficulty in organizing tasks and activities.
Avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort – such as schoolwork or homework.
Loses things necessary for tasks or activities quite often. (e.g., toys, school assignments, pencils, books, or tools)
Easily distracted by random stimuli.
Tends to be forgetful in daily activities – even those which he/she performs regularly (e.g., a routine appointment)
Symptoms of Hyperactivity/Impulsivity:
Hyperactivity
Fidgets with hands or feet or squirms in seat.
Leaves his/her seat in classroom or in other situations in which remaining seated is expected.
Runs about or climbs excessively in situations where it is inappropriate to do so.
Difficulty in playing or engaging in leisure activities quietly.
Is often “on the go” or often acts as if “driven by a motor”.
Talks excessively almost always.
Impulsivity
Blurts out answers before questions have been completed.
Difficulties in waiting for his/her turn.
Interrupts or intrudes on others. (e.g., butts into conversations or games)
For a child to be surely diagnosed with ADHD, symptoms should have persisted for at least 6 months. Some of these symptoms need to have been present as a child, at 12 years old or younger. The symptoms also must exist in atleast two separate settings (for example, at school and at home). The symptoms should be creating a significant impairment in social, academic or occupational functioning or relationships.
Causes of ADHD -
Genetic Factors – Some evidence exists that there is a possibility of a genetic factor which causes ADHD. Babies that are restless from birth have no time to be conditioned and hence there is a chance that genetic factor exists. Most parents of children with ADHD have a mild degree of an underlying psychological illness. Research has reported sociopathy and hysteria in the parents of hyperkinetic (hyperactive) children.
Intelligence - ADHD usually occurs in the mentally subnormal children. These children are bubbling with energy and cannot use their energy in the right way. They present with useless overactivity. Also children with exceptional intelligence may likewise present with ADHD. These children find studies easy and cannot settle down in class. Learning difficulties were an important part of ADHD though their exact relationship is not clear. However low IQ has been found in children with ADHD than for normal children of the same age.
Brain Damage – Any child who has suffered a brain damage is more likely to present with ADHD. In such cases, a detailed history with examination will help us diagnose ADHD due to a brain damage. Many children are mentally subnormal which depends on the degree of brain damage, though those having gross brain damage are preferably excluded from being classified as ADHD. The regions of the brain responsible for managing the attention capacity of the child receive reduced blood flow thus resulting in selective inattention and distribution i.e. inability to control and direct attraction to the demands of the task.
The Epileptic Child – Children suffering from epilepsy are often detected as suffering from ADHD. There is a chance of ADHD, Mental Subnormality and Epilepsy being in the same patient.
The Schizophrenic Child – Children suffering from Schizophrenia may also suffer from ADHD. But many a times the symptoms of ADHD are considered to be a part of Schizophrenia itself and hence the diagnosis of ADHD is masked.
Scholastic Difficulties – Childrenwith Scholastic Backwardness (especially at school) may manifest with Separation Anxiety or School Phobia and thus may also come up with symptoms of ADHD. Academic failures, peer rejection, low aspirations and goals, poor adaptation to school and poor attendance in school have all been known to be associated with ADHD.
Dietetic Factors - Vitamin deficiencies of Niacin and Pyridoxine play an important factor in ADHD. A child having a sugar-rich diet and with significant food allergies is considered to be more prone to suffering from ADHD. Hence various foodstuffs like cow’s milk, wheat flour, food dyes, citrus fruits etc are best to be avoided.
The Overprotective Mother – There are some mothers who usually cling to their child and will not let them go and play with other children or perform any other activity. These mothers have queer notions and are neurotic and bothered about the safety and security of their children. Their children are very precious to them as they are the only son or daughter for such mothers. This kind of overprotection eventually causes a bottling up of energy thereby manifesting as ADHD in the child.
The Disharmonious Family – In families where extensive tension anxiety and chaos prevails, the general atmosphere of tension automatically has an effect on the child thereby manifesting as ADHD. Economic deprivation, health problems, poor parental supervision, family conflict, low parental involvement and high rate of violence and alcoholism are associated with families having children suffering from ADHD.
Homoeopathic Approach in treating ADHD:
The fundamental problem in ADHD appears to be genetic. Homoeopathy looks for the underlying causes of ADHD thereby dealing with it at the root level.
ADHD treated in the conventional method is usually with the help of medical supplements which treat the inattentiveness, hyperactivity or the other behavioural problems that are seen in children with ADHD. Individual psychotherapy along with behaviour therapy is also advised during the treatment of ADHD. Homoeopathy helps in targeting the root cause of the problem and thereby deals with the causes of ADHD from within. The main aim and objective of Homoeopathy has always been to treat a person individually and relieve the patient of their symptoms from within.
Homoeopathy helps in treating the hyperactive and attention problems of an ADHD child. Homoeopathy thereby helps in improving the core nature of the child. Thus by means of which the ADHD child can continue his daily routine and lifestyle like any other normal child. The ADHD child can concentrate and pay better attention at school and at home.
The homoeopathic treatment for ADHD is based on an extensive case study of the patient with regards to his/her characteristic symptoms, genetic predisposition, and their mental state. The total time taken for the treatment differs from person to person depending on the duration, intensity and frequency of the suffering, maintaining causes, susceptibility and general health of the patient.
The goal of homoeopathic treatment for ADHD is to identify the main cause for the occurrence of symptoms. Homoeopathy then uses the body’s own mental powers to behave normally like other children. Children with ADHD have a lot of energy bottled up inside them. With the help of homoeopathy, the hyperactive behaviour of children with ADHD can be fine tuned and the health of the child can be enhanced. This leads to channelizing the energy of the child into healthy and productive work so as to let the child lead a normal life.
Children with ADHD need an outlet for all the pent up excess energy within them. This is possible through play therapies which involve making the child indulge in running and jumping in a playground, cycling, swimming etc. In case of an indoor setting, the child may be given a tub of sand to play with or a sandbag to punch on and remove his/her aggression or finger/hand painting also proves to be useful. Hence play therapies along with homoeopathy can help in streamlining all the excess energy into useful and positive fields.
Hence homoeopathic treatment along with cognitive, play therapies and behavioural training can help in improving the lifestyle of a child diagnosed with ADHD and thus let the child lead a normal life.
It is therefore advisable to choose Homoeopathy for treating your child’s hyperactive and inattentive behaviour, because it helps to deal with the behavioural troubles faced by the parents of an attention deficit hyperactive child thus letting the child live like any other normal child.
0 notes
Text
I'm getting really annoyed because there is too much to know and not enough time to learn it. So whatever, I'll just post all the diagnostic criteria according to UpToDate. But based on these criteria, I could have ADHD! This is really annoying. I'm just going to let the psych med NP take care of it. But anyway, this is from UpToDate:
DSM-5 diagnostic criteria — The American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) diagnostic criteria for ADHD are described below [53]. These criteria are used to diagnosis ADHD in both children and adults. Changes from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) include modifications to criterion B, which now requires that several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years, versus age 7 years in DSM-IV. Some examples of ADHD symptom manifestations in adults were added to the criteria, which are described as follows:
●A. A persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development, as characterized by (1) and/or (2):
•1. Inattention – Six (or more) of the following symptoms have persisted for at least six months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities:
Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required. The patient often:
-a. Fails to give close attention to details or makes careless mistakes in schoolwork, at work, or during other activities (eg, overlooks or misses details, work is inaccurate).
-b. Has difficulty sustaining attention in tasks or play activities (eg, has difficulty remaining focused during lectures, conversations, or lengthy reading).
-c. Does not seem to listen when spoken to directly (eg, mind seems elsewhere, even in the absence of any obvious distraction).
-d. Does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (eg, starts tasks but quickly loses focus and is easily sidetracked).
-e. Has difficulty organizing tasks and activities (eg, difficulty managing sequential tasks; difficulty keeping materials and belongings in order; messy, disorganized work; has poor time management; fails to meet deadlines).
-f. Avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (eg, schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers).
-g. Loses things necessary for tasks or activities (eg, school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones).
-h. Is easily distracted by extraneous stimuli (for older adolescents and adults, may include unrelated thoughts).
-i. Is forgetful in daily activities (eg, doing chores, running errands; for older adolescents and adults, returning calls, paying bills, keeping appointments).
•2. Hyperactivity and impulsivity – Six (or more) of the following symptoms have persisted for at least six months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities:
Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or a failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required.
-a. Often fidgets with or taps hands or feet or squirms in seat.
-b. Often leaves seat in situations when remaining seated is expected (eg, leaves his or her place in the classroom, in the office or other workplace, or in other situations that require remaining in place).
-c. Often runs about or climbs in situations where it is inappropriate. (Note: In adolescents or adults, may be limited to feeling restless.)
-d. Often unable to play or engage in leisure activities quietly.
-e. Is often "on the go," acting as if "driven by a motor" (eg, is unable to be or uncomfortable being still for extended time, as in restaurants, meetings: may be experienced by others as being restless or difficult to keep up with).
-f. Often talks excessively.
-g. Often blurts out an answer before a question has been completed (eg, completes people' sentences; cannot wait for turn in conversation).
-h. Often has difficulty waiting his or her turn (eg, while waiting in line).
-i. Often interrupts or intrudes on others (eg, butts into conversations, games, or activities; may start using other people's things without asking or receiving permission; for adolescents and adults, may intrude into or take over what others are doing).
●B. Several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years.
●C. Several inattentive or hyperactive-impulsive symptoms are present in two or more settings (eg, at home, school, or work; with friends or relatives; in other activities).
●D. There is clear evidence that the symptoms interfere with, or reduce the quality of, social, academic, or occupational functioning.
●E. The symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder and are not better explained by another mental disorder (eg, mood disorder, anxiety disorder, dissociative disorder, personality disorder, substance intoxication or withdrawal). (See 'Differential diagnosis' below.)
Specify whether:
●Combined presentation: If both Criterion A1 (inattention) and Criterion A2 (hyperactivity-impulsivity) are met for the past six months.
●Predominantly inattentive presentation: If Criterion A1 (inattention) is met but Criterion A2 (hyperactivity-impulsivity) is not met tor the past six months.
●Predominantly hyperactive/impulsive presentation: If Criterion A2 (hyperactivity-impulsivity) is met and Criterion A 1 (inattention) is not met for the past six months.
Specify if:
●In partial remission: When full criteria were previously met, fewer than the full criteria have been met for the past six months, and the symptoms still result in impairment in social, academic, or occupational functioning.
Specify current severity:
●Mild: Few, if any, symptoms in excess of those required to make the diagnosis are present, and symptoms result in no more than minor impairments in social or occupational functioning.
●Moderate: Symptoms or functional impairment between "mild" and ''severe" are present.
●Severe: Many symptoms in excess of those required to make the diagnosis, or several symptoms that are particularly severe, are present, or the symptoms result in marked impairment in social or occupational functioning.
ADHD criteria in DSM-5 are applicable to diagnosis in children and adults, and include examples of adult manifestations of the disorder [21]. Examples of hyperactivity and impulsivity that are likely to be manifested by adults with ADHD include fidgetiness and verbal impulsivity, respectively.
16 notes
·
View notes
Text
just did some research on the mental disorder i have (ADHD)
i always thought that there was a big distinction between ADD and ADHD because when i was younger (and diagnosed) there was still a distinction...but now there’s not. now it’s just ADHD with different subtypes and i have the inattentive ADHD (previously known as just ADD) basically meaning i don’t have any of the symptoms that hyperactive-impulsive ADHD types have.
...ya learn something new every day
but it’s been a while since i’ve really thought about it and after researching it and reading the symptoms i kinda started to cry because i didn’t realize how it affected me still as an adult. in case you’re curious, here are the symptoms for inattentive ADHD...because it’s more common than people realize
Often fails to give close attention to details or makes careless mistakes
Often has difficulty sustaining attention
Often does not seem to listen when spoken to
Often does not follow through on instructions and fails to finish projects
Often has difficulty organizing tasks and activities
Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort
Often loses things necessary for tasks or activities
Is often easily distracted by extraneous stimuli
Is often forgetful in daily activities
#every single one of these symptoms is me#adhd#add#adhd inattentive#it me#i'm a little shook#its just been so long since i've thought about it#mental disorder#psychology#mine#mental disorder awareness#adhd awareness#awareness#psa#mental health
17 notes
·
View notes
Text
OH right ok adhd things maybe
A. A persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development, as characterized by (1) and/or (2):
1. Inattention: Six (or more) of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities:
Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required.
a. Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or during other activities (e.g., overlooks or misses details, work is inaccurate).
well as a kid, yeah. little mistakes in my math, using the wrong cursive letter in my spelling tests. wouldn’t rinse all the soap off the dishes, that sort of thing. the closest thing i can think of now, though, is i often have little mistakes in my fics cause i don’t bother to proofread? i’m just like “okay i’m finished posting time is now” (or when i do proofread i don’t do it as thoroughly as i should). not sure this is Enough though
b. Often has difficulty sustaining attention in tasks or play activities (e.g., has difficulty remaining focused during lectures, conversations, or lengthy reading).
eh. not sure. as a kid, for sure i spaced out in classes. i’d do the whole “okay i’m gonna pay attention. ........fuck. okay i’m gonna pay attention. .........fuck. okay for real now i’m gonna--fuCK” on a semiregular basis? but not like. every day? uh. and for sure i spaced out during lectures, and i remember having to reread pages over and over cos the words just weren’t going in. now, though, i just space out when people are talking sometimes, and have a little trouble focusing on audio stories. don’t really have trouble focusing on like, visual stuff or actions or whatever. just the listening. so, again, not sure it’s Enough
c. Often does not seem to listen when spoken to directly (e.g., mind seems elsewhere, even in the absence of any obvious distraction).
um. i dunno? i’m not other people so i can’t be sure how i seem to them
d. Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., starts tasks but quickly loses focus and is easily sidetracked).
for sure did this as a little kid. like, constantly. i’d forget to do chores, i’d forget to do homework, i’d forget to bring homework home in the first place, i’d forget to bring library books, etc. etc. now, though, i tend to follow through on my shit? or. i mean. sometimes i’ll forget chores still, and self-assigned tasks often end up not getting done, but like. eh
e. Often has difficulty organizing tasks and activities (e.g., difficulty managing sequential tasks; difficulty keeping materials and belongings in order; messy, disorganized work; has poor time management; fails to meet deadlines).
maybe. maybe. i was always super messy as a kid and i’m still not super organized now, my locker’s a goddang disaster a little bit. and as for deadlines i mean. i don’t have any anymore, and i only ever missed one deadline w/school, just. just the once. but i also did papers at the last minute constantly so there’s your poor time management i guess. and my room in my apartment was a small disaster 95% of the time, so. yeah, i guess i have trouble with that. sure. i’ll call this one. i’ve got it.
f. Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (e.g., schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers).
yes and no, i guess? like i said, i always wrote papers at the very last minute, and i’ve been putting off reworking my resume for the last uhhh. couple months now, so there’s that. and i keep putting off story-writing, which i love the fuck out of, because, y’know, y’sorta have to know what happens for that, and figuring out what happens is like, effort. but i don’t have the Extreme executive dysfunction that i’ve seen other people struggle with, so i’m kinda over here like. uh. [shrug emoji]. can i give myself half on this one? i’d give myself half on this one
g. Often loses things necessary for tasks or activities (e.g., school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones).
i mean it varies like hell, y’know, it’s worse when i’m more stressed, but generally...yeah. yeah, for sure, this is me. i lose shit all the time. most notably my phone, in the nowadays-times, but as a kid i was constantly losing pencils and books and notebooks and shit. and i’d forget where i put my keys, and my stim toys, and all kindsa shit. i’d put things down and almost immediately forget where they were. i’d be holding something and freak out like w here the hell is it????? so. yeah. definitely got this one
h. Is often easily distracted by extraneous stimuli (for older adolescents and adults, may include unrelated thoughts).
mm...dunno? maybe. maybe. i’m not sure, i’ve never really thought about it or been looking for it, but yeah i guess when i space out it’s my own thoughts i’m distracted by? so. maybe? another half-point here even though u can’t actually fuckgin do half points & that’s not how it works
i. Is often forgetful in daily activities (e.g., doing chores, running errands; for older adolescents and adults, returning calls, paying bills, keeping appointments).
well? yeah, i guess. but it depends what y’mean by often, y’know? like i’ve never forgot an appointment (though i nearly did, once, but again y’know that’s only nearly--though social anxiety could be a factor in my not forgetting i spose). and i’ve only rarely forgot the other things. like, i forgot to pay a bill once. and i NEARLY forgot to pay pg&e several times (only remembered bc text reminders from roommate). and i forget to text people back & return emails n stuff, sometimes. (the. emails especially. all summer long i meant to email back my old professor some clean copies of my papers to be used as examples and just fuckgn forgot over and over and now i feel like it’s too weird, so that kinda sucks.) so i guess? i can claim this one for me also, fairly definitively
2. Hyperactivity and impuisivity: Six (or more) of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities:
Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or a failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required.
a. Often fidgets with or taps hands or feet or squirms in seat.
bruh i can’t even halfway dick around abt this one i for sure got it. i’m rockin back n forth right goddamn now & like, i could stop, sure, definitely, but i’m not gonna bc a) stimming’s good as hell, and b) even if i tried to stop i’d start again in a bit bc i’m just Like That i wasn’t made to be still
b. Often leaves seat in situations when remaining seated is expected (e.g., leaves his or her place in the classroom, in the office or other workplace, or in other situations that require remaining in place).
oh hellllllll no. nope. nuh-uh. never, my dude. Against The Rules.
c. Often runs about or climbs in situations where it is inappropriate. (Note: In adolescents or adults, may be limited to feeling restless.)
for sure i did this as a kid. like, definitely. “no running in the house,” i got told, over & over & over. also i ran up n down the stairs in the neighbor’s house once & got in hella trouble (that’s sort of a social rules thing i missed, but also i was just. man i was wired). now i sorta? like i don’t run about, but i def. pace in places most ppl don’t pace? and occasionally maybe i feel restless sort of i dunno what are emotions anyway
d. Often unable to play or engage in leisure activities quietly.
okay so listen. this is sort of. sometimes, absolutely, yes, i gotta fuckin talk, but other times it’s like. totally chill being dead silent for hours on end. which i realize the latter in no way invalidates the former automatically, but like. how often is often, u know? and how “unable” is “unable”? (for sure as a kid i struggled with this a fair bit though)
e. Is often “on the go,” acting as if “driven by a motor” (e.g., is unable to be or uncomfortable being still for extended time, as in restaurants, meetings; may be experienced by others as being restless or difficult to keep up with).
i meaaaan this feels to me a lot like the earlier ones about stimming & getting up when other folks don’t & tbh to be honest honestly i don’t see how it’s supposed to be different. but anyway in any case, yeah, i guess, it feels weird to be still for too long. like i can do it but why would i? i’mma jus stim thanks
f. Often talks excessively.
like again this depends my dude. how fuckign often is often. also it’s situational even aside from definitions of “often.” like. if i’m socialing & not anxious, holy mfcuk i’ll talk ur goddamn ears off like a chatterbox i’ll almost feel like i can’t shut myself up like i CAN but it’ll feel a bit weird u know to just end the motormouth so abruptly. but then also on the other hand i am often very very quiet. and not always jus for anxiety reasons. though yes also for that bc when anxious i don’t talk generally speaking i’m jus sort of There. also uh. uhhhhh. uh. uh. fuck uh. i uh. i. uh. fuck. what was i saying oH RIGHT. when i was little i got told i was doing mindless chatter like Literally So Much, and that i needed to work on my “i.d., internal dialogue”, like, all the time my dude bc i would just talk talk talk talk talk (which like autism hyperverbality + trouble recognizing social rule of Shut Up & social cue of They Annoyed, but. both maybe idk)
g. Often blurts out an answer before a question has been completed (e.g., completes people’s sentences; cannot wait for turn in conversation).
well. sort of yeah. completing people’s sentences, yeah. and i interrupted a lot as a kid. and. yes answering questions ‘fore they’re done, sure, i’ve done that, yeah
h. Often has difficulty waiting his or her turn (e.g., while waiting in line).
nah, waiting in line is easy. that’s what we got phones for my dude. u read sth & u good to go.
i. Often interrupts or intrudes on others (e.g., butts into conversations, games, or activities; may start using other people’s things without asking or receiving permission; for adolescents and adults, may intrude into or take over what others are doing).
well i mean? like i guess? i. i guess, yeah, kind of. interrupting was a thing i did as a kid a fair bit. and sometimes i still sort of, like. “hey can i show u sth” when i know ppl are busy bc Wanna Share!! Excited!! u know. but i don’t interrupt in conversations that aren’t mine too much i don’t think? um. but taking over what folks are doing, that. sounds uh. familiar even if i can’t think of specific examples. but i figured that was more of me being, like, a control freak a little bit? like. gotta make sure they Do It Right u know
B. Several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years.
idk if u’d call it several but the ones that’re existing, sure, yes
C. Several inattentive or hyperactive-impulsive symptoms are present in two or more settings (e.g., at home, school, or work; with friends or relatives; in other activities).
i mean. yeah
D. There is clear evidence that the symptoms interfere with, or reduce the quality of, social, academic, or occupational functioning.
i mean?? as a kid i guess maybe, but since then i’m ? pretty well good i think. or. like. IF these were the things interfering in college then like i guESS there’s evidence. but i’m done w/college now so it’s just kinda like. eh. and what traits i do seem to maybe or probably have ain’t that bad? and so. i’unno my dude. i’unno
E. The symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder and are not better explained by another mental disorder (e.g., mood disorder, anxiety disorder, dissociative disorder, personality disorder, substance intoxication or withdrawal).
all this is like, irrelevant again bc of point D, but regardless, for the sake of completion will reiterate: is entirely possible (& likely) that the few significantly impactful thingamajigs could be bc anxiety/autism/etc.
IN CONCLUSION: ?????? lemme check numbers real quick
for inattentive it’s POSSIBLE i meet the criteria, but i only have 3 down for solid yes’s, and then there’s like 4 ??????s i think
for hyperactive/impulsive uhhhh i think there’s 3 i said yeah to as well, & 1 i said probably to, and then ?? a couple others i was just kinda Who Knows at
so uhhhhh yeah the question marks sound about right i spose. i’mma mark this down for a solid “Maybe,” w/a side of “look into it more y’dingdang goofus”
2 notes
·
View notes
Text
ADHD

Attention deficit hyperactivity disorder is a neurological condition defined by a consistent pattern of inattention and/or hyperactive impulsivity that interferes with daily functioning in at least two settings.
Symptoms of Inattentive ADHD
Fails to give close attention to details or makes careless mistakes in schoolwork, work, or other activities.
Has difficulty sustaining attention in tasks
Does not seem to listen when spoken to directly.
Does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (not due to oppositional behavior or failure to understand instructions).
Has difficulty organizing tasks and activities.
Avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort
Loses things necessary for tasks or activities
Easily distracted by extraneous stimuli.
Forgetful in daily activities.
Symptoms of Impulsive ADHD
Often fidgets with or taps hands or feet or squirms in seat.
Often leaves seat in situations when remaining seated is expected
Often restless
Is often “on the go,” acting as if “driven by a motor” (e.g., is unable to be or uncomfortable being still for extended time, as in restaurants, meetings; may be experienced by others as being restless or difficult to keep up with).
Often talks excessively.
Often blurts out an answer before a question has been completed (e.g., completes people’s sentences; cannot wait for turn in conversation).
Often has difficulty waiting his turn (e.g., while waiting in line).
0 notes
Text
and like "how often do you have trouble listening to someone, even when they are speaking directly to you — like your mind is somewhere else?" or "How often do you avoid, dislike, or are reluctant to engage in tasks that require sustained mental effort or thought?"
isn't...isn't that everyone ? Is that not normal ? It feels like normal ??
taking adhd tests online to see if it's worth talking to a doctor feels like taking the gay quiz.
6 notes
·
View notes
Note
heyyyy i think i might have adhd but i'm not sure bc i'm not all that hyper (i'm actually... the quietest person in my class oops), but i still have a lot of the other symptoms - stress, forgetfulness, hyperfocusing.. all that "good stuff." can people have adhd but be very quiet?
Yes! You can!
In 1994, the DMS-IV (a fun little document that lists all the fun diagnostic criteria for mental illnesses and the like) combined ADD and ADHD into one diagnosis with 3 subtypes. Primarily Inattentive, Primarily Hyper-Active, and Combined Type ADHD.
When someone has Primarily Inattentive type ADHD they experience (as according to the DMS-V):
Trouble with attention to details; making careless mistakes
Difficulty sustaining attention
Does not seem to listen when spoken to directly
Does not follow thru on instruction; fails to finish schoolwork, chores, etc.
Difficulty organizing tasks & activities
Avoids/dislikes/reluctant to engage in tasks that require sustained mental effort
Loses things necessary for tasks or activities
Often easily distracted by extraneous stimuli
Often forgetful in daily activities
To be diagnosed, you have to experience at least six symptoms (or five if you are at least 17) since age 7-12. If that sounds like you, you very well could have ADHD!
#i have 0 problem with self dx as long as there is basis for it#so if it sounds like u buddy#go for it#if its getting difficult in school or in other areas tho#i recommend seeking out assistance and stuff????#Anonymous
20 notes
·
View notes
Text
whine post alert
god i’m going to fail classes this semester for actual realsies. like our school has pass/no credit and i still might need to retake a course. fuck me. the executive dysfunction has been so bad i literally can barely leave my room. for weeks now. honestly i have been keeping up with schoolwork by self destructing my health since high school and like the coping mechanisms are just. not happening anymore. i think i have turned in every single assignment since we got sent home within 5 minutes of the deadline or late sometimes hilariously late and i just turned in a half finished final project sooooo. and why are BOTH my hard finals tomorrow?
i literally, actually, no exaggeration this time, can not fucking deal with this successfully. i may have another cry now to bring my total for today up to like a full hour. i know failing a class isnt the end of the world but i have NEVER gotten below a b+ in anything in my whole entire life and it feels like its a serious blemish on my worth as a person that i cant keep it together enough to learn stuff that i’m really interested in.
i know its so bad i’ve known it’s really fucking bad i’m the one living it, I’m still so upset i couldn’t get an adhd dx. i know myself i KNOW the depression is secondary to whatever it is that makes my executive functioning absolutely rock bottom shit tier because i wasnt depressed as a kid and i STILL had these issues. then i was suicidal in middle school and this has only got worse since then, and THEN i was in a great place emotionally for the last two years of high school but thats exactly when i started seriously never ever getting any god damn sleep. and my sleep pattern my whole life has been MUCH more in line with typical adhd than depression. also yeah my mood is always bad but a) we literally live in a dystopia i think its excusable and b) im always under tons of stress because im incapable of doing work. i have no issue enjoying myself when i actually clear my responsibilities and get to do fun stuff, and my self esteem is fine except for how im frequently guilty about being.... incapable.... of doing work. unless i ONLY have depression in the body and not in my emotions which really doesn’t sound like a real thing i do not know why every doctor i talk to insists that must be the only issue. there have been at least 4 so far
like. get a load of this
me:
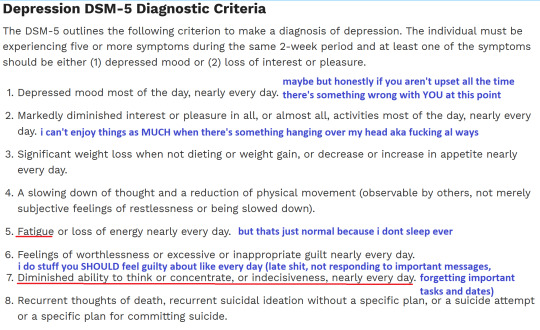
and
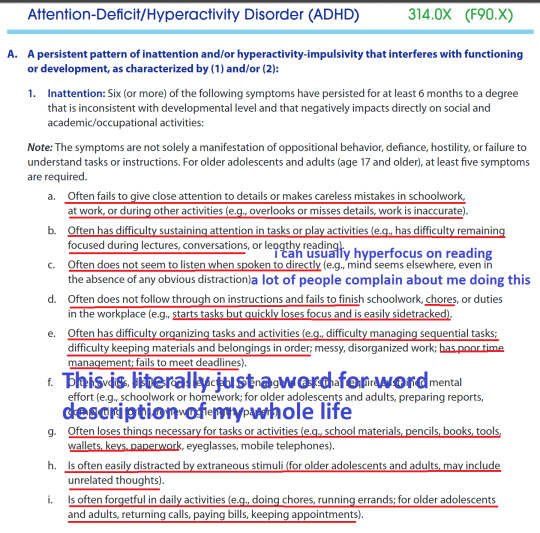

(the covered text is: “Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (e.g., schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers).” like this is THE problem this is it this is what is ruining my life)
the genius psychs i keep seeing: you have depression not adhd. you probably have just never tried using a planner. give me $300
#text post#if you re//blog it is fucking on sight#long post#you better believe im deleting this when i remember it exists l m a o
0 notes